newsletter - slda
TRANSCRIPT

1
Newsletter of the College of General Dental Practitioners of Sri Lanka
EDITORIAL
Professor Saman Warnakulasuriya
BDS, FDSRCS (Eng & Edin),
FDSRCPS (Glasg),
Dip Oral Med (EAOM),
PhD (Glasg), DSc, FKC
Emeritus Professor,
Oral Medicine and Pathology,
King’s College London.
Oral cancer: Essentials for the Dental
Practitioner
Oral cancer remains an important public health problem, in Sri
Lanka and in many south Asian Countries. The disease affects both
men and women and all racial groups. The mean age at
presentation is around 60 years but oral and oropharyngeal cancers
are now becoming more common in younger ages. Oral cancer is
predominantly found among tobacco users, betel-quid chewers and
people who drink alcohol to an excess (1). It is estimated that
around 75% of oral cancer deaths are due to risky lifestyle habits.
A proportion of oral cancers are preceded by potentially malignant
disorders (earlier referred to as precancerous lesions and
conditions). These include oral leukoplakia, erythroplakia, lichen
planus and oral submucous fibrosis (2).
NEWSLETTER Newsletter of the College of General Dental Practitioners of Sri Lanka
December 2019 VOLUME 1- ISSUE 2
COUNCIL 2019
President
Emeritus Professor
Ganananda Nanayakkara
Secretary
Dr. Malcolm Stanislaus
Vice President
Dr. Lional Dassanayake
Assistant Secretary
Dr. S. L. Perera
Treasurer
Dr. C. H. Chang
Immediate Past President
Dr. H. Cooray
Editor
Dr. Shamilka Cooray
Members
Dr. M. Mukthar
Dr. N. Chinniah
Dr. [Mrs] S. Weerapperuma
Dr. [Mrs] Kanthi Chang
CONTENTS
Guest Editorial
Annual Sessions
Invited article I
Invited article II
SLMC approval for MCGDP
Invited article III
Invited article IV
Invited article V

