mri tmj temporo mandibular jiont dr ahmed esawy
TRANSCRIPT

بسم هللا الرحمن الرحيم
Dr Ahmed Esawy

RADIOLOGY CHANNEL
IMAGING ORAL BOARD
MRI
TEMPOROMANDIBULAR
JIONT TMJ
Dr Ahmed Esawy

Dr. Ahmed Abdallah Eisawy
MBBS M.Sc MD
Dr Ahmed Esawy

TEMPROMANDIBULAR JOINT
Dr Ahmed Esawy

TMJ: is a bilateral joints permits the mandible to move as a unit with two functional patterns:
• Hinge (inferior portion) • Translation (superior portion)
(ginglymoarthroidal joint) (compound joint)
it has four anatomical parts: 1- condyle 2- articular fossa 3- articular disc 4- articular capsule
Dr Ahmed Esawy

Plain Radiography • Transcranial lateral
Projection
• Submento-vertex view: – Condylar morphology.
– Relative condylar position to the horizontal baseline.
– Mandibular asymmetry.
• Postero-anterior view – Condylar morphology
– Mandibular deviation.
Dr Ahmed Esawy

Conventional Tomography
• Lateral Tomography – Shows condylar location in closed and open mouth
– Assesses condylar morphology: size, sclerosis, erosion, etc…
– Relative size & shape of the glenoid fossa.
• High radiation dose to the eye lens.
• Has been replaced by CT
Dr Ahmed Esawy

Normal Anatomy Mandibular condyle (head)
Glenoid fossa
Articular tubercle (eminence)
Dr Ahmed Esawy

Computed Tomography
• Axial & coronal 1-2mm slice thickness
• Sagittal reconstruction is made through the condyle
3D reconstruction may be helpful to evaluate positional relationships between the joint components
Dr Ahmed Esawy

• MR imaging: modality of choice; with dedicated
surface coils
• Conventional radiology: trauma
• Multisection CT: jaw trauma & concomitant osseous
injuries
• Sonography: internal derangement & inflammation;
with interobserver variability
• Arthrography: replaced by MRI
Dr Ahmed Esawy

MR Imaging
• Protocol: (1.5T)
– STIR replaced T1WI+FS+C
☆ Oblique sagittal— T1 (close+open), T2 (open)
Oblique coronal— T1WI
Dr Ahmed Esawy

• Parasagittal & paracoronal views: angulated
perpendicular & parallel to the axis of the
mandibular condyle
Dr Ahmed Esawy

MRI • Technique & Equipment:
– Oblique sagittal PD are usually obtained in closed and open mouth positions.
– Coronal images may be needed when a meniscus is suspected to be displaced far medially or laterally.
– T2 WI are useful for detection of joint effusion.
Dr Ahmed Esawy

• The disk is firmly attaching to the capsule and the
condular neck medially and laterally
• Attached to the superior part of the pterygoid
muscle anteromedially
Dr Ahmed Esawy

• Drawing illustrates the anatomy of the TMJ.
• 1 = condyle; 2 = temporal bone, articular eminence;
• 3 = temporal bone, mandibular fossa; 4 = disk, anterior band; 5 = disk, intermediate
zone; 6 = disk, posterior band; 7 = superior retrodiskal layer;
• 8 = inferior retrodiskal layer; 9 =vasculonervous structures10 =capsular superior
attachment 11 = capsular inferior attachment 12 = superior joint space;
• 13 = inferior joint space 14 = superior head of the lateral pterygoid muscle (LPM)
15 = inferior head of the LPM 16 = interpterygoid space; 17 = external auditory
canal
Dr Ahmed Esawy

Temporomandibular disk (sagittal)
1. Anterior band
2. Posterior band
3. Intermediate zone (inconstant central water signal intensity)
4. Anterior attachment
5. Posterior attachment (bilaminar zone)
A P
Dr Ahmed Esawy
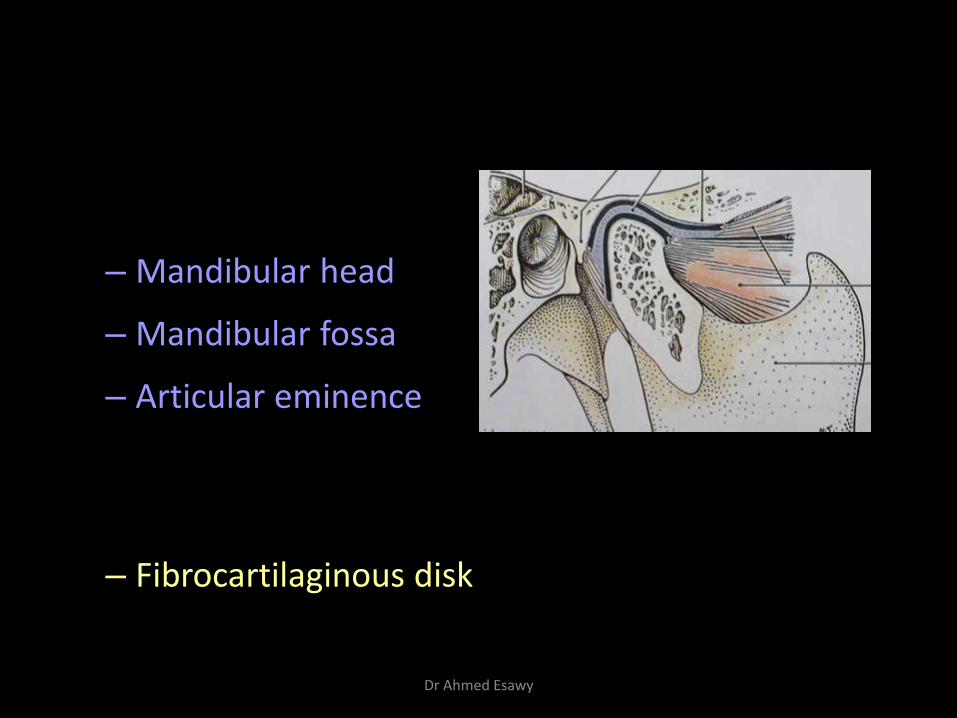
Anatomy & Biomechanics
• TMJ
– Mandibular head
– Mandibular fossa
– Articular eminence
– Hyaline cartilage covers the articulating cortical
bone
– Fibrocartilaginous disk: bow-tie shaped, biconcave
morphology
Dr Ahmed Esawy

Temporomandibular Disk
• Anterior and posterior bands: longer in the
mediolateral than in the anteroposterior dimension
• Anterior band: smaller, attaches to articular
eminence, condylar head, & joint capsule
• Posterior band: blends with highly vascularized, loose
connective tissue, the bilaminar zone, and the
capsule
Dr Ahmed Esawy

The meniscus consists of anterior band, thin intermediate zone and a
thicker posterior band.
Posteriorly, the meniscus is attached to the bilaminar zone which
contain a rich vascular bed and neural elements supplying the
meniscus.
Anteriorly it is attached to the lateral pterygoid muscle.
Intermediate
zone
Posterior
band Anterior
band
Bilaminar
zone
lateral
pterygoid
An integral part of the joint
is the meniscus. It is a
fibrocartilagenous saddle shaped
structure that divides the joint into
separate upper and lower
compartments, each lined by a
synovial membrane.
Dr Ahmed Esawy

Dr Ahmed Esawy

Dr Ahmed Esawy

Disk Evaluation
• The meniscus of the TMJ is a biconcave fibrocartilaginous structure located between the mandibular condyle and the temporal bone component of the joint.
• Its function is to accommodate a hinging action as well as the gliding action that occurs between the temporal bone and the mandible.
• The disk is round to oval, with a thin center (intermediate zone) that separates thicker peripheral portions known as the anterior and posterior bands
Dr Ahmed Esawy

Physiologic Joint (closed mouth)
• The disc positioned between the mandibular head
inferiorly and the articular eminence anteriorly and
superiorly
• The posterior band lies within 10˚ of the 12 o’clock
position
• The medial and lateral corners of the disk align with the
condylar borders and do not bulge laterally or medially
Dr Ahmed Esawy

Closed mouth position (sagittal projection)
The posterior band lies within 10˚(anteriorly) of the 12 o’clock (posteriorly) position
Dr Ahmed Esawy

Closed mouth view (sagittal)
1. Mandibular head
2. Articular eminence
3. Disk
4. Bilaminar zone
5. Lateral pterygoid muscle with interposed fat tissue (5a, superior head; 5b, inferior head)
6. Superior joint space
7. Inferior joint space Dr Ahmed Esawy

Closed mouth view (coronal)
1. Mandibular head
2. Articular fossa
3. Disk
4. Medial attachment
5. Lateral attachment
6. Superior joint space
7. Inferior joint space
8. Lateral pterygoid muscle
Dr Ahmed Esawy

Physiologic Joint (open mouth)
• The disk slides into a position between the madibular
head and articular eminence
• The loose tissue of the bilaminar zone allows the
remarkable range of motion
• The attachments of the disk prevent luxation during
opening
• The disk does not move in the coronal plane when
the joint is intact
Dr Ahmed Esawy

Open mouth view (sagittal)
1. Mandibular head
2. Articular eminence
3. Superior joint space
4. Inferior joint space
5. Disk
6. Bilaminar zone
7. Lateral pterygoid muscle with interposed fat tissue
Dr Ahmed Esawy

Open position of normal TMJ
a— sagittal; b— coronal
1. Mandibular head
2. Articular eminence
3. Disk
4. Bilaminar zone
5. Lateral pterygoid muscle
Dr Ahmed Esawy

• Sagittal oblique spin-echo T1-weighted magnetic resonance (MR) image obtained in the closed-mouth position shows the normal TMJ.
Dr Ahmed Esawy

When the mouth closes:
The head of mandible sits in the fossa at rest,
thick posterior band of the meniscus lies
immediately above the condyle
When the mouth opens:
two distinct motions occur at the joint:
The first motion is rotation around a horizontal axis through the condylar heads
The second motion is anterior translation. The condyle and meniscus (by the contraction of lateral pterygoid) move together anteriorly beneath the articular eminence
Dr Ahmed Esawy

