next generation tkis and small molecule inhibitors jennifer r brown, md phd director, cll center...
TRANSCRIPT
Next Generation TKIs and Small Molecule Inhibitors
Jennifer R Brown, MD PhDDirector, CLL Center
Dana-Farber Cancer InstituteAssociate Professor of Medicine
Harvard Medical School
October 24, 2014

Targeting Kinases in the BCR Pathway
Idelalisib (GS-1101; CAL-101)Ibrutinib (PCI-32765)
Dasatinib FostamatinibEverolimus

Agent Sponsor ORR Development Phase
BTK inhibitors Ibrutinib CC-292 ONO-4059 ACP-196
Pharmacyclics, Inc.Celgene CorporationOno Pharmaceutical
Acerta
71 – 88%31-67% (PR)
89% (PR)—
Registration Phase III Phase IbPhase IPhase I
PI3KΥ/δ inhibitors Idelalisib GS-9820 IPI-145 AMG 319 TGR-1202 SAR245408 (XL147)
Gilead SciencesGilead Sciences
Infinity PharmaceuticalsAmgen
TG Therapeutics
Sanofi
72-100%—
89% nodal33% nodal
—
40% PR
Registration Phase IIIPending Phase I
Phase IIIPhase IPhase I
Phase I
Syk inhibitors GS-9973 Fostamatinib PRT-2070
Gilead SciencesRigel Pharmaceuticals
Portola
—55% nodal
—
Phase IIPhase I/II
Pending Phase I
BCR-Directed Agents in Development for CLL

Targeting Kinases in the BCR Pathway
IPI-145TGR-1202
CC-292 (AVL-292)ONO-4059
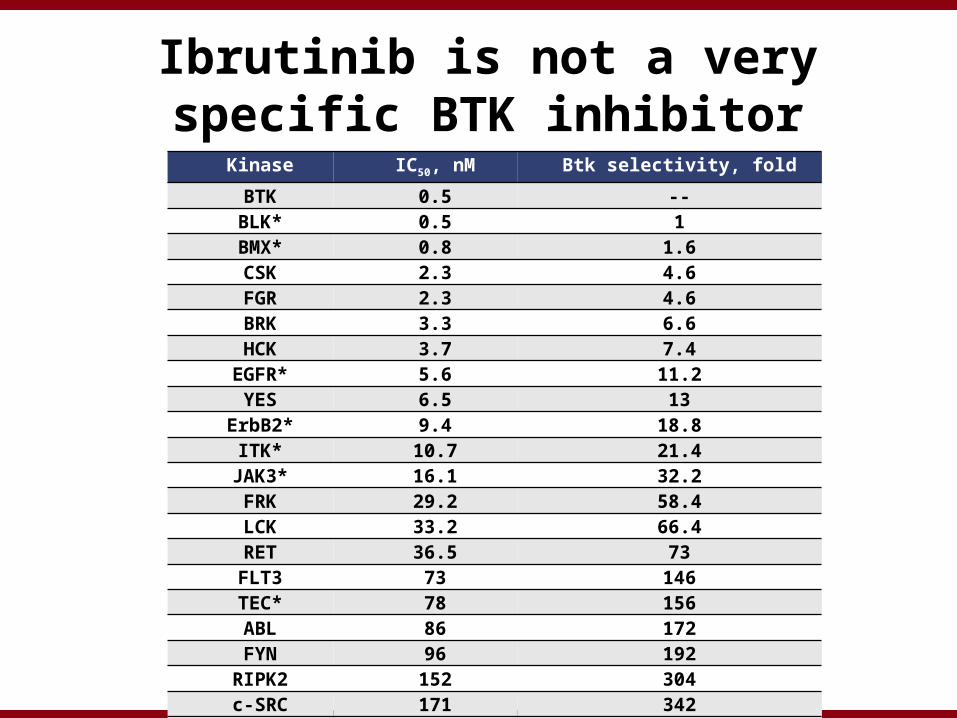
Kinase IC50, nM Btk selectivity, fold
BTK 0.5 --BLK* 0.5 1BMX* 0.8 1.6CSK 2.3 4.6FGR 2.3 4.6BRK 3.3 6.6HCK 3.7 7.4
EGFR* 5.6 11.2YES 6.5 13
ErbB2* 9.4 18.8ITK* 10.7 21.4
JAK3* 16.1 32.2FRK 29.2 58.4LCK 33.2 66.4RET 36.5 73FLT3 73 146TEC* 78 156ABL 86 172FYN 96 192
RIPK2 152 304c-SRC 171 342LYN 200 400
Ibrutinib is not a very specific BTK inhibitor

Patient AgeNo.
Prior Ther.
Cytogenetics Study Treatment
Duration on
Ibrutinib
Best Response
Identified Mutation
1 59 5del(17p13.1),
+12560 mg qd 621 days PR C481S BTK
2 75 2del(17p13.1),
complex karyotype
420 mg qd 673 days PRR665W PLCγ2
3 59 3 del(11q22.3)BR x 6 cycles,
420 mg qd388 days CR C481S BTK
4 51 2complex
karyotype
Ofatumumab x 24 weeks, 420
mg qd674 days CR C481S BTK
5 69 9del(17p13.1),
complex karyotype
840 mg qd 868 days PR C481S BTK
6 61 4del(17p13.1),
complex karyotype
Ofatumumab, x 24 weeks, 420
mg qd505 days PR
L845F PLCγ2,
C481S BTK
Mechanisms of Resistance to Ibrutinib
Chang et al., ASCO 2013; Stilgenbauer et al., IWCLL 2013; Woyach NEJM 2014

