nhs northumberland clinical commissioning group - agenda...2019/09/25 · nhs northumberland...
TRANSCRIPT

OFFICIAL
1 20190925 UC GB Agenda
Governing Body
Clinicians commissioning healthcare for the people of Northumberland
This meeting will be held 10.00 on 25 September 2019 The Corn Exchange, Morpeth Town Hall, Morpeth NE61 1LZ
AGENDA
Time Item Topic Decision
required Enc PDF
Page Sponsor
1000 1 Welcome and apologies for absence G Syers
2 Declarations of conflicts of interest
G Syers
3 Quoracy*
G Syers
4 4.1 Minutes of the previous meetings (July & August 2019) and Matters Arising 4.2 Action Log
3
21
G Syers
1005 5 Accountable and Chief Operating Officers’ Report
M Adams/ S Brown
1010 6 Finance Update
22 J Connolly
1015 7 Clinical Management Board Report • Patient Impact Report
39 G Syers
1030 8 Rothbury Community Hospital Report
72 S Brown
1050 9 Strategic Items 9.1 Director of Public Health Update: - Health Inequalities in Northumberland - Director of Public Health Annual Report 2018 – Mental Wealth 9.2 Urgent Care – Design Principles
84
101
L Morgan S Brown

OFFICIAL
2 20190925 UC GB Agenda
Time Item Topic Decision required
Enc PDF Page
Sponsor
1120 10 Assurance, Risk and Governance 10.1 Annual Audit Letter 10.2 Assurance Framework & Risk Register 10.3 EPRR Core Standards Self Assessment 10.4 Workforce Race Equality Standard (WRES) Submission
137 158
197
214
J Connolly D Elliott D Elliott D Elliott
1140 11 Locality meeting assurance/key points S Brown 12 Governing Body Forward Plan
233 S Brown
13 Any other business (items submitted prior to meeting only)
G Syers
1145 14 Close of meeting
* 6 members, including at least two of the Lay Chair/Governors, the Clinical Director of Primary Care and two Locality Directors or three Locality Directors, either the Accountable Officer, Chief Operating Officer or the Chief Finance Officer.
1
Minutes of the Governing Body Wednesday 24 July at 11.00 The Function Room, Morpeth Golf Club, Morpeth NE61 2BT
Present Janet Guy Lay Chair (Chair) Siobhan Brown Chief Operating Officer Jon Connolly Chief Finance Officer Dr Graham Syers Clinical Director of Primary Care Karen Bower Lay Member Corporate Finance and Patient and Public
Involvement Steve Brazier Lay Member - Audit Chair Margaret Scott Governing Body Nurse Dr Paula Batsford Locality Director - Blyth Valley Dr John Warrington Locality Director - Central Tony Brown Locality Director – North (Managerial) In Attendance Vanessa Bainbridge Director of Place Based Development Elizabeth Morgan Director of Public Health Debra Elliott Head of Governance Melody Price Executive Assistant (Minutes) NCCGGB/19/75 Agenda Item 1 Apologies Apologies were received from Dr Ben Frankel, Dr Chris Waite, Prof. Marios Adamou and Mark Adams. NCCGGB/19/76 Agenda Item 2 Declarations of Conflicts of Interest Vanessa Bainbridge has a system wide focused role as Director of Place Based Development. She will declare any direct conflicts of interest related to specific agenda items at every Governing Body (GB) meeting when appropriate. NCCGGB/19/77 Agenda Item 3 Quoracy The meeting was quorate. NCCGGB/19/78 Agenda Item 4.1 Minutes of the previous meeting and Matters Arising The minutes of the Annual Public Meeting (26 June 2019) were agreed as a true and accurate record, pending the following amendment:
• Page 2, bullet point 2: Amend ‘county’ to ‘country’.

