mosaic tumor vessels: cellular basis and …...mosaic tumor vessels: cellular basis and...
TRANSCRIPT

Mosaic Tumor Vessels: Cellular Basis and Ultrastructure of Focal
Regions Lacking Endothelial Cell Markers
Emmanuelle di Tomaso,1Diane Capen,
2Amy Haskell,
3Janet Hart,
1James J. Logie,
1Rakesh K. Jain,
1
Donald M. McDonald,3Rosemary Jones,
2and Lance L. Munn
1
Steele Laboratory for Tumor Biology, Departments of 1Radiation Oncology and 2Anesthesia and Critical Care, Harvard Medical Schooland Massachusetts General Hospital, Boston, Massachusetts; and 3Cardiovascular Research Institute, Comprehensive Cancer Center,and Department of Anatomy, University of California San Francisco, San Francisco, California
Abstract
Endothelial cells of blood vessels in tumors may be thin,fragile, and defective in barrier function. We found previouslythat the endothelium of vessels in human colon carcinomaxenografts in mice is a mosaic structure. Approximately 85%of tumor vessels have uniform CD31 and/or CD105 immuno-reactivity, but the remainder have focal regions that lack thesecommon endothelial markers. The present study assessed theultrastructure of the vessel lining and the integrity of thebasement membrane in these regions. Using immunolabelingand confocal microscopy, we identified blood vessels thatlacked CD31 and CD105 immunoreactivity and then analyzedthe ultrastructure of these vessels by transmission electronmicroscopy. Eleven percent of vessels in orthotopic tumorsand 24% of vessels in ectopic tumors had defects in CD31and CD105 staining measuring on average 10.8 Mm (range,1-41.2 Mm). Ultrastructural studies identified endothelialcells at 92% of CD31- and CD105-negative sites in orthotopictumors and 70% of the sites in ectopic tumors. Thus, mostregions of tumor vessels that lack CD31 and CD105immunoreactivity represent attenuated endothelial cells withabnormal expression of endothelial cell markers, but someare gaps between endothelial cells. More than 80% of thedefects lacked immunoreactivity for multiple basementmembrane proteins. (Cancer Res 2005; 65(13): 5740-9)
Introduction
Angiogenesis in tumors produces poorly formed blood vesselshaving multiple abnormalities. Morphologic and immunohisto-chemical studies of tumors have identified changes in geneexpression, defective endothelial cell barrier function, looseattachment of pericytes (mural cells and perivascular cells), andredundant layers of vascular basement membrane (1–7). In aprevious study, we assessed the cellular composition of bloodvessels in human adenocarcinomas implanted in mice usinggreen fluorescent protein (GFP)-expressing cancer cells andfluorescent antibodies to label endothelial cells (8). We foundthat 15% of the vessels examined, representing f4% of thevascular surface area, had focal regions that lacked immunore-activity to the common endothelial cell markers CD31 (platelet/endothelial cell adhesion molecule-1, PECAM-1) and CD105(Endoglin).
These vessels, termed ‘‘mosaic vessels’’, had several potentialexplanations. First, endothelial migration during rapid vesselgrowth could occur without sufficient endothelial proliferation tocomplete the endothelial lining, leaving cancer cells exposed to thelumen. Second, endothelial cells could be shed from the vessellining, leaving similar regions of exposed underlying tumor cells.Third, migrating tumor cells could invade the vessel wall,displacing endothelial cells from the lining. And fourth, theseregions could be lined by endothelial cells that do not expresscommon endothelial markers, and were consequently not detected.These scenarios have implications for vessel physiology and
therapeutic targeting (8, 9). Holes in the endothelium due tomissing endothelial cells might be responsible for the leakiness oftumor vessels, which can actually hinder uniform drug delivery(10, 11). Alternatively, the presence of tumor cells in the vessel wallcould be an indication of tumor aggressiveness or metastasis.Absence of detectable CD31 and CD105 might be accompanied byother alterations in protein expression in tumor endothelial cells,possibly induced by the hostile tumor microenvironment. Thiscould also influence endothelial functions including barrierformation and angiogenesis.The present study sought to determine the cellular basis of the
mosaicism in CD31/CD105 staining found in tumor vessels. Toaddress this issue, we developed a four-step approach that enabledus to examine the ultrastructure of regions of endothelium thatlack expression of CD31 and CD105 identified by confocalmicroscopy. First, endothelial cells of tumor vessels were labeledin vivo by injection of antibodies to CD31 and CD105. Second,tumors were harvested and embedded in a resin compatible withboth confocal and transmission electron microscopy (TEM). Third,adjacent 2-Am and 80-nm sections were cut, and fourth, bloodvessels that had focal defects in CD31/CD105 immunoreactivityidentified by confocal microscopy were examined by electronmicroscopy in adjacent sections. The approach made it possibleto examine endothelial cell ultrastructure in regions lacking endo-thelial markers.We found that most mosaic vessels in mouse models of colon
carcinoma had a continuous, thin endothelial lining which lackedCD31 and CD105 immunoreactivity, rather than absence ofendothelial cells or presence of tumor cells in the vessel wall.Focal openings in the endothelium were present in some tumorvessels, particularly in ectopic xenografts, which had a rapidgrowth rate.
Materials and Methods
Green fluorescent protein construct. To provide an endogenous
marker for cancer cells, a LS174T colon carcinoma cell line was transfected
with a GFP construct driven by a constitutive promoter, EF1a. Selection was
Requests for reprints: Lance L. Munn, Department of Radiation Oncology,Harvard Medical School and Massachusetts General Hospital, 100 Blossom Street,Cox-7, Boston, MA 02114. Phone: 617-726-4085; Fax: 617-726-1962; E-mail: [email protected].
I2005 American Association for Cancer Research.
Cancer Res 2005; 65: (13). July 1, 2005 5740 www.aacrjournals.org
Research Article
Research. on June 5, 2020. © 2005 American Association for Cancercancerres.aacrjournals.org Downloaded from

carried out by exposing the transfected cell lines to puromycin (1 Ag/mL).Stable transfectants were obtained using fluorescence-activated cell sorting
gated on the GFP-positive population (8).
