medicina nucleare, azienda ospedaliero- universitaria di ... · medicina nucleare, azienda...
TRANSCRIPT
Brain lesions:
PET/CT
Paolo CastellucciMedicina Nucleare, Azienda Ospedaliero-
Universitaria di Bologna Policlinico S.Orsola-Malpighi
Reggio Emilia17 aprile 2010
MR is the Imaging of choice in brain lesions. However, in some applications the accuracy of MR is limited:
1) Grading
2) Guide biopsy
3) Detect the presence of relapse after surgery and /or RT
4) Monitoring therapy & prognosticate
PET (with different radiopharmaceuticals) is an imaging method potentially useful in case of inconclusive findings at MR.REMEMBER: MR is the imaging method of choice !
Brain PET/CT:
clinical applications1. Grading
2. Guide stereotactic biopsy
6. Prognosticate
5 Monitoring therapy
3. Suspect of relapse after surgery and /or RT.
4. PET-guided contouring for RT
33 newly diagnosed glioma.LAT1 expression was higher in high grade gliomas.LAT1 expression was correlated with SUVmax
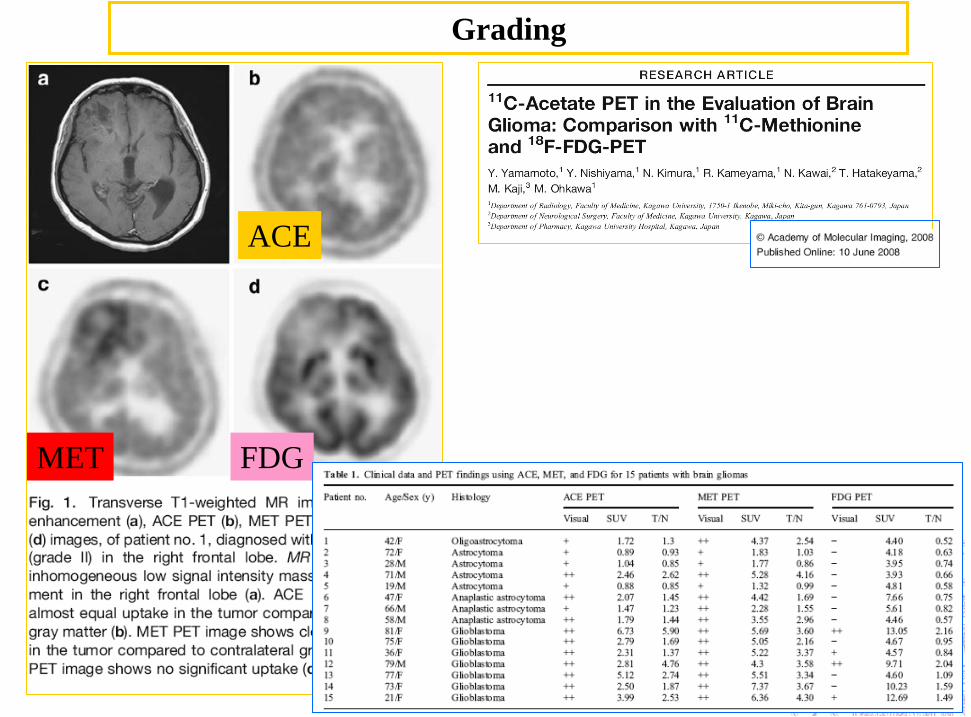
ACE
MET FDG
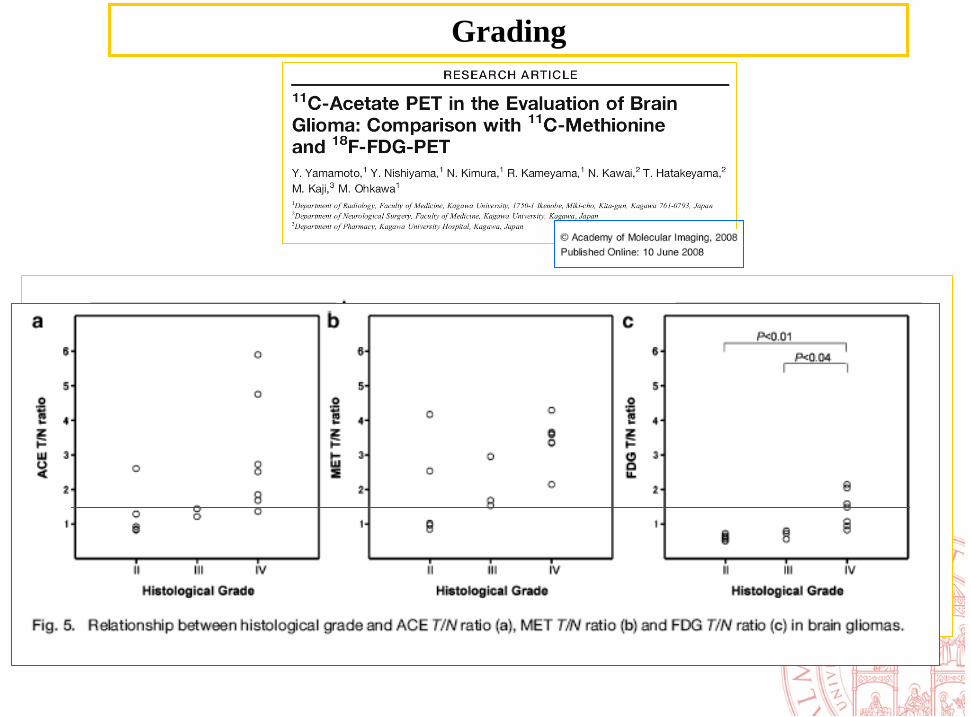
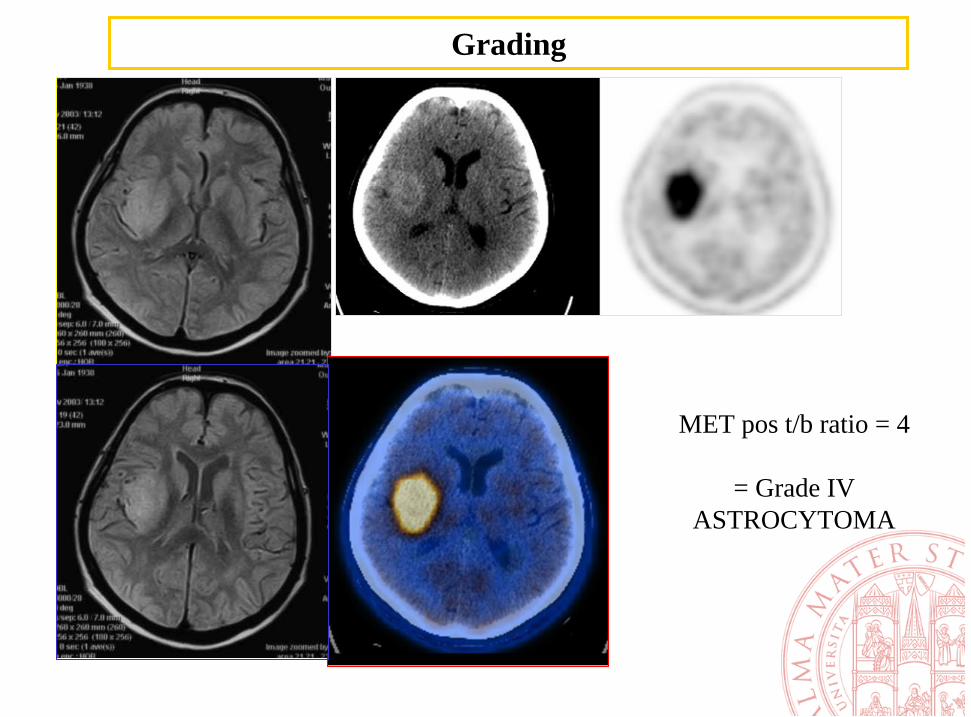
Grading
Grading

Grade III astrocyt
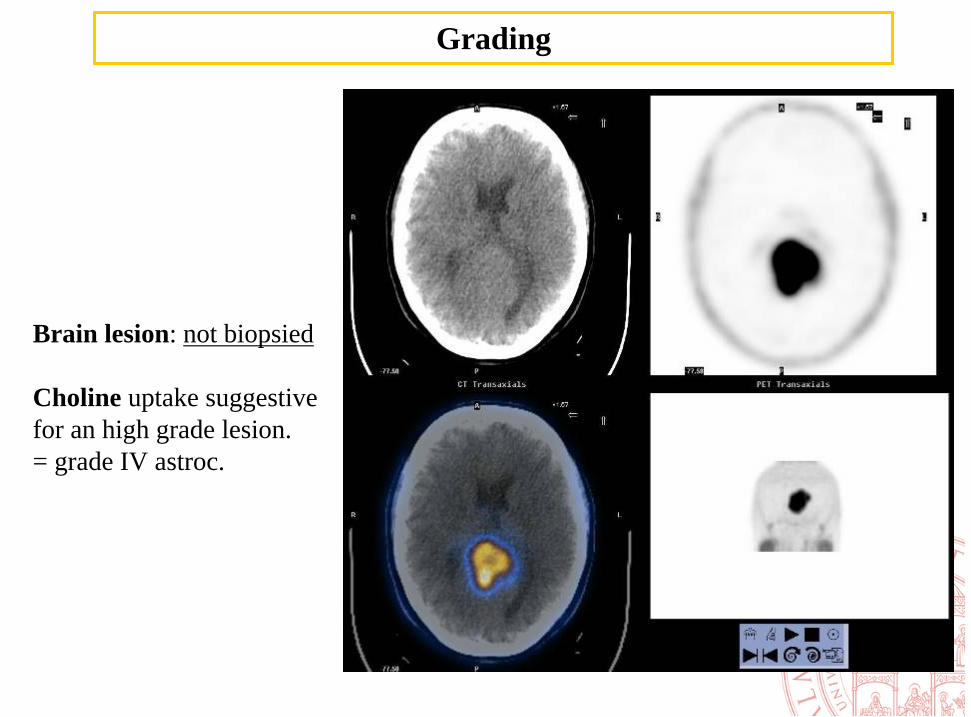
Brain lesion: not biopsied
Choline uptake suggestive for an high grade lesion.= grade IV astroc.