2
NCCGGB/19/79 Agenda Item 4.2 Action Log The action log was reviewed and the following update given: Action NCCGGB/19/69/02: Siobhan Brown to discuss with Annie Topping an update on E.Coli actions for the CMB Quality Exceptions report. Paula Batsford said fluid management guidance needed to be included as part of the E.Coli discussion with Annie Topping. NCCGGB/19/80 Agenda Item 5 Accountable and Chief Operating Officers’ Report Siobhan Brown provided an update on recent significant meetings and developments in the NHS Northumberland Clinical Commissioning Group (CCG). Northumbria Healthcare NHS Foundation Trust (NHCFT) launched the Joint Musculoskeletal and Pain Service (JMAPS) on 1 July 2019. The transition period from the providers’ previous physiotherapy service to the new model has attracted a large amount of patient and public feedback. As a consequence, the CCG working with the provider has retained services on 17 sites across the county and this includes the seven main NHCFT sites and 10 additional GP practice sites across the county. The Community Paramedic Service three month pilot in Berwick commenced on 1 July 2019. A full evaluation of its effectiveness will be undertaken to inform future commissioning decisions. The service will be fully integrated with the two primary care practices in Berwick and also Berwick Infirmary and local services. The national launch of Primary Care Networks (PCNs) took place on 1 July 2019. Northumberland has six PCNs ranging from a population size of 30,000 up to 80,000 plus. Special Measures and Legal Directions have been removed from the CCG as a result of the 2018/19 annual CCG rating of ‘Good’ from NHS England (NHSE)/NHS Improvement (NHSI), published on 11 July 2019. The result is a testament to the whole CCG team including the Lay Governors, Governing Body, clinical leaders and the CCG team delivering every day on the ground. Debra Elliott is leading a CCG governance review and refresh in Q2 2019. NHSE/NHSI published the NHS Long Term Plan (LTP) Implementation Framework on 5 July 2019. It contains guidance on the development of sustainability and transformation partnerships (STPs) and integrated care systems (ICSs) as they undertake strategic planning over the Summer. The first submission is due on 27 September 2019. Janet Guy thanked all CCG staff for their hard work which has led to the 2018/19 annual CCG assurance rating of ‘Good’ and the removal of Special Measures and Legal Directions. She especially acknowledged the work of Vanessa Bainbridge as the CCG’s previous Accountable Officer, Ian Cameron as the CCG’s previous Chief Finance Officer and Siobhan Brown. NCCGGB/19/81 Agenda Item 6 Finance Update Jon Connolly said the CCG’s Month 3 draft financial position for the period to 30 June 2019 had been reviewed in detail at the July 2019 Corporate Finance Committee (CFC) and assurance was received. The CFC recommended the Month 3 finance report to GB for consideration and comment. The CCG remains on target to deliver its financial plan.

3
Overall for the acute sector at Month 3, the main provider contract positions for NHCFT and Newcastle Hospitals NHS Foundation Trust (NUTHFT) have been forecast in line with plan until more 2019-20 data is received. Non NHS providers are showing a small £19k under spend. The data received to date for the Continuing Healthcare (CHC) partnership agreement with the local authority is in line with planning assumptions, and therefore reported in line with the budget agreed in the planning process. Prescribing data runs two months in arrears and therefore at the time of reporting there was one month’s worth of data available from the Business Services Authority (BSA). The forecast at Month 3 remains in line with plan. There is an expenditure risk on the Section 117 packages for the CCG in 2019/20 and the forecast has been increased in month to £0.5m over performance. The Out of Hours (OOH) contract was re-negotiated in 2018-19 and the revised contract value is being forecast at Month 3. This is lower than the planned budget and therefore the CCG is showing an under spend of £137k. Running cost budgets are showing an under spend of £556k at Month 3. There had been an increase in staffing part way through 2018/19 to help the CCG to meet its delivery targets as part of the financial recovery plan. Running costs will continue to be monitored closely. In Month 3, the CCG received the first non-recurrent tranche of the Children and Young People’s (CYP) trailblazer funding of £909k. NCCGGB/19/82 Agenda Item 7 Clinical Management Board Report Graham Syers highlighted the following Clinical Management Board (CMB) quality and performance exception reports:
• Access challenges due to month on month deterioration in waiting lists which increased by 820 in April 2019
• The variation in waiting list sizes and the CCG underperformance in April 2019 against the 18 week 92% threshold
• The continued deterioration of NUTHFT performance against the diagnostic six week performance threshold
• CCG and provider performance against the cancer two week wait and 62 day referral to treatment target. The CCG team is meeting with NUTHFT staff and Newcastle Gateshead and North Tyneside CCGs to agree system actions to improve performance
• The underperformance against the four hour Accident and Emergency target by the CCG and both local providers. Opening hours in Minor Injury Units (MIU) (Blyth and Alnwick) also continue to be challenging due to staffing issues. Karen Bower asked for an update on the impact of MIU recruitment. Siobhan said a meeting was being organised with NHCFT.
• Increasing Access to Psychological Therapies (IAPT) and Children and Young People’s Services’ performance remains strong. IAPT recovery rates are the strongest in the North East. However, CMB noted the future of IAPT services are clinically fragile and agreed that an exploration of future opportunities to reinforce clinical sustainability was required