2
Newsletter of the College of General Dental Practitioners of Sri Lanka
Oral cancer can affect the lip, oral cavity or the oropharynx. Lip cancer is a distinct entity, is rare in dark-
skinned populations and is mostly caused by exposure to UV sunlight among people not protected by the
melanin pigment. Oropharyngeal cancer is now considered a separate entity as it is primarily caused by
certain high-risk types (eg. types 16 & 18) of the human papillomavirus (HPV).
Clinical aspects
Oral cancer has multiple forms of presentation, and this sometimes makes the disease difficult to
recognize, especially in its early stages (3). This article describes the clinical manifestations of oral
cancer and its differential diagnosis to help the practitioner to differentiate the early forms from other
(non-cancerous) disease conditions.
Oral squamous cell carcinoma (OSCC) arises from the lining mucosa of the mouth and is by far the most
frequent type, accounting for over 90% of all oral malignancies. Other types of malignancies that arise
from different cell lineages are less frequent and include melanomas, sarcomas, malignant salivary gland
tumours and odontogenic tumours, as well as malignancies of the jaws, those metastasising to jaws from
distant organs and hematopoietic neoplasms such as lymphomas, leukaemias and multiple myeloma. Our
focus here is primarily on oral squamous cell carcinomas that are of epithelial in origin, and as stated
earlier that account for nearly 90% of all oral malignancies.
In Europe and North America over 50% of OSCCs are located on the lateral margins of the tongue and
the floor of the mouth while in Sri Lanka and in neighbouring countries OSCCs are mostly found on the
buccal mucosa, buccolabial commissure, sulci and around the retromolar trigone. However, OSCCs can
also be found in any other locations of the oral cavity such as on the palate and gingiva.
Described below are the principal clinical characteristics of OSCCs and an appraisal on their differential
diagnoses to facilitate early diagnosis.
Oral squamous cell carcinoma can be broadly divided in to initial or early stages and late or advanced
stages of the disease based on the size and extent of the tumour at presentation. As cancers grow at
different rates of proliferation what is usually referred to as early or late does not reflect on their times of
evolution but simply the size at presentation, i.e. small or large in terms of the extent of the disease.
Early stages of oral squamous cell carcinoma
OSCCs initially manifest as localized and usually well-demarcated white/red (erythroleukoplakic) areas.
Apart from their red or combined white-red colour, the only salient features of these lesions are their
hardened texture and some surface granularity.
The early lesions of OSCC are usually non-ulcerated, though over time one or more ulcerated zones may
appear on the erythroleukoplakic plaques, characterized by somewhat irregular margins, a gradual
increase in depth, elevated margins and especially some loss of elasticity.
3
Newsletter of the College of General Dental Practitioners of Sri Lanka
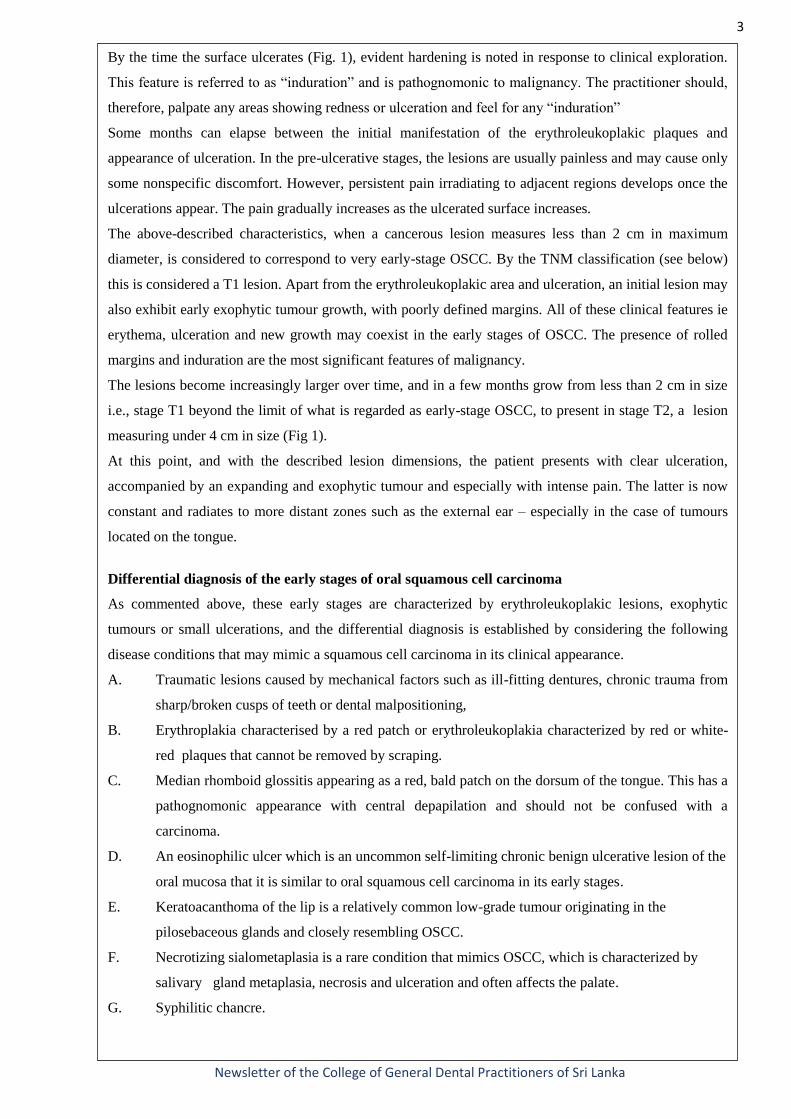
By the time the surface ulcerates (Fig. 1), evident hardening is noted in response to clinical exploration.
This feature is referred to as “induration” and is pathognomonic to malignancy. The practitioner should,
therefore, palpate any areas showing redness or ulceration and feel for any “induration”
Some months can elapse between the initial manifestation of the erythroleukoplakic plaques and
appearance of ulceration. In the pre-ulcerative stages, the lesions are usually painless and may cause only
some nonspecific discomfort. However, persistent pain irradiating to adjacent regions develops once the
ulcerations appear. The pain gradually increases as the ulcerated surface increases.
The above-described characteristics, when a cancerous lesion measures less than 2 cm in maximum
diameter, is considered to correspond to very early-stage OSCC. By the TNM classification (see below)
this is considered a T1 lesion. Apart from the erythroleukoplakic area and ulceration, an initial lesion may
also exhibit early exophytic tumour growth, with poorly defined margins. All of these clinical features ie
erythema, ulceration and new growth may coexist in the early stages of OSCC. The presence of rolled
margins and induration are the most significant features of malignancy.
The lesions become increasingly larger over time, and in a few months grow from less than 2 cm in size
i.e., stage T1 beyond the limit of what is regarded as early-stage OSCC, to present in stage T2, a lesion
measuring under 4 cm in size (Fig 1).
At this point, and with the described lesion dimensions, the patient presents with clear ulceration,
accompanied by an expanding and exophytic tumour and especially with intense pain. The latter is now
constant and radiates to more distant zones such as the external ear – especially in the case of tumours
located on the tongue.
Differential diagnosis of the early stages of oral squamous cell carcinoma
As commented above, these early stages are characterized by erythroleukoplakic lesions, exophytic
tumours or small ulcerations, and the differential diagnosis is established by considering the following
disease conditions that may mimic a squamous cell carcinoma in its clinical appearance.
A. Traumatic lesions caused by mechanical factors such as ill-fitting dentures, chronic trauma from
sharp/broken cusps of teeth or dental malpositioning,
B. Erythroplakia characterised by a red patch or erythroleukoplakia characterized by red or white-
red plaques that cannot be removed by scraping.
C. Median rhomboid glossitis appearing as a red, bald patch on the dorsum of the tongue. This has a
pathognomonic appearance with central depapilation and should not be confused with a
carcinoma.
D. An eosinophilic ulcer which is an uncommon self-limiting chronic benign ulcerative lesion of the
oral mucosa that it is similar to oral squamous cell carcinoma in its early stages.
E. Keratoacanthoma of the lip is a relatively common low-grade tumour originating in the
pilosebaceous glands and closely resembling OSCC.
F. Necrotizing sialometaplasia is a rare condition that mimics OSCC, which is characterized by
salivary gland metaplasia, necrosis and ulceration and often affects the palate.
G. Syphilitic chancre.