Tumor models. Fluorescent LS174T cells, designated LSEFG, were
implanted in female severe combined immunodeficiency mice anesthe-tized with ketamine/xylazine (100/10 mg/kg, i.m.). All GFP-expressing
tumor cells were implanted at the same passage number. To assess the
effect of host microenvironment on tumor vasculature, tumors were grown
in orthotopic (cecum) or ectopic (ovarian pedicle) sites. For the orthotopictumor model, a midline incision was made in the abdominal wall to
expose the cecum. A thin cut was made in the serosa of the cecum, and
0.05 to 0.1 mL of LSEFG tumor slurry was injected into a pocket in the
cecal wall. Tumors in this site grew slowly, reaching a diameter of 6 to10 mm over a period of 7 to 10 weeks. Alternatively, a small piece
(0.125 mm3) of tumor tissue was implanted in the cecal wall. In this case,
tumors reached a diameter of 6 to 10 mm in 3 to 4 weeks. In both models,the tumor blood supply formed from cecal blood vessels. Because the size
and overall wall structure of tumor vessels formed after implantation of a
slurry of cells or piece of tumor were similar, the data were analyzed
together.In the ectopic model, 0.1 mL of tumor slurry was injected into the
ovarian pedicle after ovariectomy. Tumors were isolated from surrounding
tissue by enclosure in a bag of Parafilm (American National Can Company,
Menasha, WI). In this model, the tumor blood supply originates frombranches from the main artery and vein in the ovarian fat pad (12). Ectopic
tumors grew to a diameter of 6 to 10 mm within 10 to 14 days (13). A total
of nine orthotopic tumors and six ectopic tumors were studied.Antibody infusion. For confocal microscopy, endothelial cells of tumor
vessels were labeled in situ by i.v. injection of a mixture of two fluorescent
antibodies: rat anti-mouse CD31 (PECAM-1, clone MEC 13.3, PharMingen,
San Diego, CA) and rat anti-mouse CD105 (Endoglin, PharMingen). Anti-CD31 and anti-CD105 antibodies label most endothelial cells in mice
uniformly, but anti-CD105 labeling is particularly strong in angiogenic
tumor vessels (14–16). Before injection, both antibodies were labeled with
Cy5 fluorophore according to the manufacturer’s protocol (FluoroLink kit,Amersham Pharmacia Biotech, Piscataway, NJ). After anesthesia with
ketamine/xylazine (100/10 mg/kg, i.m.), mice were infused with a mixture of
the two antibodies (total antibody protein, 50-60 Ag in 200 AL) via tail veinover a 30-minute period. The antibodies were allowed to circulate for 1 hour
before the tumors were fixed by vascular perfusion (see below). No signal
was detected when Cy5-labeled rat IgG was injected according to the same
protocol as a negative control. Labeling tumor vessels with systemicallyinjected antibodies ensured that the analyzed vessels were functional and
perfused with blood at the time of fixation. Few vessels were unperfused or
completely devoid of CD31 and CD105 expression, as judged by comparing
the electron microscopy and confocal microscopy vessel maps of the sametissue.
Sequential confocal microscopy and electron microscopy analyses.For correlation of confocal and TEM images, tumors were fixed by vascular
perfusion of fixative consisting of 3% paraformaldehyde and 0.1%glutaraldehyde in 0.9% PBS (pH 7.4; ref. 17). The thorax was opened, a
blunt 18-gauge needle was inserted into the left ventricle, the auricles of
both atria were opened, and then the fixative was perfused through thevasculature for 10 minutes at a pressure of 80 to 100 mm Hg. Tumors were
left in situ for 1 hour, removed, cut in half and immersed in the same
fixative for at least 2 hours. One half of the tumor was then prepared for
sequential confocal and electron microscopy analysis, and the other forimmunohistochemical analysis of the basement membrane (see below).
For the sequential confocal and electron microscopy study, the tissue was
dehydrated and embedded in LR White without postfixation in osmium
tetroxide (18).Serial sections were cut in the following sequence: (a) a 1 Am section was
cut for toluidine blue staining; (b) a 2 Am section was cut for assessing
CD31/CD105 immunoreactivity by confocal microscopy; (c) 10 sections,80 nm thick, were cut for TEM; (d) another 2 Am section was cut to confirm
the same immunolabeling in the vessel by confocal microscopy, and finally
(e) another 1 Am section was cut for toluidine blue staining. This procedure
made it possible to identify regions of endothelium lacking detectableCD31/CD105 immunoreactivity in the first confocal section and then to
determine the corresponding ultrastructural features in the adjacent TEM
sections. The two confocal microscopy sections were analyzed to identify
changes in the staining pattern over the f5 Am span of the serial sections.Only vessels with the same CD31/CD105 staining pattern in both confocal
sections were included in the analysis.
Using this combined confocal/TEM approach, we obtained images from
six orthotopic tumors (three slurries and three chunks) and three ectopictumors using either a Leica TCS-NT 4D or Zeiss LSM Pascal confocal
microscope and a Philips TEM 300 electron microscope equipped with a
digital camera. All vessels analyzed in this way had at least some CD31/
CD105 staining and thus had blood flow. Vessels with focal regions lackingboth endothelial markers were mapped by confocal microscopy and
reanalyzed by electron microscopy. Tumor cells were identified by
endogenous expression of GFP. Measurements of acquired images weremade with NIH Image (http://rsb.info.nih.gov/nih-image/). At least five
vessels with labeling abnormalities were analyzed in three different mice for
each of the two tumor models.
