modernising the serbian health system
TRANSCRIPT

SUPPORTED BY
MODERNISING THE SERBIAN HEALTH SYSTEMTHE NEED FOR A RELIABLE DECISION-MAKING COMPASS
A country case study by The Economist Intelligence Unit
Serbia encapsulates many of the health challenges facing less-developed Balkan countries. Its healthcare system is decentralised and fragmented in places, and levels of out-of-pocket (OOP) payments and corruption are high. In addition, the country lacks a transparent and comprehensive system of assessing the value of its healthcare investments and determining how to pay for them.
All of these issues undermine access to healthcare and contribute to relatively poor health outcomes. In addition, they are likely to be a factor in discussions with the EU over accession as the country aims to become a full member by 2020.
MISMATCH BETWEEN HEALTHCARE SPENDING AND HEALTH OUTCOMES
Compared with eight other Balkan countries (Albania, Bosnia and Hercegovina, Bulgaria, Croatia, Macedonia, Montenegro, Romania and Slovenia), Serbia actually ranks first in the region
© The Economist Intelligence Unit Limited 2016 1
Total expenditure on health as a percentage of GDP, 2014 (% of GDP)
Serbia
Bosnia and Hercegovina
Slovenia
Bulgaria
Croatia
Macedonia
Montenegro
Albania
Romania
Source: WHO Global Health Expenditure Database.
Chart 1
10.4
9.6
9.2
8.4
7.8
6.5
6.4
5.9
5.6

2 © The Economist Intelligence Unit Limited 2016
MODERNISING THE SERBIAN HEALTH SYSTEM THE NEED FOR A RELIABLE DECISION-MAKING COMPASS
in terms of total health expenditure as a share of GDP, according to health-spending data from the World Health Organisation (see chart 1). However, Serbia only ranks fourth in terms of total health spending per capita at purchasing power parity rates (see chart 2).
Yet this spending is not fully translating into positive health outcomes. Life expectancy in Serbia is significantly below the EU average and slightly below the average in the south-east European region as defined by the World Health Organisation (WHO).1
A 2014 study by The Economist Intelligence Unit compared health spending and outcomes in 166 countries.2 The study divided the countries into six tiers (with Tier 1 the best and Tier 6 the worst) according to their overall population health outcomes. Serbia was placed in Tier 3, along with Albania, Bulgaria, Macedonia and Romania, whereas Bosnia and Hercegovina, Croatia and Slovenia were placed in Tier 2. But even more tellingly, among Tier 3 countries Serbia was ranked more highly for healthcare spending than for outcomes, unlike Albania and Macedonia, for example (see chart 3).
This mismatch between healthcare spending and health outcomes is due to several contributing factors, according to healthcare consultant Peter Pazitny, a partner of the Healthcare Consulting and Research Centre in Bratislava, Slovakia. Corruption, old equipment and facilities, inefficiency in hospitals, poor quality of services and waiting lists contribute to poor health outcomes, he points out.
Total health spending per capita, 2014 (Intl$; purchasing power parity)
Slovenia
Croatia
Bulgaria
Serbia
Romania
Bosnia and Hercegovina
Montenegro
Macedonia
Albania
Source: WHO Global Health Expenditure Database.
Chart 2
2,698
1,652
1,399
1,312
1,079
957
888
851
615
1 World Health Organi-sation Regional Office for Europe, European health for all data-base (HFA-DB). Avail-able at: http://data.euro.who.int/hfadb/
2 The Economist Intel-ligence Unit, Health outcomes and cost: A 166-country compari-son, 2014. Available at: http://www.eiu.com/public/than-kyou_download.aspx?activity=download&campaignid=Healthoutcome2014

3© The Economist Intelligence Unit Limited 2016
MODERNISING THE SERBIAN HEALTH SYSTEM THE NEED FOR A RELIABLE DECISION-MAKING COMPASS
“Generally, the Serbian health system is stuck in the past, facing many issues such as the poor quality of hospitals (buildings, furniture, linen etc), long lines for different tests, unavailability of innovative therapies and procedures,” says Jelena Cugurovic, the steering committee member responsible for international co-operation at the CML Association of Serbia, a non-profit organisation that acts on behalf of patients with chronic myeloid leukaemia, and member of the Initiative for Innovative Approach to Improving Access to New Medicines in Serbia. “On the other hand, we have very good and specialised doctors who are educating themselves, but are also forced to leave because of the poor living conditions. Serbia needs systemic solutions and improvements.”
