multi-center research of small-sized polymyxin b hemoperfusion
DESCRIPTION
Multi-center research of small-sized polymyxin B hemoperfusion. Naohiro Wada Department of Pediatric Nephrology Shizuoka Children’s Hospital Shizuoka, JAPAN. Polymyxin B. Polymyxin B. LPS =Endotoxin Polysaccharide Lipid A. Lipid A. polymyxin B immobilized fiber column. - PowerPoint PPT PresentationTRANSCRIPT

Multi-center research of small-sized polymyxin B hemoperfusion
Naohiro Wada
Department of Pediatric NephrologyShizuoka Children’s HospitalShizuoka, JAPAN
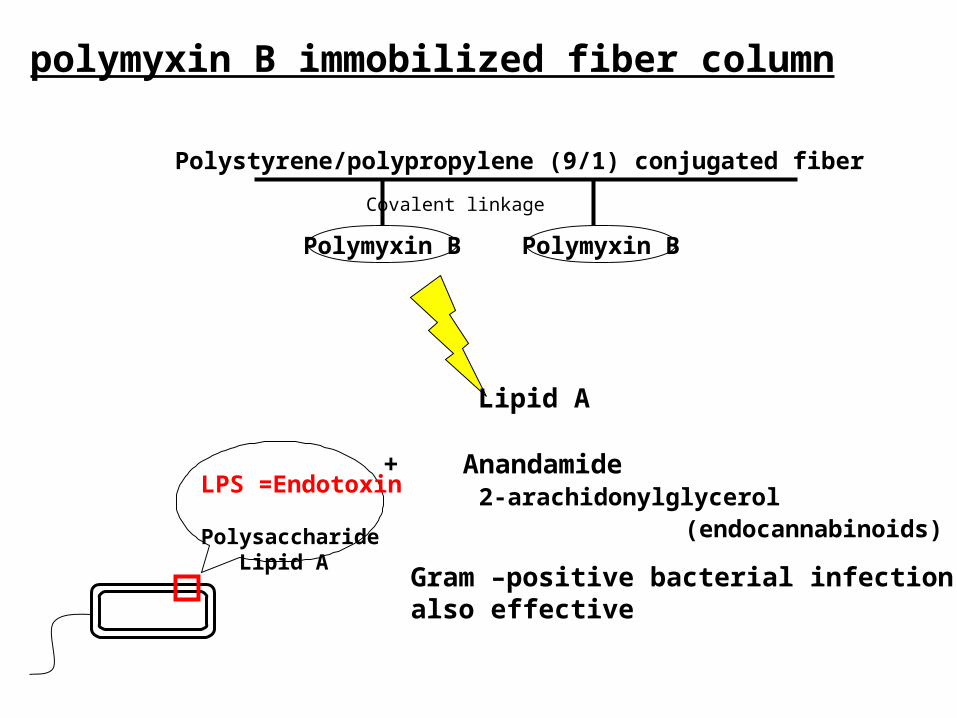
polymyxin B immobilized fiber column
+ Anandamide 2-arachidonylglycerol (endocannabinoids)
LPS =Endotoxin Polysaccharide Lipid A
Polystyrene/polypropylene (9/1) conjugated fiber
Polymyxin B Polymyxin B
Lipid A
Covalent linkage
Gram –positive bacterial infectionalso effective
Crus DN et al (Crit Care 2007;11:R47)
“Effectiveness of polymixin B immobilized fiber column in sepsis: a systematic review” Review : meta-analysis Favorable effect : MAP, dopamine use, PaO2/FiO2 ratio, mortality Consideration : publication bias, lack of blinding
Cruz DN et al (JAMA 2009;301:2445-2452)
“Early Use of Polymyxin B Hemoperfusion in Abdominal Septic Shock. The EUPHAS Randomized Controlled Trial.”
