methamphetamine and the brain: new knowledge; new treatments methamphetamine and the brain: new...
TRANSCRIPT
Methamphetamine and the Methamphetamine and the Brain: New Knowledge; New Brain: New Knowledge; New
TreatmentsTreatmentsRichard A. Rawson, Ph.DRichard A. Rawson, Ph.D
Adjunct Associate ProfessorAdjunct Associate ProfessorSemel Institute for Neuroscience and Human BehaviorSemel Institute for Neuroscience and Human Behavior
David Geffen School of MedicineDavid Geffen School of MedicineUniversity of California at Los AngelesUniversity of California at Los Angeles
[email protected]@mednet.ucla.edu
Supported by:Supported by: National Institute on Drug Abuse (NIDA)National Institute on Drug Abuse (NIDA)
Pacific Southwest Technology Transfer CenterPacific Southwest Technology Transfer Center (SAMHSA) (SAMHSA)International Network of Treatment and Rehabilitation Resource Centres (UNODC)International Network of Treatment and Rehabilitation Resource Centres (UNODC)
MethamphetamineMethamphetamine
The DrugThe Drug

Forms of MethamphetamineForms of Methamphetamine
Methamphetamine Powder
IDU Description: Beige/yellowy/off-white powder
Base / Paste Methamphetamine
IDU Description: ‘Oily’, ‘gunky’, ‘gluggy’ gel, moist, waxy
Crystalline Methamphetamine
IDU Description: White/clear crystals/rocks; ‘crushed glass’ / ‘rock salt’
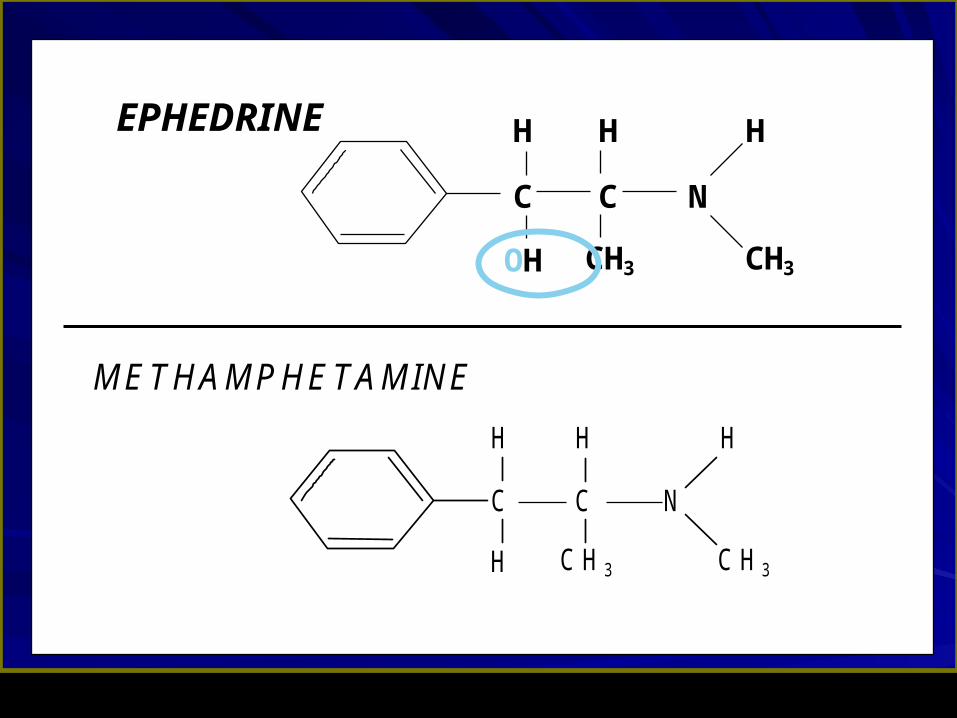
EPHEDRINE
OH
CC
HHH
3CH 3CH
N
M ETH AM PH ETAM IN E
H
CC
HHH
3CH 3CH
N