High levels of informal payments and corruption further undermine the system, Mr Pazitny says, with the result that “the main problem is access to care”. Health spending is failing to cover essential care, so that OOP payments make a large contribution to overall spending in Serbia. Given the impact of corruption and other private co-payments, OOP spending accounts for almost 40% of total health expenditure in Serbia (see chart 4). Overall, private health expenditure in Serbia, expressed as a percentage of GDP, has risen in recent years and is the highest in the region (see chart 5).
This is partly due to embedded corruption at all levels of government, with nearly three-quarters of respondents to a 2013 survey in Serbia naming the health system as the most corrupt, after the
EIU Health Outcomes Index, Tier 3 countries, 2014Ranking differences: Outcomes versus spending
Source: The Economist Intelligence Unit, World Health Organisation.
Chart 3
-40
-30
-20
-10
0
10
20
30
40
50
60
70
-40
-30
-20
-10
0
10
20
30
40
50
60
70
Braz
ilLit
huan
iaHu
ngar
ySl
ovak
iaLa
tvia
Bulg
aria
Turk
eyIra
nA
zerb
aija
nSe
rbia
Ven
ezue
laPa
ragu
ayRo
man
iaJo
rdan
Libya
Surin
ame
Beliz
eA
lger
iaG
eorg
iaM
aced
onia
Jam
aica
Dom
inic
an R
epub
lic
Alb
ania
Nic
arag
uaTh
aila
ndC
abo
Ver
de
Vie
tnam
Sri L
anka
Rank higher for outcomesthan for spending
Rank higher for spendingthan for outcomes

4 © The Economist Intelligence Unit Limited 2016
MODERNISING THE SERBIAN HEALTH SYSTEM THE NEED FOR A RELIABLE DECISION-MAKING COMPASS
Out-of-pocket expenditure as a percentage of total health expenditure, 2014 (%)
Albania
Bulgaria
Montenegro
Macedonia
Serbia
Bosnia and Hercegovina
Romania
Slovenia
Croatia
Source: WHO Global Health Expenditure Database.
Chart 4
49.9
44.2
42.8
36.7
36.6
27.9
18.9
12.1
11.2
Source: World Bank.
Chart 5
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
4.5 2014201320122011
SloveniaSerbiaRomaniaMonte-negro
MacedoniaCroatiaBulgariaBosniaand
Hercegovina
Albania
Private health expenditure(% of GDP)

5© The Economist Intelligence Unit Limited 2016
MODERNISING THE SERBIAN HEALTH SYSTEM THE NEED FOR A RELIABLE DECISION-MAKING COMPASS
country’s political parties.3 In most cases, corruption takes the form of “informal” co-payments, including bribes. According to recent studies, Mr Pazitny says, the average bribe in the healthcare sector is €205 (with average monthly wages of around €370), and approximately half of all bribes are in cash.
A 2015 report on corruption in Serbia’s healthcare sector suggested that the most important way to combat the problem would involve reforming the health insurance system, specifically the introduction of a more precise compulsory package covering a smaller number of clearly defined services that can be topped up with various levels of voluntary insurance; at the same time direct payments for services rendered would be legalised and formalised in order to avoid concealment and secrecy and promote transparency in cash flows.4
CHALLENGES IN PROVIDING ACCESS TO HEALTHCARE
Serbia faces a number of challenges in modernising its health system, including budgetary constraints and problems accessing innovative healthcare solutions, principally owing to the absence of a sustainable, comprehensive and transparent way to evaluate and procure new health technology.
At the crux of the problems facing Serbia is finding ways to meet commitments to healthcare access for the population with the resources the government has at its disposal.
Under the existing system, employee- and employer-financed social health insurance (SHI) covers most general medical services, with uninsured groups covered by state budget funds; there is also a voluntary health insurance (VHI) system in Serbia. Co-payments officially exist for certain medicines and are informally required to access many others, making many drugs unaffordable and out of reach for large segments of the population.