Immunohistochemistry. The other half of the tissue from theharvested tumors was prepared for immunohistochemical analysis of the
basement membrane. This tissue was rinsed five times with PBS,
infiltrated with 30% sucrose in PBS overnight and embedded in ornithine
carbamyl transferase for cryostat sectioning. Cryostat sections (10- to80-Am-thick) were cut at varying depths and stained by conventional
immunohistochemistry. The vascular basement membrane was labeled
using antibodies to rabbit anti-mouse type IV collagen (1:2,000), rat anti-mouse laminin (1:120,00), rat anti-mouse nidogen (entactin, 1:24,000), or
rat anti-mouse perlecan (1:80,000; Chemicon, Temecula, CA; ref. 19).
Antibodies to basement membrane markers were visualized by incubation
with Cy3-labeled donkey anti-rat or anti-rabbit secondary antibodies (1:400dilution, 3 hours, 25jC; Jackson Immunoresearch, West Grove, PA).
Endothelial cells were labeled by the injected Cy5-labeled antibodies,
and tumor cells had endogenous expression of GFP. Three-color images
were obtained with an Olympus Fluoview 500 confocal microscope toreveal the cancer cells, the endothelial cells, and the basement membrane
component.
Conventional electron microscopy. For conventional electron micros-copy, tumors were fixed by vascular perfusion as above except that the
fixative consisted of 3% glutaraldehyde in cacodylate buffer (20). Tumors
were removed, and pieces measuring f1 to 3 mm were cut, rinsed with
100 mmol/L cacodylate buffer, fixed with 1% OsO4 in 100 mmol/Lcacodylate buffer at 4jC for 2 hours, rinsed with water, stained en bloc
with 2% aqueous uranyl acetate for 48 hours at 38jC, dehydrated with
acetone, and embedded in epoxy resin (20). Sections 0.5 Am in thickness
were stained with toluidine blue for light microscopy, and sections 60 to80 nm in thickness were stained with lead citrate and examined with a Zeiss
EM-10C or Philips TEM 300 electron microscope. All vessels visible by
electron microscopy in sections of orthotopic tumors from three mice were
photographed sequentially until images of 100 vessels were obtained. Inaddition, 38 vessels with a potentially abnormal wall structure were
identified in toluidine blue–stained sections of ectopic tumors from two
mice, and then 80 nm sections of the same vessels were cut, stained withuranyl magnesium acetate, counterstained with lead citrate, and photo-
graphed by electron microscopy. Endothelium was identified by the
following criteria: (a) the cells formed a continuous polarized surface layer
adluminal to basement membrane, (b) all cells had an intact plasmalemmalmembrane, (c) junctions (overlapping or abutting) were evident between
adjacent cells, and (d) in nucleated regions, extensive rough and smooth
endoplasmic reticulum, some vesicles and an occasional Golgi complex
were evident.Peeling of the endothelium due to sectioning was very rarely observed.
However, in some vessels, the endothelial lining was extremely fragile and
the 80 mm Hg perfusion was sufficient to detach it. This does not occurwhen the same procedure is used for normal tissue. On the rare occasion
when plasmalemma membrane disruption was visible, the vessels were
excluded from the study.
Ultrastructure of Tumor Vessel Defects
www.aacrjournals.org 5741 Cancer Res 2005; 65: (13). July 1, 2005
Research. on June 5, 2020. © 2005 American Association for Cancercancerres.aacrjournals.org Downloaded from

Results
Comparison of orthotopic and ectopic xenografts. The twoxenograft models of LS174T colon carcinoma had differentpatterns of growth. Tumors implanted orthotopically in thececum grew slowly, invaded the gut wall, and formed multiplesmall tumor nodules surrounded by host tissue (Fig. 1A). Bycomparison, ectopic tumors grew rapidly, supported by a bloodsupply from branches of ovarian arteries and veins, but theParafilm bag prevented the tumors from invading neighboringtissue (Fig. 1B ; ref. 12). Blood vessels within orthotopic andectopic tumors were approximately the same size (6-16 Am indiameter, Fig. 1C and D).Frequency of regions lacking CD31 and CD105. A quantitative
analysis of tumor vessels examined by confocal microscopy afterstaining for CD31 and CD105 immunoreactivity revealed focalregions without detectable CD31 or CD105 immunoreactivity in11% (226 vessel profiles) and 24% (353 vessels profiles) of vessels inthe orthotopic and ectopic tumors, respectively. The remainingvessels had uniform CD31 and/or CD105 (CD31/CD105) immuno-reactivity (Fig. 2A and B). This feature applied both to orthotopicand to ectopic tumors. Most blood vessels of both types of tumorwere surrounded by multiple, irregular layers of basementmembrane that extended well beyond the endothelium into thestroma (Fig. 2C). Electron microscopic studies revealed thatendothelial cells of most tumor vessels were thin in regions other
than the nucleus (Fig. 2D and E). Tumor cells were located close tothe wall in most vessels (Fig. 2E).Transmission electron microscopy analysis of regions
lacking CD31 and CD105. A total of 46 tumor vessels with focalregions lacking detectable CD31/CD105 immunoreactivity (26 insix orthotopic tumors and 20 in three ectopic tumors) wereexamined sequentially by confocal microscopy and electronmicroscopy. Thin endothelial cells, some focally detached fromthe matrix, were found in 24 of the 26 vessels (92%) lackingdetectable CD31/CD105 staining in orthotopic tumors. In only twovessels, representing 0.8% of vessel profiles examined in orthotopictumors, did focal lack of CD31/CD105 immunoreactivity coincidewith an ultrastructurally confirmed opening in the endothelium.The gaps ranged from 1.9 to 4.1 Am.Among the 20 vessels in ectopic tumors with focal lack of
detectable CD31/CD105 immunoreactivity, 14 were confirmed byTEM to have a luminal cell layer in these locations. In mostinstances, these cells were extremely thin endothelial cells. (Fig. 3A-F).In rare cases, the subcellular structure of the cell layer and limitedresolution prevented classification of the cell (Fig. 3G-I).The remaining six vessels from ectopic tumors (30% of the
vessels with CD31/CD105-negative regions) had focal openings inthe endothelium or regions where endothelial cells had separatedfrom one another or were missing (Fig. 4).Size and number of endothelial gaps in tumor vessels. We
selected LR White for our combined confocal/TEM study
Figure 1. Comparison of colon carcinomaxenografts grown in orthotopic and ectopiclocations. Toluidine blue–stained epoxysections of LS174T human coloncarcinomas grown from a cell slurryimplanted orthotopically in the wall of thececum of mice (A and C ) or ectopicallyin the ovarian fat pad after ovariectomy(B and D ). Green lines delineate thetumor; red lines highlight the largest bloodvessels; yellow lines mark the intestinalmuscle; and magenta line shows theborder of the host fat and connective tissuearound the ectopic tumor. Dissemination ofthe orthotopic tumor is evident from thepresence of multiple nodules in the cecalwall. By comparison, ectopic tumors didnot infiltrate because growth was localizedby the Parafilm bag. Blood vesselssupplying ectopic tumor in (B) arosefrom branches of ovarian arteries (*)and veins (**). Only small blood vesselswithin the tumor mass (e.g., * in C and D)were analyzed for endothelial defects.Bar, 500 Am (A and B); 10 Am (C and D ).
