neurological problems and management
TRANSCRIPT

8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 1/52
ACUTE AND INTERMEDIATE PHASE NURSING IN
TBI: NEUROLOGICAL AND OTHER ROUTINE
NURSING INTERVENTIONS: ASSESSING VITAL
NEUROLOGICAL SIGNSAssessing Vital Neurological Signs frequently and looking for
deviation trends (stability, deterioration, or improvement)
• Perform an initial baseline assessment and frequent subsequent
assessments:
o Every 5 - 15 minutes for unstable patients
o Every 2 - 4 hours after patient is well stabilized
Onset of cerebral herniation and new intracranialhemorrhage are the major life threatening problems
associated with acute deterioration• Include the following in the neurological assessment:
o Level of consciousness
Orientation to time, place, and person is
assessed in patients who can respond verbally
Glasgow Coma Score is used in patients who arecomatose
o Cognition
Assess by asking simple questions, e.g., "showme 2 fingers", in patients who can respond
verbally
Glasgow Coma Score is used in patients who arecomatose
o Brain stem function
Pupil assessment for any change in size or reaction; e.g.
1 pupil becomes dilated and
progressively nonreactive to light as aresult of transtentorial herniation or a
focal lesion
an oval or ovoid pupil is usually an early
sign of transtentorial herniation.
The automated pupillometer is more accurate
and reliable than the manual examination in
measuring pupil size and reactivity (Meeker, et
al 2005)
o Other assessment; e.g.
Absent corneal and gag reflexes usually indicate
a poor prognosis Absent corneal reflex should be treated with
special protective eye care and lubrication
Grimacing in response to the insertion of acotton-tipped applicator, in one nostril and thenthe other, can indicate a facial nerve deficit
Absent gag reflex may indicate a high risk for
aspiration pneumonia Eyes can be checked for doll's eye reflex
o Motor function

8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 2/52
Asymmetrical spontaneous movement and
lateralization (e.g. hemiparesis and hemiplegia)suggest a focal mass lesion on the side of the
brain opposite the side of motor weakness
Decortication and decerebration are seen
in comatose patients following TBI Bilateral or unilateral flaccidity may be
seen in spinal injuries
o Other assessments
Abrasions or contusions on the face and scalp
Ecchymosis on the mastoid bone (Battle's sign)
Periorbital ecchymosis (raccoon's eyes) Conjunctival hemorrhage
Clear or bloody drainage from ear, nose, or
postnasal area Nuchal rigidity of the neck
Elevated ICP and shape of P1, P2, and P3
components
http://calder.med.miami.edu/pointis/tbiprov/NURSING/neuro3.html
Neurological
8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 3/52
COMMON LAB TESTS FOR NEUROLOGICAL DISORDERS: CEREBROSPINALFLUID
1. Appearance colorless, clear
2. Pressure 50-180 mm H2O3. Protein
a. Lumbar 15-50 mg/dlb. Cisternal 15-25 mg/dlc. Ventricular 6-15 mg/dl
4. Cell Counta. RBCs negativeb. WBCs 0-5
5. Glucose 50-80 mg/dl6. Gram stain negative for organisms7. Culture and sensitivity: no growth
Cerebrospinal fluid analysis
a. obtained via lumbar, cisternal or ventricular punctureb. indications: inflammation, infectionc. standard precautions are requiredd. maintain strict asepsis
Cerebrospinal Fluid (CSF)
Definition: A watery cushion that protects the brain and spinal cord from physical impact and bathesthe brain in electrolytes and proteins.
Formation: The fluid is formed by the choroid plexuses of the lateral and third ventricles. That of the
lateral ventricles passes through the foramen of Monro to the third ventricle, and through theaqueduct of Sylvius to the fourth ventricle. There it may escape through the central foramen of Magendie or the lateral foramina of Luschke into the cisterna magna and to the cranial and spinalsubarachnoid spaces. It is reabsorbed through the arachnoid villi into the blood in the cranial venoussinuses, and through the perineural lymph spaces of both the brain and the cord.
Characteristics: The fluid is normally watery, clear, colorless, and almost entirely free of cells. Theinitial pressure of spinal fluid in a side-lying adult is about 100 to 180 mm of water. On average, thetotal protein is about 15 to 50 mg/dl, and the concentration of glucose is about two-thirds theconcentration of glucose in the patient's serum. Its pH, which is rarely measured clinically, is slightlymore acidic than the pH of blood. Its concentration and alkaline reserve are similar to those of blood.It does not clot on standing. Turbidity suggests an excessively high number of cells in the fluid,
typically white blood cells in infection or red blood cells in hemorrhage.
CSF may appear red following a recent subarachnoid hemorrhage or when the lumbar puncture thatobtained the CSF caused traumatic injury to the dura that surround the fluid. Centrifugation of thefluid can distinguish between these two sources of blood in the spinal fluid: the supernatant is usuallystained yellow (xanthochromic) only when there has been a recent subarachnoid hemorrhage.
Many conditions may cause increases in total protein: infections, such as acute or chronic meningitis;multiple sclerosis (when oligoclonal protein bands are present); Guillain-Barré syndrome; and chronicmedical conditions like cirrhosis and hypothyroidism (when diffuse hypergammaglobulinemia ispresent). The concentration of glucose in the CSF rises in uncontrolled diabetes mellitus and dropsprecipitously in meningitis, sarcoidosis, and some other illnesses. Malignant cells in the CSF,
demonstrated after centrifugation or filtering, are hallmarks of carcinomatous meningitis.
Microorganism: The CSF is normally sterile. Meningococci, streptococci, Haemophilus influenzae,Listeria monocytogenes , and gram-negative bacilli are recovered from the CSF only in cases of meningitis. Syphilitic meningitis is usually diagnosed with serological tests for the disease, such asthe venereal disease research laboratory (VDRL) test, the rapid plasma reagin (RPR) test, or thefluorescent treponemal antibody test. Cryptococcal infection of the CSF may be demonstrated byIndia ink preparations, or by latex agglutination tests. Tuberculous meningitis may sometimes bediagnosed with Ziehl-Neelsen stains, but more often this is done with cultures. These last threeinfections (syphilis, cryptococcosis, and tuberculosis) are much more common in patients who haveacquired immunodeficiency syndrome (AIDS) than in the general population.

8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 4/52
Electroencephalogram (EEG)
a. records electrical activity at various brain sitesb. specific nursing interventions
i. do not stop anticonvulsant medicationsii. the night before test, adult clients should have
minimal sleepiii. hair should be washed prior to testiv. after test, help client remove paste

8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 5/52

8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 6/52
Tomography and resonance imaging
Computerized tomography (CT) scans
a. use a roentgen ray and a computer to provide accurate
images of cross sections of the bodyb. a non-invasive procedure using very little radiation thatvisualizes slices of tissuesc. usually takes less than one hour d. sharper images than conventional x-rayse. contraindicated in pregnancyf. nursing interventions
i. explain test to clientii. some clients may require mild sedationiii. client must lie very stilliv. client receives radiopaque solution to visualize
blood vessels
v. client is NPO past midnight when contrast is usedvi. if barium studies were done, wait at least four days
for CT scan, or barium will obscure film
Positive emission tomography (PET)
a. uses an intravenous injection of radioactive substancefollowed by a head scanb. various shades of color indicate levels of glucosemetabolism in the brainc. nursing interventions: same as CT scan
Magnetic resonance imaging (MRI)
a. tomography based on the magnetic behavior of protons inthe body tissuesb. used to detect neurologic and musculoskeletal disordersc. contraindicated in clients with metal implants such aspacemakers, aneurysm clips, medication patches that are foil backed, metallicorthopedic devices, can be uncomfortable with multiple tattoosd. nursing interventions
i. explain test to clientii. client must lie very stilliii. client may become claustrophobic in chamber iv. soft humming sound may annoy some clientsv. client must remove all metal jewelry and watches
Lumbar puncture (LP) (Spinal Tap)
a. needle inserted into the subarachnoid space between L3and S1b. uses
i. measure cerebrospinal fluid (CSF) pressureii. obtain CSF for visual and laboratory examinationiii. to inject medications, anesthetic agents, diagnostic
agents.
1. Contraindicated if client has increased intracranial pressure (ICP)2. Place client in lateral decubitus position (knee-chest)3. Complications include post-puncture headache
4. CSF findings 5. Nursing interventions
a. explain procedure to client

8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 7/52
b. administer sedative if orderedc. assist client to maintain proper position and stillness duringprocedured. strict asepsise. maintain standard precautionsf. label specimens sequentially
g. provide emotional support as procedure can be painfulh. post-procedure
i. keep client flat on back from four to 12 hoursii. give analgesics & ice pack as orderediii. perform neuro checks and vital signs prequently to
assure stabilityiv. encourage fluids unless contraindicatedv. observe for post-puncture headache, leakage of
CSF, tingling sensation, numbness or pain in lower extremities
Intracranial pressure (ICP) monitoring
a. invasive: measuring device is placedi. in a ventricle
ii. in a subarachnoid space
iii. outside dura mater
iv. within parenchyma b. types of devices include aventricular catheter; asubarachnoid bolt; an epidural sensor c. changes in intracranial pressure are converted to anelectrical impulse by a transducer and displayed on a screen or on graphpaper d. measurements include volume-pressure relationships,pressure waves and cerebral perfusion pressurese. normal ICP: 10-15 mm Hgf. nursing interventions
i. maintain strict sterile techniqueii. maintain patency of deviceiii. observe for CSF leaks or bleeding, signs of
infectioniv. monitor pressure and report deviations

8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 8/52
I. Neurological Anatomy and Physiology
A. Central nervous system (CNS) - coordinates and controls body functions1. Braina. cerebrum
i. hemispheres right and leftii. frontal lobe - higher intellectual functions, social
behavior, personalityiii. parietal lobe - perceives and interprets sensory
inputiv. temporal lobe - emotional response, memory,
language, organization of sensory input (hearing,taste and smell)
v. occipital lobe - visionb. cerebellum - provide equilibrium and muscle coordinationc. brain stem - midbrain, pons and medulla oblongata;
controls basic body functions and relays impulses to andfrom spinal cord; the connection between the brain andspinal cord

