new hcv treatments any access to resource limited...
TRANSCRIPT

New HCV treatmentsAny access to resource‐limited countries ?
Maud LemoineMRC, The Gambia Unit, West Africa
10 REASONS TO OPEN ACCESS TO NEW HEP‐C TREATMENT IN RLC
A SPECIAL LOOK AT AFRICA
1‐ HCV infection is a public health issue in RLC
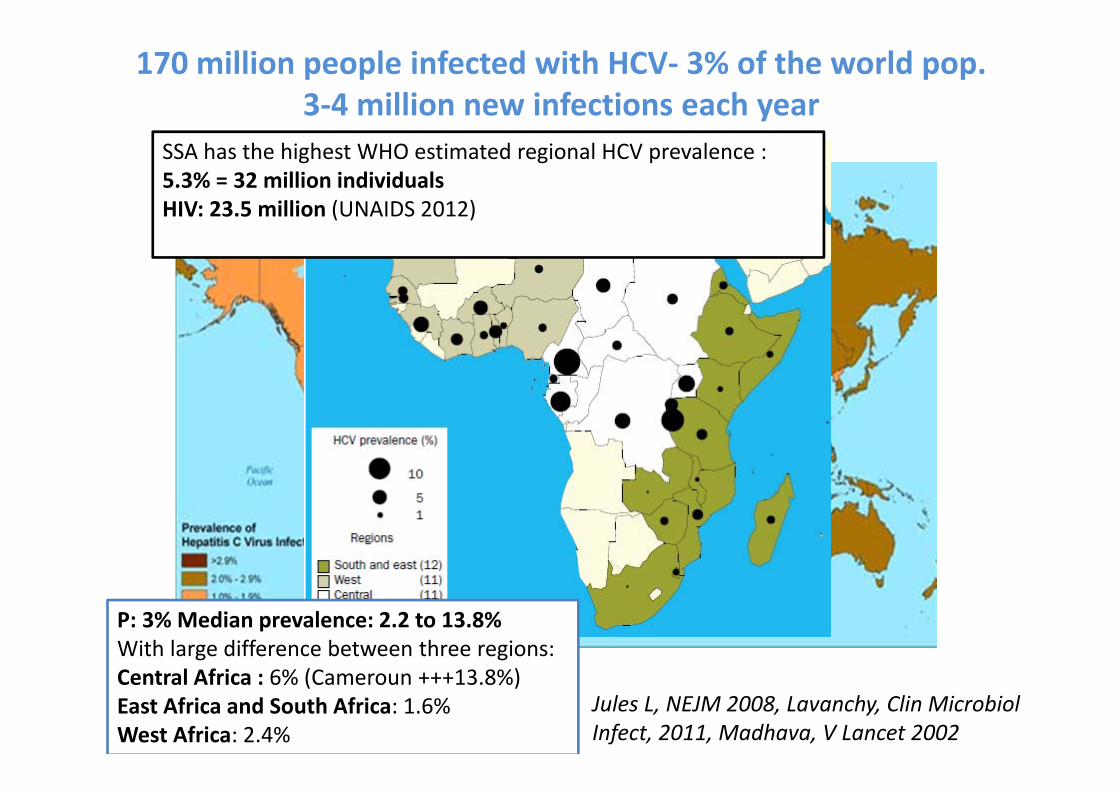
Jules L, NEJM 2008, Lavanchy, Clin MicrobiolInfect, 2011, Madhava, V Lancet 2002
SSA has the highest WHO estimated regional HCV prevalence : 5.3% = 32 million individualsHIV: 23.5 million (UNAIDS 2012)
P: 3% Median prevalence: 2.2 to 13.8%With large difference between three regions:Central Africa : 6% (Cameroun +++13.8%)East Africa and South Africa: 1.6%West Africa: 2.4%
170 million people infected with HCV‐ 3% of the world pop.3‐4 million new infections each year
HCV is a leading cause of deaths worldwide
• 350,000 annual deaths • 30% of cirrhosis• 20% of Hepatocellular carcinoma 5th cancer worldwide
Lavanchy, Liver Int, 2009Globocan, 2008Salmon‐Ceron D, 2009Gellad, ZF AVT 2012
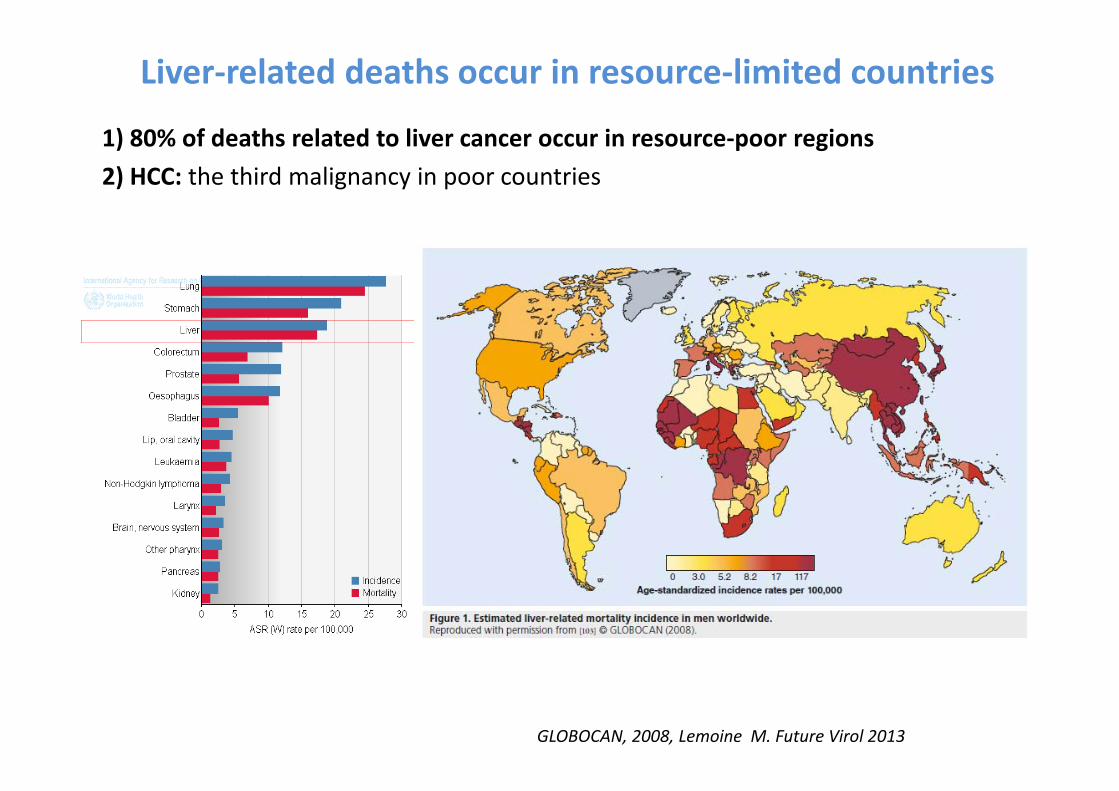
1) 80% of deaths related to liver cancer occur in resource‐poor regions2) HCC: the third malignancy in poor countries
Liver‐related deaths occur in resource‐limited countries
GLOBOCAN, 2008, Lemoine M. Future Virol 2013

