myeloma primary care - hgs.uhb.nhs.uk€¦ · myeloma patients in asymptomatic patients without...
TRANSCRIPT

Myeloma Primary Care
Dr R Lovell
Feb 2015

Aims
• Balance of pathophysiology and cases
• Explain diagnostic changes (minimal)
• Staging
• UK influence
• Autologous stem cell transplants
• Primary care myeloma problems

Why I love blood !

Plasma cell differentiation
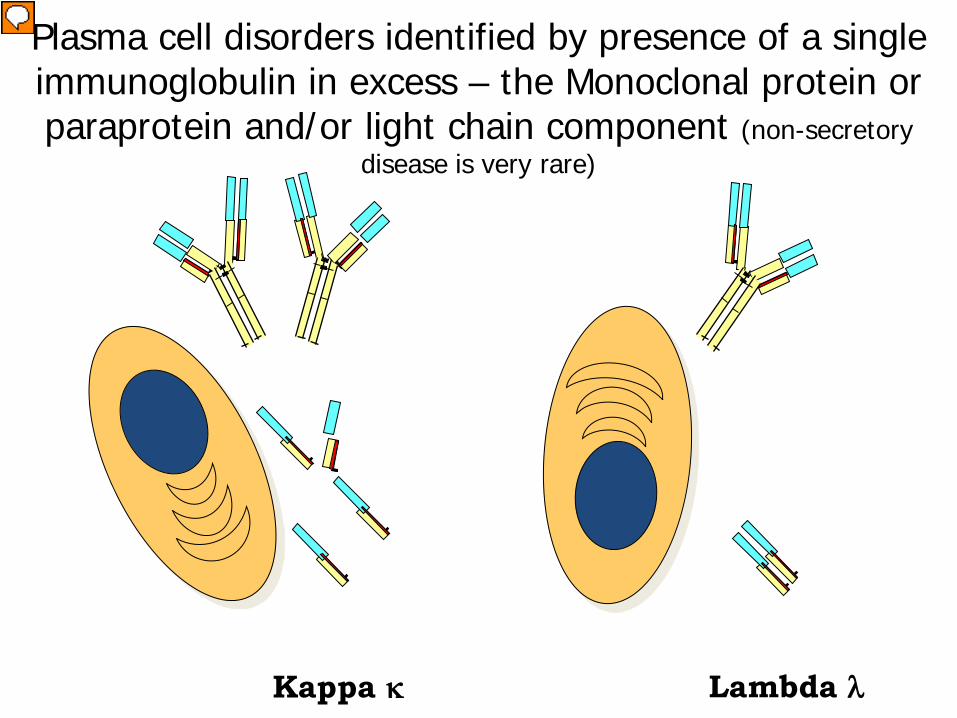
Plasma cell disorders identified by presence of a single immunoglobulin in excess – the Monoclonal protein or paraprotein and/or light chain component (non-secretory
disease is very rare)
Kappa κ Lambda λ
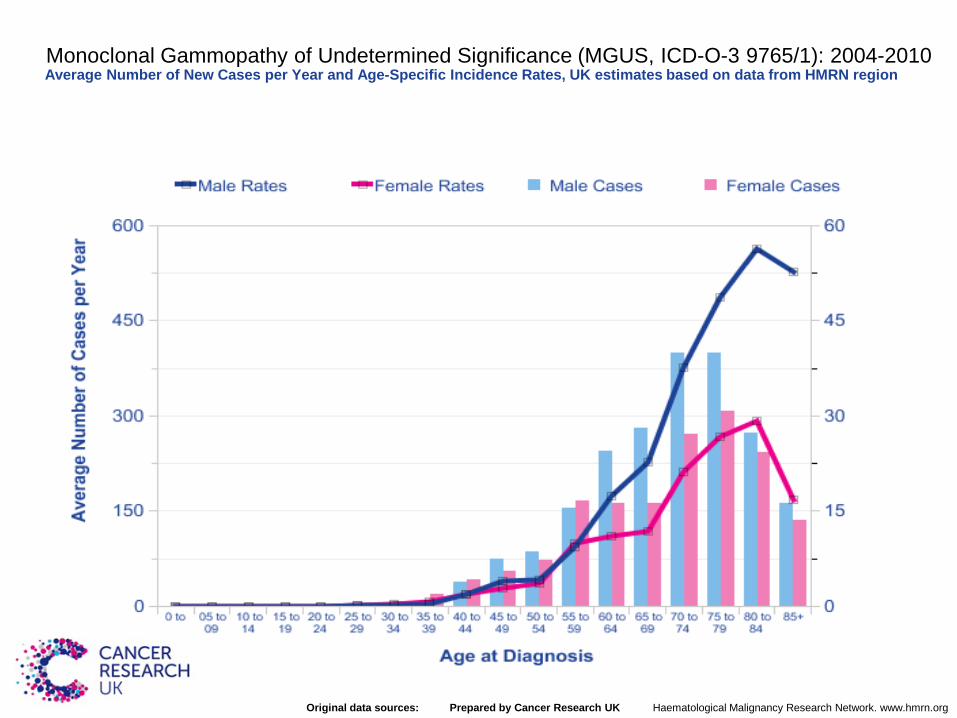
Monoclonal Gammopathy of Undetermined Significance (MGUS, ICD-O-3 9765/1): 2004-2010Average Number of New Cases per Year and Age-Specific Incidence Rates, UK estimates based on data from HMRN region
Prepared by Cancer Research UKOriginal data sources: Haematological Malignancy Research Network. www.hmrn.org