8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 9/52
2. Spinal corda. descending tract - anterior portion of cord carrying motor
information; associate "d"escending to "d"own impulsesare carried to peripheral nerves
b. ascending tract
i. the posterior portion of cord that carries sensoryinformation up to the brainii. 31 segments
• eight cervical: neck and upper extremities• 12 thoracic: thoracic and abdomen• five lumbar: lower extremities• five sacral: lower extremities, urine and
bowel control• one coccygeal
8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 10/52
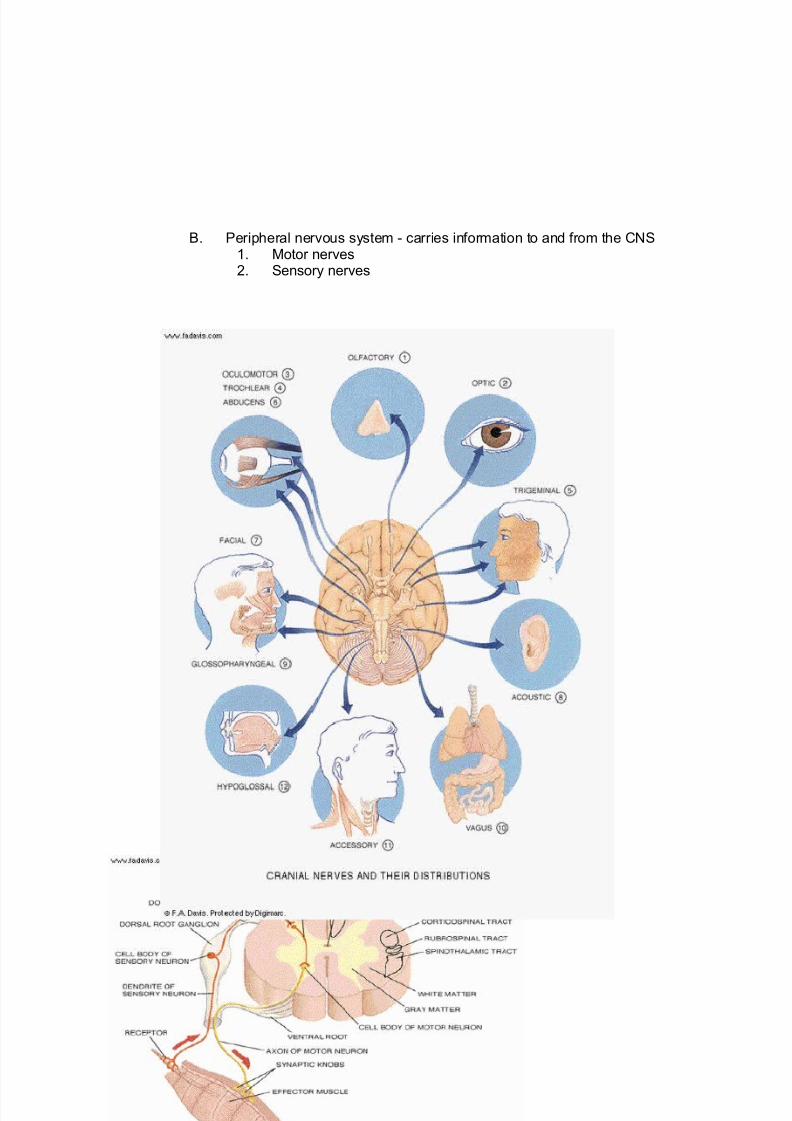
B. Peripheral nervous system - carries information to and from the CNS1. Motor nerves2. Sensory nerves

8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 11/52
C. Autonomic nervous system - regulates body's internal environment1. Sympathetic - prepares body for fight or flight; used only as
needed when scared or excessively happy2. Parasympathetic - controls normal body functioning for day to day
activities, e.g., increases muscle tone, maintains secretions withmoist mucous membranes; maintains heart rate within normallimits; maintains GI and GU peristalsis
D. Cranial nerves
These nerves are the vital bridges between the brain and the rest of thebody.

8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 12/52
E. Physiology - nervous system coordinates and controls all activities of thebody
1. Receives internal and external stimuli2. Processes information to determine appropriate response
3. Transmits information over varied motor pathways to effector organs
F. Findings for increased intracranial pressure (ICP)1. Early
a. change in level of consicousness (LOC): restlessness,agitation, irritability, disorientation, confusion, lethargy,stupor
b. pupils: dilated ipsilaterally, react slowly to light
c. abnormal motor activity: contralateral hemiparesis d. abnormal reflexes - hyper or hypo reflexiae. vital signs within normal parameters
2. Latea. LOC: semicomatose, comab. pupils: dilated bilaterally and fixed; no reaction to light
c. motor function: decorticate posture then decerebrateposture; flaccid muscles at end stage
d. vital signs - increased systolic pressure to result in awidened pulse pressure, decreased respirations withbradycardia (Tip: heart and lungs go in similar directions -both increase or decrease), temperature initially may risethen fall below normal parameters
II. Degenerative Disorders A. Parkinson's disease
1. Definition: degenerative disorder of the dopamine hydrochloride -
producing neurons a. result: dopamine hydrochloride depletionb. usually occurs in older adults and males more than
femalesc. etiology unknown
2. Findings: first unilateral, then bilateral movements
a. resting tremors of the lips, jaw, tongue, and limbs,especially a resting pill-rolling tremor of one hand that isabsent during sleep. This tremor is often labeled - "nonintention" tremor. This is different from an essential or intention tremor in which the tremor is action related andlabeled "intention" tremor.
b. bradykinesia c. fatigued. stiffness and rigidity with movemente. mask-like facial expression often accompanied with
droolingf. slow, shuffling walk in a stooped-over posture; gradually
more difficulty with walkingg. difficulty rising from sitting positionh. ultimately confined to a wheelchair i. mind stays intact unless other aggravating conditions
j. echolalia in most cases3. Diagnostics
a. based on findings with historyb. EEGc. MRId. computerized tomogram (CT scan)
4. Managementa. expected outcomes: palliative and to postpone
dependenceb. pharmacologic

8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 13/52
I. anticholinergics - minimize extrapyramidal effectsI. benzotropine mesylate (Cogentin)
II. procyclidine (Kemadrin)II. dopamine hydrochloridergics: Levodopa (L-Dopa)III. antiparkinsonian agent: amantadine HCl
(Symmetrel) reduces rigidity and tremor
IV. MAO inhibitors: selegiline (Eldepryl)V. coenzyme Q-10VI. others
I. selegiline (Carbex)II. COMT inhibitorsIII. tolcapone (Tasmar)IV. entacapone (if combined with carbidopa and
levodopa the medication is Stalevo)c. therapies
I. physicalII. occupationalIII. speech
d. surgery: to decrease tremor I. stereotaxic thalamotomy
II. pallidotomy - pinpoint the areas to be treatedsurgically
III. deep brain stimulation5. Nursing interventions
a. maintain safety of clientb. prevent effects of immobilityc. foster independence in activities of daily living (ADL)d. reinforce the use of assistive devices for ambulation as
indicatede. promote good nutrition
I. small, frequent mealsII. soft foodsIII. roughage with sufficient fluids to decrease
constipationf. monitor effectiveness or ineffectiveness of administered
medicationsg. provide emotional support to client and family membersh. teach client
I. when and what side effects of the drugs to report
II. the benefits of daily exercise
III. the benefits of "drug holidays"
B. Huntington's disease1. Definition
a. progressive atrophy of basal ganglia and some parts of cerebral cortex
b. etiology - genetic disorder, autosomal dominant2. Findings: usually occurs in middle age, increased involuntary
movements, progressive decline in cognitive functiona. motor function
I. impaired chewing and swallowing
II. chorea
III. dystonic postureIV. gradually becomes bedridden
b. cognitive function: less able to organize, plan andsequence behavior
c. mental function: personality changes, depression, evenpsychosis
3. Diagnostics: history and physical exam4. Management
a. expected outcome: postpone dependenceb. supportive care for findings

8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 14/52
c. therapies: speech, physicald. genetic counseling
5. Nursing interventionsa. foster independence in ADLb. reinforce the use of assistive devices for ambulation as
needed
c. teach client toI. maintain good nutrition
II. get emotional support from support groups, friendsIII. seek genetic counseling
C. Amyotrophic lateral sclerosis (ALS, Lou Gehrig's disease)1. Definition
a. progressive atrophy of spinal muscle; bulbar palsy b. progressive degeneration of the motor neurons of the
anterior horn cells of the spinal cord, brainstem, and motor cortex
c. onset in later middle age; more in men than in women
d. clients with ALS usually die within two to six yearse. etiology unknown
2. Findingsa. usually beginning in the upper body - the head and arms,
the distal portion firstb. mild clumsiness progressing to total incapacityc. muscle wasting, atrophy, spasticityd. speech disorderse. no change in sensation or autonomic systemf. death most often from complications: respiratory failure,
urinary or pulmonary infections for stasisg. mind usually intact while client has loss of voluntary and
eventually involuntary muscle functions3. Diagnostics: history and physical exam4. Management
a. expected outcome: keep functional independence as muchas possible
b. no curec. management of findings
I. muscle relaxants for spasticity II. therapies:
I. speechII. physicalIII. respiratory support
IV. nutritional support5. Nursing interventions
a. provide for respiratory care and referralsb. maintain a safe environment focused toward infection
preventionc. prevent complications of immobility especially pulmonary
and urinary stasisd. postpone dependencee. promote balanced nutritionf. provide emotional support and referrals to support groups
D. Dementia
1. Etiologya. characterized by irreversible, progressive cerebral
dysfunction
b. Alzheimer's disease - most common cause of dementia
I. characterized by brain atrophyII. development of senile plaques and neurofibrillary
tangles in the cerebral hemispheresIII. etiology unknown

