módulo tórax - criandoelo.com.br · tosse e dor pleurítica galactomanana 0,8 lma refratária...
TRANSCRIPT

Micoses invasivas pulmonares Porto Alegre, 22/junho/2018
Alessandro C. Pasqualotto, MD PhD FECMM
Santa Casa de Porto Alegre Universidade Federal de Ciências da Saúde de Porto Alegre
Módulo Tórax




All hail the king

All hail the king


Sinal do halo
Herbrecht, et al. N Engl J Med 2002; 347: 408-15

• Aspergilose angioinvasiva • Infarto • Necrose de coagulação
Greene RE, et al. ECCMID 2003
Sinal do halo

Hemorragia alveolar
Greene RE, et al. ECCMID 2003
• Aspergilose angioinvasiva • Infarto • Necrose de coagulação
Sinal do halo
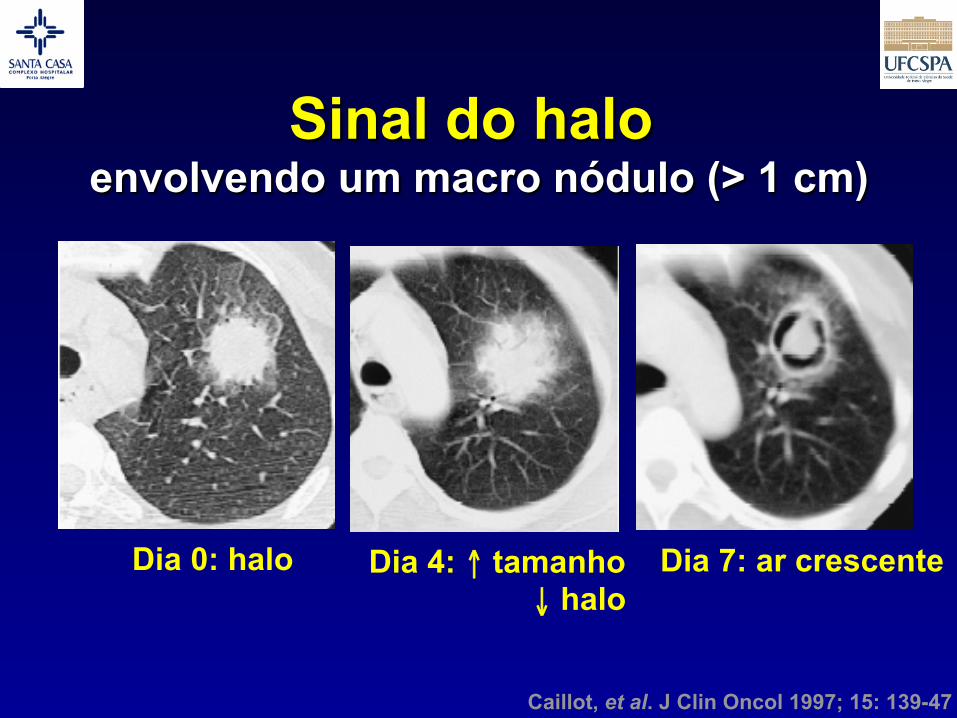
Dia 0: halo Dia 4: ↑ tamanho ↓ halo
Dia 7: ar crescente
Caillot, et al. J Clin Oncol 1997; 15: 139-47
Sinal do halo envolvendo um macro nódulo (> 1 cm)

Greene RE, et al. Clin Infect Dis 2007; 44: 373-9
• Melhor sobrevida (12 semanas) – 52% vs. 29% (p<0,001)
Diagnóstico precoce!
Sinal do halo