MGUS
• Normal FBC Renal Ca• No bone lesions• Rest of Igs normal
• Paraprotein <30
• SFLC ratio and B2m normal low risk

Monoclonal gammopathy of uncertain significance
No evidence of end organ damage (anaemia, high calcium, renal failure, infection, bone pain or lesion)
Monoclonal protein is less than 30g/L (3g/dL)
Less than 10% plasma cells in the bone marrow
IT IS COMMON AND RELATED TO AGEING (>5% over 80 years of age)
RISK OF PRGRESSION is low = around 1% per year for an individual
RISK OF PROGRESSION stays the same each year
MGUS is associated with an increased infection risk, osteoporosis and rarely with renal disease (monoclonal gammopathy of renal significance)

Light chain only MGUS does exist
15-20% of myelomas are light chain only
Only found if serum free light chains or urine light chain analysis done – THEREFORE rarely found
Approximately 0.5-1% of population >50 years have light chain only MGUS(Dispenzieri et al, 2010)
Rate of progression to myeloma, AL amyloid probably less than that for intact immunoglobulin MGUS (perhaps <0.5% per year)

Mr PS
• Age 72• TATT• Hb 146 Wcc 6.8 PLts 268• Cr, U, Ca2+, all normal• IgG 16 IgA IgM normal• SS OA changes only
• MGUS
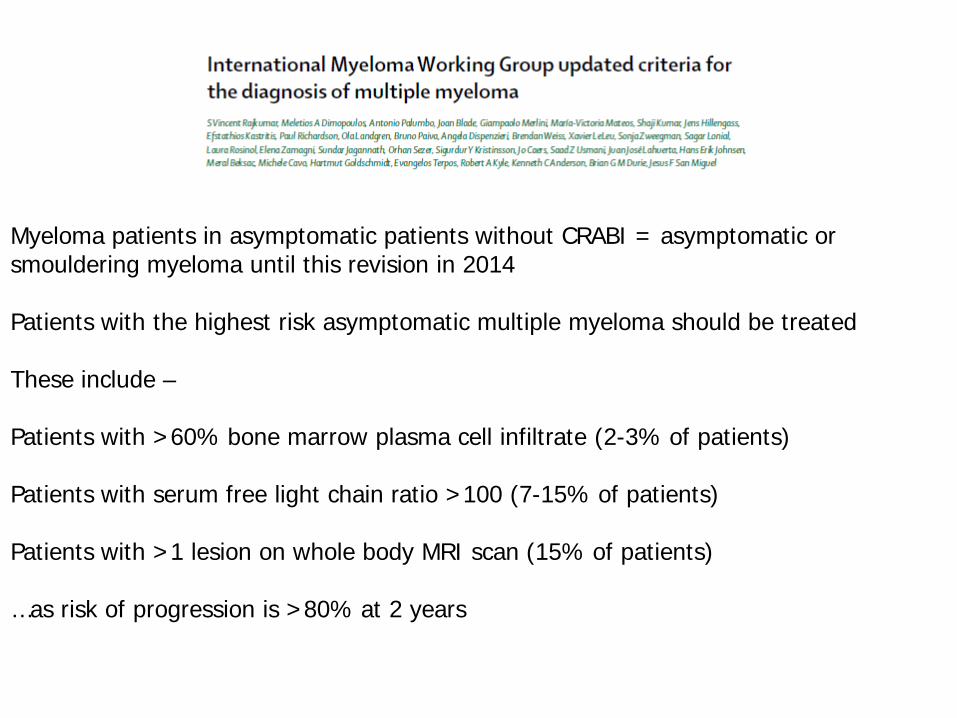
Myeloma patients in asymptomatic patients without CRABI = asymptomatic or smouldering myeloma until this revision in 2014
Patients with the highest risk asymptomatic multiple myeloma should be treated
These include –
Patients with >60% bone marrow plasma cell infiltrate (2-3% of patients)
Patients with serum free light chain ratio >100 (7-15% of patients)
Patients with >1 lesion on whole body MRI scan (15% of patients)
…as risk of progression is >80% at 2 years

