newsletter 02 2015
DESCRIPTION
IPPC newsletterTRANSCRIPT

1
DCH / IPPC Monthly Newsletter
Newsletter # 2, 2015
Dear DCH / IPPC Participants, Tutors and Alumni,
It is a great pleasure to welcome our new Participants for 2015
as you begin a journey of enhancing your knowledge,
confidence and skills in caring for children and young people.
Our recent Graduates have reported benefits in their day-to-
day practice as new knowledge from DCH / IPPC is assimilated
into action. I liked the description of new knowledge becoming
a clearer lens through which to view each patient.
Please let us know your feedback throughout the year: this is key to our continuing
refinement of our program. We welcome online feedback, phone, email and appreciate
the time you take in contributing this to benefit others.
We want you to gain the most from your year of immersion in paediatric best practice
from our experts here at the Sydney Children’s Hospitals Network, which is augmented for our international
Participants through your local expert Tutors. To do this I need to emphasise the importance of:
Reading your Participant Handbook (please insert hyperlink) to help you with:
o An overview of the program
o Additional resources: free online journals; factsheets; reference texts
Viewing every webcast: our presenters share pearls of wisdom from years of experience throughout each
webcasts; the accompanying notes are intended as a useful summary for you to add to.
Monthly Newsletters provide an opportunity to refine your clinical reasoning skills as well as building on
webcast content.
In 2015, we are beginning the recording of additional webcasts with a focus on enhancing our international content.
These will include: Severe Acute Malnutrition, Malaria, Dengue, Parasitic Diseases, Typhoid and HIV.
We are also commencing a pilot series of webinars to provide interactive sessions for our Australian Participants. Our
international Participants will continue to benefit from ongoing interaction with their in-country Tutors and will be able
to access these recorded webinars in addition to their Tutorials. Dates are listed in this Newsletter on page 8; topics
will include cases covering: emergency, neonatology, adolescent medicine and general paediatrics. Further details will
follow.
Thanks to all of our Webcast Presenters, our Tutors and our Team for their great support again in 2015.
Your comments and recommendations are always most welcome. I look forward to hearing from you and to meeting,
wherever possible, throughout this year.
Kind regards,
Adjunct Associate Professor Kathryn Currow
Discipline of Paediatrics and Child Health, University of Sydney Executive Principal, DCH/IPPC, Senior CMO Emergency Department, Sydney Children’s Hospitals Network (SCHN), Executive President, COMHAD
In this Issue
Principal’s Letter
Dates for Diaries
Question to Lecturer
Newsletter Case
Image and a Diagnosis
Key Dates and Notices
eADVICE Pilot Study
Who are we?
Belinda Shepherd
2