Pharmaceutical spending accounted for 18% of expenditure by the National Health Insurance Fund (RFZO) in 2013, with generics making up the majority of dispensed drugs, 70% of which were locally manufactured.5 The RFZO decides on reimbursement rates, which range from 10% to 100% in Serbia, with hospital drugs and very expensive drugs for certain conditions fully reimbursed in theory.
Until 2011 the RFZO experienced difficulties collecting contributions from employers, with the result that the funds transferred from the state budget were insufficient to cover commitments, leading to delayed payments to pharmacies, manufacturers and providers, and ultimately a shortage of necessary drugs. The government made the decision to take on all of the RFZO’s debt as part of
3 Health Policy In-stitute, Serbia: Brief health system re-view, January 28th 2014. Available at: http://www.hpi.sk/en/2014/01/serbia-brief-health-system-review/
4 Southeast Europe Leadership for Devel-opment and Integrity (SELDI), Assessment of Corruption in the Health Care Sector in Serbia, background document 4, Febru-ary 2015, pp. 21-22. Available at: http://seldi.net/publica-tions/publications/seldi-background-document-4-assess-ment-of-corruption-in-the-healthcare-sector-in-serbia/
5 Godman B and Gus-tafsson LL, Potential changes to the Phar-maceutical Policy in Serbia, Karolinska Insti-tutet, Stockholm, Swe-den, 2014. Available at: http://rfzo.rs/down-load/farmakopolitika/Dokument%20o%20farmakopolitici%20-%20engleska%20ver-zija%202.pdf

6 © The Economist Intelligence Unit Limited 2016
MODERNISING THE SERBIAN HEALTH SYSTEM THE NEED FOR A RELIABLE DECISION-MAKING COMPASS
public debt, giving it a clean slate, according to Bojan Trkulja, managing director at the Serbian Association of the Manufacturers of Innovative Drugs (INOVIA). Legal changes approved at the same time meant that companies could not pay salaries unless they had also paid all health and other contributions at the same time. As a result, since 2012 the health fund has been making all of its payments within 100 days.
However, the regular amounts that the fund pays to pharmacies and hospitals are not enough to cover actual costs, Dr Trkulja notes. Consequently, some pharmacies and hospitals are again delaying payments to distributors and pharmaceutical companies, with the result that some distributers have stopped supplying them, increasing the potential for shortages. A report by the European Commission in November 2015 concluded that “the poor financial situation of the public health fund puts the sustainability of the [healthcare] sector in question”.6
The deficits are evident in some of the most vital but costly medicines, according to Dr Trkulja. For example, out of more than 2,000 who are potentially eligible, only 200-300 new patients are getting the prescribed treatment for hepatitis C each year, he adds.
“In oncology, it’s even worse,” Dr Trkulja says, referring to the shortage of funds collected by the RFZO that has limited the resources available for high-cost medicines “because not only is the health fund decreasing the number of reimbursed indications, but even those patients are not getting it because the fund has only enough medicine to treat [a small number of] patients and has to agree on who they will be.”
DECISION-MAKING WITHOUT A RELIABLE COMPASS
Serbia lacks a transparent and comprehensive system of assessing the value of healthcare investments and determining how to pay for them. The development of a health technology assessment (HTA) infrastructure in Serbia lags well behind that in neighbouring countries such as Croatia and Slovenia, which have more advanced—albeit not yet fully functioning—systems.
There is no official HTA agency in Serbia, although the RFZO carries out some related activities, including pharmacoeconomic assessment and budget-impact analysis in support of reimbursement decisions. The Medicines and Medical Devices Agency of Serbia (ALIMS) evaluates the quality, safety and efficiency of pharmaceuticals based on technical dossiers. The Ministry of Health also has an HTA Committee, which has significant responsibilities but little technical support.7 Serbia, unlike Croatia and Slovenia, does not participate in the European Network for Health Technology Assessment (EUnetHTA).
7 Djukic, P, “Develop-ing HTA frameworks in emerging markets: the road ahead: The case of Serbia”, Eurohealth, Vol. 16, No. 4, 2010.
