neonatal sepsis author: sherrill roskam rnc mn nnp cns updated presentation: susan greenleaf rnc,...
TRANSCRIPT
Neonatal Sepsis
Author: Sherrill Roskam RNC MN NNP CNSUpdated presentation: Susan Greenleaf RNC, BSN
Objectives
Identify major causative organisms and routes of transmission of sepsis.
Discuss clinical manifestations and modalities used in diagnosis of sepsis.
Describe antibiotic therapy used in the treatment of neonatal sepsis.
Sepsis
Definition: A systemic response to an invasive organism. Frequently signified by a positive blood culture.A systemic illness due to the presence of bacteria and or bacterial toxins in the blood
Neonatal Immune System
Sepsis occurs in 1-8:1000 term infants and 1:250 premature infantsNeonates are immunocompromised even at term gestationThe neonatal immune system is functional at birth, but not mature
Sepsis
Two types of sepsisEarly-onset sepsis, with in the first 72 hours of lifeLate-onset sepsis, those infections acquired later by horizontal transmission. Highest risk for the first month of life

Predisposing Factors: Pregnancy
PrematurityPROM < 36 weeksProlonged ROMProlonged laborExcessive manipulation
Predisposing Factors: Maternal
History of infectionBacterialViral
History of GBS bacteriuriaHistory of previously affected infantTemperature in labor
Predisposing Factors: Neonatal
Invasive proceduresResuscitationIntubationIV starts / PICC linesUmbilical Catheterization
Skin colonization
Predisposing Factors: Nursery
HumidifiersRespiratory therapy equipmentStaff membersUnsterile equipment
ScalesStethoscopesThermometers

Transmission
TransplacentalAscendingBirthNosocomialAntibodies
IgGIgMIgA

Human Immunoglobulins
Antibodies are the immunoglobulins produced in response to specific antigensIgG is the only antibody that crosses the placenta and provides immuological protection over the first few months Transfer peaks at 32 weeks gestation
Immunoglobulins cont.
IgM and IgA are directly responsible for antibodies against bacteriaNeonatal IgM production starts at 30 weeks gestation and increases over the first year of lifeIgA passes through breast milk to provide early defense against infection. Found in the intestinal tract.
Causative Organisms:Bacterial
Group B strepE ColiHaemophilus InfluenzaeCoagulase Negative StaphStaph AureusNeisseria MeningitisListeria

Causative Organisms: Viral Maternal in origin
ToxoplasmosisRubellaCytomegalovirusHerpesHepatitis BHIV
Recognition: Clinical Signs
Temperature instabilityLethargyPallor, mottling, poor cap refillRespiratory distressPoor feedingApneaNeurologicJaundiceHypoglycemia
Recognition
Recognition is of utmost importance, because newborns with sepsis can get very sick very fastBe aware of risk factors – review maternal history

Diagnostic tests for sepsis
CBCCultures
Blood ~ Most common Gold StandardUrineSurface - only indicates colonization
CSF Lumbar punctureCRP
C-Reactive Protein
What is CRP?Laboratory test that identifies an inflammatory response in the body.
Binds to Calcium and phosphocholine sites; forming CRP-ligand complexes.
CRP
CRP’s unique binding characteristics have led to the identification of elevated CRP levels in over 70 different infectious and noninfectious disorders.It is associated with acute and chronic inflammatory disorders.
CRP Continued. . .
Paired mother and infant sampling shows that CRP does not cross the placenta.
4 types of inflammatory response to tissue injury
Infectious, noninfectious, chemical, physical or immunologic toxins.
Use of CRP
2 schools of thought
Early diagnostic tool for confirming sepsisScreening tool to r/o the presence of sepsis
CRP Levels: What is normal?
In the neonatal period: Level of 10mg/L is considered normal
Healthy full-term and preterm infants may range from 2 to 5mg/L during the first few days of life.
More than 1 Level?
Conflicting information about obtaining more than one level
Serial CRP levels drawn 12 to 24 hours after onset of S/S of sepsis may be superior to a single level.
More About the CBC: WBC
White cell countDifferential
Neutrophils - bacteria fighting cellsPolys, Segs - most matureBands - immatureMetas – really immature
Absolute Neutrophil CountI:T Ratio

