medication and participation a qualitative study of patient experiences with antipsychotic drugs....
TRANSCRIPT
Medication and participation
A qualitative study of patient experiences with antipsychotic drugs.
Geir Lorem

Study aim
• User experiences with treatment• Their participation/influence in decision-making processes regarding own
treatment• How do they perceive the relationship to clinicians
Why do we write about
• Medication• Involuntary treatment/care• Stress
Developing the perspective
• There is an increased emphasis on the patient perspective, that is, the patient’s sense of autonomy and empowerment.
• Studies suggest that it is essential to take advantage of patients’ internal resources and that individual action plans can empower patients and improve their experience of care.
Different variations on patient adherence
COMPLIANCE
• Actual use of drugs seen against prescription
• Actual behavior seen against medical recommendations
• Result of taking the drugs
• Vermeire, E., Hearnshaw, H., VanRoyen, P., & Denekens, J. (2001). Patient adherence to treatment: three decades of research. A comprehensive review. Journal of Clinical Pharmacy and Therapeutics, 26(5), 331-342.
CONCORDANCE
• More active form of adherence• Treatment aims to generate
clinically meaningful outcomes in agreement with patient preferences and goals
• a composite of knowledge, health beliefs and collaboration
• Snowden, A., & Marland, G. (2012). No decision about me without me: concordance operationalised. Journal of Clinical Nursing, n/a-n/a. doi: 10.1111/j.1365-2702.2012.04337.x

But …
• Despite these ideals, we know that many patients experience pressure in ‘shared decisions’ (Haman, et al)
• Other challenges for patient autonomy occurs when the patient is temporarily ‘unavailable’ to provide valid consent (Appelbaum, 2004).
• The link between psychosis and lack of insight is problematic to user involvement (Grisso & Appelbaum 1996).
• Expectation of meaning is crucial for communication with the user (Lorem 2006;2008)
Question
• One could ask whether the expectations of the patients’ role is really in accordance to patient centered medicine.

Project overview
Insight and user participationAwareness, insight and
decision-making-competenceUser experience with
participationEvidence based and user based
knowledge
Sub study 1: 2006-2009 Sub study 1: Ongoing Sub study 3: Ongoing Post-doc:Participants: Staff InterviewsResults: Insight, cooperation, understanding and awareness of suffering
PhD project:Participants: users/patients with exp from district psych. wardsMethod: Interviews/narrative approachesaim: user perspectives on insight and participation
PhD project:Participants: StaffMethod: Ethnographical study (interviews, focus groups, participation) Aim: attitudes and praxis regarding participation
Student project:The importance of participation for patients with psychotic disordersMethods: Interviews/narrative approachesResults: Antipsychotics, coercion, stress/coping skills
Methods
• Design– This article reports findings from interviews with patients at a
hospital in Norway. – Narrative interviews with 9 participants. – Aiming to articulate their experiences, self-understanding and
assessment of situations– Particularly useful in cases of a major life disruption that
participants wish and are able to describe through detailed stories.
– Participants’ stories ranged from the episodic to more complex, long-term events that could describe extensive epochs in their lives.
– All had stories about medication and participation.

Narrative approaches
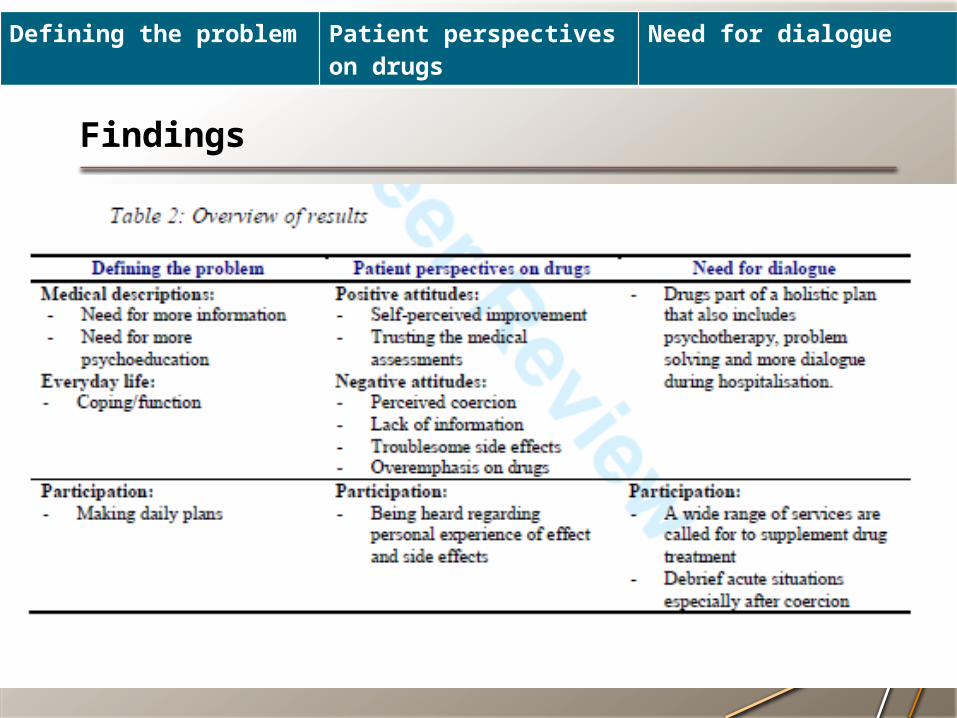
Findings
Defining the problem Patient perspectives on drugs Need for dialogue