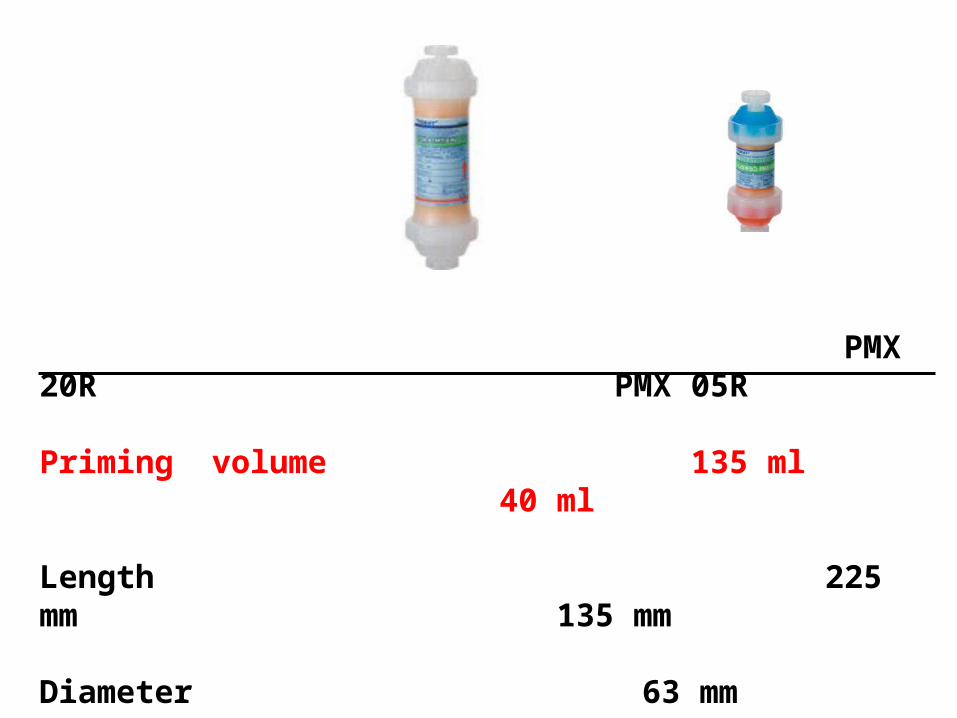
PMX 20R PMX 05R
Priming volume 135 ml 40 ml
Length 225 mm 135 mm
Diameter 63 mm 55 mm
PURPOSE
The effectiveness and safety of small-sized polymyxin B hemoperfusion in the severe septic shock children. Retrospective analysis in three units. Complete count survey in the units.
Units: pICU, Nagano Children’s Hosp. Neonatal section, Kurashiki Central Hosp. Nephrology section, Shizuoka Children’s Hosp.
PATIENSSeptic shock Definitions for sepsis and organ dysfunction in pediatrics (Pediatr Crit Care Med 2005;6:2-8)
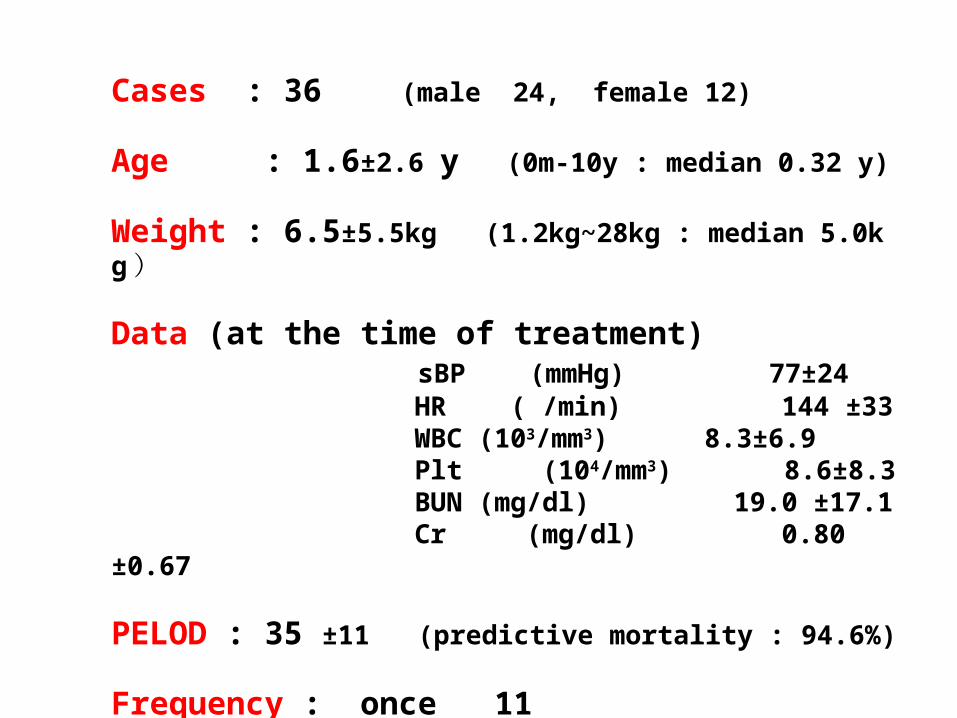
Cases : 36 (male 24, female 12)
Age : 1.6±2.6 y (0m-10y : median 0.32 y)
Weight : 6.5±5.5kg (1.2kg~28kg : median 5.0kg )