White Blood Cells
The main defense against invading microorganismsNeutrophils (pack man cells) and macrophages(monocytes)
Circulating cells that migrate to sites of inflamation, ingesting and killing foreign material or bacteria (phagocytosis)Small stores in neonates, not as effective in killing bacteria, quickly depleted
Differential of the WBC
Mature Neutrophils – SegmentedImmature Neutrophils – BandsMonocytesBasophilsEosinophilsLymphocytes
Neutrophils
As mature neutrophols (polys, segs, neuts, or PMNs) are mobilized and consumed in the presence of a pathogen, their numbers decrease and immature cells are released from the bone marrow.Immature neutrophils (bands, metas or stabs)

Absolute Neutrophil Count (ANC)
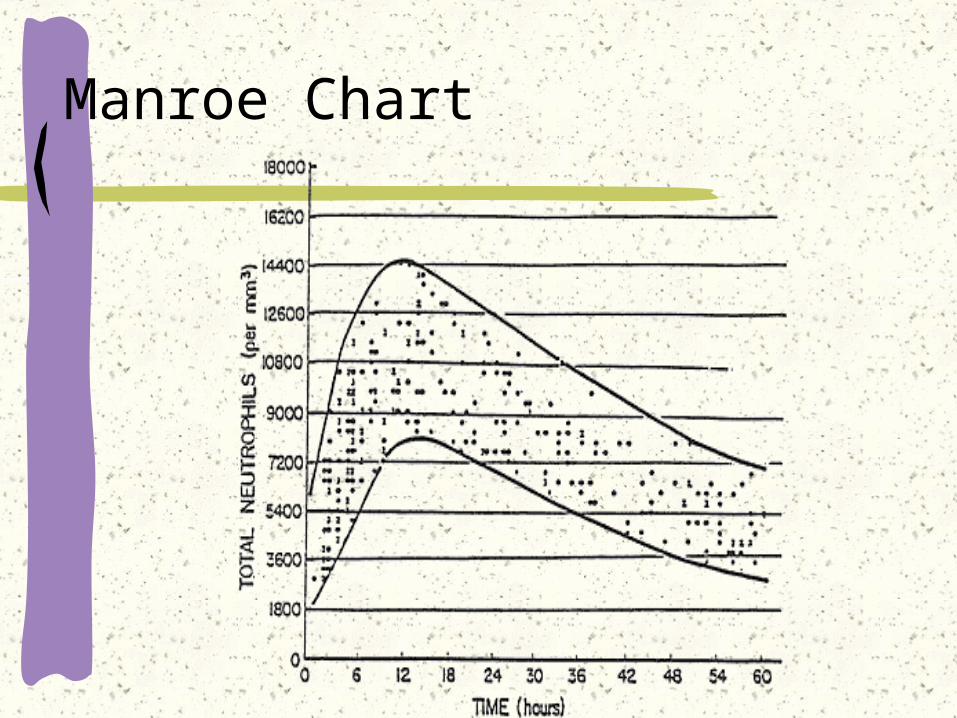
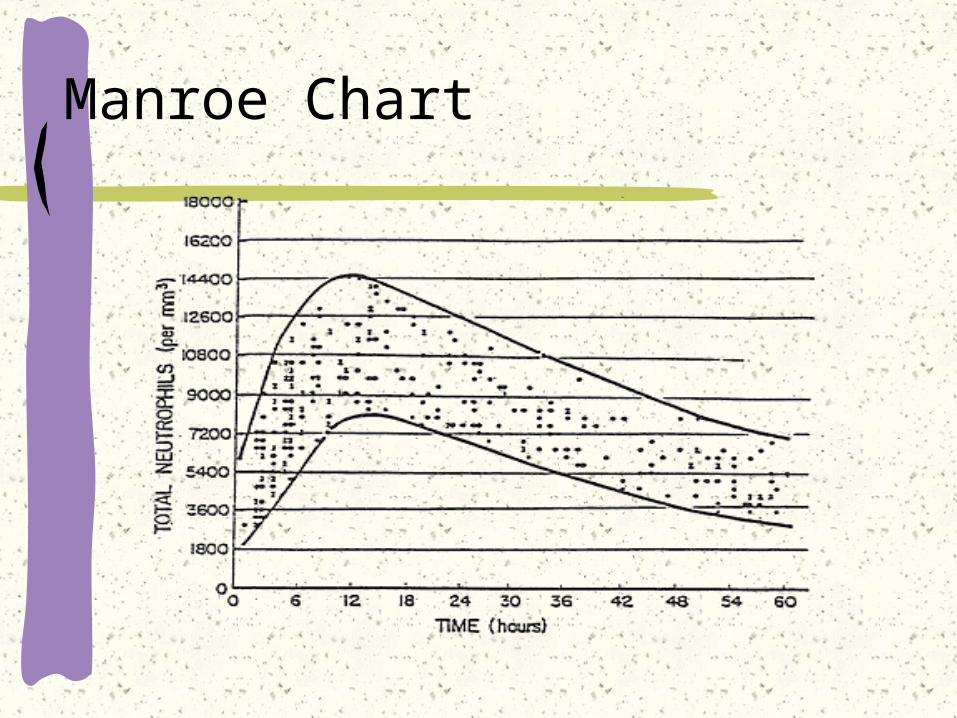
Helps determine how many neutrophils are available to fight bacterial infectionsPremature infants have lower ANC than term infantsMust plot on the Manroe chart
How to calculate an ANC
Identify the immature and the mature neutrophils on the CBC.Add the segs, bands and metas ( total number of neutrophils) together and turn it into a percentageMultiply this number by the total WBC This resulting number is the ANC
Manroe Chart
WBC: 20,000Differential is expressed as a percent of
total white cellsPoly’s (Segs, Neuts): 48%Bands 12%Lymphs: 20%Monos: 17%Eso: 3%
ANC: Absolute number of neutrophils WBC X % Neutrophils
ANC WBC X % Neutrophils20,000 X .6 (60%) = 12,000
Manroe Chart