Closed position of normal TMJ
a— sagittal; b— coronal
1. Mandibular head
2. Articular fossa
3. Disk
4. Bilaminar zone
5. Lateral pterygoid muscle
Dr Ahmed Esawy

Drawings illustrate TMJ function. (a) Initial closed-mouth position. (b) At the beginning of the open-mouth position, the digastric muscle forces the condyle downward. The condyle then rotates in the lower joint space, and condylar displacement begins when the jaw is opened beyond 20–25 mm. Retrodiskal ligaments stabilize the disk.
(c) Condylar protraction (maximum open-mouth position). Involvement of the inferior LPM is basic to this step, and the superior LPM can displace the disk, probably to maintain joint congruence. The superior retrodiskal layer prevents complete abnormal displacement. (d) Progression to the maximum clenching position. The inferior LPM is normally very active in this phase as well.
Dr Ahmed Esawy

• Superior belly of lateral pterygoid musle
– Originates from the greater sphenoid wing and inserts on the the disk
– Plays a key role in upholding the physiologic position of the disk as it pulls the disk forward when the jaw is opened
Dr Ahmed Esawy

sagittal MR imaging
• the meniscus appears as a biconcave structure with homogeneous low signal intensity
• the bilaminar zone demonstrates intermediate signal intensity.
• The posterior band and retrodiskal tissue are best depicted in the open-mouth position , slightly hyperintense, more frequently hypointense in patients with disk disease
• Typically, the anterior band and the intermediate zone are hypointense , lies immediately in front of the condyle and the junction of the bilaminar zone
Dr Ahmed Esawy

• Morphologic features of the normal disk. (a) On a sagittal oblique gradient-echo T2-weighted MR image (closed-mouth position), the anterior and posterior bands are thick and the intermediate zone (arrow) is thin, creating a biconcave disk shape.
(b) Sagittal oblique gradient-echo T2-weighted MR image (open-mouth position) more clearly depicts the posterior band and retrodiskal tissue (arrow). These anatomic entities are best depicted in the open-mouth position.
Dr Ahmed Esawy

MRI
• MRI of normal TMJ: – Disc Biconcave
– Posterior band superior to the condyle
– In open mouth: • Thin zone lies between condyle &
tubercle
• Posterior band articulates against posterior surface of the condyle
Dr Ahmed Esawy

Dr Ahmed Esawy

Lateral pterygoid muscle raphe
Lower head of lateral pterygoid muscle
Anterior band of articular disc
Mandibular condyle (head)
Posterior band of articular disc
Posterior disc attachment
Dr Ahmed Esawy

Mandibular condyle (head)
Articular disc
Dr Ahmed Esawy
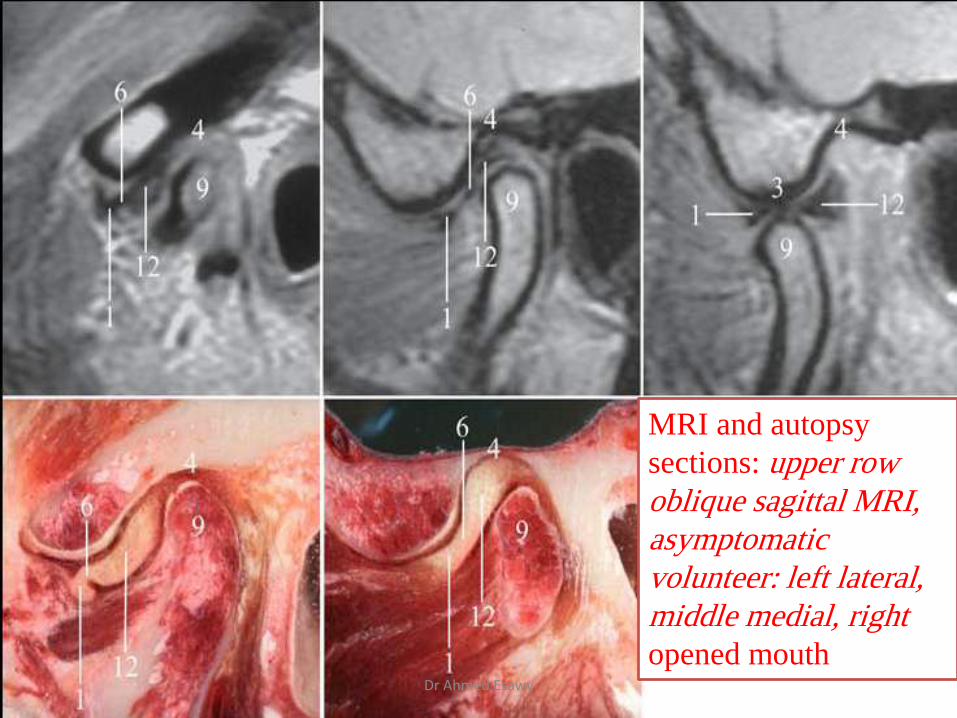
MRI and autopsy
sections: upper row
oblique sagittal MRI,
asymptomatic
volunteer: left lateral,
middle medial, right
opened mouth Dr Ahmed Esawy

Retrodiskal layers
• retrodiskal layers (superior and inferior) and vasculonervous structures constitute an anatomic area called retrodiskal tissue, or the bilaminar zone. The inferior retrodiskal layer is made up of collagen fibers, and the superior retrodiskal layer consists of elastic fibers
• These retrodiskal layers play an important role in normal disk displacement.
• Improvements in MR imaging currently allow detailed depiction of these structures and related pathologic changes. Rupture of superior retrodiskal layer fibers may produce significant disk instability.
Dr Ahmed Esawy

• Normal retrodiskal tissue.
• (a) Sagittal oblique gradient-echo T2-weighted MR image (closed-mouth position) clearly depicts the retrodiskal layers (arrow). These structures play an important role in normal disk movement and can easily be visualized at MR imaging.
• (b) Sagittal oblique spin-echo proton-density–weighted MR image (open-mouth position) shows the superior retrodiskal layer (arrow) between the posterior band and the mandibular fossa.
Dr Ahmed Esawy

Temporomandibular Joint Disk Position Assessed at Coronal
MR Imaging
Dr Ahmed Esawy

• (a, b) Schematic illustrations of left TMJ measurements in (a) closed-mouth and (b) opened-mouth positions. a = longest mediolateral distance of condyle, b = line perpendicular to a and tangential to condyle, c = line parallel to b and tangential to disk, = distance between b and c at lateral aspect of joint, = distance between b and c at medial aspect of joint, l = lateral, m = medial.
Dr Ahmed Esawy

• Two-dimensional coronal oblique of TMJ in closed-mouth position in 20-year-old female . Both the medial (left *) and the lateral (right *) edges of the TMJ disk are medial to the condyle (c).
Dr Ahmed Esawy

• Two-dimensional coronal oblique MR of TMJ in opened-mouth position in female Both the medial edge (black *) and the lateral edge (white *) are medial to the condyle (c). These findings combined with those in emphasize the medial shift of the TMJ disk.
Dr Ahmed Esawy

Age changes of theTMJ:
1- Flattened condyle
2- osteoporosis of the condyle bone.
3- Thickning of the fibrous covering of the condyle.
4- Thinning of the cartilagenous zone of condyle.
5- Thinning of the disc
6- Fibrotic synovial folds
7- Thickening of the b.v. walls
8- Decrease the number of nerves
Dr Ahmed Esawy

Disorders of the TMJ: 1- limitation of movement: - temporary - permanent 2- dislocation 3- pain 4- hyperplasia 5- neoplasm 6- loose bodies in the TMJ
Dr Ahmed Esawy

These age changes lead to:
-Decrease in the synovial fluid formation
-Impairment of motion due to decrease in the disc and capsule extensibility
-Decrease the resilience during mastication due to chondroid changes into collagenous elements
-Dysfunction in older people
Dr Ahmed Esawy

patients of TMJ disease divided into 3 groups according severity of clinical manifestation and we found that: Group I. EARLY cases who presented with painless clicking with No restricted motion. Group II. INTERMEDIATE group who presented with frequent pain, joint tenderness, headaches, locking restricted motion and painful chewing. Group III. LATE cases who presented with trismus, joint crepitus and marked chronic pain. Clinical manifestations were evaluated and registered and were correlated to the degree of ADD in MRI.
Dr Ahmed Esawy

• Category 0 (Normal disc position)
• Category I (Partial anterior disc displacement with reduction (PADDWR))
• Category II (Partial anterior disc displacement without reduction (PADDWOR))
• Category III (Complete anterior disc displacement with reduction (CADDWR))
• Category IV (Complete anterior disc displacement without
reduction (CADDWOR))
According to the degree of anterior disk displacment (ADD) our series was classified into 4 categories
Dr Ahmed Esawy

• Category 0
• Normal disc position (the thin intermediate zone interposed between the condyle and the adjacent temporal bone, wherever the two bones are most closely apposed to one another regardless of whether or not the mouth was open or closed)
Dr Ahmed Esawy