Key Dates for Diaries
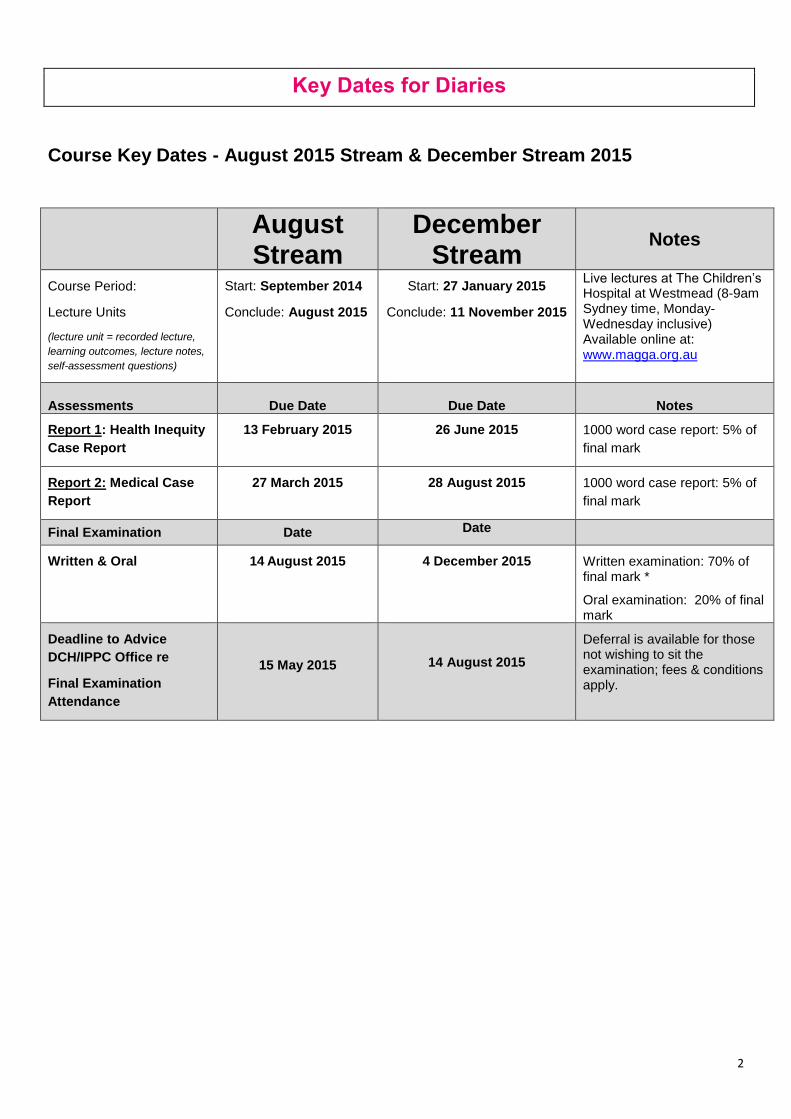
Course Key Dates - August 2015 Stream & December Stream 2015
August Stream
December Stream
Notes
Course Period:
Lecture Units
(lecture unit = recorded lecture,
learning outcomes, lecture notes,
self-assessment questions)
Start: September 2014
Conclude: August 2015
Start: 27 January 2015
Conclude: 11 November 2015
Live lectures at The Children’s Hospital at Westmead (8-9am Sydney time, Monday-Wednesday inclusive) Available online at: www.magga.org.au
Assessments
Due Date
Due Date
Notes
Report 1: Health Inequity
Case Report
13 February 2015 26 June 2015 1000 word case report: 5% of
final mark
Report 2: Medical Case
Report
27 March 2015 28 August 2015 1000 word case report: 5% of
final mark
Final Examination Date Date
Written & Oral 14 August 2015 4 December 2015 Written examination: 70% of
final mark *
Oral examination: 20% of final mark
Deadline to Advice
DCH/IPPC Office re
Final Examination
Attendance
15 May 2015
14 August 2015
Deferral is available for those not wishing to sit the examination; fees & conditions apply.

3
Question to Lecturer
Bone and Joint Infections
Question from participant:
“I had a question regarding investigation - if I was a GP in the community, RMO working in ED etc, who had a child
with hx bone pain (Eg for 7 days) and point tenderness, with no other cause identified and I wanted to look for
osteomyelitis- given that XR changes may not be useful for the first 10 days, would it be reasonable to initially send for
bloods- if raised WCC and inflammatory markers go straight to a bone scan? or do you do an XR first anyway?”
Dr Paul Gibbons:
I would do an X ray first as I would wish to exclude other causes such as fracture or bone tumour. If the XR was
normal and inflammatory markers were raised and the clinical pictures fit with osteomyelitis I would treat with
antibiotics. If the picture did not fit then I would do a bone scan
Newsletter Case
Case Presentation
CB is a 2 year old boy who presented to the emergency department of a small metropolitan hospital with a reduced
level of consciousness after a period of being unwell. His parents were worried that he was not responding and that
he had nothing to eat or drink for the last 8 hours.
What questions on history will help?
General health prior to presentation
Immunisations
Recent history of travel
History of fever
History of persistent vomiting, diarrhoea
Urine output
History of head injury or other trauma
History of medication or other toxic ingestions
Any background illness: eg: diabetes, metabolic disease, hypertension; liver disease
CB has been unwell for the last 3 days with fever and mouth ulcers. He was lethargic and slept on the couch all of the
previous day. He started becoming unresponsive in the last 8 hours. He is otherwise a healthy boy with no known
illnesses. His immunisations are up to date. There is no recent history of travel. There is no history of witnessed
head injury or drug ingestions.
