mental health care pathway - leicestershire ... patient and carer or support workers, providing...
TRANSCRIPT
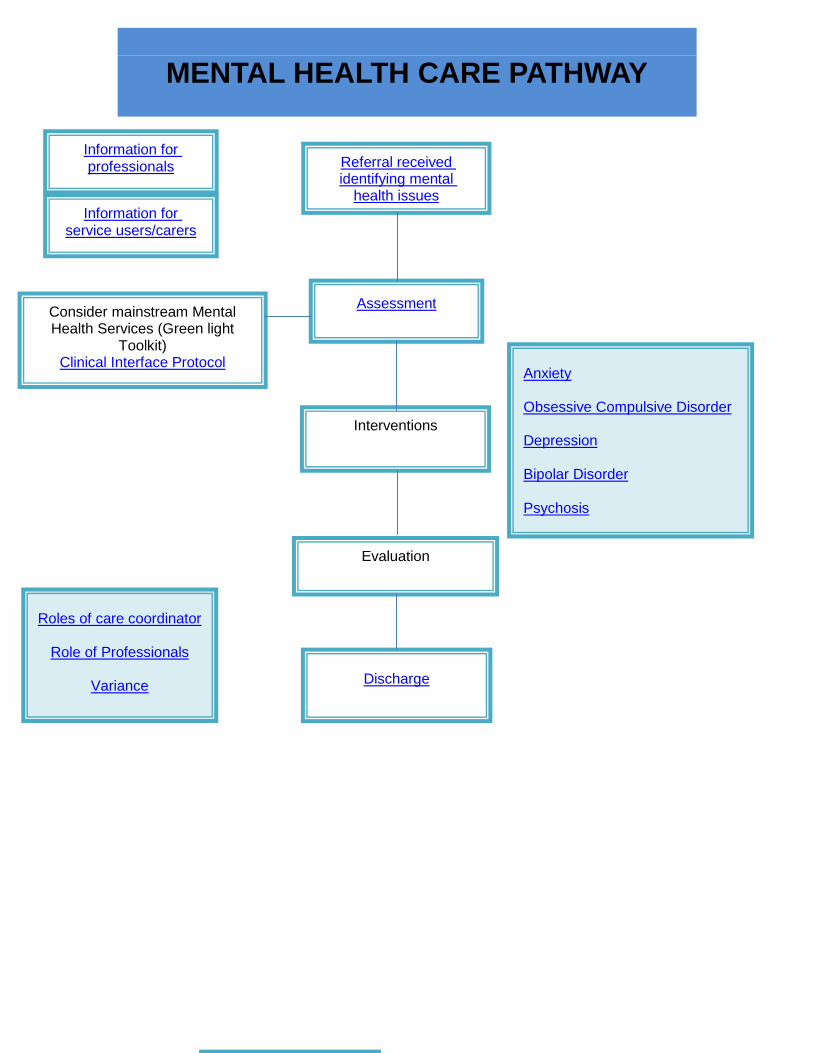
MENTAL HEALTH CARE PATHWAY
Referral received identifying mental
health issues
Assessment
Consider mainstream Mental Health Services (Green light
Toolkit) Clinical Interface Protocol
Interventions
Evaluation
Information for service users/carers
Information for professionals
Anxiety Obsessive Compulsive Disorder Depression Bipolar Disorder Psychosis
Discharge
Roles of care coordinator
Role of Professionals
Variance

Triggers
HONOS-LD items to consider as triggers for discussion whether mental health assessment needed
Anxieties/phobias/obsessive compulsive behaviour (score 2) Behaviour(s) sufficiently frequent and severe to produce some disruption of and impact on own or other people’s functioning Problems with hallucinations or delusions (score 1) Occasional odd or eccentric beliefs or behaviours suggestive of hallucinations or delusions Problems associated with mood changes (score 2) Mood change producing significant impact on self or others (e.g. weeping spells, decrease in skills, withdrawal and loss of interest
Go back to Pathway

Information for Professionals People with Learning Disability are likely to have a higher prevalence of mental health problems. Mental health problems are complex in presentation and can present a diagnostic challenge. Therefore, people with Learning Disability are more likely to have unmet mental health needs. Some flexibility is advised with the assessment approach, in that the assessment may need to be done over a period of time (rather than in one setting) and information from carers is very valuable. Caution is advised with diagnoses especially when there are other issues such as diagnostic overshadowing, cognitive distortion in difficult life situations and when there are symptoms related to other developmental disorders. Specific information for the following disorders:
Anxiety Obsessive compulsive disorder Depression Bipolar disorder Psychosis
Go back to Pathway

Information for Service Users and Carers
Depression Leaflet
Anxiety Leaflet
Psychosis Leaflet
Bipolar Disorder Leaflet
Go back to Pathway
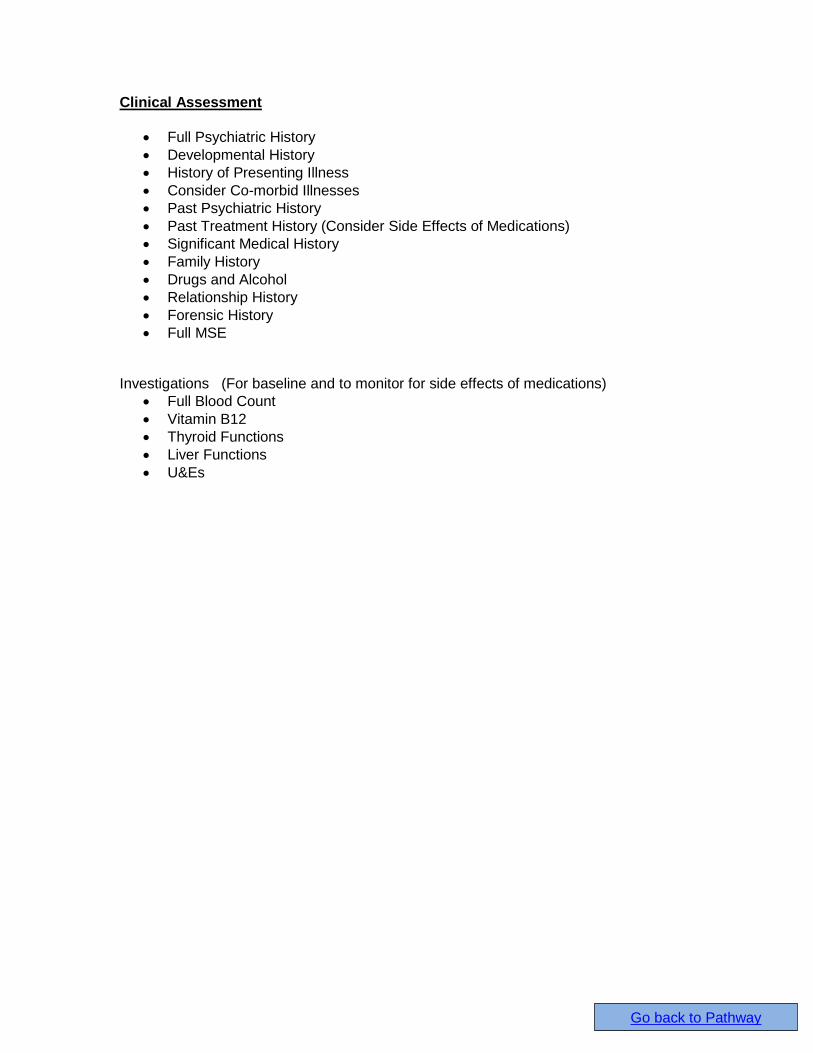
Clinical Assessment
Full Psychiatric History
Developmental History
History of Presenting Illness
Consider Co-morbid Illnesses
Past Psychiatric History
Past Treatment History (Consider Side Effects of Medications)
Significant Medical History
Family History
Drugs and Alcohol
Relationship History
Forensic History
Full MSE Investigations (For baseline and to monitor for side effects of medications)
Full Blood Count
Vitamin B12
Thyroid Functions
Liver Functions
U&Es
Go back to Pathway