O que é galactomanana?
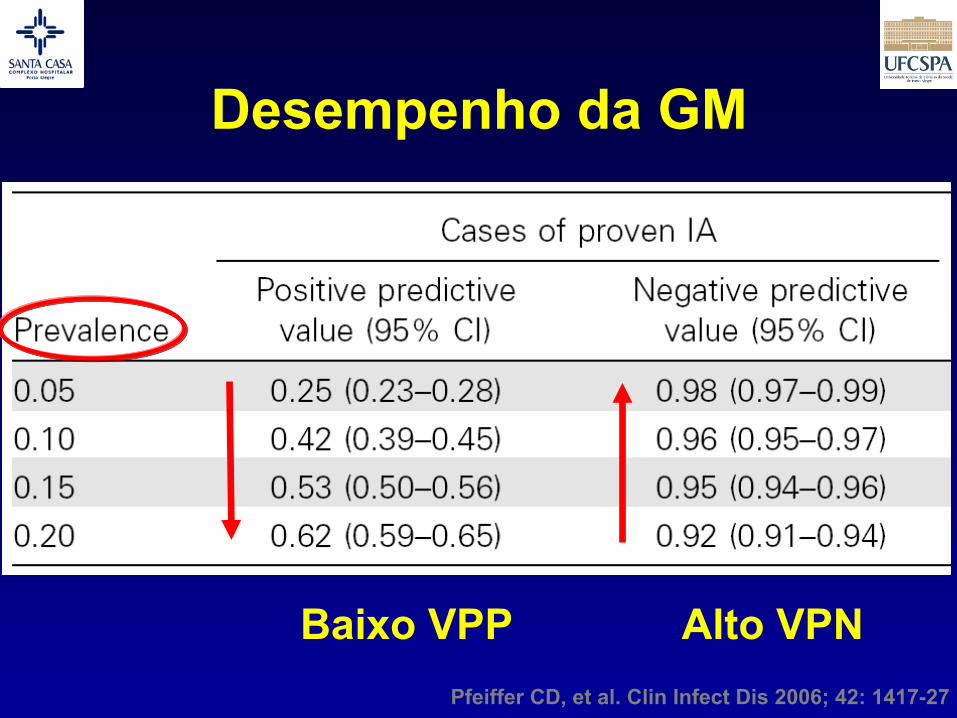
Pfeiffer CD, et al. Clin Infect Dis 2006; 42: 1417-27
Desempenho da GM
Baixo VPP Alto VPN

LMA refratária >50 dias de neutropenia
Febre persistente Galactomanana 7,8
Maertens J. ICAAC 2006

Maertens J. ICAAC 2006
Síndrome mielodisplásica Esteroides/DECH grau III
Tosse e dor pleurítica Galactomanana 0,8
LMA refratária >50 dias de neutropenia
Febre persistente Galactomanana 7,8

Dagenais TRT, Keller NP. Clin Microbiol Rev 2009; 447-65
Patogênese da AI

GM no LBA Positive likelihood ratio
D'Haese J, et al. J Clin Microbiol 2012; 50: 1258-63

GM no LBA Negative likelihood ratio
D'Haese J, et al. J Clin Microbiol 2012; 50: 1258-63


Kradin R. In: Aspergillosis: from diagnosis to prevention. Pasqualotto AC, ed. Springer, 2010
Diagnóstico de certeza

Diferentes fungos filamentosos
Scedosporiose
Fusariose
Aspergilose
Mucormicose Kradin R. In: Aspergillosis: from diagnosis to prevention. Pasqualotto AC, ed. Springer, 2010

Figure 1. Images from a 49-year-old woman who presented with febrile neutropenia during treatment for recurrent acute myelogenous leukemia.A, Contrast-enhanced chest CT image at presentation, showing the reversed halo sign, a solid ring (arrows) with central ground-glass opacities. B,Contrast-enhanced chest CT image, which was obtained 4 weeks later because of some chest tightness and persistent fever, showing a better formedperipheral soft tissue ring with interval development of lingular consolidation. The arrow points to an air bubble that separates the infarcted reversedhalo from the still viable consolidated lung peripheral to it. C, The patient developed a pseudoaneurysm (arrow) and underwent lobectomy. D, Lobectomyspecimen, 7 weeks after presentation, showing that the reversed halo sign (arrow) was attributable to infarcted lung. The tissue surrounding thereversed halo sign (*) is lingular consolidation. E, Photomicrograph of the lobectomy specimen showing that the reversed halo sign was attributableto infarcted lung, with a greater amount of hemorrhage at the periphery (P) than in the center (C) (hematoxylin-eosin stain, !10). F, Photomicrographshowing fungal hyphae with 90! branching, consistent with Zygomycetes hyphae (arrows). (GMS staining, !40). A color version of the figure isavailable in the online edition of Clinical Infectious Diseases.
at IFPI - Instituto Federal do PiauÃ- on A
ugust 4, 2014http://cid.oxfordjournals.org/
Dow
nloaded from
Wahba H, et al. Clin Infect Dis 2008; 46: 1733-7
Sinal do halo reverso
• Lembrar de Mucor
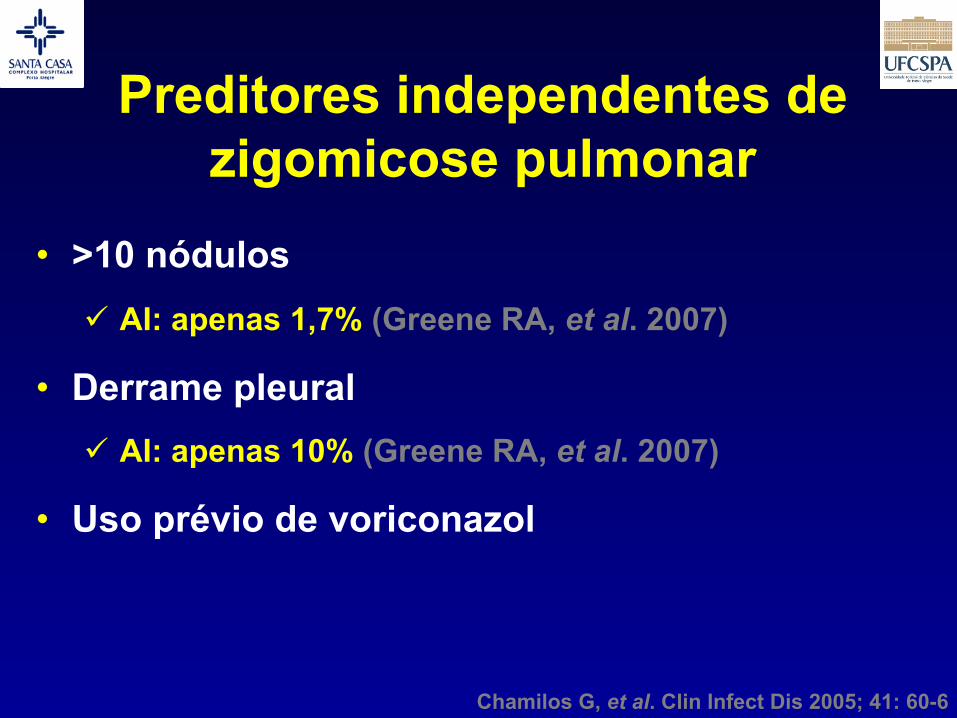
Chamilos G, et al. Clin Infect Dis 2005; 41: 60-6
• >10 nódulos ü AI: apenas 1,7% (Greene RA, et al. 2007)
• Derrame pleural ü AI: apenas 10% (Greene RA, et al. 2007)
• Uso prévio de voriconazol
Preditores independentes de zigomicose pulmonar