Cancer Research
Cancer Res 2005; 65: (13). July 1, 2005 5742 www.aacrjournals.org
Research. on June 5, 2020. © 2005 American Association for Cancercancerres.aacrjournals.org Downloaded from

because it allowed analysis of the same vessels by bothtechniques. To supplement our TEM data, we completedadditional studies in which tissue was embedded in epoxy resinto optimize preservation of cellular detail. Although it was notpossible to visualize immunofluorescence using this medium(and thus, could not confirm lack of CD31/CD105 expression),we were able to confirm the existence of the same endothelial
abnormalities seen in the LR White embedded tissue. In asystematic TEM study of 100 sequential vessels in threeorthotopic tumors, half of the vessel profiles had regions ofthin endothelium (mean thickness, 0.4 Am; range, 0-2 Am)immediately adjacent to tumor cells, separated by an averagedistance of only 0.2 Am (range, 0.01-1.6 Am; Fig. 5A and B). Thisanalysis also revealed the presence of small gaps (mean size,
Figure 2. Confocal microscopic images of orthotopic LS174T tumor showing blood vessels with uniform staining for CD31/CD105 immunoreactivity (A-C, red),GFP labeled tumor cells (A, green ), and laminin in vascular basement membrane (C, blue ). A -C show a projection of a 60 Am confocal stack. C, redundant layersof vascular basement membrane that cover and extend away from tumor vessels. Bar, 20 Am (A-C ). Electron microscopic images showing that endothelial cellsin LS174T tumors were extremely thin (D and E ), and tumor cells were located adjacent to the vessel wall (E ). Pericytes are next to endothelial cells and tumor cells.In the higher magnification view (E), basement membrane can be seen between the endothelial cell (thickness, 0.24 Am) and pericyte (thickness, 1.36 Am) and betweenthe pericyte and the tumor cell. Basement membrane thickness is 0.24 Am between the endothelial cell and pericyte and 0.8 Am between the pericyte and tumorcell. Bar, 5 Am (D and E).
Ultrastructure of Tumor Vessel Defects
www.aacrjournals.org 5743 Cancer Res 2005; 65: (13). July 1, 2005
Research. on June 5, 2020. © 2005 American Association for Cancercancerres.aacrjournals.org Downloaded from

0.9 Am; range, 0.1-3.3 Am) between endothelial cells in 15% ofvessel profiles (Fig. 5C-E).In a separate study, vessels of ectopic tumors embedded in epoxy
resin were examined and similar ultrastructural defects wereidentified, first in 1 Am toluidine blue sections and then by TEM. Ofthe 31 vessels identified, 39% had a complete endothelial lining andunderlying basement membrane, 19% had a thin but completeendothelial cell lining and attenuated basement membrane withtumor cells close to the endothelium, and 42% had an abnormallytented or discontinuous endothelium (size range, 0.5-25 Am).Basement membrane of tumor vessels with CD31/CD105-
negative regions. Immunohistochemical staining showed thatbasement membrane was present in some CD31/CD105-negative
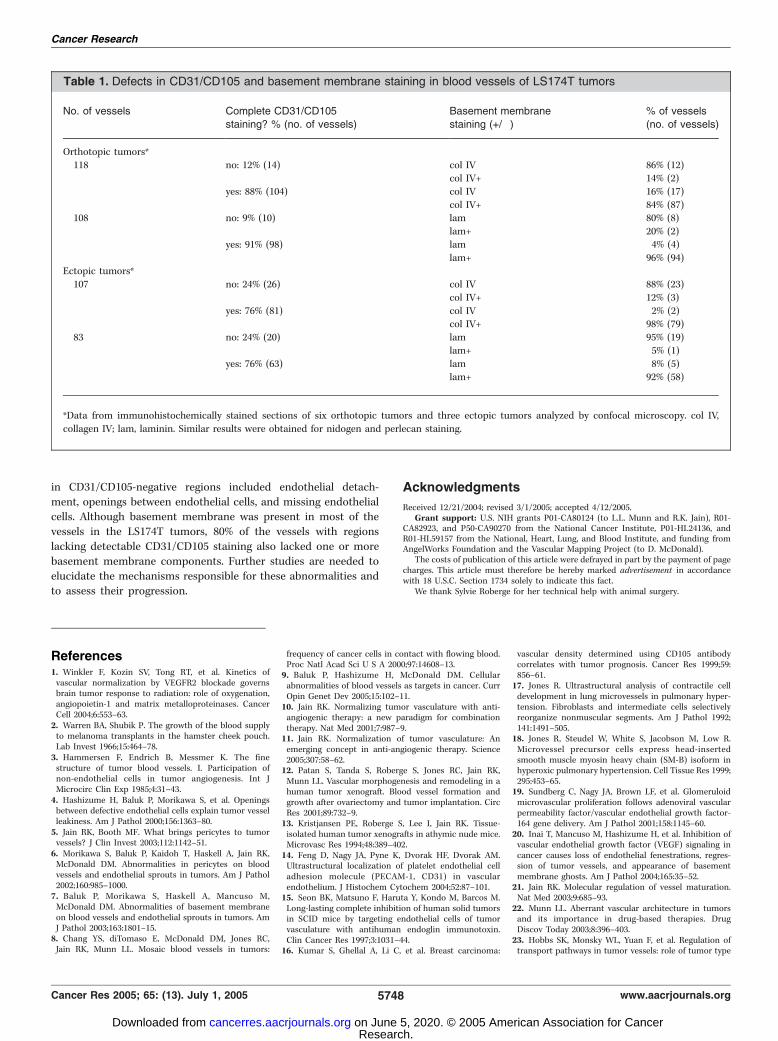
regions (Fig. 6A), but was missing in most of these regions (Fig. 6B).Ultrastructural analysis showed similar basement membraneabnormalities at endothelial gaps (Figs. 5E and 6C). In order toassess basement membrane association in CD31/CD105-negativeregions, we labeled type IV collagen and laminin (major basementmembrane components). In orthotopic tumors, only 10% of vesselswith intact CD31/CD105 staining had regions lacking immunore-activity for one of the basement membrane proteins, but 83% ofvessels with CD31/CD105-negative regions had sites lacking abasement membrane marker (Table 1). In ectopic tumors, all but3% of vessels with intact CD31/CD105 had staining for thebasement membrane markers, but 90% of vessels with CD31/CD105-negative regions had focal defects in basement membrane