Discharge Planning
Ensure global outcomes achieved Agree on discharge with service user/carer Letter to Refer and GP
Reason for referral Outcome of assessment Outcome of intervention Advice on management of condition in primary care Advice on early symptoms/signs of recurrence Advice on re-referral
Go back to Pathway
Responsibilities of Care Pathway Coordinator
The Care Co-ordinator has responsibility for co-ordinating care, maintaining contact with the Service User ensuring that the CPA Care plan is delivered and reviewed as required. The Care Co-ordinator will be a qualified individual with the requisite knowledge, skills and experience and will in most cases be registered to a profession and be the person “best placed” to oversee Care Planning and resource allocation. The Care Co-ordinator can be of any discipline depending on capability and capacity. The assessment of need may highlight certain areas requiring specialist intervention and support, for example tissue viability. Referrals should be made to the appropriate organisations for these to be further assessed and managed, for example the Community Health services/ GP. Each professional group will have its own assessment tools and measures for assessing need and monitoring progress, however for the purposes of the Pathway, the Leicestershire Learning Disability Service User Reported Outcome Measure is recommended for general use. It is important to incorporate outcome measures at this stage of the assessment, to ensure that the focus of any intervention chosen is clear, and to help monitor progress.
Go back to Pathway

Variance
Variance analysis is a critical part of using this care pathway. Variance can identify deviations from the expected pathway and if so, for what reasons. This can used to amend the care pathway itself or the processes followed. Variance should be recorded with the Care Pathway form on the Learning Disability Core Information.
Go back to Pathway