4
Newsletter of the College of General Dental Practitioners of Sri Lanka
H. Benign growths which have a soft, smooth appearance of the overlying mucosa. eg.
fibroepithelial polyp, epulis or granulomas
Some of these conditions may require biopsy verification to exclude malignancy (see later section)
Advanced stages of oral squamous cell carcinoma
Advanced stage OSCC is defined by the presence of a tumour measuring over 4 cm in size or infiltrating
neighbouring structures. These stages of the disease manifest as extensive ulceration with significant in-
depth infiltration or as exophytic growths sometimes with a verrucous component. It is common to
observe combined clinical presentations characterized by ulceration and exophytic growth within the
same tumour (Fig 2)
Advanced stage OSCC is associated with constant pain, with the need for frequent doses of analgesic
medication. Narcotic agents are commonly required to control the pain, which radiates towards
neighbouring structures such as the ear, or throat.
In addition to pain, advanced stage OSCC can be associated with mobility of teeth, bleeding and
paraesthesia, Dental mobility usually manifests when the tumour infiltrates the periodontal tissues and the
jaw bone. In the case of teeth not affected by periodontal disease secondary to dental plaque, spontaneous
dental mobility manifesting in a short period of time should cause us to suspect underlying malignancy –
particularly when the gum enveloping the tooth is swollen. If the dentist has removed such mobile teeth
the socket may not heal as expected. A patient wearing a denture may complain of a lack of fitness of the
denture.
A patient with an advanced malignancy will present with limitation of jaw movement, bad odour and
fixation of the tongue. As the disease progresses a patient may present with facial asymmetry or an
extraoral sinus tract with a fleshy outgrowth.
In the absence of antecedents of trauma (e.g., tooth extraction, dental surgery or injury), the presence of
paraesthesia in an area such as the chin is always suggestive of a malignant lesion – whether clinically
manifest or otherwise.
Neck metastasis
During the clinical examination, it is important to conduct a neck examination by palpation to assess the
status of lymph nodes. The anatomy of the neck with reference to levels of lymph nodes is shown in Fig 3
to assist proper palpation.
OSCCs of the tongue, the floor of the mouth or mandibular gingiva have a strong tendency to produce
neck metastases. The risk of regional lymph node metastasis in oral cancer is directly conditioned by the
location of the primary tumour, its size (T stage), depth of invasion and, of course, some histological
features such as lack of cohesiveness of tumour islands at the invasive front leading to vascular or
lymphatic spread.
Cancers of the oral cavity usually drain to the upper lymph node levels I, II, and III, and to a lesser extent
to lymph node level IV. Neck metastases can have a negative impact on prognosis.

5
Newsletter of the College of General Dental Practitioners of Sri Lanka
Classification by TNM system
The TNM classification considers tumour size (T), the presence of affected regional lymph nodes (N),
and the existence of distant metastatic spread (M) for staging the disease. Classifying a tumour by the
TNM staging system allows the specialist in making treatment decisions and conveys prognostic
information specific to cancer. Despite easy accessibility, most oral cancers are detected in T3 and T4
stages.
Adjunctive tests
A variety of optical devices and vital staining techniques are now commercially available to aid the
clinician to inspect morphological changes that may be found in the oral cavity. These tools are referred
to as diagnostic adjuncts or mistakenly as screening adjuncts. The most frequently reported adjunctive
test to assess oral mucosal abnormalities is the toluidine blue (TB) test (Fig 4). Staining with Lugol’s
iodine (Fig 5) is practised by maxillofacial surgeons. They have their place in secondary care facilities as
these staining tools may assist in selecting the biopsy site, to determine the margins of cancer during
surgery or in the surveillance of OPMDs during follow up. The optical devices (for example, VELscope,
Vizilite, Microlux and Orascoptic) generally detect changes in the optical properties of the surface
epithelium and submucosa based on light absorption, scattering, or fluorescence of tissue. Optical
detection systems are based on the assumption that the structural and metabolic changes that take place
in the mucosa during carcinogenesis give rise to distinct profiles of absorption and reflection when
exposed to different types (wavelengths) of light or energy. Though these tools are highly sensitive to
detect any abnormality their specificity is low and can result in false-positive detections, particularly
when used as screening devices. They are generally not recommended for use in primary care facilities
(4). There are also some novel salivary based detection systems. The OncAlert RAPID Test is a
qualitative point-of-care assay to aid in the decision to biopsy patients with a potentially malignant
disorders and or cancer. On application, the results are displayed either red (high risk of oral cancer),
yellow (intermediate risk), green (low risk). These systems need to be tested in primary care.
Referral
Once the dental practitioner notices any mucosal alteration suspicious of cancer (i.e. a red patch, a white
and red patch with soreness, ulceration or a growth persisting for more than 2 weeks or a non-healing
socket) it is paramount that the patient is urgently referred to a hospital consultant for further
investigation. The criteria for early referral when suspecting oral cancer can be found in the NICE
guidelines developed by the UK Department of Health (5). A patient arriving in a hospital with
suspected cancer should be immediately investigated by a biopsy to rule out cancer and to confirm the
diagnosis by a pathology examination.