Grading
Grading
MET pos t/b ratio = 4
= Grade IV ASTROCYTOMA
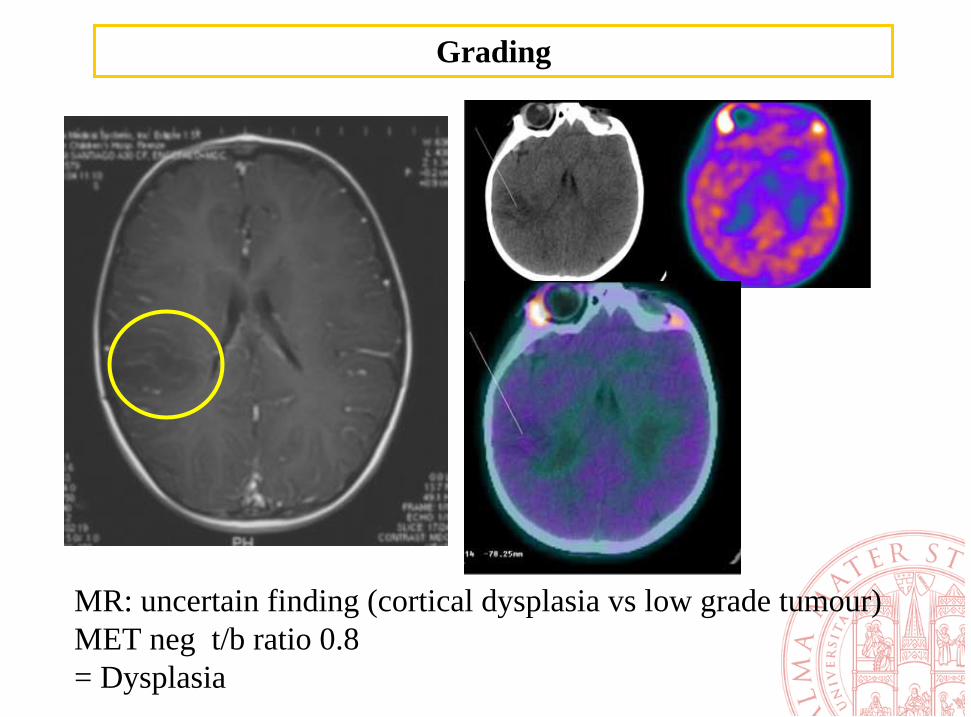
MR: uncertain finding (cortical dysplasia vs low grade tumour)MET neg t/b ratio 0.8= Dysplasia
Grading

FDG NEG
MET POS
= Astroc. low grade II
Grading
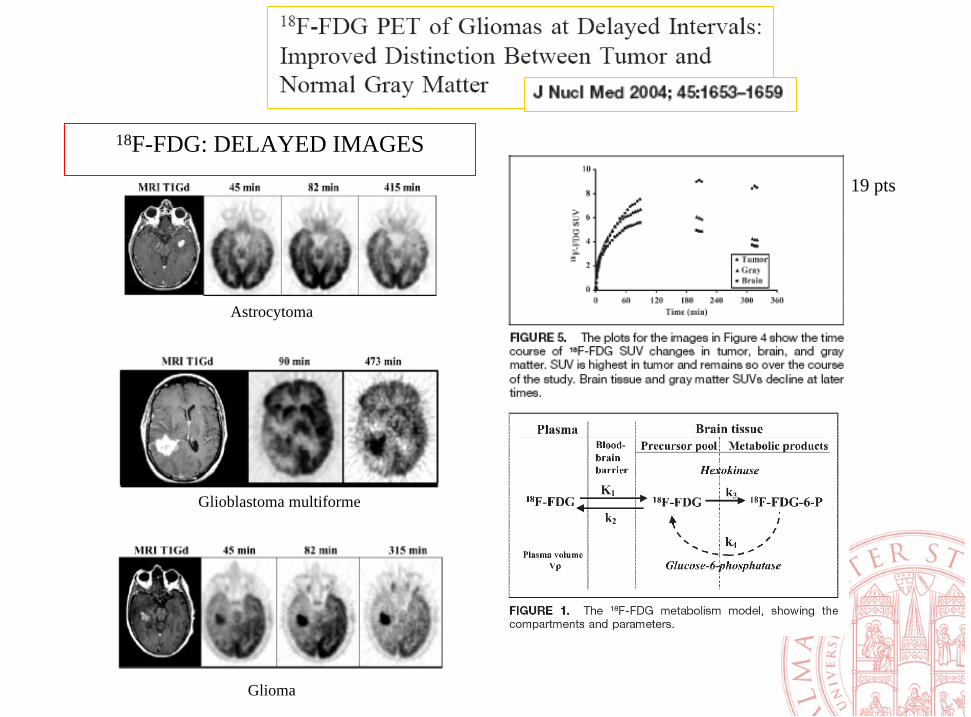
18F-FDG: DELAYED IMAGES
Astrocytoma
Glioblastoma multiforme
Glioma
19 pts
1. Grading
2. Guide for stereotactic biopsy
6 Prognostic informations
5 Therapy response evaluation
3. Suspect of relapse after surgery and /or RT.
4. PET guided contouring for RT
Brain PET/CT:
clinical applications
PET guided biopsy
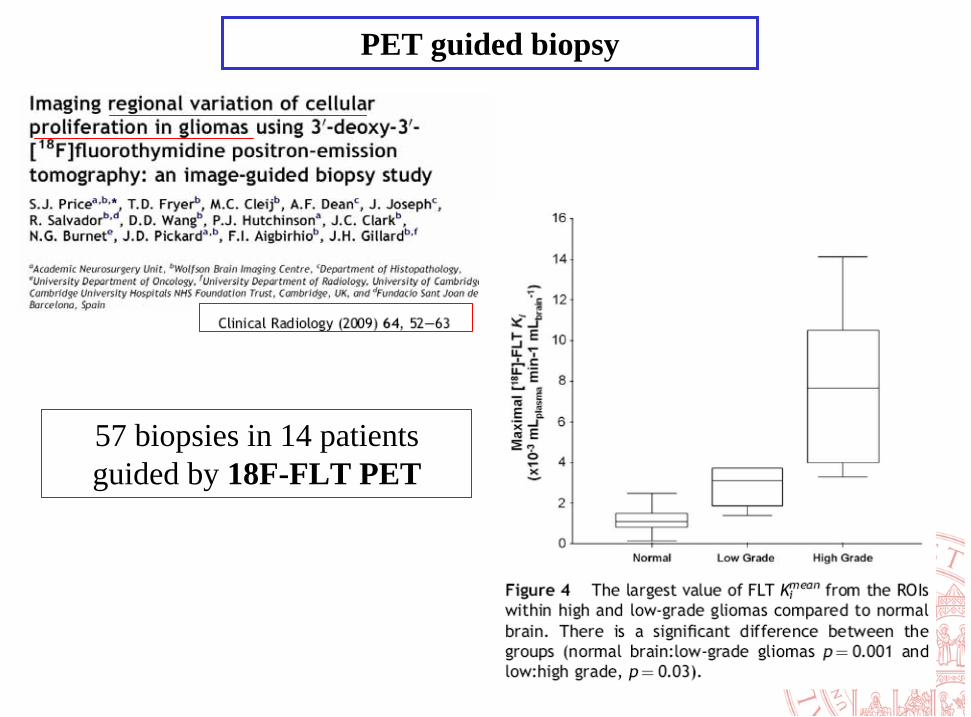
57 biopsies in 14 patientsguided by 18F-FLT PET
PET guided biopsy
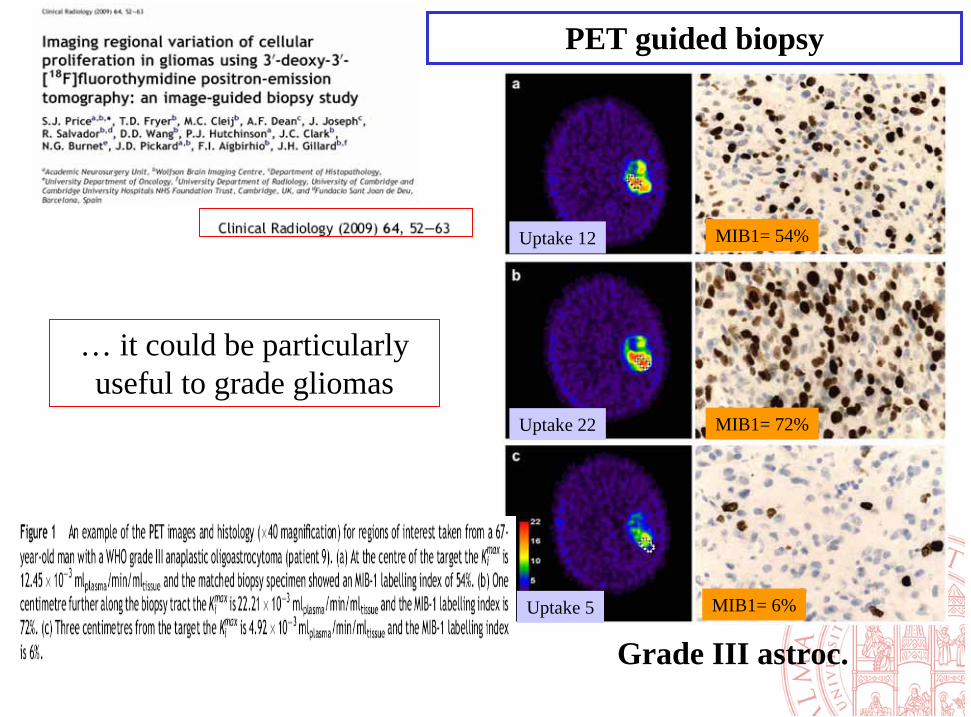
MIB1= 54%
MIB1= 72%
MIB1= 6%
Grade III astroc.
