new 2013 acc/aha guidelines on treatment of blood cholesterol to reduce atherosclerotic...
TRANSCRIPT

New 2013 ACC/AHA Guidelines on Treatment of Blood Cholesterol to Reduce
Atherosclerotic Cardiovascular Risk in Adults
John Raymond MS, PA-C, MHP
February 7, 2015

There are no longer treatment targets for LDL or non-HDL
• This is a huge change for patients and providers.
• No longer treat to target
• Doesn’t fit in well with “know your numbers.”
• Goal is no longer “lower is better.”

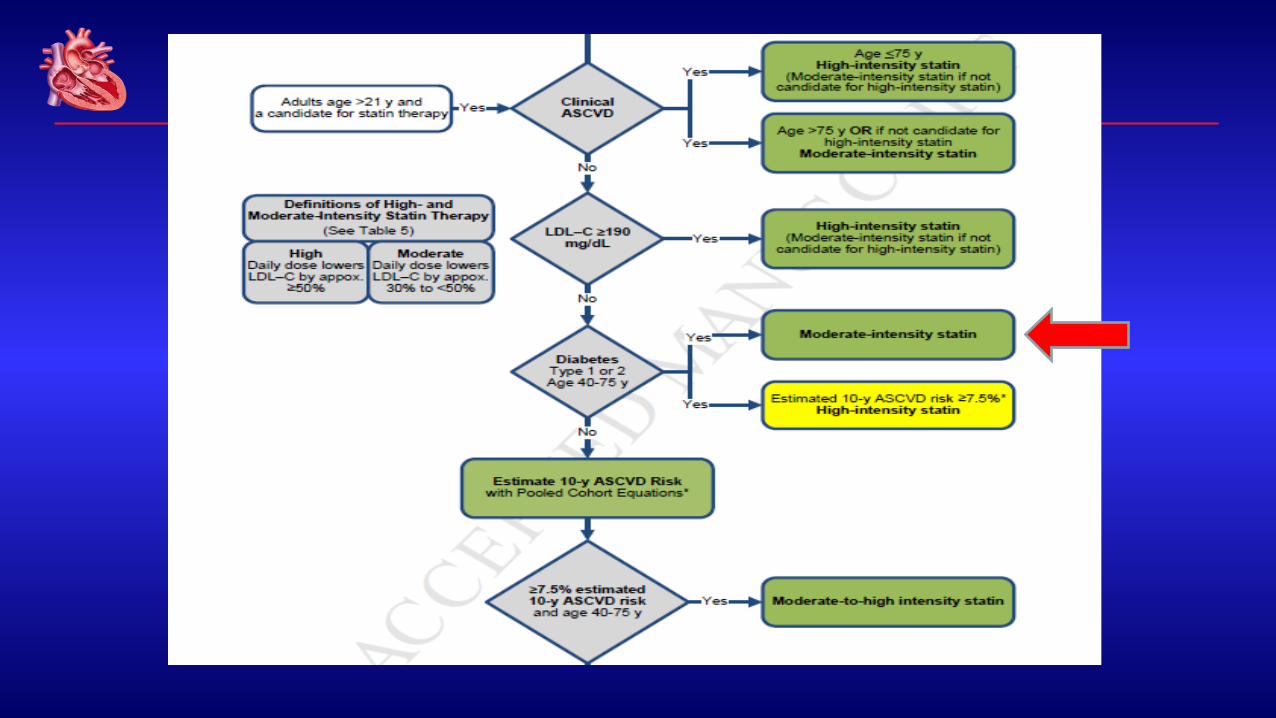
Four Major Statin Benefit Groups
1) Individuals with clinical ASCVD
2) Individuals with LDL >190
3) Individuals with dm, 40-75 yo with LDL 70-189 and without clinical ASCVD
4) Individuals without clinical ASCVD or dm with LDL 70-189 and estimated 10-year ASCVD risk >7.5%

Don’t Forget Healthy Lifestyle
• Healthy diet
• Regular exercise
• No tobacco
• Maintain healthy weight