Denning DW, et al. Clin Infect Dis 2011; 52: 1123-9
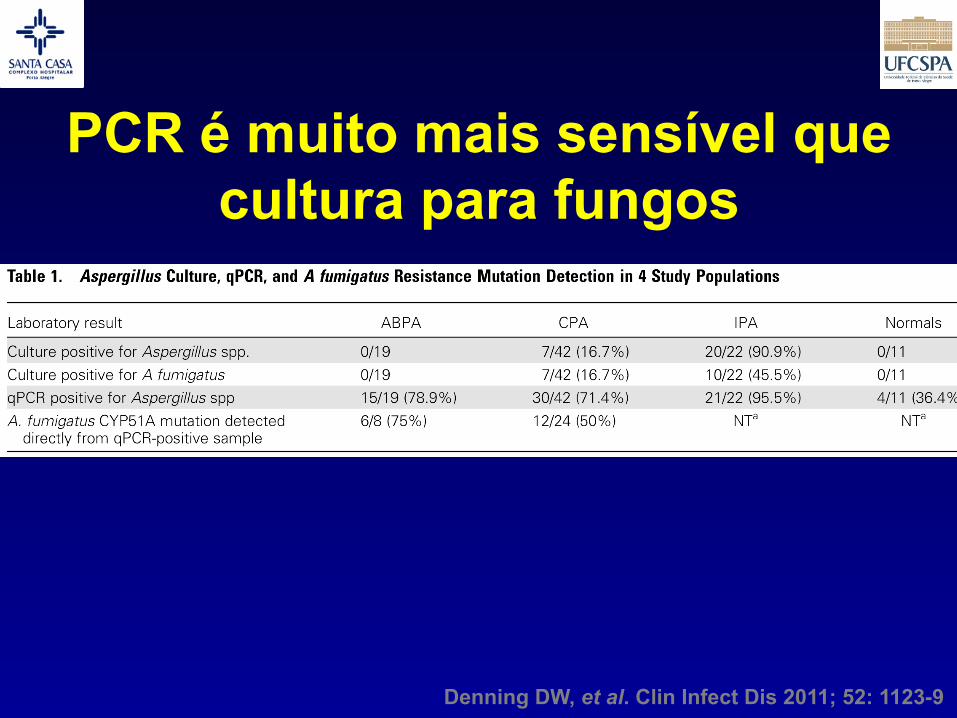
PCR é muito mais sensível que cultura para fungos
Denning DW, et al. Clin Infect Dis 2011; 52: 1123-9
Nem toda a aspergilose é invasiva

Aspergilose pulmonar cavitária crônica (CCPA)
• Mulher de 47 anos
• TB pulmonar no passado
• Cavidade no LSE