Uptake 12
Uptake 5
Uptake 22
… it could be particularly useful to grade gliomas
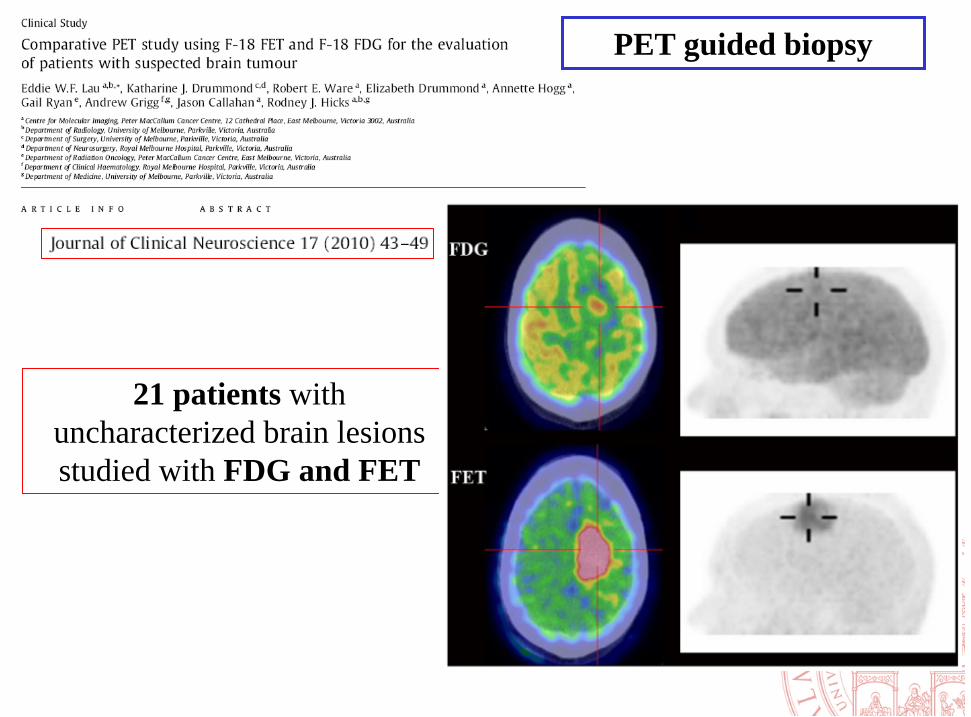
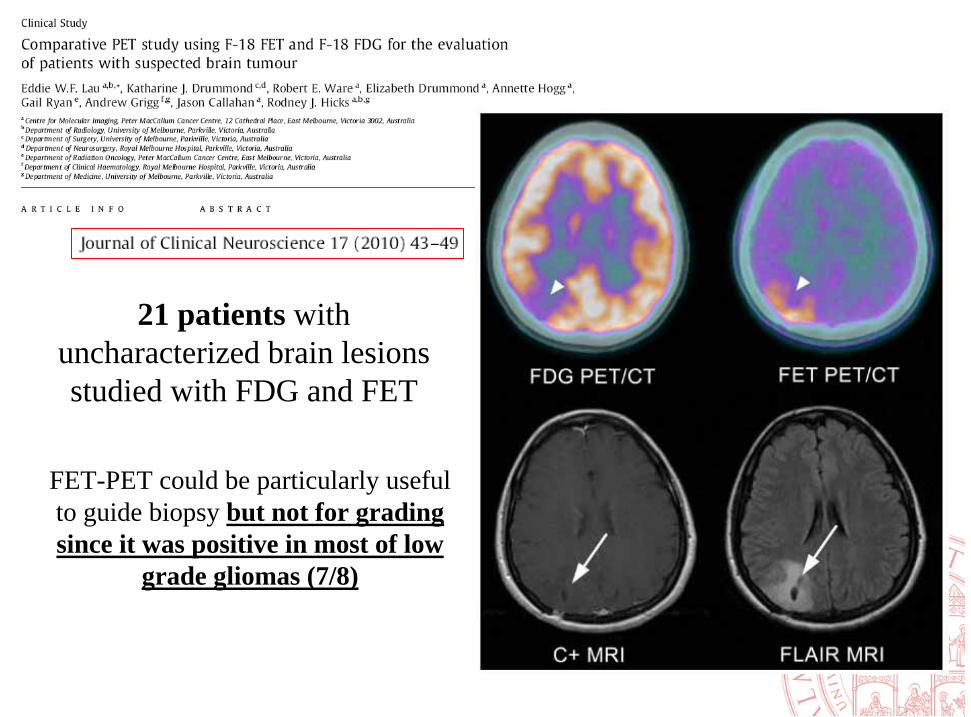
21 patients with uncharacterized brain lesions studied with FDG and FET
PET guided biopsy
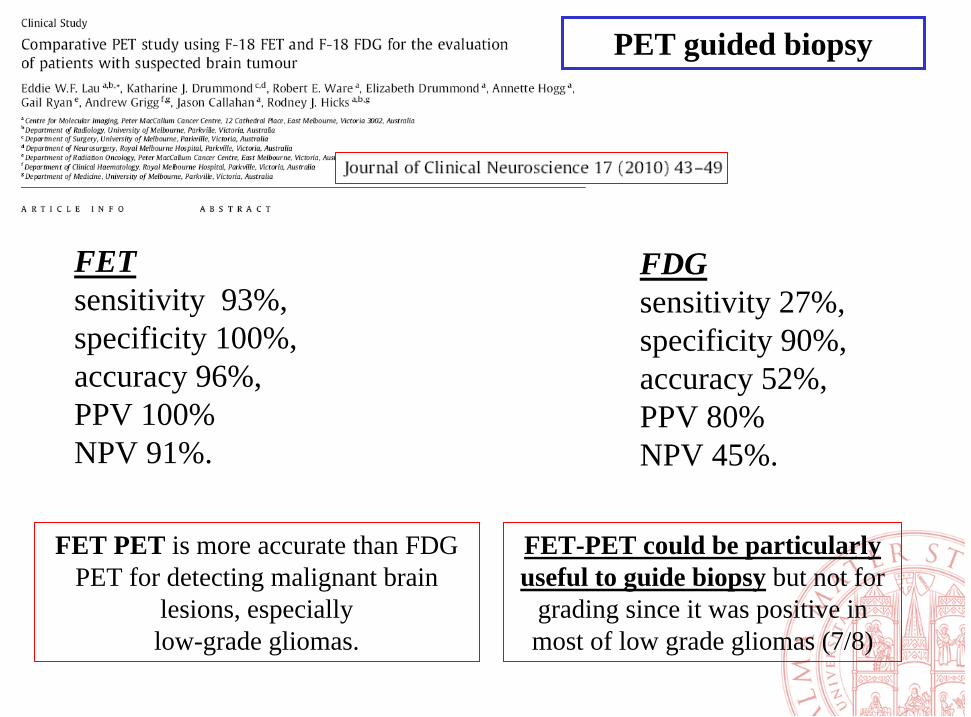
FET sensitivity 93%, specificity 100%, accuracy 96%, PPV 100% NPV 91%.
FDGsensitivity 27%, specificity 90%, accuracy 52%,PPV 80% NPV 45%.
FET PET is more accurate than FDG PET for detecting malignant brain
lesions, especiallylow-grade gliomas.
FET-PET could be particularly useful to guide biopsy but not for
grading since it was positive in most of low grade gliomas (7/8)
PET guided biopsy
1. Grading
2. Guide for stereotactic biopsy
5. Prognostic informations
4. Therapy response evaluation
3. Suspect of relapse after surgery and /or RT.
PET/CT:
clinical applications
Suspect of relapse after surgery and /or RT.
Suspect of relapse after surgery and /or RT.
Suspect of relapse after surgery and /or RT.
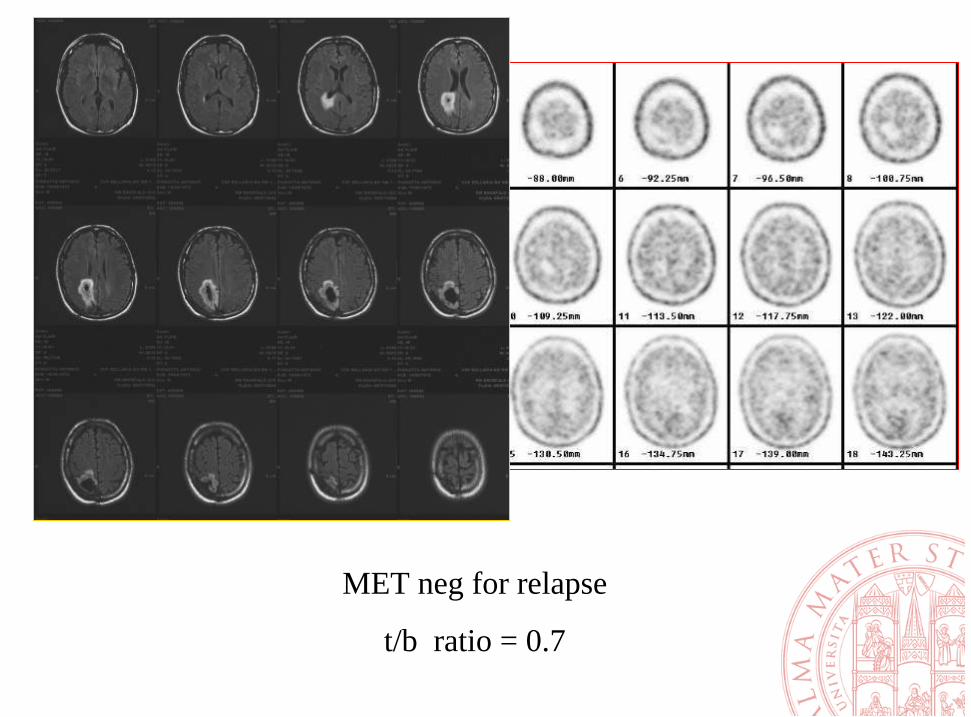
MET neg for relapse
t/b ratio = 0.7
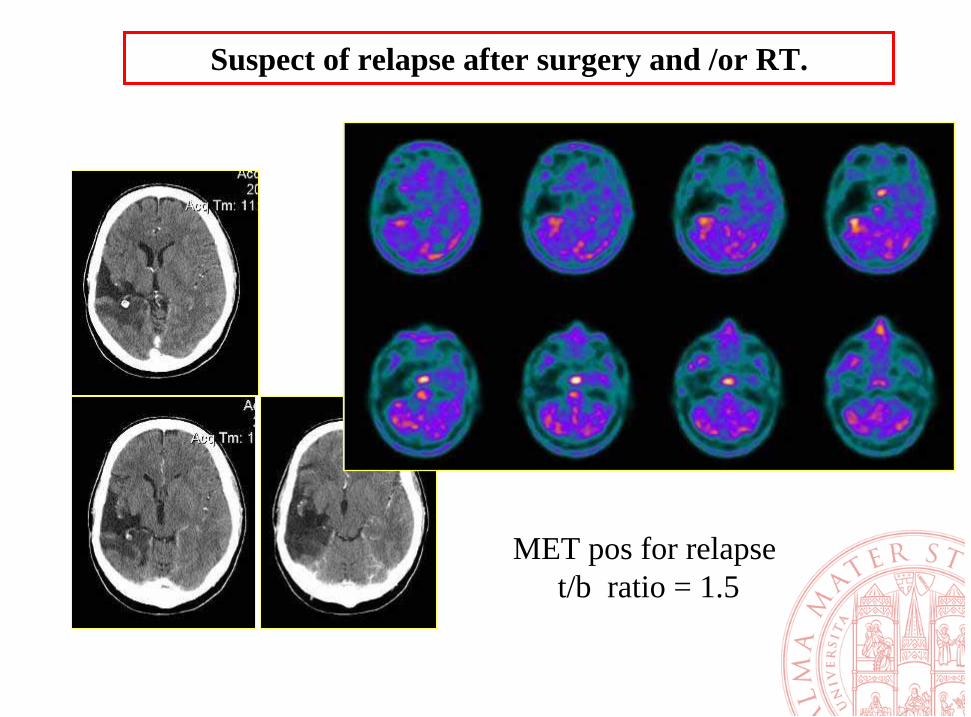
Suspect of relapse after surgery and /or RT.