Figure 3. Ultrastructure of vessels lackingdetectable CD31/CD105 immunoreactivity.A (inset ), tumor vessel in a toluidineblue–stained 1-Am section of an LRWhite-embedded tumor viewed by lightmicroscopy. A and B, the same vesselin an adjacent 2 Am section viewed byconfocal microscopy (red , CD31/CD105immunoreactivity of endothelium; green ,GFP-expressing tumor cells). Only the redchannel of this vessel is shown in (B ); bar,20 Am in (A and B). C and D, detail of theboxed region at left in (B ). C, TEM image froman 80 nm section adjacent to the one shownin (A and B). D, enhanced version of (C ) toshow the cancer cells (pale green ) and theendothelium (blue ). Note the endotheliallayer is complete although there is lack ofimmunostaining in some regions (A and B ).E, detail of the boxed region in (B , right).F, enhanced version of (E ) to show the cancercells (pale green) and the endothelium (blue ).Note the endothelial layer and immunostain areboth complete in this region. Bar, 5 Am (C-F ).G , blood vessel in an orthotopic tumor with aregion of endothelium lacking CD31/CD105staining. G (inset ), vessel in a 1 Am toluidineblue–stained section. Confocal microscopicimage of the same vessel (red , CD31/CD105immunoreactivity) surrounded by GFPexpressing tumor cells (green ). CD31/CD105is partially missing in the boxed region. H andI, TEM image of the same tumor vessel showsthe presence of cell processes in the regionlacking CD31/CD105 staining. Here, thesubcellular structure of the cell layer andthe limit of resolution prevented cleardetermination of cell phenotype. Furthermore,the unstained cell processes in this region werenot continuous with the recognizable regions ofadjacent endothelium, and no overlapping orabutting cell junctions could be identified.I, diagram showing enhanced version of thisimage. CD31/CD105-positive endothelial cellsare blue, tumor cells are pale green, and CD31/CD105-negative/GFP-negative cell processesare orange. Bar, 5 Am (G-I ).
Cancer Research
Cancer Res 2005; 65: (13). July 1, 2005 5744 www.aacrjournals.org
Research. on June 5, 2020. © 2005 American Association for Cancercancerres.aacrjournals.org Downloaded from

staining (Table 1). Two other basement membrane components,perlecan and nidogen, gave similar values for the proportion ofvessels with basement membrane defects (data not shown). Thesefindings suggest a possible link between the loss of CD31/CD105immunoreactivity and focal disruption of the underlying vascularbasement membrane.
Discussion
In a previous study, we reported that f15% of blood vessels inhuman colon carcinoma xenografts have focal regions that lackimmunoreactivity for the endothelial cell markers CD31 andCD105 (8). The present study of the same tumors extends thisprevious study by assessing whether CD31/CD105-negativeregions represented missing endothelial cells or were, instead,defects in endothelial cell expression of these markers. WhenCD31/CD105-negative regions were examined by TEM in bothorthotopic and ectopic tumors, we found an extremely thinendothelium closely apposed to tumor cells; surprisingly, theendothelium was generally continuous even in regions with no
observed expression of common endothelial markers. In coloncarcinoma xenografts implanted orthotopically, the majority(92%) of the mosaicism was explained by undetectable CD31and CD105 expression rather than missing endothelial cells.However, in tumors implanted ectopically in the ovarian bursa,30% of vessel profiles with CD31/CD105-negative regions hadopenings in the endothelium or missing endothelial cells. MostCD31/CD105-negative regions did not have detectable immuno-reactivity for the basement membrane proteins type IV collagenor laminin.Our approach of combining immunofluorescence, confocal
microscopy, and TEM analysis allowed assessment of specificimmunoreactivity of cell markers and tissue ultrastructure in thesame vessel. The perfusion of antibodies conjugated with Cy-5labels the endothelium of functional vessels expressing CD31and/or CD105, whereas TEM provides high-resolution images ofthe cells forming the vessel wall. These two techniques wereexploited to determine the ultrastructure of the walls of tumorvessels lacking both CD31 and CD105. The specific ultrastructuralchanges identified in tissue embedded in LR White (thin
Figure 4. A-D, confocal and TEM viewsof a tumor vessel with a broad regionof endothelium lacking CD31/CD105immunoreactivity. A and B, confocalmicroscopic images showing CD31/CD105staining (red) of part of the vessel wallsurrounded by GFP expressing tumor cells(green ). B, shows only the CD31/CD105immunoreactivity of the same vessel. Thewhite box outlines a region where CD31and CD105 signal is similar to backgroundlevel. C and D, TEM images of the sametumor vessel. By high-magnificationanalysis, the cell process lining the vesselseems to be continuous throughout theboxed region. Bar, 5 Am (A-C ) and1.2 Am (D ).
