michigan medicaid pharmacy cost containment paul reinhart, director medical services administration...
TRANSCRIPT

Michigan Medicaid Pharmacy Cost Containment
Paul Reinhart, Director
Medical Services Administration
Michigan Department of
Community Health
October 8, 2004
2
Conclusions
• Preferred drug list program has reduced the rate of growth in Medicaid pharmaceutical spending
• Savings will grow as more states join the new multi-state initiative
• No adverse beneficiary impact• Medicare pharmacy reform will have both
positive and negative impact on states

3
“Medicaid is the bleeding ulcer of state government.”
State Rep. Marc ShulmanDetroit News, April 19, 2004

4
Growth in Michigan Medicaid Vs. Growth in Michigan Revenue
-20%
0%
20%
40%
60%
80%
100%
FY95 FY97 FY99 FY01 FY03 FY05
Medicaid
Revenue

5
Michigan Medicaid Caseload
1,000
1,050
1,100
1,150
1,200
1,250
1,300
1,350
1,400
1,450
Fiscal Year
In T
hou
san
ds
1999 2000 2001 2002 2003
1,071,900
1,401,800*
Previous Record
*August 2004
2004
6
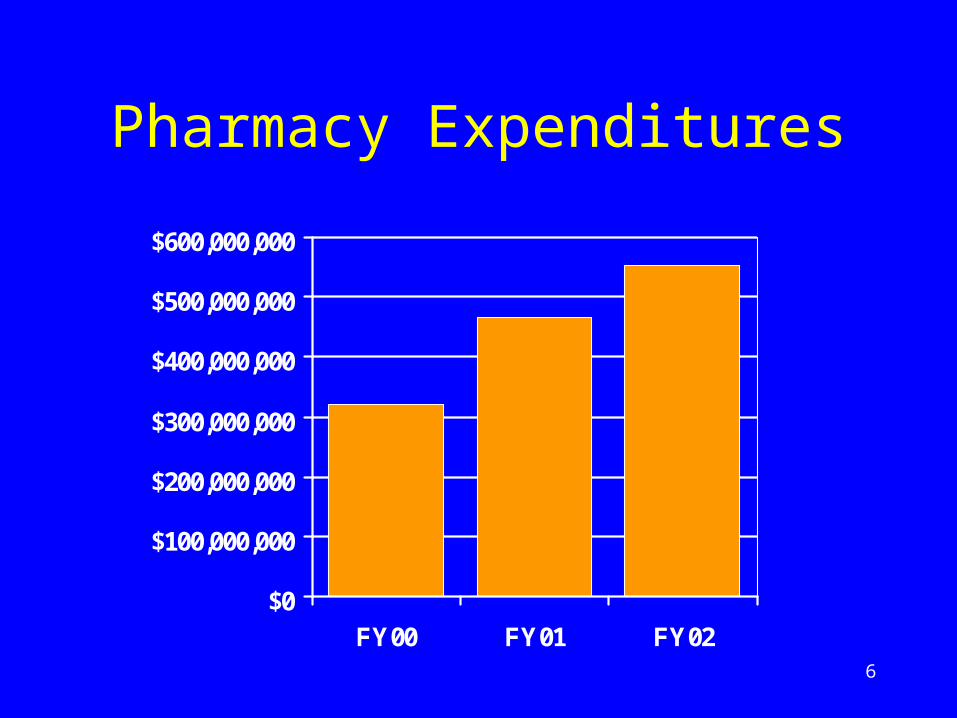
Pharmacy Expenditures
$0
$100,000,000
$200,000,000
$300,000,000
$400,000,000
$500,000,000
$600,000,000
FY00 FY01 FY02