Need for information
– Little or no information– It’s very important for the course of the disease that one has good
information in order to live with the disease. It’s not just drugs that are important but also how you spend your life, that you pick up early signs of when things start going a little wrong, and take action then, to prevent it going seriously wrong. (Participant)
– Participation on daily basis– I was treated as a person that was not supposed to hear anything, know
anything, think anything, and that should only be . . . well, like ‘vegetables’, like plants [ . . . ] that need to be treated. And that cannot care for themselves, and that are not supposed to participate in that. (Participant)
Defining the problem Patient perspectives on drugs Need for dialogue
Drug treatment • Self-perceived improvement
– They give me drugs that clearly work [ . . . ] They’ve had a good effect. I notice that, in my daily living, I’m better now than I was before. (Participant)
– I think I’ve tried all the drugs now, and it feels like that’s all I’ve done: Increasing and decreasing dosages to see whether this or that kind suited me. (Participant)
• Perceived coercion– Most recalled experiences of not being listened to and having no influence on their drug
treatment during hospitalization: They just said ‘swallow’ and I wasn’t allowed to ask questions about the drugs. (Participant)
– Yes, you can refuse to take these tablets, but if you do, then there’s no reason for you to stay here any longer. Then you’ll be discharged immediately. (Participant)
• Lack of information– Now: take this, and now: take that’, and I don’t know what I’m taking. They just tell me the
name of the drug and that doesn’t tell me anything. (Participant)
• Troublesome side effects– The first thing he did was change my drugs. I hadn’t even spoken to him before he changed
my drugs. And it felt like I was . . . that the decisions were being made over my head. [ . . . ] that I felt that nobody was taking any notice of me. (Participant)
• Overemphasis on drugs– Instead of talking to you about your problems or your fears or whatever you have or
don’t have, they say all the time that you should calm down until they’ve found the right drugs for you. (Participant)
Defining the problem Patient perspectives on drugs Need for dialogue
Need for dialogue
• But no one talks to you there. Even if you’ve had a shock, something terrible has happened to you, there’s nobody . . . who prepares you for your future life that talks to you about it. [ . . . ] I think most people who have a serious problem will respond positively if they have someone to talk through the problems. (Participant)
• It was just me and my problems that I had to focus on, right? It was pretty terrible. I felt as if I was going to explode in that bed, in that damned bed. [ . . . ] It’s not up to them to get your mind to switch off . . . when you’re actually trying to tackle the problems. All they’re interested in is ‘turning you off’. But you cannot find solutions to your problems that way. (Participant)
• You know, I want to know things and understand quite a bit. They can discuss things with me, and I want to work things out instead of being afraid. [ . . . ] I always want to know what’s going on with me, what’s happened and what I experience. [ . . . ] In order to calm myself down I need to find out about what’s going on with me, and what they’re trying to do. (Participant)
Defining the problem Patient perspectives on drugs Need for dialogue
What is autonomy?
• The participants emphasized autonomy and control and wanted to be heard regarding their previous medication experiences.