Ultrastructure of Tumor Vessel Defects
www.aacrjournals.org 5745 Cancer Res 2005; 65: (13). July 1, 2005
Research. on June 5, 2020. © 2005 American Association for Cancercancerres.aacrjournals.org Downloaded from

endothelium, gaps, missing endothelial cells, basement mem-brane defects) were also validated in tissue prepared forconventional TEM (which is optimally preserved by using a highglutaraldehyde concentration and secondary fixation withosmium tetroxide techniques not used for embedding tissue inLR White).Tumor vessels lack a hierarchical arrangement and have
irregular diameters, high tortuosity, random branching, anddefective endothelial barrier function (21, 22). Pericytes andbasement membrane of tumor vessels are also abnormal (6, 7).These abnormalities result from the bizarre microenvironment intumors, with growth factor under- or overproduction combinedwith hypoxia and metabolic disturbances. The present studyaddressed a peculiar abnormality in tumor vessels—focalabsence of endothelial expression of CD31 and CD105—that isrelevant to endothelial barrier function in tumors (8). The resultsconfirmed the frequency of this abnormality, which affected 11%of vessels in orthotopic tumors and 24% in ectopic tumors, anddemonstrate that defects in CD31/CD105 expression in tumorvessels are associated with multiple structural aberrations. It is
possible that the focal hyperpermeability of tumor vessels couldbe caused by these defects in the endothelial lining andbasement membrane (23). Although relatively rare, these hyper-permeable regions could significantly dissipate the transvascularhydrostatic pressure gradient necessary for efficient delivery oftherapeutics (1, 10, 11).Abnormalities in the endothelium may reflect the dynamic
nature and continuous remodeling of tumor vessels undergoingangiogenesis, which can be accompanied by degradation of thevascular basement membrane and temporary loss of pericytes (24).Basement membrane degradation and emigration of pericytes arenot, however, a consistent feature of tumors (1, 6, 7). Loss of CD31/CD105 expression could also be a response to inflammatory factorssuch as tumor necrosis factor-a, histamine, or vascular endothelialgrowth factor, which cause redistribution of junctional moleculesto the lateral plasma membrane (14, 25) or down-regulate theirexpression (26, 27). It remains to be seen whether haphazardcooption of preexisting vessels (28) or high levels of protease activityin tumors (29) contribute to basement membrane degradation andendothelial defects.
Figure 5. Electron micrographs showingunusual features of blood vessels inorthotopic LS174T tumors. A and B,tumor vessel with thin endothelium closelyapposed to tumor cells. Region in blackbox in (A) is shown at higher magnificationin (B ). B, long arrows mark both sides ofthe endothelial cell. Short arrows mark thesurface of the closely adjacent tumor cell.C-E, examples of endothelial gaps (shortarrows ) in tumor vessels with otherwisecontinuous endothelium (long arrows ).E, endothelial gap that exposes acontinuous underlying basementmembrane. Bar, 1.4 Am in (A ); 0.4 Amin (B ); 2.2 Am in (C ), 1.2 Am in (D ); and0.8 Am in (E).
Cancer Research
Cancer Res 2005; 65: (13). July 1, 2005 5746 www.aacrjournals.org
Research. on June 5, 2020. © 2005 American Association for Cancercancerres.aacrjournals.org Downloaded from

An unexpected finding in this study was the higher incidence ofendothelial cell defects in ectopic tumors. This observationsuggests that vessel wall abnormalities can be affected by the siteof tumor growth, such as differences in host microenvironment,infiltrating blood vessels, or stromal cells (30, 31). Orthotopictumors developed within the wall of the cecum and recruited bloodvessels and stromal cells from neighboring tissues. By comparison,ectopic tumors, which were partially isolated by the Parafilmenclosure, recruited vessels and stromal cells from branches of theovarian artery and vein. In addition, LS174T tumor cells grew moreslowly in the orthotopic location. Perhaps the slower growth rateenabled tumor vessels to develop a more stable wall structure.It is unclear whether the greater endothelial abnormalities in
ectopic tumors would influence their response to angiogenesisinhibitors (32, 33). If any, the effect may be small because theendothelial cell defects occupy such a small proportion of the totalvascular surface area in these tumors. It is known that ectopic
tumors respond more favorably to low-dose metronomic chemo-therapy (34–36). Similar vascular abnormalities have been identi-fied from human tumor specimens (8), but the relevance to tumorgrowth in patients remains to be determined.In summary, the present study sought to determine the cellular
basis of focal lack of endothelial CD31 and CD105 expression intumor blood vessels. We developed a novel method for labelingtumor vessels in vivo and then analyzing the same vessel byimmunofluorescence confocal microscopy and transmissionelectron microscopy. The results confirmed our earlier suggestion(8) that the tumor environment induces altered expression ofPECAM-1 (CD31) and Endoglin (CD105) in endothelial cells,causing the observed mosaicism. The most common finding wasloss of detectable CD31/CD105 immunoreactivity despite thepresence of ultrastructurally identifiable endothelial cells. Theinvolved endothelial cells, however, usually were thin and closelyapposed to tumor cells. Other abnormalities in the endothelium
Figure 6. Basement membrane defectsin regions of endothelium lackingCD31/CD105 staining. A, confocal imagesof blood vessel in ectopic tumor withmultiple sites lacking CD31/CD105immunoreactivity. CD31/CD105expression (white ) of tumor vesselsurrounded by GFP-expressing tumor cells(green ). CD31/CD105 immunoreactivityis not detectable in at least two sites(arrow and arrowheads). B, anotherconfocal image of the same vesselshowing the basement membrane proteinnidogen (red), which envelopes mostof the vessel including one of theCD31/CD105 defects (arrowheads ) but isnot detectable at another (arrow ). Notethat some small structures seem to havethe basement membrane protein nidogenwhereas no CD31/CD105 is detectable;these are likely vessels that were notcarrying blood at the time of CD31injection. C, electron micrograph ofa tumor vessel with two endothelialgaps (arrows ). Basement membraneis attenuated and incomplete in the regionof the upper gap. Bar, 0.5 Am (C ).
