msk interesting case (17/8/2017) dr yap sheau huey · unisystem, multifocal multisystem
TRANSCRIPT

MSK Interesting Case (17/8/2017)
Dr Yap Sheau Huey

3 cases of clavicular swelling with different diagnoses.
Case 1
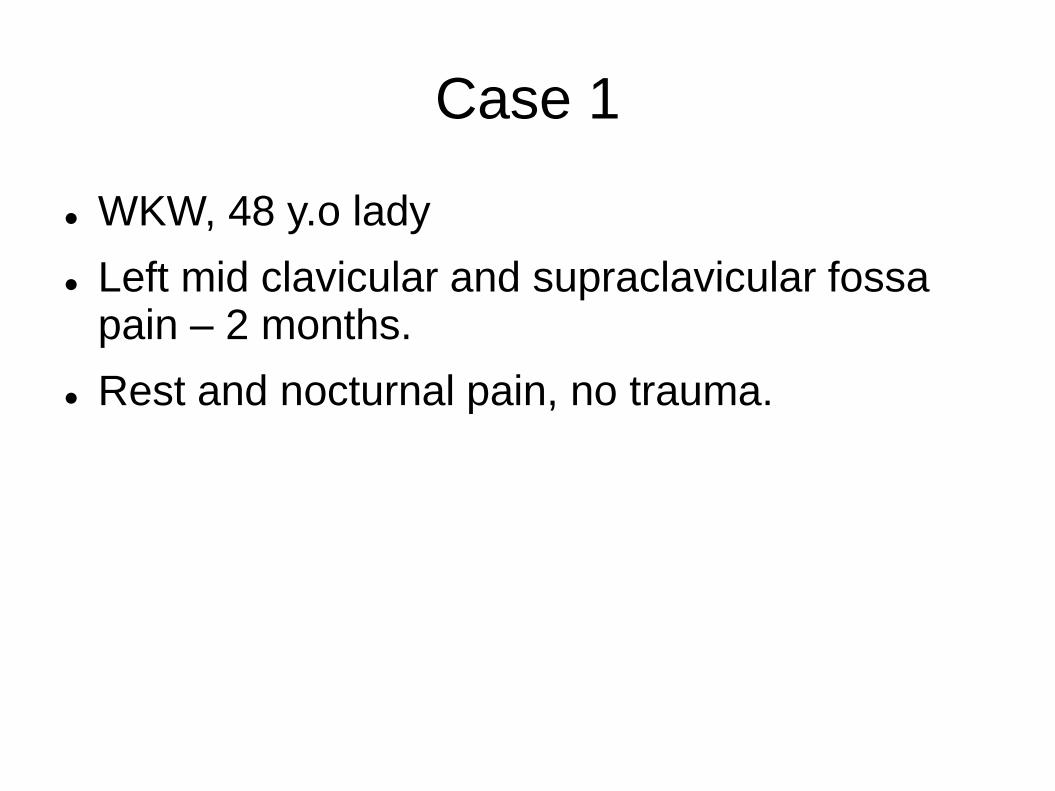
WKW, 48 y.o lady
Left mid clavicular and supraclavicular fossa pain – 2 months.
Rest and nocturnal pain, no trauma.
Plain XR