Lytic lesion (not sclerotic like breast cancer or other tumours)

Immunoglobulins = laboratory will do serum electrophoresis (and
if find a peak suggestive of a monoclonal protein will do immmunofixation and densitometry)
ANDSerum free light chains (or urine for Bence Jones
protein)
Only exception is rare cases of AL amyloidosis have been reported where FLC only detectable in urine with no abnormality in serum so URINE for FLC needed if AL amyloid suspected but no M-protein or FLC in serum
Urinalysis is not necessary for screening for myeloma
Screening for plasma cell disorders

50.6% of myeloma patients visited their primary care doctor three or more times before hospital referral in
the UKAt least 33% present via emergency admission
Often a delay in suspecting myeloma

Myeloma pathophysiology

Myeloma
• 2nd commonest haem malignancy • Longest delays in diagnosis• Indolent• Malignant growth plasma cells• Plasma cells terminally differentiate B cells• Paraprotein • Increase light chains• Bone destruction • Renal failure• Bone marrow failure (low Hb low WCC low Plts)• Spectrum of disease MGUS vs PCL • Still incurable • Rates increasing

Bone disease and destruction (40-70%)
• Osteoclast activity is increased, causing increased reabsorption
• Osteoblast activity is decreased and cannot keep up with the osteoclast activity.
• This results in lytic lesions and hypercalcaemia• NB cytokines implicated in the above not only
increase osteoclast activity but also stimulate myeloma cell growth

Myeloma

Anaemia, fatigue and infection 10-60%
• Physical inhibition of normal haemopoesis
• Myeloma cells secrete inhibitory cytokines (TNF, IL-1) also contributing
• Leucopenia
• Aetiology of fatigue is not fully understood but it can be caused by anaemia, renal failure, psychological factors. It is not relieved by rest


Myeloma diagnosis minor changes
• Plasmacytosis in marrow (if >60% nil else)• Paraprotein / SFLC• End organ damage
• CRAB
• New parameters for bone lesions and cut offs for SFLC

International staging system
Stage III=B2m >5.5Stage II= not othersStage I=B2m <3.5 Alb >35JCO MAY 20, 2005 VOL. 23 NO. 15 3412-3420

Myeloma (C90): 2009-2011 Average Number of New Cases Per Year and Age-Specific Incidence Rates per 100,000 Population, UK
http://info.cancerresearchuk.org/cancerstats/faqs/#How Prepared by Cancer Research UK - original

Myeloma (C90): 1975-2011European Age-Standardised Incidence Rates per 100,000 Population, by Age, Persons, Great Britain
http://info.cancerresearchuk.org/cancerstats/faqs/#How
Treatments
• First line
• Stem cell transplantation
• Radiotherapy
• Second/third line treatments
• Maintenance
• Supportive care
• Novel therapies

Bisphosphonates
• Bisphosphonates– Relieve pain by binding to the bone surface,
reducing destruction and may aid repair
– Gold standard IV Zolendronate
– Dose adjust in renal failure
– Clear evidence from MM IX trial has an anti-myeloma effect

NICE?

Myeloma NICE
• The good the bad and the ugly
• Messed with myeloma from the start
• Mostly helped standardised use of novel agents
• Draft guidelines Nov 2014


Myeloma
• Over 4,500 new myelomas are diagnosed each year in the UK. A full time GP is likely to diagnose approximately 2-3 people with myeloma in their career.
• Five year survival is nearly 50%. • They looked at all symptoms in elderly >60yrs• No common single factor• When combined with hypercalcaemia OR leucopenia
often correlation• Offer very urgent electrophoresis <48hrs !!