Professional Roles
TIER 2
Psychiatry Education and Support Training mainstream services (adult mental health services,
other community and hospital health services) about Learning Disability, to build capacity within these services, advice on management of mental health problems within primary care services and other mainstream services such as IAPT.
Advice to all members of the MDT team about presentation of mental health problems and management of common mental health problems
Assessment Review of mental health, gathering information from records
and review of patient including mental state examination. Discussion of case with the MDT. Psychiatric formulation of behaviours and bio-psychosocial care plan.
Intervention Consideration of medical treatment for mental health
problem. Involvement would include regular reviews and discussion with MDT
Giving information to carers / users regarding the diagnosis and prognosis.
Advice GP regarding treatment strategies and expected prognosis
Involvement will be time limited
Psychology Generalised anxiety disorder - Assessment and Formulation Low Intensity interventions if step 1 not helpful - Self-help and Psycho-education Depression - Clinical psychologists may support others to do the direct work using manualised materials. In LD these materials may need adapting for the individual’s needs. On occasion clinical psychologists may be needed to help the person understand the package and monitor it weekly to see how it’s being used, whether successful or if needs adapting further. Guided self-help based on CBT (with Carers/ Staff support in between sessions)
Community Nursing
Education and support: Enabling access to mainstream services. Community Nurse.
Educating patient and carer or support workers, providing accessible information on mental health conditions. Supporting patient or carer to recognise signs and symptoms of mental health condition.
‘We need to do mental health promotion’
Go back to Pathway
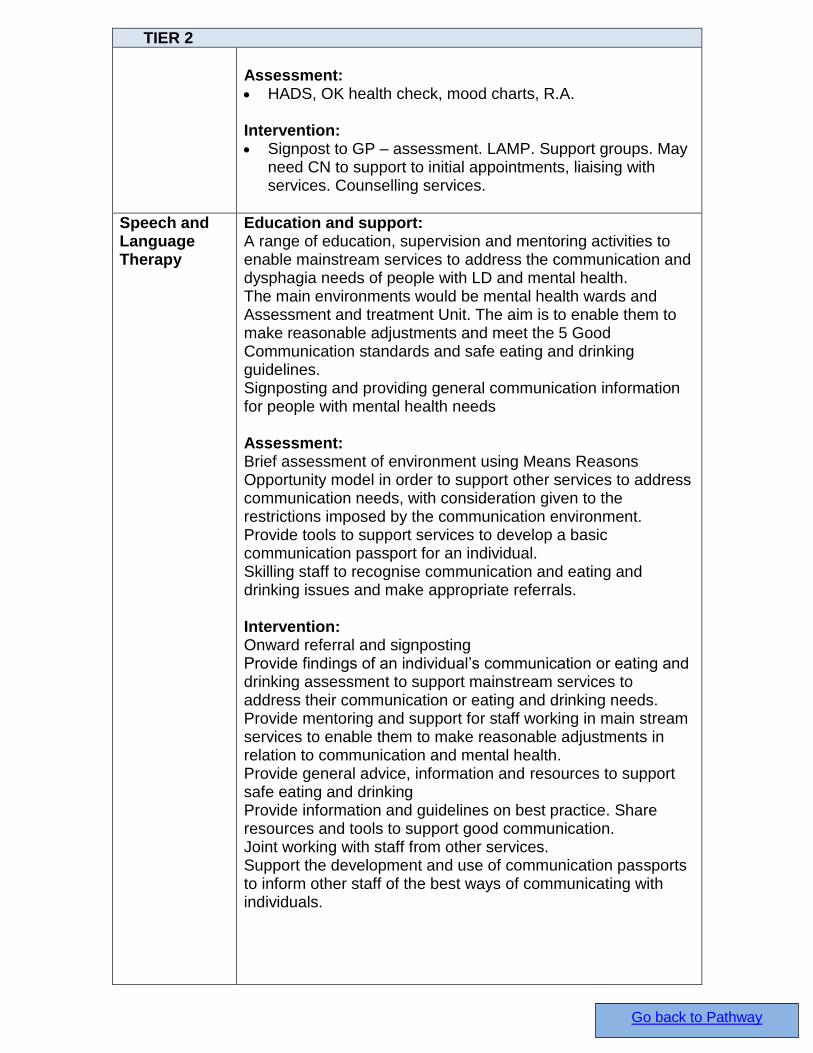
TIER 2
Assessment: HADS, OK health check, mood charts, R.A. Intervention: Signpost to GP – assessment. LAMP. Support groups. May
need CN to support to initial appointments, liaising with services. Counselling services.
Speech and Language Therapy
Education and support: A range of education, supervision and mentoring activities to enable mainstream services to address the communication and dysphagia needs of people with LD and mental health. The main environments would be mental health wards and Assessment and treatment Unit. The aim is to enable them to make reasonable adjustments and meet the 5 Good Communication standards and safe eating and drinking guidelines. Signposting and providing general communication information for people with mental health needs Assessment: Brief assessment of environment using Means Reasons Opportunity model in order to support other services to address communication needs, with consideration given to the restrictions imposed by the communication environment. Provide tools to support services to develop a basic communication passport for an individual. Skilling staff to recognise communication and eating and drinking issues and make appropriate referrals. Intervention: Onward referral and signposting Provide findings of an individual’s communication or eating and drinking assessment to support mainstream services to address their communication or eating and drinking needs. Provide mentoring and support for staff working in main stream services to enable them to make reasonable adjustments in relation to communication and mental health. Provide general advice, information and resources to support safe eating and drinking Provide information and guidelines on best practice. Share resources and tools to support good communication. Joint working with staff from other services. Support the development and use of communication passports to inform other staff of the best ways of communicating with individuals.
Go back to Pathway
TIER 2
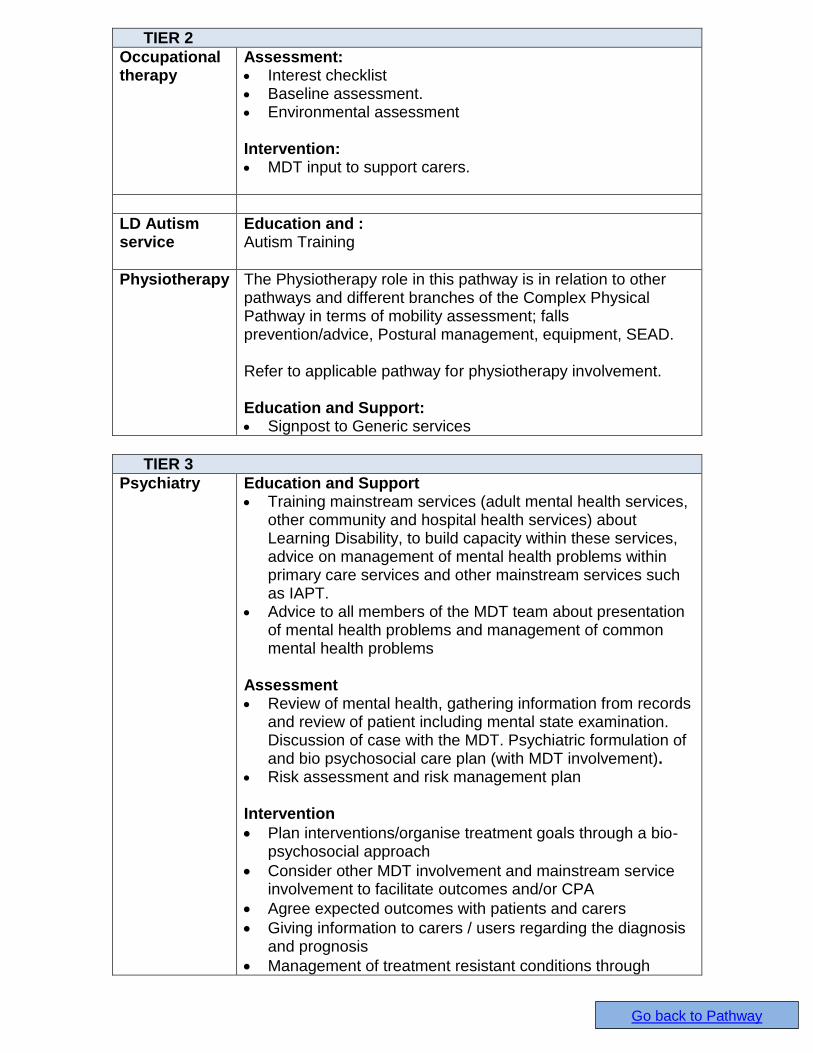
Occupational therapy
Assessment: Interest checklist Baseline assessment. Environmental assessment Intervention: MDT input to support carers.
LD Autism service
Education and : Autism Training
Physiotherapy The Physiotherapy role in this pathway is in relation to other pathways and different branches of the Complex Physical Pathway in terms of mobility assessment; falls prevention/advice, Postural management, equipment, SEAD. Refer to applicable pathway for physiotherapy involvement. Education and Support: Signpost to Generic services
TIER 3
Psychiatry Education and Support Training mainstream services (adult mental health services,
other community and hospital health services) about Learning Disability, to build capacity within these services, advice on management of mental health problems within primary care services and other mainstream services such as IAPT.
Advice to all members of the MDT team about presentation of mental health problems and management of common mental health problems
Assessment Review of mental health, gathering information from records
and review of patient including mental state examination. Discussion of case with the MDT. Psychiatric formulation of and bio psychosocial care plan (with MDT involvement).
Risk assessment and risk management plan Intervention
Plan interventions/organise treatment goals through a bio-psychosocial approach
Consider other MDT involvement and mainstream service involvement to facilitate outcomes and/or CPA
Agree expected outcomes with patients and carers
Giving information to carers / users regarding the diagnosis and prognosis
Management of treatment resistant conditions through
Go back to Pathway
TIER 3
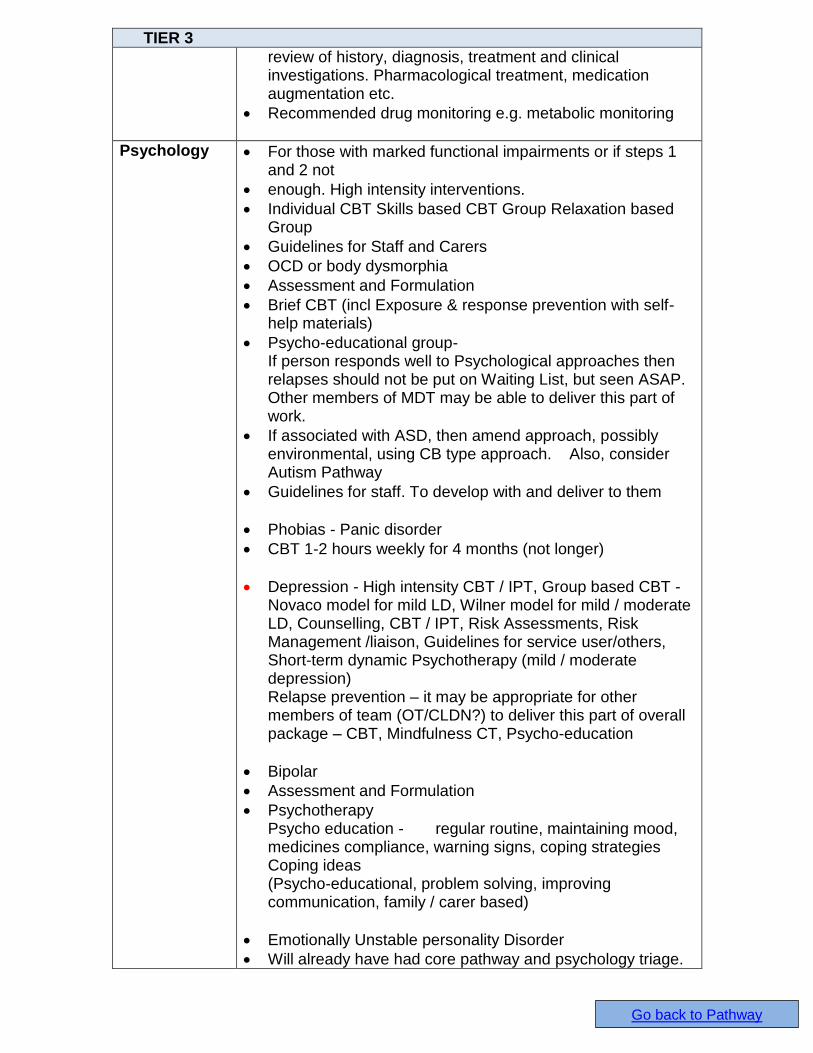
review of history, diagnosis, treatment and clinical investigations. Pharmacological treatment, medication augmentation etc.
Recommended drug monitoring e.g. metabolic monitoring
Psychology For those with marked functional impairments or if steps 1 and 2 not
enough. High intensity interventions.
Individual CBT Skills based CBT Group Relaxation based Group
Guidelines for Staff and Carers
OCD or body dysmorphia
Assessment and Formulation
Brief CBT (incl Exposure & response prevention with self-help materials)
Psycho-educational group- If person responds well to Psychological approaches then relapses should not be put on Waiting List, but seen ASAP. Other members of MDT may be able to deliver this part of work.
If associated with ASD, then amend approach, possibly environmental, using CB type approach. Also, consider Autism Pathway
Guidelines for staff. To develop with and deliver to them
Phobias - Panic disorder
CBT 1-2 hours weekly for 4 months (not longer)
Depression - High intensity CBT / IPT, Group based CBT - Novaco model for mild LD, Wilner model for mild / moderate LD, Counselling, CBT / IPT, Risk Assessments, Risk Management /liaison, Guidelines for service user/others, Short-term dynamic Psychotherapy (mild / moderate depression) Relapse prevention – it may be appropriate for other members of team (OT/CLDN?) to deliver this part of overall package – CBT, Mindfulness CT, Psycho-education
Bipolar
Assessment and Formulation
Psychotherapy Psycho education - regular routine, maintaining mood, medicines compliance, warning signs, coping strategies Coping ideas (Psycho-educational, problem solving, improving communication, family / carer based)
Emotionally Unstable personality Disorder
Will already have had core pathway and psychology triage.
Go back to Pathway