Data (at the time of treatment) sBP (mmHg) 77±24 HR ( /min) 144 ±33 WBC (103/mm3) 8.3±6.9 Plt (104/mm3) 8.6±8.3 BUN (mg/dl) 19.0 ±17.1 Cr (mg/dl) 0.80 ±0.67
PELOD : 35 ±11 (predictive mortality : 94.6%)
Frequency : once 11 twice 25

Bacterial culture detected 22 E.coli 2 ( blood 2) Klebsiella 2 ( blood 1 、 ascites 1) Pseudomonas 3 ( blood 2 、 urine 1) Serratia 1 ( blood) MSSA 5 ( blood 5) MRSA 4 ( blood 2 、 sputum 2) GBS 3 ( blood 3 ) Streptococcus 2 ( blood 2 )
Endotoxin ( before treatment )
detected 11 (1-714 : mean 150.6 土 227.4 ; median 49.9) not detected 9 not done 16
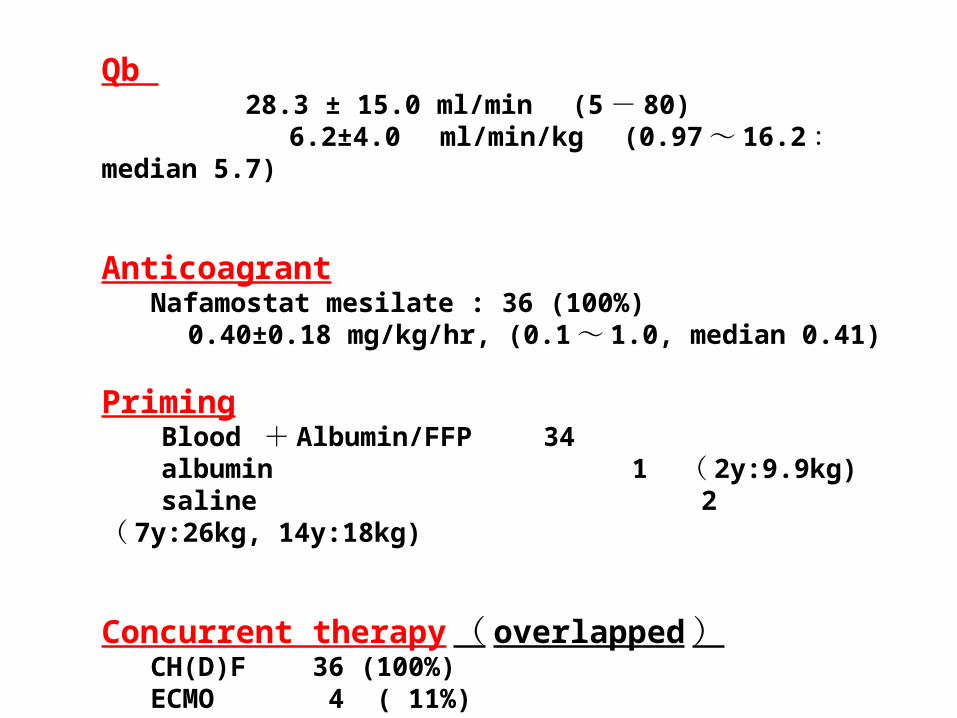
Qb 28.3 ± 15.0 ml/min (5 - 80) 6.2±4.0 ml/min/kg (0.97 ~ 16.2 : median 5.7)
Anticoagrant Nafamostat mesilate : 36 (100%) 0.40±0.18 mg/kg/hr, (0.1 ~ 1.0, median 0.41)