CT Biopsy ( 11/4/2017)
Very hard sclerotic bone.
Osteobell (9G), Oncontrol Drill (11G) failed to get bone tissue.
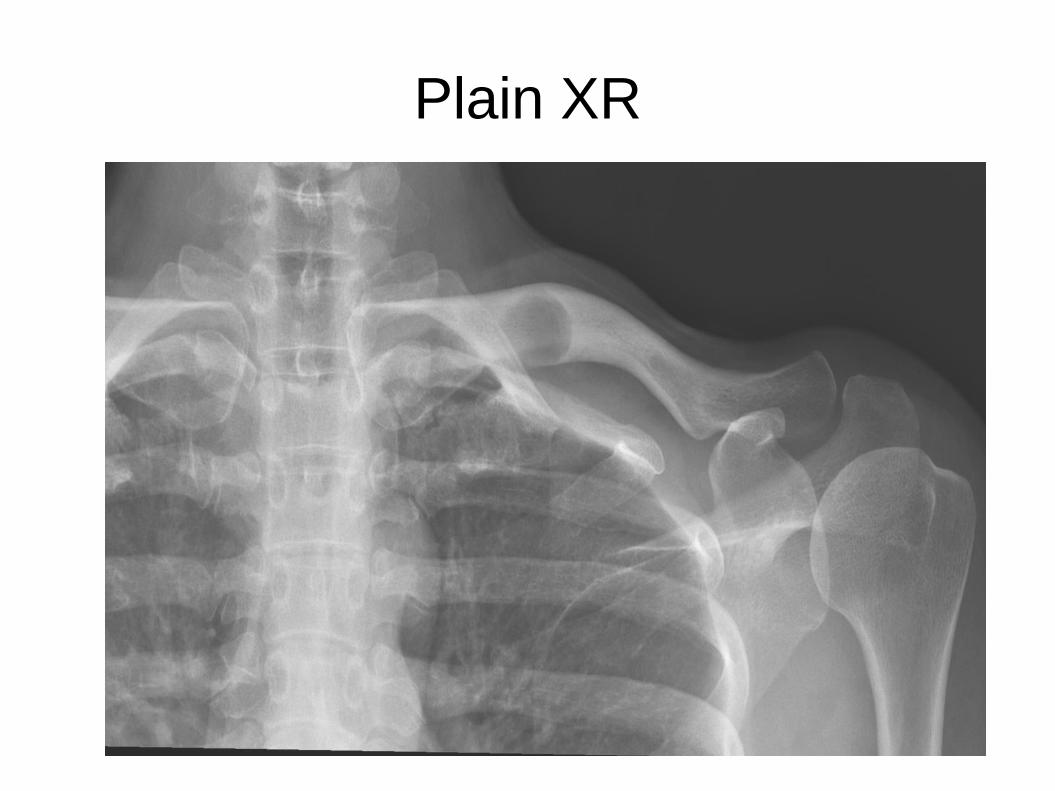
Coronal view
Finally, obtained the soft tissue lesion with 16G Temno.
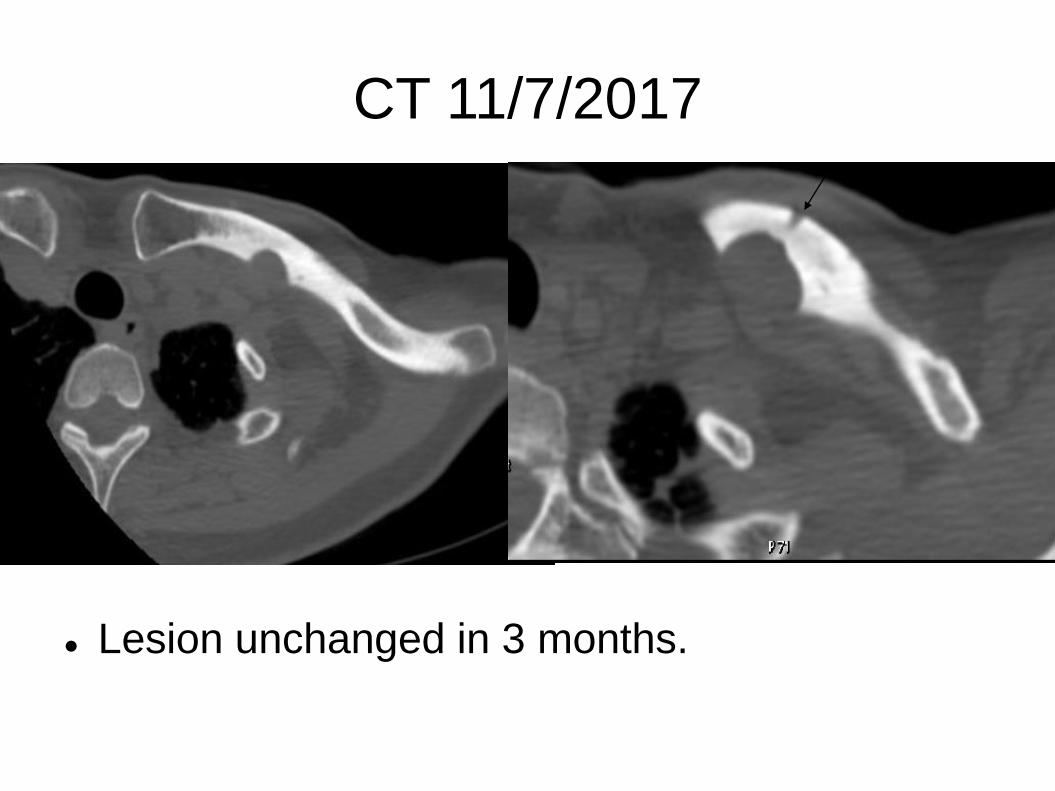
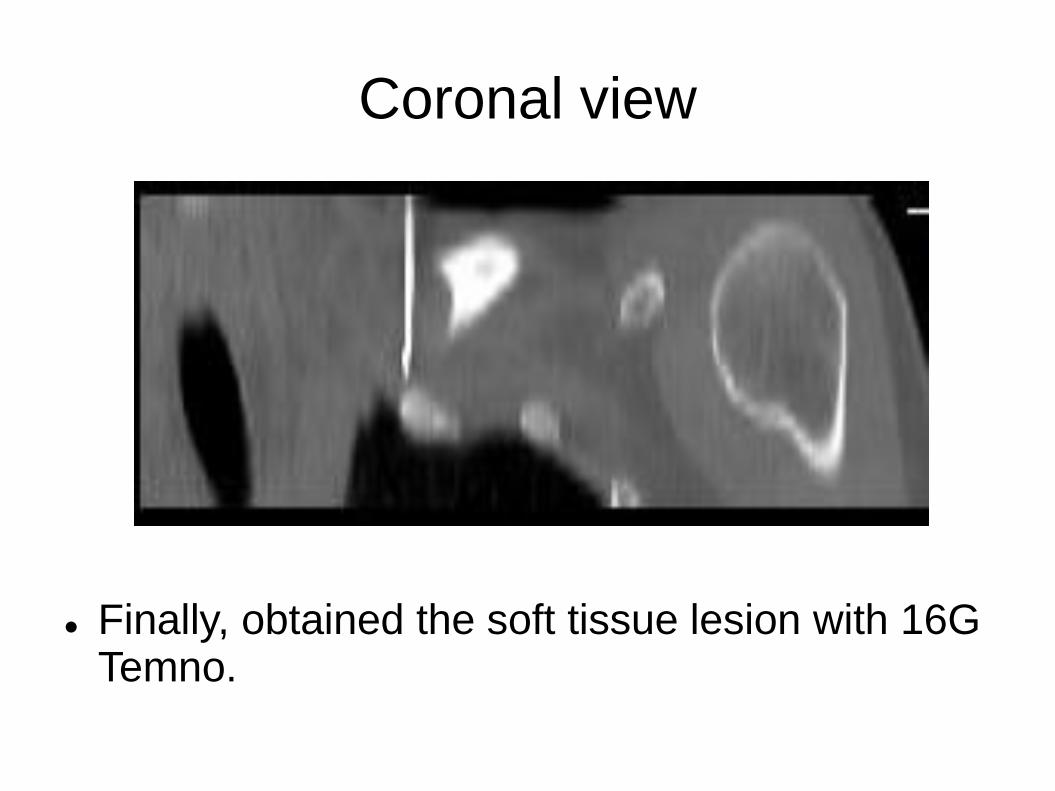
CT 11/7/2017
Lesion unchanged in 3 months.
HPE
Features are most suggestive of epitheloid vascular tumour including epitheloid hemangioma or hemangioendothelioma.
Discussion
Vascular tumour of the bone
From benign → intermediate → malignant.
Epithelioid hemangioma
Histiocytoid hemangioma, angiolymphoid hyperplasia w eosinophilia.
New entity in 2013 WHO classification
Composed of small vessels lined by epitheloid endothelial cells.
Long bone > flat bone > vertebra.
Locally aggressive, recurrence ~ 10%.
Radiology:
Ranges from well defined osteolytic lesion, sclerotic margin eccentrically located →
Mixed lytic sclerotic, cortical expansion and thinning.
Treatment:
Primary curettage, marginal en bloc resection.
Case 2
LTW, 9 y.o boy
Presented for painful left clavicular swelling for 2 months.
No constitutional symptoms.