6
Newsletter of the College of General Dental Practitioners of Sri Lanka
Discussion
Unfortunately, OSCC often progresses undetected or is misdiagnosed by primary care practitioners.
Almost half the patients experience diagnostic delays and over 50% present with advanced-stage disease.
Cancers detected in the late stages are difficult to treat and morbidity and mortality associated with oral
cancer are very high. Hence, early detection is key to a favourable prognosis. A high level of clinical
suspicion and an awareness of the early symptoms is required among dental practitioners to enable its
early detection.
References
1. Wong T, Wiesenfeld D. Oral Cancer. Aust Dent J. 2018 Mar;63 Suppl 1: S91-S99.
2. Warnakulasuriya S. Clinical features and presentation of oral potentially malignant disorders.
Oral Surg Oral Med Oral Pathol Oral Radiol. 2018 Jun;125(6):582-590.
3. Fanaras N, Warnakulasuriya S. Oral Cancer Diagnosis in Primary Care. Prim Dent J. 2016 Feb
1;5(1):64-68.
4. Warnakulasuriya S. Diagnostic adjuncts on oral cancer and precancer: an update for
practitioners. Br Dent J. 2017 Nov 10;223(9):663-666.
5. Head and neck cancers - recognition and referral. https://cks.nice.org.uk/head-and-neck-cancers-
recognition-and-referral#!scenarioRecommendation:2
Figure 1:A malignant ulcer of the tongue with rolled margins in T2 stage
Figure 2: An exophytic growth with a granular surface showing features of a squamous cell
carcinoma

7
Newsletter of the College of General Dental Practitioners of Sri Lanka
Figure 3: Diagrammatic representation of lymph node levels in the neck
Figure 4. A palatal ulcer stained with toluidine blue. A biopsy confirmed an early in-situ
carcinoma
Figure 5. Lugol’s iodine used to demarcate margins of a tongue carcinoma.

8
Newsletter of the College of General Dental Practitioners of Sri Lanka
ANNUAL SESSIONS
37th Annual Scientific Sessions of the
College of General Dental Practitioners, Sri Lanka
Theme: Current Trends in Cosmetic Dentistry and
Management of Oral Diseases
&
33rd Britto Muthunayagam Oration
will be held on
7th, 8th and 9th February 2020
at
The Sri Lanka Foundation Institute
100, Padanama Mawatha,
Independence Square, Colombo 07.
Chief Guest: Emeritus Professor Saman Warnakulasuriya
BDS, FDSRCS (Eng & Edin), FDSRCPS (Glasg), Dip Oral
Med (EAOM), PhD (Glasg), DSc, FKC
Emeritus Professor, King’s College London and Director
WHO Collaborating Centre for Oral Cancer.
Guest of honour: Dr. Lionel Dassanayake
LDS, FCGDP, FICCDE
Senior General Dental Pratitioner, Sri Lanka.
Orator: Professor A.M. Attygalla
BDS, MS, FDSRCS
Professor in Oral and Maxillofacial Surgery,
Dept. of Oral and Maxillofacial Surgery,
Faculty of Dental Sciences,
University of Peradeniya.

9
Newsletter of the College of General Dental Practitioners of Sri Lanka
ANNUAL SESSIONS Cont.
Pre Congress Workshops 7th & 8th Feb 2020
Workshop: 1
Professor Prasad Amaratunga (Sri Lanka) & Dr. Varun Achariya (India)
DENTAL IMPLANTS
Aim: Update dental professionals regarding Dental Implants and Hands on Practicals.
Venue: SLFI Lecture room 1
Date: 07th Feb 2020 - 8.30 A.M to 4.30 P.M
Workshop: 2
Emeritus Professor Saman Warnakulasuriya (United Kingdom)
ORAL MEDICINE:
Recent advances on oral potentially malignant disorders (precancers)
Oral ulcers: how to diagnose and manage them
Aim: Update dental professionals regarding best practice in the management of oral ulcers and the
early detection and prevention of oral precancer.
Venue: SLFI Lecture room 1
Date: 08th Feb 2020 - 8.30 A.M to 11.00 A.M
Workshop: 3
Dr. Andrew Paul Dias (Australia)
DENTAL PROSTHODONTICS:
Complete Denture Problems: examination, diagnosis & management
Aim: Update dental professionals regarding complete denture problems, ascertaining the most likely
cause and management.
Venue: SLFI lecture room 1
Date: 08th Feb 2020 - 1.00 P.M to 4.00 P.M

10
Newsletter of the College of General Dental Practitioners of Sri Lanka
ANNUAL SESSIONS Cont.
Sunday 9th February 2020
08.00 – 08.30 Registration
08.30 – 09.15 Lecture 1: Complete Denture Problems: examination, diagnosis & management, Dr.
Andrew Paul Dias
09.15 – 10.15 Keynote Lecture: Saving lives; The role of dental practitioners in the early detection
and prevention of oral cancer
Emeritus Professor Saman Warnakulasuriya
10.15 – 10.45 Morning Tea
10.45 – 11.30 Lecture 2: Pre-Surgical Assessment, Surgical Insertion and Implant Prosthodontics
Professor Prasad Amaratunga
11.30 – 12.15 Lecture 3: Guided Implant Surgery – Dr. Varun Acharya
(Sponsored by Duravit Dental Implants)
12.30 – 13.30 Lunch
13.30 – 14.15 Lecture 4: Endodontics: Prognosis and restoration of root filled teeth
Dr. P. Palipana
14.15– 15.00 Lecture 5: Orthodontics: Management of common orthodontic problems in developing
dentition
Dr. W M Senadeera
15.00 -15.30 TEA
15.30 – 16.00 Annual General Meeting of the College of General Dental Practitioners, Sri Lanka