In Africa, HCC is a major killer
Jemal A, WHO/IARC, Cancer 2012
HCV: 20-50% of the cases according to the HCV local endemicityKirk GD, Hepatology 2004, Perz JF, J Hepatol 2006

Data on HIV‐HCV co‐infection are lacking and conflicting
• Cameroun: HCV‐HIV prevalence: 12.4% (n=169 HIV Pos)
Laurent C, HIV Med, 2010
• Nigeria, Jos University Teaching Hospital:n=19 408 HIV Pos (2014‐2010) HCV‐HIV prevalence: 11.3%
Ladep N, W J Gastro 2013
• Ghana: 3.6% (n=138 HIV subjects)Sagoe, KW J Med Virol 2012
• Senegal: 1.6% (95%[0.6‐3.5])Diop‐Ndiaye H, J Med Virol 2008

Liver disease has become a major cause of death in HIV patients
The D.A.D study group, AIDS. 2010 Jun 19;24(10):1537‐48.
11.5% hepatitis related
Resource‐limited countries will facethe same burden of liver‐related morbi‐mortality !
UNDETECTABLE FOR HCV
AS WELL ???
Only 5% of the 170 million HCV-infected people are aware of their infection
Thomas DL, Lancet 2010;376:1441‐1442Thomas DL, AVT 2012

Risk factors of HCV infection in Africa
Kandeel AM, BMC Infect Dis, 2012

Is injecting drug abuse an issue in SSA ?
Estimation of IDU number per countries‐UNODC 2008, RaguinG, Girard PM Trop Med Int Health 2009
0.5 to 3 million IDU
Dakar and urban areasn=1324 IDUSHIV: 5.2%HCV : 23.3% Ba I et al. 2011Tine J et al. Poster 20,interest 2013
NairobiHCV:22.2% in IDU(n=314)
Muasya,T . East Afr Med J 2008

10 REASONS TO OPEN ACCESS TO NEW HEP‐C TREATMENT IN RLC
A SPECIAL LOOK AT AFRICA
2‐ New innovative diagnostic tools adapted to the resource‐poor settings