Priming Blood + Albumin/FFP 34 albumin 1 ( 2y:9.9kg) saline 2 ( 7y:26kg, 14y:18kg)
Concurrent therapy ( overlapped ) CH(D)F 36 (100%) ECMO 4 ( 11%)
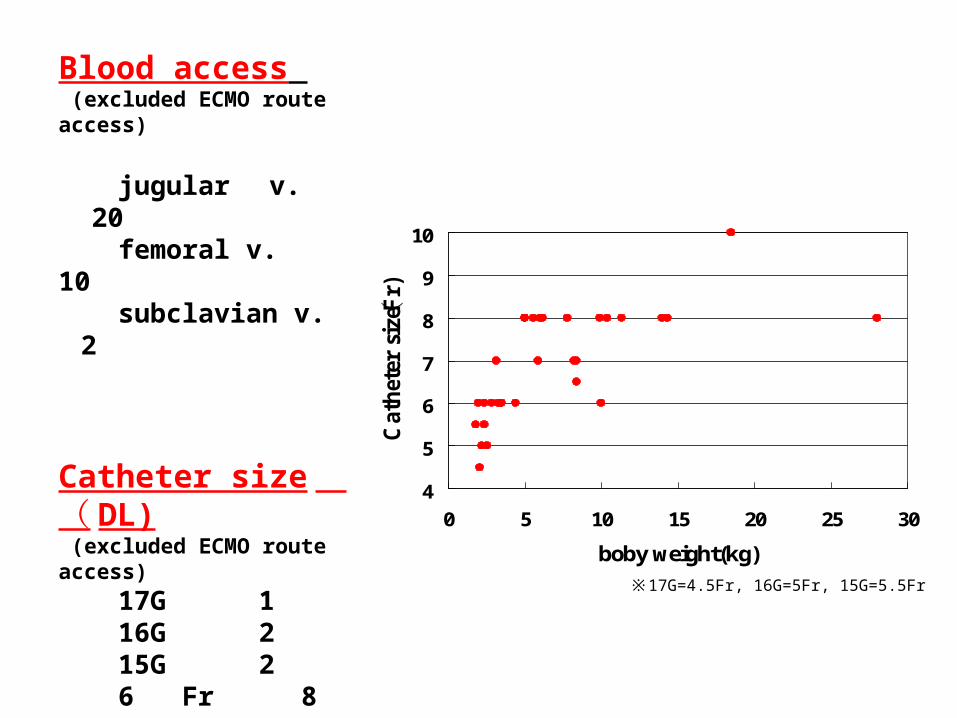
Blood access (excluded ECMO route access)
jugular v. 20 femoral v. 10 subclavian v. 2
Catheter size ( DL) (excluded ECMO route access)
17G 1 16G 2 15G 2 6 Fr 8 6.5Fr 1 7 Fr 4 8 Fr 13 10 Fr 1
※17G=4.5Fr, 16G=5Fr, 15G=5.5Fr
4
5
6
7
8
9
10
0 5 10 15 20 25 30
boby weight(kg)
Ca
thet
er s
ize (F
r)
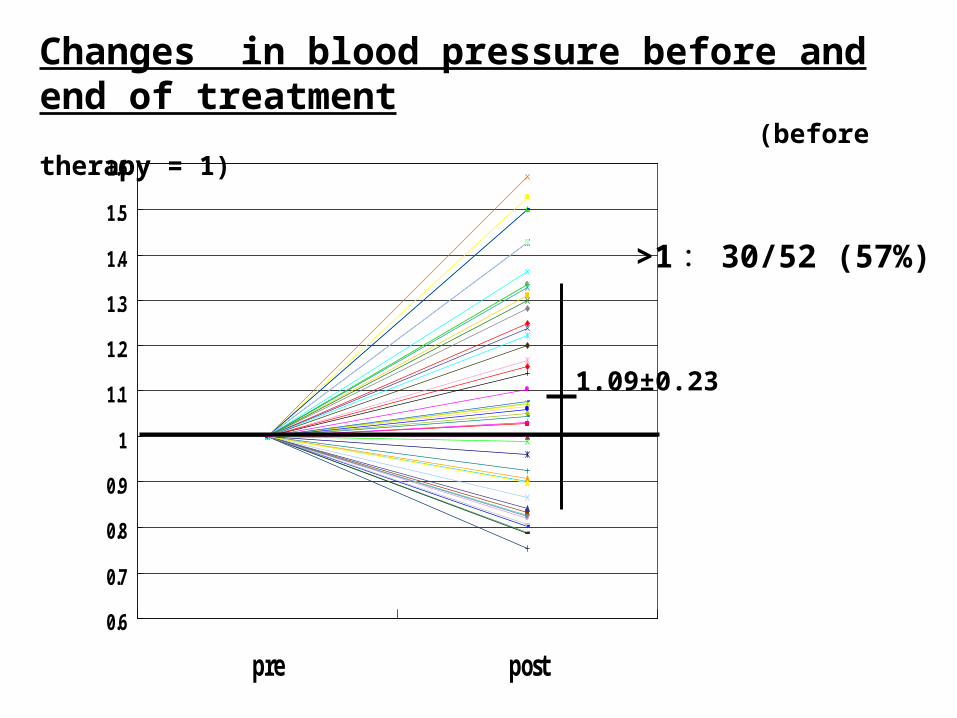
Changes in blood pressure before and end of treatment (before therapy = 1)
0.6
0.7
0.8
0.9
1
1.1
1.2
1.3
1.4
1.5
1.6
pre post
>1 : 30/52 (57%)
1.09±0.23

0.6
0.8
1
1.2