6 anos depois
• Piora clínica
• Tosse produtiva
• Dispnéia
• Perda de peso

• Precipitinas positivas contra Aspergillus
• Escarro e LBA:
A. fumigatus
6 anos depois

3 anos depois • Deteriorou
• Múltiplas cavidades
• Derrame pleural
• Hemoptise
• Dispnéia, tosse
• Perda de peso

Tratada até 2007

BRIEF REPORT • CID 2007:45 (1 October) • e101
B R I E F R E P O R T
The Value of Computed Tomography–Guided Percutaneous Lung Biopsy forDiagnosis of Invasive Fungal Infectionin Immunocompromised Patients
Cornelia Lass-Florl,1 Gudrun Resch,2 David Nachbaur,2 Astrid Mayr,1
Gunther Gastl,2 Jutta Auberger,2 Ralf Bialek,4 and Martin C. Freund3
1Department of Hygiene, Microbiology and Social Medicine, University ofInnsbruck, 2Clinical Division of Haematology and Oncology, Innsbruck MedicalUniversity, and 3Department of Radiology, University Hospital Innsbruck,Innsbruck, Austria; and 4Clinical Microbiology, Catholic Children’s HospitalWilhelmstift, Hamburg, Germany
We assessed Calcofluor white staining, Aspergillus polymer-ase chain reaction, and a galactomannan enzyme immuno-assay for diagnosis of fungal infection with use of computedtomography–guided percutaneous lung biopsy specimens ob-tained from 61 patients. The sensitivity and specificity ofcomputerized tomography, Aspergillus polymerase chain re-action, and galactomannan enzyme immunoassay were 100%and 50%, 100% and 86%, and 88% and 94%, respectively.
Invasive aspergillosis (IA) is a major cause of morbidity andmortality among immunosuppressed patients. Case-fatalityrates range from 30% to 80% among neutropenic patients, anddeath results, at least in part, from difficulties in obtaining areliable diagnosis in the early stage of disease [1]. No methodhas proven to be sufficiently sensitive and specific to allowadequate diagnosis.
The use of CT allows diagnosis early in the course of pul-monary IA and helps to improve the overall survival rate amongfebrile, neutropenic patients [2]. Previous studies reported thatthe CT finding of a halo sign is indicative of pulmonary as-pergillosis in neutropenic patients [3]. Thus far, it is impossibleto distinguish Aspergillus species from other fungi on the basisof clinical signs [4]. However, identification of the causativeorganisms is highly warranted in the clinical context to deter-
Received 28 February 2007; accepted 23 May 2007; electronically published 20 August2007.
Reprints or correspondence: Dr. Cornelia Lass-Florl, Dept. of Hygiene, Microbiology andSocial Medicine, Section of Hygiene and Medical Microbiology, Innsbruck Medical University,Fritz Pregl Str. 3/3, A-6020 Innsbruck, Tirol, Austria ([email protected]).
Clinical Infectious Diseases 2007; 45:e101–4! 2007 by the Infectious Diseases Society of America. All rights reserved.1058-4838/2007/4507-00E4$15.00DOI: 10.1086/521245
mine adequate therapy. Zygomycetes have in vivo and in vitroresistance to the newer antifungals, such as voriconazole andcaspofungin [5]. The number of infections due to zygomyceteshave increased in our hospital and in other health care centers,indicating the need for a powerful means of diagnosis [6].
We evaluated the utility of Calcofluor white staining (CFWS),galactomannan EIA (GM EIA), and Aspergillus PCR of CT-guided lung biopsy specimens for diagnosis of rapidly invasivefungal infection in immunosuppressed patients.
Methods. A prospective study conducted from October 2003through September 2006 evaluated 61 patients who had he-matologic malignancies (46 patients) or who had undergonesolid-organ transplantation (15 patients) and who had CT find-ings highly suggestive of an invasive fungal infection. The spec-imens were obtained by CT-guided percutaneous biopsy andwere investigated for the presence of fungal elements. All CT-guided percutaneous biopsies were performed with an auto-mated biopsy gun that contained a detachable coaxial cuttingneedle system, as described by Lucidarme et al. [7]. In ourstudy, an outer coaxial needle with a 17-gauge diameter andan inner biopsy needle with an 18-gauge diameter were chosen.Interventions were performed only for patients with plateletcounts of 50,000 platelets/mL and with prothrombin and partialthromboplastin times within the normal limits. Lesions thathad a diameter 11 cm and that were most easily assessable werechosen for biopsy.
Biopsy specimens were transferred to 2 mL of NaCl, minced,and homogenized aseptically. Samples were then vortexed,stored at room temperature for 30 min, and centrifuged. Su-pernatants and homogenized tissues were examined for thepresence of fungi by application of the Fungi-Fluor CFWS so-lution (Polysciences), by Aspergillus PCR [8], and by GM EIA(Platelia Aspergillus ELISA; BioRad); a 0.5 cutoff optical densitywas used. In parallel, all samples were cultured in brain heartinfusion broth at 37"C for 14 days. Selected samples thatshowed unseptate hyphae by CFWS and that yielded negativeresults of GM EIA and Aspergillus PCR were evaluated by aPCR specific for mucormycoses [9]. For controls, we examined12 CT-guided lung biopsy specimens that had been obtainedpreviously to rule out cancer or bacterial infection.
CTs were assessed for the presence and distribution of nod-ules, opacities (including ground glass opacities), halo signs,crescent signs, and cavitations. Proven pulmonary IA was de-fined as positive tissue biopsy specimen with typical septate,acute-branching hyphae, with or without an Aspergillus-positiveculture. Non-Aspergillus fungal infection was defined as a pos-
by guest on May 16, 2013
http://cid.oxfordjournals.org/D
ownloaded from
Lass-Florl C, et al. Clin Infect Dis 2007; 45: e101-4
TC + GM + PCR + microscopia com calco flúor + cultural

