modern management of prolonged rupture of membranes joseph r. biggio jr., m.d. department of...
TRANSCRIPT

Modern Management of Prolonged Rupture of
Membranes
Joseph R. Biggio Jr., M.D.Department of Obstetrics &
GynecologyDivision of Maternal-Fetal Medicine
University of Alabama at Birmingham
PROM
Amniorrhexis prior to onset of active labor regardless of gestational age
Premature Rupture of Membranes

PPROM
Amniorrhexis < 37 weeks’ gestational age
prior to onset of active labor
Preterm Premature Rupture of Membranes

Latency
Interval from Rupture of Membranes
to Onset of Active Labor
Diagnosis History Avoid digital exam Vaginal Pool Nitrazine Paper Ferning Ultrasound Amniocentesis/Dye Study

PROM near Term
Management gestational age dependent
Induction vs. awaiting spontaneous labor
Antibiotic prophylaxis per ACOG/CDC recommendations

Induction vs. Expectant Management
>5,000 women randomized Oxytocin, PGE2 or expectant
management up to 4 days No difference in cesarean section
or neonatal infection Less chorioamnionitis in induction
with oxytocin groupHannah, NEJM, 1996

Epidemiology of Preterm Birth
PPROM
Spontaneous Preterm Delivery
Indicated Preterm Delivery
28 %
46 %26 %
Andrews, 1995
PPROMRisk Factors
Lower/Upper Genital Tract Infection Proteases Prostaglandins
History of PPROM Incompetent Cervix Abruption Polyhydramnios Multiple Gestation Smoking
PPROMComplications
Maternal/Fetal Infection Premature Labor and Delivery Umbilical Cord Prolapse Fetal Hypoxia 2º Cord Compression Increased Rate of Cesarean Section Intrauterine Growth Restriction Abruption Stillbirth
PPROMStandard Management
Confirmation of Diagnosis Verification of Gestational Age R/O Labor/Infection/Fetal
Compromise Avoid Digital Vaginal Examinations In Hospital Observation Bedrest
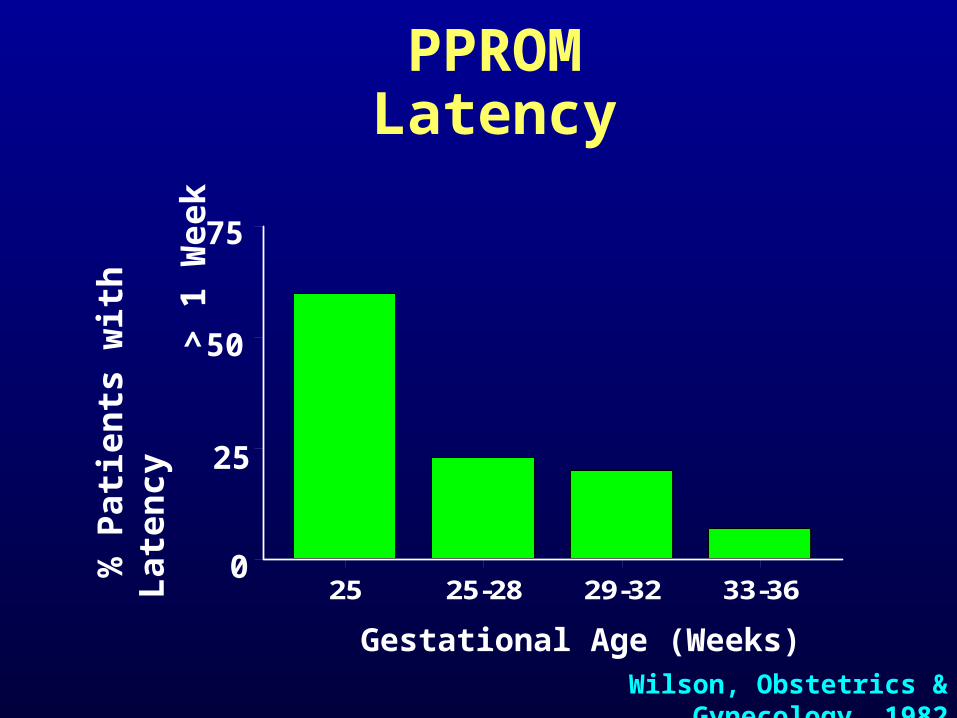
PPROMLatency
Gestational Age (Weeks)
% P
ati
en
ts w
ith
La
ten
cy
>
1 W
ee
k
25
50
75
25 25-28 29-32 33-360
Wilson, Obstetrics & Gynecology, 1982