MethamphetamineMethamphetamine
The US EpidemicThe US Epidemic

According to surveys and estimates by WHO According to surveys and estimates by WHO and UNODC, methamphetamine is the most and UNODC, methamphetamine is the most widely used illicit drug in the world except for widely used illicit drug in the world except for cannabis.cannabis.
World wide it is estimated there are over 26 World wide it is estimated there are over 26 million regular users of million regular users of amphetamine/methamphetamine, as compared amphetamine/methamphetamine, as compared to approximately 16 million heroin users and 14 to approximately 16 million heroin users and 14 million cocaine usersmillion cocaine users
Scope of the Methamphetamine Scope of the Methamphetamine Problem WorldwideProblem Worldwide
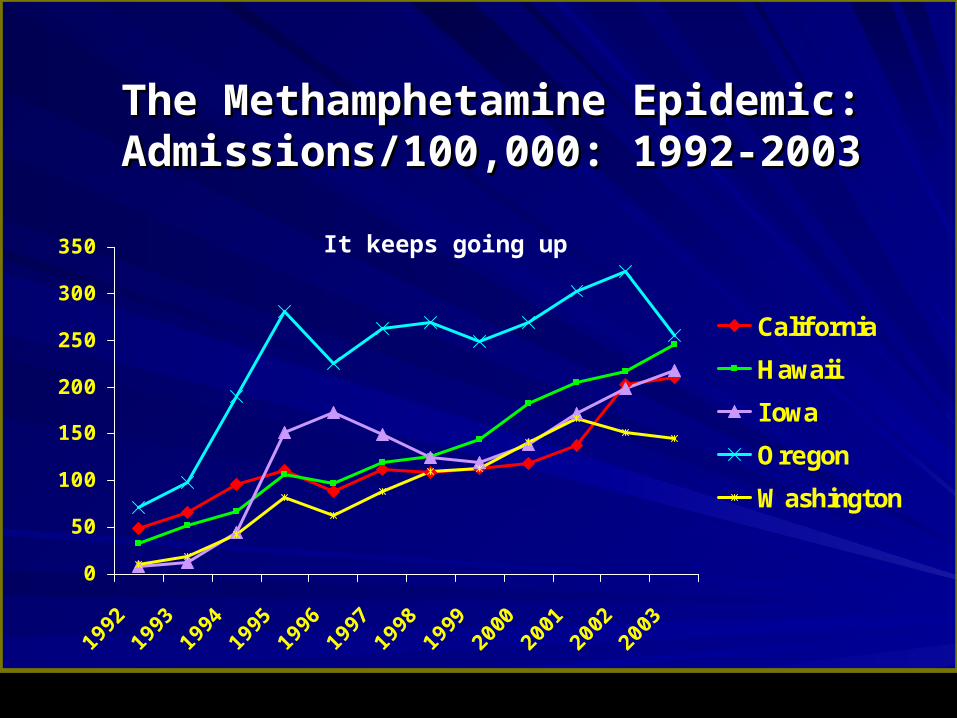
The Methamphetamine Epidemic:The Methamphetamine Epidemic:Admissions/100,000: 1992-2003Admissions/100,000: 1992-2003
0
50
100
150
200
250
300
350
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
California
Hawaii
I owa
Oregon
Washington
It keeps going up
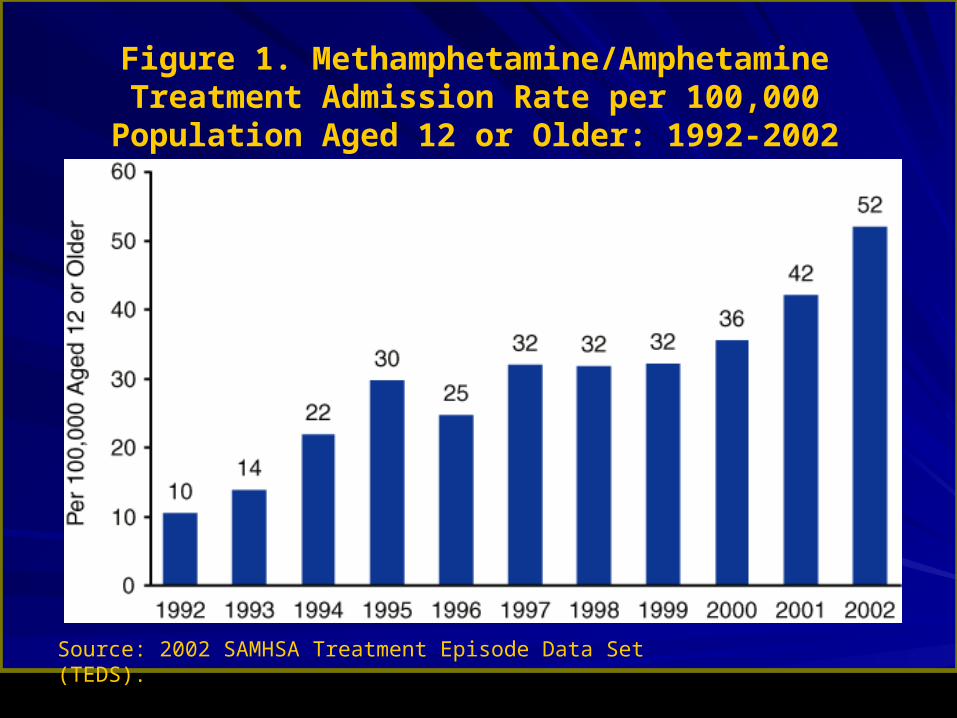
Figure 1. Methamphetamine/Amphetamine Treatment Admission Rate per 100,000 Population Aged 12 or Older:
1992-2002
Source: 2002 SAMHSA Treatment Episode Data Set (TEDS).