322 Unis G, Severo LC
J Bras Pneumol. 2005; 31(4):318-24
Tratamento e evolução: o paciente recebeucetoconazol (200 mg/dia) e teve alta hospitalar,não retornando ao serviço.
A Tabela 1 mostra os achados diagnósticos dospacientes deste estudo, comparando-os com oscasos anteriormente descritos em nosso meio. ATabela 2 apresenta os dados demográficos, quadro
clínico, tratamento e evolução dos casos da pre-sente série, bem como os anteriormente descritos.
DISCUSSÃO
A primeira grande série de HPC foi encontradaem sanatórios para tuberculose entre pacientes su-postamente tuberculosos.(6) Inicialmente, praticamen-te todos os pacientes recebiam tuberculostáticos antesdo diagnóstico da micose, como demonstram dozedos treze casos (92%) de HPC cavitária descritos poralguns autores.(7) Como vimos, em nosso meio aindaé alto o percentual (50%) de teste terapêutico paratuberculose, o que denota uma visão direcionadapara a tuberculose, a qual retarda o reconhecimentoda manifestação clínica da micose, com conseqüen-te progressão da doença.
A lesão precoce consiste em uma pneumoniteintersticial, contendo freqüentemente espaços aére-os enfisematosos, especialmente do tipo centrilo-bular ou bolhoso.(4) A colonização desses espaçosaéreos determina a produção de material líquidorico em antígenos fúngicos que, por dissemina-ção brônquica, causam uma pneumonite segmen-tar. A lesão tardia tem como característica essen-cial uma área de cavitação preexistente. As cavi-dades infectadas tendem a causar doença progres-siva, ocasionando fibrose pulmonar e exacerba-ção da insuficiência respiratória.(4) A rápida mu-
Figura 3 - A radiografia de tórax demonstrou opacidades maldefinidas e possíveis cavidades compredomínio em lobos superiores (Figura 3A). A TC de tórax mostrou desarranjo da estrutura de ambos ospulmões, principalmente nos lobos superiores, com áreas de consolidação e atelectasia de distribuiçãopredominante ao longo dos interstícios axiais, manifesto por bronquiectasias, cavidades cistóides eopacidade do parênquima e bolhas de enfisema paracicatriciais. À esquerda, as cavidades eram demaiores dimensões e algumas destas contendo septações ou vegetações intracavitárias. Não haviaadenomegalia ostensiva no mediastino embora alguns linfonodos tivessem dimensões ligeiramenteacima do usual (Figura 3B).
TABELA 1
Diagnóstico micológico
Casos Material GMS Cultivo IDh
LITERATURA
1(13) Escarro + + H, M
2(13) Escarro + + H, M
3(13) Escarro + + H, M
4(5) Escarro + + NF
LBA + +
Biópsia + +5(5) Escarro + + M
Biópsia + +PRESENTE SÉRIE
6 Escarro - - M(caso 1) LBA + -
7(caso 2) Escarro - - M
Biópsia + +8
(caso 3) Escarro + + M9
(caso 4) Escarro + - M
Unis G, Severo LC. J Bras Pneumol 2005; 31: 318-24
Histoplasmose crônica
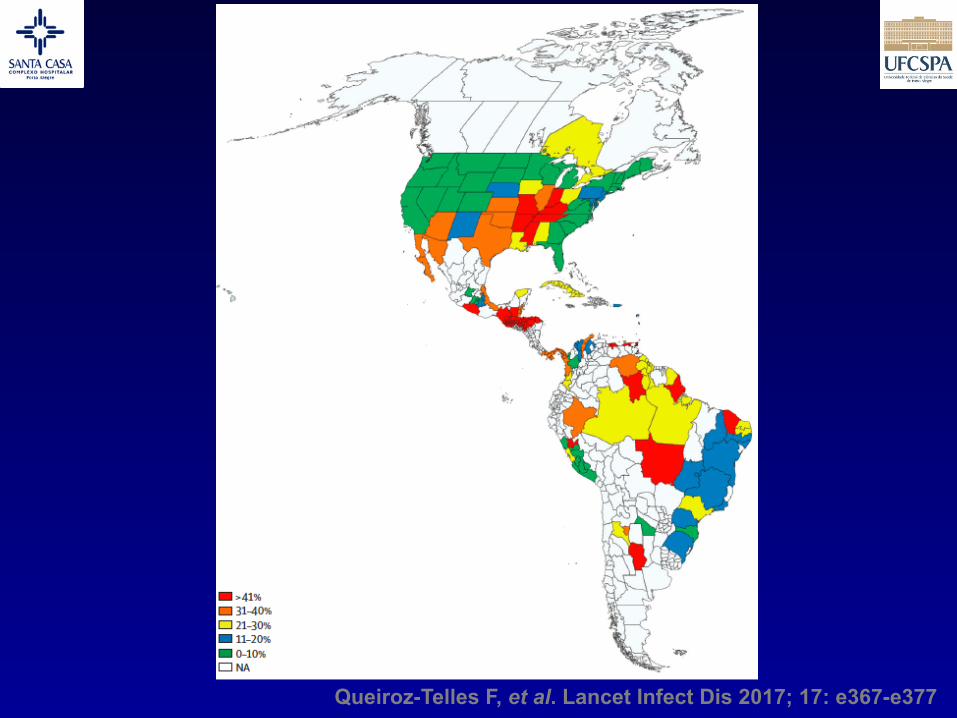
Queiroz-Telles F, et al. Lancet Infect Dis 2017; 17: e367-e377