Dr Ahmed Esawy
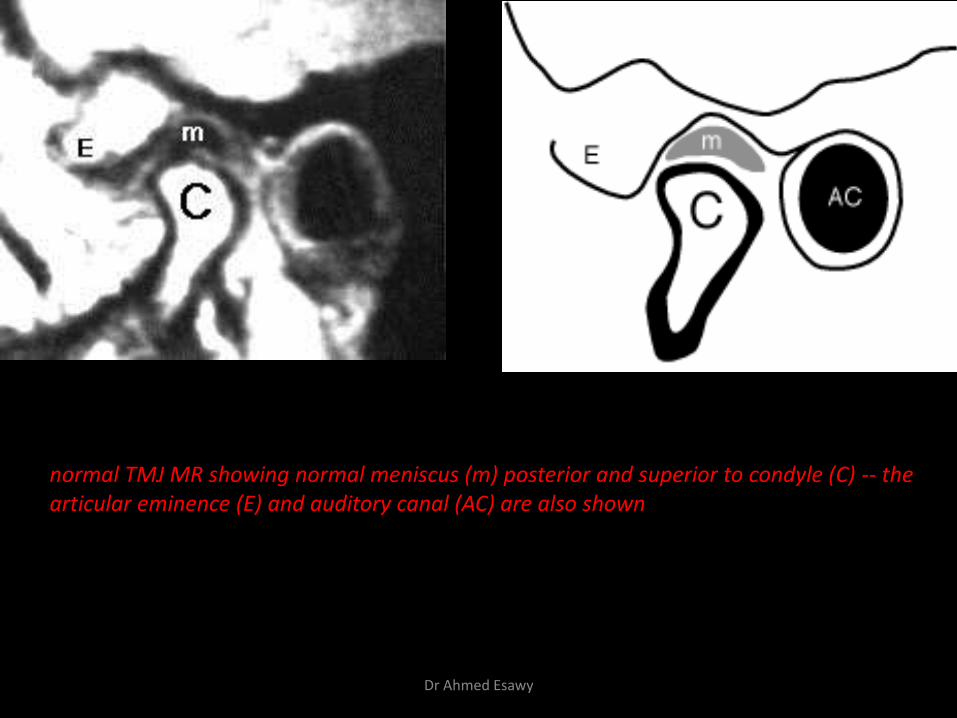
normal TMJ MR showing normal meniscus (m) posterior and superior to condyle (C) -- the articular eminence (E) and auditory canal (AC) are also shown
Dr Ahmed Esawy

Drawing of normal temporomandibular joint showing normal relationship between temporal fossa, disk, and mandibular condyle. (A) A closed-mouth sagittal image shows mandibular
condyle articulating with temporal fossa. The disk is at the 11 o'clock position.
(B) An open-mouth sagittal image illustrates normal translation of disk and condyle. The condyle is positioned at the apex of the articular eminence
Dr Ahmed Esawy

T1-Weighted sagittal magnetic resonance images in (a) closed- and (b) open-mouth positions showing normal disc positions (arrows)
Dr Ahmed Esawy

A 20-year-old woman with a normal temporomandibular joint. (A) A closed-mouth sagittal T1-weighted image
shows a normal relationship of the mandibular condyle (large arrow), the disk (small arrow) at the 11 o'clock position, the temporal fossa (arrowhead), and the articular eminence (curved arrow).
(B) Open-mouth sagittal T1-weighted image shows normal translation of the disk (small arrow) and condyle (large arrow) at the apex of the articular eminence (arrowhead).
Dr Ahmed Esawy

Sagittal oblique spin-echo proton-density–weighted MR image (closed-mouth position) shows the disc in its normal position between the condyle and temporal bone and centred in the intermediate zone (arrow).
Sagittal oblique spin-echo proton-density–weighted MR image (open-mouth position) shows that the disc has maintained its normal position during condylar movement (arrow).
Dr Ahmed Esawy

• Category I: Partial anterior disc displacement with reduction (PADDWR); disc displaced anteriorly in closed mouth up to the posterior band interposed between the two most closely apposed cortical bone surfaces of the condyle and eminence with disc reduction to normal location in open mouth position
Dr Ahmed Esawy

Sagittal oblique spin-echo proton-density–weighted MR image (closed-mouth position) shows partial anterior disc displacement with intermediate signal of degeneration (large arrow) and anterior osteophyte of the condyle (small arrow).
Sagittal oblique spin-echo proton-density–weighted MR image (open-mouth position) shows that the disc has maintained its normal position during condylar movement (arrow).
Dr Ahmed Esawy

Internal Derangements
• General orthopedic term implying a mechanical fault that interferes with the smooth action of a joint
• The most common internal derangement is disc displacement
Clinical Features
• Clicking sounds from joint (s)
• Restricted or normal mouth opening capacity
• Deviation on opening
• Pain
Dr Ahmed Esawy

Disk Displacement
Unidirectional multidirectional
Vertical axis Anterior posterior
transverse axis medial lateral
Antero-lateral Antero-medial Postero-lateral Postero-medial
anterior displacement with reduction.
anterior displacement without reduction.
Dr Ahmed Esawy

Disk Displacement
• May be uni- or multidirectional
– Unidirectional anterior and multidirectional anterolateral and
anteromedial displacements are the most common type
– Unidirectional transverse and posterior displacements are rare
Dr Ahmed Esawy

• Assessment of disk position
– Both sagittal and coronal images
– The jaw is firstly assessed in the closed position
• Whether displaced disks relocate to a physiologic
position during jaw opening or stay displaced is an
important issue in the grading and prognosis
– Stay displaced: more likely to develop disk degeneration
and rupture
– Disc may have normal (biconcave) or deformed morphology
Dr Ahmed Esawy

Unidirectional Disk Displacement
• Anterior & posterior disk displacements are diagnosed
on sagittal images by using the position of posterior
band as a discriminator
– Posterior band is ventral to the 11 clock position
– Posterior displacment when posterior band is
displaced posteriorly and exceeds 1 o'clock position
• Medial and lateral displacements: the coronal plane
– Normally do not extend beyond the border of the
condylar head. Bulging disk displacement
Dr Ahmed Esawy

• Partial displacement— the disk continues to stay in contact with the regular articular surface of the condylar head . lower prevalence of symptoms than full displacement
• Complete displacement— the relationship lost
findings Direction of displacment
Posterior band is ventral to the 11 clock position
Anterior disk displacment
Posterior band is dorsal to the 13 (1) clock position
posterior disk displacment
Medial attachment and disk bulge medial to the medial border of the mandibular head
medial disk displacment
Lateral attachment and disk bulge lateral to The lateral border of the mandibular head
lateral disk displacment
Dr Ahmed Esawy

• Drawings (sagittal oblique views) illustrate disk displacement in the closed-mouth position. (a) A pathologic condition is considered to be present if the angle between the posterior band and the vertical orientation of the condyle (twelve o’clock position) exceeds 10°.
(b)recommendation that anterior disk displacement of up to 30° be considered normal to better correlate disk displacement with clinical symptoms of TMJ dysfunction.
Dr Ahmed Esawy

displaced meniscus anteriorly (arrows, m) anterior to the condyle (C) and auditory canal (AC) and beneath the articular eminence (E)
Dr Ahmed Esawy

Indirect signs of internal derangement include large joint effusion rupture of retrodiscal layers thickening of lateral pterygoid muscle attachment osteoarthritic changes.
Dr Ahmed Esawy

Category II: Partial anterior disc displacement without reduction (PADDWOR) disc displaced anteriorly in closed mouth as described in category I, that maintained displaced with mouth opening
Dr Ahmed Esawy

Sagittal oblique spin-echo proton-density–weighted MR image (closed-mouth position) shows (flattened shape) partial anterior disc displacement (arrow).
Sagittal oblique spin-echo proton-density–weighted MR image (open-mouth position) shows that the disc remains partially displaced from its normal location (arrow), associated with Grade I joint effusion.
Dr Ahmed Esawy
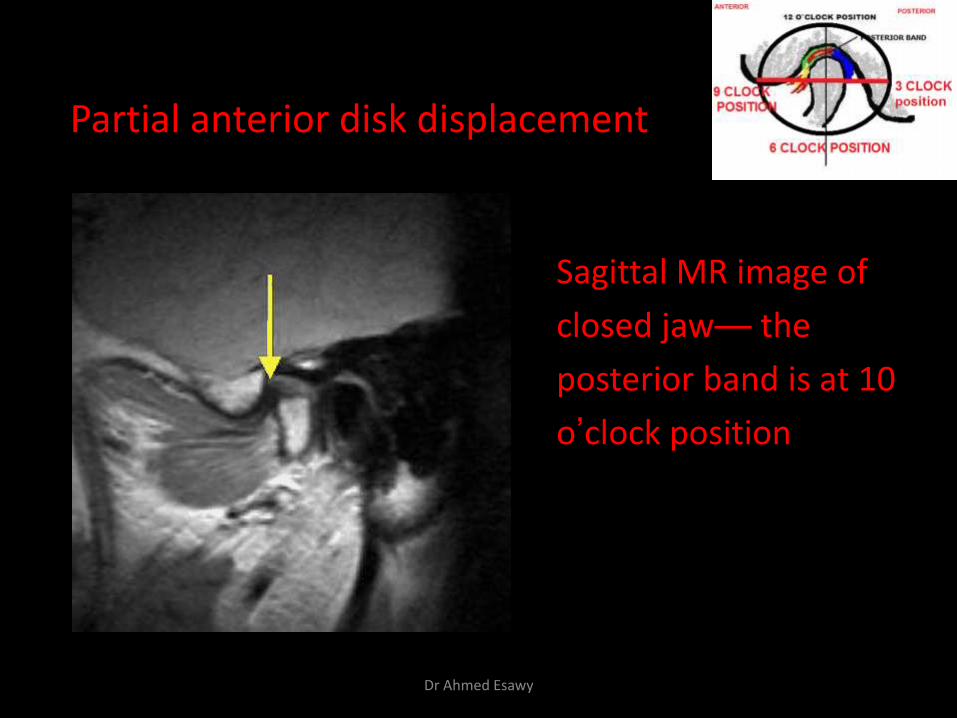
Partial anterior disk displacement
Sagittal MR image of
closed jaw— the
posterior band is at 10
o’clock position
Dr Ahmed Esawy

lateral sections central sections open-mouth
Partial anterior disc displacement at baseline
Dr Ahmed Esawy

• (a) closed-mouth position) shows a disk (arrow) in its normal position between the condyle and temporal bone and centered in the intermediate zone.
(b) (open-mouth position) shows that the disk (arrow) returns back has maintained its normal position during condylar movement. This interposition of the disk prevents abnormal contact between osseous joint surfaces.
Normal disk mobility
Dr Ahmed Esawy

Internal Derangement
• anterior displacement when the mouth is closed, the meniscus is sandwitched between the anterior aspect of condyle (anterior to the superior portion of the condyle ) and the eminence.
• When the mouth is opened the displaced posterior band will usually return to its normal position as the condyle reaches a certain point. This is termed anterior displacement with reduction.
In opened mouth position disc may be in a normal position (“with reduction”) or continue to be displaced (“without reduction”)
Dr Ahmed Esawy