PPROMVaginal Examination
24-26 26-28 28-30 30-32 32-34 34-35
Gestational Age (Weeks)
20
15
10
5Lat
ency
Day
s No Exam
Exam
Lewis, Obstetrics & Gynecology, 1992
Previable PPROM
< 24 weeks
Poor prognosis for successful outcome
Outcome may be different for spontaneous vs. iatrogenic

Previable PPROMComplications
Uterine Infection
Pulmonary Hypoplasia
Limb Compression Deformities
Intrauterine Growth Restriction

Previable PPROMOutcomes
Study# of
Infants Chorio. Survival
NormalNeurologicalDevelopment
Taylor 60 25% 22% 38%
Major 71 43% 65% 31%
Moretti 124 39% 32% 33%
Bengston 63 46% 51% 16%
Overall 318 39% 41% 30%

PPROMManagement Issues
Timing of Delivery Tocolysis Antibiotics Steroids Amniocentesis Observation vs. Induction Fetal Lung Maturity Testing Fetal Surveillance
Timing of Delivery

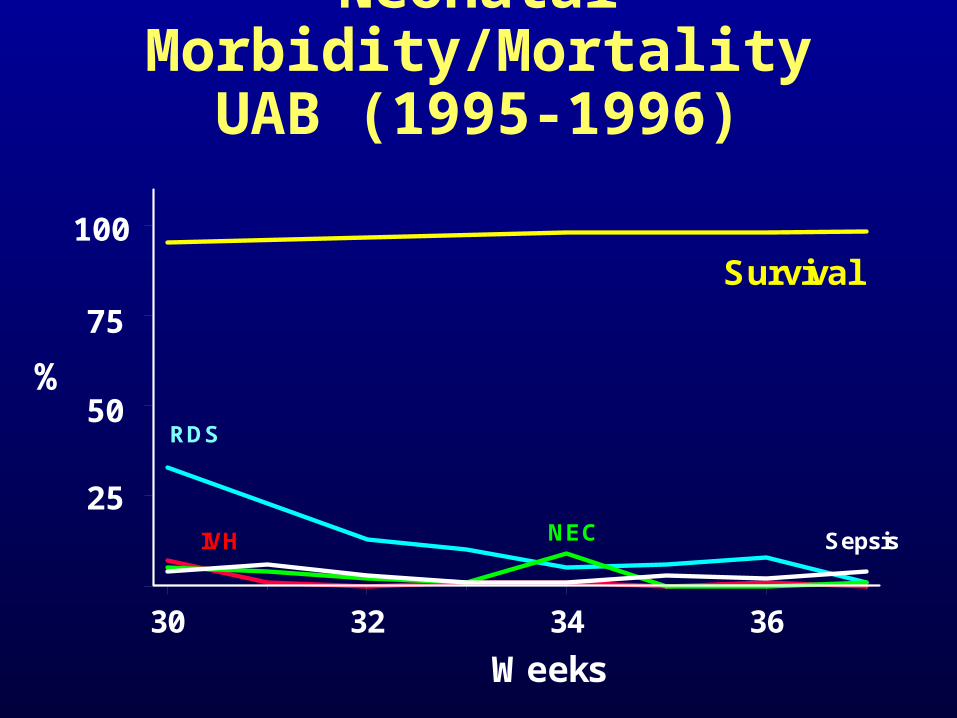
Neonatal Morbidity/MortalityUAB (1995-1996)
%
23 25 27 29 31 33 35 >37
Survival100
25
50
75
Gestational Age (Weeks)
RDS IVH NEC Sepsis
0

