neurological risk at younger ages - nittoli schoonbee...neurological risk at younger ages 2012 aaim...
TRANSCRIPT
Neurological Risk at Younger Ages
2012 AAIM Triennial
Paul J. Nittoli, MDMassMutual Financial Group
John Schoonbee, MBChBSwiss Re
Presentation Objectives
• Discuss risk stratification of seizure disorders for both disability and life underwriting: clinical, diagnostic, treatment, and lifestyle factors
• Discuss mortality assessment in Multiple Sclerosis: risk implications of clinical features, diagnostic findings, and disease-modifying medication use
Brief History of Epilepsy
• 4500-1500 BC: described in Ayurvedic literature (‘apasmara’ = loss of consciousness)
• 1000 BC: described in a Babylonian tablet as supernatural
• 400 BC: Hippocrates’ monograph disputes supernatural cause
• 130-200 AD: Galen theorized it a brain disorder with manifestations governed by the moon (‘lunatics’)
• 1494: Malleus Maleficarum links seizures with witchcraft
• 1800s: John Harvey Kellogg (of corn flake fame) attributed epilepsy to masturbation
Temkin. The Falling Sickness: A history of Epilepsy from the Greeks to the Beginnings of Modern Neurology. 2nd ed. 1971. The Johns Hopkins University Press
Seizure Disorders: Defining Terms
• “an excessive and disorderly discharge of central nervous system tissue on muscle”– John Hughlings Jackson MD, 1870
• Motor (convulsive)
• Sensory
• Autonomic
• Psychic
• Epilepsy: A) 2 unprovoked seizures 24 hrs apart; B) 1 seizure within the context of a predisposing cause
Seizure Disorders: Defining Terms
• Partial (focal) seizures – focal onset• Simple – no alteration of consciousness
• Complex – impaired consciousness
• Generalized seizures – bilateral onset, presumption of impaired consciousness
• Secondary generalization of partial seizures
• Absence (petit mal)
• Tonic +/- clonic (grand mal)
• Juvenile seizure disorders
• Pseudoseizures
Electroencephalogram
• “excessive and disorderly discharge” of cortical neurons
• Anticonvulsants are most effective at blocking propagation of neural activity from the seizure focus
• Asymptomatic interictalspikes may be present
• Absence of epileptiformdischarges does not rule out a seizure disorder

Alternative AED Uses
• Valproic acid: psychiatric, analgesic
• Carbamazepine: psychiatric, analgesic
• Gabapentin: psychiatric, analgesic, menopausal sx
• Lamotrigine: psychiatric, analgesic
• Topiramate: psychiatric, analgesic, substance abuse, obesity
• Levetiracetam: psychiatric, autism, Tourette syndrome
• Primidone: essential tremor, LQTS
• Phenobarbital/ethosuximide/phenytoin: AED only
Seizure Recurrence after AED
Withdrawal• Poor prognostic factors
• Abnormal (sleep-deprived) EEG• Abnormal brain MRI• Poor control with monotherapy• Certain epileptic syndromes (JME)• FHx of seizure disorder• <2-5 years seizure-free on treatment
» 65-75% of pre-adolescents (≤12yo) & 60% of adults who are seizure-free x several years (mean 3 yrs) and w/o negative indicators will remain seizure-free off AEDs)
Neurology 1996;47:600
• Risk windows for relapse in children• 50% during 1st 3-6 months• 60-80% within 1st year• >80% within 1st 5 years
Nonpharmacologic Seizure
Management• Surgery
• Usually done for intractable epilepsy• Generalization improvement• Focal seizures often not ameliorated and may worsen• Residual neurological deficits• Best outcomes: unilateral temporal or hippocampal loci
• Vagal nerve stimulation• Palliative not curative• Partial seizures
• Ketogenic diet• Failure of AED control• Mimics starvation – little or no carbs (Crisco)• Effectiveness: 1/3-1/3-1/3
Occupational and Lifestyle
Precautions
• Motor vehicle operation
• Water• Swimming
• Bathing
• Boating
• Heights
• Fire (esp. cooking-related burns)
• Power tools
• Sports