1.4
1.6
1.8
2
pre just afterTx
pre 2nd Tx just after2nd Tx
24hrs afterTx
48hrs afterTx
Changes in blood pressure ( before therapy = 1)
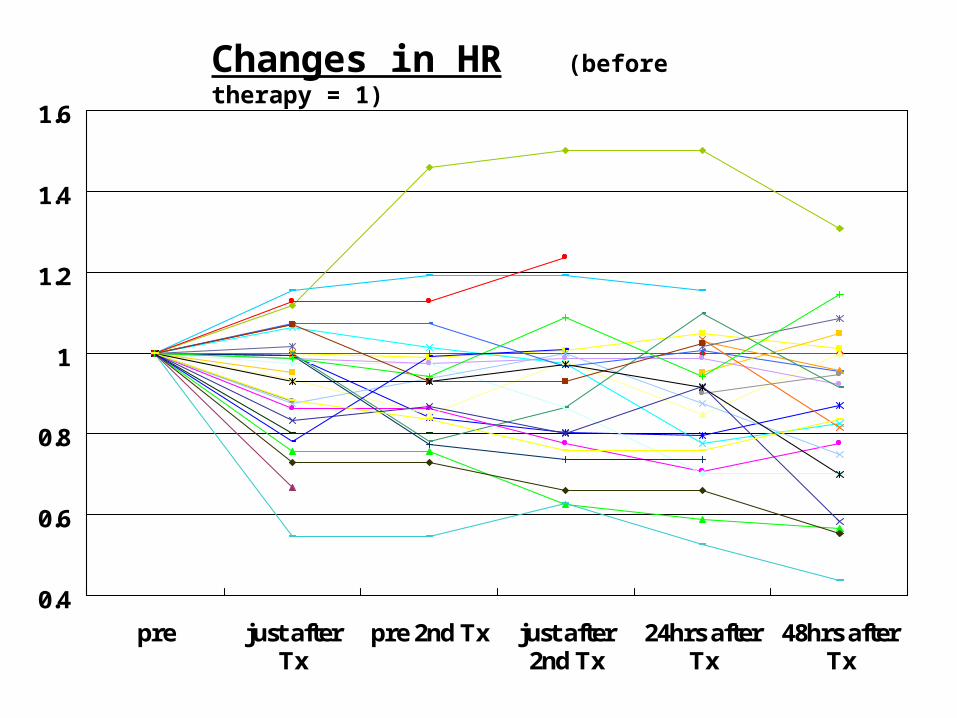
0.4
0.6
0.8
1
1.2
1.4
1.6
pre just afterTx
pre 2nd Tx just after2nd Tx
24hrs afterTx
48hrs afterTx
Changes in HR (before therapy = 1)
0
0.5
1
1.5
2
2.5
3
3.5
pre post
0
1
2
3
4
5
6
7
pre post
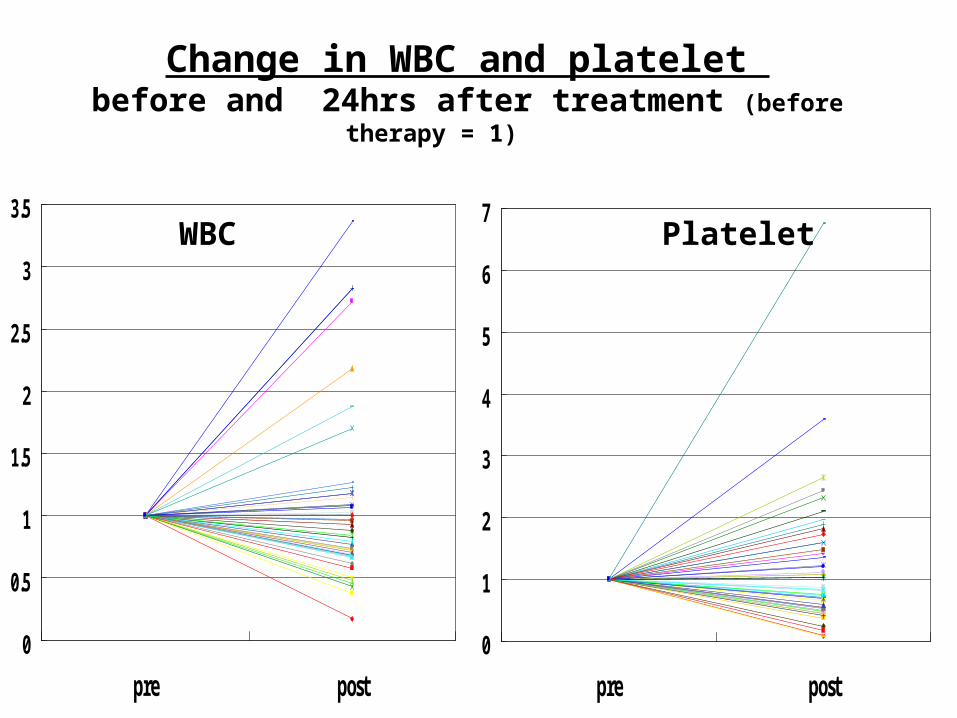
Change in WBC and platelet before and 24hrs after treatment (before therapy = 1)
WBC Platelet
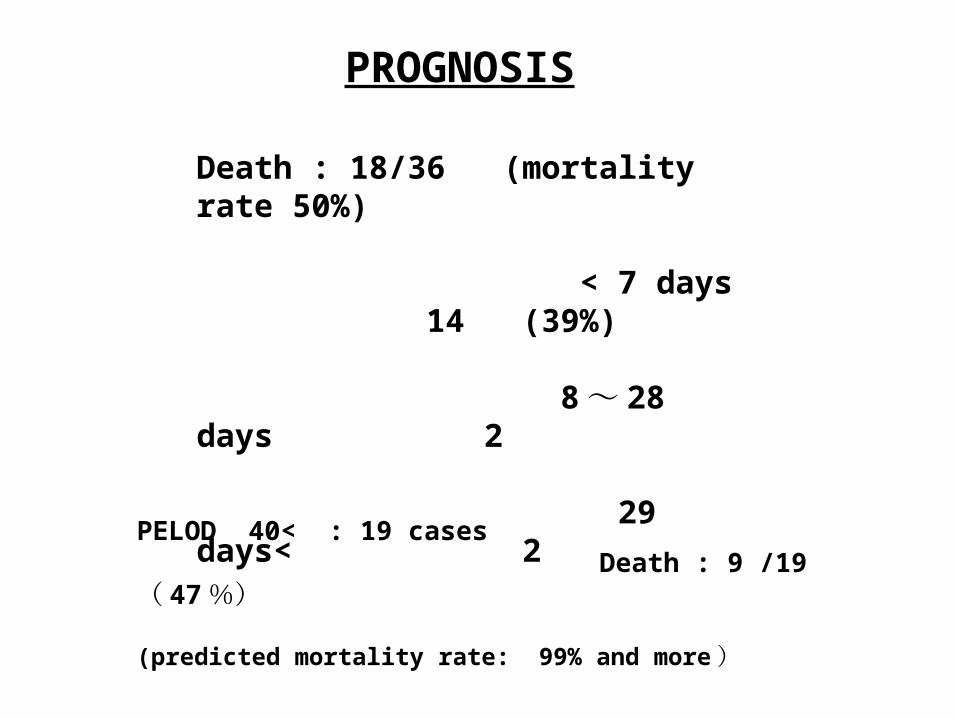
PROGNOSIS
Death : 18/36 (mortality rate 50%)
< 7 days 14 (39%) 8 ~ 28 days 2 29 days< 2
PELOD 40< : 19 cases Death : 9 /19 ( 47 %) (predicted mortality rate: 99% and more )