7
Michigan Medicaid Pharmacy Cost Containment
8
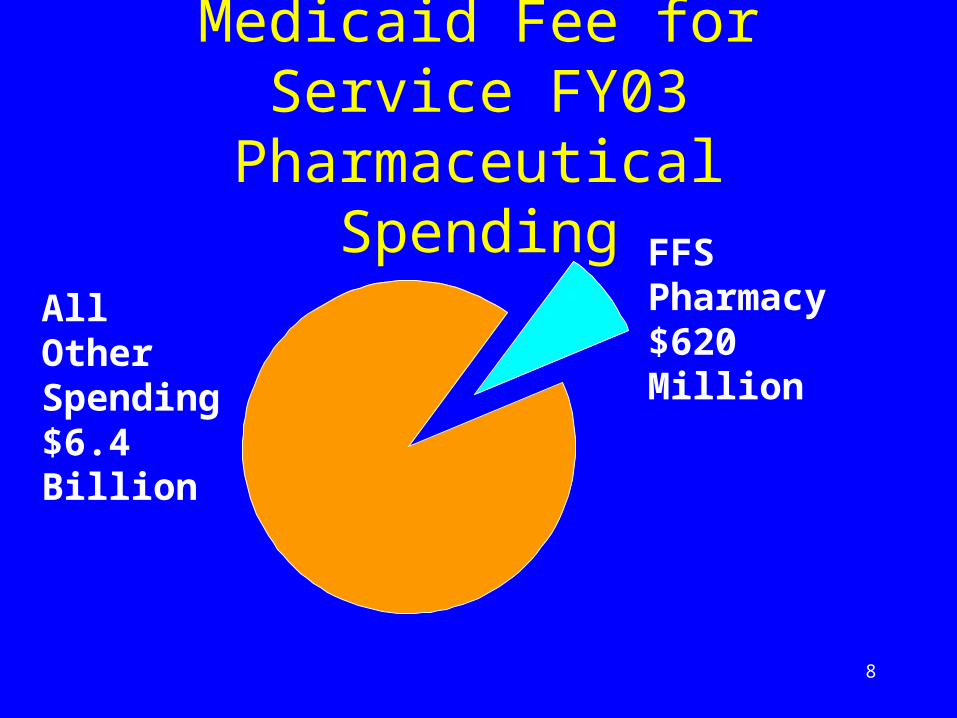
Medicaid Fee for Service FY03 Pharmaceutical Spending
FFS Pharmacy $620 MillionAll Other
Spending $6.4 Billion

9
Medicaid Pharmacy Program Prior to PDL
Pre-PDL
Preferred Drugs Some Generics
Federal Rebate Yes
Supplemental Rebate
No
Pharmacist Payments
AWP, MAC, etc.

10
Medicaid Pharmacy Program After PDL
Pre-PDL Post PDL
Preferred Drugs Some Generics Larger List
Federal Rebate Yes Yes
Supplemental Rebate
No Yes
Pharmacist Payments
AWP, MAC, etc.
Same