8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 15/52
2. Findingsa. initially characterized by decreased intellectual functioningb. Alzheimer's disease has three stages
I. early stageI. memory loss
II. subtle personality changes
III. difficulty with abstract thinkingII. middle stage
I. impaired judgmentII. impaired languageIII. difficulty with motor activity and object
recognitionIV. wanderingV. inability to carry out ADL
III. final stageI. complete loss of language function
II. loss of bowel and bladder controlc. prognosis - poor, incurable
3. Management - expected outcome: maintenance of functionalcapacity
4. Nursing interventionsa. meet client's physical needsb. promote client's independencec. promote contact with realityd. assist client/family to establish a routinee. provide emotional support or caregiver support with
appropriate referrals

8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 16/52
E. Organic brain syndrome1. Definition - a general term used to categorize physical conditions
that can cause decreased mental function2. Etiology
a. degenerative disordersb. drug and alcohol related conditionsc. infectionsd. repiratory conditionse. trauma-induced brain injuryf. cardiovascular disordersg. dementia from metabolic disorders
3. Findingsa. findings vary with the specific diseaseb. in general, organic brain syndromes cause varying
degrees of confusionc. delirium - severe often sudden short term loss of brain
function as with high temperatures, drug withdrawald. agitatione. dementia - long term loss of brain functionf. aggression - typical of some of the conditions contributing
to this diagnosis4. Management
a. therapy varies with the specific disorder
b. many of the disorders have nonspecific treatmentsc. the priority in many instances is supportive care to assist
the person in areas where brain function is lostd. medications may be needed to reduce aggressive
behaviors typical of some of the conditions in this category5. Nursing interventions
a. assist to meet the client's physical needsb. refer family to support systemsc. monitor the effectiveness of medication therapyd. evaluate changes to where the client is unable to maintain
independence with ADL
III. Cerebrovascular Accident (CVA, Stroke, Cerebral Infarction) A. Definition: decreased blood supply to the brain

8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 17/52
1. Risk factorsa. hypertension, uncontrolledb. smokingc. obesityd. increased blood cholesterol and triglyceridese. chronic atrial fibrillation
2. Five classes of stroke: by "severity" - least to most severea. transient ischemic attack (TIA), "angina" of the brain
i. TIA is warning sign of strokeii. localized ischemic eventiii. produces neurological deficits lasting only minutes
or hoursiv. full functional recovery within 24 to 48 hours
b. reversible ischemic neurological deficit (RIND)i. similar to TIAii. findings last between 24 hours and three weeksiii. usual full functional recovery within three to four
weeks
c. partial, nonprogressing stroke: some neurological deficit,but stabilized
d. progressing stroke (stroke in evolution)i. deterioration of neurological status often with grand
mal seizure activityii. has residual neurological deficits that last
indefinitelye. completed stroke - results from a stroke in evolution
3. Two types of stroke by "cause"a. ischemic (also known as occlusive) stroke (clot) - slower
onset
i. results from inadequate blood flow leading to acerebral infarction
ii. caused by cerebral thrombosis or embolism withinthe cerebral blood vessels
iii. most common cause: atherosclerosisb. hemorrhagic stroke (bleeding) - abrupt onset
i. intracerebral hemorrhagic stroke• blood vessels rupture with a bleed into the
brain• occurs most often in hypertensive older
adults• may also result during anticoagulant or
thrombolytic therapyii. subarachnoid hemorrhage (SAH)
• most often caused by rupture of saccular intracranial aneurysms
• more than 90% are congenital aneurysmsiii. epidural bleeds
• cerebral arterial vessels are involved• often a loss of consciousness for a short
period of time called transientunconsciousness
• recall clue: associate that "e" in epidural and"a" in artery are together at the top of the
alphabetiv. subdural bleeds
• veins are involved• may not be evident until months after an
initial trauma• recall clue: associate that "s" in subdural
and "v" in vein are together at the bottom of the alphabet

8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 18/52
B. Findings (depends on the location of the lesion)
Types of CVA
C. Diagnostics1. History and physical exam2. Computerized tomogram (CT) scan3. Magnetic resenance imaging (MRI)4. Doppler echocardiography flow analysis5. Carotid artery duplex doppler ultrasonography6. EEG - shows abnormal electrical activity7. Lumbar puncture - shows if blood is found in the cerebral spinal
fluid as a result of a cerebral bleed8. Cerebral angiography - shows blood flow in cerebral arteries
a. may be done with or without contrastD. Management - to prevent or minimize the damaging effects of stroke;
dependent on the type of CVA1. Expected outcomes
a. prevent or minimize the damaging effects of stokeb. depends on the type of CVA
2. Occlusive strokea. pharmacologic

8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 19/52
1. thrombolytics2. anticoagulant therapy: heparin, coumadin3. antiplatelet therapy: aspirin, dipyridamole
(Persantine)1. platelet aggregation inhibitor: clopidogrel
(Plavix), ticlopidine HCL (Ticlid)
4. steroids: dexamethasone (Decadron)b. surgery - bypass - carotid endarterectomy
3. Hemorrhagic strokea. pharmacologic
1. antihypertensive agents2. systemic steroids: dexamethasone (Decadron)3. osmotic diuretics: mannitol4. antifibrinolytic agents: aminocaproic acid (Amicar)5. vasodilators6. alpha-blockers and beta-blockers7. anticonvulsants
b. surgical excision of aneurysm
4. Common to both types of strokea. care based on findingsb. therapies
1. nutritional support2. physical3. speech4. behavioral5. occupational
E. Nursing interventions1. In acute stage of stroke
a. maintain airway patency; if grand mal seizure activity notetime, length, behaviors
b. monitor neuro status and vital signsc. maintain adequate fluidsd. position with head of bed elevated 15 to 30 degrees with
client turned or tilted to unaffected sidee. provide activity as orderedf. perform passive and/or active range of motion exercisesg. maintain client's proper body alignmenth. administer medications as orderedi. care for post op client as indicated
j. provide care for client with increased intracranial pressure
2. Long-term care of client with strokea. monitor to facilitate normal elimination patternsb. teach/evaluate the use of supportive devicesc. maintain client in a safe environment
CARE OF CLIENT WITH INCREASED INTRACRANIAL PRESSURE
1. Institute seizure precautions2. Administer oxygen as ordered3. Monitor for changes in intracranial pressure4. Monitor neuro vital signs as ordered5. Maintain fluid restriction as ordered6. Observe for herniation syndrome7. Raise head of bed at 30-45 degrees; avoid 90 degrees since pressure in hip area increases ICP8. Prevent any activities that increase ICP such as: laughing, straining at stool, coughing, vomiting,
any restrictive clothing around neck, anxiety, pushing up in bed with heels, pulling on rails when
turning, neck rotation, flexion or extension9. Provide for the care of the unconscious clients if decreased LOC

8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 20/52
d. prevent the effects of immobilitye. support the maintenance of adequate nutrition in light of
feeding and swallowing problemsf. assist with eating and ADL as indicatedg. provide emotional supporth. provide methods of communication for client with aphasia
IV. Infectious Inflammatory DisordersA. Meningitis
1. Definition/coursea. acute or chronic inflammation of the meningesb. average length of illness is four months
2. Typesa. bacterial: mostly contagious; requires isolation
i. mostly common meningococcal• the covering of the brain and spinal cord are
involved• in children 2 to 18 years-old• in high risk groups
o infantso adults with weakened or suppressed
immune systemso college students – freshman in
particular who reside in dormitorieso travelers to foreign countries where
disease is endemico 10 – 15% of cases are fatal

8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 21/52
o 10 – 15 % of cases result in brain
damage or other serious side effectsii. Haemophilus influenzae; those at risk are
• children in child care settings• children with no access to vaccine
iii. pneumococcal; those at risk are• children under the age of 2 years-old• adults with weakened or suppressed
immune systemsb. viral
i. isolation is not requiredii. aseptic meningitis is the most common form in the
USAc. cryptococcal fungal
i. often from bird droppingsii. organism is found in dirtiii. common in clients with AIDS
3. Findings
a. severe headacheb. sudden fever c. altered LOC – decreasedd. photophobiae. nuchal rigidity – severe pain in the back of neck when the
chin is moved toward the chest with the client resistingmovement
4. Diagnosticsa. history and physical examb. positive Kernig's sign: 90-degree flexion of hip and knee
with extension of knee causes painc. positive Brudzinski's sign: flexion of neck causes flexion of
hip and kneed. lumbar puncture for characteristics of cerebral spinal fluid -
decreased glucose in bacterial or fungal infectionse. CT or MRI with and without contrastf. EEG
5. Managementa. expected outcomes: to cure the infection and prevent
complicationsb. pharmacologic
i. antibiotic therapy depends on the type of pathogenii. preventive therapy for people exposed to those with
meningococcal or haemophilus influenzae (H flu)
meningitis: rifampin (rifadin)iii. H flu vaccineiv. antifungals if fungusv. anticonvulsants to prevent seizures
c. actions to minimize fever d. prevention of increased intracranial pressure or seizures
6. Nursing interventions
a. care of client with increased ICP
b. seizure precautionsc. administer drugs as orderedd. provide comfort measures for pain
e. reduce external stimuli and lighting if photophobia
SEIZURE PRECAUTIONS
Before seizure1. Bed rest with padded side rails2. Suction available at the bedside3. Oxygen available at bedside
During seizures1. Loosen any tight or restrictive clothing.2. If clients are falling, gently help them to the ground and position clients on their side.3. Do not place anything in the mouth.4. Observe the seizure as it runs its course.5. If it lasts longer than 5 minutes, notify health care provider immediately.6. Note the activity and the time it begun and ended.
Daily life precautions1. For children discourage climbing over 10 feet high.2. Recommend for clients not to lock bathroom or shower doors.3. If swimming, clients are to have someone with them who can rescue.4. If old enough to drive, clients should be seizure free for six months. The time may vary in some states.