Epileptic Syndromes - Infancy
• Seizures within 24-48 HOL are often indicative of severe cerebral insult (less common are benign familial & idiopathic neonatal convulsions – begin 48-72 HOL and remit by 2-6 mos)
• Simple febrile seizure• Ages 6mos-5yo, <15 min duration, recurrent in 1/3
• 2x risk for epilepsy c/w general population risk
• West Syndrome/Infantile Spasm• Recurrent trunk/limb flexion “salaam seizures”
• Hypsarrhythmia (severely disordered EEG)
• Remit by 4-5 yo but may have residual mental impairment or seizure disorder
Epileptic Syndromes - Childhood
• Lennox-Gastaut syndrome – poor px
• Rolandic epilepsy• Benign childhood epilepsy w/ centrotemporal spikes
• Onset 5-9yo, disappears during adolescence
• Auto Dom, control w/monotherapy
• Absence (petit mal) seizures• 3Hz spike-and-wave pattern diagnostic
• Complex seizure disorder
• Good AED response; nearly ½ develop GTCS
Epileptic Syndromes - Adolescence
• Most common window of clinical presentation
• Idiopathic seizures
• Juvenile myoclonic epilepsy• Peak incidence 12-18 yrs
• Complex seizure disorder in most
• Control w/low dose monotherapy
• Lifelong seizure risk
Epileptic Syndromes - Adulthood
• Idiopathic
• Trauma
• Intracranial mass lesions
• Intracranial vascular lesions (blood isepileptogenic)
• Infections
• Metabolic encephalopathies
• Substance abuse

Pseudoseizures
• Psychogenic nonepileptic seizures
• 20-50% of referrals to tertiary epilepsy centers
• Somatoform disorder vs. factitious
• Typically begin in adolescence but incidence in all ages; 70% female
• Dx by video-EEG monitoring (gold std), provocative techniques, and CPK measurement
Epilepsy-related Mortality
• Japanese population of an epilepsy center (1765); 43 deaths over an 8-year period– Accidents 30% (drowning & head injury)
– SUDEP 23%
– Status epilepticus 16%
– Suicide 14% (all temporal lobe epilepsy)
– Other 16%Fukuchi T, et al. Epilepsy Res 2002;51:233.
• Other community-based studies in Western countries show most of the mortality in accidents and “other” (CNS tumors, vascular disease, pneumonia)Lhatoo SD, et al. Epilepsia 2005;46 s11:36
Status Epilepticus
• Continuous seizures for >1 hour
• Neuronal death: combination of systemic and
CNS- specific factors (intraneuronal calcium)
• Mortality increases with age
• Frequently the initial presentation in children
• Mortality risk is defined by age, etiology, and
ability to achieve control (<5% mortality directly
attributable to SE)
Sudden Unexpected Death in
Epilepsy (SUDEP)• Defined as SUD with or without evidence of a seizure in
a person without identified status epilepticus or toxicological, traumatic, anatomical cause
• Cardiopulmonary etiologies postulated
• Low incidence in community-based cohort: 0.35-2.7/1000 p-yrsLhatoo SD, et al. Epilepsia 2005;46 s11:36
• Risk factors• Males, age 20-40
• Frequent GTC seizures, polytherapy
• Treatment noncompliance
• AlcoholHesdorffer DC, et al. Epilepsia 2011;52:1150
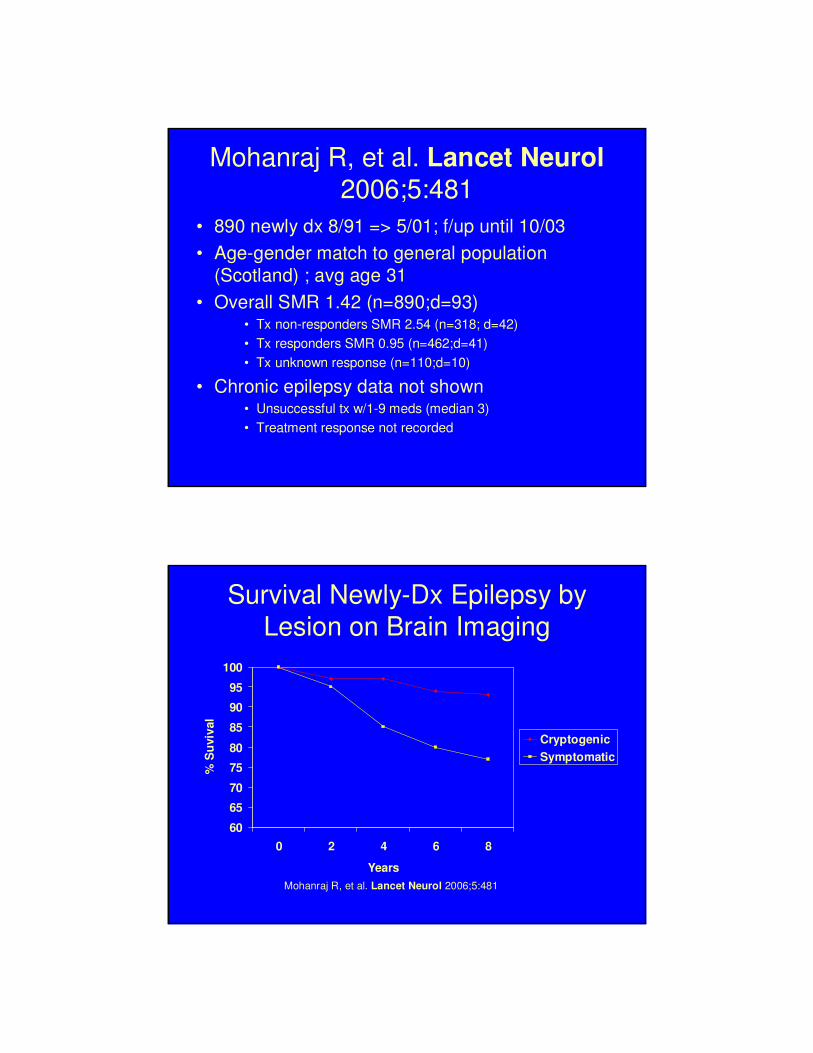
Mohanraj R, et al. Lancet Neurol
2006;5:481
• 890 newly dx 8/91 => 5/01; f/up until 10/03
• Age-gender match to general population
(Scotland) ; avg age 31
• Overall SMR 1.42 (n=890;d=93)• Tx non-responders SMR 2.54 (n=318; d=42)
• Tx responders SMR 0.95 (n=462;d=41)
• Tx unknown response (n=110;d=10)
• Chronic epilepsy data not shown• Unsuccessful tx w/1-9 meds (median 3)
• Treatment response not recorded
Survival Newly-Dx Epilepsy by
Lesion on Brain Imaging
60
65
70
75
80
85
90
95
100
0 2 4 6 8
Years
% S
uviv
al
Cryptogenic
Symptomatic
Mohanraj R, et al. Lancet Neurol 2006;5:481