MET pos for relapset/b ratio = 1.5
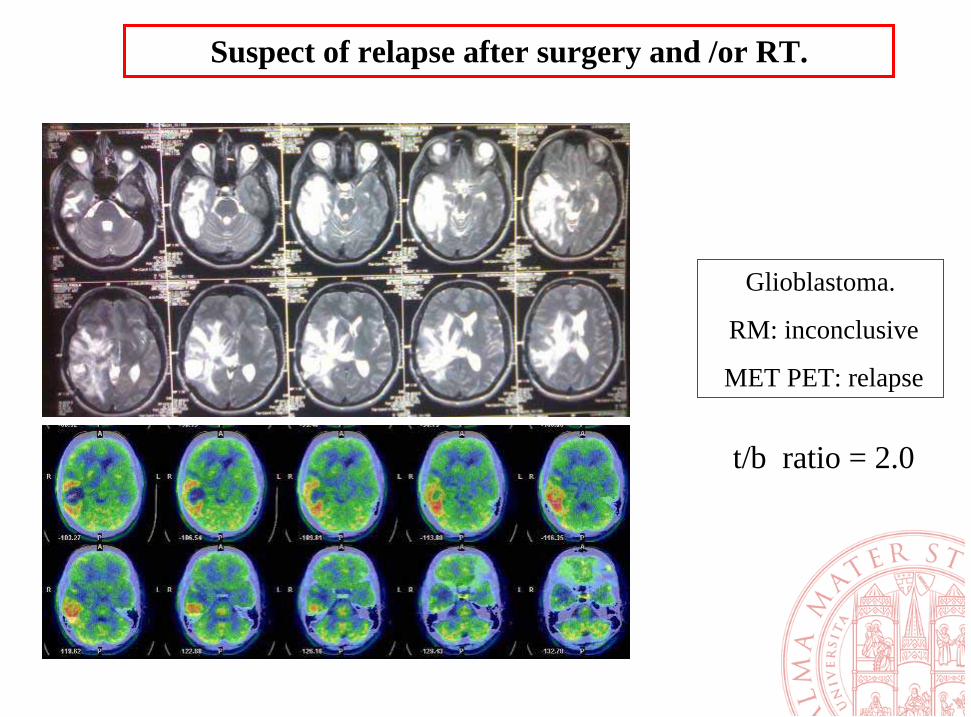
Glioblastoma.
RM: inconclusive
MET PET: relapse
Suspect of relapse after surgery and /or RT.
t/b ratio = 2.0
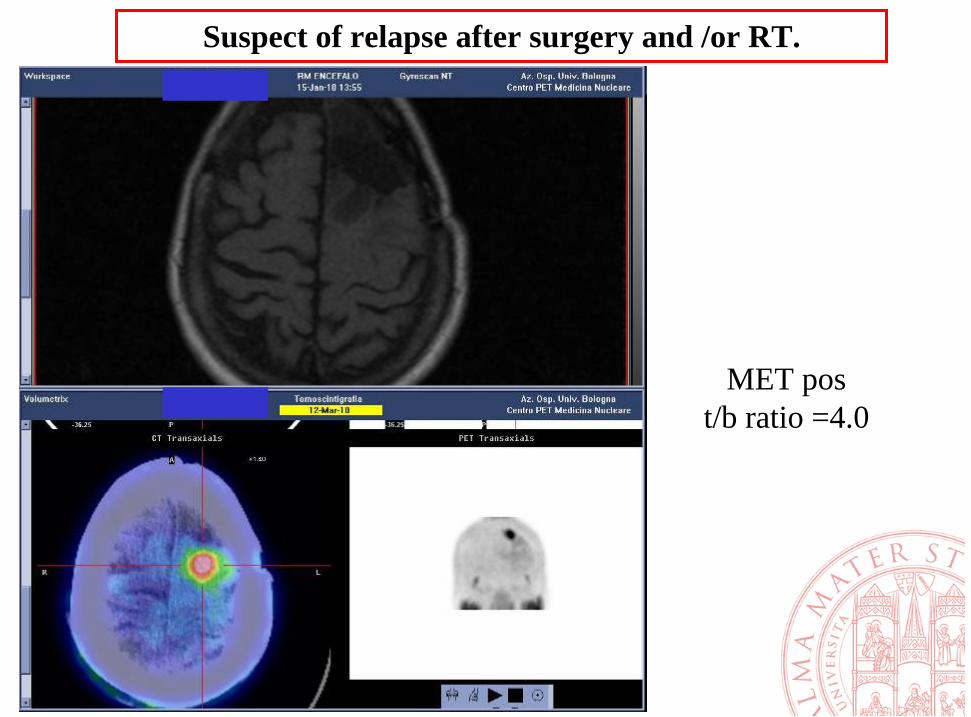
Suspect of relapse after surgery and /or RT.
MET post/b ratio =4.0
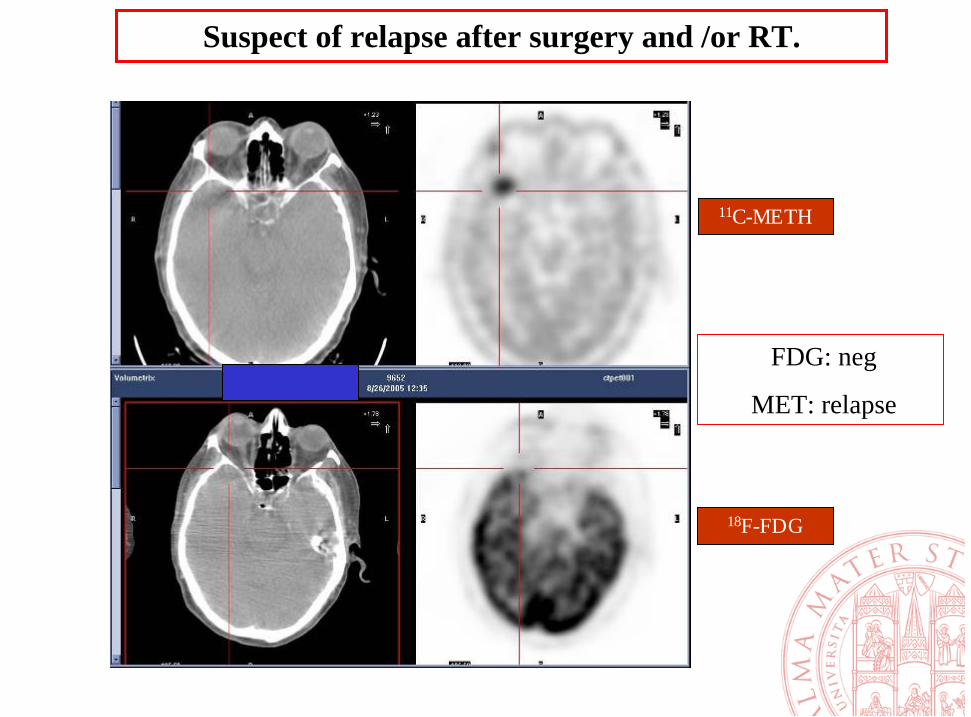
11C-METH
18F-FDG
Suspect of relapse after surgery and /or RT.
FDG: neg
MET: relapse
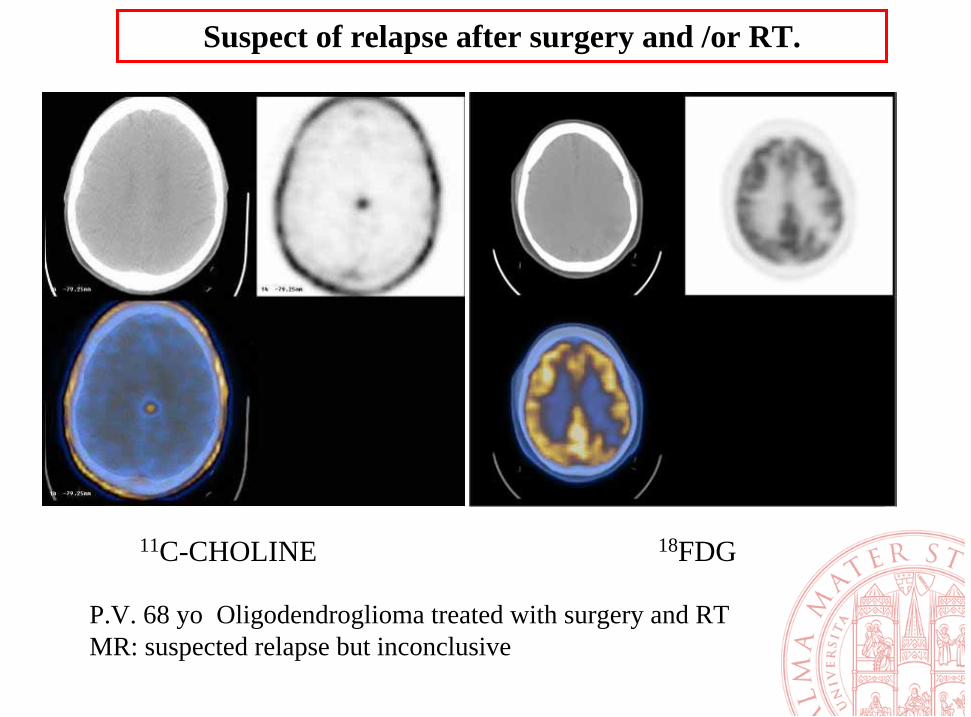
P.V. 68 yo Oligodendroglioma treated with surgery and RTMR: suspected relapse but inconclusive
11C-CHOLINE 18FDG
Suspect of relapse after surgery and /or RT.