RNICU Survival and Morbidity Data (1995-
1996)
23 25 27 29 31 33 35 >37
Survival100
25
50
75
Weeks
RDS
IVH
NEC
Sepsis% N
eon
ates
Tocolysis
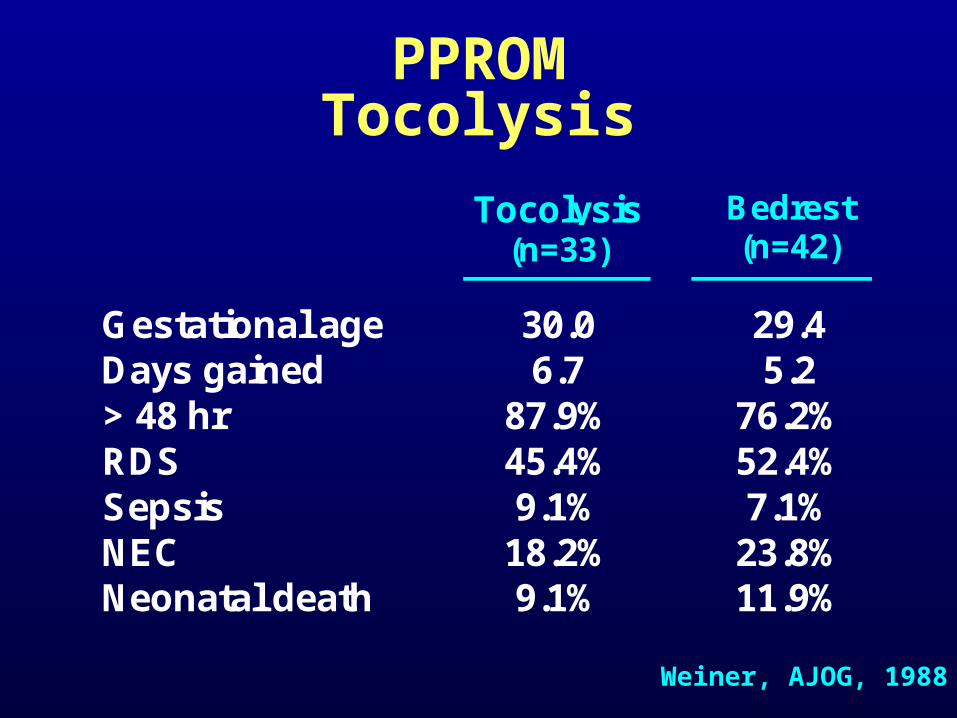
Tocolysis(n=33)
Bedrest(n=42)
Gestational age 30.0 29.4Days gained 6.7 5.2> 48 hr 87.9% 76.2%RDS 45.4% 52.4%Sepsis 9.1% 7.1%NEC 18.2% 23.8%Neonatal death 9.1% 11.9%
PPROMTocolysis
Weiner, AJOG, 1988
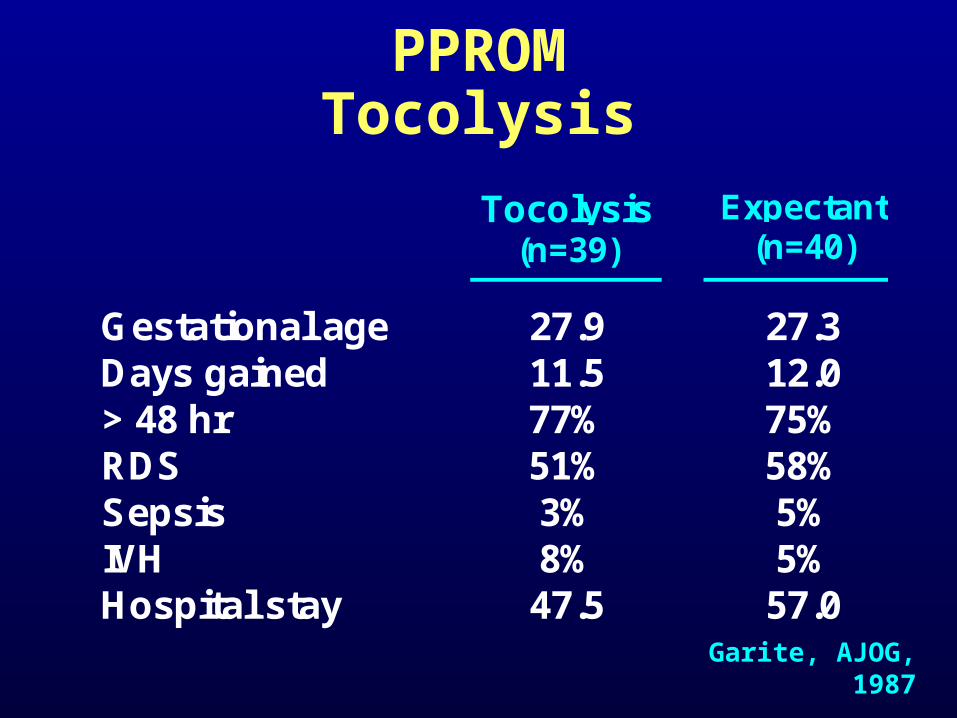
Tocolysis(n=39)
Expectant(n=40)
Gestational age 27.9 27.3Days gained 11.5 12.0> 48 hr 77% 75%RDS 51% 58%Sepsis 3% 5%IVH 8% 5%Hospital stay 47.5 57.0
PPROMTocolysis
Garite, AJOG, 1987