Category III: Complete anterior disc displacement with reduction (CADDWR); disc displaced anteriorly in closed mouth up to no disc substance interposed between the two most closely apposed cortical bone surfaces of the condyle and eminence with disc reduction to normal location in open mouth position
Dr Ahmed Esawy

Sagittal oblique spin-echo proton-density–weighted MR image (closed-mouth position) shows (thickened shape) complete anterior disc displacement (arrow) and associated joint effusion in both upper and lower joint recesses.
Sagittal oblique spin-echo proton-density–weighted MR image (open-mouth position) shows that the disc (arrow) has maintained its normal position during condylar movement.
Dr Ahmed Esawy

• Anterior disk displacement with reduction.
(open-mouth position) shows that the disk (arrow) has returned to its normal position between the condyle and the temporal bone. This return movement generally produces a clicking or popping noise
(a) Sagittal oblique gradient-echo T2-weighted MR image (closed-mouth position) shows an anteriorly displaced disk (arrow).
Sagittal T2
Dr Ahmed Esawy

• Disk displacement with reduction:
posterior posterior
Dr Ahmed Esawy

T1-Weighted sagittal magnetic resonance images in (a) closed- and (b) open-mouth positions showing anterior disc displacement with reduction (arrows)
Dr Ahmed Esawy

Category IV: Complete anterior disc displacement without reduction (CADDWOR) disc displaced anteriorly in closed mouth as described in category III, that maintained displaced with mouth opening
Dr Ahmed Esawy

Sagittal oblique spin-echo proton-density–weighted MR image (closed-mouth position) shows complete anterior disc displacement (arrow).
Sagittal oblique spin-echo proton-density–weighted MR image (open-mouth position) shows that the disc remains displaced from its normal location (arrow) and cortical erosion of the condyle (small arrow). Note the marked restricted mobility of the condyle apex where it translates to less than the apex of the articular eminence.
Dr Ahmed Esawy

• Anterior disk displacement without reduction.
(b) the open-mouth position, the disk (arrow) remains displaced from its normal location
(a) (closed-mouth position) shows a disk (arrow) displaced from its normal location.
Sagittal T2-
Dr Ahmed Esawy

• Disk displacement without reduction:
Dr Ahmed Esawy

T1-Weighted sagittal magnetic resonance images in (a) closedand (b) open-mouth positions showing anterior disc displacement without reduction (arrows)
Dr Ahmed Esawy

Unidirectional complete anterior disk displacement
Sagittal MR image with
the jaw closed—
• Disk deformity
• Condyle deformity
due to OA changes
Dr Ahmed Esawy

Complete anterior disc displacement
Open-mouth MRI medial section Autopsy
Dr Ahmed Esawy

Multidirectional Disk Displacement
• Combination of signs of unidirectional disk displacement
• Careful interpretation of sagittal and coronal images
• Impossibility of identifying the complete disk in a single
coronal or sagittal image
Dr Ahmed Esawy
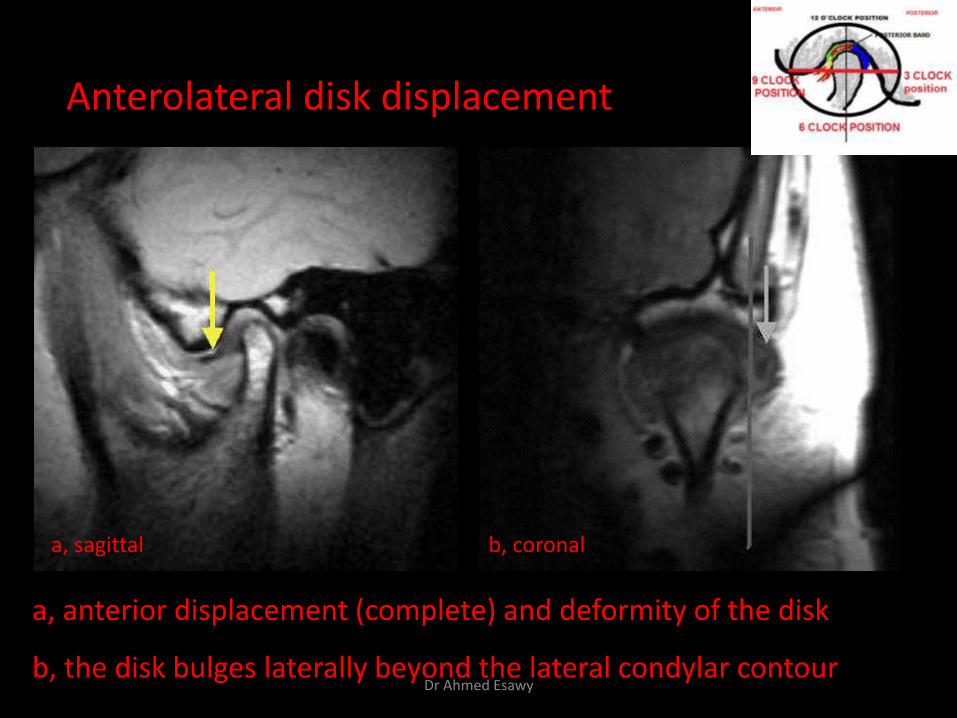
Anterolateral disk displacement
a, sagittal b, coronal
a, anterior displacement (complete) and deformity of the disk
b, the disk bulges laterally beyond the lateral condylar contour Dr Ahmed Esawy

Sagittal T1-weighted magnetic resonance image in open-mouth position shows condylar hypermobility (white arrow) and posterior displacement of articular disc (black arrow)
Dr Ahmed Esawy

Posterior disc displacement
posterior
posterior
Dr Ahmed Esawy

Normal disc morphology is biconcave structure in sagittal images with homogenous low signal intensity. Disc deformities including thickening , irregularity , flattening, folded , degeneration , and perforation were reported
Disc morphology
Dr Ahmed Esawy

Sagittal oblique spin-echo proton-density–weighted MR images (closed-mouth position) show abnormal disc morphology: (a) shows intermediate signal of degeneration within the disc (arrow).
Shows fattened, irregular disc with complete anterior displacement (arrow) associated with osteoarthritic changes and joint effusion
Dr Ahmed Esawy

Shows ballooning of posterior disc band with complete anterior displacement (arrow) associated with osteoarthritic changes and joint effusion
Shows perforated disc with complete anterior displacement (arrow) associated with osteoarthritic changes (cortical erosion and irregular articular surface of the condyle and small anterior osteophyte)
Dr Ahmed Esawy

(a) (closed-mouth position) shows a displaced disk (arrow) that has lost its typical biconcavity, having become crumpled and irregular.
(b) (closed-mouth position) obtained in a different patient shows a pathologic displaced disk with a rounded shape (arrow).
Sagittal T2-
Abnormal morphologic features of the disk.
Anterior disk displacement
Dr Ahmed Esawy

(c) (closed-mouth position) obtained in a third patient shows a flattened displaced disk (arrow).
(d (closed-mouth position) obtained in a another patient demonstrates perforation of the intermediate zone of the disk (arrow).
Abnormal morphologic features of the disk
Anterior disk displacement
Dr Ahmed Esawy
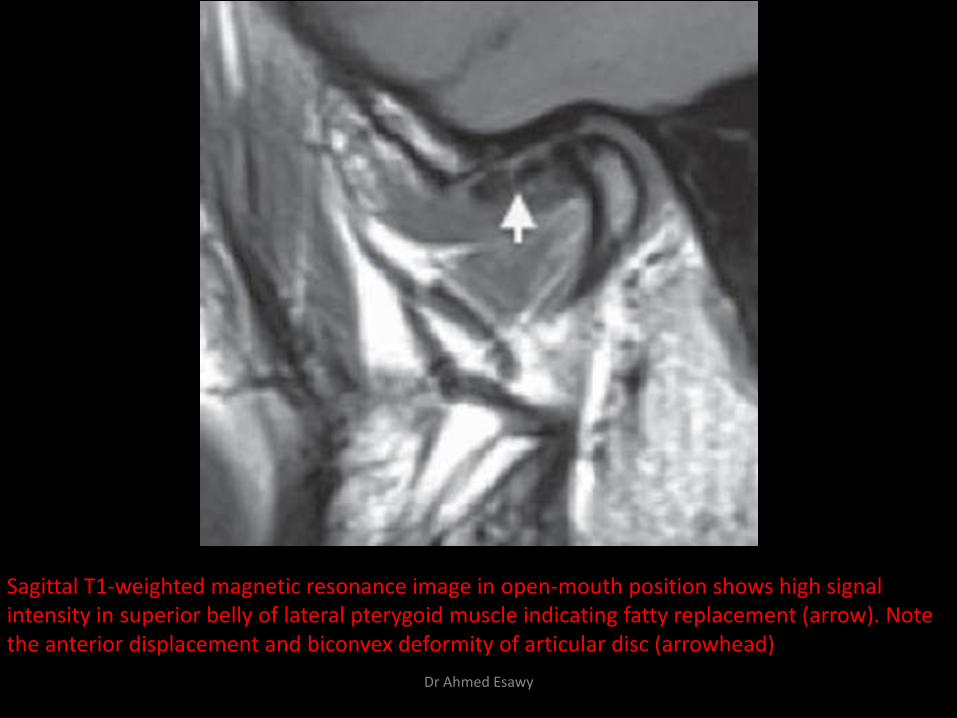
Sagittal T1-weighted magnetic resonance image in open-mouth position shows high signal intensity in superior belly of lateral pterygoid muscle indicating fatty replacement (arrow). Note the anterior displacement and biconvex deformity of articular disc (arrowhead)
Dr Ahmed Esawy

• Disk Deformity: – Chronic displacement leads to
deformity of the disc leading to:
• Loss of the normal biconcave morphology
• Thickening of its posterior band
• Irregular folding of its anterior band
Significant for clinical management as a
deformed disc cannot be
surgically repositioned.
Dr Ahmed Esawy

• (a) Sagittal T2-weighted MR image (closed-mouth position) shows significant disk displacement. The intermediate zone is clearly beyond the condyle, and the angle between the posterior band (dashed line) and vertical (solid line) is close to 50°.
(b) Sagittal oblique gradient-echo T2-weighted MR image (closed-mouth position) obtained in a different patient clearly depicts anteromedial disk displacement. The disk (arrow) appears to be "floating" by itself, and the condyle is no longer visualized.
Abnormal disk displacement in TMJ dysfunction
Dr Ahmed Esawy