4
• The incidence of E.Coli against the provider and CCG trajectories remains a concern; as do the recent CCG MRSA cases (two in April and one in May).
Steve Brazier asked if the increase in waiting lists size was due to the pension contributions taxation issue. Graham said it was having an impact on Outpatients appointments and surgery. Discussions are ongoing between the British Medical Association and the Department for Health. Siobhan Brown highlighted the detailed waiting lists report included in the quality and performance exception report. Tony Brown said cervical HPV screening tests are delayed and patients are being told to contact their GP practice for information. CMB were introduced to an integrated performance, quality and finance report that compares Northumberland, North Tyneside and Newcastle Gateshead CCGs with a view to a better understanding and closer working with each other in the Integrated Care Partnership (ICP). CMB received a process update regarding the Trailblazer project and a presentation from Dr Sam Bethapudi on behalf of Public Health England about Medical Champions. With regard to Trailblazers, Vanessa Bainbridge said the Educational Mental Health Practitioners will work within an early help and prevention framework as part of the Special Education Needs and Disability (SEND) graduated response, providing evidence based one to one interventions and group work to children and young people with low to moderate mental health issues. CMB asked for a piece of work to be undertaken by mid-September between the CCG and NHCFT to identify how to make Consultant Connect successful or find an alternative solution before it further funds the service. CMB considered the current position of Northumberland patients accessing elective care services in Scotland and agreed a new set of actions to (1) engage with the practices most affected by the patient pathways, (2) re-engage with NHS Lothian at the most senior level and from there (3) agree a favourable solution for patients. GB will then receive a paper for consideration and decision making, noting the high profile and sensitivities associated with these pathways. CMB received a presentation from Northumberland County Council’s (NCC) Public Health Team (PH) following results of a Health Needs Assessment (HNA) in Co-existing Mental Illness and Substance Misuse (CMISM). The HNA found several areas where there are opportunities to strengthen services for people with CMISM in Northumberland, either due to issues in pathways, the interface between services, misconceptions about CMISM or service user perceptions. The report makes recommendations in relation to communication and workforce, pathways and interventions and governance. CMB agreed to assist with implementation. Vanessa said misconceptions about abstinence are still an issue affecting clients accessing services. NCCGGB/19/83 Agenda Item 8 Quarterly Commissioning Plan Progress Update Siobhan Brown outlined the CCG’s progress in implementing its Commissioning Plan, specifically in relation to 2019/20 planning guidance national deliverables, local priorities and the related impact on the CCG Improvement and Assessment Framework (IAF) metrics.

5
A new dashboard has been developed for each of the programmes of work providing an ‘at a glance’ overview of the RAG status of each project and identifying delivery highlights and risks. 2019/20 Q1 successes:
• The mobilisation of the CCG’s newly procured JMAPS was completed and the contract signed by the provider. The service is operational from 1 July 2019. This will improve the RAG rating of this project from Amber to Green in Q2
• Good progress has been made in developing the strategic direction for Urgent Care. The CCG’s strategy document is now subject to a period of engagement with key stakeholders and an opportunity for public comment during Q2 before the next phase of the review
• The development of the six Primary Care Networks (PCNs) in Northumberland. Work to establish and develop clear plans for each PCN continues with CCG management support aligned to each network. The Northumberland System Transformation Board (STB) has recognised the importance of the PCNs and how existing provision needs to align as they emerge
• The CCG has met the national requirement to make Personal Health Budgets (PHB), the default option for Continuing Healthcare (CHC) home care packages from April 2019
• Good progress has been made with the Trailblazer project. Northumberland, Tyne and Wear NHS Foundation Trust (NTW) have appointed a Matron to oversee the 4-week wait work-stream and designated mental health leads in Schools have been identified across 28 schools.
Risks:
• Children’s commissioning staffing resource gap – this is now resulting in delays to key pieces of work, particularly with respect to SEND and developing a joint Framework for Children’s Continuing Care with NCC. A joint commissioning post to be established with NCC
• Avastin – continued lack of significant progress with this regionally-led project. No progress expected until October 2019 at the earliest. Quality, Innovation, Productivity and Prevention (QIPP) forecast has been reduced accordingly
• Gastro FIT Test - RAG status has moved from Green to Amber as despite strong uptake of the FIT test and expected deflection rates, there has not been a reciprocal reduction in secondary care activity. A task and finish group has been established to identify the issues and action required. QIPP forecast to be closely monitored
• MIU staffing issues. Karen Bower said the new dashboards were very helpful. She said the red RAG status data in the Project Delivery section of the Mental Health, Learning Disabilities and Children’s Programme Dashboard does not match the data in the 2019/20 Programme Overview section of the dashboard. Siobhan said it is incorrect and will be amended. Paula Batsford asked if a programme overview could be added to the Project Delivery Section of each dashboard. Action NCCGGB/19/83/01: Siobhan Brown to ensure programme overview information is added to the Project Delivery Section of each Operational Plan Programme Dashboard.

6
Liz Morgan asked for an update regarding Avastin. Jon Connolly said there continues to be a lack of significant progress with the regionally-led project as issues with the manufacture and packaging of Avastin persist, as do concerns from the Ophthalmic Consultants regarding the prescription of 'off-licence' drugs. Margaret Scott said the Tele-Dermatology Pilot RAG status has moved from Amber to Red and asked for an update. Siobhan said referral activity into the service was very low and it is clear the current model is not viable, so the pilot has been temporarily suspended. A period of engagement with GP practices will follow to understand the barriers which prevented wider use of the service. Dr Ben Frankel is leading on the project. NCCGGB/19/84 Agenda Item 9 Public Health Quarterly Update Liz Morgan provided an update on Public Health developments and issues at a local, regional or national level. Northumberland Suicide Prevention Strategy and Action Plan
Suicide remains a national and local public health priority. The patterns for deaths arising from suicide in Northumberland reflect the national pattern although the numbers are relatively small (but not the rates). However, the ‘years of life lost’ through suicide is higher than the national average which will reflect deaths in younger men. The Northumberland Suicide Prevention Strategy 2017-2022
and action plan is based on the
national strategy and action plan and on Public Health England (PHE) recommendations on local authority actions
to impact on suicide. It is augmented by regional and sub-regional
work supported by the Integrated care System (ICS) and the public health led regional Public Mental Health Network. The Northumberland Suicide Prevention Strategy required the development of a multi-agency suicide prevention group. It was agreed suicide prevention would be brought under the remit of the Crisis Care Concordat. Key areas of progress:
• The local response to sudden deaths • Supporting individuals with mental health issues leaving prison settings • Responding to national audits and reports • Mapping mental health and suicide training • Bereavement support - Identified that suicide specific bereavement support was ad
hoc. Trauma and post-intervention support have now been commissioned across the county, provided through Northumberland and North Tyneside MIND. Barnardo’s provide support for children and young people
• Social media and suicide Primary care has a crucial role to play in identifying people who could be at risk of suicide and ensuring they receive appropriate treatment and care. The Centre for Mental Health and the Samaritans
have undertaken a review of primary care in suicide prevention and identified a
number of improvement areas including emotional support for GPs, particularly following the death of a patient by suicide. Additional funding through the sub-regional suicide prevention group will have a tangible impact on the provision of post-intervention support, training and suicide surveillance. This is supported by more upstream public mental health activities such as the development of