Myeloma my clues
• Bone pain/fracture high Ca = myeloma• Renal failure high calcium = myeloma• High protein low albumin = paraprotein• Low / suppressed IGs = myeloma OR severe
cachexia
• Cost Igs screen = £1 rest of tests 80p• Cost of Lenalidomide 1 year £52 K !
JF
• Presented in Oct 2001 to A&E with
Acute renal failure
Extensive bony pains throughout the body
Fatigue

JF
• Investigations showed
Hb:4.0 WBC:9.6 N:6.8 PLT:442
Urea:54 Creat:1172 K:5.7
Ca:2.6 B2M:32 Alb:40

JF
• No paraprotein detected
Urine for BJP +
Skeletal survey : multiple lytic lesions
BMA: 50% plasma cells
Diagnosis: Multiple Myeloma

JF





JF
• HD
• R femoral nailing
• Intensive chemo
• Bisphosphonate
• DXT
JF
• 4x bolus VAD
• July2002 PBSCHarvest
• 3/12 Cyclophosphamide
• Relapsed March04
• Reinduction 2xVAD
• Mel140 PBSCT
• 2nd plateau

JF
• Monitored with serum free light chain assay
• Remission for almost 20 months
• Relapsed February 2006
• Started Melphalan reduced dose-poor response

JF
• DXT for shoulder pain
• Thalidomide and Dexamethasone no significant improvement
• Recently added cyclophosphamide
• PCT have turned down Velcade

Light chain assay
0
2000
4000
6000
8000
10000
12000
date
kap
pa a
nd
lam
da
0
200
400
600
800
1000
1200
k/l
rati
o klk/l
k 2153 476 457 10493 5429 3113 1435 129 71.2 32.17 32.5 39.79
l 25.22 30 13 10.93 415 13 22.58 53 54.26 45.42 32.89 42.15
k/l 85.9 15.7 25 1009.913 415.69 237.271 63.552 2.5 1.312 0.7 0.98 0.94
7-Apr 11/11/2006
9/9/2006 8/8/2006 7/7/2006 5/5/2006 1/1/2006 9/9/2005 4/4/2005 12/12/2004
11/11/2004
10/10/2004

Conclusions
• Light chain myeloma 15% of myeloma patients• Renal failure 80%• Serum free light chain assay important• JF ISS 3 predicted survival 29/12• JF now survived 72/12

Conclusions
• Incurable terminal disease
• Auto PBSCT used for disease control not curative
• VAD followed by SCharvest was gold std
• Relapse treatment

Overall survival from diagnosis of multiple myeloma.
Kumar S K et al. Blood 2008;111:2516-2520

Induction
• Aim get the best remission with least toxicity• Why CR patients have longer PFS OS
• MM XI• Bortezomib based
• Pethema group high risk• Meta analysis suggests benefit
• DTPACE for PCL