6 European Com-mission, Serbia 2015 Report, November 10th 2015. Available at: http://ec.europa.eu/enlargement/pdf/key_docu-ments/2015/20151110_report_serbia.pdf

7© The Economist Intelligence Unit Limited 2016
MODERNISING THE SERBIAN HEALTH SYSTEM THE NEED FOR A RELIABLE DECISION-MAKING COMPASS
Pricing and reimbursement negotiations in Serbia currently do not take into account any formal review of HTA submissions and have only limited patient data, according to David Danko, research leader at Corvinus University Institute of Management in Budapest and managing partner at consulting firm Ideas & Solutions. At the Fifth International Conference on Challenges for Efficient Healthcare in Central and Eastern Europe, held in Belgrade in October 2015, Dr Danko said that improved use of both strands could help negotiators to take into account the added clinical benefits of the new technology, its alignment with national health policy and social and ethical considerations, as well as aiding the formation of a budget-impact analysis.8
Since 2006 the Serbian Ministry of Trade, Tourism and Telecommunications has set maximum prices based on the lowest prices in three reference countries, Slovenia, Croatia and Italy. In March 2016 the government began negotiations on creating a framework for the introduction of managed entry agreements (MEAs), according to Dr Trkulja. However, in the absence of a transparent HTA process, launching the first such agreements is likely to be a more complicated process.
MEAs are risk-sharing agreements between payers and drug manufacturers that are traditionally used to identify issues material to a reimbursement decision; without a consistent system for determining coverage in place, such agreements will be hard to reach. The agreements are designed to address uncertainty about the performance of new technologies, manage their adoption to maximise effective use, or limit their budget impact through the sharing of risk between producers and purchasers. Consequently, only the involvement of all stakeholders, especially clinicians and patients, is likely to lead to a sustainable system.
Overall, the process for deciding the reimbursement and pricing of pharmaceuticals and medical devices remains patchy, and even the observance of existing rules, those interviewed for this study say, is contributing to difficulties in accessing healthcare. Although an April 2014 rulebook determined that all new drugs—or more precisely, all international nonproprietary names (INNs) submitted for reimbursement—should undergo a cost-effectiveness and budget-impact analysis and all other medicines should be subject to a budget analysis9, it is unclear whether the government is adhering to these guidelines in most cases, says Tanja Novakovic, president of the pharmacoeconomics section of the Pharmaceutical Association of Serbia.
Moreover, Dr Trkulja notes that the exchange rate used by the government in pricing negotiations is often opaque, further undermining transparency and making it unclear how decisions are made.
The lack of a consistent system for HTA is one of the main reasons why access to innovative therapies appears to be significantly lower in Serbia than in other countries in the region. Between
8 Draft Meeting Report: Fifth International Conference on Challenges for Efficient Healthcare in Central and Eastern Europe, Belgrade, October 2015.