What examination would you do?
Airway: patency, any signs of obstructed breathing?
Breathing: effort and efficacy of breathing (including checking O2 saturations), respiratory rate
Circulation: pulse rate and volume, capillary return, blood pressure, heart sounds, signs of cardiac failure.
Level of consciousness: AVPU scale initially (is he Alert, responsive to Voice, responsive to Pain, or Unresponsive), modified Glasgow Coma Scale when time permits.
Pupillary size and response to light
Other vital signs: temperature; bedside blood glucose level
General examination for rashes, trauma, deformity, posturing
Systemic examinations: Respiratory, cardiovascular, neurological, abdominal, ENT

4
What are the differential diagnoses and what investigations would be helpful?
Differential Diagnoses:
Severe sepsis
Viral encephalitis: HSV, EBV, enteroviruses, Japanese encephalitis, TB
Bacterial meningitis
Increased intracranial pressure (intracerebral haemorrhage, ischemic stroke, hydrocephalus, brain tumour)
Encephalopathy; hypertensive, metabolic (OTC deficiency, urea cycle defects, poisoning)
Status epilepticus
Metabolic disturbance eg hypoglycaemia
Cerebral malaria
Investigations:
Venous blood gas
Full blood count and blood film ?
Serum electrolytes, urea, creatinine
Liver function tests
Blood ammonia and lactate
Blood culture
Urine culture and urinalysis
Urine toxicology screen
CT head
Consider lumbar puncture
Collect additional blood and urine for later testing
Examination and investigation findings
CB was lying on the bed, not moving spontaneously.
He had a patent airway with occasional snoring sounds. His respiratory rate was 15-20/minute with a periodic
breathing pattern; good air entry bilaterally; oxygen saturations 98% in room air.
His pulse rate was 40/min; blood pressure was high for his age at 140/90 mmHg; capillary refill time was 2 seconds.
He responded to painful stimuli only by withdrawing and moaning. He did not open his eyes when called repeatedly (P
on the AVPU scale). His modified Glasgow Coma Score was 8/15. His pupils were symmetrical but responded
sluggishly to light. Examination of the fundi showed fullness on the optic discs but no evidence of retinal
haemorrhages. There was no nystagmus or tonic deviation of the eyes. There was no evidence of convulsions or
abnormal limb positioning.
His axillary temperature was 35 degrees Celsius and felt cool and clammy. His bedside blood glucose level was 6.9
mmol/L.
Blood gas analysis showed respiratory acidosis
Blood ammonia was normal at 40 micromol/L (<50 micromol/L)
Test Result Range Test Result Range
HB 136 (135-165 g/L) Na 147 (135 – 147 mmol/L)
MCV 80 (80 – 100 fl) K 3.0 (3.2 – 5.2 mmol/L)
WCC 7.8 (4.5 – 10.0 109/L) Urea 10.0 (2.5 – 10.7 mmol/L)
Platelets 156 (120-500) Creatinine 0.11 (0.06 – 0.12 mmol/L)

5
The examination findings are consistent with increased intracranial pressure (ICP):
decreased level of consciousness, a slow pulse rate and high blood pressure (Cushing’s triad), slow pupillary
responses, full optic discs.
The absence of tonic eyes deviation/nystagmus makes non-convulsive status epilepticus unlikely as a cause for the
coma.
The normal bedside glucose rules out hypoglycaemia and diabetic keto-acidosis as a cause for coma. Normal blood
ammonia excludes Urea cycle defects and organic acidaemias
Regardless of the cause this child needs prompt resuscitation:
Airway and Breathing: CB has a GCS of 8 indicating that he is at risk of aspiration / airway obstruction. He
has evidence of respiratory failure with periodic breathing and a respiratory acidosis on blood gas analysis.
He requires urgent support of his breathing with bag-valve-mask ventilation, oxygen and monitoring while
preparation is made for intubation and ventilation.