Figure 2. Methamphetamine/Amphetamine Treatment Admissions, by Route of Administration: 1992-2002
Source: 2002 SAMHSA Treatment Episode Data Set (TEDS).

The Eastward Spread of The Eastward Spread of MethamphetamineMethamphetamine
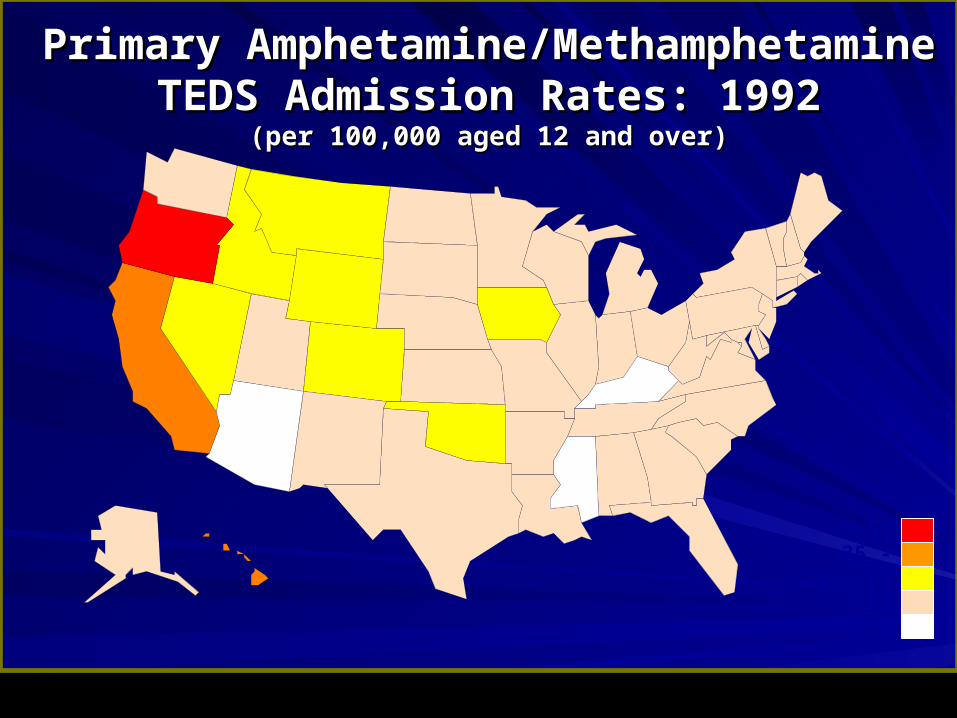
Primary Amphetamine/Methamphetamine Primary Amphetamine/Methamphetamine TEDS Admission Rates: 1992TEDS Admission Rates: 1992
(per 100,000 aged 12 and over)(per 100,000 aged 12 and over)
35 - 5812 - 35
< 12No data
> 58

< 12
Primary Amphetamine/Methamphetamine Primary Amphetamine/Methamphetamine TEDS Admission Rates: 1997TEDS Admission Rates: 1997
(per 100,000 aged 12 and over)(per 100,000 aged 12 and over)
35 - 5812 - 35
< 12No
data
> 58
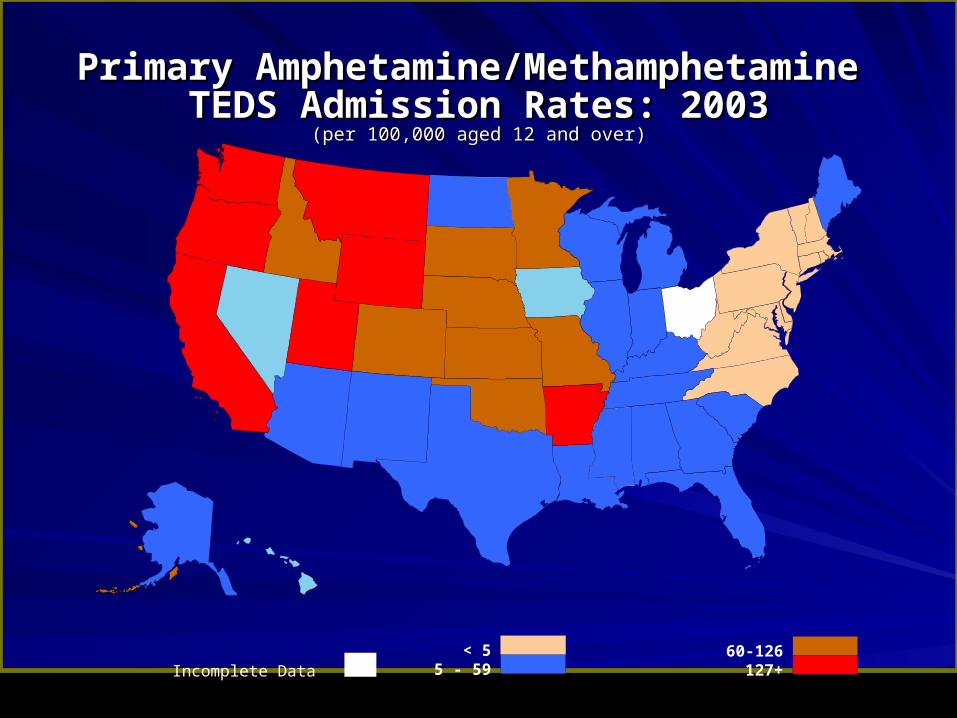
Primary Amphetamine/Methamphetamine Primary Amphetamine/Methamphetamine TEDS Admission Rates: 2003TEDS Admission Rates: 2003
(per 100,000 aged 12 and over)(per 100,000 aged 12 and over)
127+< 5
5 - 5960-126
Incomplete Data