Why auto ?History MM VII
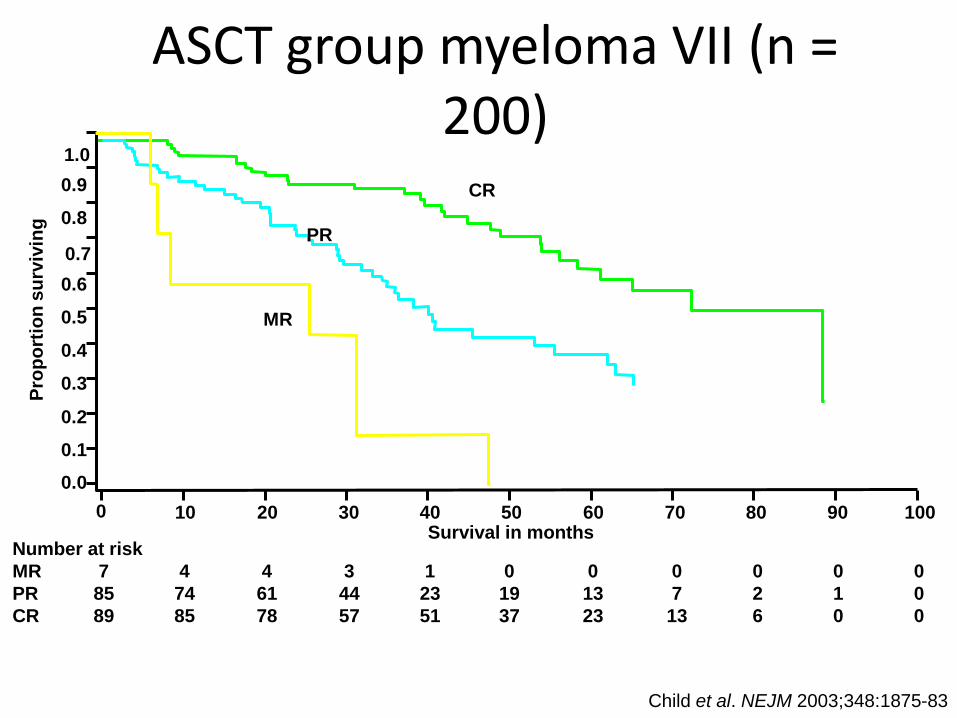
ASCT group myeloma VII (n = 200)
Child et al. NEJM 2003;348:1875-83
Prop
ortio
n su
rviv
ing
Survival in months
0.0
0.1
0.2
0.3
0.4
0.5
0.60.7
0.8
0.91.0
0 10 20 30 40 50 60 70 80 90 100
MR
PR
CR
Number at riskMR 7 4 4 3 1 0 0 0 0 0 0PR 85 74 61 44 23 19 13 7 2 1 0CR 89 85 78 57 51 37 23 13 6 0 0
0%
20%
40%
60%
80%
100%
Induction:CVAD
Induction:CTD
Day 100:CVAD
Day 100:CTD
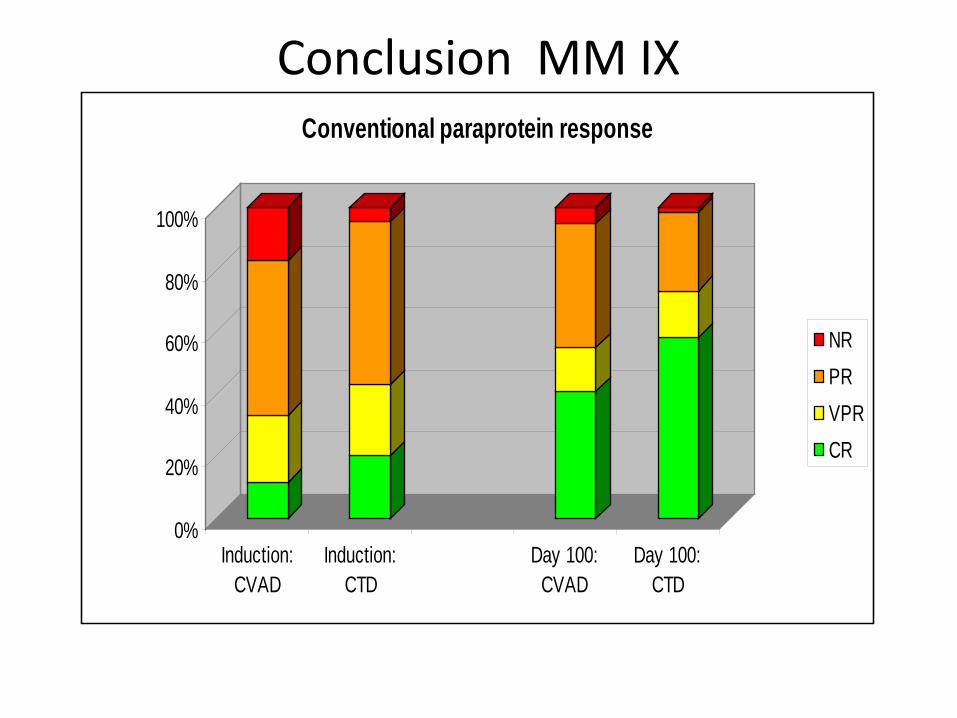
Conventional paraprotein response
NRPRVPRCR
Conclusion MM IX