Normal disk mobility Translation of the condyle
Dr Ahmed Esawy

• (a) closed-mouth position) shows a disk (arrow) in its normal position between the condyle and temporal bone and centered in the intermediate zone.
(b) (open-mouth position) shows that the disk (arrow) returns back has maintained its normal position during condylar movement. This interposition of the disk prevents abnormal contact between osseous joint surfaces.
Normal disk mobility
Dr Ahmed Esawy

• the posterior band (arrow) remains close to the mandibular fossa. Opening of the jaw in this case was seriously limited.
Stuck disc occurs when the disc fails to displace in open or closed mouth position and becomes fixed to the temporal bone due to adhesion.
closed-mouth
open-mouth
Dr Ahmed Esawy

• Posterior disk displacement. (a) (closed-mouth position) shows a posterior band displaced posteriorly.
• Sagittal T2
• (b) obtained in the open-mouth position, the posterior band (arrow) remains displaced. The jaw was nearly locked in this case.
Dr Ahmed Esawy

Translation of the condyle Condyle translation was assessed in PD sagittal oblique images in open mouth position as follows; 1-apex of the condyle translates to less than the apex of the articular eminence, 2-apex of the condyle translates to the apex of the articular eminence, which is a position many authors consider normal, 3-apex of the condyle translates beyond the apex of the articular eminence
Dr Ahmed Esawy

Sagittal oblique spin-echo proton-density–weighted MR images (open-mouth position) show the translation of the condyle in relation to the articular eminence (a) the apex of the condyle (arrow head) translates to the apex of the articular eminence (asterisk), which is considered normal.
Shows complete anterior disc displacement without reduction and restricted mobility of the condyle i.e., the apex of the condyle (arrow head) translates to less than the apex of the articular eminence (asterisk).
Shows normal disc position with hypermobility of the condyle i.e. the apex of the condyle (arrow head) translates beyond the apex of the articular eminence (asterisk).
Dr Ahmed Esawy

Sagittal T2 fat sat Closed Note both the mandibular condyle and fibrocartilaginous disc sitting in the fossa.
Sagittal T2 fat sat Open Note the disc and condyle translating forward out of the fossa
Dr Ahmed Esawy

Coronal MR image of closed jaw
Right : slight medial disk displacement
Left : slight lateral disk displacement Dr Ahmed Esawy

Lateral disc displacement and normal bone
Coronal MR image
Dr Ahmed Esawy

• Lateral Disk displacement :
Coronal MR image
Dr Ahmed Esawy

Coronal T1-weighted magnetic resonance image in closed-mouth position shows lateral displacement of articular disc (arrow)
Dr Ahmed Esawy

Medial disc displacement
Oblique coronal MRI coronal MRI
Coronal MR image
Dr Ahmed Esawy

Recapture of Displaced Disk
• Recapture
– Displaced disks regain their normal position during jaw
opening
– Synonym: Reduction
– Indicates the attachments and capsule are less
compromised
• Open jaw image allows further evaluation of the soft
tissue structures
– Rupture of diskal attachments— more severe, at risk for
developing sequelae
Dr Ahmed Esawy

Unidirectional anterior disk displacement without recapture
Sagittal MR image
(2800/15) with the jaw
open—
• the anteriorly
displaced disk does not
relocate with deformity
Dr Ahmed Esawy

Anterolateral disk displacement with complete recapture
Coronal (closed)
Lateral bulging of the disk
Sagittal (open)
The disk is in normal position
Sagittal (closed)
Anterior displacement of the disk
Dr Ahmed Esawy
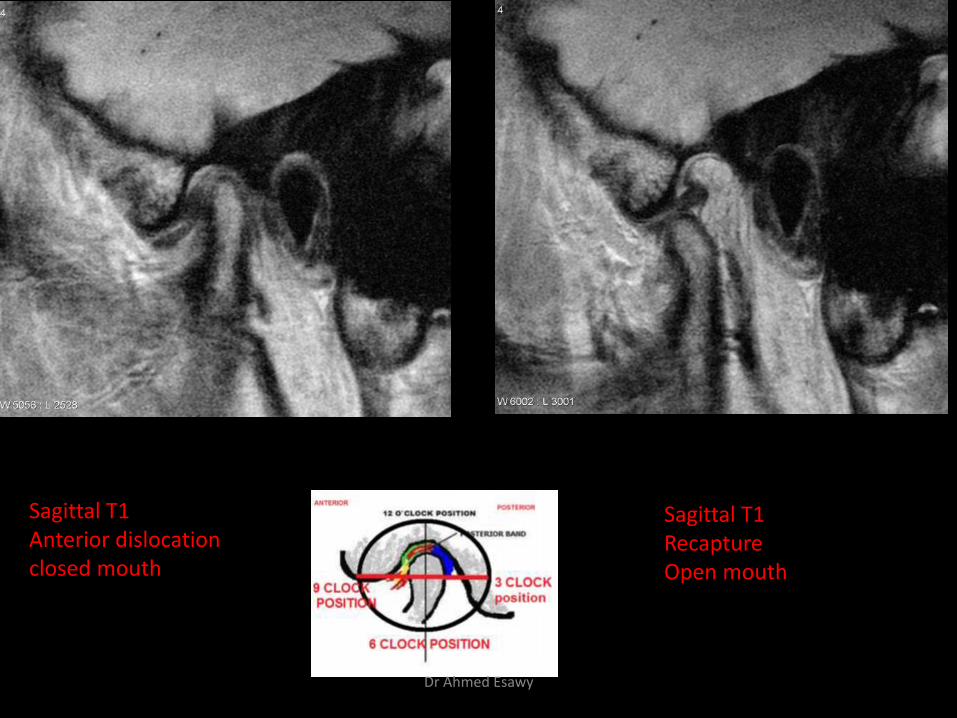
Sagittal T1 Recapture Open mouth
Sagittal T1 Anterior dislocation closed mouth
Dr Ahmed Esawy

Sagittal T1 anterior dislocation - closed Sagittal T1
No Recapture Open mouth
Dr Ahmed Esawy

LABRUM
Dr Ahmed Esawy

Thickening of an LPM Attachment
• two parts of the LPM
• the superior LPM and the inferior LPM
• pseudomeniscus sign," or thickening of the posterior meniscal attachment that occurs in some patients with an anteriorly displaced meniscus
Dr Ahmed Esawy

Sagittal oblique spin-echo proton-density–weighted MR image (closed-mouth position) shows normal disc position (large arrow) and normal thickness of inferior LPM insertion (small arrow).
Sagittal oblique spin-echo proton-density–weighted MR image (closed-mouth position) shows complete anterior disc displacement (arrow) and thickened inferior LPM insertion (arrow head), compared with (a).
thickness of LPM
Dr Ahmed Esawy

Normal LPM. (a) Sagittal oblique spin-echo proton-density–weighted MR image (closed-mouth position) shows a thin attachment of the inferior LPM (arrow) just below the disk
(b) Sagittal oblique gradient-echo T2-weighted MR image (closed-mouth position) shows a thin attachment of the superior LPM (arrow) just in front of the disk
Dr Ahmed Esawy

(c) Sagittal oblique gradient-echo T2-weighted MR image (closed-mouth position) shows the thin insertional area of the inferior LPM (arrow).
(d) On a sagittal oblique gradient-echo T2-weighted MR image obtained in the open-mouth position, the insertional area of the inferior LPM (arrow) has increased due to contraction of the muscle during this phase.
Normal LPM
Dr Ahmed Esawy

Abnormal LPM. (a) Sagittal oblique gradient-echo T2-weighted MR image (closed-mouth position) of a symptomatic TMJ shows complete disk displacement.
(b) Sagittal oblique gradient-echo T2-weighted MR image (closed-mouth position) of the contralateral asymptomatic TMJ shows subtle disk displacement. The insertional areas of the superior (arrowhead) and inferior (arrow) LPMs are markedly thinner than those in the symptomatic TMJ (cf a).
Dr Ahmed Esawy

Double disk sign. (a) Sagittal oblique gradient-echo T2-weighted MR image (closed-mouth position) of a symptomatic TMJ shows complete disk displacement. The thick insertional area of the inferior LPM (arrow) is parallel to the disk (arrowhead), creating the double disk sign.
(b) Sagittal oblique gradient-echo T2-weighted MR image (closed-mouth position) of a symptomatic TMJ in a different patient demonstrates severe internal derangement (arrowhead). A thick inferior LPM attachment (arrow) is again seen. The double disk sign must be recognized to distinguish between disk and muscle attachment. Dr Ahmed Esawy

Sequelae of Internal Derangement
• Disk displacement indicates damage to the
attachments, capsule, and ligaments of TMJ
• Compromised structural integrity functional
disturbance
• A process of degeneration to osteoarthritis may be
initiated
Dr Ahmed Esawy

• Active stages
– Synovitis, effusion, & bone marrow edema
• Advanced stages
– Joint space narrowing, subchondral sclerosis & cyst
formation, contour irregularity, osteophyte formation
– Neovascularity & remodeling of the disk (deformity,
rupture, & SI changes)
Dr Ahmed Esawy

Osteoarthritis
Definition Non-inflammatory focal degenerative disorder of
synovial joints, primarily affecting articular cartilage and sub-condylar bone; initiated by deterioration of articular soft-tissue cover and exposure of bone.
Clinical Features Crepitation sounds from joint(s) Restricted or normal mouth opening capacity Pain or no pain from joint areas and/or of
mastication muscles Occasionally, joints may show inflammatory signs Women more frequent than men
Dr Ahmed Esawy

TMJ osteoarthritis changes
Narrowing of the joint space.
fattening of the articular surface subcortical sclerosis or cyst surface erosion Osteophytes ( arise only from the anterior margin
of the condyle) generalized sclerosis for the condylar head Flattening of the articular eminence subcortical sclerosis, Surface erosions for the fossa
Dr Ahmed Esawy

anteriorly displaced and deformed, degenerated disc and irregular cortical outline with osteophytosis and sclerosis of condyle .
Dr Ahmed Esawy