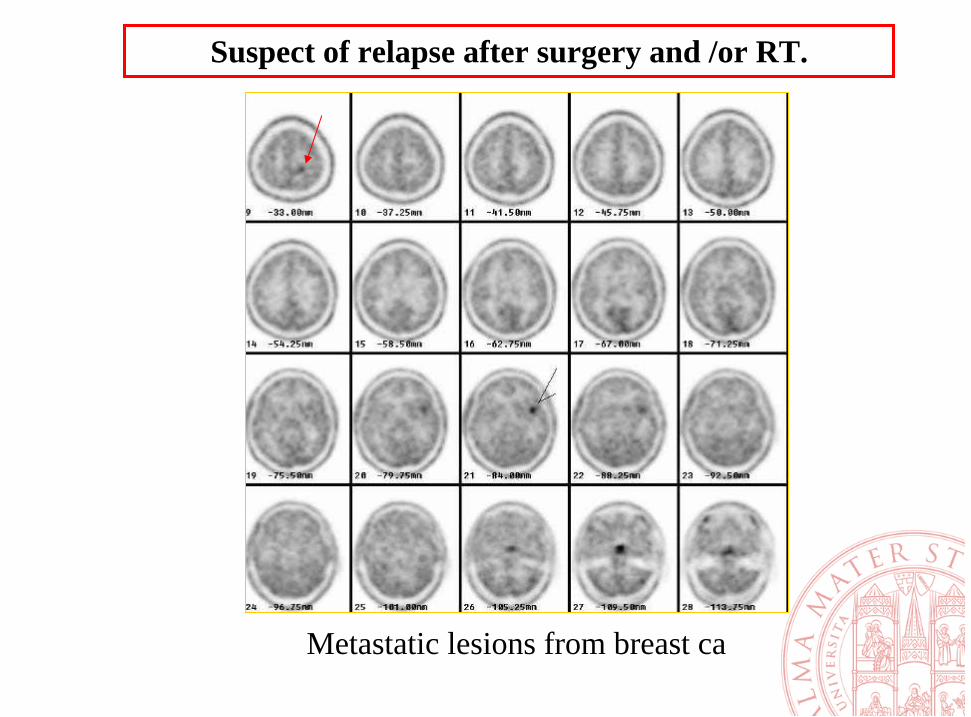
Metastatic lesions from breast ca
Suspect of relapse after surgery and /or RT.
1. Grading
2. Guide for stereotactic biopsy
6. Prognostic informations
5 Therapy response evaluation
3. Suspect of relapse after surgery and /or RT.
4. PET guided contouring for RT
Brain PET/CT:
clinical applications
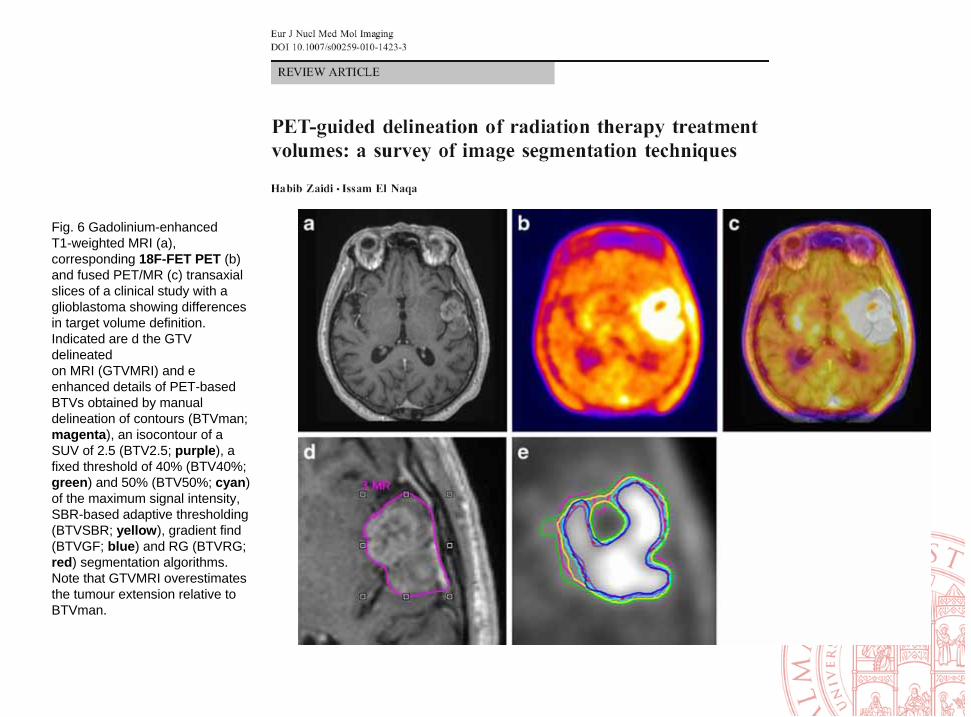
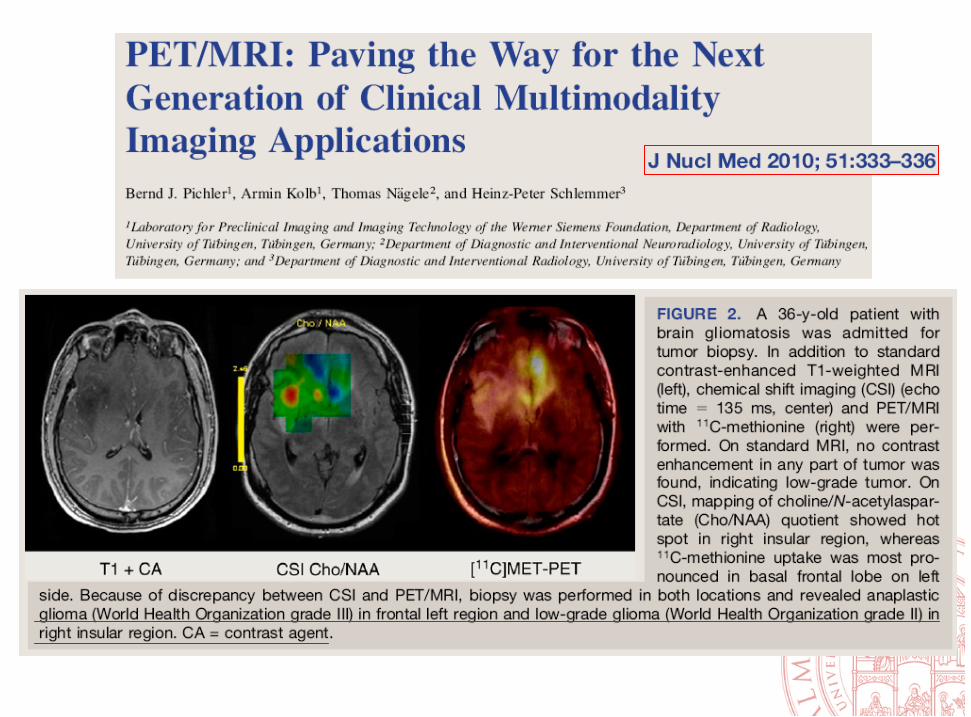
Fig. 6 Gadolinium-enhancedT1-weighted MRI (a),corresponding 18F-FET PET (b)and fused PET/MR (c) transaxialslices of a clinical study with aglioblastoma showing differencesin target volume definition.Indicated are d the GTV delineatedon MRI (GTVMRI) and eenhanced details of PET-basedBTVs obtained by manualdelineation of contours (BTVman;magenta), an isocontour of aSUV of 2.5 (BTV2.5; purple), afixed threshold of 40% (BTV40%;green) and 50% (BTV50%; cyan)of the maximum signal intensity,SBR-based adaptive thresholding(BTVSBR; yellow), gradient find(BTVGF; blue) and RG (BTVRG;red) segmentation algorithms.Note that GTVMRI overestimatesthe tumour extension relative toBTVman.
Brain PET/CT:
clinical applications
1. Grading
2. Guide for stereotactic biopsy
6 Prognostic informations
5 Therapy response evaluation
3. Suspect of relapse after surgery and /or RT.
4. PET guided contouring for RT
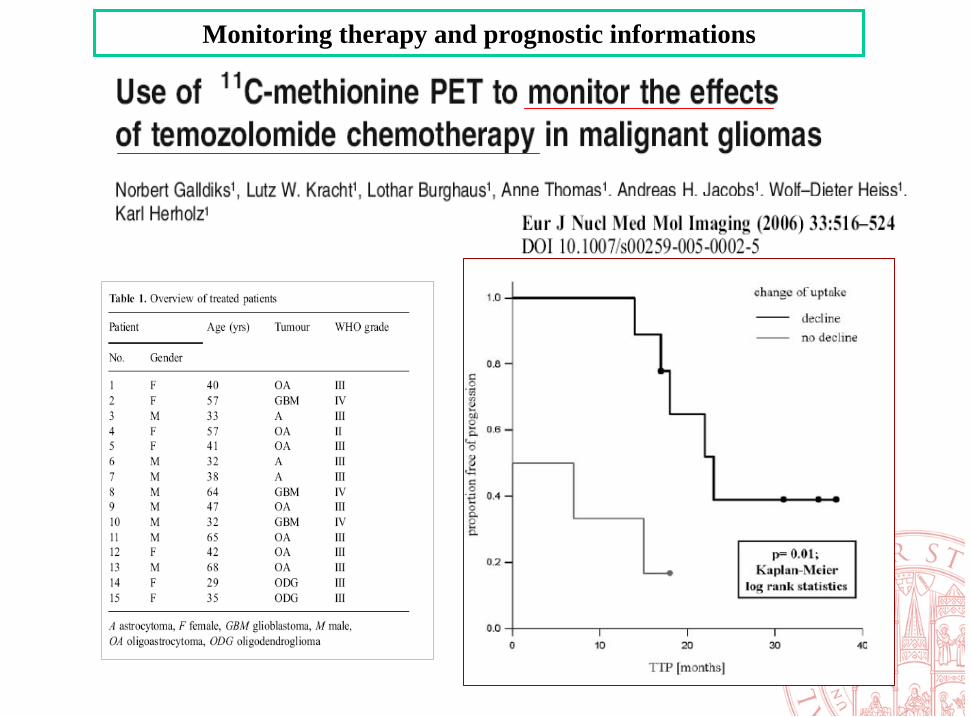
Monitoring therapy and prognostic informations

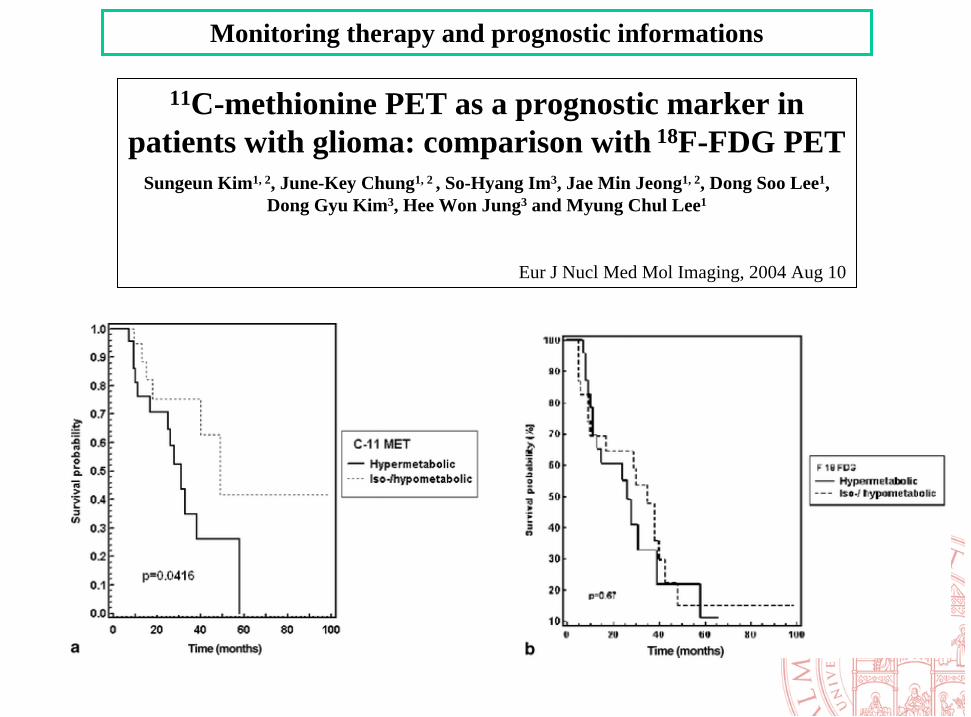
11C-methionine PET as a prognostic marker in patientswith glioma: comparison with 18F-FDG PET
Sungeun Kim1, 2, June-Key Chung1, 2 , So-Hyang Im3, Jae Min Jeong1, 2, Dong Soo Lee1, Dong Gyu Kim3, Hee Won Jung3 and Myung Chul Lee1
Eur J Nucl Med Mol Imaging, 2004 Aug 10
• 47 gliomas
• RM, FDG-PET, MET-PET
• MET Uptake is an independnt prognostic factor
Monitoring therapy and prognostic informations
Monitoring therapy and prognostic informations
11C-methionine PET as a prognostic marker in patients with glioma: comparison with 18F-FDG PET
Sungeun Kim1, 2, June-Key Chung1, 2 , So-Hyang Im3, Jae Min Jeong1, 2, Dong Soo Lee1, Dong Gyu Kim3, Hee Won Jung3 and Myung Chul Lee1
Eur J Nucl Med Mol Imaging, 2004 Aug 10
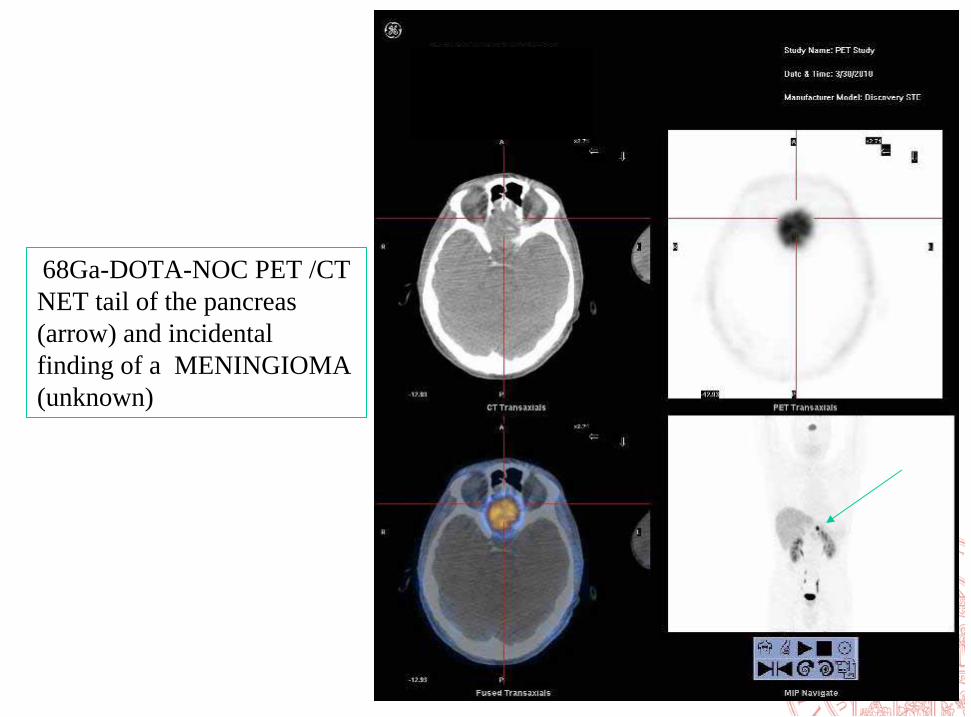
68Ga-DOTA-NOC PET /CTNET tail of the pancreas (arrow) and incidentalfinding of a MENINGIOMA (unknown)
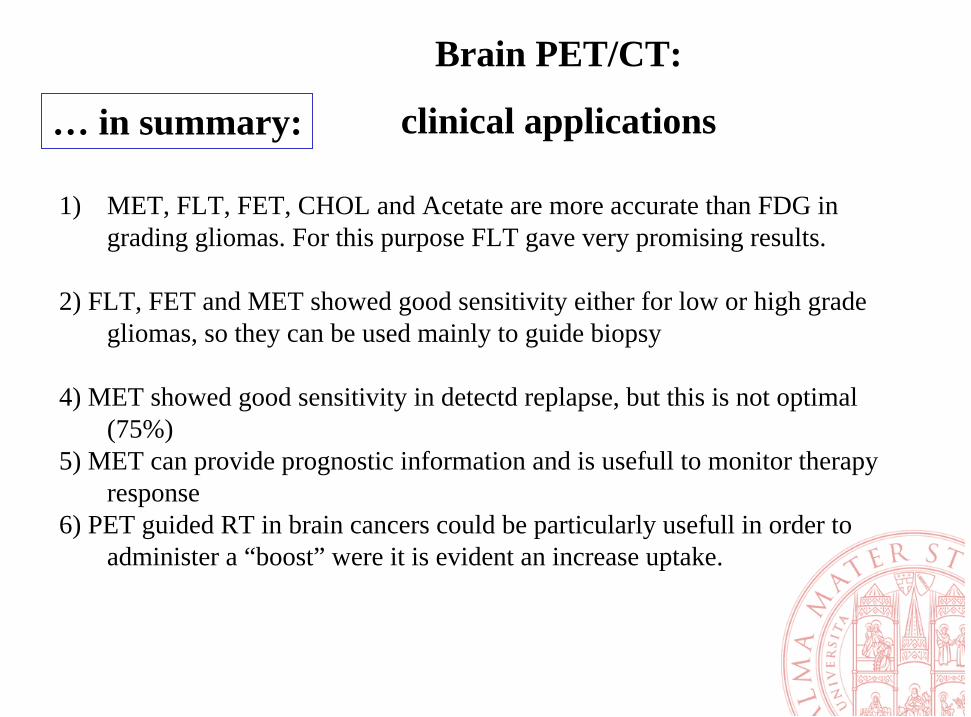
1) MET, FLT, FET, CHOL and Acetate are more accurate than FDG in grading gliomas. For this purpose FLT gave very promising results.