9 RFZO, Rulebook covering the criteria, methods and conditions for listing medicines. Available at: http://www.rfzo.rs/download/pravilnici/lekovi/Pravilnik_uslovi_ListaLekova-10062015.pdf
8 © The Economist Intelligence Unit Limited 2016
MODERNISING THE SERBIAN HEALTH SYSTEM THE NEED FOR A RELIABLE DECISION-MAKING COMPASS
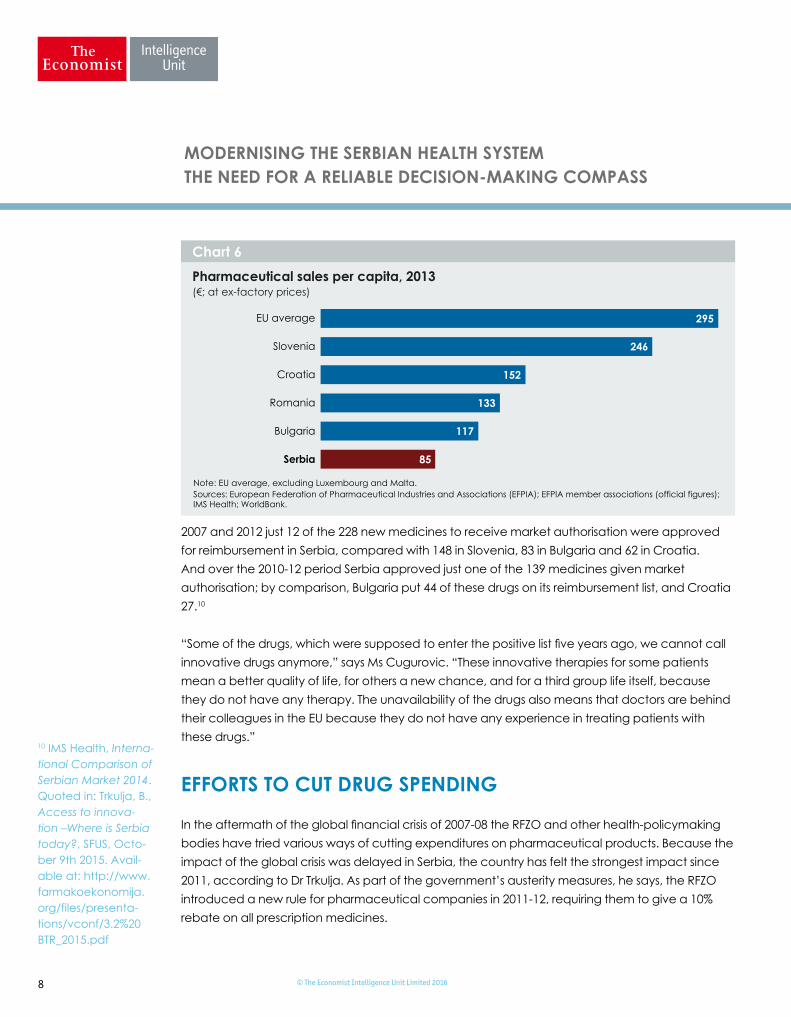
2007 and 2012 just 12 of the 228 new medicines to receive market authorisation were approved for reimbursement in Serbia, compared with 148 in Slovenia, 83 in Bulgaria and 62 in Croatia. And over the 2010-12 period Serbia approved just one of the 139 medicines given market authorisation; by comparison, Bulgaria put 44 of these drugs on its reimbursement list, and Croatia 27.10
“Some of the drugs, which were supposed to enter the positive list five years ago, we cannot call innovative drugs anymore,” says Ms Cugurovic. “These innovative therapies for some patients mean a better quality of life, for others a new chance, and for a third group life itself, because they do not have any therapy. The unavailability of the drugs also means that doctors are behind their colleagues in the EU because they do not have any experience in treating patients with these drugs.”
EFFORTS TO CUT DRUG SPENDING
In the aftermath of the global financial crisis of 2007-08 the RFZO and other health-policymaking bodies have tried various ways of cutting expenditures on pharmaceutical products. Because the impact of the global crisis was delayed in Serbia, the country has felt the strongest impact since 2011, according to Dr Trkulja. As part of the government’s austerity measures, he says, the RFZO introduced a new rule for pharmaceutical companies in 2011-12, requiring them to give a 10% rebate on all prescription medicines.
10 IMS Health, Interna-tional Comparison of Serbian Market 2014. Quoted in: Trkulja, B., Access to innova-tion –Where is Serbia today?, SFUS, Octo-ber 9th 2015. Avail-able at: http://www.farmakoekonomija.org/files/presenta-tions/vconf/3.2%20BTR_2015.pdf
Pharmaceutical sales per capita, 2013 (€; at ex-factory prices)
EU average
Slovenia
Croatia
Romania
Bulgaria
Serbia
Sources: European Federation of Pharmaceutical Industries and Associations (EFPIA); EFPIA member associations (official figures);IMS Health; WorldBank.
Note: EU average, excluding Luxembourg and Malta.
Chart 6
295
246
152
133
117
85

9© The Economist Intelligence Unit Limited 2016
MODERNISING THE SERBIAN HEALTH SYSTEM THE NEED FOR A RELIABLE DECISION-MAKING COMPASS
In addition, a particularly controversial new regulation, Article 29, was introduced in April 2014 with the aim of reducing the price of off-patent originators by up to 49% compared with current list prices, depending on the number of generic versions of them in the market.11 RFZO sources were quoted in local newspapers as saying that the new ordinance was meant to address the fact that Serbia pays as much as 30% more for some medicines than west European countries; the RZFO estimated at the time that the change could save more than RSD5bn (US$46m) and lead to lower co-payments for insured Serbians.12
“The official reason given to industry for the introduction of such a measure was that the savings would be used for the introduction of new innovative medicines on the reimbursement list,” Dr Trkulja says. “However, not only did that not happen, but it was clear looking at the RFZO’s 2015 financial plan [in which the drug budget was reduced by RSD5bn compared with 2014] that they used it to decrease the drug budget.”