TIER 3
Assessment and Formulation
NICE Guidelines for psychological approaches for people with emotionally unstable personality disorder suggest a minimum of 18months intervention Frequency may be weekly or fortnightly and may reduce towards end of work. Attachment work - supporting them and the MDT to manage endings and support transitions to minimise distress and enable coping.
Support other colleagues with issues of dynamics such as ‘splitting’’ idealisation’’ polarisation’ etc
Reflective work with team colleagues
Stop & Think Group
Individual Stop & Think Staff / Carer work -
Crisis Management / Risk Management - assessing risk and developing risk/crisis management plans as part of or in addition to their ongoing therapeutic work.
Assessment and formulation, Intervention
Teaching re PD/attachment re an individual
Psychosis - Acute phase
Assessment and Formulation
CBT Family Intervention (Psycho-educational, crisis management, problem-solving, relationships & expressed emotions)
Hearing Voices Group Individual hearing voices workbook Trauma based
Community Nursing
Education and support: Provide information on Mental Health wellbeing and how to
keep yourself well. Recognise signs and symptoms of mental health. Education on side effects. Education on keeping mood charts/diary. Education regarding access to other services. Provide personality disorder training and/or accessible information.
Assessment: HADS, OK health, ‘Who am I?’ self-awareness pack, self-
esteem questionnaire, functional analysis, risk assessments, CPA.
Storm Assessment? (call staff to be trained) Metabolic monitoring. West Wales capacity/consent.
Statement of advanced wishes. Intervention: One to one work with patient/carer/support on depression,
anxiety, bipolar, psychosis. CBT/talking therapies. Depression group, relaxation, bereavement work,
Go back to Pathway

TIER 3
anxiety/anger management, group/clinic one to ones, desensitisation, self-esteem work. Mindfulness, admin – depots, relationship work, keeping safe, CPA/MDT working, medication monitor, psychological interventions.
‘Stop. Think’ personality disorder Contingency/crisis plans.
Speech and Language Therapy
Education and support: Specific training around an individual or (with appropriate fee) for services supporting individuals within a mental health setting or living in the community with legal restrictions relating to their mental health status in place. Assessment: Assessment of communication within the context of the mental health issues, along with attendant issues such as high levels of CB, personality disorder, autism spectrum disorder. This should contribute to any wider risk assessment being undertaken. It is essential to consider any legal restrictions relating to the client. Bryan and Roach (2001) note that “Speech and language assessment in psychiatry may…contribute information to assist psychiatric diagnosis.” Intervention: Intervention may involve working with the individual in order to enhance current, or develop new communication skills, it may involve supporting carers to enhance or develop new communication skills. It may additionally involve recommending environmental changes to better support the individual’s communication within the restrictions that may need to be imposed as a matter of law. Interventions can be framed within the Royal College of Speech and Language Therapists’ (2014) Five Good Communication Standards, and in terms of the Proactive, Active and Reactive strategies which underpin best practice when working with individuals who challenge.
Occupational therapy
Assessment: OT’s use a range of different assessment methods looking
at functional and cognitive skills, for activities of daily living, activity levels, engagement in occupations, sensory needs and wellbeing, in order to understand how the person’s mental health impacts on them and make appropriate advice/recommendations.
Sensory integration therapy: Evidence suggests that Sensory Integration Therapy programs can reduce challenging behaviour and self-stimulatory behaviour (Reisman, 1993), improve interaction with the environment (Green et al, 2003) and improve a person’s attention and performance in daily activities (Urwin, 2004).
Sensory assessment: Observations of each modality i.e. tactile, visual etc.
Go back to Pathway