Ultrastructure of Tumor Vessel Defects
www.aacrjournals.org 5747 Cancer Res 2005; 65: (13). July 1, 2005
Research. on June 5, 2020. © 2005 American Association for Cancercancerres.aacrjournals.org Downloaded from
in CD31/CD105-negative regions included endothelial detach-ment, openings between endothelial cells, and missing endothelialcells. Although basement membrane was present in most of thevessels in the LS174T tumors, 80% of the vessels with regionslacking detectable CD31/CD105 staining also lacked one or morebasement membrane components. Further studies are needed toelucidate the mechanisms responsible for these abnormalities andto assess their progression.
Acknowledgments
Received 12/21/2004; revised 3/1/2005; accepted 4/12/2005.Grant support: U.S. NIH grants P01-CA80124 (to L.L. Munn and R.K. Jain), R01-
CA82923, and P50-CA90270 from the National Cancer Institute, P01-HL24136, andR01-HL59157 from the National, Heart, Lung, and Blood Institute, and funding fromAngelWorks Foundation and the Vascular Mapping Project (to D. McDonald).
The costs of publication of this article were defrayed in part by the payment of pagecharges. This article must therefore be hereby marked advertisement in accordancewith 18 U.S.C. Section 1734 solely to indicate this fact.
We thank Sylvie Roberge for her technical help with animal surgery.
Table 1. Defects in CD31/CD105 and basement membrane staining in blood vessels of LS174T tumors
No. of vessels Complete CD31/CD105
staining? % (no. of vessels)
Basement membrane
staining (+/�)
% of vessels
(no. of vessels)
Orthotopic tumors*
118 no: 12% (14) col IV� 86% (12)col IV+ 14% (2)
yes: 88% (104) col IV� 16% (17)
col IV+ 84% (87)108 no: 9% (10) lam� 80% (8)
lam+ 20% (2)
yes: 91% (98) lam� 4% (4)
lam+ 96% (94)Ectopic tumors*
107 no: 24% (26) col IV� 88% (23)
col IV+ 12% (3)
yes: 76% (81) col IV� 2% (2)col IV+ 98% (79)
83 no: 24% (20) lam� 95% (19)
lam+ 5% (1)
yes: 76% (63) lam� 8% (5)lam+ 92% (58)
*Data from immunohistochemically stained sections of six orthotopic tumors and three ectopic tumors analyzed by confocal microscopy. col IV,
collagen IV; lam, laminin. Similar results were obtained for nidogen and perlecan staining.
References1. Winkler F, Kozin SV, Tong RT, et al. Kinetics ofvascular normalization by VEGFR2 blockade governsbrain tumor response to radiation: role of oxygenation,angiopoietin-1 and matrix metalloproteinases. CancerCell 2004;6:553–63.
2. Warren BA, Shubik P. The growth of the blood supplyto melanoma transplants in the hamster cheek pouch.Lab Invest 1966;15:464–78.
3. Hammersen F, Endrich B, Messmer K. The finestructure of tumor blood vessels. I. Participation ofnon-endothelial cells in tumor angiogenesis. Int JMicrocirc Clin Exp 1985;4:31–43.
4. Hashizume H, Baluk P, Morikawa S, et al. Openingsbetween defective endothelial cells explain tumor vesselleakiness. Am J Pathol 2000;156:1363–80.
5. Jain RK, Booth MF. What brings pericytes to tumorvessels? J Clin Invest 2003;112:1142–51.
6. Morikawa S, Baluk P, Kaidoh T, Haskell A, Jain RK,McDonald DM. Abnormalities in pericytes on bloodvessels and endothelial sprouts in tumors. Am J Pathol2002;160:985–1000.
7. Baluk P, Morikawa S, Haskell A, Mancuso M,McDonald DM. Abnormalities of basement membraneon blood vessels and endothelial sprouts in tumors. AmJ Pathol 2003;163:1801–15.
8. Chang YS, diTomaso E, McDonald DM, Jones RC,Jain RK, Munn LL. Mosaic blood vessels in tumors:
frequency of cancer cells in contact with flowing blood.Proc Natl Acad Sci U S A 2000;97:14608–13.
9. Baluk P, Hashizume H, McDonald DM. Cellularabnormalities of blood vessels as targets in cancer. CurrOpin Genet Dev 2005;15:102–11.
10. Jain RK. Normalizing tumor vasculature with anti-angiogenic therapy: a new paradigm for combinationtherapy. Nat Med 2001;7:987–9.
11. Jain RK. Normalization of tumor vasculature: Anemerging concept in anti-angiogenic therapy. Science2005;307:58–62.
12. Patan S, Tanda S, Roberge S, Jones RC, Jain RK,Munn LL. Vascular morphogenesis and remodeling in ahuman tumor xenograft. Blood vessel formation andgrowth after ovariectomy and tumor implantation. CircRes 2001;89:732–9.
13. Kristjansen PE, Roberge S, Lee I, Jain RK. Tissue-isolated human tumor xenografts in athymic nude mice.Microvasc Res 1994;48:389–402.
14. Feng D, Nagy JA, Pyne K, Dvorak HF, Dvorak AM.Ultrastructural localization of platelet endothelial celladhesion molecule (PECAM-1, CD31) in vascularendothelium. J Histochem Cytochem 2004;52:87–101.
15. Seon BK, Matsuno F, Haruta Y, Kondo M, Barcos M.Long-lasting complete inhibition of human solid tumorsin SCID mice by targeting endothelial cells of tumorvasculature with antihuman endoglin immunotoxin.Clin Cancer Res 1997;3:1031–44.