2013 ACC/AHA/NHLBI Guideline on Lifestyle for CVD Prevention
• Eat a dietary pattern that is rich in fruit, vegetables, whole grains, fish, low-fat dairy, lean poultry, nuts, legumes, and nontropical vegetable oils consistent with a Mediterranean or DASH-type diet.
• Restrict consumption of saturated fats, trans fats, sweets, sugar-sweetened beverages, and sodium.
• Engage in aerobic physical activity of moderate to vigorous intensity lasting 40 minutes per session three to four times per week

1. Patients with clinical ASCVD
• Defined by the inclusion criteria for the secondary prevention statin RCT
• Coronary artery disease or peripheral artery disease
• Acute coronary syndromes
• Coronary or other arterial revascularization
• Stroke or TIA
• PVD presumed to be atherosclerotic

Identifying ASCVD
• This could be identified in several ways
• Heart catheterization
• Q waves on ECG
• TEE
• Coronary CTA
• Noninvasive testing including, carotid duplex, upper or lower extremity arterial duplex
• Peripheral angiography


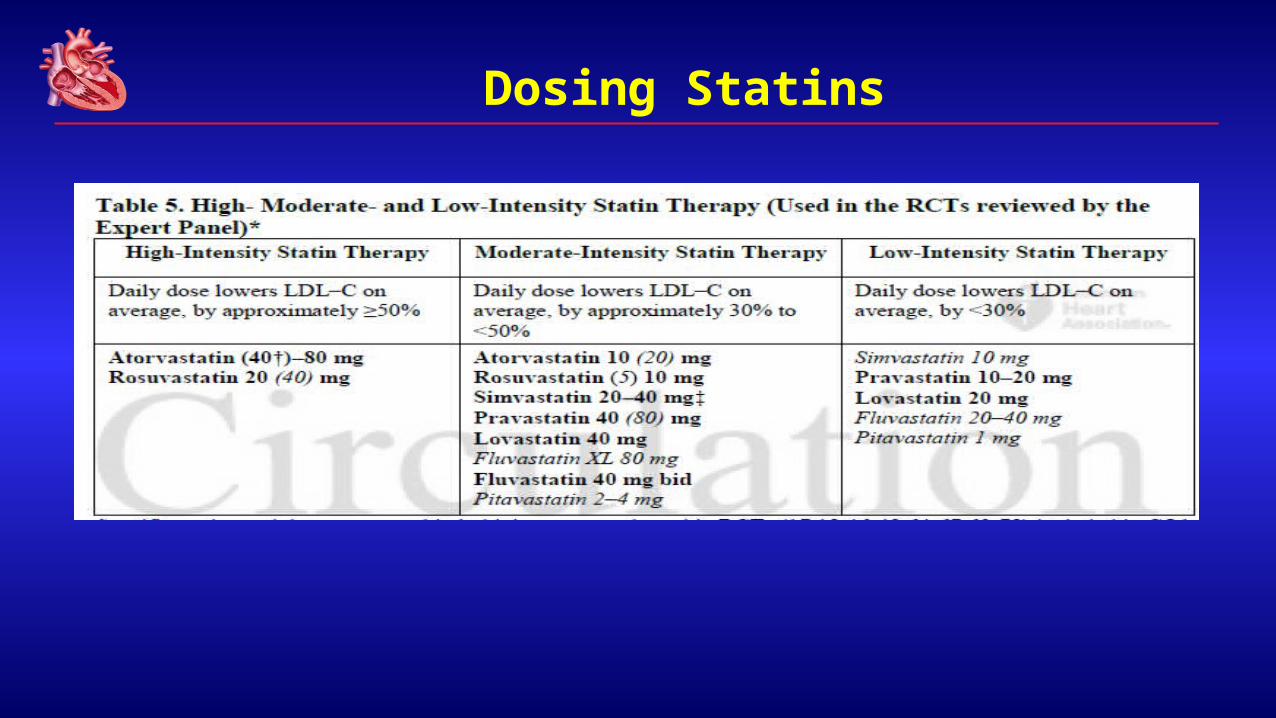
Dosing Statins

2. LDL greater than 190 mg/dl
• This is one of the few times level of cholesterol mentioned in the guidelines
• These are patients with familial hyperlipidema
• They deserve special consideration
• Often start with untreated LDL of 325-400 mg/dl