CC-292 Specificity
Kinase Cell Line CC-292Cellular
EC50
Btk Ramos 8 nM
EGFR A431 >4000 nM
Jak-3 CTLL-2 500-1000 nM
Itk Jurkat 1000 nM
Kinase CC-292 (IC50)
Btk <0.5
Brk 2430
c-Src 1729
Csk >10000
Fyn 7146
Hck 14460
Lck 9079
Syk 1134
Lyn 4401
Yes 723

Uncoupling PK PD with CC-292:Normal Volunteers, 2 mg/kg dose

Study Design
iNHLDose TBD
PART 1: Identify RP2D PART 2
CLL/SLL 500 mg BID
Cohort Dose (mg)
Once dailyDL 1DL 2DL 3DL 4DL 5DL 6a
125 QD250 QD400 QD625 QD750 QD
1000 QD
Twice dailyDL 6bDL7
375 BID500 BID
• Continuous 28-day oral dosing until PD or intolerable toxicity
– 3 + 3 design for cohorts 1-5
– 12 patients per cohort 6a, 6b, and 7 (6 CLL/SLL, 6 NHL/WM)
•Reported analyses focused on patients with CLL or SLL
Ongoing phase 1, multicenter, open-label, dose-escalation study (NCT01351935)
CLL/SLL 750 mg QD
RP2DCLL Expansion
Cohort
Dose Escalation
DLBCLDose TBD
Brown et al, EHA 2013

Baseline Characteristics (84 CLL/SLL patients enrolled from Aug 1, 2011 to July 1, 2013)
Median age, yrs (range) 66.5 (34-89)
Gender, male 58.8%
Rai stage 3-4 disease 53.6%
Median prior therapies, n (range) 3 (1-12)
Refractory 34.5%
Poor-risk factors11q del17p delUnmutated IgVH
56 (66.7%)18 (21.4%)20 (23.8%)45 (53.6%)
Study Population

Time on Study – All Patients

BTK Occupancy 4 Hrs Post Dose
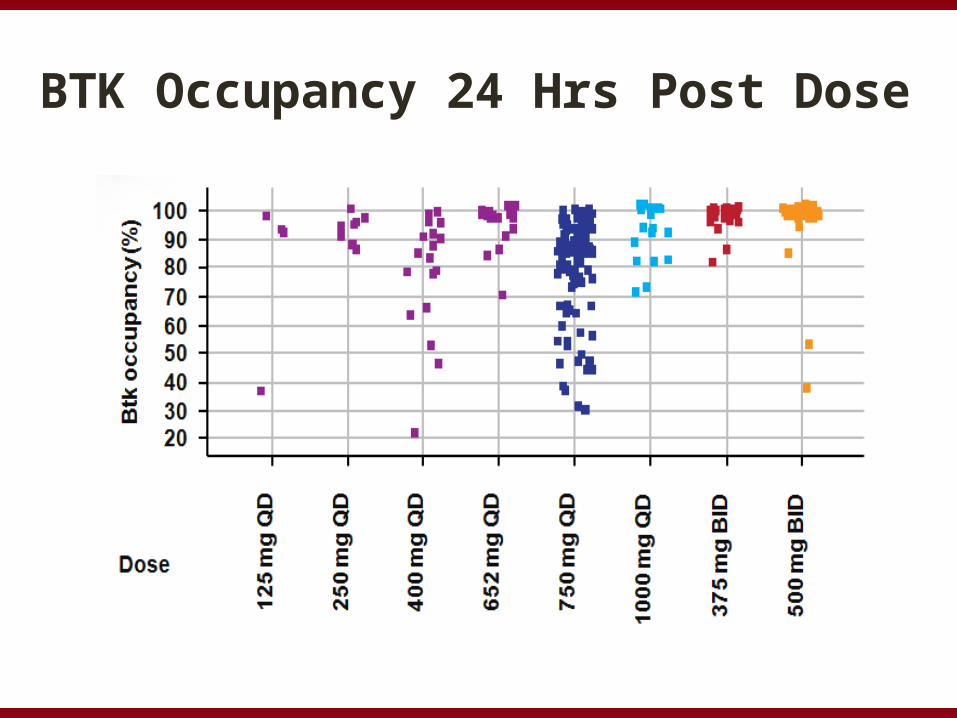
BTK Occupancy 24 Hrs Post Dose