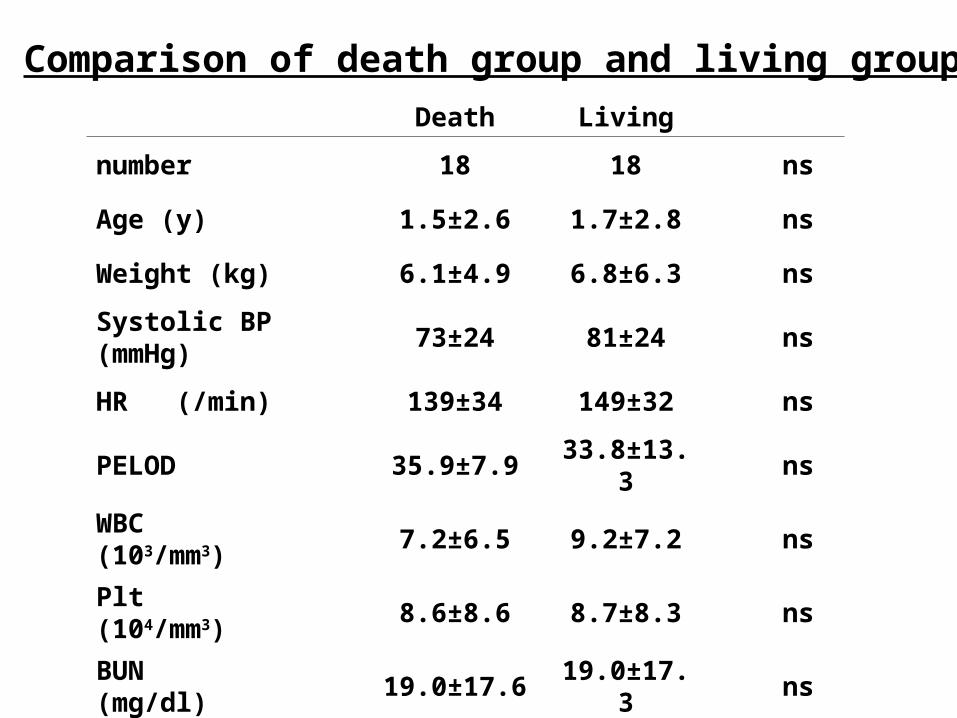
Comparison of death group and living group
Death Living
number 18 18 ns
Age (y) 1.5±2.6 1.7±2.8 ns
Weight (kg) 6.1±4.9 6.8±6.3 ns
Systolic BP (mmHg) 73±24 81±24 ns
HR (/min) 139±34 149±32 ns
PELOD 35.9±7.9 33.8±13.3 ns
WBC (103/mm3) 7.2±6.5 9.2±7.2 ns
Plt (104/mm3) 8.6±8.6 8.7±8.3 ns
BUN (mg/dl) 19.0±17.6 19.0±17.3 ns
Cr (mg/dl) 0.89±0.71 0.72±0.63 ns

Conclusion
Polymyxin B hemoperfusion treatment was possible to be effective to the septic shock children safely even at low body weight and contributed to the prognosis improvement. However, other therapies effect to the mortality, randomized control trial and definite indication are necessary for the effectiveness of polymyxin B hemoperfusion itself.