Plain XR

CT
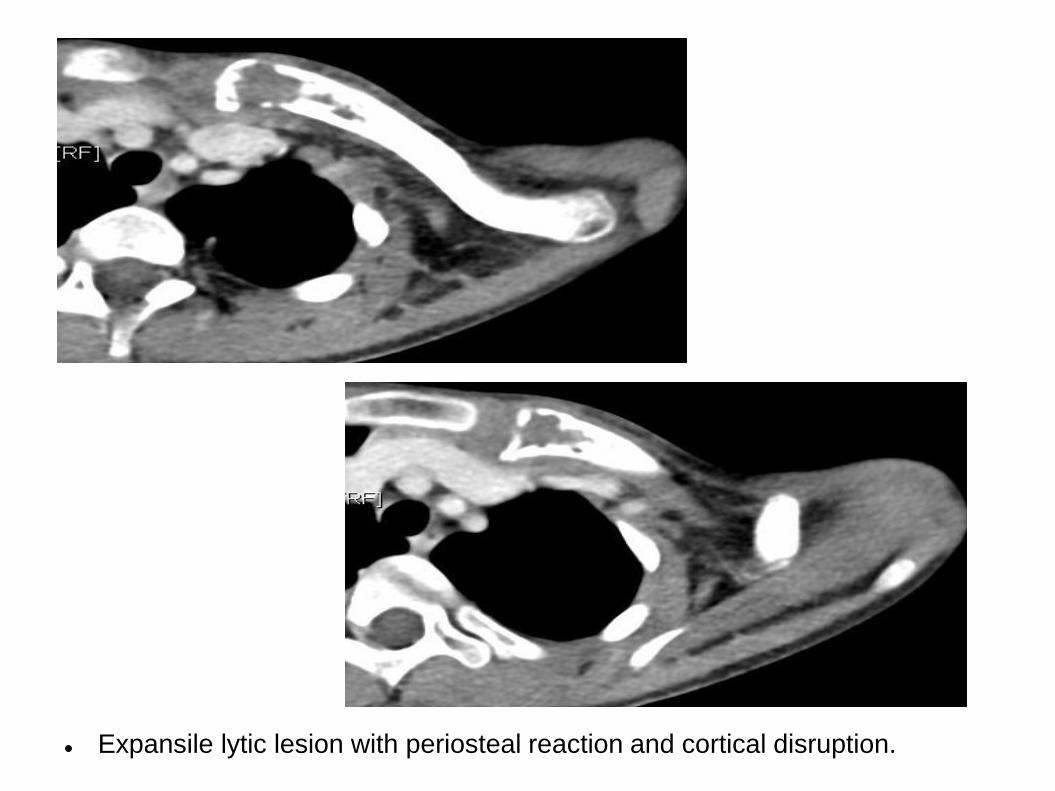
Expansile lytic lesion with periosteal reaction and cortical disruption.

Bone Scan

Diagnosis
Histopathology:
Consistent with Langerhans cell histiocytosis.
Langerhans Cell Histiocytosis
A group of diseases due to abnormal proliferation of Langerhans cells in 1 @ > organs.
Causes:unknown.
Divided into: unifocal(localized), multifocal unisystem, multifocal multisystem.
Most common in children.
Osseous manifestation: most common ( >flat bone)
Long bone: diaphysis/ metaphysis.
Intramedullary lesion
Early lesion: lytic, expansile, aggressive
Mature lesion: sharply defined sclerotic margin
Chronic: may resolve/appear sclerotic.
Case 3
KKM, 52 y.o man
Left clavicular painless swelling for 2 years.
Swelling is fluctuated in size.

CT
Severe hypertrophy, hyperostosis, sclerosis of both clavicle ( >at left)

Ankylosis of bilateral sternocostal joint, calcifications of costocalvicular ligament