8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 22/52
B. Parameningeal infections1. Definition
a. localized collection of exudate in the brain or in the spinalcord
b. a recurrent aseptic meningitisc. considered noninfectious
2. Findingsa. similar to meningitisb. headache, fever, stiff neck, altered consciousness -
decreased3. Diagnostics
a. NO lumbar puncture; may cause herniationb. computerized tomogram (CT) scan
4. Managementa. expected outcomes: to cure infection and prevent
complicationsb. surgical decompression of abscessc. symptomatic and preventive treatment as with meningitisd. drugs: antibiotics
5. Nursing interventions: same as meningitis except that infectiousprecautions are not required
C. Encephalitis1. Definition
a. acute viral or less commonly bacterial inflammation,irritation and swelling on the brain tissue
b. can occur as epidemics or sporadicallyc. death rate ranges up to 70%d. most cases in the USA associated with sporadic
encephalitis is herpes simplex virus types 1 and 2, rabiesvirus, or arboviruses from the bite of infected ticks,mosquito or other blood sucking insects, i.e., Equine, LaCrosse, St. Louis, West Nile
e. may follow a systemic viral illness such as chicken pox2. Findings
a. adult1. sudden fever 2. severe headache3. altered LOC – decreased progressing to stupor
then coma with seizure activity4. nuchal rigidity5. speech or hearing de6. change in personality7. mild flu-like complaints
b. infant
1. vomiting2. body stiffness3. constant crying that worsens when child picked up4. constant full or bulging anterior fontanel
3. Diagnosticsa. history and physical examb. CT scan, MRI, EEGc. brain biopsy

8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 23/52
d. cerebral spinal fluid – decreased glucose suggestsbacterial or fungal infection
4. Managementa. expected outcomes: to cure infection and prevent
infectionsb. uncomplicated cases require supportive and preventive
carec. bed or chair restd. support nutritional needse. monitor for fluid balance maintenancef. herpes simplex calls for antivirals: vidarabine (viraA),
acyclovir (Zovirax)
g. prevention of increased ICPh. antivirals such as acyclovir or ganciclovir i. anticonvulsants - prevent seizures
5. Nursing interventionsa. comfort measures for fever b. administer drugs as ordered
c. seizure precautionsd. care of the client with increased ICPe. when needed, ensure isolation and airborne-droplet
precautions
V. Various Disorders of the Neurologic System A. Multiple sclerosis
1. Definitiona. demyelination of white matter throughout brain and spinal
cordb. third most common cause of disability in clients aged 15 to
60
c. specific cause unknownd. increased incidence in temperate to cool climatese. illness improves and worsens unpredictably
2. Findings depend on the location of the demyelinationa. cranial nerve: blurred vision, dysphagia, diplopia, facial
weakness and/or numbnessb. motor: weakness, paralysis, spasticity, gait disturbances
c. sensory: paresthesias, decreased proprioception
d. cerebellar: dysarthria, tremor, incoordination, ataxia,vertigo
e. cognitive: decreased short-term memory, difficulty withnew information, word-finding difficulty, short attention
spanf. urinary retention or incontinence
g. loss of bowel controlh. sexual dysfunctioni. fatigue
3. Diagnosticsa. history and physical examb. lumbar puncture

8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 24/52
c. magnetic resonance imagery (MRI)d. computerized tomogram (CT) scane. evoked potentials or response - the EEG record of
electrical activity at one of several levels in the CNS bystimulation of an area of the sensory nerve system
4. Management
a. expected outcomes: to alleviate findings and preventcomplications
b. pharmacologic: adrenocorticotropic hormone (ACTH)c. therapies based on findings
I. physicalII. occupationalIII. pharmacologic
5. Nursing interventionsa. maintain client's functional independence in ADLb. determine effectiveness of administed medicationsc. prevent complications of immobilityd. prevent injury from difficulties walking
e. provide emotional support to client and familyf. provide counseling for sexual dysfunction
g. teach client to:I. avoid fatigue and stress
II. conserve energyIII. exercise regularlyIV. know drugs and side effectsV. use self-help devicesVI. maintain a diet that supports nutrition and energy
needs
B. Guillain-Barre syndrome
1. Definitiona. acquired inflammatory diseaseb. process: demyelinization of peripheral nervesc. precipitating factors include prior bacterial or viral infection
within one to two weeks2. Findings
a. muscle weakness: progressive, ascending, bilateral b. leads to paralysis of voluntary musclesc. loss of superficial and deep tendon reflexes
d. bulbar weaknesse. dysphagiaf. dysarthria
g. respiratory failureh. sensory findings: paresthesias, burning paini. paralysis may vary from being total to partial of only one-
half way up the body3. Diagnostics
a. history and physical examb. lumbar puncture will show increased protein in CSF
c. electromyography (EMG)4. Management
a. expected outcomes: to prevent complications and maintainbody functions until any reversal
b. steroids in acute phase
c. care as dictated by areas involved5. Nursing interventions
a. maintain the care of client on ventilatory support b. provide for care of the immobilized clientc. have a safe environment to minimize infectiond. maintain nutrition and fluid balancee. refer families or client to support groups

8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 25/52
f. supply referrals to therapies such as speech, physical,occupational and counseling
CARE OF THE CLIENT ON VENTILATOR
Nutrition
1. Administer as ordereda. IV fluids, medsb. Enteral feedings
2. Evaluate for a. balanced fluid intake and output
b. adequate and balanced nutrition
Hygiene
1. Providea. a rigorous, scheduled mouth care – prevents ventilator acquired pneumonia
bed baths and skin care as necessary
b. eye care if client has decreased LOCc. meticulous perineal care to prevent yeast infectionsd. for the initiation of a bowel regimen with stool softeners with expected bowel movements at
least every three days
Skin and Muscle Integrity
1. Prevent the effects of immobility by routine passive or active range of motion exercises or getclient OOB as tolerated
2. Minimize decubitus ulcers by avoidance of rubbing or massaging reddened areas 3. Reposition client every hour if bed ridden
Safety
1. Apply bilateral splints as ordered to prevent footdrop and wristdrop2. Provide a safe environment - bed in low position, side rails up, call light within reach3. Initiate seizure precautions if indicated
Sensory Stimulation
1. Provide appropriate stimulation which means to schedule groups of tasks to preventoverstimulation
2. Talk to clients before and during procedures or when any direct care or when in the room for other reasons
3. Explain procedures before beginning them4. Encourage family members to talk with clients about usual family activities5. Enhance stimulation by
a. insertion of hearing aidsb. a check of glasses for cloudy smeared lens then clean and put them nearby or on clientc. a change of lighting in the room to mimic natural light changesd. promotion of the use of electronic battery devices such as CD – DVD – MP3 players, radio,
television. Have maintenance check for leakage of currents before use.

8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 26/52
C. Myasthenia gravis (MG)1. Definition
a. antibodies destroy acetylcholine receptors where nerves join muscles - myoneural junction
b. two age clusters: women in early adulthood and men inlate adulthood
c. progressive with occurances of crises
2. Findingsa. progressive fatigue or weakness of voluntary muscles, but
no muscular atrophy
b. sensation remains intactc. facial
i. ptosis (drooping eyelid) and reduced eye closureii. weak smile
iii. diplopia, blurred visioniv. speech and swallowing disordersv. weakness of facial muscles - difficulty to raise
eyebrows, make different facesd. signs of restrictive lung disease
3. Diagnosticsa. history and physical examb. edrophonium (tensilon) test: improved muscle strength
after tensilon injection indicates a positive test for MG4. Management
a. expected outcomes: to improve strength and enduranceb. pharmacologic
i. anticholinesterase agents: pyridostigmine(mestinon), neostigmine (prostigmin)
ii. corticosteroid therapyiii. immunosuppressants: azathioprine (imuran)
8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 27/52
c. thymectomy
d. plasma exchangee. myasthenic crisis management
i. crisis usually follows stressor or during dosagechanges usually when being increased
ii. signs: sudden inability to swallow, speak, or maintain patent airway
iii. cholinergic crisis may follow over dosage of medication
iv. positive edrophonium (tensilon) test signalsmyasthenia
v. if negative endophronium test, client has notmyasthenic but cholinergic crisis, so treat withatropine
vi. ventilatory support as indicated5. Nursing interventions
a. identify aggravating factors, such as:i. infectionii. stressiii. changes in medication regime - especially when
increasing dose
b. if client is in crisis: provide care of the client on ventilatorysupport
c. give medications as ordered and on time d. help with ADL and feeding as indicatede. provide
i. emotional supportii. adequate rest periodsiii. care of the post-surgical client
f. teach clienti. energy conservation techniques

8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 28/52
ii. expectations, side effects and medicationsiii. signs of impending crisis, both myasthenic and
cholinergic along with what actions to takeiv. to avoid stressors or how to minimize stressors
VI. Seizure Disorders A. Definition/etiology
1. Sudden, transient alteration in brain function2. Disorderly transmission of electrical activity in the brain3. Causes
a. cerebral lesionsb. biochemical alterationc. cerebral traumad. idiopathic
B. A classification of seizure types: partial, simple, complex, generalized1. Partial seizures
a. focal motor b. seizure activity only in specific parts of the brainc. usually client remains conscious
2. Simple with findings associated witha. motor activityb. special sensory feelingsc. autonomic activityd. psychic issuese. psychomotor actionsf. no loss of consciousness
3. Complexa. impairment of consciousnessb. secondarily generalizedc. progressing to generalized tonic-clonic
4. Generalized seizures: eight typesa. petit mal - called absence seizuresb. myoclonic
i. sudden, uncontrollable jerking movements of oneor more extremities
ii. usually occurs in the morningc. clonic
i. characterized by violent bilateral musclemovements
SEIZURE CLASSIFICATIONS
A. Types of generalized seizures - one classification system1. Absence seizures (petit mal seizures)2. Myoclonic seizures (bilateral massive epileptic myoclonus)3. Generalized tonic-clonic seizures (grand mal seizures)4. Akinetic seizure
B. Proposed international classification of epilepsies and epileptic syndromes1. Idiopathic2. Benign childhood epilepsy
3. Primary reading epilepsy4. Symptomatic
a. chronic progressive epilepsia partialis continua of childhoodb. syndromes characterized by seizures with specific triggers
5. Cryptogenica. presumed to be symptomatic but etiology is unknownb. differs from Symptomatic by lack of etiologic evidence