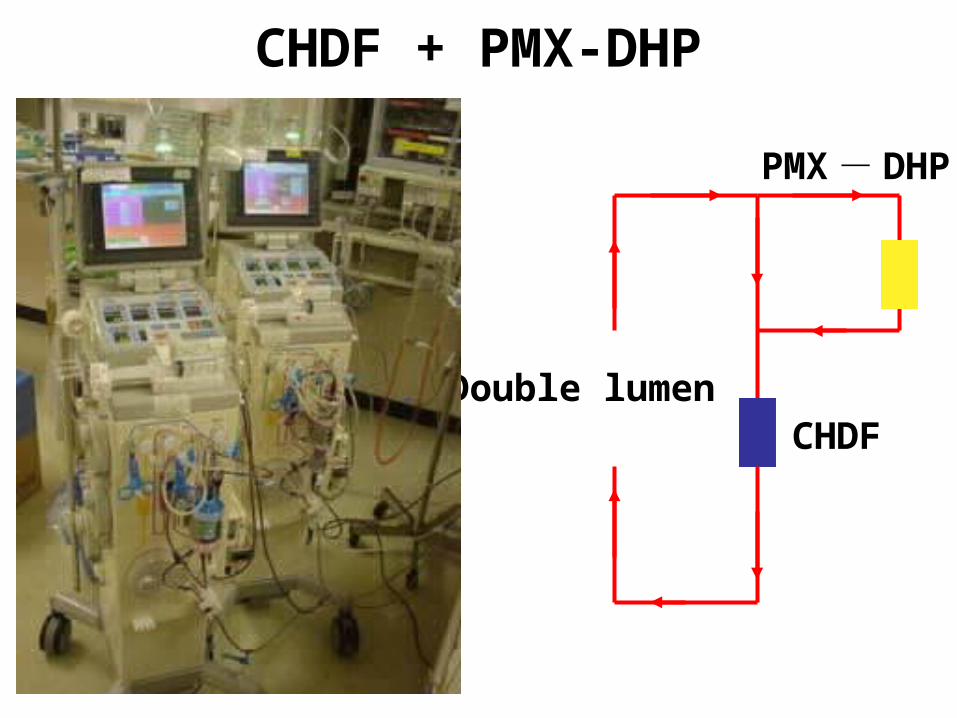
PMX - DHP
CHDFDouble lumen
CHDF + PMX-DHP
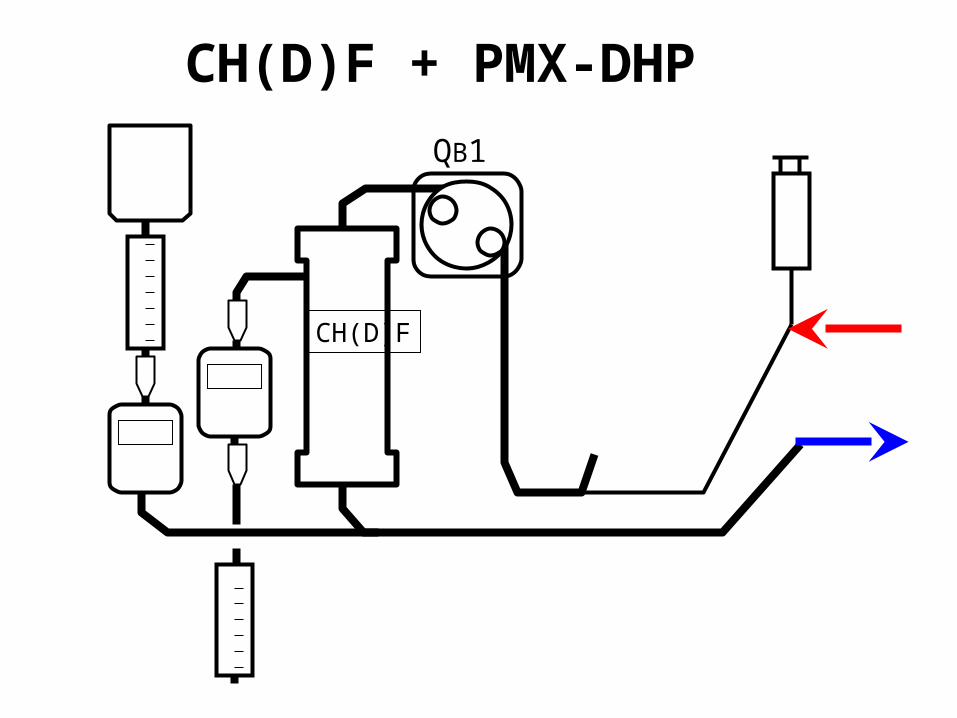
CH(D)F + PMX-DHP
QB1
CH(D)F