Sclerosis of anterior edge of T4-T6 vertebrae.
Ankylosis of manubriosternal joint
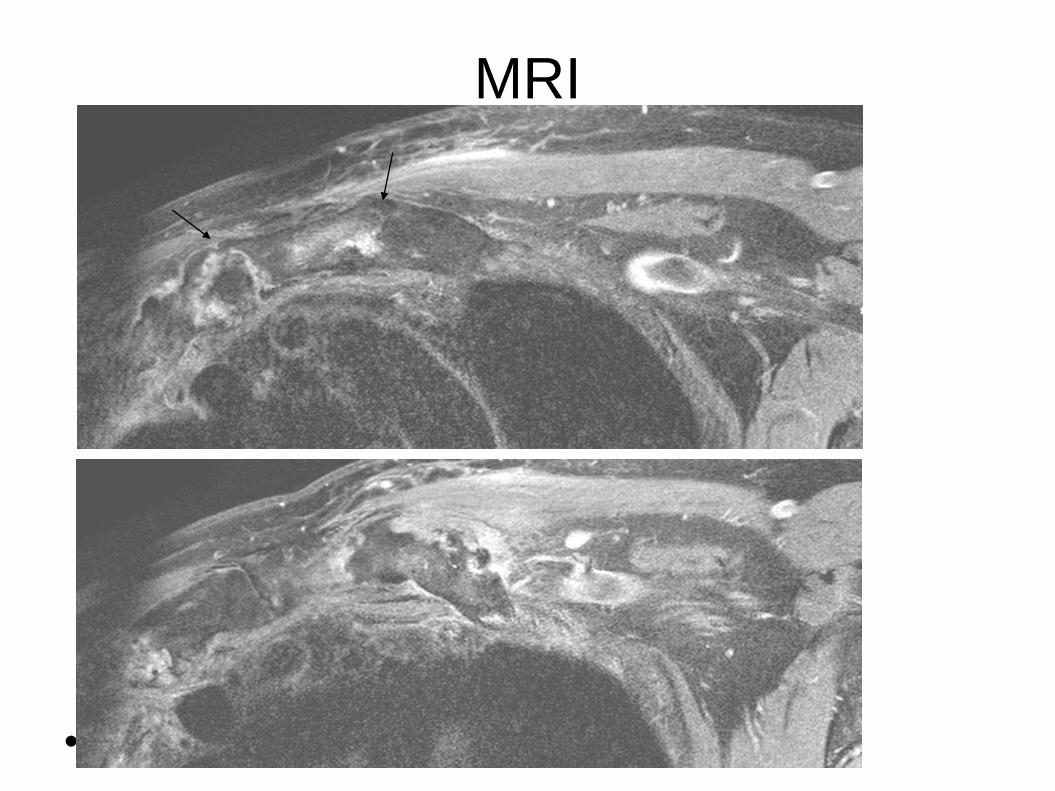
MRI
PDFS 1: SCJ
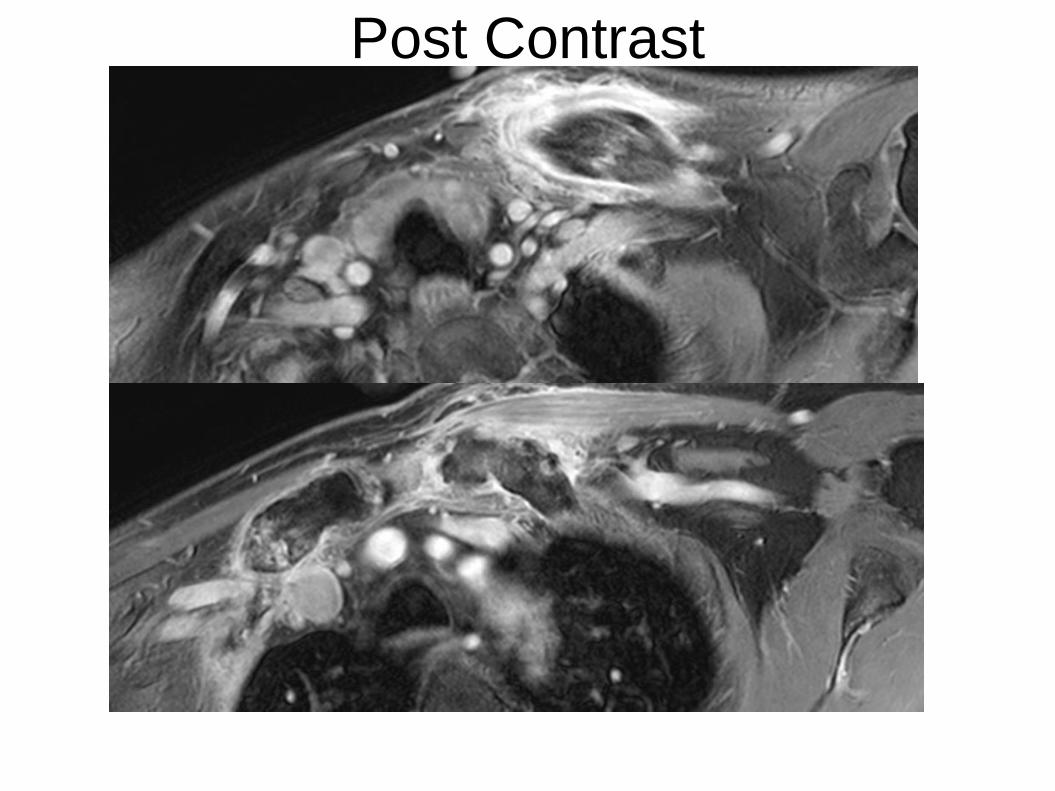
Post Contrast
SAPHO
Acronym of
Synovitis, Acne, Pustulosis, Hyperostosis, Osteitis
Inflammatory condition whose denominator is
Aseptic osteoarticular lesions
Skin lesions
Both manifestations need not co-exist for diagnosis
Osteoarticular lesions:
Synovitis, hyperostosis, osteitis, arthropathy, enthesopathy
Osteodestructive (early stage); osteoproliferative ( later stage)
Adult: Anterior chest wall ( sterno-costo-clavicular junction) > axial skeletal ( spine, SI Joint)
Can have surrounding soft tissue inflammation.
NO abscess, fistula, large paravertebral masses.
Case 4
18 y.o man.
Recurrent hip pain at anterior hip and greater trochanter.
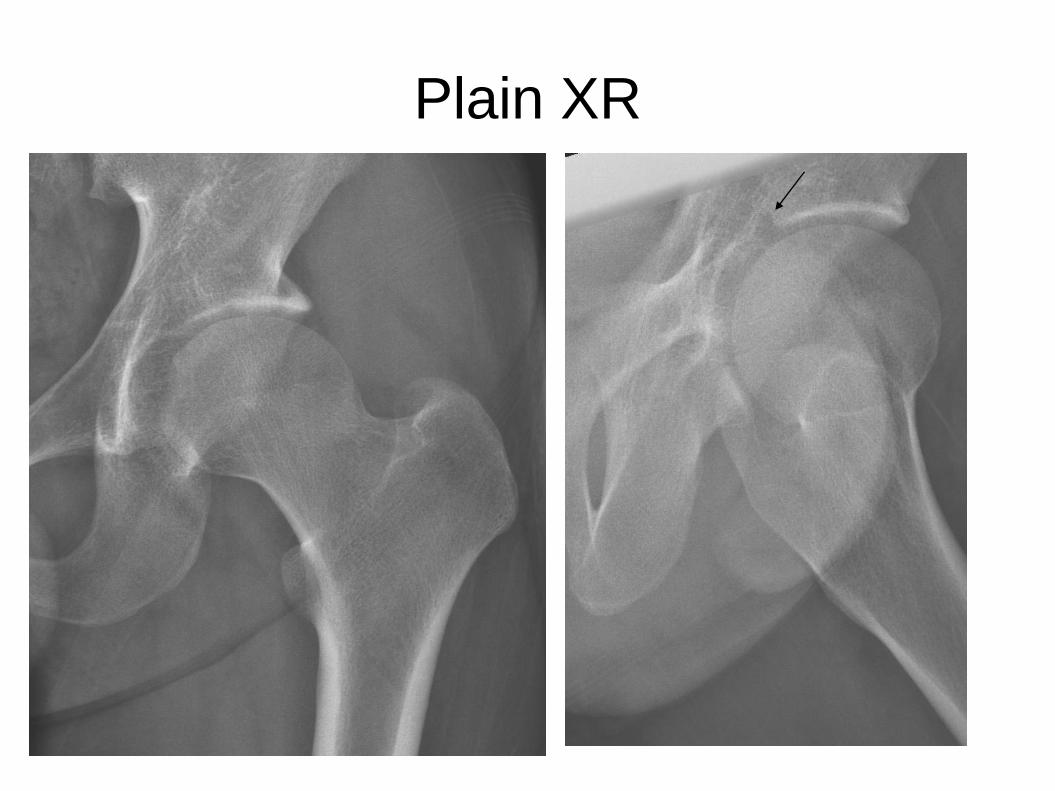
Plain XR

MRI Coronal View
Supraacetabular fossa (Pseudo-cartilage defect)
Normal variant, in about 10% of MRI hip.
Type 1: with contrast
Type 2: with cartilage
Location: 12 o'clock of acetabular roof
Distinguished with osteochondral/chondral defect by:
Location
Normal underlying marrow signal
No cartilage defect in arthroscopy

Case 5
YLY 65 y.o lady
Initially has sudden onset right wrist swelling and mild pain 6 months ago.
Swelling later 'moved' to the distal forearm.
Stable in size.
No h/o trauma.