Methamphetamine: A Growing Menace Methamphetamine: A Growing Menace in Rural Americain Rural America
In 1998, rural areas In 1998, rural areas nationwide reported 949 nationwide reported 949 methamphetamine labs. methamphetamine labs.
Last year, 9,385 were Last year, 9,385 were reported. reported.
This year, 4,589 rural labs This year, 4,589 rural labs had been reported as of had been reported as of July 26.July 26.
Source: El Paso Intelligence Center (EPIC), Source: El Paso Intelligence Center (EPIC), U.S. DEAU.S. DEA

MethamphetamineMethamphetamine
Medical/Psychiatric Effects Medical/Psychiatric Effects and Consequencesand Consequences

Cardiovascular problemsCardiovascular problems
↑ ↑ Heart rateHeart ratePalpitations Palpitations Arrhythmia Arrhythmia ↑ ↑ Blood pressureBlood pressure Chest Pain Chest Pain – Acute coronary syndrome Acute coronary syndrome
Valve thickening Valve thickening

Neurological problemsNeurological problems
Seizures Seizures
Stroke Stroke
Cerebral Cerebral hemorrhage hemorrhage
Cerebral vasculitis Cerebral vasculitis
MydriasisMydriasis

Respiratory problemsRespiratory problems
Dyspnea Dyspnea
Pulmonary Pulmonary
hypertension hypertension
Pleuritic chest pain Pleuritic chest pain

Other problemsOther problems
Eye ulcers Eye ulcers
Over-heatingOver-heating
Rhabdomyolysis Rhabdomyolysis
Obstetric complications Obstetric complications
Anorexia / weight loss Anorexia / weight loss
Tooth wear, cavitiesTooth wear, cavities
““Speed bumps”Speed bumps”
TraumaTrauma
Interpersonal Interpersonal traumatrauma– AssaultAssault
– GunshotGunshot
– KnifeKnife
Motor VehiclesMotor Vehicles
Suicide attemptsSuicide attempts

MethamphetamineMethamphetamine
The BrainThe Brain

A Major Reason People Take a Drug is they Like
What It Does to Their Brains
A Major Reason People Take a Drug is they Like
What It Does to Their Brains



00
5050
100100
150150
200200
00 6060 120120 180180
Time (min)Time (min)
% o
f B
asal
DA
Ou
tpu
t%
of
Bas
al D
A O
utp
ut
NAc shellNAc shell
EmptyEmpty
BoxBox FeedingFeeding
Source: Di Chiara et al.Source: Di Chiara et al.
FOODFOOD
100100
150150
200200
DA
Co
nce
ntr
ati
on
(%
Bas
elin
e)D
A C
on
cen
tra
tio
n (
% B
asel
ine)
MountsMountsIntromissionsIntromissionsEjaculationsEjaculations
1515
00
55
1010
Co
pu
latio
n F
req
ue
nc
yC
op
ula
tion
Fre
qu
en
cy
SampleNumberSampleNumber
11 22 33 44 55 66 77 88 99 1010 1111 1212 1313 1414 1515 1616 1717
ScrScrScrScrBasBasFemale 1 PresentFemale 1 Present
ScrScrFemale 2 PresentFemale 2 Present
ScrScr
Source: Fiorino and PhillipsSource: Fiorino and Phillips
SEXSEX
Natural Rewards Elevate Dopamine Natural Rewards Elevate Dopamine LevelsLevels
Natural Rewards Elevate Dopamine Natural Rewards Elevate Dopamine LevelsLevels