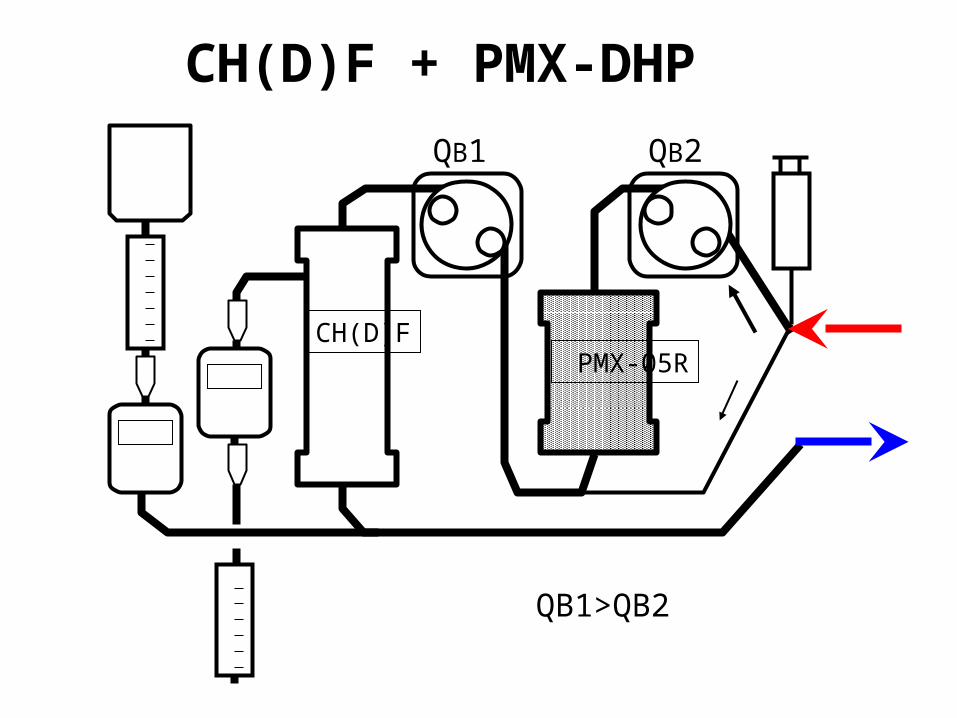
CH(D)F + PMX-DHP
QB1
CH(D)F
QB2
PMX-05R
QB1>QB2
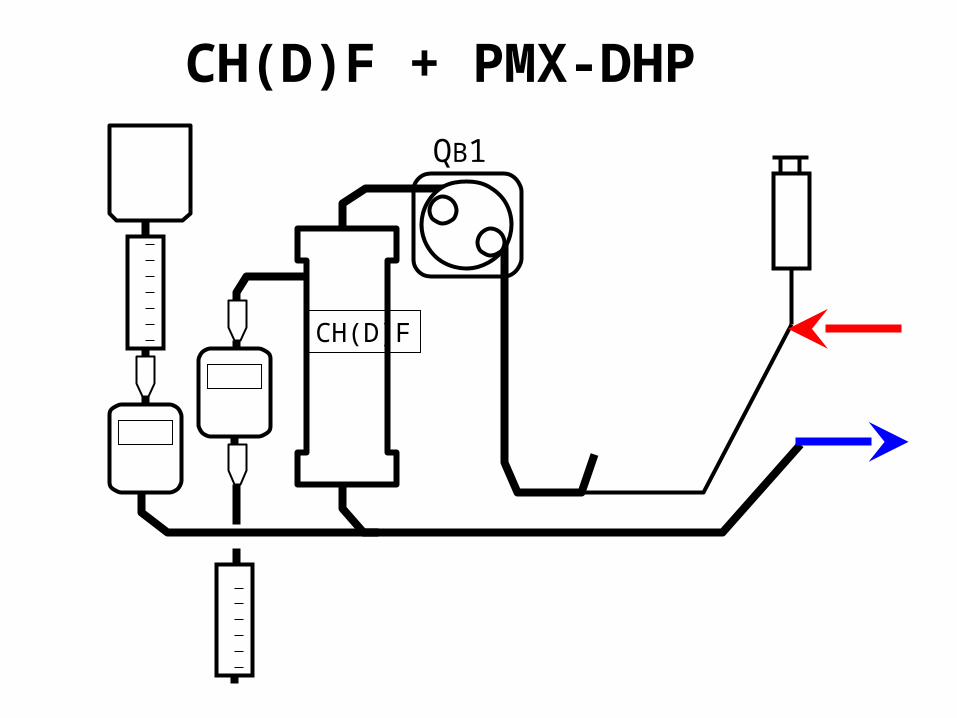
CH(D)F + PMX-DHP
QB1
CH(D)F