3. Patients with diabetes, age 40-75 years
• All have indication for statin
• Level of intensity of statin treatment depends on calculated 10 year risk.

http://clincalc.com/Cardiology/ASCVD/PooledCohort.aspx

Diabetics aged 40-75 yoa
• Diabetics with > 7.5% 10 year risk get high intensity statin therapy
• Diabetics with < 7.5% 10 year risk of CAD get moderate intensity statin therapy
• Statin indicated in all patients with diabetes


4. Age 40-75 years that do not meet above criteria, but have a 10 year risk of >7.5 %
• 10 year and lifetime risk as determined by CV Risk Calculator
• Specifically designed for this trial
• Downloadable on AHA or ACC site
• Not without controversy, as the calculator has never before been published or validated


Non-statin therapies
• For hyperlipidemia, non statin therapies, alone or in combination with statins, do not provide acceptable risk reduction benefits compared to adverse effects.
• These include:
– Zetia
– Fibrates
– Fish oil
– Niacin
• For the most part, these should be avoided with few exceptions

STATIN Safety recommendations
• conditions that could predispose pts to statin side effect:o Impaired renal or hepatic function
o History of previous statin intolerance or muscle disorder
o Age >75
o Unexplained ALT elevation > 3x ULN
o History of hemorrhagic stroke
o Asian ancestry

STATIN Safety recommendations
• Select the appropriate dose
• Keep potential Side effects and drug-drug interaction In mind (grade A)
• If high or moderate intensity statin not tolerated, use the maximum tolerated dose instead

What is your patient cannot tolerate statin due to muscle weakness?
• Readdress lifestyle issues
• Decrease the dose of statin
• Try another statin
• Check vitamin D levels and replace
• Evaluate for other conditions that may cause muscle weakness
Consider CoQ 10 at greater than 200 mg daily

Summary
• No longer use targets for cholesterol levels
• Identify patients at risk
• Know the 4 high risk groups
• Use medications proven to reduce risk, ie statins
• Encourage healthy lifestyle
• Understand that questions and concerns remain

Case 1
50 year old white female
•Total cholesterol 180
•HDL: 50
•SBP: 130
•taking anti-hTN meds
•+diabetic
•+smoker
•Calculated 10 yr ASCVD: 9.8%

Dosing Statins

Case 2
22 yo white male
•LDL: 195
•SBP: 120
•Not taking anti-hTN meds
•Non-diabetic
•Non-smoker


Dosing Statins

IMPIMProved roved RReduction of eduction of OOutcomes: utcomes: VVytorin ytorin EEfficacy fficacy IInternational nternational TTrialrial
A Multicenter, Double-Blind, Randomized Study to Establish the A Multicenter, Double-Blind, Randomized Study to Establish the Clinical Benefit and Safety of Vytorin (Ezetimibe/Simvastatin Tablet) vs Clinical Benefit and Safety of Vytorin (Ezetimibe/Simvastatin Tablet) vs Simvastatin Monotherapy in High-Risk Subjects Presenting Simvastatin Monotherapy in High-Risk Subjects Presenting With Acute Coronary SyndromeWith Acute Coronary Syndrome

Patients stabilized post ACS ≤ 10 days:LDL-C 50–125*mg/dL (or 50–100**mg/dL if prior lipid-lowering Rx)
Standard Medical & Interventional Therapy
Ezetimibe / Simvastatin 10 / 40 mg
Simvastatin 40 mg
Follow-up Visit Day 30, every 4 months
Duration: Minimum 2 ½-year follow-up (at least 5250 events)
Primary Endpoint: CV death, MI, hospital admission for UA,coronary revascularization (≥ 30 days after randomization), or stroke
N=18,144
Uptitrated to Simva 80 mg if LDL-C > 79(adapted per
FDA label 2011)
Study DesignStudy Design
*3.2mM **2.6mM
Cannon CP AHJ 2008;156:826-32; Califf RM NEJM 2009;361:712-7; Blazing MA AHJ 2014;168:205-12
90% power to detect ~9% difference