Immature to Total Ratio (I:T)
An Increased IT ratio is called a left shift. It show an increase in the number of immature sellsAn IT ratio of >.25 may indicate sepsis
I/T ratio: Ratio of immature to total neutrophils
___Bands + Meta___ Polys + Bands + Meta
WBC: 20,000Differential is expressed as a percent of
total white cellsPoly’s (Segs, Neuts): 48%Bands 12%Lymphs: 20%Monos: 17%Eso: 3%
I/T ratio: Bands + Metas Polys + Bands + Metas12/60=0.2 (not indicative of sepsis)
If WBC 3000 Polys 30 and Bands 15: 15/45=0.33 (indicative of sepsis)3,000 X .45 (45%) = 1,350

Platelet Count
Normal Values
VLBW – 275,000 +/- 60,000Preterm – 290,000 +/- 60,000Term – 310,000 +/- 60,000
Infants with infection may have a low platelet count
Management
Support SystemsNeutral Thermal EnvironmentMonitor
Cardiac/RespiratoryPulse Oximetry
Vital signsFeedingsIV
Management (con’t)
AntibioticsAmpicillin 50-100 mg/kg/dose IV q8-12 hours
Varies with gestation and age
Gentamicin 4 mg/kg/dose IV q24-48 hoursVaries with gestationGive over 30 minutesMonitor Gent levels
AntiviralAcyclovir 20 mg/kg/dose IV q8
Give over 1 hourDo not refrigerate

Prognosis
Prognosis depends on organism involved and when treatment started
A bit more practice
CBC resultsWBC 10.4Metamyelocytes 0Band Neutrophils 14Segmented neutrophils 5Platelets 141,000
What is the ANC and the IT ratio?

CBC Practice
CBC resultsWBC 1.3Metamyelocytes 2Band Neutrohils 17Segmented Neutrophils 42Platelets 262,000
Calculate the ANC and IT ratio
CBC Practice
CBC resultsWBC 6.3Metamyelocytes 6Band Neutrophils 44Segmented Neutrophils 23Platelets 95,000
What is the ANC and the IT ratio?
Same patient, 6 hours later
CBC resultsWBC 0.8Metamyelocytes 2Band Neutrophils 4Segmented Neutrophils 2Platelets 24,000
What is the ANC and IT ratio?
References
Behrman, R. E., Kliegman, R.M.,Editors (1998) Nelson Essentials of Pediatrics, 3rd Ed. Philadelphia: W.B. Saunders Co.
Cloherty, J.P., Eichenwald, E.C., Stark, A.R. (2004) Manual of Neonatal Care, 5th Ed. Philadelphia: Lippincott, Williams & Wilkins.
Hengst, J.M., The Role of C-Reactive Protein in the Evaluation and Management of Infants with Suspected Sepsis. Advances in Neonatal Care. 2003;3(1):3-13.
References
Karlsen, K.A. (2001) The S.TA.B.L.E. Program: Transporting Newborns the S.T.A.B.L.E.Way, Learner Manual, 8th Ed.
Merenstein, G.B., Gardner, S.L. (2002) Handbook of Neonatal Intensive Care, 5th Ed. St. Louis:Mosby Inc.