11
2002-2003 PDL
• Limited to Michigan• Pharmacy and Therapeutics Committee
identified clinically necessary drugs in 40 drug classes
• Contractor (First Health) negotiated supplemental rebates
• Clinically necessary and drugs with supplemental rebates are not subjected to prior authorization
12
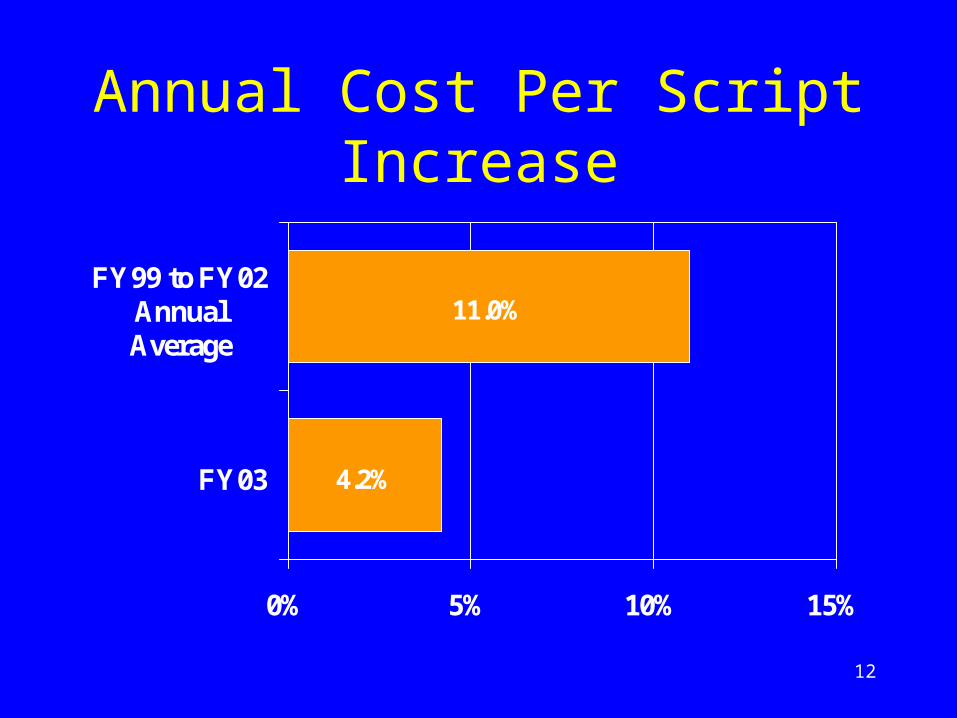
Annual Cost Per Script Increase
4.2%
11.0%
0% 5% 10% 15%
FY03
FY99 to FY02AnnualAverage

13
Estimated Pharmacy Cost Containment Savings
$0$100$200$300$400$500$600$700$800
FY99 FY 00 FY 01 FY 02 FY 03 FY 04
Mill
ions
Actual Trend

14
Preferred Drug List Impact on Beneficiaries

15
Prior Authorization Denials
• 14,300,000 claims
• 106,000 prior authorization requests
• 39,000 approved by technician
• 61,000 approved by pharmacist
• 3,500 approved by state physician
• 2,500 denied by state physician
• 1 denial reversed after administrative appeal

16
Multi-State Preferred Drug List Program

17
Michigan Multi-State Pooling Agreement• Approved by the federal government on
April 22, 2004
• States in the initial pool: Michigan, Vermont, Nevada, Alaska, New Hampshire
• Hawaii and Minnesota state plan amendments approved in September

18
“Matrix” Bid Theory: More Lives, More Exclusivity = Lower Cost
Lives 1 of 1 1 of 2 1 of 3 1 of 4
< 3 m $1.00 $1.10 $1.20 $1.30
3 – 6 m $.90 $1.00 $1.10 $1.20
6 – 9 m $.80 $.90 $1.00 $1.10
> 9 m $.70 $.80 $.90 $1.00
More Exclusivity
M
ore
Liv
es
19
Medicare Prescription Drug, Improvement, and Modernization
Act of 2003
20
Impact on Medicaid
• January 1, 2006 federal government assumes responsibility for processing claims for dual eligibles
• Dual eligibles account for over 2/3 of our fee-for-service pharmacy spending
• “Clawback” requires states to pay federal government for dual eligibles
• Could increase state costs

21
“Clawback” Will Increase Michigan’s Costs
$180$190
$200$210
$220$230
$250
$170$180$190$200$210$220$230$240$250$260
FY03 FY04 FY05 FY06 FY07
Stat
e C
osts
in M
illi
ons
State Operated Federal Clawback

22
Other MMA Impacts
• New state administrative costs
• Reduced state pharmacy bargaining power
• State pharmacy assistance program savings
• State pharmacy assistance coverage expansion opportunities

23
Conclusions
• Preferred drug list program has reduced rate of growth in Medicaid pharmaceutical spending
• Savings will grow as more states join the new multi-state initiative
• No adverse beneficiary impact• Medicare pharmacy reform will have both
positive and negative impact on states