TIER 3
Assessment of ADL (personal, productive and independence) linking in with the recovery model and social inclusion.
MOHOST (model of human occupation screening tool) Environmental assessment, AMPs (assessment of process and motor skills) Activity analysis / meaningful activities Provide practical input which involves modelling providing
guidelines to problem solve promoting skills and grading tasks
Goal setting To consider future planning/accommodation needs Depression screening Intervention: Psychosocial education / group work for anger / anxiety
management / depression(references/pictorial timetables) Part of MDT/CPA reviews Meaningful activities/grading activities PADL/DADL advice guidelines skills promotion CBT SI
LD Autism service
Education and Support:
Training, including outside agencies (with cost attached) – often relating to individuals and interventions
Assessment:
Functional analysis (if not previously undertaken
DISDAT, ABAS Intervention: Support may be comissioned if there is a gap in services
Work alongside carers, modelling interventions
Risk assessment
Interventions in crisis situations
Transition support
Physiotherapy Education and Support:
Advise carers on safe practices when using equipment
Support client/carers and advice regarding services available.
Take into consideration of the client and carers wishes/needs are and work in consolidation with them to meet this.
Assessment:
FRAT Falls assessment and care plan ( part of core assessment)
General Physiotherapy Assessment to identify Physiotherapy needs: Postural Management, Mobility & falls assessment to include Tinetti, Berg balance, Elderly mobility scale, specialist sleep system, seating systems
Go back to Pathway
TIER 3
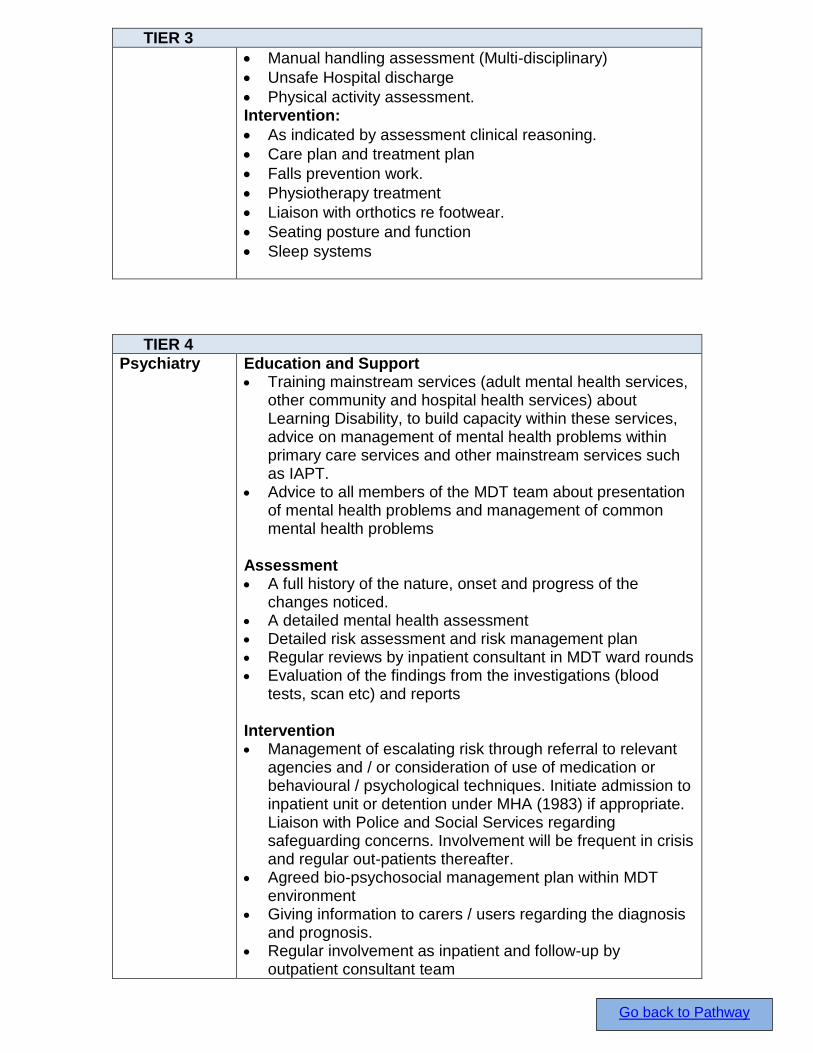
Manual handling assessment (Multi-disciplinary)
Unsafe Hospital discharge
Physical activity assessment. Intervention:
As indicated by assessment clinical reasoning.
Care plan and treatment plan
Falls prevention work.
Physiotherapy treatment
Liaison with orthotics re footwear.
Seating posture and function
Sleep systems
TIER 4
Psychiatry Education and Support Training mainstream services (adult mental health services,
other community and hospital health services) about Learning Disability, to build capacity within these services, advice on management of mental health problems within primary care services and other mainstream services such as IAPT.
Advice to all members of the MDT team about presentation of mental health problems and management of common mental health problems
Assessment A full history of the nature, onset and progress of the
changes noticed. A detailed mental health assessment Detailed risk assessment and risk management plan Regular reviews by inpatient consultant in MDT ward rounds Evaluation of the findings from the investigations (blood
tests, scan etc) and reports Intervention Management of escalating risk through referral to relevant
agencies and / or consideration of use of medication or behavioural / psychological techniques. Initiate admission to inpatient unit or detention under MHA (1983) if appropriate. Liaison with Police and Social Services regarding safeguarding concerns. Involvement will be frequent in crisis and regular out-patients thereafter.
Agreed bio-psychosocial management plan within MDT environment
Giving information to carers / users regarding the diagnosis and prognosis.
Regular involvement as inpatient and follow-up by outpatient consultant team
Go back to Pathway
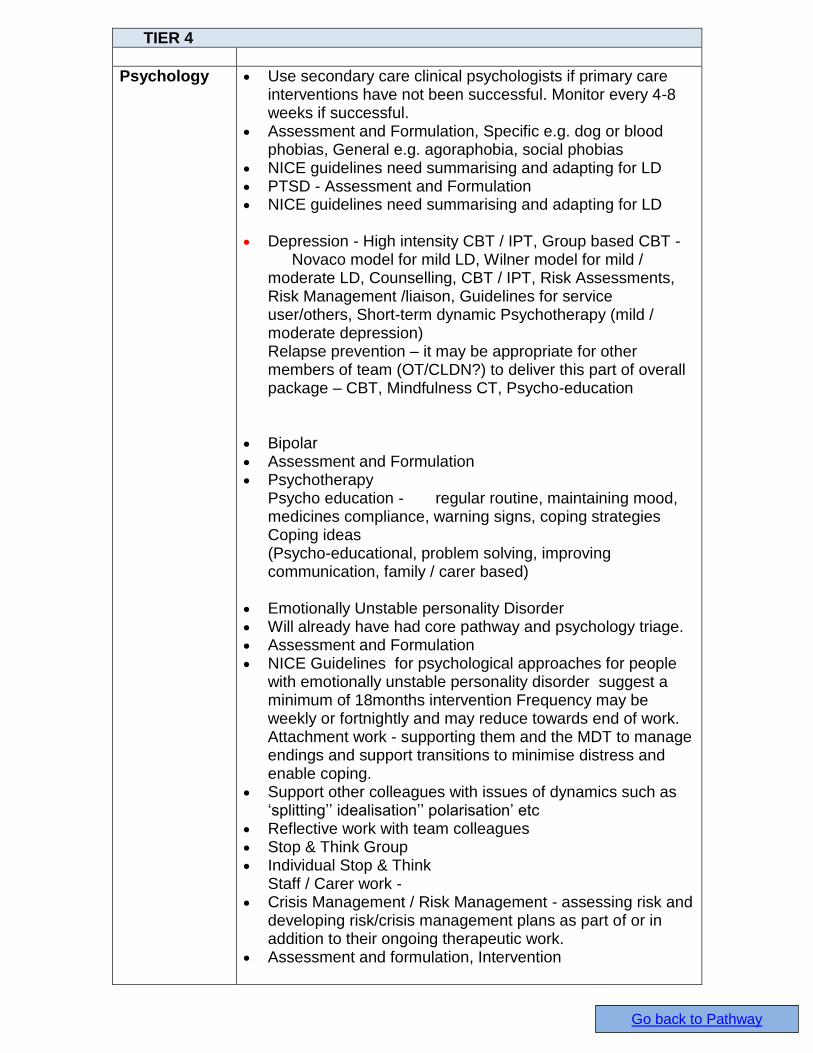
TIER 4
Psychology Use secondary care clinical psychologists if primary care interventions have not been successful. Monitor every 4-8 weeks if successful.
Assessment and Formulation, Specific e.g. dog or blood phobias, General e.g. agoraphobia, social phobias
NICE guidelines need summarising and adapting for LD PTSD - Assessment and Formulation NICE guidelines need summarising and adapting for LD Depression - High intensity CBT / IPT, Group based CBT -
Novaco model for mild LD, Wilner model for mild / moderate LD, Counselling, CBT / IPT, Risk Assessments, Risk Management /liaison, Guidelines for service user/others, Short-term dynamic Psychotherapy (mild / moderate depression) Relapse prevention – it may be appropriate for other members of team (OT/CLDN?) to deliver this part of overall package – CBT, Mindfulness CT, Psycho-education
Bipolar Assessment and Formulation Psychotherapy
Psycho education - regular routine, maintaining mood, medicines compliance, warning signs, coping strategies Coping ideas (Psycho-educational, problem solving, improving communication, family / carer based)
Emotionally Unstable personality Disorder Will already have had core pathway and psychology triage. Assessment and Formulation NICE Guidelines for psychological approaches for people
with emotionally unstable personality disorder suggest a minimum of 18months intervention Frequency may be weekly or fortnightly and may reduce towards end of work. Attachment work - supporting them and the MDT to manage endings and support transitions to minimise distress and enable coping.
Support other colleagues with issues of dynamics such as ‘splitting’’ idealisation’’ polarisation’ etc
Reflective work with team colleagues Stop & Think Group Individual Stop & Think
Staff / Carer work - Crisis Management / Risk Management - assessing risk and
developing risk/crisis management plans as part of or in addition to their ongoing therapeutic work.
Assessment and formulation, Intervention
Go back to Pathway

TIER 4
Teaching re PD/attachment re an individual Psychosis - Acute phase Assessment and Formulation CBT
Family Intervention (Psycho-educational, crisis management, problem-solving, relationships & expressed emotions)
Hearing Voices Group Individual hearing voices workbook Trauma based
Community Nursing
Education and support: Follow crisis plan. Educate patients and carers about
support available – out of hours. Support access to inpatients if admission required.
Assessment: Support AMP. Risk assessments. Intervention: Liaising with wider MDT – Psychiatry, Crisis Team,
Outreach, GP, AMP. Request mental health assessment form.
Speech and Language Therapy
Education and support: Specific training around an individual or (with appropriate fee) for services supporting individuals within a mental health setting or living in the community with legal restrictions relating to their mental health status in place. Assessment: Assessment of communication within the context of the mental health issues, along with attendant issues such as high levels of CB, personality disorder, autism spectrum disorder. This should contribute to any wider risk assessment being undertaken. It is essential to consider any legal restrictions relating to the client. Bryan and Roach (2001) note that “Speech and language assessment in psychiatry may…contribute information to assist psychiatric diagnosis.” Intervention: Intervention may involve working with the individual in order to enhance current, or develop new communication skills, it may involve supporting carers to enhance or develop new communication skills. It may additionally involve recommending environmental changes to better support the individual’s communication within the restrictions that may need to be imposed as a matter of law. Interventions can be framed within the Royal College of Speech and Language Therapists’ (2014) Five Good Communication Standards, and in terms of the Proactive, Active and Reactive
Go back to Pathway