Innovative diagnostic tools
Rapid Testing‐ Point‐of‐care tests‐ Salivary rapid testing
Yaari,A J Viral Methods 2006
Easier assessment of the infection and the liver disease‐ Dry‐blood spots (HCV viral load quantification/genotyping)
Tuaillon E Hepatology 2010
‐ Portative Fibroscan (Echosens)‐ Portative sonography

10 REASONS TO OPEN ACCESS TO NEW HEP‐C TREATMENT IN RLC
A SPECIAL LOOK AT AFRICA
3‐ HCV infection is a CURABLE disease

Treatment has been significantly improved% of p
atients w
ith su
staine
d virological respo
nse (SVR
)
IFN
24 W
70
50
30
20
10
60
40
IFN
48 W
IFN+RBV
24 W
IFN+RBV
48 W
PEG‐IFN+RBV
48 W
0
80
90
IFN = Interferon‐αPEG‐INF = Peg‐Interferon‐αRBV = RibavirinW = weeksPEG = PEG‐IFN‐α
PEG‐IFN+RBV+new IP
TelaprevirOr Boceprevir
INF‐free regimens12 weeks
? 95‐100% SVR
2002
2011
1999
2014

0
10
20
30
40
50
60
70
80
90
Naive Prior relapsers Prior partialresponders
Prior nullresponders
Peg‐RibaPeg‐Riba + TelaprevirPeg‐Riba + Boceprev
SVR has been significanly improved with the first generation of Direct Antiviral Agents (DAA)
SVR(%)
+30%
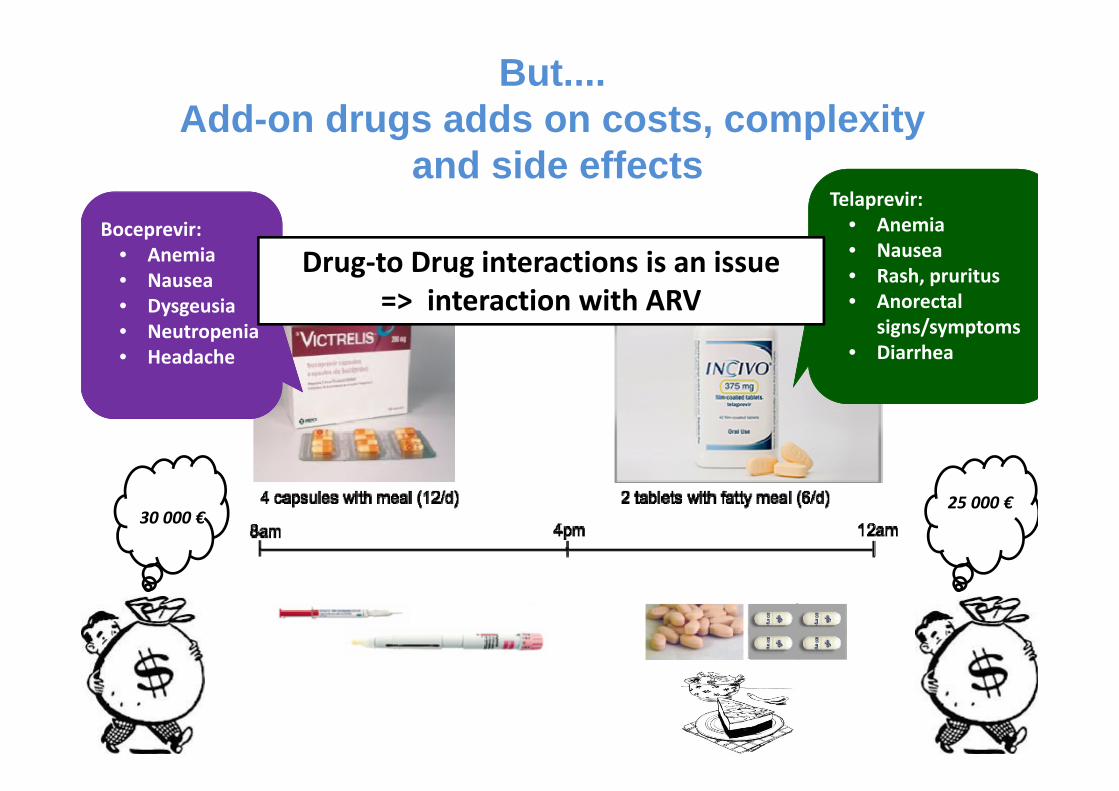
But....Add-on drugs adds on costs, complexity
and side effects Boceprevir:
• Anemia• Nausea• Dysgeusia• Neutropenia• Headache
Telaprevir:• Anemia• Nausea• Rash, pruritus• Anorectal
signs/symptoms• Diarrhea
30 000 €25 000 €
Drug‐to Drug interactions is an issue=> interaction with ARV
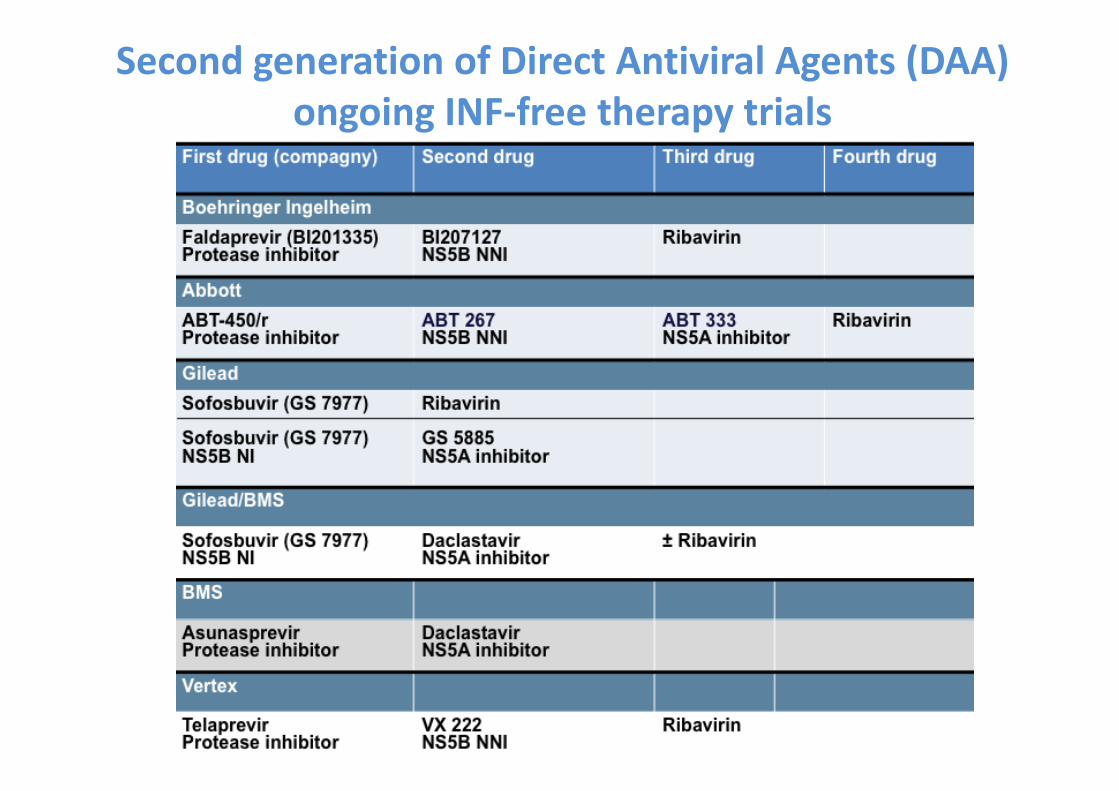
Second generation of Direct Antiviral Agents (DAA)ongoing INF‐free therapy trials