2) FLT, FET and MET showed good sensitivity either for low or high gradegliomas, so they can be used mainly to guide biopsy
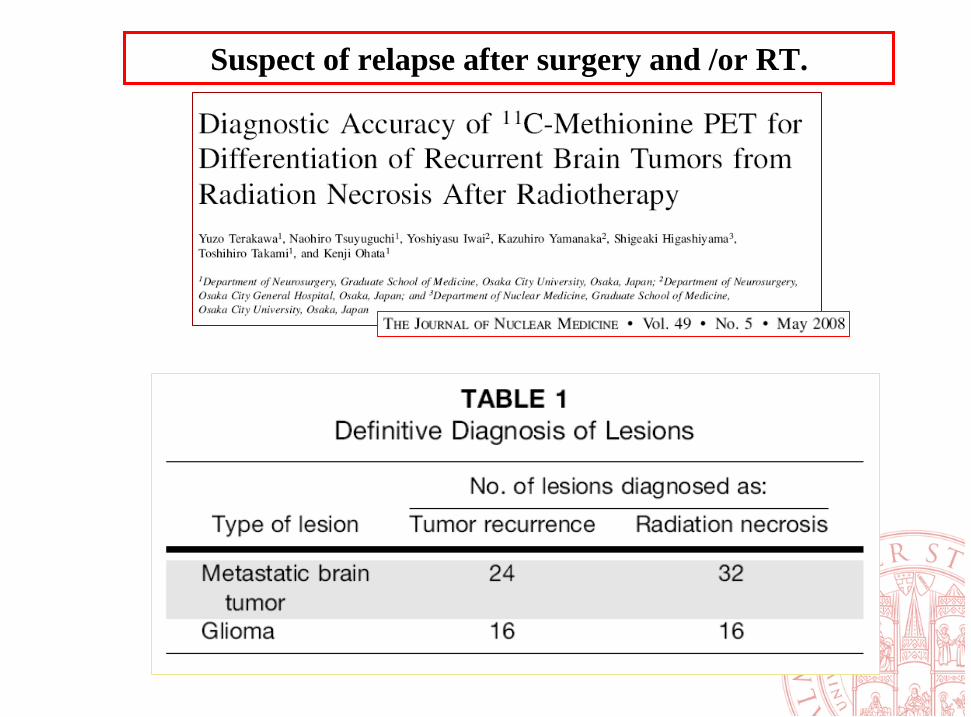
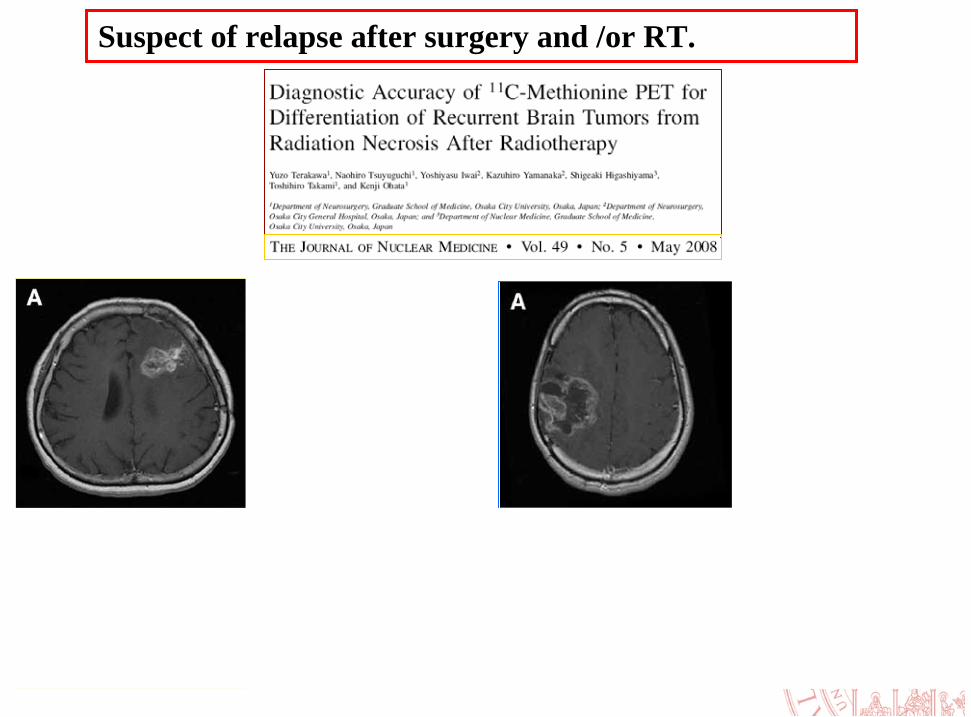
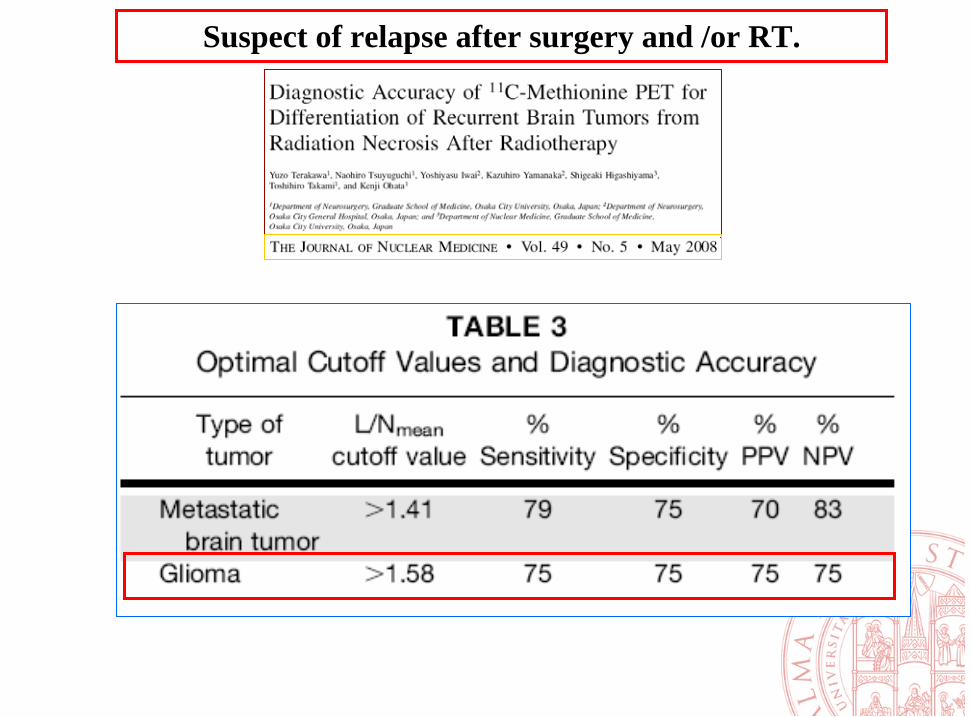
4) MET showed good sensitivity in detectd replapse, but this is not optimal(75%)
5) MET can provide prognostic information and is usefull to monitor therapyresponse
6) PET guided RT in brain cancers could be particularly usefull in order toadminister a “boost” were it is evident an increase uptake.
… in summary:
Brain PET/CT:
clinical applications
IN CONCLUSION
Main clinical applications of brain PET are:– Grading– Guide biopsy– Guide RT– Detect relapse after surgery or RT– Monitoring therapy– Prognosticate
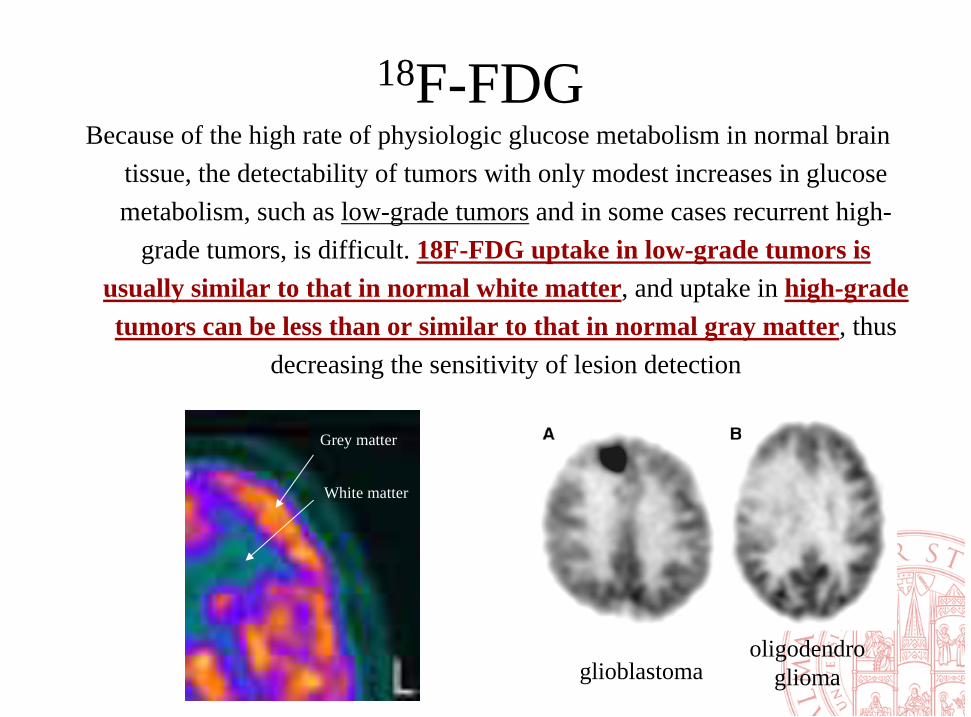
Because of the high rate of physiologic glucose metabolism in normal braintissue, the detectability of tumors with only modest increases in glucosemetabolism, such as low-grade tumors and in some cases recurrent high-
grade tumors, is difficult. 18F-FDG uptake in low-grade tumors isusually similar to that in normal white matter, and uptake in high-gradetumors can be less than or similar to that in normal gray matter, thus
decreasing the sensitivity of lesion detection
glioblastomaoligodendro
glioma
Grey matter
White matter
18F-FDG
Delayed Imaging. Early studies reported enhanced detectionof brain tumors with glucose loading, with a 27%
increase in the 18F-FDG uptake ratio of tumor to normalgray matter (ref1). However, glucose loading can be difficult
to perform clinically because of the need for intravenousglucose infusion and blood glucose monitoring. Recently,an interesting study showed that 18F-FDG imaging 3–8 hafter injection can improve the distinction between tumor
and normal gray matter (ref2)
18F-FDG
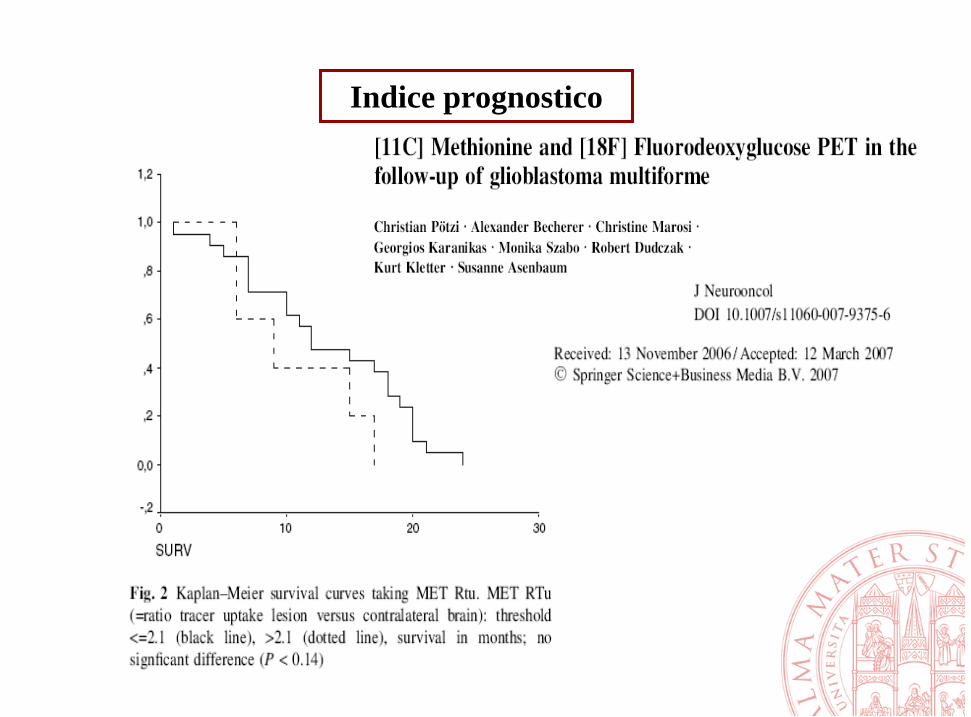
Indice prognostico
• 32 with glioma
• 32/32 MET-PET positive
• 70 biopsies: 61 diagnostic (MET POS)
9 non diagnostic (MET NEG)
PET guided biopsy
33 newly diagnosed glioma.LAT1 expression was higher in high grade gliomas.LAT1 expression was correlated with SUVmax
FET-PET could be particularly useful to guide biopsy but not for grading since it was positive in most of low
grade gliomas (7/8)
21 patients with uncharacterized brain lesions studied with FDG and FET
• As a general rule, suspicious lesions on MR imaging that show increasedFDG uptake are likely to represent tumor recurrence.