8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 29/52
ii. hyperventilationiii. face contortioniv. excessive salivationv. diaphoresis
vi. tachycardia d. tonic
i. first, client loses consciousness suddenly andmuscles contract bilaterally
ii. body stiffens in opisthotonos position
iii. jaws clenchediv. may lose bladder controlv. apnea with cyanosisvi. pupils dilated and unresponsivevii. usually lasts less than a minute
e. grand mal: most common typei. tonic-clonic movements bilaterally
ii. may be preceded by prodromal iii. lasts two to three minutesiv. often incontinent of bowel/bladder v. after clonic phase, client is unresponsive for about
five minutesvi. arms and legs go limpvii. breathing returns to normalviii. possible disorientation or confusion for sometime
afterwardsix. possible headache and fatigue afterwards
f. atonic: sudden loss of postural muscle tone with collapseg. unclassified seizuresh. status epilepticus
i. rapid sequence of seizures without interruption or pauses
ii. medical and nursing emergencyiii. client in postictal state when next seizure beginsiv. sometimes occurs if a sudden stop of maintenance
anticonvulsantsv. if cerebral anoxia occurs, brain damage or death
can follow
vi. risk for severe organ and muscle hypoxia5. Diagnostics
a. by the event itself - see aboveb. history and physical examc. electroencephalogram (EEG)d. computerized tomogram (CT) scan
6. Management

8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 30/52
a. expected outcomes: to control or minimize the seizureactivity and prevent complications
b. correction of underlying problemc. medications
i. benzodiazepines, I.V. such as diazepam (valium),lorazepam (ativan) for active seizures
ii. hydantoin anticonvulsants such as phenytoin(dilantin) - maintenance
iii. barbiturates such as phenobarbitol - maintenanceiv. succinimides such as ethosuximide (zarontin) -
maintenance7. Nursing interventions
a. administer medications as ordered
b. seizure care
c. seizure precautionsd. teach client
i. to wear MedicAlert jewelryii. about medication effects, interactions, and side
effectsiii. to learn when a seizure may be triggerediv. techniques to reduce stressv. seizure care at home or at work
vi. if in public area, after the tonic phase turn client toside
VII. Headache A. Definition
1. Pain located in the upper region of the head2. One of the most common neurologic complaints
B. Classifications1. Recurrent migraine headache
a. onset during adolescence or early adulthoodb. familialc. involves unilateral, throbbing paind. subtypes
i. classic migraineii. common migraineiii. cluster headacheiv. hemiplegic headachev. ophthalmoplegic headache
SEIZURE CARE
1. Do not leave the client who is seizing2. Attempt to prevent or break client's fall by assisting him/her to horizontal position on the bed or the
floor 3. Loosen tight clothing around neck and chest4. Remove objects near the client5. Place a pillow under the client's head if possible and available6. Place the client's head in a lateral position if possible to maintain airway7. Place nothing in the client's mouth8. Cover the client if possible9. Document
a. type of seizure - describe behavior rather than labelingb. durationc. activity during and if incontinenced. if any precipitating factorse. client's response - immediate, then at 15 minute intervals until stability is established

8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 31/52
2. Recurrent muscular-contraction headache (pressure, tensionheadache)
a. most common form of headacheb. may be direct result of stress, anxiety, depression, drastic
changes in caffeine consumption3. Nonrecurrent headaches
a. occur with systemic infections and are usually associatedwith fever
b. occur as the result of a lesion, after an invasive spinal cordprocedure such as a lumbar puncture, or subarachnoidbleed
c. caused by increased intracranial pressureC. Findings
1. Vary by type of headache2. May include throbbing, nausea, vomiting, visual disturbance,
tenderness, neck stiffness, and focal neurological signsD. Diagnostics
1. History and physical exam
2. Computing tomogram (CT) scan3. Magnetic resonance imaging (MRI)
E. Management of headaches1. Expected outcomes: to alleviate pain and treat underlying cause2. Vasoconstriction by pressure or cold3. Management of migraine
a. nonnarcotic analgesics usually when onset noted: aspirin,acetaminophen (Tylenol), ibuprofen
b. narcotic analgesics: codeine, meperidine (Demerol),morphine
c. alpha-adrenergic blocking agentblocker: ergotaminetartrate (Ergostat) without or with caffeine
d. steroids: dexamethasone (Decadron)e. prophylactic treatment with beta-adrenergic blocking
agents, serotonin antagonists, antidepressants, imipramine(Tofranil)
f. avoid headache-precipitating foods such as MSG,tyramine, or milk products, or sudden stopping of caffeinated drinks
4. Management of cluster headaches - a type of migrainea. narcotic analgesics: codeine sulfateb. alpha-adrenergic blocking agentblocker: ergotamine
tartrate (Ergostat)c. prophylactically with serotonin antagonists
5. Management of tension headachesa. nonnarcotic analgesicsb. muscle relaxantsc. prophylactically: antidepressants and/or doxepin
(Sinequan)F. Nursing interventions
1. Suggest a quiet, dark environment2. Manage pain by prompt medication administration or other
comfort measures3. Help client identify precipitating factors and actions for prevention4. Keep NPO until nausea and vomiting subside5. Teach client
a. to keep a headache diaryb. expected medication actions and side effectsc. alternatives for pain relief including referrals for alternative
approachesd. to avoid or minimize trigger factors

8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 32/52
VIII. Head Trauma
A. Classifications1. Closed versus open injury
a. closed is nonpenetrating; no break in the integrity of theskull
b. open injury: skull is broken with the brain exposed2. Severity
a. mild: only momentary loss of consciousness with noneurological sequelae
b. moderate: momentary loss of consciousness with achange afterwards in neurological function which is usuallynot permanent
c. severe: decreased LOC with serious neurologicalimpairment and sequelae

8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 33/52
B. Types of skull fractures1. Linear: simple break in the bone; no displacement of the skull2. Depressed: part of skull is pushed in3. Basilar: at base of skull; may extend into orbit or ear; ear or nose
may leak CSF; most difficult to verify by x-ray

8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 34/52
4. Concussion: temporary loss of neurologic function with completerecovery
C. Types of bleeding or hematomas1. Epidural
a. usually something lacerates the blood vessels (arteries) of the middle meninges
b. since this is arterial bleeding, the risk of death is greatestc. client commonly looses consciousness after injury then is
lucid; then LOC drops quickly with the next 24 hours2. Subdural
a. something has lacerated the blood vessels (veins) crossingthe subdural space
b. acute: findings surface in 24 to 72 hours after injury withrapid neurologic deterioration
c. subacute: findings surface 72 hours to 2 weeks after injurywith a slower progression of deterioration
d. chronic: gradual clot formation over time, possibly monthswith minimal deterioration
D. Progression of skull fracture injury1. Onset: contusions and lacerations of nerve cells2. Neuron death: gradual demyelinization of affected nerve fibers3. Scarring: meninges adheres to injured area of brain
E. Complications1. Cerebral edema
a. results in increased intracranial pressureb. results directly from cerebral ischemia, anoxia, and
hypercapnia2. Diabetes insipidus (DI)
a. DI results from a decrease release of antidiuretic hormone(ADH) and body excretes too much fluid
b. the increase in urinary output results in a low specificgravity
c. more common in the initial acute phase of head injury3. Stress ulcer
a. head injuries activate both the sympathetic andparasympathetic systems
b. stimulation of sympathetic system leads to gastric ischemiafrom vasoconstriction
c. stimulation of parasympathetic system leads to increasedrelease of hydrochloric acid (HCL) into the stomach
d. steroid therapy may contribute to the development of ulcers since steroids increase HCL acid
4. Syndrome of inappropriate anitdiuretic hormone (SIADH)a. too much ADH is producedb. water is excessively retained - hemodilutionc. urinary output decreases; urine specific granity increases
effectd. more common in the chronic phase of care after a head
injury5. Seizure disorders6. Infection: brain, lungs, urinary system from immobility7. Hyperthermia or hypothermia
F. Findings of head trauma1. Degree of neurological damage varies with type and location of
injury2. Restlessness and irritability - initially3. Decreased LOC - lethargy, difficulty with arousal4. Headache5. Nausea and vomiting - projectile vomiting indicates increased ICP
G. Diagnostics1. History and physical exam2. Computerized tomogram (CT) scan

8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 35/52
3. Magnetic resonance imaging (MRI)4. Electroencephalogram (EEG)
H. Management
1. Expected outcomes: to reduce or minimize increases inintracranial pressure and protect the nervous system
2. Medications for increased ICP
a. osmotic diuretics; mannitol (osmitrol) - IV drip or pushb. steroids: dexamethasone (decadron) - IV push
c. barbiturate coma may be induced to treat refractory increased intracranial pressure
3. Surgical correction of underlying cause4. Treatment for evident findings: seizures, fever, infection5. Therapy
a. nutritional supportb. physicalc. speechd. behaviorale. occupational
I. Nursing interventions1. Provide care of the client with increased intracranial pressure
a. seizure precautions
b. seizure care
c. care of the client on ventilator d. care of the client undergoing surgery
2. Monitor for balanced nutrition and fluids3. Assist with ADL as indicated4. Prevent complications of immobility5. Monitor neuro vital signs6. Give medications as ordered
7. Provide emotional support with appropriate referrals8. Manage pain within agency's guidelines
IX. Brain Tumors A. Growth of tissue within the brain tissue enclosed by the skull
1. May be cancerous or benign2. Classified according to tissue type3. May be primary or metastatic
B. Findings1. Depend on the size and the location of tumor
2. Locations and findingsa. frontal lobe: personality changes - classic, focal seizures,visual disturbances, hemiparesis, aphasia
b. occipital lobe: visual hallucinations, focal seizuresc. temporal lobe: headache, seizuresd. parietal lobe: visual losses, seizurese. cerebellum: coordination or mobility difficulties
3. Increased intracranial pressure as tumor enlargesC. Diagnostics
1. History and physical exam
2. CT scan 3. Magnetic resonance imaging (MRI)
D. Management1. Expected outcome: removal of the tumor with minimal harm to the
nervous system2. Depends on the location and size of the tumor 3. Treatment for associated increased intracranial pressure from
tumorsa. surgeryb. craniotomy to remove tumor