Clinical

Xray
US

Left Right


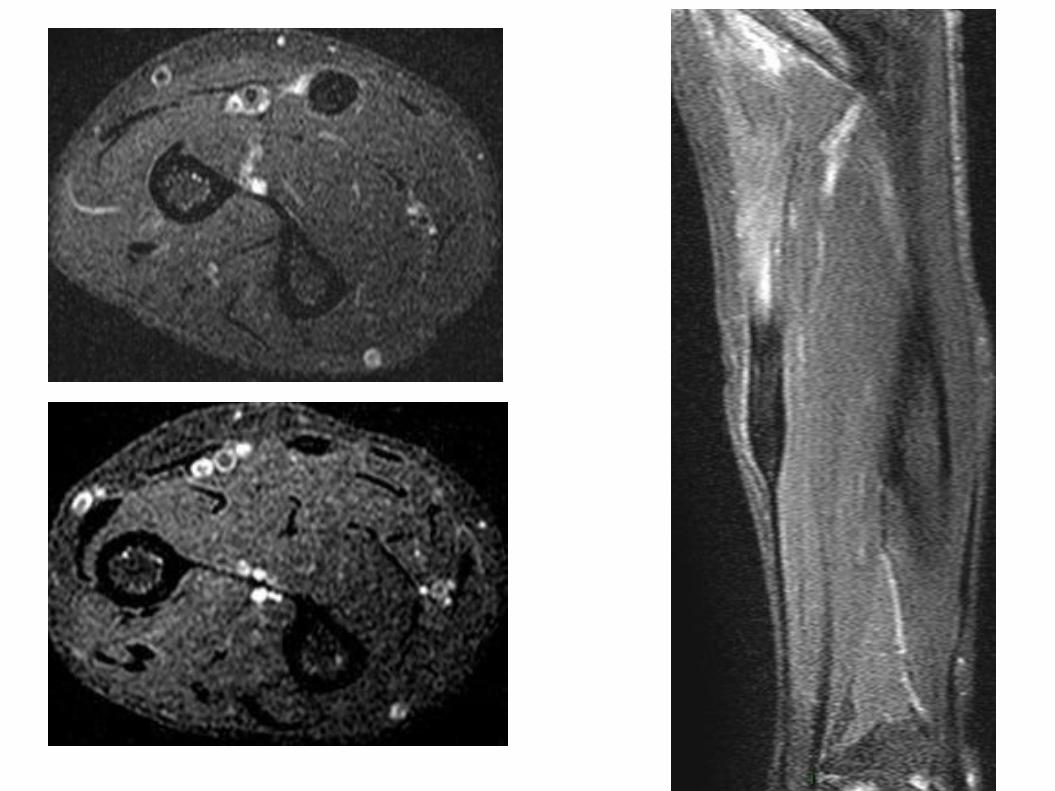
Diagnosis
Partial tear of flexor carpi radialis secondary to triscaphe osteoarthtitis.
Discussion
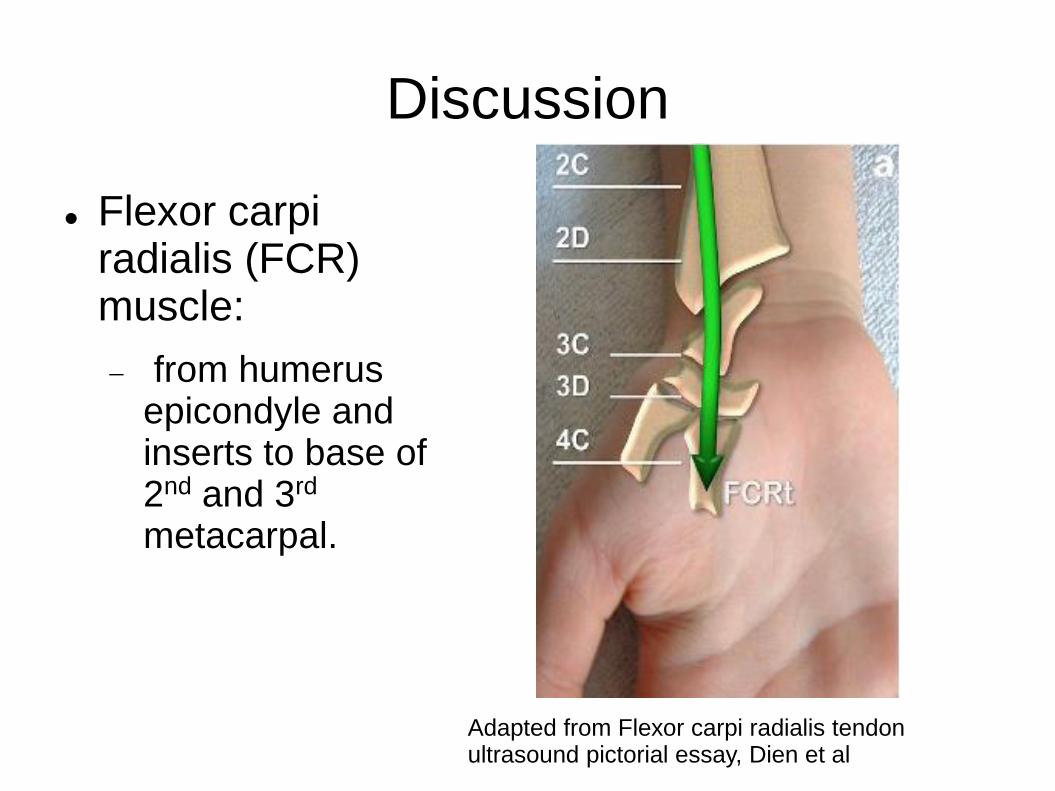
Flexor carpi radialis (FCR) muscle:
from humerus epicondyle and inserts to base of 2nd and 3rd
metacarpal.
Adapted from Flexor carpi radialis tendon ultrasound pictorial essay, Dien et al

Adapted from Flexor carpi radialis tendon ultrasound pictorial essay, Dien et al

FCR tendon lies in close contact with STT joints; the tendon sheath smtm communicates.
FCR tendon rupture/tear
RA/chronic inflammatory disorder
Non RA: most common cause: OA
Bony spur penetrates tendon sheath, tendinosis, then tear.
Other causes: trauma
Treatment: usually conservative dt minor functional deficit.