Sífilis do mundo fúngico

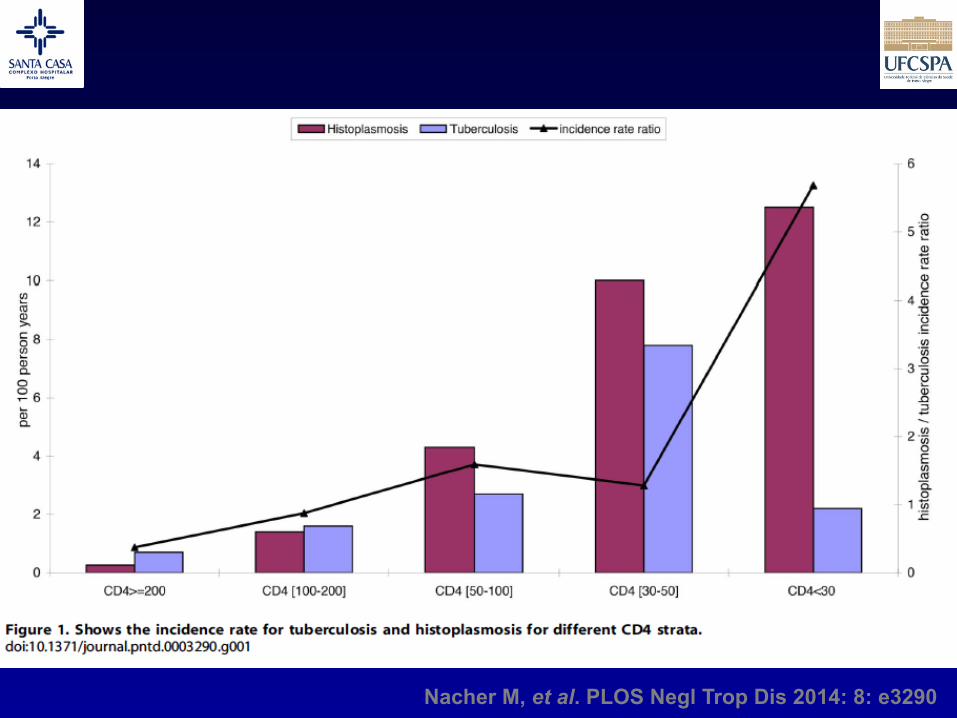
Nacher M, et al. PLOS Negl Trop Dis 2014: 8: e3290
Tempo para diagnóstico
Frequência de doença cutânea
Mortalidade global
Aspectos importantes