8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 36/52
c. stereotactic laser surgeryd. radiation therapy for malignancy
4. Medications for malignant tumors: chemotherapyE. Nursing interventions
1. Provide:
a. care of the client with increased intracranial pressure from
tumors b. care of the client undergoing
I. surgeryII. radiation therapyIII. chemotherapy
c. seizure precautions
d. seizure care e. balanced nutrition and fluid
2. Facilitate emotional support with referrals to support groups for theclient and family
X. Peripheral Nerve and Cranial Nerve DisordersA. Trigeminal neuralgia (tic douloureux)
1. Syndrome of paroxysmal facial paina. occurs more often in middle age and older adultsb. affects cranial nerve five (trigeminal nerve)c. has unknown etiologyd. involves one side onlye. is triggered by harmless events such as a breeze, hot or
cold liquids2. Findings
a. intense facial pain lasting about one to two minutes alongthe nerve branchesb. extreme facial sensitivityc. pain may be described as "burning" or "shooting"
3. Diagnostics: history and physical exam4. Management
a. expected outcomes: to relieve pain and to minimizefrequency
b. anticonvulsants: carbamazepine (tegretol), phenytoin(dilantin)
c. surgeryI. minor
I. radio-frequency gangliolysis: heat destroystrigeminal ganglion
II. glycerol gangliolysis: glycerol injected intosubarachnoid space around gasserianganglion
II. major - microvascular compression: move arterialloop away from posterior trigeminal root
5. Nursing interventionsa. help clients to name trigger points with identification of
triggering incidentsb. recommend restful environment with scheduled rest
periodsc. reinforce the need for balanced nutritiond. provide appropriate care of the client undergoing surgerye. teach client
I. about medications and side effectsII. to avoid triggering agentsIII. to chew on the opposite side of the mouthIV. to avoid draftsV. to avoid very hot or cold foods or fluids

8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 37/52
B. Facial nerve paralysis (bell's palsy)1. Definition/etiology
a. is a disorder of cranial nerve seven (facial nerve)
b. involves one side only; unilateral c. has an unknown etiology
d. often occurs during periods of high stress2. Findings often occur suddenly over ten to 30 minutes
a. ptosis b. cannot close or blink eye with excessive tearing
c. flat nasolabial foldd. impaired tastee. lower face paralysisf. difficulty eating - impaired mastication of food and difficulty
swallowing3. Diagnostics: history and physical exam4. Management
a. expected outcome: to restore cranial nerve functionb. medications
I. prednisoneII. analgesics
c. local comfort measures: heat, massage and electricalnerve stimulation for muscle tone
d. alternative therapies: reiki, massage, imagery5. Nursing interventions
a. reinforce balanced nutrition with a soft dietb. administer drugs as orderedc. teach client
I. to chew on the opposite sideII. how to use protective eye wear during risk periods -
patch or glasses over eyeIII. effects of steroidsIV. the use of eye drugs or ointment to protect the eye
from corneal irritationV. that once findings disappear their return may occur
especially in times of high stress
Points to Remember
• In multiple sclerosis, early changes tend to be in vision and motor sensation; late changes tend to bein cognition and bowel control.
• Peripheral nerves can regenerate. However, nerves in the spinal cord are thought to not be able toregenerate.
• During a seizure, do not force anything into the client's mouth or attempt to suction the mouth.• A major problem often associated with a left-sided brain infarction (CVA) is an alteration in
communication.• Clients with CVAs are at a greater risk for aspiration. Initially these clients must be evaluated to
determine if dysphagia is present.• Changes in a client's respirations (rate, rhythm and depth) are more sensitive indicators of
increases in intracranial pressure than blood pressure and pulse.• When caring for a comatose client, remember that the hearing is the last sense to be lost.• Clients after a CVA often have a loss of memory, emotional lability and a decreased attention span.• Communication difficulties of a client with a CVA usually indicate involvement of the dominant
hemisphere, usually the left brain, and is associated with right sided hemiplegia or hemiparesis.• The client with myasthenia gravis will have more severe muscle weakness in the evening due to the
fact that muscles weaken with activity - described as progressive muscle weakness - and clientsusually regain strength with rest.

8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 38/52
XI. Senses: Eye and Ear I. Eye structures
A. Three layers of the eye: sclera, choroid, and retina1. Sclera: maintains eye shape
2. Choroid: packed with blood vessels and pigmented toabsorb light and prevent blurring of an image
a. choroid forms iris and lens in front
b. Schlemm's canal (venous sinus) circles wherecornea and iris meet; iris gives eye its color
c. muscles of iris adjust pupild. pupil adjusts to
i. protect retinaii. allow enough light to stimulate retinaiii. improve depth perceptioniv. respond to sympathetic nervous system
with dilation
e. ciliary body (smooth muscle) contracts to reducetension of suspensory ligament on the lens
f. lens converges light onto the retina3. Retina: inner, posterior layer that is photosensitive
a. consists of four layers
i. pigmented epithelial cellii. photoreceptor cells (rods and cones)
iii. bipolar neuron
iv. ganglion neuron
b. optic disk: retinal area of optic disk contains nophotoreceptors (blind spot)

8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 39/52
c. photoreceptor cells: turn light into nerve impulses tooptic nerve, cranial nerve II
i. rods: located more peripherally - aroundedges of retina
I. black, white, gray visionII. peripheral vision
ii. cones: located in fovea centralisI. three types: red, green, and blue
receptorsII. fine discrimination and color vision
B. Optic nerve, cranial nerve II
1. Nerve fibers from median half of each retina cross at chiasm andtravel to opposite sides of the brain
2. Nerve fibers from lateral halves of retina remain uncrossedC. Chambers
1. Anterior chamber (locus of intraocular pressure [IOP])
2. Posterior chamber
D. Vitreous body
E. Lens 1. Separates the posterior chamber from the vitreous body2. Are transparent3. Are held in position by suspensory ligaments attached to the
ciliary bodyF. Accessory structures
1. Protective structures: sockets, eyelids, eyelashes, eyebrows,conjunctiva
EYE STRUCTURES
A. Chambers1. Anterior chamber filled with aqueous humor
a. Secreted near ciliary bodyb. Circulates through suspensory ligament and pupil and under corneac. Exits through the canal of Schlemmd. Enhances light refractione. Cleans and nourishes the eye structures
f. Determines intraocular pressure: Normal 16-30 mm Hg 2. Posterior chamber
a. Narrow passage behind the irisb. In front of the lens and the ciliary body
B. Vitreous body1. Filled with vitreous humor 2. Holds the retina in place
C. Optic nerve1. Nerves from each eye meet at the optic chiasm2. Nerve fibers from median half of each retina cross at chiasm and travel to
opposite sides of the brain
3. Nerve fibers from lateral halves of the retina remain uncrossed

8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 40/52
2. Lacrimal duct: secretes and drains fluid that moistens andlubricates the front surface of the eye; with decreased blinkingless secretions result with complaints of "dry" or maybe "itchy"eyes
3. Six oculomotor muscles surround and enter the eyeball
II. Eye Functions A. Light reception
1. Light passes through the cornea, aqueous humor, lens, andvitreous body to the retina
2. The density of the cornea slows the light, and the curvature of thecornea bends the light (called refraction)
3. The lens further bends and redirects the light to a point on theretina
4. At this point, the light stimulates photoreceptor cells (rods, cones)which transmit electrical impulses
5. These impulses travel through the optic nerve to the brainB. Accommodation - decreases with aging and the loss begins int the 40 to
50 year olds1. Process by which the lens changes shape to view an object at
close range (or long range)
2. Proper vision requires three processes:
a. convergence: image of the object falls exactly on the foveacentralis retinae of both eyes
b. focus: focusing of the lens (ciliary body [ciliary muscles] tocontract or relax)
c. light regulations constriction or relaxation of the pupils toregulate light and to clarify the image on the retina
3. When muscles that carry out these three processes are weak or paralyzed the finding is called strabismusC. Binocular vision
1. Allows the brain to judge distance2. Brain judges
a. the difference between two imagesb. the amount of retina taken up by the image