LDL-C and Lipid ChangesLDL-C and Lipid Changes1 Yr Mean LDL-C TC TG HDL hsCRP
Simva 69.9 145.1 137.1 48.1 3.8
EZ/Simva 53.2 125.8 120.4 48.7 3.3
Δ in mg/dL -16.7 -19.3 -16.7 +0.6 -0.5
Median Time avg69.5 vs. 53.7 mg/dL

Primary Endpoint — ITTPrimary Endpoint — ITT
Simva — 34.7% 2742 events
EZ/Simva — 32.7% 2572 events
HR 0.936 CI (0.887, 0.988)
p=0.016
Cardiovascular death, MI, documented unstable angina requiring rehospitalization, coronary revascularization (≥30 days), or stroke
7-year event rates
NNT= 50

Simva† EZ/Simva†
Male 34.9 33.3Female 34.0 31.0 Age < 65 years 30.8 29.9Age ≥ 65 years 39.9 36.4
No diabetes 30.8 30.2Diabetes 45.5 40.0
Prior LLT 43.4 40.7No prior LLT 30.0 28.6
LDL-C > 95 mg/dl 31.2 29.6LDL-C ≤ 95 mg/dl 38.4 36.0
Major Pre-specified Major Pre-specified SubgroupsSubgroups
Ezetimibe/Simva Better
Simva Better
0.7 1.0 1.3†7-year
event rates
*
*p-interaction = 0.023, otherwise > 0.05
ConclusionsConclusions
IMPROVE-IT:IMPROVE-IT: First trial demonstrating incremental clinical benefit when First trial demonstrating incremental clinical benefit when adding a non-statin agent (ezetimibe) to statin therapy: adding a non-statin agent (ezetimibe) to statin therapy:
YES:YES: Non-statinNon-statin lowering LDL-C with ezetimibelowering LDL-C with ezetimibereduces cardiovascular eventsreduces cardiovascular events
YES:YES: Even Lower is Even BetterEven Lower is Even Better(achieved mean LDL-C 53 vs. 70 mg/dL at 1 year)(achieved mean LDL-C 53 vs. 70 mg/dL at 1 year)
YES:YES: Confirms ezetimibe safety profileConfirms ezetimibe safety profile
Reaffirms the LDL hypothesis, Reaffirms the LDL hypothesis, that reducing that reducing LDL-C prevents cardiovascular eventsLDL-C prevents cardiovascular events
Results could be considered for future guidelinesResults could be considered for future guidelines
Hypertension

2014 Guidelines for Management of High Blood Pressure in Adults (JNC 8)
John Raymond MS, PA-C, MHPFebruary 7, 2015

Hypertension
Hypertension is the most common condition in primary care.
1 in 3 patients have hypertension according to NHLBI
Risk factor for MI, CVA, ARF, death
What is the goal BP?
Joint National Committee (JNC)Panel appointed by the National Heart,
Lung, and Blood Institute (NHLBI)First guidelines (JNC-1) published in
1977Subsequent updates published in 3- to 6-
year intervalsLast edition (JNC-7) published in 2003
Chobanian AV et al. JAMA 2003;289:2560-72.

Development of JNC-8
And then we wait…and wait…

JNC 8
2014 Evidence-Based Guidelines for the Management of High Blood Pressure in AdultsJAMA. 2014;311(5):507-520December 18, 2013

JNC 8: Hypertension ManagementQuestions Guiding Review
In adults with HTN:
1. Does initiating antihypertensive pharmacologic therapy at specific BP thresholds improve health outcomes?
2. Does treatment with antihypertensive pharmacologic therapy to a specified goal lead to improvements in health outcomes?
3. Do various antihypertensive drugs or drug classes differ in comparative benefits and harms on specific health outcomes?