7
emotional wellbeing and resilience in younger people, the Mental Health Trailblazer, and the development of a whole school approach to good mental health, starting with a supported network of school mental health leads. Adult smoking prevalence in Northumberland in 2018 Smoking has fallen to its lowest level on record in Northumberland, according to newly released 2018 figures published in Adult Smoking Habits in the UK: 2018 (Office of National Statistics). 12.1% of adults are now smoking compared with 17.6% in 2013, a fall of 5.5% over that time. This is the lowest smoking prevalence compared with our neighbouring local authority areas in the North East region and is statistically better than the England average of 14.4% of adults smoking. Smoking rates in some vulnerable groups, such as pregnant women and people from routine and manual occupations are not reducing as quickly. Results showed that routine and manual workers in England were more than twice as likely to be smokers as other occupations and in Northumberland three and a half times more likely. Smoking rates for these groups are reducing in Northumberland according to the Annual People Survey but reducing the gap between socioeconomic groups remains a challenge. Karen Bower asked for an update regarding the future commissioning of sexual health services. Liz said NHS LTP had proposed a ‘stronger role for the NHS’ in the commissioning of sexual health, health visiting and school nursing services. The Department of Health and Social Care has confirmed that key public health services will remain the responsibility of local authorities. NCCGGB/19/85 Agenda Item 10.1 Communications and Engagement Quarterly Report Siobhan Brown outlined the CCG’s communications and engagement quarterly activity report. NHCFT has signed a Service Level Agreement (SLA) with the CCG to provide communication and engagement services. A review of the CCG’s communications and engagement strategy will be undertaken. A refreshed strategy will be developed and implemented to increase awareness and understanding of the CCG, including its vision and values and leadership. Key priorities for the next quarter include improving engagement at practice and Patient Participation Group (PPG) level, plans to re-design the CCG’s website, and ensuring an appropriate level of engagement with stakeholders on the transformation of urgent care services. Karen Bower asked if public engagement was included when developing the JMAPS specification. Siobhan Brown said the CCG conducted a very thorough early period of engagement which included PPGs, practices and the public. The transition period from the provider’s previous physiotherapy service to the new model has attracted a large amount of patient and public feedback, and there are lessons to be learnt about the engagement process. Karen Bower asked if there is an option to sign up to CCG news alerts on the website. Action NCCGGB/19/85/01: Siobhan Brown to confirm if the option to sign up for CCG news alerts is available via the CCG’s website.

8
NCCGGB/19/86 Agenda Item 11.1 NHS England Assurance Letter The 2018/19 NHS England and NHS Improvement CCG annual assessment letter and Removal of Directions letters were received for information. NCCGGB/19/87 Agenda Item 11.2 CCG Complaints Annual Report 2018/19 Siobhan Brown outlined the North of England’s Commissioning Support Unit’s (NECS) complaints annual report 2018/19 which details the CCG’s performance and benchmarks it against other CCGs in the North East and North Cumbria. The complaints received are very much in line with other CCGs. The key themes across all CCGs are:
• Continuing Healthcare (CHC) funding decisions and processes • Individual Funding Request (IFR) process/decisions and Value Based Clinical
Commissioning Policy (VBCCP) and eligibility criteria • Access to patient transport • Commissioning decisions - most frequently raised subjects were access to some
medications on NHS prescription and provision of NHS wigs. The huge amount of time and work is dedicated to dealing with and learning from complaints is not reflected at all in the report. This was an observation made when the report was presented at CMB. Janet Guy said it is interesting to note that although Northumberland has the second biggest population out of the 11 CCGs in the North East and Cumbria, it received the eighth lowest number of formal complaints in 2018/19. NCCGGB/19/89 Agenda Item 12 Locality meeting assurance/key points
• 2018/19 Annual CCG rating from NHSE/NHSI and thanks to staff • Northumberland Suicide Prevention Strategy and Action Plan – Support for Primary
Care – offer of Director of Public Health visits to localities NCCGGB/19/90 Agenda Item 13 Governing Body Forward Plan
• September 2019 - Joint Targeted Area Inspection (JTAI) on Child Exploitation (Sexual and Criminal) Update.
NCCGGB/19/91 Agenda Item 14 Any other business No any other business. NCCGGB/19/92 Agenda Item 15 Date and time of next meeting Wednesday 28 August 2019 at 10.00 in Committee Room 2, County Hall, Morpeth.