11
Newsletter of the College of General Dental Practitioners of Sri Lanka
ANNUAL SESSIONS Cont.
The College of General Dental Practitioners of Sri Lanka
Application for Inauguration & Oration on 08th February 2020
&
Annual Sessions on 09th February 2020
@ Sri Lanka Foundation Institute, 100, Padanama Mawatha, Indipendance Square, Colombo 07.
Name: _______________________________________________________________
Name of accompanying person: ___________________________________________
Mailing Address: _________________________________________________
Telephone: ________________________ Email: _____________________________
Registration Details
Category Registration fee paid
on or before
30.01.2020
Registration fee paid
after 30.01.2020
Conference Registration on 9th Feb. 2020
Member
Non member
Students
Rs. 4000.00
Rs. 4500.00
Rs. 500.00
Rs. 4500.00
Rs. 5000.00
Rs. 500.00
Accompanying Persons CGDP Dinner only Rs. 2000.00 Rs. 2500.00
Preconference Workshop 1 Rs. 4000.00 Rs. 4500.00
Preconference Workshop 2 Rs. 4000.00 Rs. 4500.00
Preconference workshop 3 Rs. 4000.00 Rs. 4500.00
Conference Registration includes…………
Inauguration and oration 08th February 2020 &
Access to all Scientific Programmes and Trade Exhibition 09th February 2020
Entry to trade Exhibition will be allowed only to registered delegates
Dinner on 08th February and Lunch and Tea on 09th February 2020
Meals will be served only on production of meal coupons
Important: All workshop participants must be registered for the conference

12
Newsletter of the College of General Dental Practitioners of Sri Lanka
ANNUAL SESSIONS Cont.
Mode of Payment:
Cash/ Cheque
Amount: Rs……………
Date:………………………… Signature……………………………
Bank details:
Account name College of General Dental Practitioners of Sri Lanka
Payment reference Cash/ Cheques
Bank name Commercial Bank
Branch Borella
Account number 1050801201
Swift code CCEYLKLX
Contact number 0777347899
E mail [email protected]
Duly completed applications with payment (Account No: 1050801201, Commercial Bank, Borella) or
cheques drawn in favor of the College of General Dental Practitioners of Sri Lanka should be submitted
to the Honorary Secretary of the College, Dr. Malcolm Stanislaus, No. 50, Hekiththa Cross Rd,
Handala, Wattala. Phone 0777347899. E Mail [email protected]
Cancellation and Refund Policy:
Requests for cancellation of registration must be sent to Honorary Secretary of the College, Dr. Malcolm
Stanislaus, No. 50, Hekiththa Cross Rd, Handala, Wattala by post or email to [email protected]
All cancellations will be subjected to a cancellation fee of 50% for requests made on or before 31st Jan
2020 and no refunds or cancellations could be made after 31th Jan 2020.
For office use only
Registration number
Date received
Receipt number

13
Newsletter of the College of General Dental Practitioners of Sri Lanka
INVITED ARTICLE I
Dr A Jayathilaka
MBBS, MD, MRCS
Senior Registrar,
Teaching Hospital Peradeniya.
Thoracoscopic sympathectomy
Division of the thorasic ganglia of the sympathetic chain is done for following indications
Hyperhydrosis
Sympathetic dystrophy
Buergers disease
In these situations 2nd to 4th thorasic ganglia are removed. Caution is required to preserve the Stellate
ganglion in order to prevent Horners syndrome.
This procedure used to be done by open surgery via neck or axilla. However at our institute we perform
this using thoracoscopy. With minimal access approach the morbidity is reduced. In addition with
thoracoscopy only up to second ganglion is visualized protecting the Stellate ganglion.
Recently two patients with a cardiac arrhythmia were recently referred for symathectomy to denervate
heart. In this situation it was necessary to remove supply from Stellate ganglion as well. In order to
prevent Development of Horners syndrome dissection was continued along sympathetic chain and lower
half of Stellate ganglion was divided.
Thoracoscopic sympathectomy is performed under general anaesthesia. Conventionally lung collapse to
obtain space for dissection is obtained by using a double lumen endotracheal tube and one lung
ventilation. However as there are problems associated with placing a double lumen tube we use a more
convenient and safe technique. We provide ventilation using a single lumen and obtain a lung collapse
by a capnothorax. We have studied this and found using an insufflation pressure of 6-8Hgmm is safe and
effective. Surgery is done in a semi-prone or full prone position. This position allows the collapsed lung
to fall away from posterior mediastinum.
Professor KB Galketiya
MBBS, MS, FRCS, FCSSL, FMAS, FEVSI
Professor in Surgery & Honorary Consultant Surgeon
Faculty of Medicine,
Teaching Hospital Peradeniya.