Case 6
History of Ultrasound diathermy for physiotherapy.
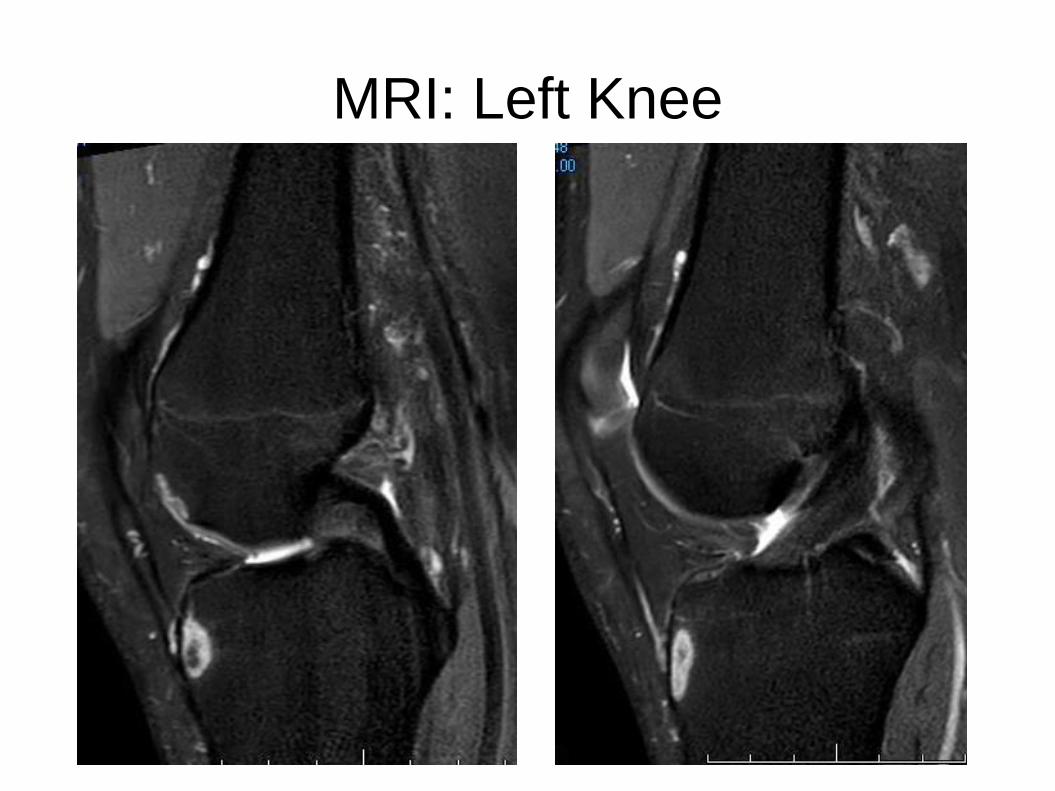
MRI: Left Knee
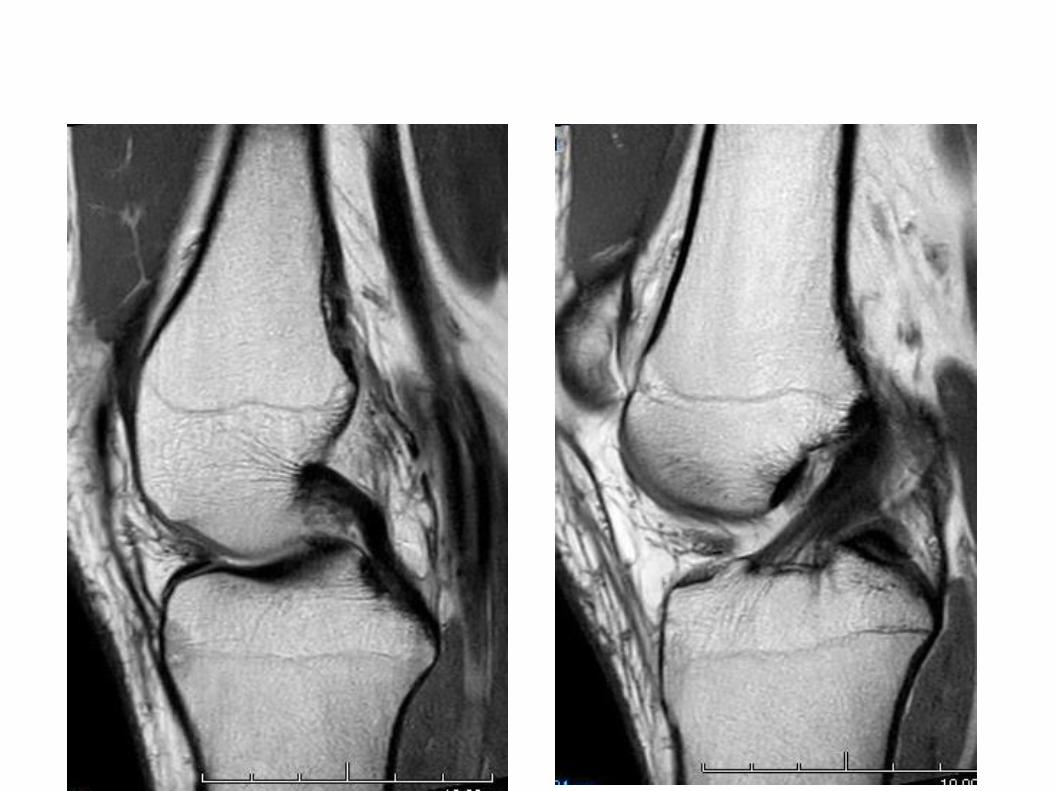
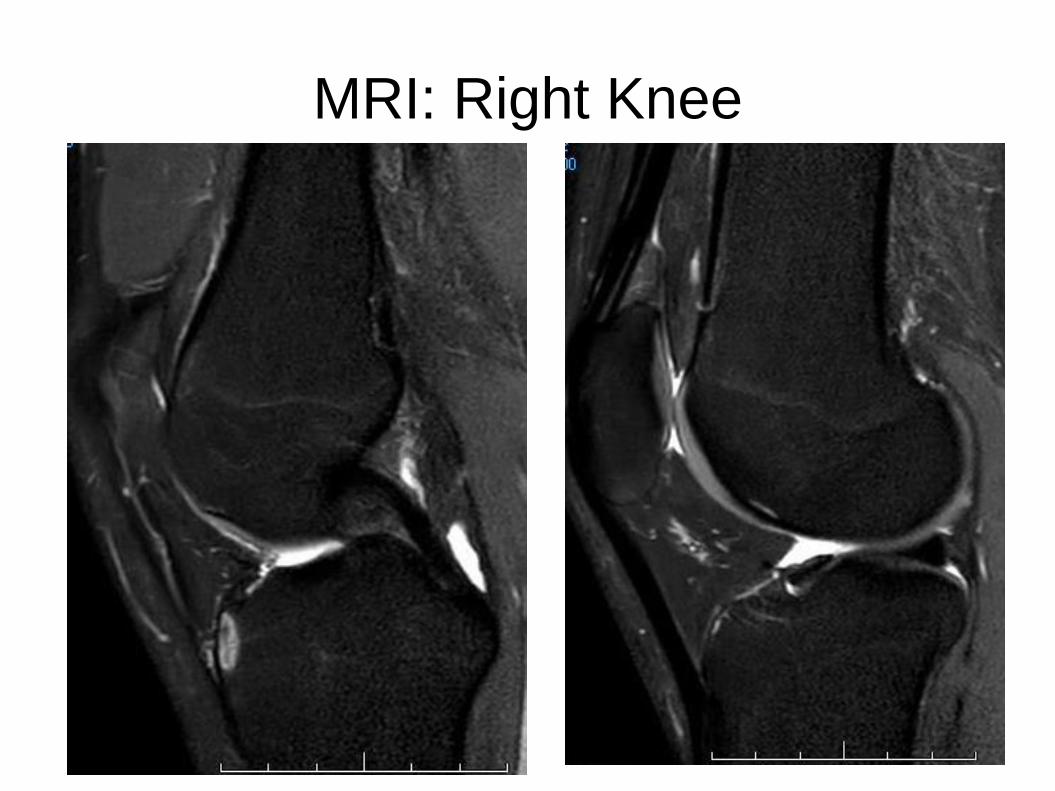
MRI: Right Knee