1
Minutes of the Extraordinary Governing Body Wednesday 28 August at 10.00 Angus Armstrong Hall, Rothbury Jubilee Institute, Bridge Street, Rothbury NE65 7SD
Present Siobhan Brown Chief Operating Officer (Chair) Jon Connolly Chief Finance Officer Karen Bower Lay Member Corporate Finance and Patient and Public
Involvement Margaret Scott Governing Body Nurse Prof. Marios Adamou Governing Body Secondary Care Doctor Dr John Warrington Locality Director – Central Dr Ben Frankel Locality Director – West Dr Chris Waite Locality Director – North (Clinical) Tony Brown Locality Director – North (Managerial) In Attendance Helen Ray Chief Operating Officer, Northumbria Healthcare NHS
Foundation Trust Rachel Mitcheson Senior Head of Commissioning Elizabeth Morgan Director of Public Health, Northumberland County Council Debra Elliott Deputy Head of Governance Melody Price Executive Assistant (Minutes) Siobhan Brown welcomed members of the public to the NHS Northumberland Clinical Commissioning Group (CCG) Governing Body (GB) extraordinary meeting to consider a proposal by Northumbria Healthcare NHS Foundation Trust (NHCFT) regarding Rothbury Community Hospital. Siobhan said the CCG fully recognises this is an emotive issue for the local community but what has been long and sometimes difficult journey is now drawing towards a resolution. As Commissioners, the CCG needs to be satisfied that services are safe, effective, what people need, value for money and sustainable. There will be open and transparent discussion to enable GB members to make an informed recommendation on the proposal, whilst acknowledging the challenges and mitigations required to sustainably deliver the new model, embed it into the community, and staff the model consistently. GB will consider the PricewaterhouseCoopers (PwC) Independent Data Analysis, the Social Care and Continuing Healthcare Analysis, the Clinical Senate’s Independent Audit Report headlines. Helen Ray, Chief Operating Officer, NHCFT will present the proposal. Rachel Mitcheson, Senior Head of Commissioning, CCG will present the evidence that demonstrates the CCG has met its requirements from the Secretary of State for Health and Social Care, the

2
Independent Reconfiguration Panel (IPR) and Northumberland County Council’s (NCC) Health and Wellbeing Overview and Scrutiny Committee’s (HWB OSC) Rothbury Review Group. Councillor Steven Bridgett (Rothbury) will address GB before the decision. Katie Scott, Save Rothbury Hospital Campaign Group and Councillor Steven Bridgett who will speak on behalf of Councillor Trevor Thorne (Shilbottle) will address GB after the decision. Siobhan said a Chair for the meeting needs to be appointed. Debra Elliott said the CCG’s Constitution Standing Orders state that if both the Chair and Deputy Chair are absent, a member of GB shall be chosen by the members present, or by a majority of them, and shall preside. Debra asked for a nomination. Marios Adamou nominated Siobhan Brown. GB approved the nomination and Siobhan was confirmed as Chair. Introductions were made. NCCGGB/19/93 Agenda Item 1 Apologies Apologies were received from Janet Guy, Mark Adams, Dr Graham Syers, Dr Paula Batsford and Steve Brazier. NCCGGB/19/94 There were no declarations of interest. NCCGGB/19/95 Agenda Item 3 Quoracy The meeting was quorate. NCCGGB/19/96 Agenda Item 4.1 Rothbury Community Hospital Update Helen Ray gave a presentation on the ‘Art of the Possible’ proposal. Helen said the proposal is not the end of the journey but the beginning of the process. It is acknowledged the model of care might reshape over time due to population changes. A key principle of NHCFT is ‘Local first – as long as it is safe, sustainable and good quality’. Since the closure of the beds at Rothbury Community Hospital in September 2016, the local population, supported by the Save Rothbury Hospital Campaign Group and local Councillors, have been consistently clear that there is an ongoing need for a vibrant hospital at Rothbury, which includes inpatient beds. In response to the IRP report, the CCG and NHCFT have worked with the Rothbury Engagement Group (independently chaired) to relook at the model for the hospital considering the judgement of the IRP, the genuine challenges of care provision in this rurally isolated area, and co-designing a longer term solution. NHCFT has also been discussing and testing ideas for the ‘Art of the Possible’ with Save Rothbury Hospital Campaign Group members. Engagement with the campaign group, local parish councillors, county councillors, Healthwatch Northumberland, patient participation group members, a member of the National Community Hospital Association, and local clinicians identified potential gaps in provision for the population of Rothbury and Coquetdale as follows:

3
• Long term residential and nursing care - Limited local provision and limited likelihood of
this developing in the foreseeable future • End of life care - Good wrap around care into patients’ homes if end of life is
manageable for family and carers with appropriate home support. No local bed provision where end of life becomes difficult for family/carers and community teams to manage
• Rehabilitation - Services provided at other NHCFT community hospitals and into patients’ home depending upon level of input required. These services are currently stretched and sustainability is needed
• Respite - No structured respite support which may result in hospital attendance/admission for individuals. Respite is not traditionally commissioned by the NHS. More information and work needed
• Day care services - No structured coordination of provision although a number of services running in a variety of locations across the area. Enhancement to the voluntary services offer required.
The ‘Art of the Possible’
• Beds o Previous low occupancy rates. Some use of NHS funded beds for respite o Recent reviews support this and gives rise to challenges for the viability of bed
based services o However, rurality must be considered especially in light of palliative care and
distances for travel to alternative services • Potential solution
o Develop a model that is supported by community teams to ensure patients identified by clinical teams as needing specialist support that cannot be provided either at home or as part of enhanced day serviced, can access a bed at Rothbury
o Explore a more formal partnership approach with RAFA linked to short term respite using a funded/self-funded approach
o Partnership with Northumbria Primary Care (NPC) and NHCFT specialist teams to clinically support patients who require additional specialist care
• Making this happen o Partner discussions commenced (until to the end of September 19) o Staffing model (Sept/October 19) o Social care model for respite (July/August 19) o Job planning for consultant cover (commenced) o Job planning for virtual clinics (commenced) o Technology agreed (end of October 19)
• Other Services
o Opportunity to provide more services from Rothbury Community Hospital • Potential solution
o Dentistry service - ongoing discussions o Falls clinic - managed via visiting elderly care physician o Oncology/Chemo service o Mental Health services o Utilising the digital offer to reduce miles travelled through telecare for services
such as: T&O follow up clinics

4
Rheumatology Surgical follow up clinics Cardiology Community clinics Third sector clinics supported by Hospice
• Making this happen o Further clinical discussions required.
• Levels of support
o Own bed – people supported through current community services o Virtual Ward bed – people supported in their own bed, but with additional
nursing and carer support depending on need o Rothbury Community Hospital bed – people needing increased support not able
to be provided in the community as per agreed clinical criteria
• Criteria for admission: Palliative care, Step up care and Step down care
• New model of care o Dedicated team to cover both the virtual ward and Rothbury Community
Hospital o Flexible staffing model o Access only via Emergency Healthcare Plan (EHCP) – therefore patients are
known and planned for o Criteria for admission as specified o Out of hours nursing and medical cover provided through existing contracts
• Why should we do this?
o Potentially lead the way nationally regarding the provision of outstanding services within rural communities
o NHS Long Term Plan and the focus on out of hospital and local services – need to find the right balance for rural communities
o Population base has changed locally with further growth expected
• To be worked out o Confirmed staffing model o Contractual arrangements with partners o Finalised financial plan and business case
If the proposal is agreed, subject to HWB OSC, the CCG, NHCFT and local representatives will work together to prepare a plan of action and a business case that will be adopted by the CCG and NHCFT (with named partners) to ensure the funding is secured. This planning exercise will firm up a delivery date for commencement of the new model. It is anticipated that, with early agreement, most components of this model could be operational by April 2020 allowing for staff recruitment time and detailed planning. Siobhan thanked Helen for the presentation. Siobhan said GB needs to consider the impact of the proposal on the local and wider healthcare economy in Northumberland and be satisfied and assured before making a recommendation. She invited questions from GB.

5
Siobhan asked the following questions on behalf of Janet Guy, CCG Lay Chair: ‘Clearly a considerable amount of collaborative work has gone into analysing the issues and formulating the proposed new model of care. Why is this flexible bed model of care being proposed now and was not a potential solution three years ago? How will it ensure sustainability? Helen said since the closure of the beds at Rothbury Community Hospital, the local community have been consistently clear that there is an ongoing need for a hospital at Rothbury, which includes inpatient beds. In 2016, the inpatient beds at Rothbury were not clinically or financially sustainable and the model of care could not have been implemented. With the publication of the NHS Long Term Plan and the focus on out of hospital and local services, the time is now right. NHCFT’s vision is to support the development of a fully integrated rural health and social care service model for Coquetdale through a new and innovative partnership between health and care providers, the community, wider third sector and educational partners. It will deliver person-centred care in people’s homes and community with access to hospital beds for end of life support, short term rehabilitation for prevention of acute admission and transitioned support to independent living. Karen Bower asked how did NHCFT consult with the community in order to develop the proposed flexible model of care. Helen said NHCFT had worked with the Rothbury Engagement Group and into the community to identify potential gaps in provision of care and develop the proposal, as outlined in the presentation. If the proposal is approved, community engagement and involvement will continue and feed into the co-production of the model. Tony Brown asked how NHCFT will guarantee the North Northumberland Primary Care Network (PNC) will be involved in future discussions given that they have a responsibility for future population health, and community nurse teams will be wrapping around PCNs. Helen said NHCFT will be working closely with all PCNs and plans to use Rothbury as a ‘blueprint’ model for other rural communities in Northumberland. Tony said planned elements of the new model of care might not work. Helen said metrics will be in place to measure success including the patient/relative experience, travel, staff satisfaction, feedback from partners, and the use and effectiveness of technology. Marios Adamou asked about the requirements of the model and assurance that inpatient beds will be available. Helen said wrap round services are already in place. Inpatients beds will be available but the need for a bed will be defined by clinical need only. The actual number of beds required and staffing is a challenge. Chris Waite said the idea of a flexible bed model is very interesting. How will the flexible bed capacity at the hospital be wrapped around with support from the community and what are the challenges? Helen said only patients with an EHCP in place will have access to an inpatient bed, so patients are known and planned for. Clinicians have offered sessions at the hospital and The Rothbury Practice is keen to support the model. The community nursing team is currently considering the model. Consistency and assurance is needed and the challenge remains around getting the right staff. Chris said innovations in care are great when successful. Helen said Cumbria CCG has commissioned a similar model in Alston with positive outcomes for patients, staff and the wider community. Tony said there are already examples of innovation in care being tested and delivered in other areas of Northumberland such as the Catch model in Blyth and Alnwick. NHCFT need to draw on services to bring together the best ways of working and provide reassurance.