14
Newsletter of the College of General Dental Practitioners of Sri Lanka
INVITED ARTICLE II
“My Rice Plate” an evidence-based model to lose excess body weight
Dietary changes of Sri Lankans have drastically changed in the past two decades with the evolving
urbanization, economic transition and technology growth. A study conducted presented that a
considerable percentage of the adult population failed to follow the recommended dietary guidelines.
Nearly 70% had exceeded the recommended starch intake, the daily intake of fruit (0.43 servings per
day) and vegetable portions (1.73 servings per day) had dropped well below national recommendations,
with only 3.5% of adults consuming the recommended five portions of fruits and vegetables per day. Sri
Lankans obtain nearly 72% of their calorie requirement by carbohydrates (mainly refined), while only
10% of calories are derived from proteins which is not surprising for a country where our staple food is
rice. Prevalence of Obesity is drastically increasing worldwide, and Sri Lanka has not been left behind.
Currently, over a quarter of Sri Lankan adults are suffering from obesity with a higher prevalence of
obesity seen among women and middle aged adults.
Obesity is caused mainly by the imbalance of energy intake and expenditure. With obesity the associated
major rising health burden on a country is the prevalence of Non-communicable diseases (NCDs), which
is the leading cause of morbidity and mortality worldwide. The obesity associated NCDs have reached
epidemic proportions in Sri Lankan adults for example; prevalence of metabolic syndrome is 25%,
hypertension is over 20%, and dysglycemia is 21%. Such comorbid factors have had a huge impact on
health care expenditures. Of total deaths, 75% of deaths were accounted by NCDs. Of these deaths, 40%
were Cardiovascular disease (CVD) related deaths alone. Epidemic of Obesity and associated NCDs are
results of unfavourable changes in lifestyle including unhealthy dietary habits and physical inactivity
which further impacts the energy balance affecting the body weight.
A typical rice plate of a Sri Lankan consists of 400g of boiled rice in average and the contribution of
vegetables and proteins are considerably very low. Therefore, the total plate would provide around
600kcal and thus if eaten thrice a day the daily energy requirement of a sedentary adult is exceeded. As
mentioned, excess energy intake is a major determinant with weight gain, obesity and associated chronic
NCDs. To tackle this “My Rice Plate” was designed according to the ‘Plate Model’ recommended by
local and international nutrition guidelines.
Dr. Ranil Jayawardena
MBBS(Col), MSc(Glasgow), PhD(QUT),
HND(UK), Nutr(SLMC), RNutr(UK), RNutr(Aus),
Clinical Nutritionist, Senior Lecturer, Department of Physiology,
Faculty of Medicine, University of Colombo, Sri Lanka.

15
Newsletter of the College of General Dental Practitioners of Sri Lanka
‘Plate model’ is a practical method to overcome the prevailing dietary patterns by reducing the average
portion size of the staple food in main meals and ensures the sufficient intake of vegetables and protein
rich foods synchronously.
“My Rice Plate” is a portion perfection plate designed for Sri Lanka complying with the internationally
used ‘Plate Model’ concept.
“My Rice Plate” model is key in addressing three common issues; Controlling portion size, Nutrition
balance and eating awareness. DR. Ranil Jayawardena’s team has conducted a clinical trial on this plate
concept. Key findings of the study revealed that the intervention group that followed the plate model
had a significant effect on weight and BMI reduction after 12 weeks than the control group.
There is a huge emphasis on dietary guidelines as its importance of a balance and varied diet. Meals
that include no servings or few servings of protein and vegetables lack both balance and variety. A
substantial proportion of the Sri Lankan population does not consume a varied and balanced diet which
results in unhealthy eating habits. ‘My Rice Plate’ is ideal as it is simple and is an efficient method to
follow a balanced diet, certainly it is an alternative to the traditional way of exchange-based teaching
and meal planning.
SLMC Approval for MCGDP
The College of General Dental Practitioners (CGDP) was
successful in obtaining the Sri Lanka Medical Council (SLMC)
approval for Membership of the College of General Dental
Practitioners as an additional qualification for the registered
dental practitioners under the section 24(1) of the Medical
ordinance. CGDP is planning to commence the course in 2020.

16
Newsletter of the College of General Dental Practitioners of Sri Lanka
INVITED ARTICLE III
Anaemia in clinical practice
Anaemia is present when haemoglobin (Hb) content is below the expected values for the age and sex.
The cut off values defined by the WHO for men, non-pregnant women and pregnant women are 13, 12
and 11g/dL respectively. In children the cut off values are even lower (6-5 yrs 11g, 5-11 yrs 11.5g and
12-14 yrs 12 g).
Anemia could result from a variety of causes which include reduction of Hb synthesis (Iron, B12, folate
deficiency, Bone marrow disorders) or excessive blood loss through bleeding or hemolysis. Anemia is
classified according to the size of red blood cells (RBC) into Microcytic Normocytic or Macrocytic
anaemia for the purpose of investigations. Mean cell volume (MCV) of a normal RBC is 80-100 fl.
The three commonest causes of anaemia in clinical practice are iron deficiency, anemia of chronic
disease and thalassemia.
Clinical recognition of anaemia
Loss of energy, palpitations, breathlessness and headache, particularly with exertion, and leg pain are
common symptoms of anaemia.
Pica, which means craving for items like raw rice or clay, is only associated with iron deficiency and is
a useful symptom to discriminate iron deficiency from other anaemias. History of menorrhagia or
bleeding hemorrhoids suggest blood loss leading to iron deficiency. Family history of low Hb in siblings
and consanguinity directs toward thalassemia or other hereditary causes of anaemia. Presence of
concomitant medical problems such as long standing diabetes, hypertension, kidney, joint or respiratory
disease may point towards the diagnosis of anemia of chronic disease.
Physical examination
A common observation in anemia is the pallor of skin and mucosa. Glossitis leading to a smooth and
shiny tongue and angular stomatitis suggests iron deficiency. In iron deficiency, the nails are flat or
spoon shaped. Nails may also be brittle, and excessive hair loss may be present. Petichiae in mucosae
and skin, fever, oral ulcers suggest thrombocytopenia and neutropenia together with anaemia and points
towards bone marrow failure. In advanced leukaemia, gum infiltration and hemorrhagic lesions on the
oral cavity are seen.
Professor C.K. Bodhinayake
MBBS (Ruhuna), MD(Col), MRCP(UK) Professor in Medicine & Honorary Consultant Physician, Department of Medicine,
Faculty of Medicine,
University of Ruhuna.