16. Kumar S, Ghellal A, Li C, et al. Breast carcinoma:
vascular density determined using CD105 antibodycorrelates with tumor prognosis. Cancer Res 1999;59:856–61.
17. Jones R. Ultrastructural analysis of contractile celldevelopment in lung microvessels in pulmonary hyper-tension. Fibroblasts and intermediate cells selectivelyreorganize nonmuscular segments. Am J Pathol 1992;141:1491–505.
18. Jones R, Steudel W, White S, Jacobson M, Low R.Microvessel precursor cells express head-insertedsmooth muscle myosin heavy chain (SM-B) isoform inhyperoxic pulmonary hypertension. Cell Tissue Res 1999;295:453–65.
19. Sundberg C, Nagy JA, Brown LF, et al. Glomeruloidmicrovascular proliferation follows adenoviral vascularpermeability factor/vascular endothelial growth factor-164 gene delivery. Am J Pathol 2001;158:1145–60.
20. Inai T, Mancuso M, Hashizume H, et al. Inhibition ofvascular endothelial growth factor (VEGF) signaling incancer causes loss of endothelial fenestrations, regres-sion of tumor vessels, and appearance of basementmembrane ghosts. Am J Pathol 2004;165:35–52.
21. Jain RK. Molecular regulation of vessel maturation.Nat Med 2003;9:685–93.
22. Munn LL. Aberrant vascular architecture in tumorsand its importance in drug-based therapies. DrugDiscov Today 2003;8:396–403.
23. Hobbs SK, Monsky WL, Yuan F, et al. Regulation oftransport pathways in tumor vessels: role of tumor type
Cancer Research
Cancer Res 2005; 65: (13). July 1, 2005 5748 www.aacrjournals.org
Research. on June 5, 2020. © 2005 American Association for Cancercancerres.aacrjournals.org Downloaded from

and microenvironment. Proc Natl Acad Sci U S A 1998;95:4507–12.
24. Pettersson A, Nagy J, Brown L, et al. Heterogeneityof the angiogenic response induced in differentnormal adult tissues by vascular permeability factor/vascular endothelial growth factor. Lab Invest 2000;80:99–115.
25. Leach L, Eaton BM, Westcott ED, Firth JA. Effect ofhistamine on endothelial permeability and structureand adhesion molecules of the paracellular junctions ofperfused human placental microvessels. Microvasc Res1995;50:323–37.
26. Raab M, Daxecker H, Markovic S, Karimi A,Griesmacher A, Mueller MM. Variations of adhesionmolecule expression on human umbilical vein endothe-lial cells upon multiple cytokine application. Clin ChimActa 2002;321:11–6.
27. Watts ME, Parkins CS, Chaplin DJ. Influence ofhypoxia on tumour-conditioned medium on endothelial
cell adhesion molecule expression in vitro . AnticancerRes. 2002;22:953–8.
28. Holash J, Maisonpierre P, Compton D, et al. Vesselcooption, regression, and growth in tumors mediated byangiopoietins and VEGF. Science 1999;284:1994–8.
29. Sephel GC, Kennedy R, Kudravi S. Expression ofcapillary basement membrane components duringsequential phase of wound angiogenesis. Matrix Biol1996;15:263–79.
30. Yuan F, Salehi HA, Boucher Y, Vasthare US,Tuma RF, Jain RK. Vascular permeability and micro-circulation of gliomas and mammary carcinomastransplanted in rat and mouse cranial windows.Cancer Res 1994;54:4564–8.
31. Fukumura D, Yuan F, Monsky WL, Chen Y, Jain RK.Effect of host microenvironment on the microcircula-tion of human colon adenocarcinoma. Am J Pathol 1997;151:679–88.
32. Sood AK, Fletcher MS, Zahn CM, et al. The clinical
significance of tumor cell-lined vasculature in ovariancarcinoma: implications for anti-vasculogenic therapy.Cancer Biol Ther 2002;1:661–4.
33. Rybak SM, Sanovich E, Hollingshead MG, et al.‘‘Vasocrine’’ formation of tumor cell-lined vascularspaces: implications for rational design of antiangio-genic therapies. Cancer Res 2003;63:2812–9.
34. Klement G, Baruchel S, Rak J, et al. Continuous low-dose therapy with vinblastine and VEGF receptor-2antibody induces sustained tumor regression withoutovert toxicity. J Clin Invest 2000;105:R15–24.
35. Man S, Bocci G, Francia G, et al. Antitumor effects inmice of low-dose (metronomic) cyclophosphamideadministered continuously through the drinking water.Cancer Res 2002;62:102731–5.
36. Browder T, Butterfield CE, Kraling BM, et al.Antiangiogenic scheduling of chemotherapy improvesefficacy against experimental drug-resistant cancer.Cancer Res 2000;60:1878–88.
Ultrastructure of Tumor Vessel Defects
www.aacrjournals.org 5749 Cancer Res 2005; 65: (13). July 1, 2005
Research. on June 5, 2020. © 2005 American Association for Cancercancerres.aacrjournals.org Downloaded from

2005;65:5740-5749. Cancer Res Emmanuelle di Tomaso, Diane Capen, Amy Haskell, et al. Focal Regions Lacking Endothelial Cell MarkersMosaic Tumor Vessels: Cellular Basis and Ultrastructure of
Updated version
http://cancerres.aacrjournals.org/content/65/13/5740
Access the most recent version of this article at:
Cited articles
http://cancerres.aacrjournals.org/content/65/13/5740.full#ref-list-1
This article cites 35 articles, 9 of which you can access for free at:
Citing articles
http://cancerres.aacrjournals.org/content/65/13/5740.full#related-urls
This article has been cited by 13 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. (CCC)Click on "Request Permissions" which will take you to the Copyright Clearance Center's
.http://cancerres.aacrjournals.org/content/65/13/5740To request permission to re-use all or part of this article, use this link
Research. on June 5, 2020. © 2005 American Association for Cancercancerres.aacrjournals.org Downloaded from