6
John Warrington asked if consultant geriatricians and palliative care consultants will have ‘hands on’ roles. Helen said the palliative care consultants will provide care in home and wrap around advice to the community teams. This is an extension to the current services provided. The fragility team have requested a peripatetic model with home visits and some clinical sessions at the hospital during the week. Ben Frankel said the ‘miles travelled’ metric is a very interesting and welcome for our system, given how rural the geography is. He asked for clarification as to how it would inform the local offer. Helen said the metric is currently being used in Berwick and based on patients’ postcodes that travel to Northumbria Specialist Emergency Care Hospital (NSECH) for emergency and planned care. The metric can be used to measure where patients and relatives have had to travel to since the beds were closed in Rothbury. Ben asked if it was being used for staff. Helen said it is not but it is an interesting suggestion to be considered. Liz Morgan said one of the roles of the CCG is to look at how best to meet the needs and health inequalities within our population. How are you going to evaluate this model for health inequalities due to the rurality of Rothbury and what does success look like? Helen said clinical model indicators for safety and quality will be in place. Patient and relative experience and value for money will be evaluated. Equality and Quality Impact Assessments of the new model will be fully developed to support the business case. Success will be a vibrant, well used community hospital by the end of the first year which delivers value for money. Jon Connolly said there was a balance between value for money and making sure communities get local services they need which might cost more. Helen said there may be possible compensating cost savings due to a reduction in patients going to NSECH. Margaret Scott asked if the staffing model will be available 24/7 and what the staff mix will be. Helen said staff will be available 24/7 to provide individualised care. The existing team which includes qualifies and unqualified staff will be enhanced. Rachel Mitcheson gave a presentation on how the CCG has met the requirements from the Secretary of State for Health and Social Care, the IPR and the HWB OSC Rothbury Review Group highlighting the following:
• CCG led engagement group – designed to understand the views from the local community, share key areas of work and involve community in decisions as a result
o Transport/travel assessment o Geographical assessment o Clinical audit
• NHCFT led – co-production group set up in partnership with key members of the campaign group to look at the ‘art of the possible’ and address the challenges. This group to continue.
• ‘Art of the possible created’ includes beds, flexible up and down, alongside other health and wellbeing services
• Introduction of a new metric – miles travelled • Introduction of a Northumberland Rural Health Commissioning – guide for the future • CCG and NHCFT Board support – funding agreed
Councillor Steven Bridgett thanked GB for the opportunity to speak at the meeting and addressed GB on behalf of Rothbury residents. A full transcript of the address is in Appendix 1.

7
NCCGGB/19/98 Agenda Item 4.2 Questions from the public There were no pre submitted questions from the public. NCCGGB/19/99 Agenda Item 4.3 Recommendation for approval by Governing Body Members Siobhan said the proposal provides an exciting opportunity to develop of a fully integrated rural health and social care service model for Coquetdale, which includes inpatient beds, through a new and innovative partnership between health and care providers, the community and wider third sector and educational partners. There has been thorough explanation of the proposal acknowledging the challenges and potential risks. Given the level of innovation and risk in the new model, if the model is recommended for approval, the CCG has asked the Northern England Clinical Senate if it will advise the CCG and NHCFT during the development and mobilisation phase of the model. The Northern England Clinical Senate has agreed to this work. Equality and Quality Impact Assessments of the new model will be fully developed. Success will be a vibrant, well used community hospital by the end of the first year which delivers value for money and sustainable. The evidence presented demonstrates the CCG has met its requirements from the Secretary of State for Health and Social Care, the IPR and the HWB OSC Rothbury Review Group has been considered. Siobhan asked GB for a decision regarding the recommendation for approval of NHCFT’s Rothbury proposal. Decision NCCGGB/19/99/01: GB unanimously recommended NHCFT’s Rothbury proposal for approval subject to:
• HWB OSC’s consideration of the proposal and its sign off that the CCG and wider system has met all requirements related to the process
• Decision from HWB OSC on whether the proposal constitutes a substantial change that requires consultation or is not considered a substantial change
• Agreement for the Clinical Senate to work alongside NHCFT during the mobilisation phase to independently advise on the sustainability of the model for the future including staffing; and the contracting, performance and quality metrics required for successful delivery of the model
• Fully developed Equality and Quality Impact Assessments of the new model. Siobhan said the recommendation from today’s meeting will be considered by HWB OSC at a meeting held in public on 3 September 2019. Subject to the outcome of the meeting, formal approval of the proposal will take place at the September 2019 GB meeting to be held in public on Wednesday 25 September 2019 at 10.00 in Corn Exchange, Morpeth Town Hall, Morpeth.