BP goal in the elderly

Hypertension in the ElderlyFastest growing segment of the populationPrevalence of hypertension is very highSeveral issues make managing HTN unique:
Often present with isolated systolic HTNMore likely to present with comorbiditiesMany clinical trials in HTN have excluded these patients (particularly
for those 80 years and older)Elderly are more susceptible to certain adverse effects (orthostatic
hypotension)

JNC-8 RecommendationsIn patients >60 years of age, start medications at blood
pressure of >150/90mm Hg and treat to goal of <150/90mm Hg
In patients >60 years of age, treatment does not need to be adjusted if achieved blood pressure is lower than goal and well-tolerated
James PA et al. JAMA 2014;311:507-20.
JNC-8 RecommendationsIn patients <60 years of age, start medications at blood
pressure of >140/90mm Hg and treat to goal of <140/90mm Hg
In all adult patients with diabetes or chronic kidney disease, start medications at blood pressure of >140/90mm Hg and treat to goal of <140/90mm Hg
James PA et al. JAMA 2014;311:507-20.

JNC-8 RecommendationsFor the non-black population (including diabetes), initial
antihypertensive treatment may include a thiazide, ACEI, ARB, or CCB
For the black population (including diabetes), initial antihypertensive treatment should include a thiazide or CCB
For all patients with CKD, initial (or add-on) therapy for hypertension should include an ACEI or ARB
James PA et al. JAMA 2014;311:507-20.
JNC8: Treatment Strategies If goal BP not met after 1 month of treatment:
Increase dose of initial drug, orAdd a second drug (Thiazide, CCB, ACEi, or ARB)
If goal BP not met with 2 medications:Add and titrate a third medication (Thiazide, CCB, ACEi, or
ARB)Do not use ACE and ARB together
Other classes may be used in the following scenarios:Goal BP not met with 3 medicationsContraindication to thiazide, ACE/ARB, or CCB


Case 1
62 year old AA male
•Total cholesterol: 140
•Low HDL: 35
•SBP: 130 mmHg
•Not taking anti-hypertensive medications
•Non-diabetic
•Non-smoker
•Calculated 10 yr risk of ASCVD : 9.1%


Dosing Statins
Case 3
48 yo white female
•Total cholesterol 180
•HDL: 55
•SBP: 130
•Not taking anti-hTN meds
•+diabetic
•Non-smoker
•Calculated 10 yr risk ASCVD : 1.8%

Dosing Statins
Case 5
66 yo white female
•High Total cholesterol: 230
•HDL: 55
•SBP: 150
•taking anti-hTN meds
•Non-diabetic
•Non-smoker
•Calculated 10 yr risk of ASCVD : 2.0 %


Strategies to Dose Antihypertensive Drugs
Titrate to max dose, then add a second drugAdd a second drug before achieving max
dose of the initial drugStart with 2 drugs at the same time
If SBP ≥ 160mmHg and/or DBP ≥ 100 mmHg
If SBP ≥ 20mmHg above goal and/or DBP ≥ 10mmHg above goal.