scattered nodular, mass-like, and bronchopneumonicpatterns. Single nodular and mass-like patterns weredefined when the lung lesion consisted of a single noduleand a single mass, respectively. The multiple clusterednodular pattern was defined when the lesions consisted ofmultiple variable-sized nodules confined to one lobe,whereas the multiple scattered nodular pattern was definedwhen lesions consisted of multiple variable-sized nodulesscattered throughout multiple lobes in a single lung or inboth lungs. The bronchopneumonic pattern was defined aswhen lung lesions were comprised of areas of lobular,subsegmental, or segmental consolidation, ill-definedcentrilobular small nodules (measuring 4 to 10 mm indiameter and representing peribronchiolar consolidation)or tree-in-bud (small centrilobular nodules and branchingnodules within the secondary pulmonary lobule) opacities(18). When lung lesions could not be classified into one of
the five patterns, they were classified as unclassifiable.In 11 patients, where previous CT scans were available,
the scans were also analyzed with the use of the above-mentioned methods and the findings were compared withthose seen on CT scans at the time of presentation.
PET or PET/CT Details on imaging methods have been described in
previous reports (19, 20). Briefly, the peripheral bloodglucose levels were 150 mg/dL in all patients. Patientsreceived an intravenous injection of 370 MBq (10 mCi)18F-fluorodeoxyglucose (FDG) and were then allowed torest for over 45 minutes prior to scanning. Image acquisi-tion was achieved by way of a PET (Advance, GEHealthcare, Milwaukee, WI) or PET/CT device (DiscoveryLS, GE Healthcare) consisting of an Advance NXi PETscanner and an 8-slice LightSpeed Plus CT scanner.
Song et al.
410 Korean J Radiol 11(4), Jul/Aug 2010
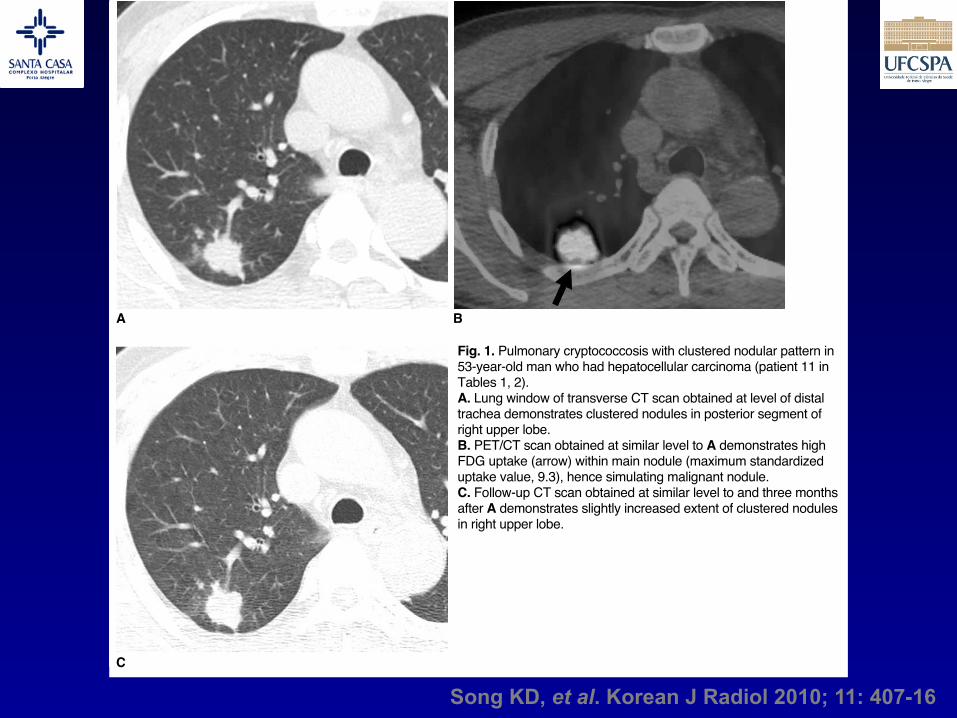
Fig. 1. Pulmonary cryptococcosis with clustered nodular pattern in53-year-old man who had hepatocellular carcinoma (patient 11 inTables 1, 2).A. Lung window of transverse CT scan obtained at level of distaltrachea demonstrates clustered nodules in posterior segment ofright upper lobe.B. PET/CT scan obtained at similar level to A demonstrates highFDG uptake (arrow) within main nodule (maximum standardizeduptake value, 9.3), hence simulating malignant nodule.C. Follow-up CT scan obtained at similar level to and three monthsafter A demonstrates slightly increased extent of clustered nodulesin right upper lobe.
A B
C
Song KD, et al. Korean J Radiol 2010; 11: 407-16