IMPETUS FOR IMPROVEMENT?
There have been limited efforts to bring in reforms to the Serbian healthcare system that could help to improve the efficiency of the system, although Serbia still remains a long way off from a transition to value-based healthcare—a new healthcare paradigm that looks at health outcomes of treatment relative to cost and is gaining traction in some parts of western Europe.13 For example, the government has introduced a capitation system in primary care and has launched payment mechanisms based on diagnosis-related groups (DRGs) for hospital care.
The World Bank’s Second Serbia Health Project, approved in February 2014, aims to support quality, efficiency and transparency of health-system financing for both primary and hospital care. The programme includes strengthening HTA and quality improvement systems for healthcare delivery as well as the management of “selected priority non-communicable diseases”.14 The government is also piloting a centralised system for the procurement of drugs, although Dr Trkulja notes that because bidding takes place only once a year, this leads to delays in providing access to medicines that have already been approved for reimbursement.
Meanwhile, Serbian healthcare providers are gradually moving towards a greater focus on monitoring health outcomes. Ms Novakovic highlights the importance of patient data and notes that Serbia currently has patient registries for melanoma, inflammatory bowel disease and rheumatoid arthritis.15 She adds, however, that collecting and using these data requires close co-operation between all key stakeholder groups, including the RFZO.
11 “Serbian pharma industry fears effects of new law on drug pricing”, IHS Life Sci-ences Perspective, Same-Day Analysis, April 29th 2014.
12 Ibid.
13 The Economist Intel-ligence Unit, Value-based healthcare in Europe: Laying the foundation, 2016. Available at: http://www.eiuperspec-tives.economist.com/sites/default/files/Valuebasedhealthca-reEurope.pdf
14 The World Bank, “Second Serbia Health Project”, Overview. Available at: http://www.worldbank.org/projects/P129539/second-serbia-health-project?lang= en&tab=overview
15 Draft Meeting Re-port: Fifth International Conference on Chal-lenges for Efficient Healthcare in Central and Eastern Europe, Belgrade, October 2015.

10 © The Economist Intelligence Unit Limited 2016
MODERNISING THE SERBIAN HEALTH SYSTEM THE NEED FOR A RELIABLE DECISION-MAKING COMPASS
As Serbia continues its negotiations with the EU over accession by 2020, modernising the country’s healthcare system will become increasingly important. Healthcare will be covered under Chapter 28 (consumer and health protection) in the accession negotiations. Serbia recently joined the Third EU Health Programme 2014-20, highlighting the country’s commitment to improving its healthcare system in line with EU standards.16 However, the European Commission continues to express major concerns, for example about the health system’s vulnerability to corruption, shortages of medical and administrative staff in primary healthcare, and the particularly weak access to healthcare for specific groups, such as prisoners and the Roma population.17
Ms Cugurovic notes that the government has announced a limited number of patient-access agreements with pharmaceutical companies, but adds that “Serbia needs a systemic solution for the approval of innovative therapies that will solve the issue now and in the future, and be in line with the EU”.
Systemic weaknesses in Serbia’s healthcare system, including corruption and the lack of a comprehensive system for assessing both new and existing healthcare solutions, are undermining access to both basic and cutting-edge health technology and contributing to poor health outcomes. As Serbia continues its preparations for EU membership, its ability to implement much-needed reforms of its health system will be in the spotlight.
Efforts to contact official government institutions in Serbia—including the health ministry and the RFZO—for comments on the subjects covered in this case study were unsuccessful.
16 “Serbia joins European health programme”, The Delegation of the European Union to the Republic of Serbia, March 16th 2016. Available at: http://europa.rs/eng/serbia-joins-european-health-programme/
17 European Com-mission, Serbia 2015 Report.