TIER 4
strategies which underpin best practice when working with individuals who challenge. NB: At tier 4 there will be a need for greater multi-disciplinary working, cases may be more urgent and complex requiring more intensive input
Occupational therapy
Assessment: All of tier 3 but there would be an expectation that in tier 4
the person would have more complex needs and we would be working as part of an MDT approach. The allocation of this case would be dependent of skills level and experience, case complexity and involvement in additional pathways
Sensory profiling/Sensory integration/ sensory diet Assess for equipment from standard NRS, referral to SSOT
for major adaptations, provision of special equipment for Clients who have full NHS funding or the equipment relates to their learning disability and requires specialist input.
Practical day to day coping strategies linked to psychology
LD Autism service
Education and Support:
Training, including outside agencies (with cost attached) – often relating to individuals and interventions
Assessment:
Functional analysis (if not previously undertaken
DISDAT, ABAS Intervention:
Work alongside carers, modelling interventions
Risk assessment
Interventions in crisis situations
Transition support
Develop strategies to re-engage the person in meaningful routines and planned activities.
Physiotherapy Education and Support:
Advise carers on safe practices when using equipment
Support client/carers and advice regarding services available.
Take into consideration of the client and carers wishes/needs are and work in consolidation with them to meet this.
Assessment:
FRAT Falls assessment and care plan ( part of core assessment)
General Physiotherapy Assessment to identify Physiotherapy needs: Postural Management, Mobility & falls assessment to include Tinetti, Berg balance, Elderly mobility scale, specialist sleep system, seating systems
Manual handling assessment (Multi-disciplinary)
Go back to Pathway

TIER 4
Unsafe Hospital discharge
Physical activity assessment.
Intervention:
As indicated by assessment clinical reasoning.
Care plan and treatment plan
Falls prevention work.
Physiotherapy treatment
Liaison with orthotics re footwear.
Seating posture and function
Sleep systems
Go back to Pathway

Anxiety Diagnosis (ICD-10 ) Generalized Anxiety Disorder Anxiety that is generalized and persistent but not restricted to, or even strongly predominating in, any particular environmental circumstances (i.e. it is "free-floating"). The dominant symptoms are variable but include complaints of persistent nervousness, trembling, muscular tensions, sweating, lightheadedness, palpitations, dizziness, and epigastric discomfort. Fears that the patient or a relative will shortly become ill or have an accident are often expressed. Panic Disorder [Episodic Paroxysmal Anxiety] The essential feature is recurrent attacks of severe anxiety (panic), which are not restricted to any particular situation or set of circumstances and are therefore unpredictable. As with other anxiety disorders, the dominant symptoms include sudden onset of palpitations, chest pain, choking sensations, dizziness, and feelings of unreality (depersonalization or derealization). There is often also a secondary fear of dying, losing control, or going mad. Panic disorder should not be given as the main diagnosis if the patient has a depressive disorder at the time the attacks start; in these circumstances the panic attacks are probably secondary to depression. Social Phobias Fear of scrutiny by other people leading to avoidance of social situations. More pervasive social phobias are usually associated with low self-esteem and fear of criticism. They may present as a complaint of blushing, hand tremor, nausea, or urgency of micturition, the patient sometimes being convinced that one of these secondary manifestations of their anxiety is the primary problem. Symptoms may progress to panic attacks. Agoraphobia A fairly well-defined cluster of phobias embracing fears of leaving home, entering shops, crowds and public places, or travelling alone in trains, buses or planes. Panic disorder is a frequent feature of both present and past episodes. Depressive and obsessional symptoms and social phobias are also commonly present as subsidiary features. Avoidance of the phobic situation is often prominent, and some agoraphobics experience little anxiety because they are able to avoid their phobic situations.
Go back to Pathway
Management and Treatment Broad Approach To Treatment In Anxiety Disorders
Consider the full range of possible co-morbidities when planning treatment Actively consider psychological approaches to treatment When making a decision about the first line of treatment (talking therapies or
medication), consider severity of illness, distress and impairment in functioning. The duration of waiting to uptake a talking therapy would also be significant
Acute Phase Of Treatment
Agree with service user/carers on treatment goals Offer appropriate doses as per guidelines to achieve a significant reduction in
symptoms Once reduction in symptoms is achieved, move to maintenance phase
Maintenance Phase Of Treatment
Focus on maintaining improvement Review dose of medication to maintenance phase Psychoeducation Return to baseline level of functioning
Guidelines for Treatment with Medication
The Frith algorithms Panic Disorder Generalised Anxiety Disorder
NICE Guidelines
Go back to Pathway

Algorithm 15.3 Treatment of generalised anxiety disorder in adults with LD
Generalised anxiety disorder
Cognitive behavioural therapy
or anxiety management training
where applicable
Poor or partial response
Predominantly somatic symptoms Minimal somatic symptoms
Propranolol up to 120mg/day [Note 1]
Poor response or side effects
Start an SSRI (preferably with a long half-life) or venlafaxine or pregabalin
Good response
Good response Poor response
Continue treatment
[Note 3]
Try another SSRI or a tricyclic antidepressant or a small dose of antipsychotc or buspirone or a benzodiazepine [Note 2]
Good response continue
Continue treatment Stop propanolol
Go back to Pathway

OCD Diagnosis (ICD-10) The essential feature is recurrent obsessional thoughts or compulsive acts. Obsessional thoughts are ideas, images, or impulses that enter the patient's mind again and again in a stereotyped form. They are almost invariably distressing and the patient often tries, unsuccessfully, to resist them. They are, however, recognized as his or her own thoughts, even though they are involuntary and often repugnant. Compulsive acts or rituals are stereotyped behaviours that are repeated again and again. They are not inherently enjoyable, nor do they result in the completion of inherently useful tasks. Their function is to prevent some objectively unlikely event, often involving harm to or caused by the patient, which he or she fears might otherwise occur. Usually, this behaviour is recognized by the patient as pointless or ineffectual and repeated attempts are made to resist. Anxiety is almost invariably present. If compulsive acts are resisted the anxiety gets worse.
Go back to Pathway

Treatment and Management
Consider the full range of possible co-morbidities when planning treatment.
Consider pervasive developmental disorders in the differential diagnosis, or as a co-morbidity.
Actively consider psychological approaches to treatment
When making a decision about the first line of treatment (talking therapies or medication), consider severity of illness, distress and impairment in functioning. The duration of waiting to uptake a talking therapy would also be significant
Acute Phase Of Treatment
Agree with service user/carers on treatment goals
Offer appropriate doses as per guidelines to achieve a significant reduction in symptoms
Once reduction in symptoms is achieved, move to maintenance phase
Consider exposure response prevention as part of the CBT approach.
Maintenance Phase Of Treatment
Focus on maintaining improvement
Review dose of medication to maintenance phase
Psychoeducation
Return to baseline level of functioning
Guidelines for Treatment with Medication o The Frith Algorithms o NICE Guidelines
Go back to Pathway

Algorithm 15.1 Treatment of obsessive compulsive disorder (OCD) in adults with LD
Not associated with autistic spectrum disorder
Try psychological approaches
Good response Poor response
Continue
treatment
Try an antidepressant eg paroxetine or fluoxetine
or sertraline
a high dose if required up to BNF
limits
Go back to Pathway
OCD
Associated with autistic spectrum disorder
Poor response
Continue
Treatment
Good response
Try a small dose of antipsychotic
eg haloperidol or risperidone
or olanzapine
Poor response or
side effects
Good response
Continue
Treatment
Withdraw antipsychotic
Try high dose of antidepressant if required upto BNF limits
eg paroxetine or fluoxetine or sertraline or clomipramine
Good response
Continue
treatment
Poor response or
side effects
Try a combination of small doses of an atypical antipsychotic and SSRI
eg risperidone and paroxetine
Try psychological approaches