CC-292 Lymph Node Response by Dose and Time

Efficacy Assessment by Dose Level
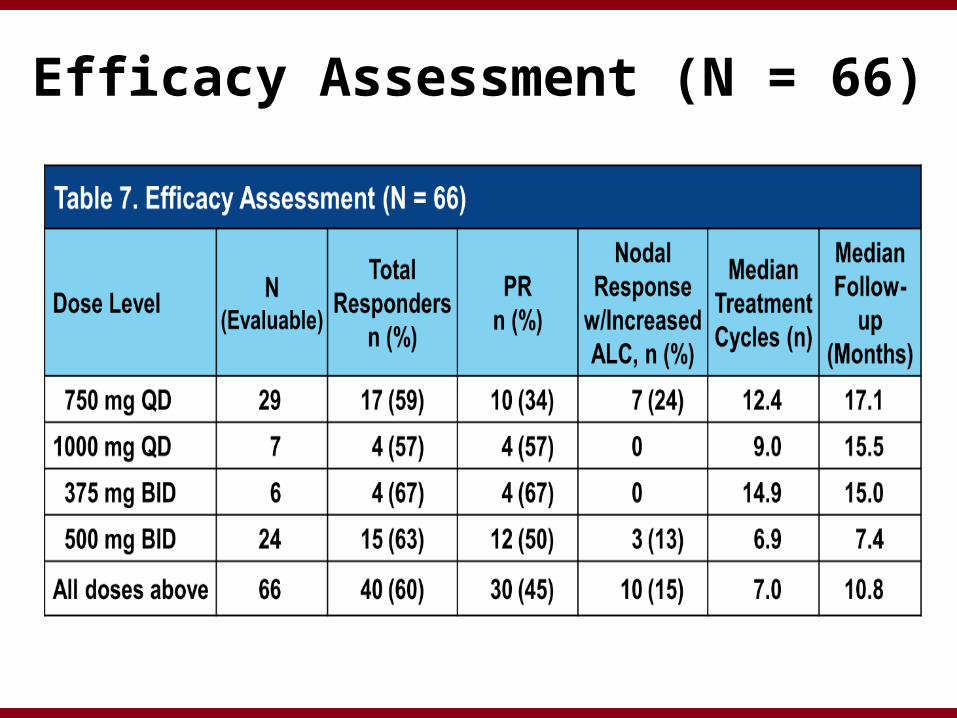
Efficacy Assessment (N = 66)

Response Based on Prognostic Factors Efficacy Evaluable Patients at Active Doses
(N = 60)

ONO-4059
• ONO-4059 is a highly potent and selective, orally available Btk inhibitor that covalently binds to Cys-481 in Btk.
• Very high selectivity towards BTK (IC50 = 2.2 nm/L).• Bio-availability 40-50% with half-life of 5-7 hours and ∼ ∼ > 90% BTK
inhibition at 12 hours in CLL cells in vivo.
SykLyn
BtkPLCg2
PI3
K
P
PIP3CD
79A
CD
79B
PP
P
PP
ONO-4059
Y223
PDK
AKT
BLNK
PI3K/Aktpathway
MAPK/NF-kBpathway
B cell receptor
B-cell activation and proliferation
P
Yoshizawa T, et al (ICML, 2013)

Study ONO-4059POE001
3 months 6 months
TUMOR ASSESSMENT
• 3+3 phase 1 design• Once daily dosing (QD)• Initial 6 month treatment, with
option of additional 18 months,
+/- dose escalation• No restrictions on growth factor,
anticoagulant use• 6 sites (UK & France)
1 month
# 1 patient experienced Rash (Grade 2) resulting in 1 week drug interruption during Cycle 1 and another patient enrolled to ensure 3 patients completed the required 28 days drug administration in Cycle 1.
ONO-4059Dose
Number of patients(N=25)
20mg 3
40mg 3
80mg 4#
160mg 3
320mg 3
400mg 3
500mg 3
600mg 3
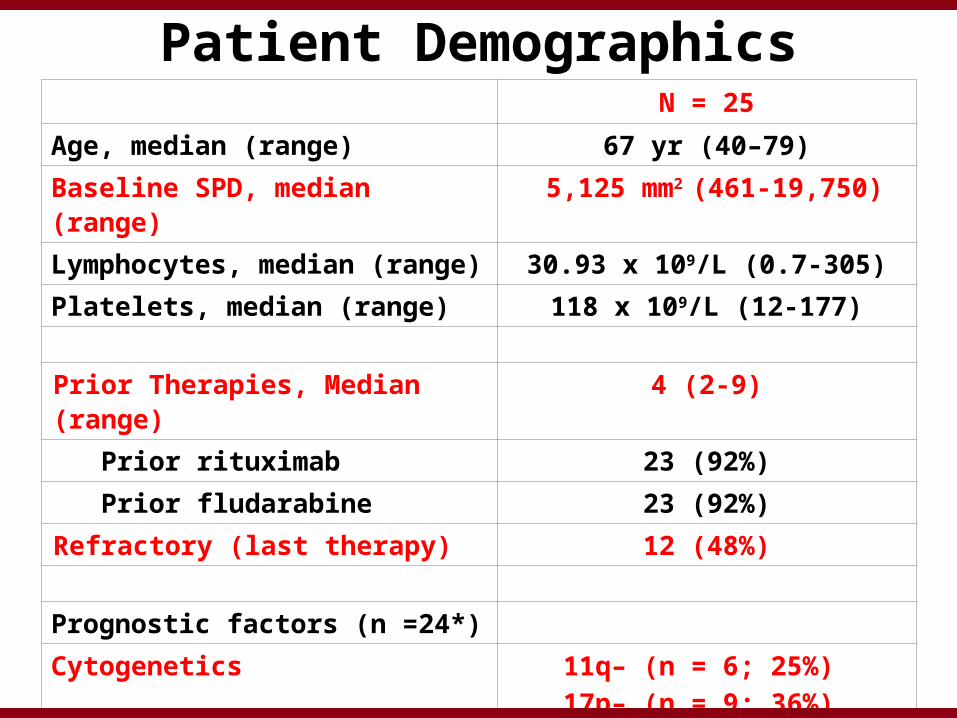
N = 25Age, median (range) 67 yr (40–79)Baseline SPD, median (range) 5,125 mm2 (461-19,750)Lymphocytes, median (range) 30.93 x 109/L (0.7-305)Platelets, median (range) 118 x 109/L (12-177)
Prior Therapies, Median (range) 4 (2-9)Prior rituximab 23 (92%)Prior fludarabine 23 (92%)
Refractory (last therapy) 12 (48%)
Prognostic factors (n =24*)
Cytogenetics 11q– (n = 6; 25%) 17p– (n = 9; 36%)
TP53 Mutated (n=13; 54%)
IgVH Unmutated (n =21; 87.5%)
Patient Demographics