Of seven patients who were treated with antifungalagents only, one patient (patient 23 in Tables 1, 2, treatedwith amphotericin and fluconazole) showed completeclearance. In the remaining six patients, who were treatedwith fluconazole, a partial response was noted. The meanfollow-up period was 14 months (range, 5 26 months). Inthese six patients with remaining disease, symptoms suchas a cough, sputum, fever, and chest pain disappearedwithin three or six months of the treatment outset.
DISCUSSION
In our study, the most frequent pattern of lungabnormalities depicted on CT scans was clustered nodules,which was observed in 10 (43%) patients. This pattern wasfollowed by solitary pulmonary nodular (n = 4, 17%) andscattered nodular (n = 3, 13%) patterns. Thus, nodularlesions localized to a lobe or scattered to lung(s) accountedfor 73% of lung parenchymal abnormalities. Our resultsconcur with findings of previous reports in which clusterednodules or a solitary pulmonary nodule was the mostcommon pattern of lung abnormalities for pulmonarycryptococcosis (9 11, 21).
Of the 11 patients that underwent previous CT scansbefore presentation, all patients showed slow progressionor no change with respect to the extent of the lung lesions.In particular, two patients, in which the lesions increased insize by more than two times the original diameter atapproximately 50 days after the initial assessment. None ofthe patients showed spontaneous resolution of parenchy-mal lung lesions. Therefore, a specific diagnosis of crypto-coccosis is mandatory for the management of this infection.On the other hand, the chronicity of lung lesions was noted
after the diagnosis of the disease was confirmed. Lunglesions were indolent and the lung lesions did not show arapid response to antifungal therapy.
In our study, 11 (48%) of 23 patients were immunocom-promised and 12 were immunocompetent. However, thedisease patterns between the two groups were not differ-ent. Furthermore, none of the immunocompromisedpatients showed a disseminated disease pattern such asdiffuse interstitial lung disease accompanied by extensivehilar and mediastinal lymphadenopathy.
It is well known that active tuberculosis or tuberculoma,acute and chronic pneumonia, lung abscess, fungalinfection, and parasitic infestation are frequent causes ofincreased FDG uptake (22). For these conditions, thepresence and activity of leukocytes account for theincreased FDG uptake. Activated macrophages andneutrophils in inflammatory tissue utilize glucose as anenergy source for chemotaxis and phagocytosis, whereasfibroblasts utilize glucose for proliferation. In our study, six(60%) of 10 patients that underwent PET or PET/CT scansshowed high FDG uptake. Moreover, five (83%) of thesesix patients had an underlying malignancy. Pulmonarymetastases could not be excluded in these five patientsbecause of the presence of multiple pulmonary noduleswith a high rate of FDG uptake were noted on the PETscans, even though the nodules showed clustering on CTscans, persisted for a quite amount of time. Thus, even inpatients with an underlying malignancy and lung nodulesthat demonstrate high FDG uptake, when nodules areclustered in a lobe, a histopathological diagnosis should beperformed for tissue confirmation.
The complete clearance of lung abnormalities wasachieved in 15 patients. Of these 15 patients, surgicalresection with or without subsequent antifungal therapywas needed for complete clearance in 14 patients. In theremaining patient, complete clearance was achieved withantifungal therapy only. In the seven patients that wereadministered antifungal therapy only, a partial responsewas noted in six patients. In these six patients, althoughclinical improvement was achieved, the lung lesionspersisted after the treatment, as seen on serial imagingstudies. In one patient that was not given a treatment, thedisease showed progression. Thus, lung lesions wereindolent and they did not show a rapid response to antifun-gal therapy.
Actinomycosis, semi-invasive aspergillosis, andpulmonary tuberculosis are well-known representativecauses of chronic pneumonias that usually show anindolent disease course, before and after treatment. Thesethree diseases usually present as single or multiplenodule(s) or mass or as a single area of dense consolidation
Song et al.
414 Korean J Radiol 11(4), Jul/Aug 2010
Fig. 5. Pulmonary cryptococcosis of solitary mass pattern in 52-year-old woman with no underlying disease (patient 8 in Tables 1,2). Lung window of CT scan obtained at level of right middle lobarbronchus shows mass in right middle lobe.
Song KD, et al. Korean J Radiol 2010; 11: 407-16
Teste do látex para criptococose
Teste do látex para criptococose
x

CrAg – LFA para criptococose

Conclusões
• Ajudem o clínico! Orientem o diagnóstico
ü Muita gente ficará grata. Pacientes também.