Circulation: a secure intravenous line is a priority. If intravenous access cannot be established, then intra-
osseous access is needed.
Disability / neurology: CB has evidence of raised intracranial pressure (Cushing’s triad). 20% intravenous
mannitol or 3% hypertonic saline should be administered to decrease cerebral oedema and temporarily
decrease ICP while urgent investigations are done and transfer to definitive care is arranged. He should be
nursed with the bed 30 degrees head up to aid reduction of ICP.
A lumbar puncture is contraindicated in these circumstances
Broad spectrum antibiotics (eg 3rd
generation Cephalosporin) and Acyclovir should be given promptly to cover
the possibility of bacterial meningitis or HSV encephalitis. Intravenous steroids given with or just before the
first dose of antibiotics may improve the long term outcomes of bacterial meningitis, and may also assist in
reducing intra-cranial pressure. Anti-malarial treatment should be started if the child lives in a malaria
endemic areaTB also needs to be considered in endemic regions
CT head becomes of major priority to see if there is a neurosurgical cause of raised ICP such as intracranial
haemorrhage, an abscess, hydrocephalus, or a tumour
Arrangements are made to transfer CB to the intensive care of a tertiary children hospital.
How can you differentiate between the above causes?
A head CT scan will show evidence of an intra-cerebral mass, bleed, hydrocephalus or midline shift with
impending herniation. Children who live in areas endemic to malaria should have thick/thin blood films to
diagnose cerebral malaria.
Viral titres are useful for EBV, CMV, and Mycoplasma IgG and IgM are useful in all patients with non-
traumatic coma where the cause remain unexplained.
CB’s head CT scan was normal. He lived in Australia and had no history of travel to areas endemic for malaria. After the above measures of resuscitation were carried out CB’s clinical condition improved. He was transferred to the intensive care unit of a tertiary hospital where a brain MRI, CSF PCR for Herpes simplex and enteroviruses was done and an EEG organised.
The MRI showed thalamic abnormalities and the CSF PCR was positive for Enterovirus71 and negative for HSV type 1.
CB required respiratory and circulatory support in the intensive care unit for 4 weeks. His level of consciousness gradually improved. On discharge from ICU he was admitted to the rehabilitation ward where he received physiotherapy, occupational therapy and nutritional support for the next 4 weeks. He was then discharged home to continue with outpatient therapy, and follow up with a paediatric neurologist in one week.
Discussion:
This case demonstrates severe viral encephalitis. Other medical causes of coma include encephalopathy caused by
metabolic disease or toxins - often characterised by lack of an acute febrile illness, lack of CSF pleocytosis, and
absence of change on brain MRI.1
Encephalitis is mostly viral, however there are some bacterial causes. The incidence of viral encephalitis worldwide is
underestimated due to differences in surveillance systems between countries. Children with immune compromise
from any cause (primary immune deficiency, HIV, oncology patients on chemotherapy) are more at risk of contracting

6
viral encephalitis. The most common causative organisms in children with immune compromise are: EBV, CMV,
human Herpes Virus 6 (HHV-6) or HHV-7.
In immune competent people viral encephalitis is more commonly caused by other viruses such as arboviruses and
enteroviruses. There have been large epidemics of Enterovirus-71 in parts of Asia and Australia. Worldwide data
report an annual incidence of viral encephalitis between 3.5-7.4/100,000.
Children with viral encephalitis present with a flu-like illness followed by severe headaches, reduced level of
consciousness, nausea and vomiting. There may also be signs of meningism, seizures, and focal neurological signs.
Reduced level of consciousness may be due to increased intracranial pressure caused by meningitis, cerebritis or
metabolic disturbances.