Depression Diagnosis Depressive Episode In typical mild, moderate, or severe depressive episodes, the patient suffers from lowering of mood, reduction of energy, and decrease in activity. Capacity for enjoyment, interest, and concentration is reduced, and marked tiredness after even minimum effort is common. Sleep is usually disturbed and appetite diminished. Self-esteem and self-confidence are almost always reduced and, even in the mild form, some ideas of guilt or worthlessness are often present. The lowered mood varies little from day to day, is unresponsive to circumstances and may be accompanied by so-called "somatic" symptoms, such as loss of interest and pleasurable feelings, waking in the morning several hours before the usual time, depression worst in the morning, marked psychomotor retardation, agitation, loss of appetite, weight loss, and loss of libido. Depending upon the number and severity of the symptoms, a depressive episode may be specified as mild, moderate or severe. Mild Depressive Episode Two or three of the above symptoms are usually present. The patient is usually distressed by these but will probably be able to continue with most activities. Moderate Depressive Episode Four or more of the above symptoms are usually present and the patient is likely to have great difficulty in continuing with ordinary activities. Severe Depressive Episode Without Psychotic Symptoms An episode of depression in which several of the above symptoms are marked and distressing, typically loss of self-esteem and ideas of worthlessness or guilt. Suicidal thoughts and acts are common and a number of "somatic" symptoms are usually present. Severe Depressive Episode With Psychotic Symptoms An episode of depression as described in F32.2, but with the presence of hallucinations, delusions, psychomotor retardation, or stupor so severe that ordinary social activities are impossible; there may be danger to life from suicide, dehydration, or starvation. The hallucinations and delusions may or may not be mood-congruent. Recurrent Depressive Disorder A disorder characterized by repeated episodes of depression as described for depressive episode (F32.-), without any history of independent episodes of mood elevation and increased energy (mania). There may, however, be brief episodes of mild mood elevation and overactivity (hypomania) immediately after a depressive episode, sometimes precipitated by antidepressant treatment. The more severe forms of recurrent depressive disorder (F33.2 and F33.3) have much in common with earlier concepts such as manic-depressive depression, melancholia, vital depression and endogenous depression. The first episode may occur at any age from childhood to old age, the onset may be either acute or insidious, and the duration varies from a few weeks to many months. The risk that a patient with recurrent depressive disorder will have an episode of mania never disappears completely, however many depressive episodes have been experienced. If such an episode does occur, the diagnosis should be changed to bipolar affective disorder (F31.-).
Go back to Pathway

Management and Treatment
Broad Approach To Treatment In Depressive Disorders
Consider the full range of possible co-morbidities when planning treatment
Actively consider psychological approaches to treatment
When making a decision about the first line of treatment (talking therapies or medication), consider severity of illness, distress and impairment in functioning. The duration of waiting to uptake a talking therapy would also be significant
Consider whether part of a recurrent depressive disorder or bipolar disorder
Acute Phase Of Treatment
Agree with service user/carers on treatment goals
Offer appropriate doses as per guidelines to achieve a significant reduction in symptoms
Once reduction in symptoms is achieved, move to maintenance phase
Maintenance Phase Of Treatment Focus on maintaining improvement Review dose of medication to maintenance phase Consider prophylaxis if recurrent depression or bipolar disorder Psychoeducation Return to baseline level of functioning
Guidelines for Treatment with Medication The Frith Algorithms NICE Guidelines
Go back to Pathway
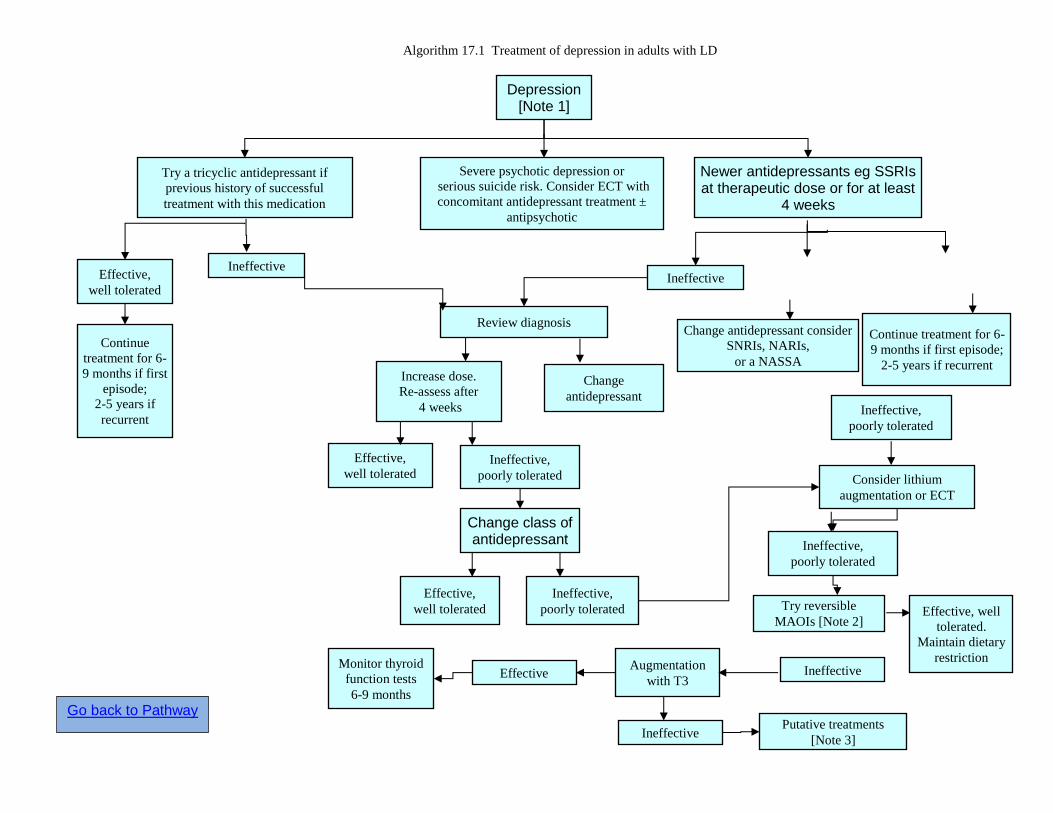
Algorithm 17.1 Treatment of depression in adults with LD
Depression [Note 1]
Severe psychotic depression or
serious suicide risk. Consider ECT with
concomitant antidepressant treatment ±
antipsychotic
Try a tricyclic antidepressant if
previous history of successful
treatment with this medication
Effective,
well tolerated Ineffective
Continue
treatment for 6-
9 months if first
episode;
2-5 years if
recurrent
Change antidepressant consider
SNRIs, NARIs,
or a NASSA Increase dose.
Re-assess after
4 weeks
Change
antidepressant
Effective,
well tolerated Ineffective,
poorly tolerated
Change class of antidepressant
Effective,
well tolerated
Ineffective,
poorly tolerated
Consider lithium
augmentation or ECT
Ineffective,
poorly tolerated
Try reversible
MAOIs [Note 2]
Ineffective
Effective, well
tolerated.
Maintain dietary
restriction
Ineffective Putative treatments
[Note 3]
Ineffective,
poorly tolerated
Newer antidepressants eg SSRIs at therapeutic dose or for at least
4 weeks
Review diagnosis Continue treatment for 6-
9 months if first episode;
2-5 years if recurrent
Augmentation
with T3 Effective
Monitor thyroid
function tests
6-9 months
Ineffective
Go back to Pathway