Antibiotics

Preterm LaborChorioamnion Colonization
0 30 weeks
31- 34 weeks
34- 36weeks
37 weeks
25
50
75
% P
atie
nts
Co
lon
ized
SpontaneousPreterm Labor
Indicated
Cassell, 1993
PPROMAntibiotic Therapy
Reduction Maternal/Perinatal
Infection
Prolong Latency Period
Improve Neonatal Outcome
Antibiotic: PPROMNIH-MFM Network Study
PPROM between 24 and 32 weeks IV ampicillin and erythromycin for 48 h Oral amoxicillin/erythromycin for 5 days Identification and Rx of GBS carriers Tocolysis and corticosteroids prohibited
Mercer, JAMA, 1997

Antibiotics(n=299)
Placebo(n=312) RR
RDS 40.5% 48.7% 0.83IVH 6.4% 7.7% 0.82Sepsis <72 hr 5.4% 6.4% 0.83NEC 2.3% 5.8% 0.40Death 6.4% 5.8% 1.10Composite 44.1% 52.9% 0.84
Antibiotic: NIH-MFM Network Study
Neonatal Morbidity
*
*
*

Antibiotic: Latency PeriodNIH-MFM Network StudyDuration of Latency Antibiotics Control
48 hrs 27.3 % 36.6 %
7 days 55.5 % 73.5 %
14 days 75.6 % 87.9 %
21 days 85.7 % 93.0 %
Median 6.1 days 2.9 days
PPROMAntibiotic Therapy
Optimal Antibiotic Regimen
Route/Duration of Administration

Antibiotics & PPROM: Summary
Reduction in maternal infectious morbidity
Reduction in births <48 h and <7 d Reduction in neonatal infectious
morbidity Reduction in neonates requiring
NICU and ventilation >28 d
Kenyon, Cochrane Library, 1999
Antibiotics & PPROM: Summary
No clear reduction in perinatal death
No clear reduction in cerebral abnormalities
Kenyon, Cochrane Library, 1999

Amniocentesis
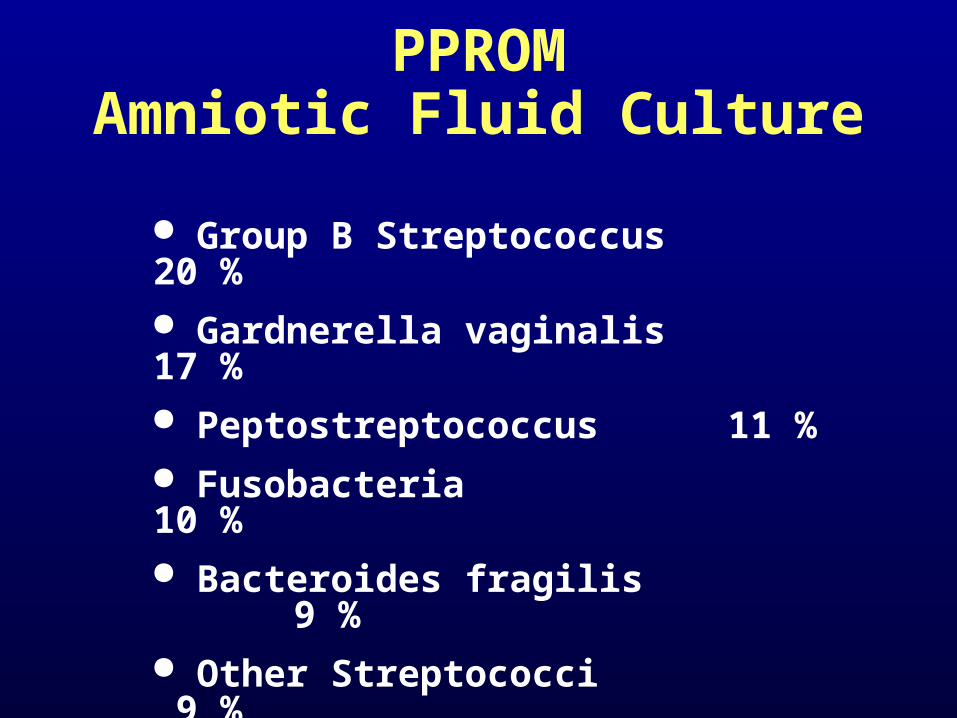
PPROMAmniotic Fluid Culture
Group B Streptococcus 20 % Gardnerella vaginalis 17 % Peptostreptococcus 11 % Fusobacteria 10 % Bacteroides fragilis 9 % Other Streptococci 9 % Bacteroides sp. 5 %