Simva — 22.2% 1704 events
EZ/Simva — 20.4% 1544 events
HR 0.90 CI (0.84, 0.97)
p=0.003
NNT= 56
CV Death, Non-fatal MI, CV Death, Non-fatal MI, or Non-fatal Strokeor Non-fatal Stroke
7-year event rates
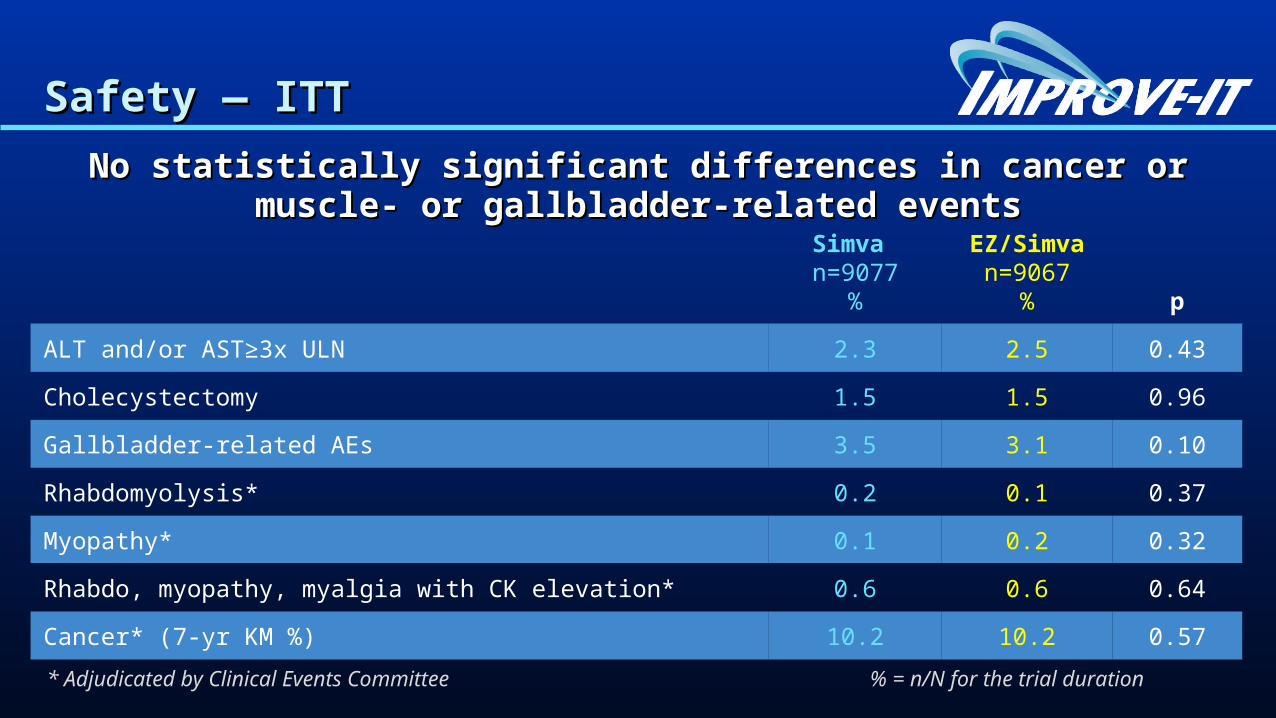
Safety — ITTSafety — ITT
No statistically significant differences in cancer or muscle- or No statistically significant differences in cancer or muscle- or gallbladder-related eventsgallbladder-related events
Simva n=9077
%
EZ/Simvan=9067
% p
ALT and/or AST≥3x ULN 2.3 2.5 0.43
Cholecystectomy 1.5 1.5 0.96
Gallbladder-related AEs 3.5 3.1 0.10
Rhabdomyolysis* 0.2 0.1 0.37
Myopathy* 0.1 0.2 0.32
Rhabdo, myopathy, myalgia with CK elevation* 0.6 0.6 0.64
Cancer* (7-yr KM %) 10.2 10.2 0.57
* Adjudicated by Clinical Events Committee % = n/N for the trial duration

Baseline CharacteristicsBaseline Characteristics
Simvastatin(N=9077)
%
EZ/Simva(N=9067)
%
Age (years) 64 64
Female 24 25
Diabetes 27 27
MI prior to index ACS 21 21
STEMI / NSTEMI / UA 29 / 47 / 24 29 / 47 / 24
Days post ACS to rand (IQR) 5 (3, 8) 5 (3, 8)
Cath / PCI for ACS event 88 / 70 88 / 70
Prior lipid Rx 35 36
LDL-C at ACS event (mg/dL, IQR) 95 (79, 110) 95 (79,110)


Overview
• NHLBI• ACC/AHA• First new guidelines since ATP III guideline update in 2004• Review the most important statements or changes presented in these guidelines
– No longer have therapeutic targets– New risk calculator– Use medications proven to reduce risk, ie statins– Avoid medications or supplements that may lower the cholesterol number, but have no data to
decrease CV risk• This guideline focuses on treatments to reduce ASCVD events• Not a comprehensive approach to lipid management• Finally, review questions and controversies that have arisen since publication.