INF‐free regimens Naive Genotype 1 patients
1. Sulkowski M, et al. AASLD 2012. Abstract LB‐2. 2. Gane E, et al. AASLD 2012. Abstract 229.3. Kowdley KV, et al. AASLD 2012. Abstract LB‐1. 4. Everson G, et al. AASLD 2012. Abstract LB‐3.
Sofosbuvir (Nuc) + daclatasvir(NS5A) + RBV x 24 wks
100
80
60
40
20
0
SVR4
, 12, or 2
4 (%
)
n/N =
100[1]
15/15
2‐3 DAAs + RBV
Sofosbuvir (Nuc) + daclatasvir (NS5A) x 24 wks
Daclatasvir (NS5A) + asunaprevir (PI) +BMS 791325 (NNI) x 12 wks
2‐3 DAAs, No RBV28/29
97[1] 94[4]
15/16
98[3]
77/79
ABT‐450/r (PI) + ABT‐333 (NNI)+ ABT‐267 (NS5A) + RBV x 12 wks
25/25
100[2]
Sofosbuvir (Nuc) + GS‐5885 (NS5A) + RBV x 12 wks
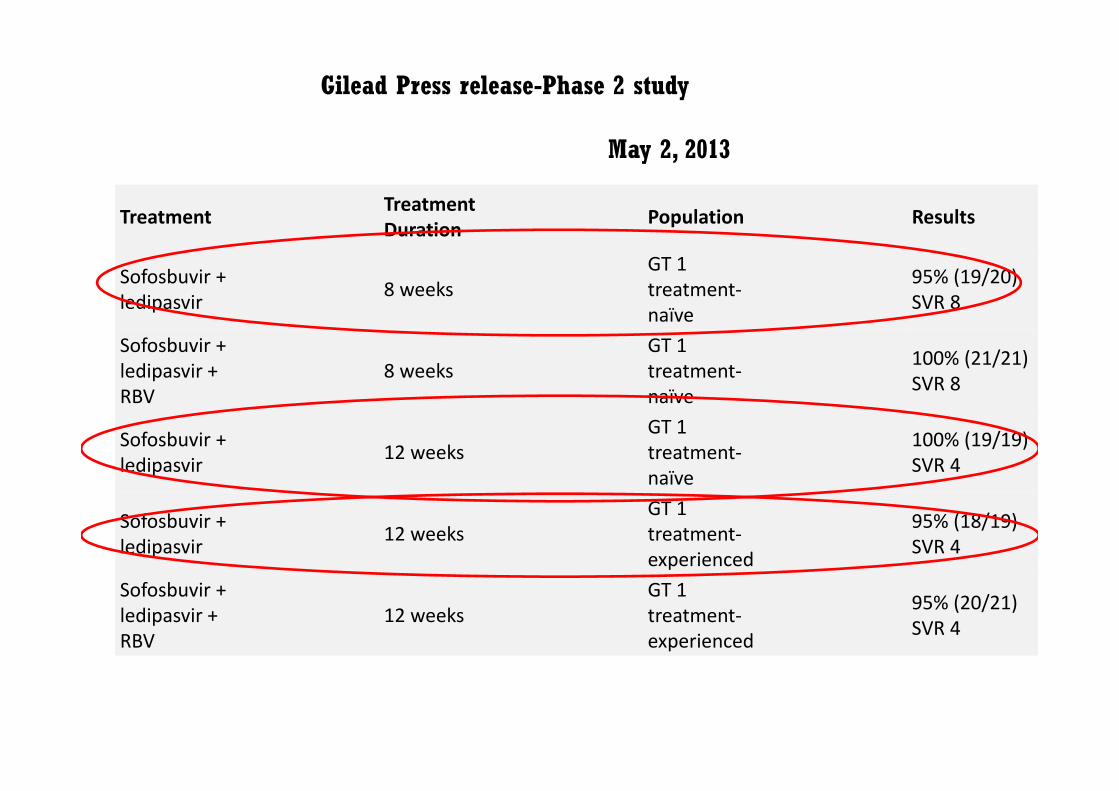
Treatment TreatmentDuration Population Results
Sofosbuvir + ledipasvir 8 weeks
GT 1 treatment‐naïve
95% (19/20) SVR 8
Sofosbuvir + ledipasvir + RBV
8 weeks GT 1 treatment‐naïve
100% (21/21) SVR 8
Sofosbuvir + ledipasvir 12 weeks