Advanced osteoarthritis and anterior disc displacement, with joint effusion
Dr Ahmed Esawy

Anterior disk displacement with osteoarthritis
Sag
Cor
Closed position
1. Condyle with areas of bone marrow edema
2. Articular fossa
3. Displaced disk
4. Effusion
5. Subchondral cyst
Dr Ahmed Esawy

Osteoarthritic changes in four different patients. (a) Sagittal oblique gradient-echo T2-weighted MR image (closed-mouth position) obtained in a patient with internal derangement shows condylar flattening (arrow).
(b) Sagittal oblique gradient-echo T2-weighted MR image (open-mouth position) obtained in a patient with internal derangement without reduction clearly depicts an osteophyte (arrow).
Osteoarthritis
Dr Ahmed Esawy

(c) Sagittal oblique spin-echo T2-weighted MR image (closed-mouth position) obtained in a patient with internal derangement shows condylar erosion (arrow).
(d) Sagittal oblique gradient-echo T2-weighted MR image (open-mouth position) obtained in a patient with internal derangement without reduction demonstrates a condylar osteophyte, flattening, sclerosis, and erosion (arrow), all of which are signs of osteoarthritic changes ( a–c).
Osteoarthritis
Dr Ahmed Esawy

– Degenerative (Osteoarthritis)
• X-ray
– Narrowing of the joint space
anteriorly with slight sclerosis
– Small osteophyte arise from
the anterior margin of the
articular surface of the
condyle
Dr Ahmed Esawy
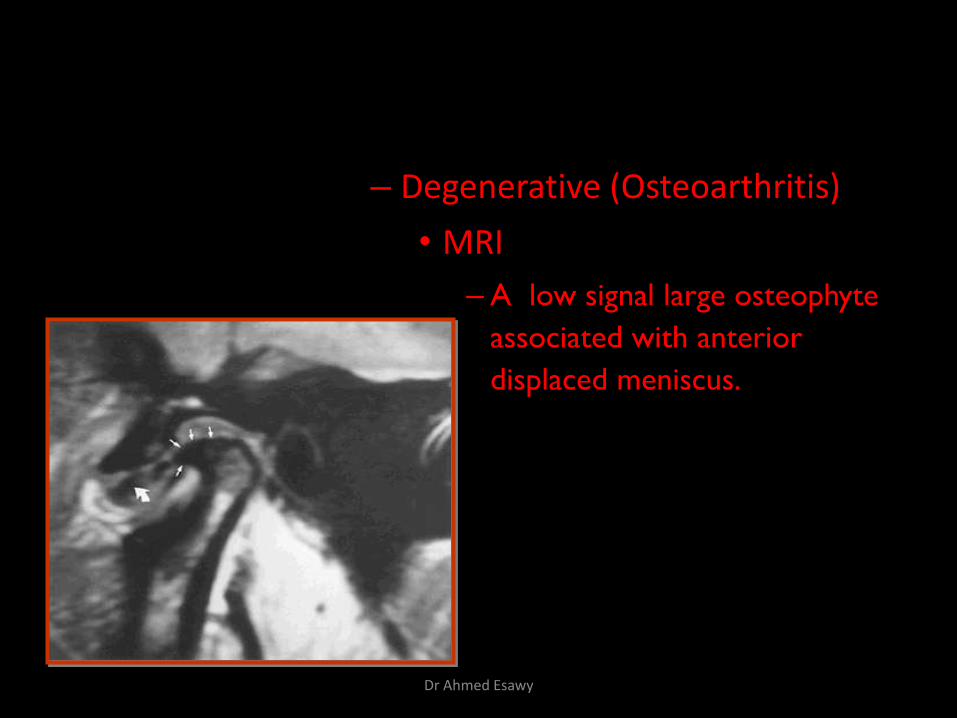
– Degenerative (Osteoarthritis)
• MRI
– A low signal large osteophyte
associated with anterior
displaced meniscus.
Dr Ahmed Esawy

Sagittal T1-weighted magnetic resonance image in open-mouth position of osteoarthritic joint shows osteophyte formation (arrowhead) and anterior displacement and folded deformity of articular disc (arrow)
Dr Ahmed Esawy

• Different grading systems have been developed to
describe the degree of internal derangement and
osteoarthritis
• The most simple to differentiate partial and total disk
displacement is on the basis of the position of the
disk relative to the condylar head and articular
eminence
Dr Ahmed Esawy

Grading System according to Wilkes
Grading System according to Vogl and Abolmaali
Dr Ahmed Esawy

Joint effusion was assessed on T2WI manifesting as area of hyperintensity, which was divided into 3 grades . Grade 0: None (no bright signal in either joint space). Grade I: Slight effusion (a bright signal in either joint space that conforms to the contours of the disc, fossa/articular eminence, and or condyle). Grade II: Frank effusion (a bright signal in either joint space that extends beyond the osseous contours of fossa/articular eminence, and or condyle and has a convex configuration in the anterior or posterior recesses.
Dr Ahmed Esawy

Joint effusion
Joint effusion. On a sagittal oblique gradient-echo T2-weighted MR image obtained in the closed-mouth position, joint fluid (arrow) clearly delineates the shape of the disk between the upper and lower joint spaces "arthrographic effect" . This phenomenon is best seen on T2-weighted images.
gadolinium-enhanced MR imaging of the TMJ may allow clear differentiation between the proliferating synovium, which enhances, and joint effusion, which does not. This technique can be useful if rheumatic inflammatory joint disease associated with joint effusion is suspected
Dr Ahmed Esawy

Sagittal T2-weighted magnetic resonance image shows fl uid effusion in superior joint cavity (arrow) and anterior displacement and folded deformity of articular disc (arrowhead)
Dr Ahmed Esawy

Sagittal T2-weighted magnetic resonance image in open-mouth position shows fl uid effusion in the superior joint space (arrows) and high signal intensity in the glenoid fossa indicating retodiskitis (arrowhead)
Dr Ahmed Esawy

Other findings related to internal derangement
• Joint effusion • Avascular necrosis &
bone oedema • Osteoarthritis
Dr Ahmed Esawy

Sagittal T2-weighted magnetic resonance image shows fl uid accumulation in superior joint space (arrowhead) and increased signal intensity of the condylar head indicating bone marrow edema (arrow)
Dr Ahmed Esawy

Sagittal oblique spin-echo proton-density–weighted MR image (open-mouth position) shows normal intact superior (large arrow) and inferior (small arrow) retrodiscal layers
Sagittal oblique T2-weighted MR image (open-mouth position) shows thickening of superior retrodiscal layer (large arrow) and normal inferior retrodiscal layer (small arrow).
RETRODI DISKAL LAYER INTEGRITY
Dr Ahmed Esawy

• Abnormal retrodiskal tissue. • (a) Sagittal oblique spin-echo proton-
density–weighted MR image (open-mouth position) obtained in a patient with internal derangement without reduction shows rupture of the fibers of the superior retrodiskal layer (arrow), resulting in loss of union with the posterior band.
• (b) Sagittal oblique gradient-echo T2-weighted MR image (closed-mouth position) obtained in a different patient again depicts rupture of the fibers of the superior retrodiskal layer (arrow).
Retrodiskal Layer Rupture
Dr Ahmed Esawy

Sagittal T1-weighted magnetic resonance image in closed-mouth position shows anteriorly displaced articular disc (arrow) and a hypointense band in the retrodiscal region (arrowhead) indicating thickening of posterior discal attachment “pseudo disc sign”
Dr Ahmed Esawy

Sagittal T1-weighted magnetic resonance image in closed-mouth position shows anteriorly displaced disc (arrow). Note the low signal intensity of lateral pterygoid tendon is parallel to the disc, giving a “double disc sign” Dr Ahmed Esawy
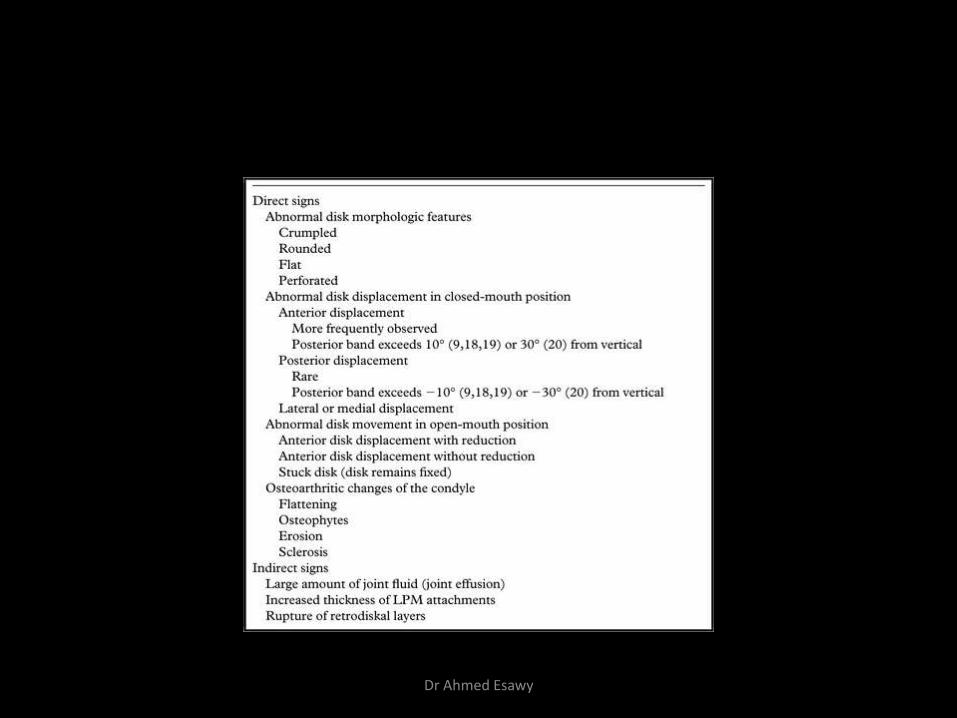
Direct and Indirect MR Imaging Signs of TMJ Dysfunction
Dr Ahmed Esawy