Strauss D, Shavelle R, et al. JIM
2003;35:155• CA Dept. of
Developmental Services– 80,682 persons, ages 5-65
yo: 47K w/epilepsy out of 506K total [p-yrs], 266 epilepsy deaths out of 1523 total
– No assist for gait/stairs; ≤moderate MR; no “degenerative illnesses” or “idiopathic epilepsy”(presumably genetic)
– Epilepsy prevalence 10X general population
MR EDR
Epilepsy w/o Events <12
mos
111% 0.3
Epilepsy w/ Event <12
mos (not GTC)
237% 3.0
GTC <12 mos 293% 5.3
Status epilepticus <12
mos
371% 6.4
CDDS pop w/o epilepsy
c/w CA gen’l pop
171% 1.1
Approach to Epilepsy Risk
Assessment• Age
• Occupation/Avocation/MVR
• Seizure type• Focal vs. generalized
• Simple vs. complex
• Seizure Control• Frequency
• Number of AEDs in use
• Altered neuroanatomy• Brain injury/depressed skull fx
• Encephalitis
• SDH/AVM
• CVA

Magnetic Resonance Imaging
• Protons in water align
with the magnetic field of
the MRI coils
• A radiofrequency pulse
causes precession about this alignment
• After the pulse is turned
off, the protons “relax” to
their previous alignment
• Different tissue types
“relax” at different rates
MRI Terminology
• T1 – fat light, H2O dark (blackholes-MS/lacune; white-WMH); used with Gd contrast (active MS plaque)
• T2 – H2O light, fat dark (top right); white-MS plaque,lacune, WMH
• T2 FLAIR – free H2O dark, edema fluid light (bottom right)
• DWI – diffusion-weighted imaging (+) from minutes up to 2 weeks after acute ischemia

What can cause T2 Lesions on MRI?
• Demyelinating Disease
• Infectious illness
• Migraines
• Ischemic disease
• Neurofibromatosis
• Small vascular anomalies
• Unidentified Bright Objects
Multiple Sclerosis
• Lesions separated by space & time– Clinical exam – attack = neuro disturbance ≥
24hrs
– MRI – Gd/T1 or T2
– Lumbar puncture/CSF – oligoclonal IgGbands in CSF
• If suspicion of MS without meeting full criteria → clinically isolated syndrome (CIS)

MS – Signs & Symptoms
• Sensorimotor deficits (many CNS areas)
• Ataxia (parietal lobe/cerebellum/brainstem)
• Neurogenic bladder (multiple CNS areas)
• Internuclear ophthalmoplegia (abbrev. INO; brainstem)
• Facial pain/tic douloureux/trigeminal neuralgia (brainstem; trigeminal nerve)
• Lhermitte sign (cervical spinal cord)
• Cognitive impairment (50% eventually; diffuse cerebral disease)
• Optic neuritis (20% initial sx; optic nerve)
MS – Clinical Subtypes