GT 1 treatment‐naïve
100% (19/19) SVR 4
Sofosbuvir + ledipasvir 12 weeks
GT 1 treatment‐experienced
95% (18/19) SVR 4
Sofosbuvir + ledipasvir + RBV
12 weeks GT 1 treatment‐experienced
95% (20/21) SVR 4
Gilead Press release-Phase 2 study
May 2, 2013
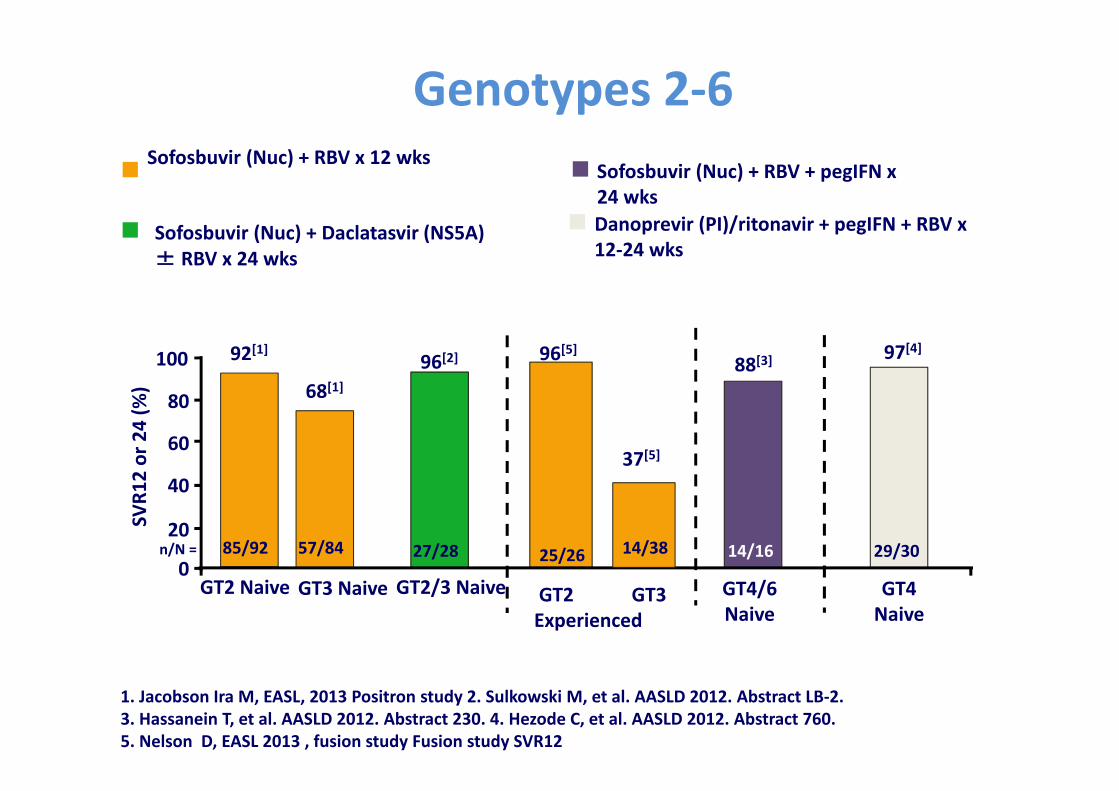
Sofosbuvir (Nuc) + RBV x 12 wks
Sofosbuvir (Nuc) + Daclatasvir (NS5A) ± RBV x 24 wks
Danoprevir (PI)/ritonavir + pegIFN + RBV x 12‐24 wks
100
80
60
40
20
0
SVR1
2 or 24 (%
)
n/N = 25/26
GT2 GT3Experienced
92[1]
85/92
GT2 Naive
96[2]
27/28
88[3]
14/16
GT4/6Naive
GT4Naive
97[4]
29/30
1. Jacobson Ira M, EASL, 2013 Positron study 2. Sulkowski M, et al. AASLD 2012. Abstract LB‐2. 3. Hassanein T, et al. AASLD 2012. Abstract 230. 4. Hezode C, et al. AASLD 2012. Abstract 760.5. Nelson D, EASL 2013 , fusion study Fusion study SVR12
Sofosbuvir (Nuc) + RBV + pegIFN x 24 wks
Genotypes 2‐6
96[5]
37[5]
14/38
68[1]
57/84
GT3 Naive GT2/3 Naive