• Respect for patient autonomy implies that health personnel not only acknowledge people’s right to hold views, to make choices and to take actions based on their personal values and beliefs but also encourage or maintain others’ capacity for autonomous choice. (Beauchamp and Childress, 2009)
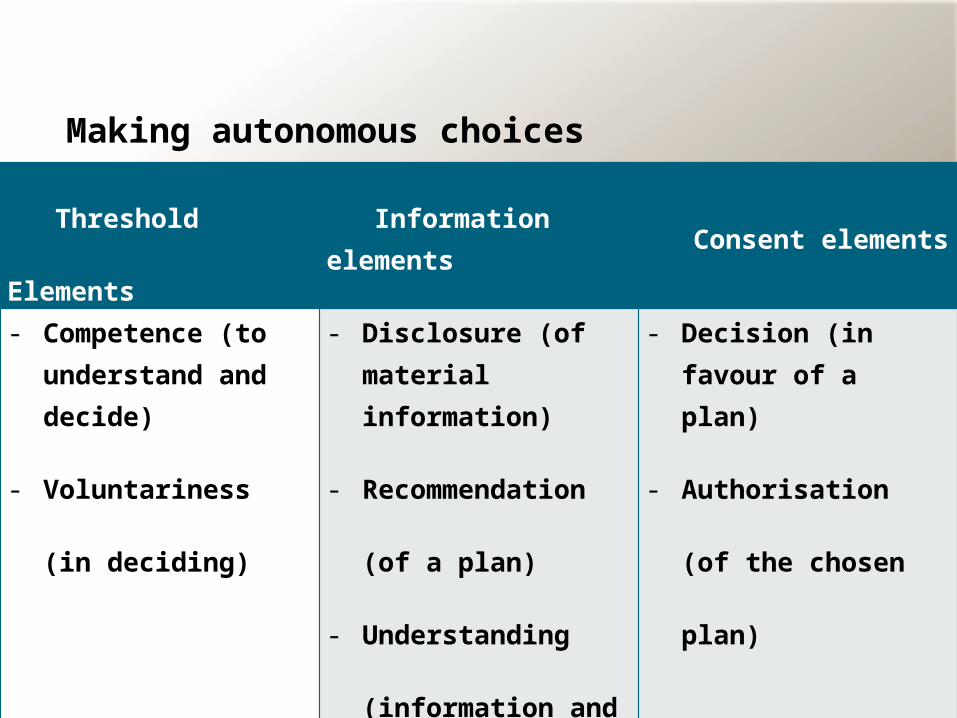
Making autonomous choices
– Therefore, informed consent implies three elements
Threshold Elements Information elements Consent elements
- Competence (to understand and decide)
- Voluntariness (in
deciding)
- Disclosure (of material information)
- Recommendation (of a
plan)
- Understanding
(information and plan)
- Decision (in favour of a plan)
- Authorisation (of the
chosen plan)
Discussion:Why do they not make their own choices?
• The most interesting part, they do not fall into the patient stereotypes• It is the meds that make me ill …
• When they complain about the drugs, the main complaint is that the staff has not followed the ordinary concerns to assure autonomy.
• In a sense, they expect what we all expect when it comes to medical decision. To be informed, to choose, and that the choices are respected.
Discussion:Debrief and Advance directives
• Advance directives allow patients to appoint surrogate decision-makers and to make treatment choices in advance should they later become incompetent.
• They aim to increase autonomy by encouraging patients and clinicians to discuss future mutually acceptable approaches to care.
» Appelbaum, 2004; Szmukler & Holloway, 2000
Debrief and dialogue
• Patient preferences could be reconstructed by – (a) considering past and present wishes and the factors that
person would consider if able to do so,– (b) permitting participation and improving the ability to
participate in any decision affecting the patient, – (c) consulting the views of other appropriate people who have
a reasonable understanding of the patient’s wishes and interests, and
– (d) assessing whether the purpose for which any action or decision is required can be as effectively achieved in a manner that restricts the individual’s freedom of action less.