00
100100
200200
300300
400400
Time After CocaineTime After Cocaine
% o
f B
as
al
Re
lea
se
% o
f B
as
al
Re
lea
se
DADADOPACDOPACHVAHVA
AccumbensAccumbensCOCAINECOCAINE
00
100100
150150
200200
250250
00 11 22 3 hr3 hr
Time After NicotineTime After Nicotine
% o
f B
as
al
Re
lea
se
% o
f B
as
al
Re
lea
se
AccumbensAccumbensCaudateCaudate
NICOTINENICOTINE
Source: Shoblock and Sullivan; Di Chiara and Imperato
Effects of Drugs on Dopamine ReleaseEffects of Drugs on Dopamine Release
100
150
200
250
0 1 2 3 4hrTime After Ethanol
% o
f B
as
al
Re
lea
se
0.250.512.5
Accumbens
0
Dose (g/kg ip)
ETHANOLETHANOL
Time After Methamphetamine
% B
as
al
Re
lea
se
METHAMPHETAMINE
0 1 2 3hr
1500
1000
500
0
Accumbens
Prolonged Drug Use ChangesProlonged Drug Use Changesthe Brain In Fundamentalthe Brain In Fundamentaland Long-Lasting Waysand Long-Lasting Ways
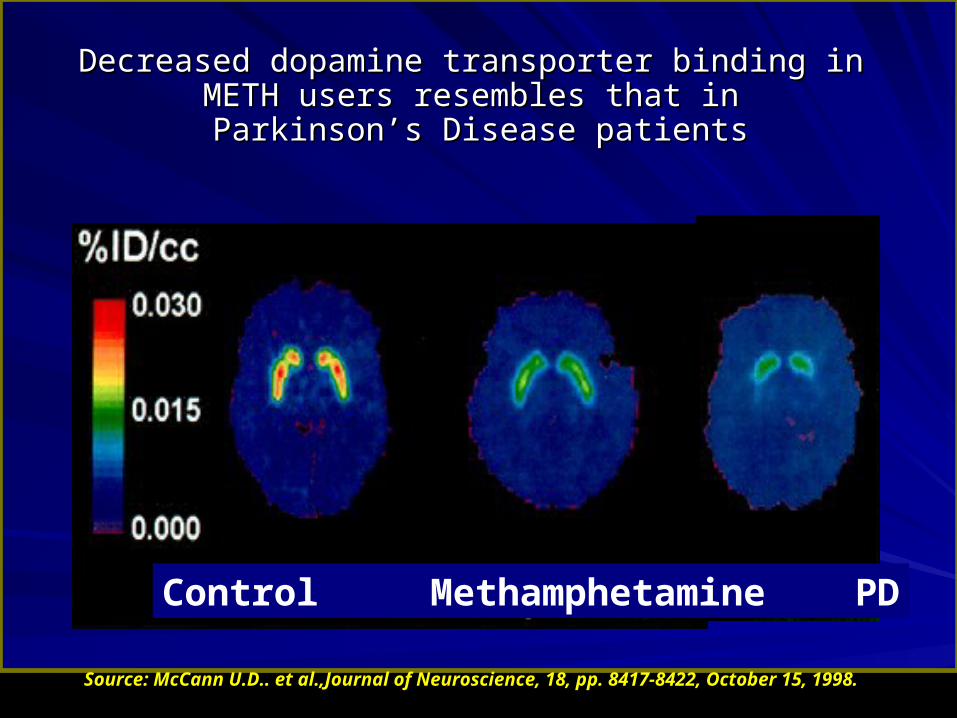
Source: McCann U.D.. et al.,Journal of Neuroscience, 18, pp. 8417-8422, October 15, 1998.
Decreased dopamine transporter binding in METH Decreased dopamine transporter binding in METH users resembles that inusers resembles that in
Parkinson’s Disease patients Parkinson’s Disease patients
Control Methamphetamine PD
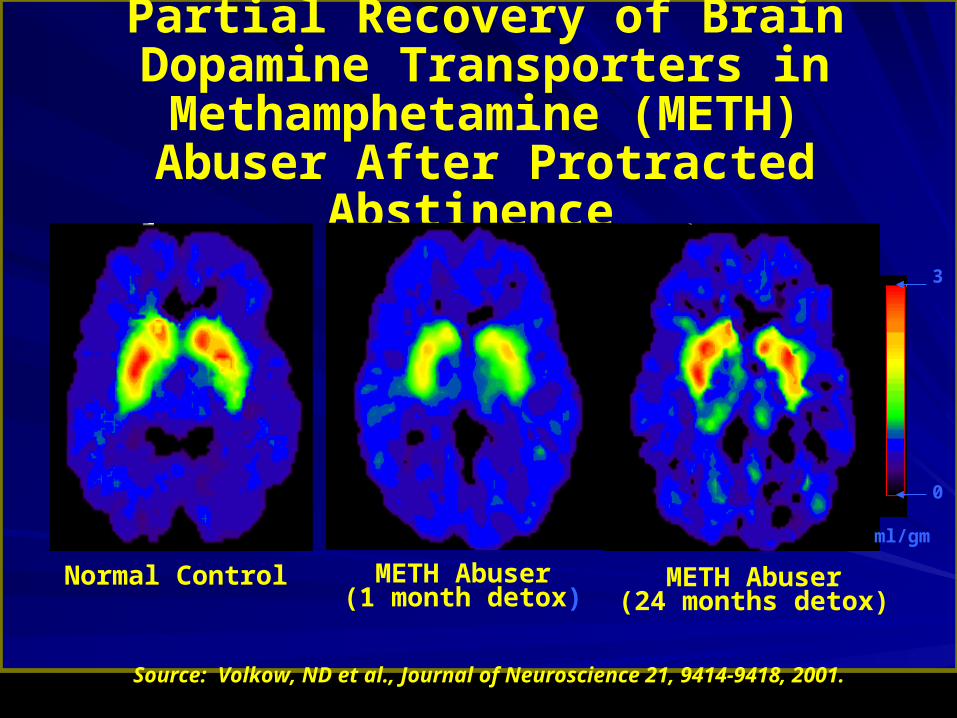
Partial Recovery of Brain Dopamine Transporters in Methamphetamine
(METH)Abuser After Protracted Abstinence
Normal Control METH Abuser(1 month detox)
METH Abuser(24 months detox)
0
3
ml/gm
Source: Volkow, ND et al., Journal of Neuroscience 21, 9414-9418, 2001.