0 4 8 12 16 20 240
50
100
150
200
250
0
20
40
60
80
100
120
Plasma concentration Btk inhibition
Time (hours)
Pla
sm
a C
on
ce
ntr
ati
on
of
ON
O-4
05
9(n
g/m
L)
Btk
In
hib
itio
n (
%)
40mg (QD) ONO-4059 Leads to Durable Btk Inhibition (pBtk/PBMCs)
Relapsed patient with 17p del; tumour reduction by CT-Scan: 64% (C3); 79% (C6); 86% (C10), 89% (C13); Haematology parameters normal at 3 month time-point

Related Grade 1-2 Adverse Events(in ≥ 2 Patients)
Adverse Event
Patient (N=25)
*CTC Grades 1-2
AEs
CTC Grade 1N
(Dose Level)
CTC Grade 2N
(Dose Level)
Haematoma 4 2 (500mg, 600mg) 2 (160mg, 400mg)
Rash 43 (40mg, 400mg,
600mg)1 (80mg)
Acne 33 (40mg, 80mg,
160mg)-
Asthenia 2 1 (160mg) 1 (20mg)
Diarrhea 2 1 (160mg) 1 (40mg)
Fatigue 2 2 (40mg, 80mg) -
Petechiae 2 1 (160mg) 1 (400mg)
Shingles 2 1 (500mg) 1 (40mg)
*Common Toxicity Criteria Adverse Events Version 4.0 (CTCAEV4.0)

Related Grade 3-4 Adverse Events (in ≥ 2 Patients)
Adverse Event
Patient (N=25)
*CTC Grade 3-4N
CTC Grade 3N
(Dose Level)
CTC Grade 4N
(Dose Level)
Neutropenia 5 2 (20mg, 40mg ) 3 (20mg, 80mg, 320mg)
• No DLTs observed• Two events of neutropenia (G3 at 20mg/G4 at 320mg) were
reversed rapidly using G-CSF• Patient who experienced neutropenia at dose 20mg (Grade 4),
also experienced an event of febrile neutropenia which was reported as an SAE. Patient’s neutrophil value at study entry was 0.1 x109/L (CTC Grade 4)
*Common Toxicity Criteria Adverse Events Version 4.0 (CTCAE V4.0)
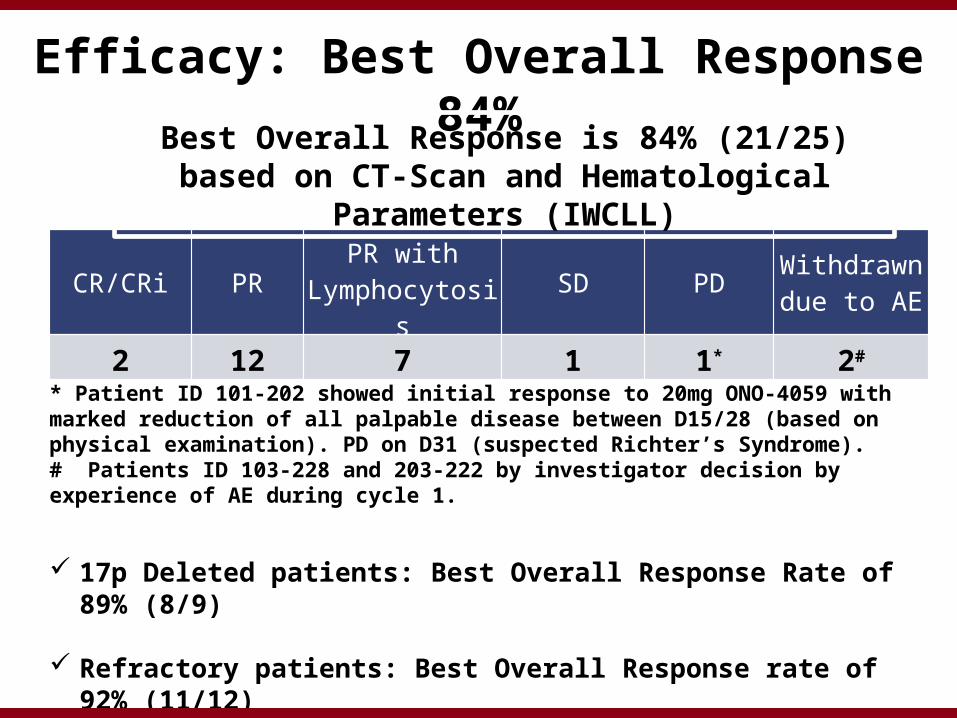
Efficacy: Best Overall Response 84%
CR/CRi PRPR with
Lymphocytosis SD PDWithdrawn due to AE
2 12 7 1 1* 2#
Best Overall Response is 84% (21/25) based on CT-Scan and Hematological Parameters (IWCLL)
17p Deleted patients: Best Overall Response Rate of 89% (8/9)
Refractory patients: Best Overall Response rate of 92% (11/12)
* Patient ID 101-202 showed initial response to 20mg ONO-4059 with marked reduction of all palpable disease between D15/28 (based on physical examination). PD on D31 (suspected Richter’s Syndrome).# Patients ID 103-228 and 203-222 by investigator decision by experience of AE during cycle 1.

