memory fact memory skills memory. cortical sensory area amygdala hippocampus diencephalon prefrontal...
TRANSCRIPT

Memory
• Fact memory
• Skills memory
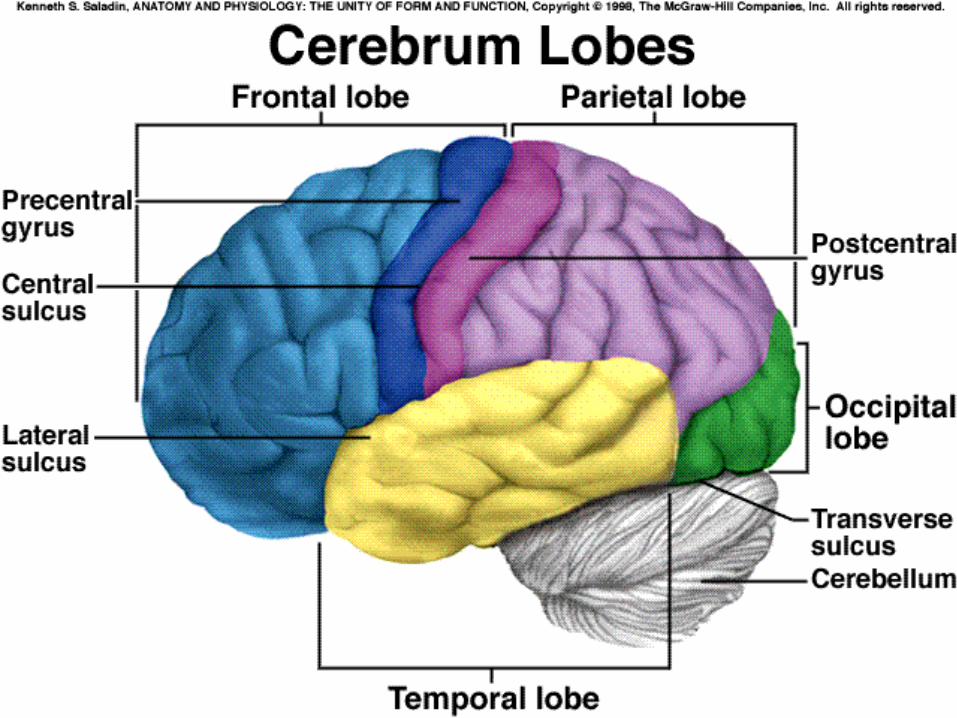


Cortical Sensory
Area
AmygdalaHippocampus
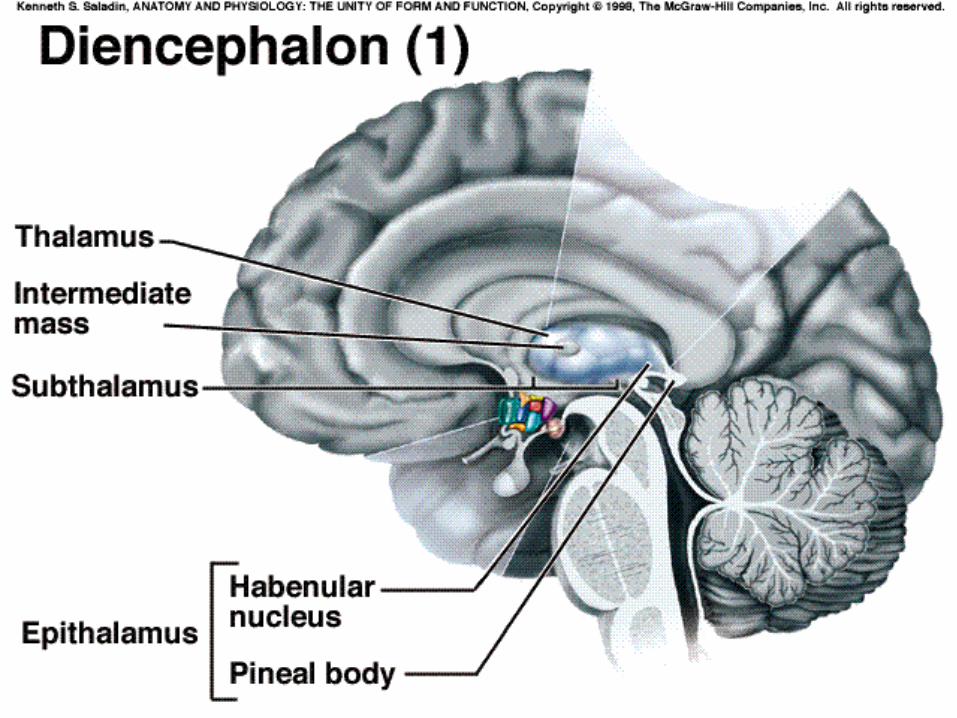
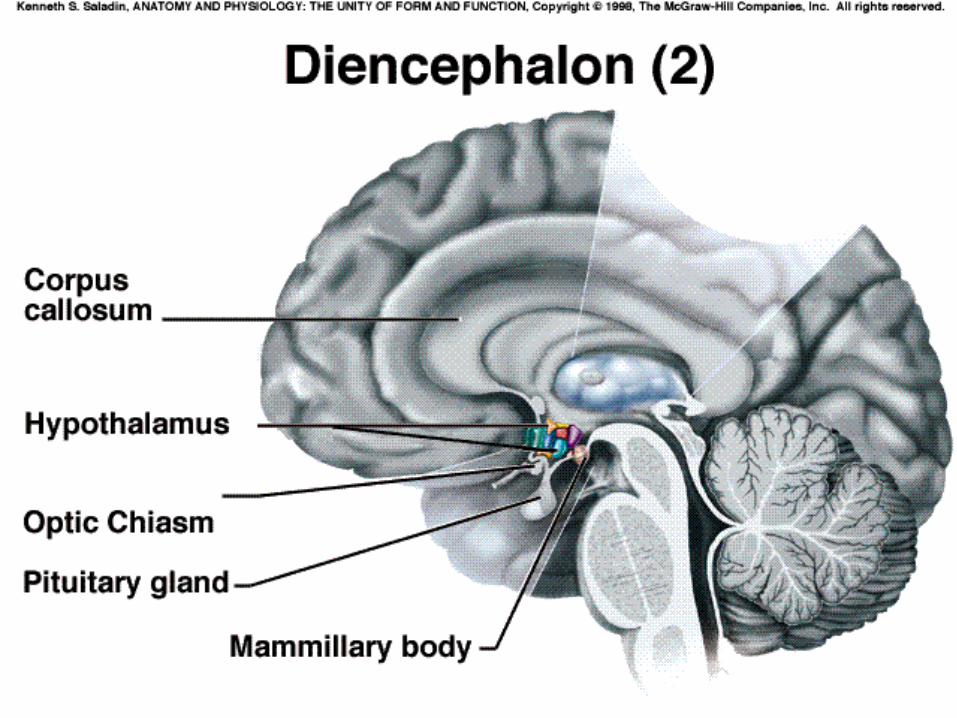
Diencephalon
PrefrontalCortex
BasalForebrain