Important clues on history:
A history of recent travel
Skin rash (varicella, slapped cheek disease (parvovirus), hand, foot and mouth disease (enterovirus)
Mouth ulcers (HSV type 1, hand foot and mouth disease)
History of parotitis, abdominal pain, testicular pain (mumps)
Important clues on examination:
Signs of meningism
Signs of increased intracranial pressure
Brainstem signs including respiratory and cardiovascular instability (enteroviruses, tuberculosis, listeria)
Movement disorders (arboviruses eg Japanese encephalitis)
Important investigations:
Blood culture
Viral Throat swab for respiratory viruses, Entervoviruses (culture and PCR)
Nasopharyngeal aspirate
Stool culture and PCR (Enteroviruses)
Serology for (HSV, CMV, VZV, EBV, Influenza viruses)
CSF culture and PCR
In cases where there is clinical evidence of increased intracranial pressure, a CT scan is the first imaging investigation
as it is fast and readily available. A normal CT does not exclude increased intracranial pressure but is useful to
exclude immediately treatable causes of high ICP such as intracranial haemorrhage or other intra-cerebral masses.
Management of children with encephalitis includes acute resuscitation, supportive therapy, and treatment for the likely
aetiology. Broad spectrum antibiotics and antiviral treatment should be initiated and continued until the results of the
diagnostic tests are available. Factors that would modify empiric treatment include history of travel, local disease and
resistance patterns, patient age and immune status.
Take Home Messages for management of Non Traumatic Coma
ABC: As with any seriously unwell patient assess Airway, Breathing and Circulation. Provide emergency support / treatment as necessary.
How deep is the coma? Allocate a GCS score, remember the rapid AVPU assessment. A conscious level of P (responds only to pain) corresponds with a GCS level of 8 or less and indicates that assessment and support of airway and breathing are needed.
Is the intracranial pressure raised? Look for clinical signs, and initiate measures to reduce intra-cranial pressure (20% mannitol IV, 3% Saline IV, steroids, position patient 30 degrees head up). Urgent consultation with senior experienced doctors is needed at this stage to direct emergency treatment, arrange diagnostic imaging (CT) and arrange transfer to a paediatric intensive care unit.
What other emergency treatments should be given? Broad spectrum antibiotics and acyclovir.
Always check the blood glucose level.

7
Image and a Diagnosis
A 11-month-old boy presented with a swollen right arm. His mother was carrying him when she fell down the stairs.
This newborn was born by an emergency cesearean section for macrosomia. He presented with the rash shown in the
pictures below. What is your diagnosis?
The rash is characteristic of blueberry muffin rash with multiple blue/purple marks or nodules on the skin. These are
due to blood producing cells in the skin (extramedullary erythropoiesis), or bleeding in the skin (purpura) or spreading
cancer (metastases).
Causes of blueberry muffin syndrome include:
Tumours: congenital leukaemia, Langerhans Cell Histiocytosis, neuroblastoma, rhabdomyosarcoma.
Blood disorders: Haemolytic disease of the newborn, hereditary spherocytosis, twin-twin transfusion
syndrome.
Congenital infections: Toxoplasmosis, Rubella, CMV, Herpes simplex, Coxsackie virus, Parvovirus, EBV,
Syphilis.
Investigations may include:
Full blood count and film – specialist review by a paediatric haematologist is recommended, as the initial features of leukaemia may be subtle.
Skin biopsy – to look for features of leukaemia or tumours.
Bone marrow biopsy – to look for features of leukaemia, blood abnormalities, infection or tumours.
Ultrasound scan of the abdomen – to look for hepatosplenomegaly and neuroblastoma.
Screening tests for congenital infection – TORCH screen, including maternal and infant serology and PCR, cerebrospinal fluid PCR, urine viral cultures, ultrasound and/or CT of the head, and other investigations as per clinical suspicion.
The treatment and prognosis will depend upon the underlying cause.
References
1. Thompson C, Kneen R, Riordan A, Key D, Pollard AJ. Encephalitis in children. Arch Dis Child 012;97:150-161
2. Blueberry muffin syndrome, http://www.dermnetnz.org/dermal-infiltrative/blueberry-muffin

8
Key Dates and Notices
Key Dates:
Case Report 2: August 2015 Steam - August 2015 stream Participants are advised that the due date for receipt of their Medical Case Report is Friday, 27
th March 2015.