Progression of TMJ Dysfunction as Seen at MR Imaging
Dr Ahmed Esawy

Imaging after Treatment
• To detect corrected position of the displaced disc
• To detect post-operative complication e.g.
– Intra-articular adhesions
– Erosion following implants
before after
Dr Ahmed Esawy

Trauma
• Mandibular fractures:
– Car accidents – 75%
– Falls and sporting accidents – the rest
• Condylar process fractures:
– 25~50% mandibular fractures
– Falls and sporting accidents – majority
• Classifiication
– Condylar neck – low, medium, high
– Condylar head – extra- or intracapsular
Dr Ahmed Esawy

Classification of condylar process fractures
Nondisplaced fractures Displaced fractures: typically displaced medially due to traction of lateral pterygoid m. Dr Ahmed Esawy
• Evaluation of the type and grade of displacement of
bony structures is essential for treatment planning
– Angle between mandibular head & ramus
– Degree of contraction in the vertical plane (influences
occlusion)
– Transverse displacement, position of the fractured head…
Dr Ahmed Esawy

• Conventional radiography, panoramic radiography –
first-line dianostic tool
• CT – method of choice for assessment and grading of
facial trauma
• MR – identify posttraumatic disc dislocation &
rupture and injury to attachments, capsule, cartilage,
& ligaments in the pretherapeutic evaluation
Dr Ahmed Esawy

Bilateral medially displaced fractures
Fracture of the mandibular neck
Small fragments on the right (coronal CT) Dr Ahmed Esawy

1. Nondisplaced fracture of the right zygomatic process
2. Vertical condylar head fracture on the right
3. Comminuted, displaced condylar head fracture on the left
Dr Ahmed Esawy

• Trauma – Condylar neck fracture is
common.
– CT & MRI are helpful in cases of intracapsular fractures
Dr Ahmed Esawy

Arthritis
Definition
• Inflammation of synovial membrane characterized by edema, cellular accumulation, and synovial proliferation (villous formation).
Clinical Features
• Swelling of joint area, not frequently seen in TMJ
• Pain (in active disease) from joints
• Restricted mouth opening capacity
• Morning stiffness, in particular stiff neck
• Dental occlusion problems; “my bite doesn’t fit”
• Crepitation due to secondary osteoarthritis
Dr Ahmed Esawy

• Arthritis
– Inflammatory arthritis (rheumatoid)
– Degenerative ( osteoarthritis)
– Septic (rare)
Dr Ahmed Esawy

Inflammation
• TMJ: synovia-lined joint
– Synovial arthropathies predominantly rheumatoid
arthritis
– Rare with gout, psoriatic arthritis, ankylosing
sondylitis, SLE, juvenile chronic arthritis, CPPD
deposition
Dr Ahmed Esawy

• No distinction between different forms of synovial
arthropathy with MR imaging
– Synovitis with tissue swelling, edema, effusion
– Joint space narrowing, cartilage destruction, erosions,
marrow edema
– Formation of granulation tissue and pannus typically
occurs in the ―bare areas‖ near the capsular insertion
Dr Ahmed Esawy

Miscellaneous Conditions involving TMJ
– Inflammatory (Rheumatoid Arthritis)
• Very common, with rare significant symptoms.
• Erosions of articular surface of the condyle may be
extensive. The articular fossa usually remain normal
• Coronal T2 WI images are valuable.
• Other diseases as SLE, systemic sclerosis, psoriasis,
juvenile chronic arthritis, pigmented villonodular
synovitis, enteropathic arthritides can affect the
TMJ but they are rare.
Arthritis
Dr Ahmed Esawy
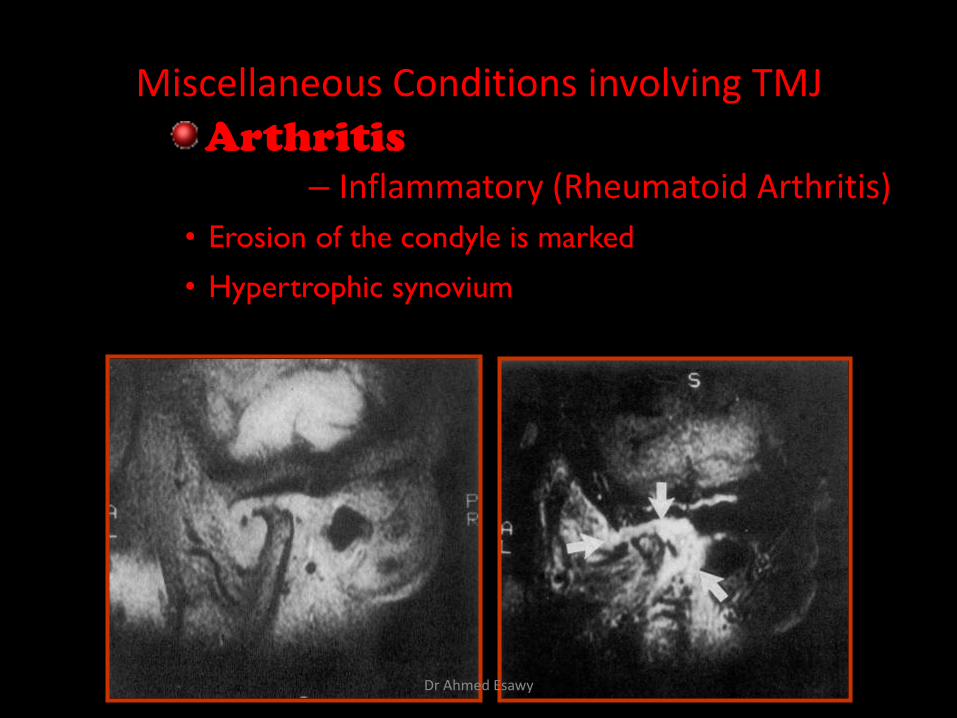
Miscellaneous Conditions involving TMJ
– Inflammatory (Rheumatoid Arthritis)
• Erosion of the condyle is marked
• Hypertrophic synovium
Arthritis
Dr Ahmed Esawy

Rheumatoid arthritis.
After 1 year Dr Ahmed Esawy

Rheumatoid arthritis. A MRI shows completely destroyed disc, replaced by fibrous or vascular pannus and cortical punched-out erosion (arrow) with sclerosis in condyle.
Dr Ahmed Esawy

Inflammed TMJ in rheumatoid arthritis
Sag STIR
1. Synovitis & inflammation of surrounding tissue
2. Small volume of intracapsular fluid in superior joint space
3. Partial anterior disk displacement
Dr Ahmed Esawy

Inflammed TMJ in rheumatoid arthritis
T1(400/15) T1+C
Slight enhancement of the bilaminar zone after contrast administration
Dr Ahmed Esawy

Psoriatic arthropathy. Oblique coronal and oblique sagittal CT images show punched-out erosion in lateral part of condyle (arrow).
Psoriatic arthropathy. MRI shows contrast enhancement within bone erosion and in joint space, consistent with thickened synovium/pannus formation. Openmouth MRI shows reduced condylar translation but normally located disc (and normal bone in this section)
Dr Ahmed Esawy
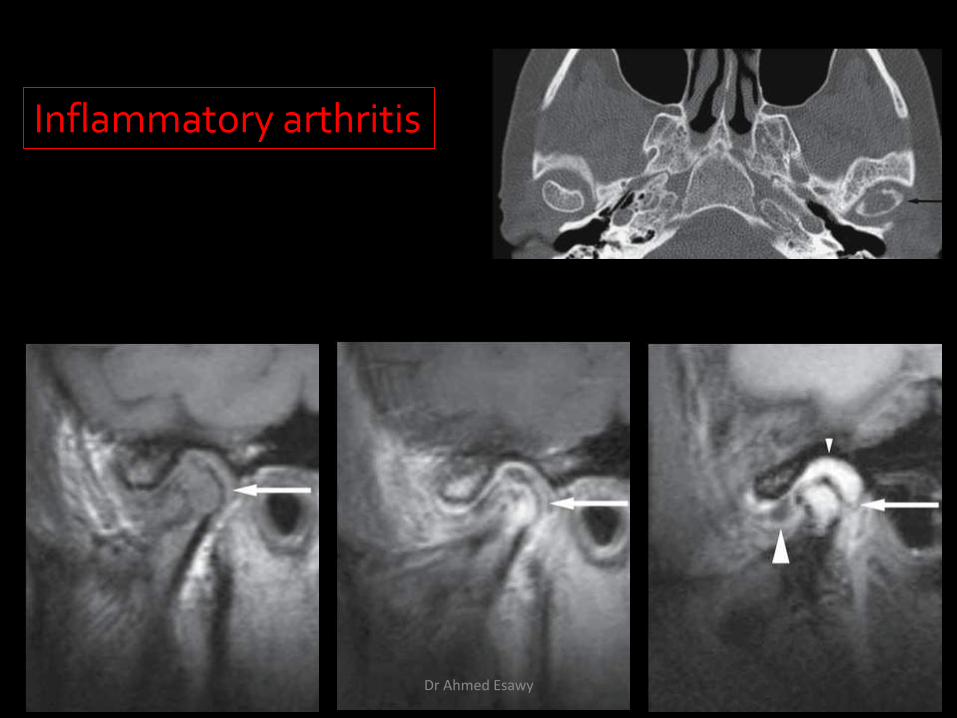
Inflammatory arthritis
Dr Ahmed Esawy

Bone Marrow Abnormalities
Definition
• Bone marrow edema: serum proteins within marrow interstitium surrounded by normal hematopoietic marrow.
• Osteonecrosis: complete loss of hematopoietic marrow.
Dr Ahmed Esawy

Imaging Features •Abnormal signal on T2-weighted image from condyle marrow: increased signal indicates marrow edema; reduced signal indicates marrow sclerosis or fibrosis •Combination of marrow edema signal and marrow sclerosis signal in condyle most reliable sign for histologic diagnosis of osteonecrosis •Marrow sclerosis signal may indicate advanced osteoarthritis without osteonecrosis, or osteonecrosis
Dr Ahmed Esawy