Prolonged Drug Use ChangesProlonged Drug Use Changesthe Brain In Fundamentalthe Brain In Fundamentaland Long-Lasting Waysand Long-Lasting Ways


My sexual My sexual drivedrive is increased by the use of … is increased by the use of …
18.1 20.5
43.9
70.655.3
11.1
85.3
55.6
0102030405060708090
100
Per
cent
Res
pond
ing
"Yes
"
opiates alcohol cocaine meth
Primary Drug of Abuse
malefemale
(Rawson et al., 2002)

My sexual activity is increased by the use of …My sexual activity is increased by the use of …
16.0 18.224.4
38.244.7
11.1
73.5 66.7
0102030405060708090
100
Per
cent
Res
pond
ing
"Yes
"
opiates alcohol cocaine meth
Primary Drug of Abuse
malefemale
(Rawson et al., 2002)

My sexual My sexual performanceperformance is improved by the use of is improved by the use of ……
19.115.9
24.432.4
18.411.1
58.8 61.1
0102030405060708090
100
Per
cent
Res
pond
ing
"Yes
"
opiates alcohol cocaine meth
Primary Drug of Abuse
malefemale
(Rawson et al., 2002)

MethamphetamineMethamphetamine
TreatmentTreatment
MA Treatment IssuesMA Treatment Issues
Acute MA OverdoseAcute MA Overdose
Acute MA PsychosisAcute MA Psychosis
MA “Withdrawal”MA “Withdrawal”
Initiating MA AbstinenceInitiating MA Abstinence
MA Relapse PreventionMA Relapse Prevention
Protracted Cognitive Impairment Protracted Cognitive Impairment and Symptoms of Paranoiaand Symptoms of Paranoia
MA “Withdrawal”MA “Withdrawal”
- Depression- Depression - Paranoia- Paranoia
- Fatigue- Fatigue - Cognitive - Cognitive ImpairmentImpairment
- Anxiety- Anxiety - Agitation- Agitation
- Anergia- Anergia - Confusion- Confusion
Duration: 2 Days - 2 WeeksDuration: 2 Days - 2 Weeks
MedicationsMedications
Currently, there are no medications that can Currently, there are no medications that can quickly and safely reverse life threatening quickly and safely reverse life threatening MA overdose.MA overdose.
There are no medications that can reliably There are no medications that can reliably reduce paranoia and psychotic symptoms, reduce paranoia and psychotic symptoms, that contribute to episodes of dangerous and that contribute to episodes of dangerous and violent behavior associated with MA use.violent behavior associated with MA use.
Bupropion: An efficacious Bupropion: An efficacious pharmacotherapy? pharmacotherapy?
Newton et al 2005 Bupropion reduces Newton et al 2005 Bupropion reduces craving and reinforcing effects of methcraving and reinforcing effects of meth
Elkashef (recently completed) Bupropion Elkashef (recently completed) Bupropion reduces meth use in an outpatient trial, reduces meth use in an outpatient trial, with particularly strong effect with less with particularly strong effect with less severe users. severe users.
Special treatment consideration should be made for Special treatment consideration should be made for the following groups of individuals:the following groups of individuals:
Female MA users (higher rates of depression; very high rates of Female MA users (higher rates of depression; very high rates of previous and present sexual and physical abuse; responsibilities for previous and present sexual and physical abuse; responsibilities for children).children).
Injection MA users (very high rates of psychiatric symptoms; severe Injection MA users (very high rates of psychiatric symptoms; severe withdrawal syndromes; high rates of hepatitis).withdrawal syndromes; high rates of hepatitis).
MA users who take MA daily or in very high doses.MA users who take MA daily or in very high doses.
Homeless, chronically mentally ill and/or individuals with high levels of Homeless, chronically mentally ill and/or individuals with high levels of psychiatric symptoms at admission.psychiatric symptoms at admission.
Individuals under the age of 21.Individuals under the age of 21.
Gay men (at very high risk for HIV and hepatitis).Gay men (at very high risk for HIV and hepatitis).