Screen-ing
Cycle 1 Cycle 3 Cycle 7 Cycle 10 Cycle 13 Cycle 19-100%
-50%
0% 20mg
40mg
80mg
160mg
320mg
600mg
400mg
500mg
% C
ha
ng
e f
rom
Ba
se
lin
e S
PD
Treatment Cycles (1 Cycle = 28 Days)
Rapid Lymph Node Reduction Observed

Change in Tumor Burden
-100%
-50%
0%
Ma
x %
Ch
an
ge
in
Tu
mo
r B
urd
en
Patient with17p deletionPatient with11q deletion
Patient without 17p or 11q deletion2 patients have no efficacy data as they withdrew after cycle 1

Absolute Lymphocyte Count over Time
Scree
ning
Cycle
1 D
ay 1
Cycle
1 D
ay 2
Cycle
1 D
ay 8
Cycle
1 D
ay 1
5
Cycle
1 D
ay 2
8
Cycle
3
Cycle
4
Cycle
5
Cycle
6
Cycle
7
Cycle
8
Cycle
9
Cycle
10
Cycle
11
Cycle
12
Cycle
13
Cycle
14
Cycle
15
Cycle
16
Cycle
17
Cycle
18
Cycle
19
0
50
100
150
200
250
300
350
400
450
20mg
40mg
80mg
160mg
320mg
600mg
400mg
500mg
Ab
so
lute
Ly
mp
ho
cy
te C
ou
nt
(10
9/L
)
Treatment Cycles (1 Cycle = 28 Days)
Scree
ning
Cycle
1 D
ay 1
Cycle
1 D
ay 2
Cycle
1 D
ay 8
Cycle
1 D
ay 1
5
Cycle
1 D
ay 2
8
Cycle
3 D
ay 1
Cycle
4 D
ay 1
Cycle
5 D
ay 1
Cycle
6 D
ay 1
Cycle
7 D
ay 1
Cycle
8 D
ay 1
Cycle
9 D
ay 1
Cycle
10
Day 1
Cycle
11
Day 1
Cycle
12
Day 1
Cycle
13
Day 1
Cycle
14
Day 1
Cycle
15
Day 1
Cycle
16
Day 1
Cycle
17
Day 1
Cycle
18
Day 1
Cycle
19
Day 1
Cycle
20
Day 1
Cycle
21
Day 1
Cycle
22
Day 1
60.00
80.00
100.00
120.00
140.00
160.00
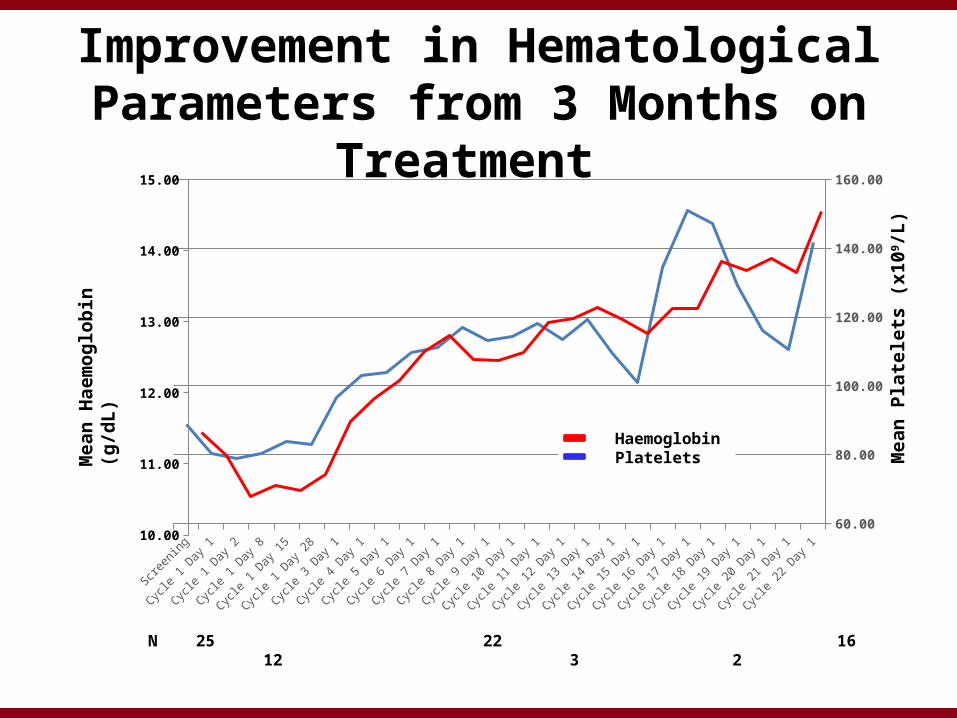
Improvement in Hematological Parameters from 3 Months on Treatment
Mea
n H
aem
og
lob
in (
g/d
L)
Mea
n P
late
lets
(x1
09/L
)
Haemoglobin Platelets
N 25 22 16 12 3 2
10.00
11.00
12.00
13.00
14.00
15.00