MS Treatment
• Steroids
• Interferon (IFN)– beta-1a (2 preps, A & R), beta-1b (B)
• Other Immune Modulator – glatiramer acetate (C)
• Lymphocyte Sequestration – fingolimod
• ?mechanism – teriflunomide, BG-12
• Monoclonal Antibody – natalizumab
• Immunosuppressive Agent – mitoxantrone
Oral cladribine development withdrawn by Merck
What Is the Impact of MS on Mortality?
• Uncommon disease(s) + variable clinical course +
expect decades of life after onset = need for large cohort
followed for many years to estimate and categorize risk
• Danish study Onset 1948-86 122,373 p-yr
MS + CIS gen’l pop controls
– SMR from onset = 3.25
– EDR from onset = 13.0/1000 p-yr
– Median survival time from onset = 30 yrs
– Median survival time from diagnosis = 25 yrs(Brønnum-Hansen. Neurology. 1994;44:1901)
(Pokorski RJ. JIM. 1997;29:100)

Underwriting MS – Forks in the Road
• Diagnosis
Indefinite Definite
CIS/ON Early Stage Late Stage
MS – Unfavorable Prognosis =
High Risk
• Immobility- think paralysis or quadriplegia
• Primary or secondary progression
• Brain atrophy & cognitive decline
• Multiple black holes on MRI
• Renal function
• Suicide/MDD/substance abuse
• “novel therapy”• Bee stings, cobra venom, pregnant cow milk
• Chronic cerebrospinal venous insufficiency (CCSVI)
MS – Favorable Prognosis = Better Risk
• ♀ (higher prevalence; better outcomes)
• Younger age @ onset (pivot = 40yo)*
• Low relapse rate in early disease (first 2 years)*
• Complete recovery after relapse*
• Sensory/CN/ON as initial sx (motor/cerebellar worse pxas initial sx)*
• Lower lesion burden & accretion by MRI*
• EDSS = 0-3, 5 yrs after dx
• Response to disease-modifying MS drugs
(*early stage prognostic factors > Scott. Neurology. 2000;55:689.)
Kurtzke Expanded Disability Status Scale
• 10 point scale ranging from no disability (0.0) to death (10.0)
• “Functional systems” used for scores < 4.0
• “Cerebral” = cognition & mood
• Emphasizes ambulation
• Key breakpoints
– 3.0 moderate disability, fully ambulatory
– 6.0 at least unilateral ambulatory assist
– 7.0 wheelchair-dept; indept transfers
Generally, disability correlates with risk(Kurtzke. Neurology. 1983;33:1444.)

EDSS & Mortality
• Canadian study - MS clinic - diagnosis 1972-1985 - insured controls
# EDSS Death MR
1394 0.0-3.5 33 1.60
789 4.0-7.0 58 1.84
165 ≥7.5 24 4.44
2384 115 2.00
(Sadovnick. Neurology. 1992;42:991)
ABCR Drugs – Positive Factors
• In the short-term, they have been shown to reduce relapse-related EDSS progression; frequency of relapses; and MRI characteristics of inflammation
• IFNβ1a vs. placebo in delaying CDMS after CIS w/+MRI: CHAMPS Trial (Jacobs. NEJM. 2000;343:898) RR=0.56 p=0.002
• Other ABCR trials reduce progression to CDMS by ~30%
• For u/w purposes, ABCR drugs are equivalent