Treatments for Stimulant-use Disorders with Treatments for Stimulant-use Disorders with Empirical SupportEmpirical Support
Motivational InterviewingMotivational Interviewing
Cognitive-Behavioral Therapy (CBT)Cognitive-Behavioral Therapy (CBT)
Community Reinforcement Approach Community Reinforcement Approach
Contingency ManagementContingency Management
12 Step Facilitation12 Step Facilitation
Matrix ModelMatrix Model
Brief InterventionsBrief Interventions

Methamphetamine Treatment: Controlled Methamphetamine Treatment: Controlled Clinical TrialsClinical Trials
Contingency ManagementContingency Management
Matrix ModelMatrix Model

Contingency ManagementContingency Management
A technique employing the systematic A technique employing the systematic delivery of positive reinforcement for delivery of positive reinforcement for desired behaviors. In the treatment of desired behaviors. In the treatment of methamphetamine dependence, vouchers methamphetamine dependence, vouchers or prizes can be “earned” for submission or prizes can be “earned” for submission of methamphetamine-free urine samples.of methamphetamine-free urine samples.

Mean number of abstinences
0
5
10
15
20
25
CM Control

Mean weeks of consecutive abstinence
0
1
2
3
4
5
6
CM Control

Methamphetamine Outcomes from CTN Methamphetamine Outcomes from CTN 006006
0
2
4
6
8
10
12
14
16
LDA # Negative Urine
Nu
mb
er
of
sa
mp
les
CM (n=55)
Standard care (n=69)


Baseline DemographicsBaseline Demographics
Participants Served (n)Participants Served (n) 10161016
Age (mean)Age (mean) 32.8 years32.8 years
Education (mean)Education (mean) 12.2 years12.2 years
Methamphetamine Use (mean)Methamphetamine Use (mean) 7.5 years7.5 years
Marijuana Use (mean)Marijuana Use (mean) 7.2 years7.2 years
Alcohol Use (mean)Alcohol Use (mean) 7.6 years7.6 years
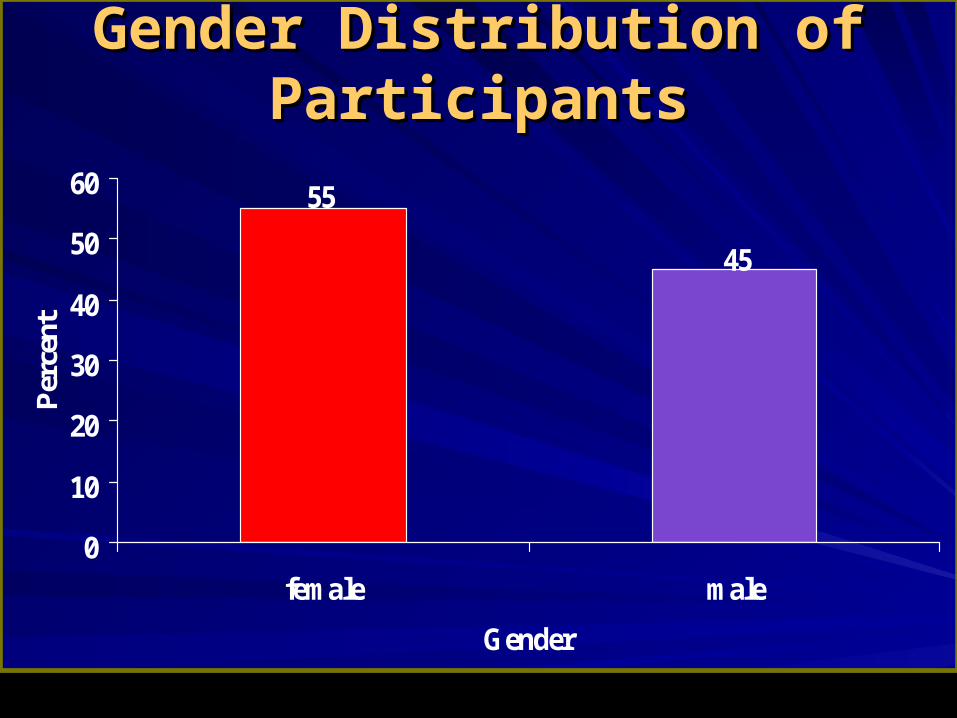
Gender Distribution of Gender Distribution of ParticipantsParticipants
45
55
0
10
20
30
40
50
60
female male
Gender
Per
cent