Bone lesion as a complication of US diathermy
Ultrasonic diathermy:
Use in physiotherapy
Generate heating effect deep in the soft tissue
At high intensities, instantaneous necrosis can occur.
Imaging of bone lesions by US diathermy:
Similar with osteonecrosis
Location: superficial location, at the site of bone facing the body surface, not involved deeper marrow
F/U MRI: resolutions of lesion
Case 7
CHT 24 y.o. Football/rugby player
Has injury over the Rt greater toe on 19/2/2017 during football game.
Unable to flex IPJ.
Had extracorporeal shock wave therapy.
However, no improvement, slightly worsening.
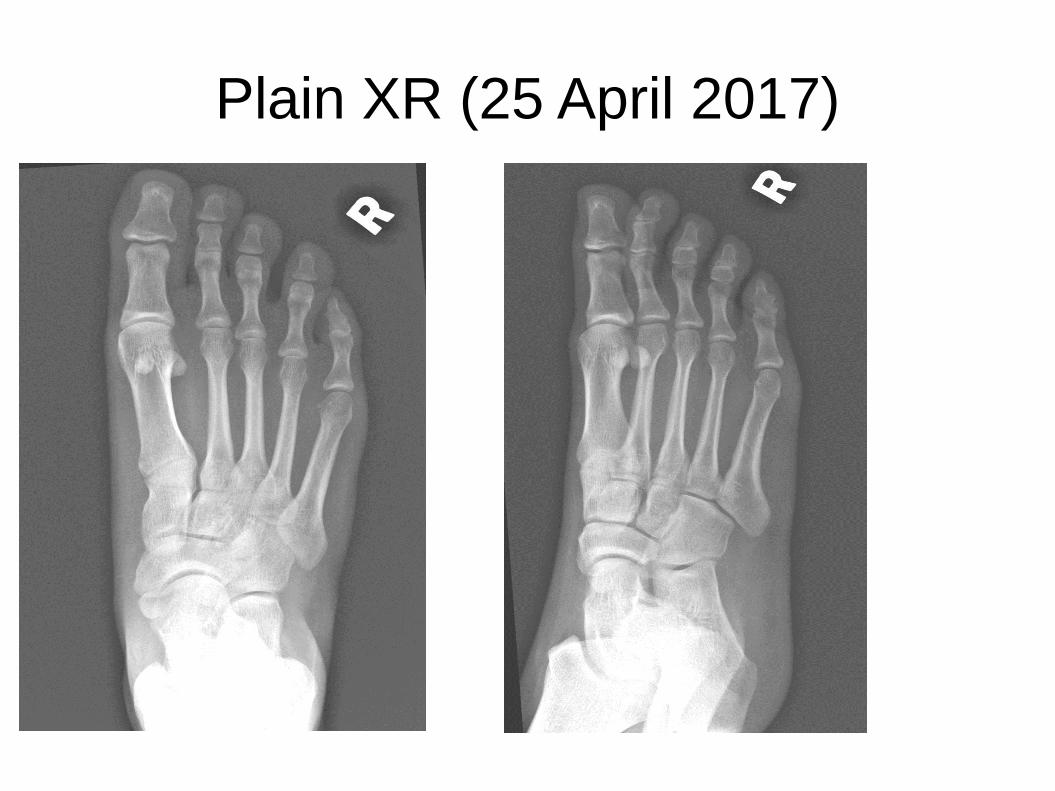
Plain XR (25 April 2017)
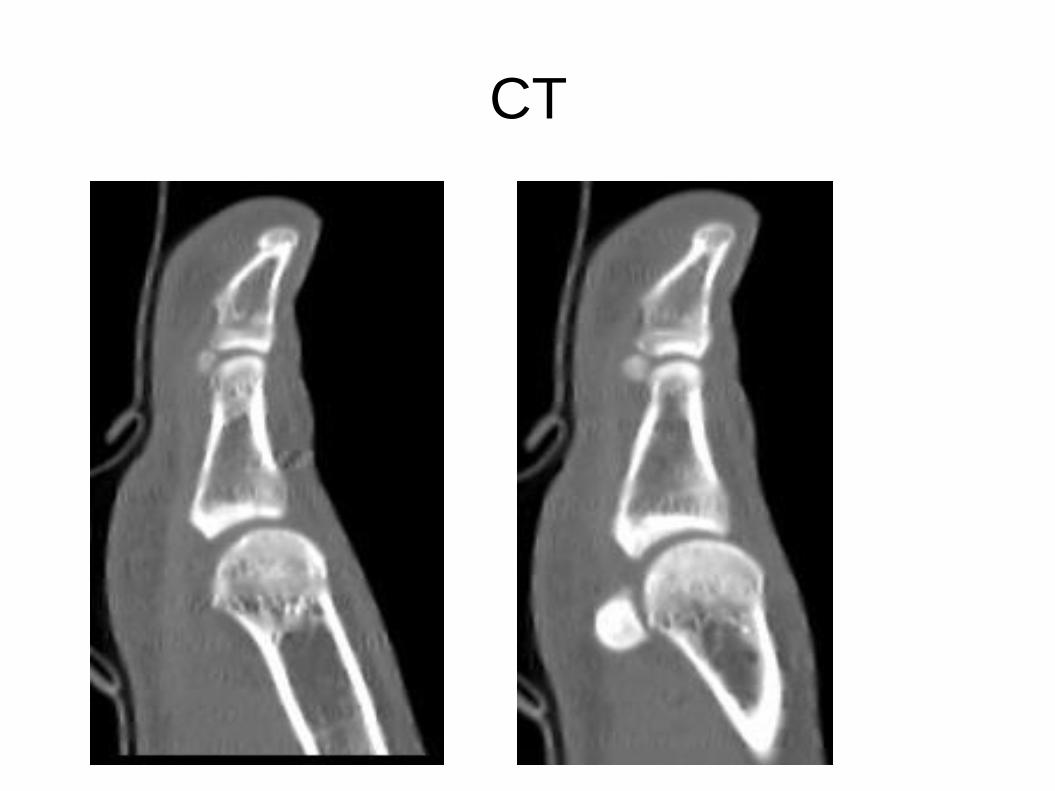
CT
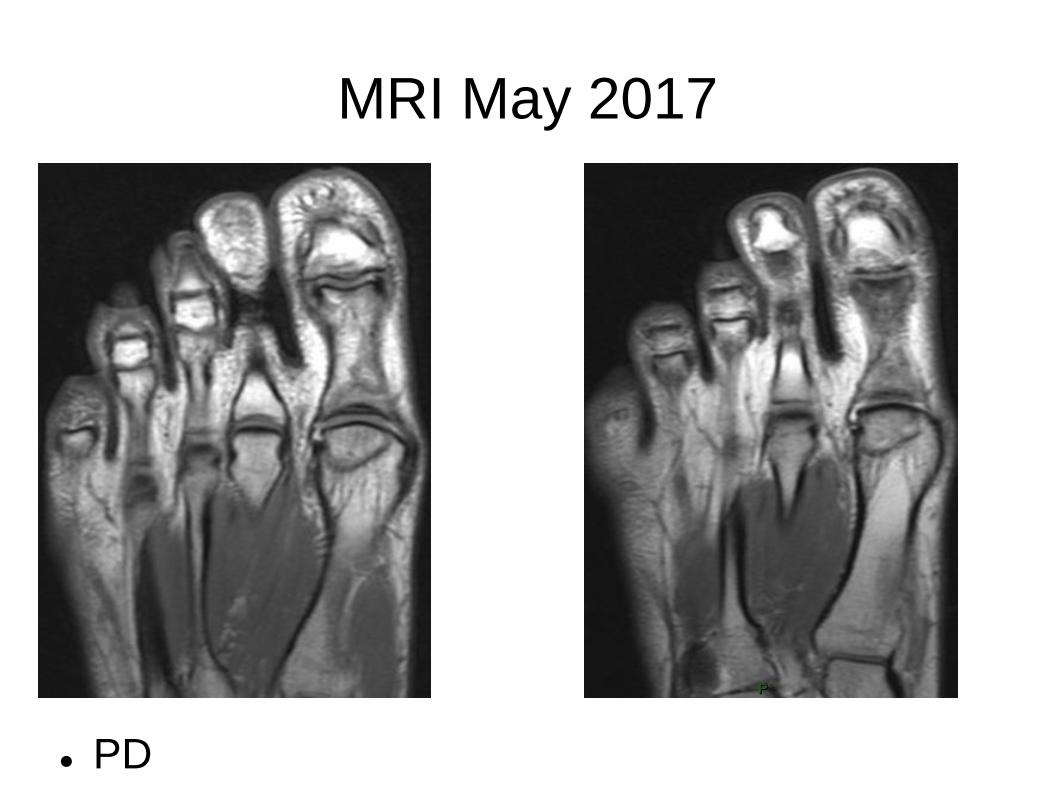
MRI May 2017
PD