IFN Reduces RRMS => SPMS Progression
Trojano M. Ann Neurol. 2007;61:300.
• Observational, non-randomized study, median f/u 5.7 yrs (up to 7 yrs)
• 1103 treated
• 401 untreated (refused; contraindicated; early drug d/c; no relapses in 2yrs & EDSS<3)
• Various ABR drugs
• End points: Secondary progressive dz; stable EDSS 4 or 6
SP EDSS 4 EDSS 6
HR-progression from first visit to end point
0.38
p<0.0001
0.70
p=0.0174
0.60
p=0.0304
Shirani A, et al. JAMA 2012;308(3):247Derfuss T, et al. JAMA 2012;308(3):290
• Well designed observational study failed to show IFN reduced disability progression over a long term (>5yrs)– IFN-treatment group
– 2 untreated groups• Contemporary untreated• Historical untreated
• Caveats– Bias against tx of benign disease
– Underpowered
• IFN reduction in long-term disability, “although plausible, remains unproven”
ABCR Caveats
• Need 6-12 months to determine efficacy• Barriers to Use
– Injection-site reactions– Depression– Flu-symptoms– Fatigue– Headache
• Adherence to therapy– Adherence = acceptance + persistence + compliance– 60-75% adhere for 2-5 yr (IFN)– Adherence rates similar to insulin for type 2 diabetes– Majority who discontinue do so in the first 2 yrs (ABCR)– Other studies show first 6 mos indicative of persistence
(Costello. Medscape J Med. 2008;10:225)
(Tremlett HL. Neurology. 2003;61:551)
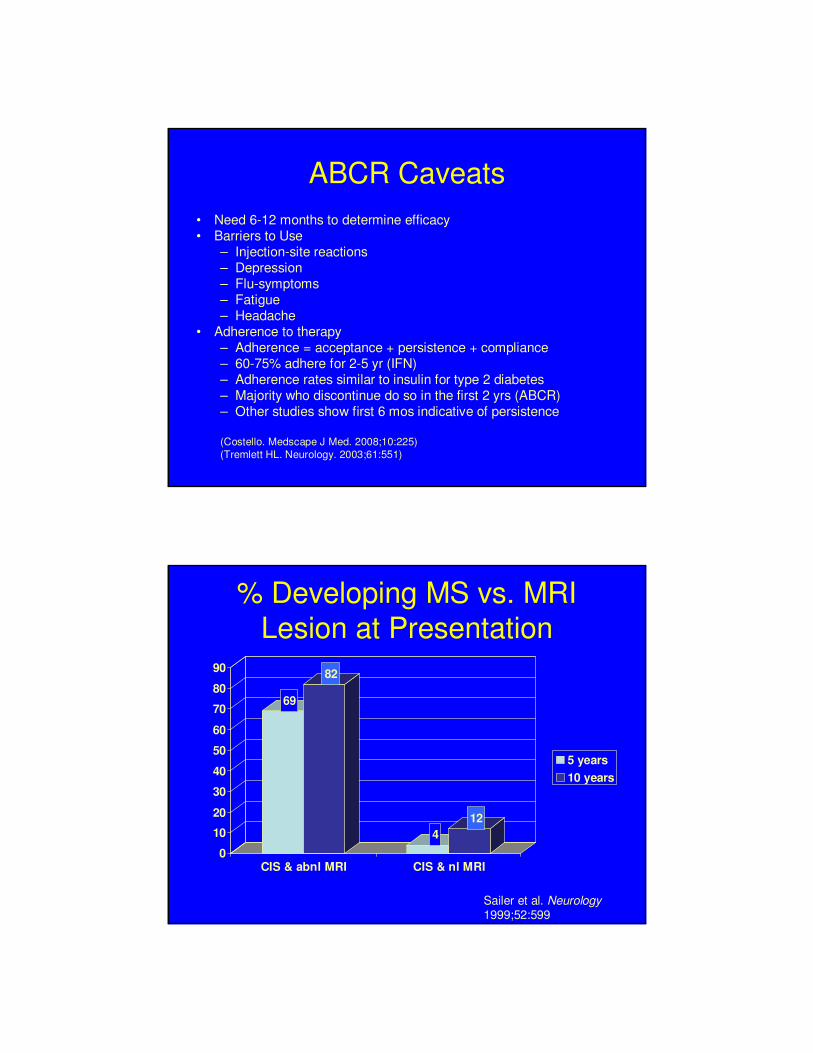
% Developing MS vs. MRI Lesion at Presentation
69
82
4
12
0
10
20
30
40
50
60
70
80
90
CIS & abnl MRI CIS & nl MRI
5 years
10 years
Sailer et al. Neurology
1999;52:599

MS Risk After Optic Neuritis Based on MRI Lesion Load
• Cumulative Probablility of MS vs. Lesions at Dx
0
10
20
30
40
50
60
70
80
90
0 Lesions 1-2 Lesions 3+ Lesions
5Years
10Years
15Years
ON Study Group. Arch Neurol. 2008;65:727.
MS Risk After Optic Neuritis Based on MRI Lesion Load
• Conditional Probablility of MS vs. Lesions at Dx
0
5
10
15
20
25
30
35
40
45
0 lesions 1+ lesions
0-5Years
6-10Years
11-15Years
ON Study Group. Arch Neurol. 2008;65:727.
Approach to MS Risk Assessment
• MRI
• Lesion burden & accretion
• Black holes
• Relapse rate
• Frequency
• Proximity to pre-lapse baseline
• Clinical subtype
• EDSS – 3 & 6 are important scores
• Disease-modifying therapy
• Response to treatment
• Medication choice
• Markers of high risk