Interferon therapy is not adapted to the African setting
1) INJECTABLE
2) REQUIRING COLD STORAGE (2° to 8°C)
3) SIDE‐EFFECTS FatigueFlu‐like syndromepsychiatric effects NeutropeniathrombopeniaAnemia
4) AFRICAN HCV‐infected SUBJECTS:Genotype 1 and 4,non‐C/C IL28B
=> LOWER RESPONSE to Peg‐INF‐ RBV therapy
Interferon‐free regimensalso affordable to resource‐limited countries
10 REASONS TO OPEN ACCESS TO NEW HEP‐C TREATMENT IN RLC
A SPECIAL LOOK AT AFRICA
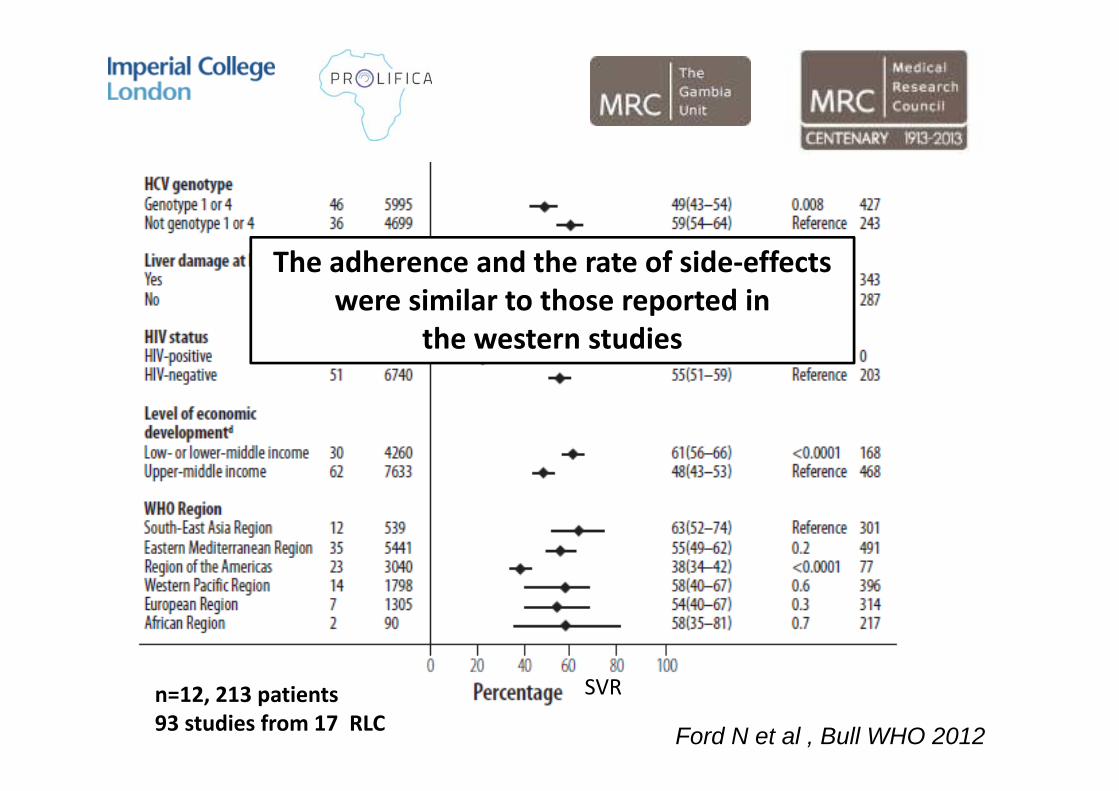
4‐ Hep.C treatment is feasible in RLC
Ford N et al , Bull WHO 2012
n=12, 213 patients93 studies from 17 RLC
SVR
The adherence and the rate of side‐effectswere similar to those reported in
the western studies
10 REASONS TO OPEN ACCESS TO NEW HEP‐C TREATMENT IN RLC
A SPECIAL LOOK AT AFRICA
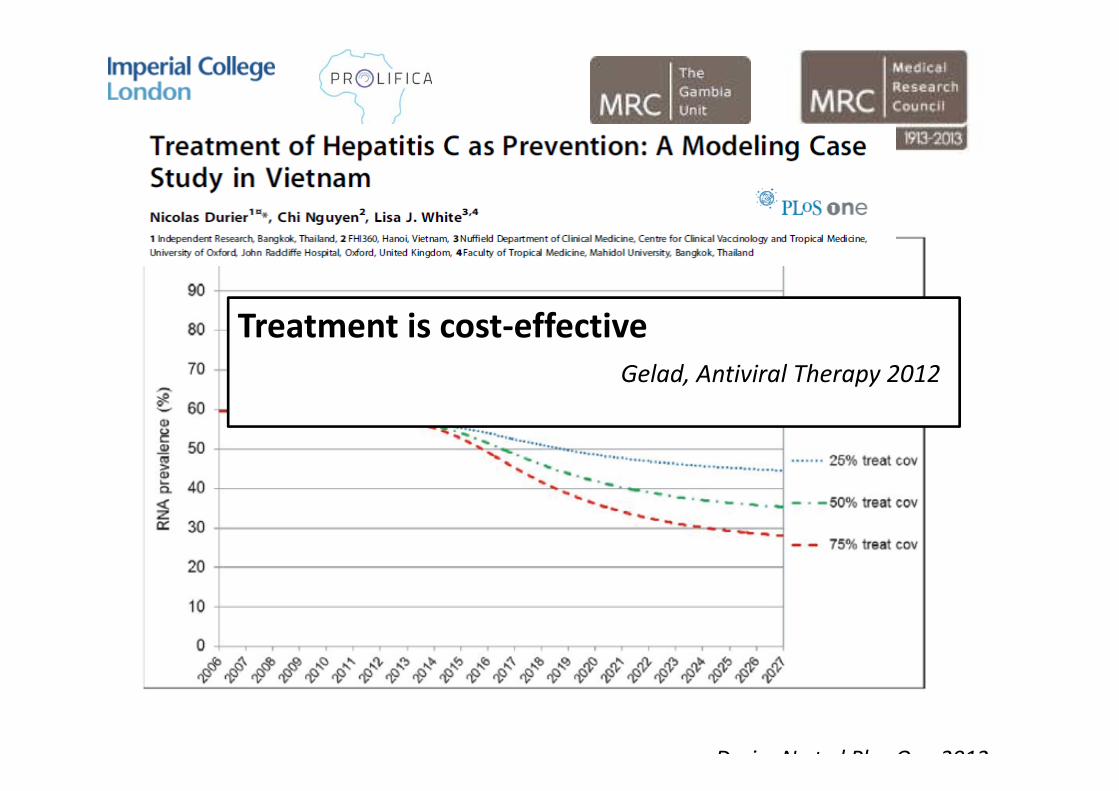
5‐ In the absence of vaccine, treatmentis preventive
Durier N et al Plos One 2012
Treatment is cost‐effectiveGelad, Antiviral Therapy 2012