Durable Responses Observed with ONO-4059 (QD)
20mg
40mg
80mg
320mg
600mg
160mg
500mg
400mg
0 10 20 30 40 50 60 70 80 90
Duration of Treatment (Weeks)
Withdrawn due to PD
Withdrawn due to AE
Continuing ONO-4059 Treatment
Median duration of treatment is 11.5 cycles (min 1/max 22)

Conclusion• ONO-4059
– Was safe with mostly grade 1 and 2 AEs and no DLTs.
– Achieved sustained Btk inhibition at doses of ≥ 40mg and has a half-life of 5-7 hours.
– Showed good efficacy over a range of doses with a best overall response of 84% in phase I with 21/25 patients.
– Showed particularly good efficacy in refractory and in 17p Del patients.
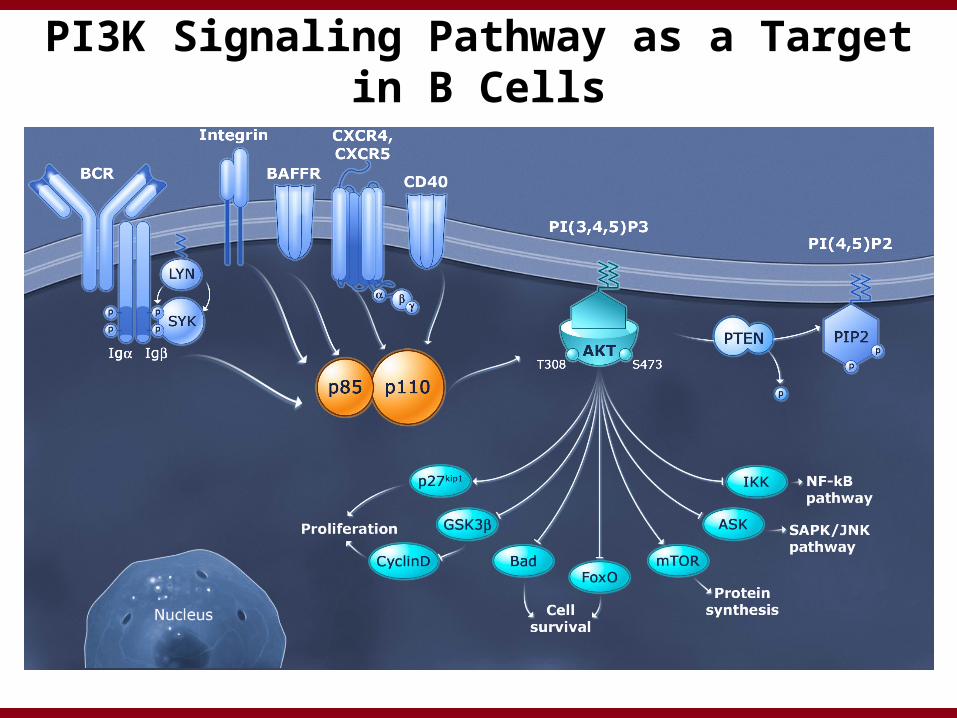
PI3K Signaling Pathway as a Target in B Cells

PI3K Delta: Target for B Cell Diseases
Tyrosine Phosphorylation
Class I PI3K Isoforms
Isoform Alpha Beta Delta Gamma
Expression Broad Broad Leukocytes Leukocytes
Gene KO effect on development Lethal Lethal Benign Benign
Primary physiological role
Insulin signalingAngiogenesis unknown
B-cell signaling, development & survival
Neutrophil &T-cell function