Ankyloses Definition Fibrous or bony union between joint components.
Dr Ahmed Esawy

Growth Disturbances (Anomalies) Definition Abnormal growth of mandibular condyle; overgrowth, undergrowth, or bifid appearance.
Dr Ahmed Esawy

Normal TMJ
Condylar Hypoplasia Condylar hypoplasia and facial asymmetry
Dr Ahmed Esawy

Bifid condyle.
Dr Ahmed Esawy

Miscellaneous Conditions involving TMJ
• Developmental anomalies
1- Hypoplasia of the Condyle • Unilateral or bilateral
• Unilateral cases is sequel of trauma or infection result in mandibular asymmetry
• Bilateral cases are developmental, result in very small mandible (bird face)
Dr Ahmed Esawy

Miscellaneous Conditions involving TMJ
• Developmental anomalies
2- Hyperplasia of the Condyle • Rare
• Unknown etiology, always unilateral
• Generalized enlargement of the condylar head
• High activity in scintigram
Dr Ahmed Esawy

Miscellaneous Conditions involving TMJ
• Developmental anomalies
2- Hyperplasia of the Coronoid process: • Bilateral enlarged coronoid process extends
above the zygomatic arch.
• The anterior margin of both coronoid processes are in face-to-face contact with the posterior aspect of the zygomatic bone in the open mouth position.
Dr Ahmed Esawy

Inflammatory or Tumor-like Conditions Calcium Pyrophosphate Dehydrate Crystal Deposition Disease (Pseudogout)
Dr Ahmed Esawy

Benign Tumors
Synovial Chondromatosis • Benign tumor characterized by cartilaginous metaplasia of
synovial membrane, usually in knee, producing small nodules of cartilage, which essentially separate from membrane to become loose bodies that may ossify.
Dr Ahmed Esawy
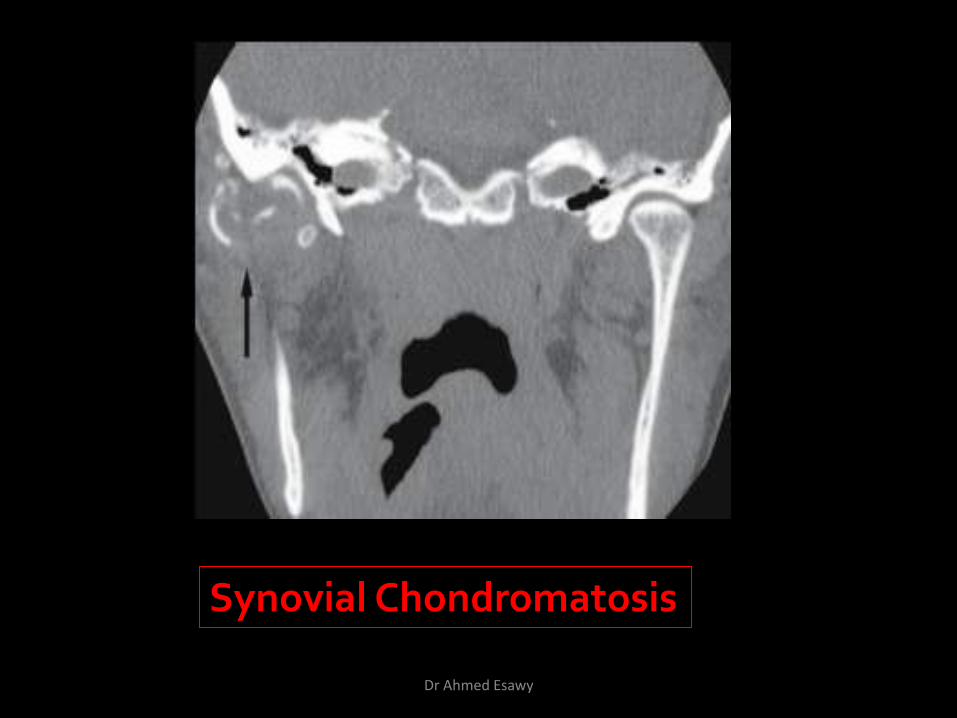
Synovial Chondromatosis
Dr Ahmed Esawy

– Synovial chondromatosis
Tumours & Tumour-like conditions
Dr Ahmed Esawy

The disc-condyle relationship appears normal but the condyle-disc complex is displaced inferiorly (a and b). Significant bony changes are not evident. The T2-weighted image (c) shows an extremely large amount of synovial fluid visible as a high signal intensity that expands the joint capsule. Arrow = loose body.
Synovial chondromatosis
Dr Ahmed Esawy

The disc-condyle relationship appears more or less normal but the condyle-disc complex is displaced inferiorly. Loose bodies are not visible in these cuts.
Synovial chondromatosis
Dr Ahmed Esawy

An extremely large amount of synovial fluid and several hypointensive loose bodies are visible in the superior joint space (a). The calcified loose bodies are visible also on the CT image (b). The outline of the joint capsule in the MRI picture (a) is marked by the white triangles, while the arrows show the loose bodies in the CT image (b). C = condylar head.
Synovial chondromatosis
Dr Ahmed Esawy

This image does not show a capsular expansion although the superior joint space is largely filled with synovial fluid (high signal intensity, white arrow). C = condylar head.
Synovial chondromatosis
Dr Ahmed Esawy

The disc-condyle relationship appears normal (a and b), but the disc is displaced superiorly (b) because the inferior joint space is affected. The T2-weighted image (c) shows a very large amount of synovial fluid with remarkable capsular expansion of the inferior joint space
Synovial chondromatosis
Dr Ahmed Esawy

– Simple bone cyst
Tumours & Tumour-like conditions
Dr Ahmed Esawy

Osteochondroma Definition Benign tumor characterized by normal bone and cartilage, near growth zones.
Dr Ahmed Esawy

– Osteochondroma
Tumours & Tumour-like conditions
Dr Ahmed Esawy
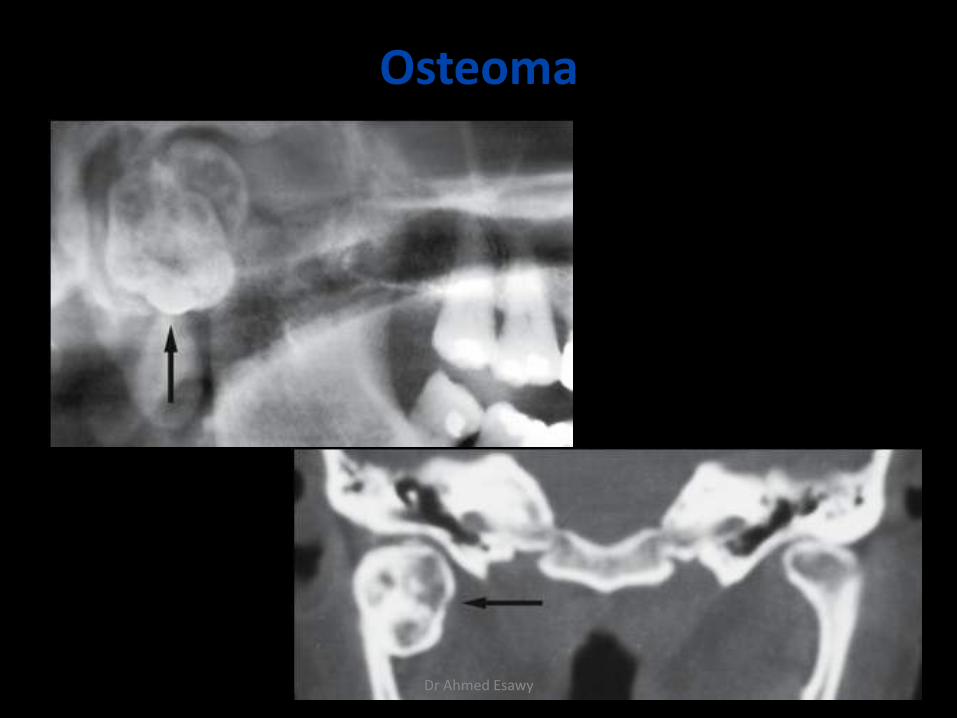
Osteoma
Dr Ahmed Esawy

Malignant Tumors
Osteosarcoma mandible; 18-year old female Dr Ahmed Esawy

Malignant tumor, mandible; 70- year-old male with metastasis from lung cancer
Dr Ahmed Esawy

1-limitation of mandibular movement: due to: a-intracapsular causes:
Infective arthritis
Juvenile arthritis
Traumatic arthritis
Intracapsular condyle fracture
b-pericapsular causes:
Irradiation
Dislocation
Condylar neck fracture
Infection of adjacent tissues
Dr Ahmed Esawy

c-muscular:
Tmj dysfunction syndrome
Myalgia due bruxism
Haematoma from ID block
Tetanus
d-Others:
Oral submucous fibrosis
Systemic sclerosis
Zygomatic & maxillary fracture
Drugs
Craniofacial anomalies involving the joint
Dr Ahmed Esawy

Limitation of TMJ movements:
Temporary persistent
(trismus) (ankylosis)
Dr Ahmed Esawy

3-Pain in or around the joint: due to:
• injury
• infection & inflammation
• vascular disease e.g: cranial arteritis
• muscle spasm e.g: pain dysfunction syndrome
• rheumatoid & other arthritis
• salivary gland disease e.g: parotid neoplasm
• ear disease e.g: otitis media, externa
Dr Ahmed Esawy

4-Hyperplasia:
Is rare unilateral overgrowth of the condyle.
It causes: facial asymmetry, deviation of the jaw to the unaffected side on opening and crossbite.
Treated by:
-If it is stabilized at the end of puberty --- corrective osteotomies to restore occlusion & facial asymmetry
-If it is still active --- intracapsular condylectomy
Dr Ahmed Esawy
5-Neoplasms: (rare):
• osteochondroma
• osteoma
• chondroma
Dr Ahmed Esawy

6-Loose bodies in the TMJ: (rare):
• osteochondritis disssecans:
due to trauma
• synovial chodromatosis
benign neoplasm
Dr Ahmed Esawy