» Szmukler and Holloway (2000)
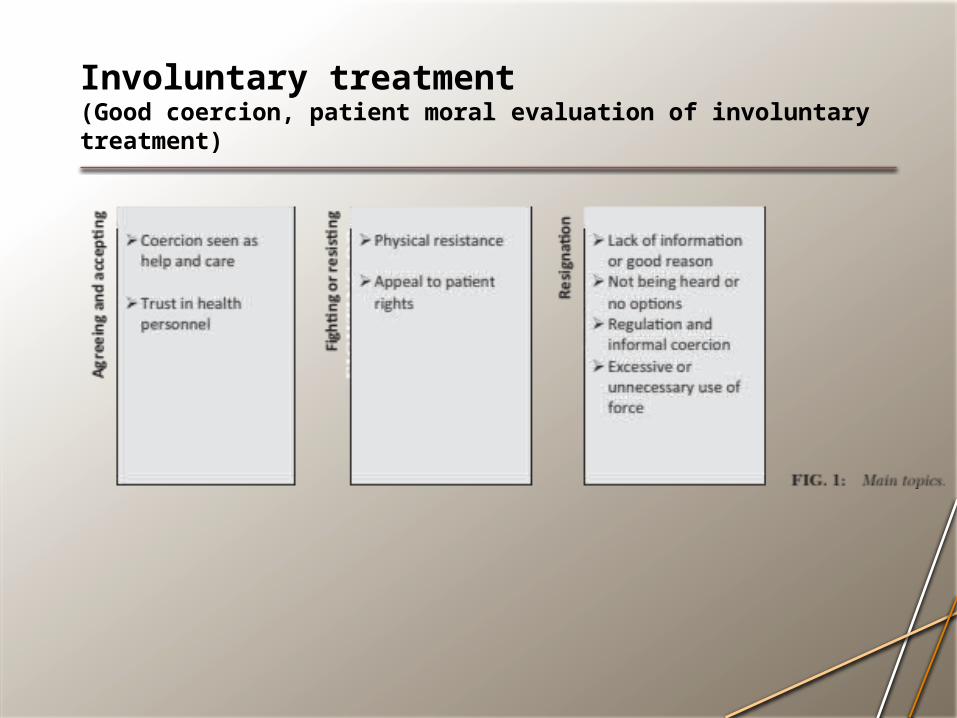
Involuntary treatment(Good coercion, patient moral evaluation of involuntary treatment)
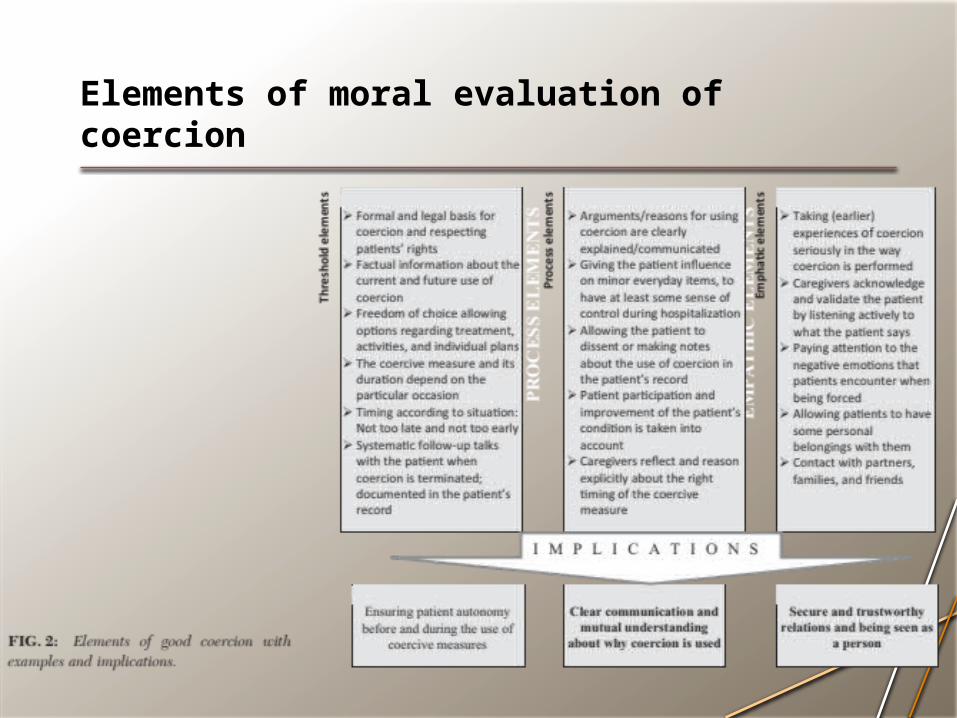
Elements of moral evaluation of coercion
Conclusion• Improving the elements of consent will not only strengthen
participation but may also lead to better relationships and thus better experiences with clinicians.
• use debriefing to help summarize and provide two-way feedback on the patient’s positive and negative experiences
Background
• Follow up on insight– The first project focused on break down of communication, and the
isolation that it entails. • Now we asked clinicians:
• What is insight?• How do you know that a person lacks insight?• And what do you do then?
Insight
• General opinion:– To know that you have an illness, knowing what it is, and how to deal
with it! (participant, psychiatrist)
» Lorem, G. F. (2009). The Patient Experience with Psychosis as Seen from the Helper’s Point of View. In K. R. Myers (Ed.), The Patient - Global Interdisciplinary Perspectives (pp. 103-124). Oxford: Inter-Disciplinary Press.
Insight
• The MacArthur group’s opinion– Understanding relevant information– Recognize need for assistance– Understand the consequences of the choices– Being able to communicate a choice).
» Appelbaum, P. S., & Grisso, T. T. (1998). Competence to consent to voluntary psychiatric hospitalization: a test of a standard proposed by APA. American Psychiatric Association. Psychiatric services, 49(9), 1193-1196.
Insight
• The clinicians’ stories– a far more nuanced picture is revealed. – Insight is connected to how the patient function and copes with
everyday life– Compliance and cooperation. – Human aspects: There are key aspects of the patient experiences
escapes the medical language, and that these are crucial to understand their choices, actions and suffering.
» Lorem, 2009
Insight
The patient
Adherence
Intentional actionsBehaviour
Rationality
Social life