Phase 1 Trial of IPI-145 in Hematologic MalignanciesPreliminary Outcomes in CLL
Dose Escalation 8 mg BID 100 mg BID
MTD = 75 mg BIDCLL cohort 3
Tx Naïve 25 mg BIDn = 15
• R/R CLL (n=52) − Enrolled in dose-escalation and expansion cohorts (25 mg and 75 mg BID)
− Treatment Naïve CLL (n=15)− ≥ 65 years or 17p(del) / p53 mutation
• No restriction on cytopenias in CLL expansion cohorts− 40% ≥ Grade 3 cytopenias at baseline in R/R CLL
CLL cohort 1R/R ≤ 25 mg BID
n = 28
CLL cohort 2R/R 75 mg BID
n = 24
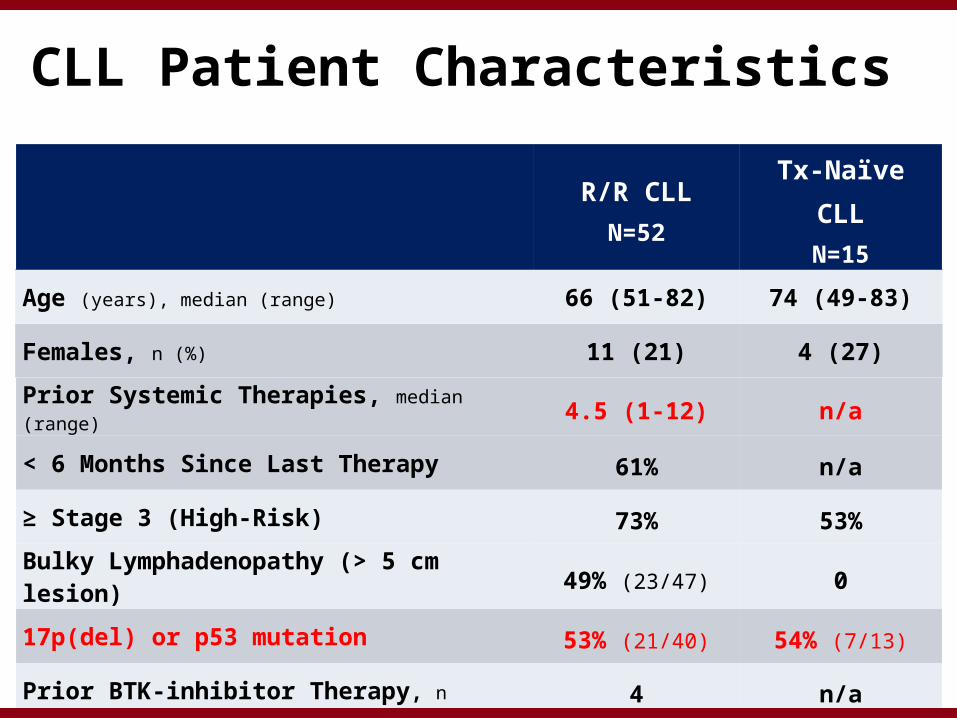
R/R CLL
N=52Tx-Naïve CLL
N=15
Age (years), median (range) 66 (51-82) 74 (49-83)
Females, n (%) 11 (21) 4 (27)
Prior Systemic Therapies, median (range) 4.5 (1-12) n/a
< 6 Months Since Last Therapy 61% n/a
≥ Stage 3 (High-Risk) 73% 53%
Bulky Lymphadenopathy (> 5 cm lesion) 49% (23/47) 0
17p(del) or p53 mutation 53% (21/40) 54% (7/13)
Prior BTK-inhibitor Therapy, n 4 n/a
CLL Patient Characteristics

AEs ≥ Grade 3 in CLL Patients (All Causality, ≥ 5%)IPI-145 at <=25 mg BID
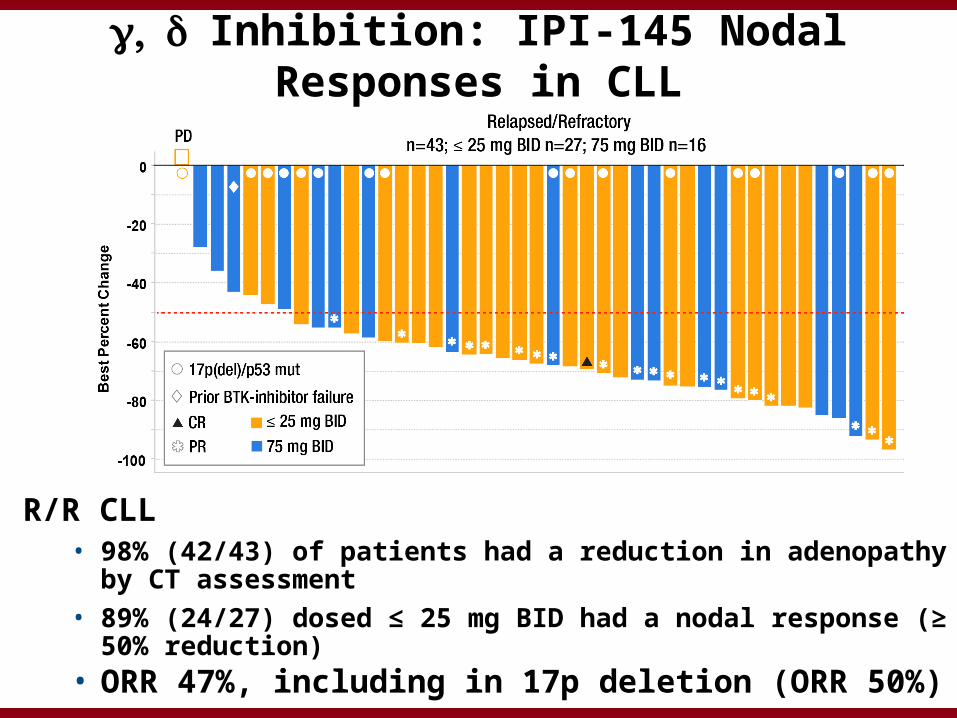
, g d Inhibition: IPI-145 Nodal Responses in CLL
R/R CLL• 98% (42/43) of patients had a reduction in adenopathy by CT
assessment • 89% (24/27) dosed ≤ 25 mg BID had a nodal response (≥ 50%
reduction)• ORR 47%, including in 17p deletion (ORR 50%)
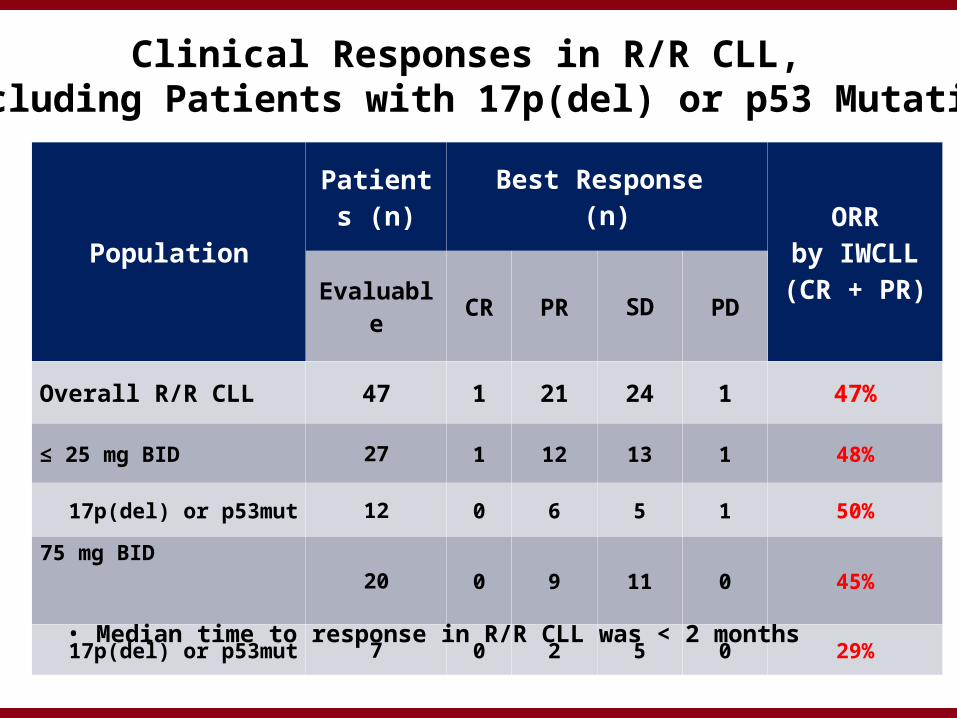
Population
Patients (n)
Best Response (n) ORR
by IWCLL(CR + PR)
Evaluable CR PR SD PD
Overall R/R CLL 47 1 21 24 1 47%
≤ 25 mg BID 27 1 12 13 1 48%
17p(del) or p53mut 12 0 6 5 1 50%
75 mg BID
20 0 9 11 0 45%
17p(del) or p53mut 7 0 2 5 0 29%
Clinical Responses in R/R CLL, Including Patients with 17p(del) or p53 Mutation
• Median time to response in R/R CLL was < 2 months