17
Newsletter of the College of General Dental Practitioners of Sri Lanka
Beta thalassemia major leads to marrow expansion and altered facies such as frontal bossing and malar
prominence. It is important to note that in Sri Lanka, minor forms of thalassemia with mild anaemia are
commoner, and are generally passed unnoticed or confused with iron deficiency.
Presence of hypertension together with anaemia suggest chronic renal disease which is also common in
clinical practice.
Investigations
A full blood count (FBC) confirms the presence of anaemia, the type of anaemia according to the size of
RBCs, as described earlier and the state of white blood cells (WBC) and platelets. Blood film is an
essential initial investigation, which is complementary to the FBC and will show the cell morphology
clearly. When Hb, WBC and platelets are all reduced which is known as pancytopenia, bone marrow
failure is indicated.
Mean cell volume(MCV) is used to classify anemia into different types and further investigations can be
planned accordingly. Iron deficiency is confirmed by the presence of microcytic RBC, and low serum
ferritin levels. Thalassemia is differentiated from iron deficiency by normal or high serum ferritin
despite the presence of microcytic RBC. Anaemia of chronic disease is increasingly common in adullts
and is distinguished by the presence of normocytic RBC, with normal or elevated ferritin.
In addition to the three common types of anaemia which need to be readily recognized by the clinician,
there are other less common aetiologies which need further evaluation beyond office practice.

18
Newsletter of the College of General Dental Practitioners of Sri Lanka
INVITED ARTICLE IV
Orthodontics in Sri Lanka, a Way Forward……..
There has been a major change in orthodontics during the second half of the last century.
Especially, with the development of straight wire technique towards the latter part of the century
which has made the life of an orthodontist much more comfortable. At present, even the general
dental practitioners with an adequate depth of knowledge in Orthodontic diagnosis, basic
Orthodontic treatment planning and moderate skill in manipulation of appliances, practice straight
wire appliance (SWA) technique worldwide.
Even though SWA looks like a simple appliance superficially, it demands a thorough knowledge
and understanding of bio mechanics involved in it. With the improvement of information
technology, patients and parents are becoming more and more aware of the facilities and
treatment modalities available for correction of Malocclusion and also of the final treatment outcome
expected. Therefore, the demand for Orthodontic Specialists’ care is ever increasing worldwide. But
in Sri Lanka the situation is completely different. We are still left with a handful of
Orthodontists who are unevenly distributed in the country making overcrowding of existing
Orthodontic units. There is also a substantial proportion of Orthodontic patients with unmet demand.
This makes the contribution of the general dental practitioner in the management of orthodontic
patients is very important in the present context.
The goals of modern Orthodontic treatment can be categorized in to five main headings. They are,
improvement of facial esthetics and dental esthetics, maintenance of functional occlusion, maintain or
improve health of periodontal support and masticatory system and also obtain a stable result. The goals
of facial esthetics differ from population to population. In general there should be adequate naso-
labial angle, reasonably prominent chin and ability to close the lips without a muscular strain.
With regard to smile esthetics, a smile line in which the crowns of the upper incisor teeth and
1-2 mm of gingival margin should be visible. The lower lip should cover 3 mm of labial
surface of upper incisors at the end of Orthodontic treatment.
There should be an adequate proclination of upper incisors, 105 degrees to the Frankfort Plane
judged by clinical observation or 109 degrees inclination to the Maxillary Plane determined with
cephalometric assessment. Upper central incisors should be 1 mm longer than lateral incisors
with flat incisal edge and upper lateral incisors should have a rounded edge.
Professor Nandani Nagarathne
BDS, MS(Orthodontics),
Professor in Orthodontics,
Department of Community Dental Health,
Faculty of Dental Sciences,
University of Peradeniya.