• Sensitivity is low, especially but not exclusively with low-grade gliomas,
• It seems clear that only the combination of FDG with MET can provide a comprehensive characterization of suspected brain tumor recurrence.
• Delayed images could help in the diagnosis
Radiol Clin North Am. 2005 Jan;43(1):35-47.
Suspect of relapse after surgery and /or RT.
….. and FDG ???
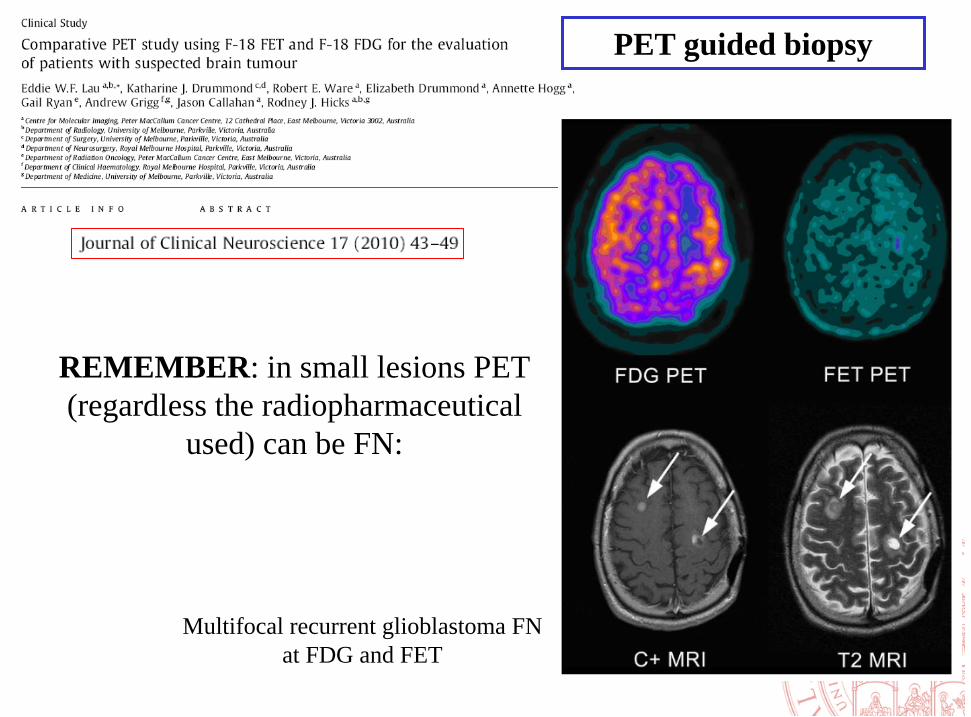
REMEMBER: in small lesions PET (regardless the radiopharmaceutical
used) can be FN:
Multifocal recurrent glioblastoma FN at FDG and FET
PET guided biopsy
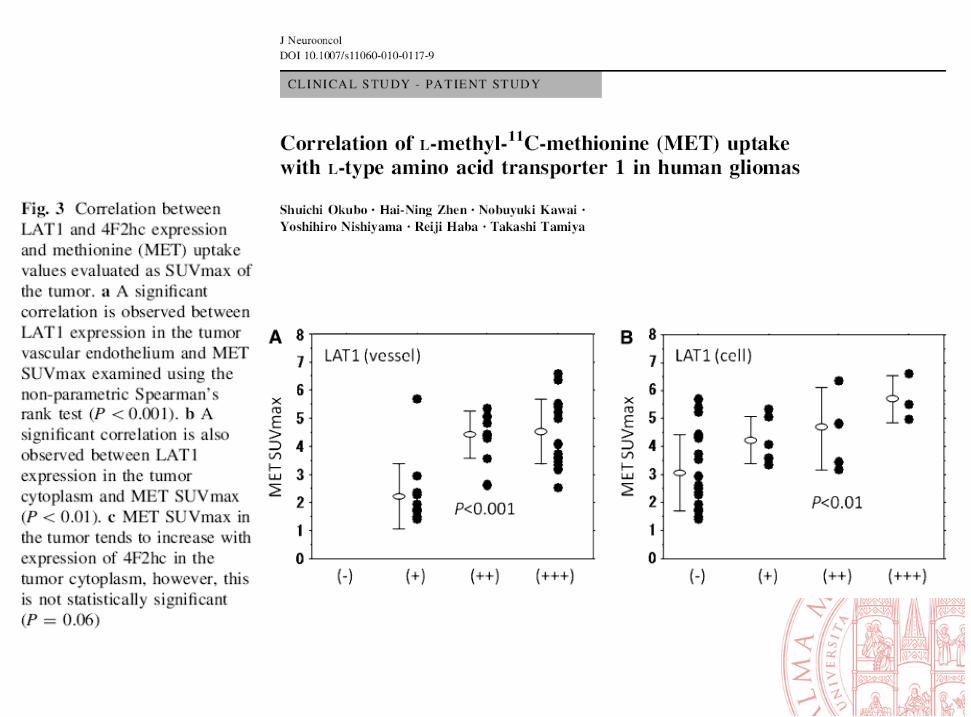
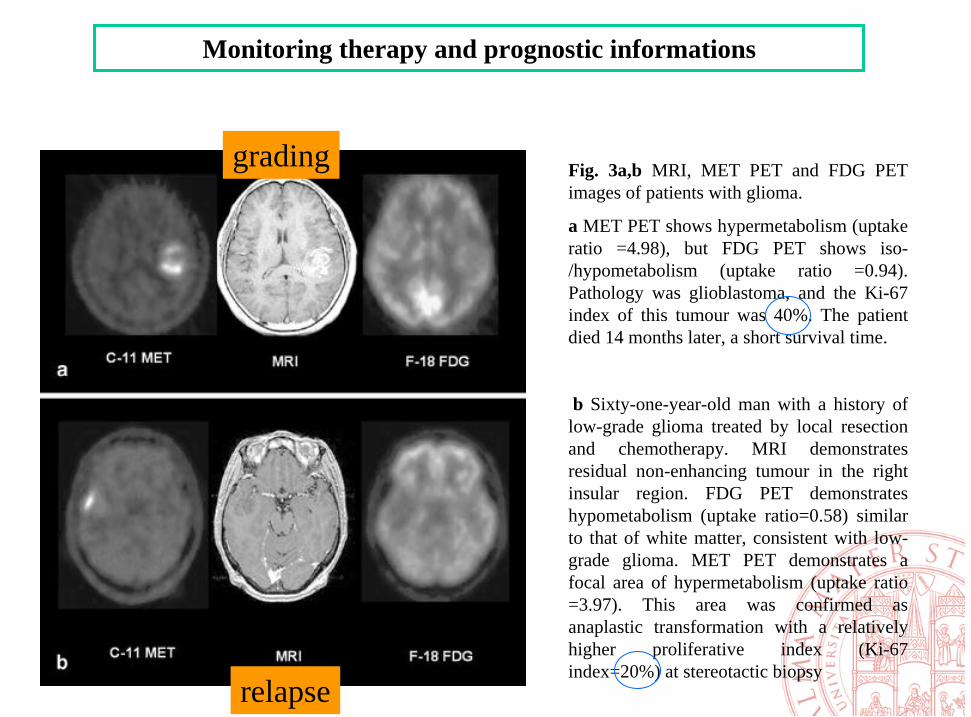
Fig. 3a,b MRI, MET PET and FDG PET images of patients with glioma.
a MET PET shows hypermetabolism (uptake ratio =4.98), but FDG PET shows iso-/hypometabolism (uptake ratio =0.94). Pathology was glioblastoma, and the Ki-67 index of this tumour was 40%. The patientdied 14 months later, a short survival time.
b Sixty-one-year-old man with a history of low-grade glioma treated by local resectionand chemotherapy. MRI demonstratesresidual non-enhancing tumour in the rightinsular region. FDG PET demonstrateshypometabolism (uptake ratio=0.58) similarto that of white matter, consistent with low-grade glioma. MET PET demonstrates a focal area of hypermetabolism (uptake ratio =3.97). This area was confirmed asanaplastic transformation with a relativelyhigher proliferative index (Ki-67 index=20%) at stereotactic biopsy
Monitoring therapy and prognostic informations
grading
relapse
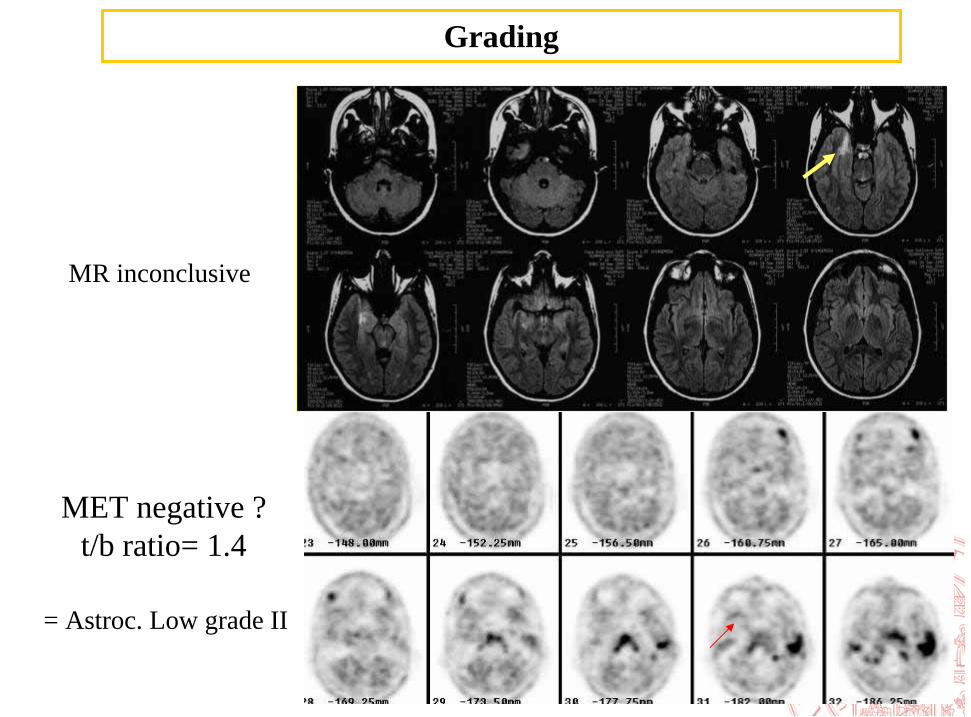
MR inconclusive
= Astroc. Low grade II
Grading
MET negative ?t/b ratio= 1.4