Bipolar Disorder
Diagnosis Bipolar Affective Disorder A disorder characterized by two or more episodes in which the patient's mood and activity levels are significantly disturbed, this disturbance consisting on some occasions of an elevation of mood and increased energy and activity (hypomania or mania) and on others of a lowering of mood and decreased energy and activity (depression). Repeated episodes of hypomania or mania only are classified as bipolar. Bipolar Affective Disorder, Current Episode Hypomanic The patient is currently hypomanic, and has had at least one other affective episode (hypomanic, manic, depressive, or mixed) in the past. Bipolar Affective Disorder, Current Episode Manic Without Psychotic Symptoms The patient is currently manic, without psychotic symptoms (as in F30.1), and has had at least one other affective episode (hypomanic, manic, depressive, or mixed) in the past. Bipolar Affective Disorder, Current Episode Manic With Psychotic Symptoms The patient is currently manic, with psychotic symptoms (as in F30.2), and has had at least one other affective episode (hypomanic, manic, depressive, or mixed) in the past. Bipolar Affective Disorder, Current Episode Mild Or Moderate Depression The patient is currently depressed, as in a depressive episode of either mild or moderate severity (F32.0 or F32.1), and has had at least one authenticated hypomanic, manic, or mixed affective episode in the past. Bipolar Affective Disorder, Current Episode Severe Depression Without Psychotic Symptoms The patient is currently depressed, as in severe depressive episode without psychotic symptoms (F32.2), and has had at least one authenticated hypomanic, manic, or mixed affective episode in the past. Bipolar Affective Disorder, Current Episode Severe Depression With Psychotic Symptoms The patient is currently depressed, as in severe depressive episode with psychotic symptoms (F32.3), and has had at least one authenticated hypomanic, manic, or mixed affective episode in the past. Bipolar Affective Disorder, Current Episode Mixed The patient has had at least one authenticated hypomanic, manic, depressive, or mixed affective episode in the past, and currently exhibits either a mixture or a rapid alteration of manic and depressive symptoms. Bipolar Affective Disorder, Currently In Remission The patient has had at least one authenticated hypomanic, manic, or mixed affective episode in the past, and at least one other affective episode (hypomanic, manic, depressive, or mixed) in addition, but is not currently suffering from any significant mood disturbance, and has not done so for several months. Periods of remission during prophylactic treatment should be coded here.
Go back to Pathway
Management and Treatment
Broad Approach To Treatment In Bpad Consider whether part of a recurrent depressive disorder or bipolar
disorder. Due consideration to prophylaxis
Acute Phase Of Treatment Agree with service user/carers on treatment goals Offer appropriate doses as per guidelines to achieve a significant
reduction in symptoms Once reduction in symptoms is achieved, move to maintenance phase
Maintenance Phase Of Treatment Focus on maintaining improvement Review dose of medication to maintenance phase. Psychoeducation Return to baseline level of functioning
Guidelines for Treatment with Medication
The Frith Algorithms NICE Guidelines
Go back to Pathway
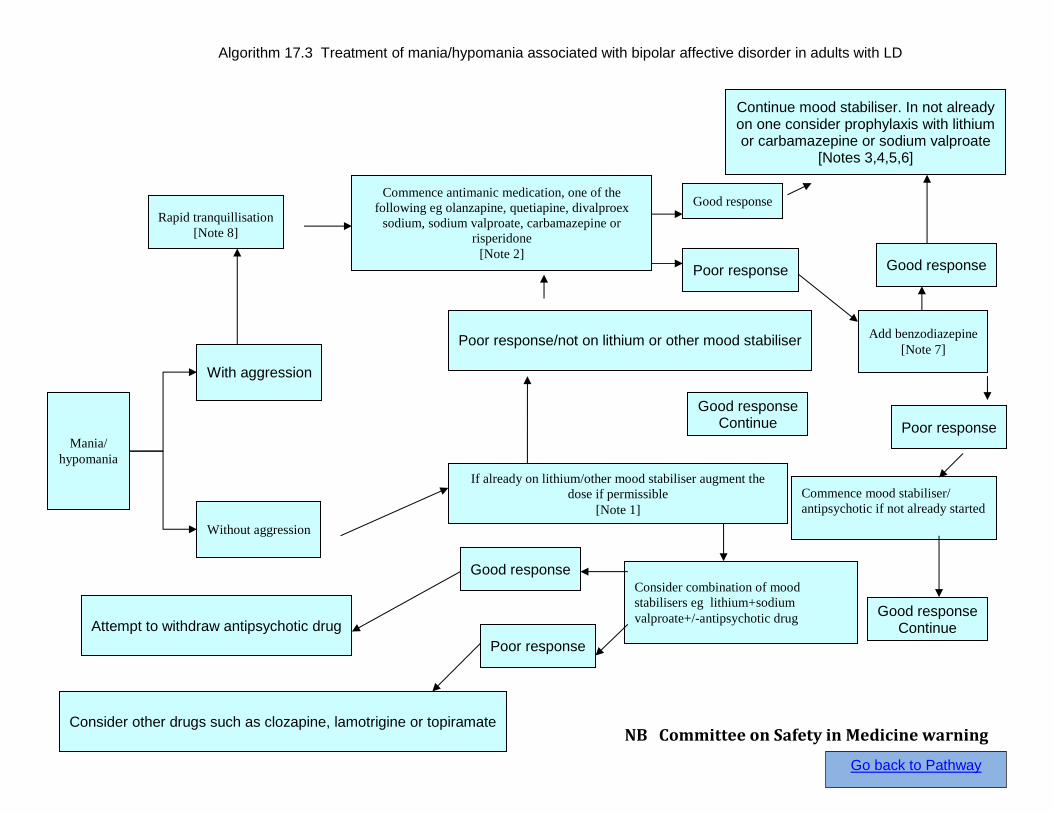
Algorithm 17.3 Treatment of mania/hypomania associated with bipolar affective disorder in adults with LD
With aggression
Rapid tranquillisation
[Note 8]
Commence antimanic medication, one of the
following eg olanzapine, quetiapine, divalproex
sodium, sodium valproate, carbamazepine or
risperidone
[Note 2]
Without aggression
Consider combination of mood
stabilisers eg lithium+sodium
valproate+/-antipsychotic drug
Good response
Poor response
Mania/
hypomania
Commence mood stabiliser/
antipsychotic if not already started
Add benzodiazepine
[Note 7]
Continue mood stabiliser. In not already on one consider prophylaxis with lithium or carbamazepine or sodium valproate
[Notes 3,4,5,6]
Poor response
Good response
Good response Continue Attempt to withdraw antipsychotic drug
Consider other drugs such as clozapine, lamotrigine or topiramate
Poor response
Good response
If already on lithium/other mood stabiliser augment the
dose if permissible
[Note 1]
Poor response/not on lithium or other mood stabiliser
Good response Continue
NB Committee on Safety in Medicine warning
Go back to Pathway
Psychosis Diagnosis Schizophrenia The schizophrenic disorders are characterized in general by fundamental and characteristic distortions of thinking and perception, and affects that are inappropriate or blunted. Clear consciousness and intellectual capacity are usually maintained although certain cognitive deficits may evolve in the course of time. The most important psychopathological phenomena include thought echo; thought insertion or withdrawal; thought broadcasting; delusional perception and delusions of control; influence or passivity; hallucinatory voices commenting or discussing the patient in the third person; thought disorders and negative symptoms. The course of schizophrenic disorders can be either continuous, or episodic with progressive or stable deficit, or there can be one or more episodes with complete or incomplete remission. The diagnosis of schizophrenia should not be made in the presence of extensive depressive or manic symptoms unless it is clear that schizophrenic symptoms antedate the affective disturbance. Nor should schizophrenia be diagnosed in the presence of overt brain disease or during states of drug intoxication or withdrawal. Similar disorders developing in the presence of epilepsy or other brain disease should be classified under F06.2, and those induced by psychoactive substances under F10-F19 with common fourth character .5.
Go back to Pathway

Management and Treatment Broad Approach To Treatment In Psychotic Disorders
Focus on containing risks Consider joint working with teams like PIER
Acute Phase Of Treatment
Agree with service user/carers on treatment goals Offer appropriate doses as per guidelines to achieve a significant
reduction in symptoms Once reduction in symptoms is achieved, move to maintenance
phase
Maintenance Phase Of Treatment Focus on maintaining improvement Review dose of medication to maintenance phase. Psychoeducation Return to baseline level of functioning
Guidelines for Treatment with Medication
NICE Guidelines
Go back to Pathway

Algorithm 15.2 Treatment of panic disorders in adults with LD
Panic disorders
Try cognitive behaviour therapy
or anxiety management
Good response Continue treatment
Partial or poor response
Try an SSRI or SNRI
eg paroxetine, sertaline,
escitalopram or venlafaxine
Try imipramine
Try benzodiazepines
Try propranolol
Partial or poor response
Partial or poor response
Partial or poor response
Good response
Good response
Good response
Good response
Continue treatment
Continue treatment
Continue treatment
Continue treatment but limit to 4 weeks
Go back to Pathway

Approach to Treatment Resistant Conditions
o Review history o Review diagnosis o Review doses of medication o Review compliance to treatment o Consider undiagnosed co-morbidites
Review investigations: consider neuro-imaging Consider exploring for other developmental disorders
o Consider influence of environmental factors o Consider other classes of drugs, augmentation strategies o Consider a period of assessment in the inpatient unit
Go back to Pathway