8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 41/52
c. the difference between familiar and unfamiliar objects(example: person standing next to an elephant)
d. the different shades of color
3. Both eyes must move together for clear focus (called conjugateeye movements). Thus, to immobilize one eye, both eyes must becovered
III. Disorders of the Eye
Overview and content: eye disorders from the front to the back of the eye
Eye disorders from most common to least common
A. Disorders of refraction 1. Myopia (near-sightedness) - blurred distance vision, but clear
close vision2. Hyperopia (far-sightedness) - blurred close vision, but clear distant
vision3. Presbyopia - in middle age, lens loses elasticity with results of
hyperopia
4. Astigmatism - lens refracts light rays to focus on two differentpoints of retina
B. Eye trauma care1. Foreign body
1. use eversion procedure
2. if foreign body has penetrated, do not remove the foreignbody
3. irrigate affected eye with sterile normal saline eye irrigant
2. Corneal abrasion 1. disruption of the cells and loss of superficial epithelium2. caused by trauma, chemical irritant, foreign body, or lack of
moisture
8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 42/52
3. findings: severe pain, blurred vision, halo around lights,lacrimation, inability to open eye, photophobia
4. diagnosis by fluorescein sodium dye5. abrasions heal usually within 48 hours with no scarring or
visual deficit6. treatment includes short-acting analgesic drops, eye rest
with soft or rigid eye patch
3. Corneal laceration 1. same causes and findings as with abrasions2. lacerations are serious emergencies to require immediate
attention3. surgery is generally required
4. follow care for client undergoing eye surgery (see points toremember at the end of this section)
4. Penetrating injury1. immediate care
1. do not remove the object2. do not apply pressure of any kind to the eye or the
object3. cover the injured eye to protect movement of the
object. may use a paper or plastic cup or rigid eyepatch
4. cover uninjured eye with soft or rigid eye patch toavoid sympathetic movement
2. get client to emergency room immediately3. surgery will be required
5. Chemical irritants1. flush eye with plenty of tap water or sterile normal saline if
available2. get client to emergency room immediately3. alkaline substances penetrate the cornea rapidly and must
be removed quickly; these injuries are a priority to care for 4. acids coagulate the eye's proteins and often result in
relatively superficial, reversible damage
6. Ultraviolet burns1. often occur from sun exposure or welding flashes – looking
at a welding flame without special glasses during thewelding process
2. rritate epithelium, which swells and scales off (desquamation)
3. care is the same as with lacerations7. General pharmacotherapy for eye trauma
1. topical anesthetics2. topical anti-inflammatory3. topical mydriatic-cycloplegic agents to prevent papillary
constriction8. General management of any eye trauma
1. do copious irrigation of the affected eye2. apply bilateral rigid or soft eye patches to rest both eyes by
decreased eye movement3. have clients use tinted glasses for photophobia to reduce
eye discomfort from artificial lights or sunlight4. assist clients with activities of daily living as needed5. review with clients to avoid activities which increase IOP
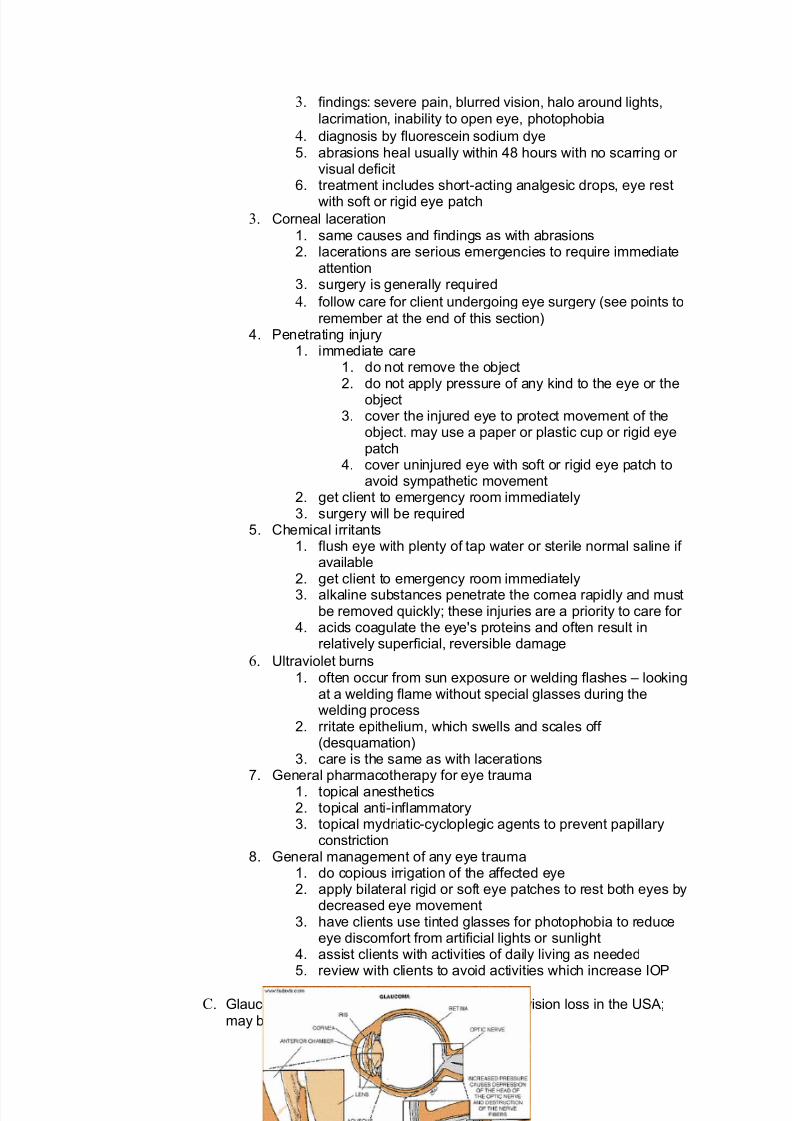
C. Glaucoma - the second most common cause of vision loss in the USA;may be unilateral or bilateral

8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 43/52
1. Most common type: chronic open-angle glaucoma (simple, adultprimary, primary open-angle)
1. etiology/epidemiology1. hereditary link2. unknown etiology
3. aqueous humor does not drain adequately whichleads to increased intraocular pressure (IOP)
4. this pressure on optic nerve causes destruction of nerve fibers in the retina to result in a vision loss
2. findings1. most clients are without findings until there is a lossof vision
2. peripheral vision loss is affected first prior to totalloss of vision
3. three classic assessment findings
1. visual field loss (peripheral)
2. elevated IOP 3. cupping of the optic disk
3. diagnostics
Diagnostic Eye Tests
A. Electroretinography1. Detects diseases of the rods and the cones2. Evaluates the electrical potential between the retina and the cornea3. Method: electrodes incorporated into contact lenses are used to measure the
changes in the wavelength and intensity of light and for the state of adaptation of theeye
B. Tonography1. Indirect measurement of intraocular pressure (IOP)2. Used to detect glaucoma
C. Intravenous fluorescein angiography1. Records the appearance of blood vessels within the eye2. Used to evaluate for retinopathy and tumors3. A contrast dye is injected intravenously and numerous photographs are taken of the
fundus oculi4. Check client for sensitivity or allergy to fluorescein dye prior to the test5. Mydriatic drops are used to dilate pupil
D. Ocular ultrasonography1. Use of high frequency sound waves to evaluate eye structures2. Particularly useful when eye is clouded with an opaque medium such as a cataract
or hemorrhageE. Electronystagmogram: record of electrical activity of eye during spontaneous, positional and
calorically-invoked nystagmus A. General nursing interventions in electrodiagnostic studies
A. always explain test to clientB. client must remain still during test unless instructed to do otherwiseC. client should avoid stimulants before test

8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 44/52
d. managementi. expected outcomes - reduction of IOP and
prevention of visual field defectsii. treatment of choice: pharmacotherapy
• miotic eyedrops (parasympathomimeticagents)
• carbonic anhydrase inhibitors - Diamox• beta-adrenergic blocking agents - Timoptic
drops• epinephrine eyedrops (contraindicated in
clients with cardiac conditions) - used moreoften in emergency care
iii. trabeculectomy or laser trabeculectomy• performed when pharmacological agents
are not effective• small piece of sclera containing the
trabecular network is removed and aniridectomy is performed
• cycloplegic and steroids eye drops areusually used
• antibiotics may be ordered• a mydriatic eye drop medication is then
used to prevent adhesions to the cornea;remember that use of this classification of medications is contraindicated withglaucoma
e. nursing interventions
i. for pharmacotherapy management• reinforce the need for compliance with
medical treatment• teach client how to instill eye drops and
when - usual recommended time is beforebedtime
• teach the need to reduce or eliminate safetyrisks related to impaired vision
ii. for trabeculectomy by traditional surgery• monitor dressing for excessive bleeding• administer antiemetics, analgesics,
mydriatics and antibiotics as ordered• assist the clients with ADL as needed
iii. for trabeculectomy by laser surgery• discuss that vision may be blurred for first
day or two post-op• teach to use soft or rigid eye patches or
sunglasses for photophobia• discuss the use of analgesics as ordered
iv. general education for clients with glaucoma• stress the need to avoid activities that
increase IOP - bending, stooping, straining,coughing, blowing nose, laughing
• stress the importance of routine eye exams-
usually yearly or more often if complicationsor noncompliance with medication regimen
2. Less common type: acute closed-angle glaucoma (shallow,narrow-angle, or congested glaucoma)
a. etiology /epidemiologyi. a medical and nursing emergency

8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 45/52
ii. iris lies near drainage channel (canal of Schlemm)and bulges forward against cornea, blocking thetrabecular network with the result of increasing IOP
iii. affects more women; usually after age of 45b. findings
i. sudden onset of blurred vision, halos or colored
rings around white lightsii. sudden frontal headache
iii. sudden severe eye pain, reddening of the eye,nausea, vomiting
iv. followed by progression of findings as the pressureincreases
• profuse lacrimation• mildly dilated, nonreactive pupil• more severe nausea/vomiting• cornea appears hazy
v. blindness may result in two to five days if leftuntreated
c. diagnosticsi. history of findingsii. ocular pressure readings
d. managementi. expected outcome: to prevent or minimize the
damaging effects of acute closed-angle glaucomaii. emergency pharmacologic treatment to decrease
IOP• intravenous osmotic agents• topical miotic eye drops• systemic carbonic anhydrase inhibitors• systemic analgesics
iii. surgery• iridotomy or iridectomy • procedure is usually then repeated on the
unaffected eyee. nursing interventions
i. monitor for effectiveness of medications as orderedii. apply eyepatch or sunglasses for post-op
photophobiaiii. discuss with clients that vision is more often blurred
for one to two days postsurgeryiv. stress the importance of routine yearly or more
frequent eye examinations
v. teach clients to avoid activities that increase IOP
D. Cataract1. Etiology
a. clouding of lens - may be unilateral or bilateral; one of themost common eye disorders
b. first type: senile cataract - result of aging processc. second type: traumatic
i. develops within a few months after eye traumaii. painless but progressive loss of sight in one or both
eyes2. Findings
• vision becoming clouded, blurred or dim
• Sensitivity to light and glare
• Halos around lights
• Fading or yellowing of colors
• Double vision or multiple vision in one eye
• You might find it harder to see at night3. Diagnostics