CorticalSensory
Area
CorpusStriatum
MotorCortexCerebellum
ExtrapyramidalMotorNuclei
Alzheimer’s
• Features
• Etiology
• Pathophysiology
• Manifestation
• Diagnosis
• All of this is in your lab book!!
Features
• degenerative
• most common dementia
• 4th most common cause of death
• not a normal part of ageing
Etiology
• no gender differences
• risk increases with age– can be 40 - 50– most over 65
• prevalence = 20% by 80
• 10-15% of cases potentially attributed to depression
Etiology
• Slow virus - incubation period 2 - 30 years, transmission difficult to prove
• An auto immune process - increased levels of brain reactive antibodies
• Aluminium toxicity - aluminium deposits have been identified in some patients.

Etiology
• Genetic predisposition - 10 - 30% of patients have familial association
• +ve correlation with fat
• defect on chromosome 21 implicated supported by Downs developing AD in 4th decade
• SDAT families produce 3x normal numbers of Downs children

The 7 Dietary Principles to Reduce Alzheimer's RiskPCRM
• 1. Minimize saturated fats and trans fats.
• 2. Vegetables, legumes (beans, peas, and lentils), fruits, and whole grains should be the primary staples of the diet.
• 3. One ounce of nuts or seeds (one small handful) daily provides a healthful source of vitamin E.
• 4. A reliable source of vitamin B12, such as fortified foods or a supplement providing at least 2.4 μg per day for adults) should be part of the daily diet.
• 5. Choose multivitamins without iron and copper, and consume iron supplements only when directed by your physician.
• 6. Avoid the use of cookware, antacids, baking powder, or other products that contribute dietary aluminium.
• 7. Engage in aerobic exercise equivalent to 40 minutes of brisk walking 3 times per week.
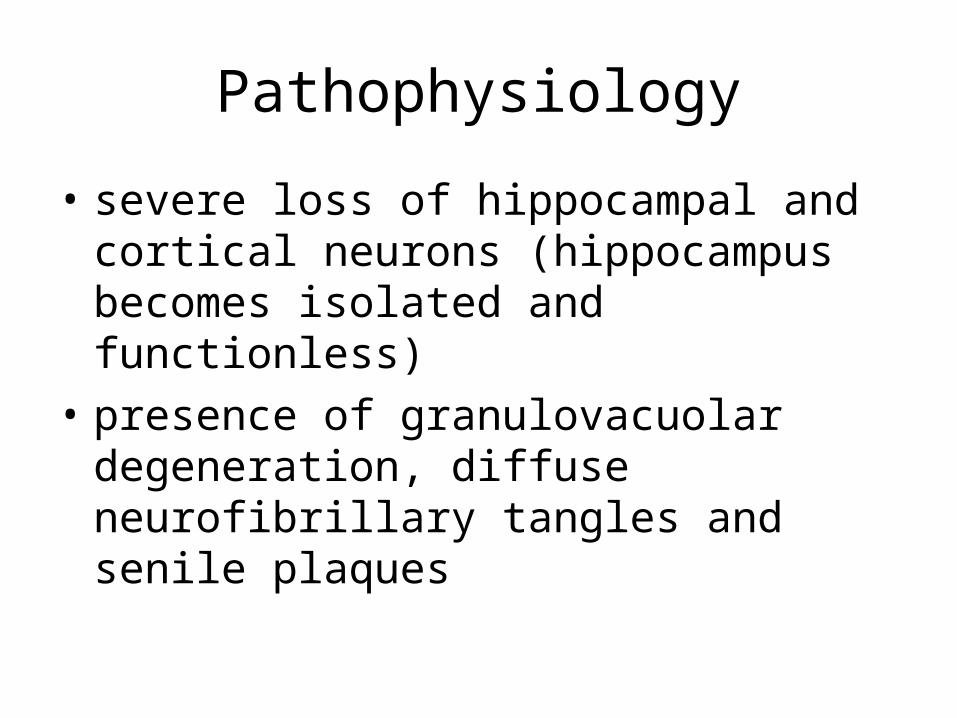
Pathophysiology
• severe loss of hippocampal and cortical neurons (hippocampus becomes isolated and functionless)