Utility of Amniocentesis
Confirm/Refute diagnosis of chorioamnionitis Glucose <15 mg/dL Culture Gram stain
Lung maturity testing
Corticosteroids

Corticosteroids for FLM
Betamethasone
Dexamethasone

PPROMCorticosteroids
BlockTaeuschPapageorgiouYoungGariteCollaborativeIamsNelsonSimpsonMorales
4317173880
1533822
112121
2624193780
1353546
105124
Author Steroids ControlEffect on
RDSNumber of Patients

Treatment Control OR
RDS 83 / 456 149 / 421 0.44
NeonatalInfection
18 / 200 20 / 188 0.82
PPROMCorticosteroids
Crowley, Ob/Gyn Clinics, 1992
*

Steroids(n=38)
No Steroids(n=39)
Gestation at ROM 29.3 29.7EGA at delivery 31.4 32.0RDS 18% 44%IVH ----- 8%NEC ----- 8%Sepsis 3% 5%Death 3% 3%Hospital days 24.8 29.2
PPROMCorticosteroids +
Antibiotics
*
Lewis, Obstetrics & Gynecology, 1996

1994 NIH Consensus Conference:
Corticosteroids in PPROM
Corticosteroids reduce incidence/severity of RDS, IVH
Benefits in PPROM up to 30-32 weeks
No significant adverse outcomes for corticosteroid use in PPROM
Impact less than with intact membranes

Observation vs. Induction
Neonatal Morbidity/MortalityUAB (1995-1996)
%
30 32 34 36
Survival100
25
50
75
Weeks
RDS
IVH NEC Sepsis

Induction(n=46)
Expectant(n=47)
Cesarean delivery 8.7% 6.4%Chorioamnionitis 10.9% 27.7%Survival 100% 100%Oxygen >24 hr 4.4% 2.1%IVH ----- -----NEC ----- -----Sepsis - W/U 28.3% 59.6%Sepsis - Confirmed 6.8% 4.3%
PPROMObservation vs. Induction
Mercer, AJOG, 1993
*
*

PPROMObservation vs Induction
Delivery(n=61)
Expectant(n=68)
Cesarean delivery 23% 12%Chorioamnionitis 2% 15%Stillbirth 0 1.4%Neonatal Death 5% 0RDS 37% 33%IVH 6% 4.3%NEC 1.6% 1.4%Sepsis 3% 7%
Cox, Obstetrics & Gynecology, 1995

Fetal Lung Maturity Testing

Fetal Lung MaturationBiologic Markers
8
6
4
2
0 0
4
2
6
8
20 24 28 32 36 40Gestational Age (weeks)
L:S
Rat
io
% P
ho
sph
olip
id
L:S
PI
PG
10

Fetal Lung Maturity Evaluation in Vaginal Pool
Specimen
L:S Ratio Not Reliable
TDX:FLM Assay Not Validated
PG Useful

Fetal Surveillance

PPROMFetal Surveillance
Daily Non-Stress Test (NST) Variables Tachycardia Loss of reactivity
Biophysical Profile (BPP) Contraction Stress Test (CST)

Summary
UAB Management of PPROM
•PPROM 34 weeks•Deliver
•Previable PROM•Outpatient observation•Antibiotic prophylaxis•Option of termination <22wk•Admission at viability
•PPROM 23 weeks, <34 weeks•Antibiotic prophylaxis: Amoxicillin 500 tid x 10d, Azithromycin 1gm d1 & d5•1 course Betamethasone if <32weeks•Test for pool PG weekly beginning at 32 weeks•Deliver at 34-35 weeks
UAB Management of PPROM