10 REASONS TO OPEN ACCESS TO NEW HEP‐C TREATMENT IN RLC
A SPECIAL LOOK AT AFRICA
6‐ A recent political will


10 REASONS TO OPEN ACCESS TO NEW HEP‐C TREATMENT IN RLC
7‐ A duty to treat

1‐ Access to Health is a Fundamental Human RightUniversal Human Right Declaration and WHO constitution, 1948
2‐ States and Supranational institutions Moral Obligation to ensure access to health for all
3‐Medical and scientific knowledge= common good accessible for all
4‐ United Nations Millenium Development Goals (2000)« ….to provide access to affordable medicines in developing countries in cooperation with pharmaceutical companies”
• Since 1995, the Trade‐Related Aspects of Intellectual Property Rights
(TRIPS) agreements (World Trade Organisation)
20‐years patent protection to pharmaceutical products
Incentives needed for Research and Development ?
90% of investments for R&D concern 10% of the richest world’s
population
Hoen et JAIDS 2011, Lemoine M, Future Virol 2013
Yet…..
“There is no evidence that the implementation
of the TRIPS agreements in developing countries
will boost research on diseases affecting these
countries”
Commission on Intellectual Property Rights, WHO, 2006

10 REASONS TO OPEN ACCESS TO NEW HEP‐C TREATMENT IN RLC
8‐We must and we can challenge the drug market
The Doha Declaration (2001)the TRIPS Agreements “can and should beimplemented in a manner (...) to protect public healthand to promote access to medicines for all”.
Each country has the right to declare any disease asa urgent public health issue
=> And to generate „compulsory licences“ to makepatented drugs available at affordable prices in the"public health interest."
The example of India
From 4,000 euros to 150 euros/month

The Egyptian experience
• Reiferon Retard®(MINAPHARM company)Biosimilar of PegINF
• Price has been negociated and divided by 15 over the last years
0
10000
20000
30000
40000
50000
60000
70000
2008 2009 2010 2011
1500
3000
Cost of treatment (€)N of patients treated/y

http://www.medicinespatentpool.org

India and China80 % of the worldwide medicine production
Lula da Silva set up the first ARVfactory in AfricaMaputo, Nov. 2010
Factory launched in July 2012

10 REASONS TO OPEN ACCESS TO NEW HEP‐C TREATMENT IN RLC
9‐ Lessons from HIV/AIDS experience

1) COST:• In 2000: ART: $10,000‐15,000/patient/year• Today < $100/year
In 2000, only 0.1% received ARV in Africa Today, almost 50%
2) COMPLEX and POLITICALLY DISREGARDED
• “Many people in Africa have never seen a clock or a watch their entire lives. If you say one pm in the afternoon, they do not know what you are talking about“.
Andrew Natsios, former USAID director, 2000
• Until 2002, WHO did not to consider ARV as essential medicines
L‘ histoire se répète ....

10 REASONS TO OPEN ACCESS TO NEW HEP‐C TREATMENT IN RLC
10‐ Respond to the civil society
4‐5 million HIV‐HCV infected peopleMostly living in RLC
International conference on HIV/AIDS, Washington 2012
CONCLUSION
• Hepatitis C in RLC is a neglected public health issue• Screening and access to treatment are critical• High time to implement programs and guidelines on Hep.C adapted to the local poor settings
• The new era of new DAA is a PERFECT opportunity to improve the burden of Hep.C and HCC in RLC

Time for action We should not let DAA being
Discriminating Access to Antivirals
AckowledgmentsFrance Isabelle CheminPierre‐Marie GirardKarine LacombeMaimuna MendyGilles RaguinChristopher WildFabien Zoulim
UK (Imperial College London) Mark ThurszSimon Taylor‐RobinsonHelen HolmesDebbie GarsideGraham CookMary CrosseyShevanthi NayagamTorben Kimhofer
The GambiaRamou NjieHarr NjaiGibril NdowYusuke ShimakawaSaydiba TambaMavis Foster‐NyakoAbdullah JattaUmberto D‘allessandroTumani CorrahMakie TaalMustapha KhalilOusman Nyan
SenegalMourtalla KaSouleyman MboupCoumba Toure‐KaneAmina Sow
NigeriaNimzing LadepMarie DuguruYakubu FiyaktuVirginia SaleSolomon BanwatEdwin Adoga
Ivory CoastSerge Eholie