Webcasts - Webcast for Monday 6th
April 2015 will not be held due to Easter holiday break.
Webinar Dates for 2015: Kindly diary the following Webinars dates (details will follow in due course): 13
th April, 2015
15th June, 2015
17th August, 2015
21st September, 2015
19th of October, 2015
Office closure: The DCH / IPPC Office is closed due to Sydney University Easter holiday break from Friday 3rd April 2015 to Monday 6th April 2015.
Notice: A/Prof Patrina Caldwell & eADVICE Pilot Study For Children With Urinary Incontinence:
In response to several queries from Participants on how to source specialist advice for children with urinary incontinence in view of the current wait period of 24 months, please see some useful information on the research study currently being conducted at The Children’s Hospital at Westmead which offers a total of 100 places open to children living in Australia. A/Prof Patrina Caldwell and her team have designed an interactive on-line program called eADVICE to help families of children with urinary incontinence. Please refer to program details and contacts appended below (Page 9).
Diploma/Certificate Distribution
Kindly note we are in the process of distributing Diploma/Certificate to all our December 2014 successful Participants. Appropriate communication will be sent once these have been posted.

9
eADVICE pilot study for children with urinary incontinence:
Thank you to A/Prof Patrina Caldwell for her recent lecture on children with urinary and faecal incontinence. We have
received several queries from Participants about how to source specialist advice as the waiting list for specialist
services this area in NSW is currently 24 months.
There is a research study currently being conducted at the Children’s Hospital at Westmead. The study is funded by a
grant from the Australian Bladder Foundation and has a total of 100 places open to children living in Australia.
A/Prof Caldwell and her team have designed an interactive on-line program called eADVICE to help families of
children with urinary incontinence.
The program asks the child and parents some basic questions and based on their response, provides tailored
treatment advice for the child. The family needs to try to follow the advice for a few weeks, and then go back into the
program and report:
1) whether they followed the advice and 2) if there were any changes to the child’s incontinence.
The program will again tailor the treatment advice and provide further information for them to follow until they visit the
program again in a few weeks. The family can access the program in this manner for up to 6 months.
The program simultaneously provides the information to the referring doctor, and the family are encouraged to see
their doctor at any time if they have questions or concerns. When the program advises medication, it asks the family
to take the child to see the doctor (with no further detail about the medication), and the doctor will be sent information
about what the program has found out about the child's condition (from the data entered), what medication (and dose)
is recommended, and why it is recommended.
It will then be left up to the doctor to make the decision about whether to use the medication, and to supervise the
treatment. eADVICE is intended to help doctors and patients start a treatment program based on current best practice.
If after discussion with the child’s family you would like to refer a patient please email the trial coordinator Sana
Hamilton:
The trial coordinator then contacts the family to further explain the study and enroll the child.
Please note that at the time the child is enrolled in the study a referral is also made to A/Prof Caldwell’s incontinence
clinic so that if treatment on the study program is not successful the child will already be on the waiting list to for
specialist incontinence services.
If you have any questions specifically for A/Prof Caldwell please email them to [email protected] and we will
forward them to her.

10
Who Are We?
Belinda Shephard
Executive Administrator
DCH / IPPC
I grew up in Wollongong, which is a city south of Sydney in a large family of eight. After completing my HSC, I began
an Arts Degree at The University of Wollongong, however, before my final year decided to travel and continue my
studies at a later date.
I spent 12 months travelling throughout Europe and another twelve months working in London before returning to
Australia and moving to Sydney. During this period I worked in various Executive Assistant/Project Administrator roles
within the hospitality and construction industries. I also married during this time and had four children, two girls and
two boys.
In 2007 I began working at The University of Sydney in various roles within the Faculty of Arts and Social Sciences,
Office of the Provost and the School of Medicine. In February 2012, I commenced work at DCH/IPPC as the Executive
Administrator and feel very honoured to be part of such a special group of people that assist in providing better health
care for children throughout the world through ongoing education.
The team at DCH/IPPC and our key supporters in Australia and around the world are a wonderful group of people and
I find it inspiring to be working towards a common goal of improving child health.