• presence of granulovacuolar degeneration, diffuse neurofibrillary tangles and senile plaques
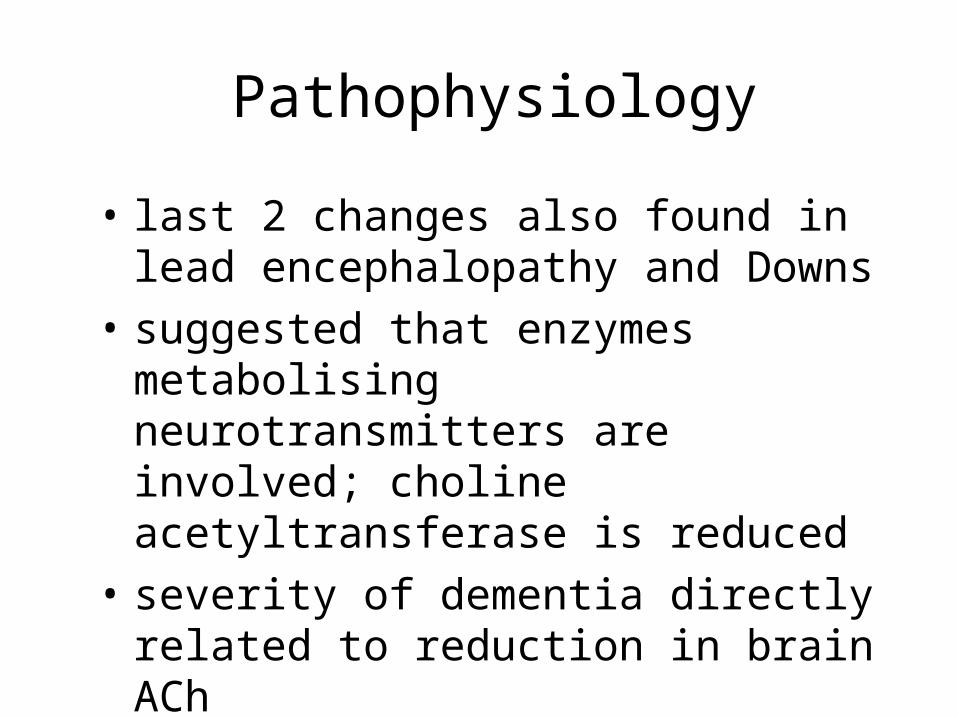
Pathophysiology
• last 2 changes also found in lead encephalopathy and Downs
• suggested that enzymes metabolising neurotransmitters are involved; choline acetyltransferase is reduced
• severity of dementia directly related to reduction in brain ACh
Manifestations
• insidious and progressive loss of memory, disorientation, impaired abstract thinking, changes in personality
• Three stages:
Manifestations
• 1 2 - 4 yrs– subjective memory deficit, random
forgetfulness, get lost easily– lack of spontaneity– subtle personality changes (loss of sense of
humour)– disorientation to time and date
Manifestations
• 2 Confusional - may last several years– impaired cognition and abstract thinking– restlessness and agitation– wandering - "Sundown Syndrome”– inability to carry out daily living activities

Manifestations
• 2 Confusional (cont’d)– impaired judgement– inappropriate social behaviour– lack of insight– repetitive behaviour– voracious appetite
Manifestations
• 3 Terminal - 1 - 2 yrs– indifference to food leads to emaciation– inability to communicate– urinary and faecal incontinence– seizures– death usually the result of malnutrition or
infection
Diagnosis
• absence of definitive test
• diagnosis only by microscopic examination of tissue from cerebral biopsy or autopsy
• patient presenting should be tested to detect potentially reversible nutritional, endocrine, and infectious causes of symptoms (eg. B12 deficiency, thyroid dysfunction and electrolyte imbalance)
Diagnosis
• requires presence of dementia established by clinical examination and documented by results of a Mini-mental status test, Blessed dementia test, or similar to yield deficits in 2 or more areas of cognition and progressive worsening of memory or other cognitive functions