Days of Methamphetamine Use in Past Days of Methamphetamine Use in Past 30 (ASI)30 (ASI)
4.4
11.5
0
2
4
6
8
10
12
BL Tx end
Mea
n D
ays U
se
Possible is 0-30; tpaired=20.90; p-value<0.000 (highly sig.)
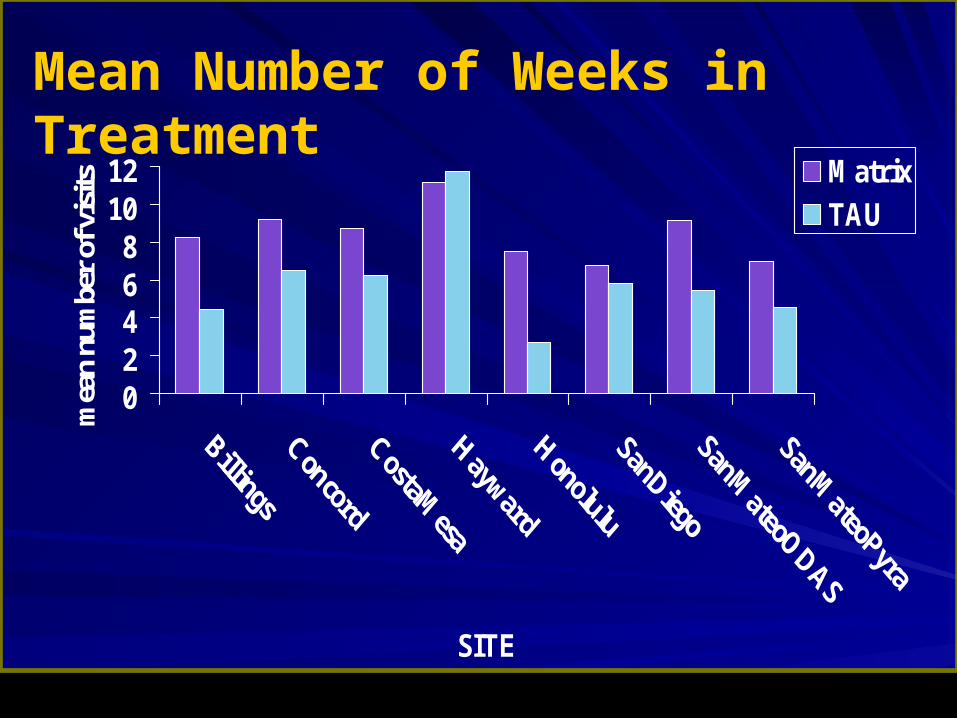
Mean Number of Weeks in Treatment
02468
1012
SITE
mea
n nu
mbe
r of
vis
its MatrixTAU

Mean Number of UA’s that were MA-free Mean Number of UA’s that were MA-free during treatmentduring treatment
0
2
4
6
8
10
SITE
mea
n nu
mbe
r of
MA
-fre
e U
A's Matrix
TAU

Urinalysis Results Urinalysis Results
Results of Ua Tests at Discharge, 6 Results of Ua Tests at Discharge, 6 months and 12 Months post admission **months and 12 Months post admission **
Matrix GroupMatrix Group TAU GroupTAU Group
D/C: 66% MA-freeD/C: 66% MA-free 65% MA-free 65% MA-free
6 Ms: 69% MA-free6 Ms: 69% MA-free 67% MA-free 67% MA-free
12 Ms: 59% MA-free12 Ms: 59% MA-free 55% MA-free 55% MA-free
**Over 80% follow up rate in both groups at all points**Over 80% follow up rate in both groups at all points

Treatment of MA-Use DisordersTreatment of MA-Use Disorders
No medications currently are available with No medications currently are available with evidence of efficacyevidence of efficacy
Two approaches, Contingency Management and Two approaches, Contingency Management and Matrix Model have data to support efficacyMatrix Model have data to support efficacy
MA users appear to respond to other MA users appear to respond to other psychosocial treatments in a manner psychosocial treatments in a manner comparable to other categories of drug users.comparable to other categories of drug users.
MA users are responsive to treatmentMA users are responsive to treatment