19
Newsletter of the College of General Dental Practitioners of Sri Lanka
The crown height of the Maxillary canines should be 1 mm longer than that of lateral incisor and
canine should have a pointed tip. The gingival margin should be symmetrical on anterior teeth
and should gradually step down towards posterior teeth. All teeth should be in correct contacts without
spacing or crowding with slightly curved or rather flat curve of Spee.
At the end of Orthodontic treatment, when upper and lower teeth are in maximum inter-
cuspation, the condyles should be in centric relation. There should be equal contacts of
centric cusps of posterior teeth. On movement, there should be sufficient incisor guidance with
posterior dis-occlusion. This needs 4 mm. of OB and 2-3 over jet in finishing occlusion. There
should be free movement of dental arches in all direction without interferences from cusps. It is
ideal if Class 1 Molar Relationship could be achieved to maintain satisfactory function. But as an
acceptable compromise, Class II full unit molar relationship could be achieved. But Class 1 canine
relationship is mandatory. Further, elimination of rotations of teeth is important in order to line up
contact point to contact point. The choice of appliance prescription and use of appropriate bio
mechanics to place individual tooth to establish centric stops of posterior teeth and obtaining
arch form which should be harmonious with original arch form of the patient which is supported by
masticatory and facial musculature are paramount. Maintenance or attainment of proper incisal and
cuspid guidance ensures adequate function. Minor surgical procedures such as Fiberotomy of rotated
teeth and eliminating tooth size discrepancies are added treatment procedures which should be
undertaken to ensure stability. Clear nasal airway and elimination of undesirable neuromuscular
habits is also important to obtain a stable result. As any tooth movement involves laying down of
irregular bone which is highly vascular which is prone to resorbtion even with slight imbalance of soft
tissue force. Therefore, adequate retention regimen should be included in the overall treatment plan.
During Orthodontic tooth movement the tooth is moved along the cancellous struff of alveolar bone.
This movement should be carried out to place teeth in planned positions without damage or minimal
damage to the tooth structure. At the end of treatment, there should be adequate periodontal support
without fenestration or dehiscence, good crestal bone height without periodontal pocketing and
gingival inflammation.
An adequate thickness of attached gingivae without any frenal pull and optimum crown root
ratios ensures health of the periodontal support. All in all health and function of periodontium and
masticatory system should not be compromised to achieve ideal esthetic goals.
The ideal goals of orthodontic treatment should be kept in mind always, otherwise there is a
risk of achieving and accepting our results as our ideal orthodontic goals. Finally we have to
save many teeth as possible, save patient from surgery, save treatment time, prevent root
resorbtion and loss of crestal bone in order to preserve tooth and supporting tissues.
All these goals could be achieved by selecting cases very carefully and timing treatment to
obtain optimal result with less inconvenience to the patient. Quality of the results achieved with
orthodontic treatment mainly depends on the detailed case assessment, correct orthodontic
diagnosis and meticulous attention given in the treatment planning stage. Selection of cases which
require adequate attention of the orthodontic specialists both in diagnosis and treatment planning stage
is mandatory to ensure quality of care provided to the patient.

20
Newsletter of the College of General Dental Practitioners of Sri Lanka
In a market oriented society there is a trend to offer short term courses in orthodontics to practitioners
without providing much emphasis on these important aspects of orthodontics. Curricula of
postgraduate courses to train orthodontic specialists are expanded and revised keeping this need for
quality assurance in mind. This makes a time demanding issue to a practitioner who opts to establish his
or her own private practice. There are many cases which do not require specialist care and these
cases could be managed by careful case selection and employing simple bio mechanics by a general
dental practitioner who updates knowledge and develops skill to manage simple cases.
It is a sad situation dividing orthodontics simply to two appliance systems, removable and fixed
appliances. We all should understand the fact that in orthodontics, it is the complexity of the case with
regard to diagnosis, need to identify limiting factors and complexity of the bio mechanics needed to
move teeth to desired position are the dividing line between the specialist and the general
practitioner. But the majority of the cases are amenable to simple mechanics.
It is the time to rethink this need and introduce a middle grade course either with short term or even
distant learning education with regular updating of the knowledge and skill of the practitioner.
It is the responsibility of the policy makers to identify this burning issue in Sri Lanka and come to an
amicable settlement to improve quality of orthodontic care provided to the public.

21
Newsletter of the College of General Dental Practitioners of Sri Lanka
INVITED ARTICLE V
Dental fluorosis
Dental fluorosis is a public health problem in many parts of the world, including the dry zone of Sri
Lanka. It is an enamel defect that results from excessive intake of fluoride during the developmental
stages of teeth. The window of susceptibility for dental fluorosis is from birth to eight years of age. The
clinical appearance of dental fluorosis varies from minor white striations to more extensive opacities
with or without pitting of enamel. Due to the disfiguring nature of severe forms of dental fluorosis it
could affect the quality of life of an individual. .From the available evidence it is clear that consumption
of water with high concentration of fluoride, infant formulas used before the age of six years, inadvertent
use and ingestion of fluoridated toothpaste during tooth development stages, use of fluoride supplements,
professionally applied topical fluorides, black tea consumption, use of amoxicillin, and some socio-
demographic factors such as socio-economic status, sex are risk factors for dental
fluorosis.
Dental fluorosis is a preventable condition. According to the WHO water quality guidelines (2017) it is
recommended that, if fluoride concentration in drinking water exceeds 1.5ppm, it is necessary to
defluoridate the water prior to consumption. If de-fluoridation is not possible, people living in high
fluoride areas should use water from alternative sources such as from wells tested for low fluoride levels,
bottled water or harvested rain water.
Dental practitioners should be aware that children are exposed to fluoride from multiple sources in recent
times. Clinicians should provide advice to parents regarding the proper use of fluoridated toothpastes.
Children under the age of 3 years should be given only a smear layer of fluoridated toothpaste on the
toothbrush while those between the ages of 3-8 years should use only a pea-sized amount of fluoride
toothpaste. Tooth brushing in young children should be supervised by parents to prevent ingestion of
fluoridated toothpaste.
Different treatment modalities are available for dental fluorosis and they include enamel micro and
macro abrasion, direct composite veneers, porcelain veneers and crown restorations.
Dr. B.K.G. Thilakarathne
BDS, MSc (Com Dent), MD (Com Dent)
Lecturer,
Department of Community Dental Health,
Faculty of Dental Sciences,
University of Peradeniya.