8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 46/52
a. historyb. physical exam of eyes
4. Managementa. expected outcome: correction of visual field defectb. treatment: only surgical
i. cataract extraction: removal of cloudy lens• most commonly done as an outpatient
procedure• usually done on one eye at a time• types of cataract extractions
o extracapsular cataract extraction
(ECCE) procedure of choice lens contents removed and
the posterior chamber is leftintact
o phacoemulsification – ultrasound
fragments of the lens contentso intracapsular cataract extraction
(ICCE) the lens contents and lens
capsule are removed eye becomes hypermetropic
c. intraocular lens implant is usually performed at the time of the extraction
d. peripheral iridectomy is usually performed as part of anECCE or ICCE
5. Potential post-surgical complications
a. hyphema (blood collects in the anterior chamber of theeye)
i. may require bed rest and eye patchingii. observe for increased IOP - indicated by complaints
of severe pain
iii. may have prescribed miotics or cycloplegics
b. vitreous prolapse
i. allows vitreous humor to fall forward into woundii. may result in pupil function blockediii. may lead to retinal detachmentiv. vitrectomy may be performed
c. intraocular infectioni. complaints of throbbing or pain with cloudy
drainage from the eyeii. antibiotics (ophthalmic and/or systemic)
6. Nursing interventionsa. teach client to avoid actions that cause IOPb. observe clients' ability to instill eyedrops correctly; provide
referrals if clients unable to do soc. provide written list for findings of complications to reportd. inform clients
i. an expected, normal feeling after cataract surgeryis that "sand" is in the eye for six to eight weeksafterwards
ii. photophobia, that may be present for months toyears, simply requires the use of sunglasses inbright light
E. Retinal detachment
8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 47/52
1. Etiology/epidemiologya. holes or breaks (tears) in the retinab. fluid, blood or a mass separates the retina's sensory layer
from the pigmented epithelium (pigment cells)c. common causes are inflammation, trauma, hemorrhage,
and tumorsd. retinal detachment often begins in the periphery andspreads posteriorly
2. Findings
a. a rapid separation gives the sense of a "curtain beingpulled over the eye" so that clients have partial vision inaffected eye
b. a slow separation may be asymptomaticc. the ophthalmic exam reveals the detached area as gray
bulge, ripple or fold3. Diagnostics
a. history
b. physical inspection4. Management
a. expected outcome: correction of and/or prevention of further vision loss: 90% are successfully repaired
b. laser surgeryi. photocoagulation: laser beam is directed through a
dilated pupilii. the effect is to seal localized breaks or rips in the
retinac. cryotherapy: extreme cold freezes rips in the retinad. diathermy: heat is applied with ultrasonic probe to repair
rips
e. scleral bucklef. pharmacotherapy: local or systemici. adrenergic-mydriatic agents
ii. cycloplegic agentsiii. antibiotics
5. Nursing interventionsa. maintain the client in proper position for bed or chair rest
as orderedb. apply a post-op rigid/soft eye patch to rest eye (or both
eyes)
c. suggest dark lens glasses for photophobia d. administer medications as ordered
e. prevent activities that increase IOP
F. Visual impairment and blindness1. Legal blindness: a maximum visual acuity of 20/200 (with optimum
correction) and/or a visual field that is reduced to a range of 20degrees (normal range: 180 degrees)
2. Most common causes: retinal degeneration, glaucoma, cataract,amblyopia, macular degeneration - called "central" loss of vision

8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 48/52
3. Nursing interventionsa. speak to clients upon entering the roomb. implement safety measures based on how clients
accomodate the loss of sightc. orient clients to new surroundings; use numbers on
traditional clock for the placement of furniture or food on
platesd. assist clients with activities of daily living as needed
e. for walking, do not take clients' arm to lead. Offer clientsan arm so that the blind person holds the arm at the elbowof the lead person who walks a little in front of the blindperson.
The Ear
I. Structures of Ear - note the pinna - this is what is pulled when ear drops aregiven
A. External auditory meatus B. Middle ear
1. Tiny, air-filled cavity containing three small bones: incus (anvil),malleus (hammer) and stapes (stirrup)
2. These bones (ossicles) are connected by joints and supported bymuscles
3. Ossicles bridge the tympanic membrane and the oval window4. Ossicles magnify small sounds by transmittting them from the
tympanic membrane to the oval window.C. Inner ear

8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 49/52
1. GeneralI. Contains the sensory receptors for sound and equilibrium
II. is connected to nasopharynx by the eustachian tubeIII. the eustachian tube opens during swallowing to equalize
inner ear pressure to the atmospheric pressure
IV. is composed of fluid-filled membranous labyrinth in asimilarly shaped bony labyrinth
V. membranous labyrinth components include the cochleaand the vestibular apparatus
2. Cochlea: a spiral tube
I. within the cochlea is a membranous duct with a triangular cross section:
I. side one lies against wall of bony labyrinth
II. side two is made up of Reissner's membraneIII. side three is Organ of Corti (basilar membrane)
which contains the tectorial membrane, connectedby hairs to sound-receptor cells
IV. hairs of receptors convert sound waves to neuralimpulses
V. impulses travel via the acoustic or eighth cranialnerve to the brain
Diagnostic1. Electrocochleogram
a. measures auditory function
b. nursing intervention: be aware that client may experiencevertigo c. assure client safety
2. General nursing interventions in electrodiagnostic studiesa. always explain test to clientb. client must remain still during test unless instructed to do

8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 50/52
II. vestibular apparatus: reflects body position
I. surrounded by perilymph and temporal boneII. consists of membranous saccule, utricle, and
semicircular canals
III. in these canals, static and dynamic equilibriumreceptors send impulses to the brain regardingbody position
II. Ear Disorders A. External ear
1. Swimmer's ear
a. diffuse bacterial otitis externab. preventable by using 70% alcohol to cleanse ears after
swimming
2. Otitis externa
B. Middle ear: otitis media
C. Inner ear: Meniere's disease1. An inner ear disorder: the endolymphatic system dilates and the
volume of endolymph expands2. Etiology unknown
a. usually develops between the ages of 40 and 60b. acute attack may require hospitalizationc. clients may average two to three attacks per year
3. Findingsa. attacks intermittentb. three recurrent and progressive findings
i. vertigo with prostrating nausea and vomiting
ii. tinnitus iii. hearing loss on involved side persists and
progresses4. Diagnostics
a. historyb. direct inspection
5. Managementa. expected outcomes: prevention of hearing loss and control
of vertigob. medical
i. cholinergic blocking agents such as atropine
ii. antihistamines or decongestantsiii. during remission• diuretics to decrease fluid accumulation• vasodilators such as histamine• vestibular suppressants such as diazepam
(valium)• adrenergic neuron-blocking agents such as
epinephrine

8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 51/52
• low-salt dietc. surgical
i. decompression of endolymphatic sac: insertion of an endolymphatic subarachnoid shunt
ii. labyrinthectomy: client will lose all hearing inaffected ear
5. Nursing interventions during an acute attack of Meniere's diseasea. keep clients on bed rest in a quiet, dark roomb. avoid unnecessary movement of clients especially of their
headc. give general care to clients with nausea and vomitingd. restrict salt and water intake as orderede. have clients avoid tobacco, caffeinef. institute precautions to prevent clients from falling
g. discuss the need to avoid a high triglyceride diet
D. Otosclerosis 1. A hereditary degenerative disorder that results in conductiondeafness
2. The formation of new bone growth in labyrinth adheres the stapesto the oval window
3. Etiology unknown4. Findings
a. hearing loss
b. tinnitus 5. Diagnostics
a. bone conducts more sound than air does6. Management
a. expected outcome: improvement of hearing in the affectedear b. medical: use of a hearing aidc. surgical: stapedectomy - replacement of stapes with a
prosthesis7. Postoperative care
a. teach clients to avoid anything that might displaceprosthesis, such as coughing, blowing nose, swimming
b. limit activity as ordered and as tolerated
c. give medications as ordered: antiemetics, analgesics,antibiotics
d. assess facial nerve function for asymmetry
e. keep external ear area dryf. instruct client not to fly for at least six months
Points to Remember
Eye • Anything that dilates the pupil obstructs the canal of Schlemm and increases
intraocular pressure.• Color blindness is caused by a deficiency in one or more types of cones and is
caused by a sex-linked recessive gene.
• Destruction of either the right or left optic nerve tract results in blindness in therespective side of both eyes
• When mydriatics are instilled and the pupils have been dilated, caution clientsthat vision will be blurred and they will have photophobia for one to two hours
• After eye surgery teach clients to avoid activities that can increase IOP for sixweeks
• Stooping• Bending from the waist

8/2/2019 Neurological Problems and Management
http://slidepdf.com/reader/full/neurological-problems-and-management 52/52
• Heavy lifting• Excessive fluid intake• Emotional upsets - crying, laughing• Constrictive clothing around neck• Straining during bowel movement (i.e., straining at stool)• Sustained coughing or blowing of the nose
• Teach clients proper administration of eyedrops; most importantly to wash their hands before drop installation
• Advise the use of sunglasses for photophobia• Assist with activities of daily living as needed• When clients wear one eye patch, they lose their depth perception. Remember
that this loss presents a safety risk during mobility or cooking activities.• Systemic disorders that can change ocular status include diabetes mellitus,
atherosclerosis, Graves' disease (hyperthyroidism), AIDS, leukemia, lupuserythematosus, rheumatoid arthritis sickle cell disease.
• If there is some problem with the pigments in the cones, the eye will not seecolors in the usual way. This is called color deficiency or color blindness.
• If just one pigment is missing, the eye might have trouble seeing certain
colors. Red-green colorblindness - where red and green might look thesame - is the most common form of colorblindness, followed by blue-yellow colorblindness.
• In some eyes, none of the pigments are present in the cones, so the eyedoes not see color at all. This most severe form is known asachromatopsia
• Color blindness is a genetic condition that only rarely occurs in women,but affects about 1 out of every 10 men to some degree.
Ear • Changes in barometric pressure will affect persons with ear disorders to cause
increased findings or malfunctions• Hearing loss can
• be partial or total• affect one or both ears• occur in low, medium or high frequencies
• In the elderly the loss of high frequency sounds may require special smokedetectors with low frequency sounds
• The American Medical Association formula for hearing loss: hearing is impaired1.5% for every decibel that the pure tone average exceeds 25 decibels (dB)
• A hearing loss of 22.5% usually affects social functionality and requires a hearingaid
• Noise exposure is the major cause of hearing loss in the United States of America
• Ask clients how they communicate: lip-reading, sign language, body gestures, or
writing• To gain a client's attention, raise a hand or touch the client's arm• When talking with clients who have a hearing loss, speak slowly and face them• Speak toward the client's good ear • If the client wears a hearing aid, allow him/her to show how it is inserted, turned
off/on, and cleaned• Speaking louder to a hearing impaired clients does not increase their chances of
hearing• Communicate about clients with a hearing loss to other staff members• Ototoxic drugs include:
• Aminoglycosides• Antimyobacterials•
Thiazides• Loop diuretics• Antineoplastics