Myeloma IXCTD non-inferior to CVAD for PFS and OS.
Morgan et al 2012 Haematologica
Maintenance / Consolidation
• Zolendronic acid
• sCR CR VGPR MR SD• Toxicity vs. efficacy
• Nordic group Bortezomib• Thal meta analysis• Lenalidomide await M XI
• Safety / QOL leave this area unclear
Maintenance in Myeloma: Still a Work in Progress?
• Provides PFS advantage– Longer follow-up needed
• OS improvements noted
• Toxicities of treatment– Myelosuppression
– Second primary malignancies
– Quality of life
• Unknown response to higher doses of lenalidomide at relapse; potential development of resistant clones
• Observation is still an option
• Unclear whether all patients benefit from maintenance– Tailor treatment choice to
individual patient
Van de Donk N, et al. Cancer Management Res. 2012;4:253-268.
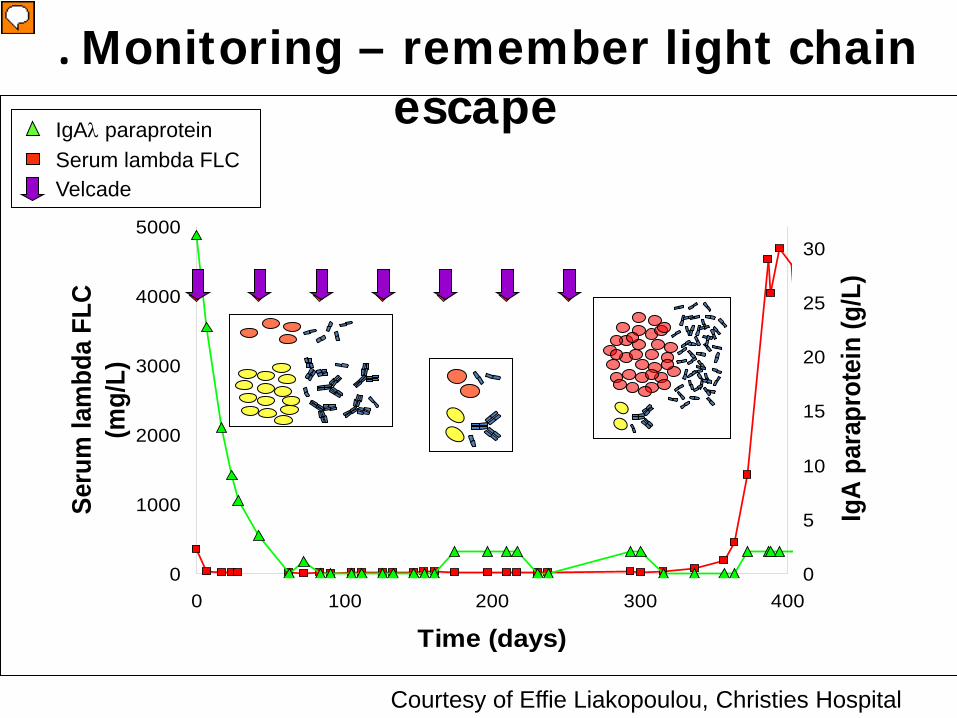
a. Monitoring – remember light chain escape
0
1000
2000
3000
4000
5000
0 100 200 300 400
Time (days)
Seru
m la
mbd
a FL
C (m
g/L)
0
5
10
15
20
25
30
IgA
para
prot
ein
(g/L
)
Serum lambda FLCVelcade
IgAλ paraprotein
Courtesy of Effie Liakopoulou, Christies Hospital

2nd Auto why ?MM X

History
• 61yr male ISS Stage 2 MM
• CTD x2 in MM9
• Increasing SOB
• O/E Sats 92% Temp 38



Answers
• CMV 220000 copies /ml blood
• Bronchoscopy CMV lavage
• Treated Ganci 14/7
• Complete resolution

Myeloma & CMV
• Little known in detail
• Not routinely monitored / screened
• Up to 50% of late non neutropenic fevers post auto can be CMV viraemia

Primary care
• Lenalidomide – LFTs, diarrhoea, SCC secondary malignancies
• Carfilzomib– LVF
• Dexamethasone– Usual but 40mg per day
• Cyclophosphamide– Usually well tolerated low counts N&V
Conclusion
• Think myeloma• Over 4,500 new myelomas are diagnosed each year
in the UK. A full time GP is likely to diagnose approximately 2-3 people with myeloma in their career.
• Five year survival is nearly 50%. • Simple tests BUT at all answers• Cheap and easy often automated
• Any questions !!