Time on Study: R/R CLL Patients Receiving ≤ 25 mg BID IPI-145
Long-term progression free
Recently enrolled, data maturing
Discontinued
Potential to optimize future patient management
• 75% (6/8) patients treated for ≥ 1 year remain progression-free on treatment
• 8 recently enrolled patients (< 6 months) in early follow-up for PFS

TGR-1202
Savona et al., ASH 2013
Second-generation PI3K-delta inhibitor in early clinical development

Preliminary Safety/Efficacy
Savona et al., ASH 2013
Definite, Probable or Possibly Related AEs (N=22)
Adverse Event, nGrade 1 & 2
(>5% of patients)Grade 3
(all events)
Diarrhea 4 -
Neutropenia - 1
Rash - 1
Thrombocytopenia - 1

BCR Pathway Inhibitors In Relapsed CLL
DRUG NNodal Resp
Rate of Incr ALC ORR PFS
LYN (?BTK)
Dasatinib 15 47% NR 20% TTF 6.7m
SYK Fostamatinib 11 55% 69% NR 6.4m
mTOR Everolimus 22 45% 36% 18% 5.1m
PI3K Delta: GS1101 55 83% 58% 39% (72%)
16 m (32 m)
Pan-PI3K: S08 10 60% 50% 40% NR
Gamma Delta: IPI-145
52* 98% 64-73% 47% Too early
BTK Ibrutinib: PCI-32765
85 88% 78% 71% 75% @ 26m
CC-292:AVL-292
64* 60% 55% 45% Too early
ONO-4059 25* 84% 67% (28%) Too early

Summary
• Great enthusiasm for additional BTK and PI3K inhibitors– How will they differentiate?
• BTK: –Greater specificity –? Alternative binding site to overcome
resistance• PI3K:
–Different isoform specificity • Other BCR targets: SYK, mTOR, LYN• Other targets: BCL2 et al.

Acknowledgments
DFCI BiostatisticsDonna NeubergLillian WernerHaesook Kim Kristen Stevenson
Brown Lab, DFCIBethany TesarStacey FernandesSasha VartanovReina ImprogoJosephine Klitgaard
NIH, NHGRICLL Research Consortium
Okonow-Lipton FundMelton Fund Rosenbach Fund
Lymphoma Program, DFCIArnold S FreedmanDavid C FisherAnn S LaCasceEric Jacobsen Philippe ArmandMatthew Davids
Clinical ResearchKaren FrancoeurKaren CampbellShannon MililloHazel Reynolds
Center for CancerGenome Discovery, DFCIMegan HannaLaura Macconaill
Ian Flinn; Stephan Stilgenbauer; Gilles Salles; Matthew Davids; David Johnson
Wu Lab, DFCICatherine WuDan-Avi LandauLili WangYouzhong Wan
Broad Institute Eric LanderGaddy GetzCarrie SougnezNir HacohenStacey GabrielMike LawrencePetar StojanovAndrey SivachenkoKristian CibulskisDavid Deluca