PDFS

Abnormal linear signal in metatarsal head.
Serpiginous line in the base of distal phalanx and proximal phalanx.

MRI July 2017


Discussion
Extracorporeal shockwave therapy (ESWT)
Treatment of sports related disorder
Plantar fascitis, lateral epicondylitis, calcified/non calcified SST tendinosis, patellar tendinopathy
Also in treatment of non-union long bone fracture, femoral head AVN.
Shockwave induced tissue repair & regeneration, neovascularization
Usually no severe complication ( local soft tissue swelling, cutaneous erosion, petechial or local subcutaneous hematoma).
One reported complication from ESWT for calcified SST tendinosis, ie AVN humeral head. by Durst et al.
Possible pathomechanism:
Shockwaves cause damage to blood vessels, can result in arterial occlusion, capillary extravasation, or vessel wall ruptured.
Leads to AVN.

Case 8
NCY 29 y.o lady, h/o RTA in 2016.
Sustained laceration wound with foreign body of left shin, surgery done.
C/O left pretibial mass, which is painful after prolonged standing.


Normal

Ultrasound
Tibialis anterior muscle herniation from fascial defect secondary to trauma.
Discussion
Muscle hernia: protrusion of muscle belly through an acquired/congenital fascial defect.
Potentiate by increases in intracompartment pressure ( muscle hypertrophy).
Most commonly in leg, and mostly affected tibialis anterior muscle (its fascia is most vulnerable to trauma).
Clinical:
Anterior tibial mass, vary in size; enlarged during leg dorsiflexion, and smaller at rest.
Dynamic ultrasound:
Muscle bulge through fascia defect on muscle contraction, retraction on relaxation.
THANK YOU!!