8
Councillor Steven Bridgett addressed GB on behalf of Councillor Trevor Thorne. A full transcript of the address is in Appendix 2. Katie Scott thanked GB for the opportunity to speak at the meeting and addressed GB on behalf of the Save Rothbury Hospital Campaign Group. A full transcript of the address is in Appendix 3. NCCGGB/19/100 Agenda Item 5 Any other business No any other business. NCCGGB/19/101 Agenda Item 6 Date and time of next meeting Wednesday 25 September 2019 at 10.00 in Corn Exchange, Morpeth Town Hall, Morpeth. NCCGGB/19/102 Agenda Item 7 Formal close of the meeting Siobhan thanked everybody for their attendance and closed the meeting. Appendix 1: Full transcript of the address by Councillor Steven Bridgett. Appendix 2: Full transcript of the address by Councillor Steven Bridgett on behalf of Councillor Trevor Thorne. Appendix 3: Full transcript of the address by Katie Scott, Save Rothbury Hospital Campaign Group.

9
Appendix 1: Full transcript of the address by Councillor Steven Bridgett. Awaiting copy of transcript. Appendix 2: Full transcript of the address by Councillor Steven Bridgett on behalf of Councillor Trevor Thorne. Awaiting copy of transcript. Appendix 3 Katie Scott, Save Rothbury Hospital Campaign Group - CCG Governing Body 28.8.19 As you know, almost exactly three years ago our community hospital inpatient ward was closed. It was agreed by all that the consultation run by the CCG to keep it closed was faulty and that the decision to take away our 12 beds was certainly not in the best interests of the health of the people in North Northumberland. The Campaign Team, and other members of the community, such as the Upper Coquetdale Churches, The Coquetdale League of Friends, Over the Bridges, local councillors, and WI groups, plus many more, have worked tirelessly to fight back against this callous and wrong decision. Over the 3 years, the Team has had up to 18 people helping with different parts of the Campaign. We have critiqued the CCG’s papers and we have proposed a different vision. In April 2017 we produced our Coquetdale Cares – The Community’s Vision. This, we argued, would be ideal for the people of Coquetdale and beyond for the foreseeable future. On 17th October 2017, at Northumberland County Council’s Scrutiny Committee Meeting, We said - and I quote: ‘Look, we have a fabulous opportunity now to make a fully integrated facility in our wonderful hospital building, with a GP surgery, step up and step down beds, palliative care, and the continuation and development of the existing clinics. We are therefore greatly pleased to hear about the plans for the amazing range of different services and clinics that are being planned to take place in our hospital. These are fantastic and we applaud the work that has gone into ensuring these. We believe that the proposals we have heard today go a long way towards meeting our Vision. We are so pleased that the Trust and the CCG are working together, and including the Community. Our thanks go to them for this. And we understand, of course we do, that there have had to be compromises on all sides. But the Campaign came about because of the closure of our ward, and, I promise, members of the Campaign Team will continue to actively monitor the hospital to ensure that beds actually are being made available, when there is a clinical need. But the new flexible bed model is really innovative and exciting. We definitely believe it can succeed for our community’s needs.

10
We promise to work wholeheartedly with the Trust and CCG to make the Art of the Possible work for us all. So, at this point, sincere and heartfelt thanks need to be made – to you - wonderful people, our community, who have backed the Campaign all the way, and believed in us, and our optimism. Thank you for all who have told us their stories, of how beneficial a stay in the former hospital ward was, and of how they wish they, or their loved ones, had been able to be there while it has been closed. A personal Thanks must go to the most wonderful, sensitive, intelligent bunch of people I know, who make up the Campaign Team. I applaud you all. But a most specific and profound appreciation goes to my wise and tenacious friend, Maurice Cole. We could not have done without his acumen and doggedness. I call him Maurice the Magnificent. Thank you to everyone. Katie Scott Co-ordinator Save Rothbury Community Hospital Campaign

OFFICIAL
NCCGGB/19/83/01 25/09/2018 24/07/2019
Siobhan Brown to ensure programme overview information is added to the Project Delivery Section of each Operational Plan Programme Dashboard. Siobhan Brown
Complete
NCCGGB/19/85/01 25/09/2018 24/07/2019
Siobhan Brown to confirm if the option to sign up for CCG news alerts is available via the CCG’s website. Siobhan Brown
CompleteTo be considered as part of the current CCG website redeveloped.
Description and Comments Owner Status CommentNumber Date Identified
Target Completion
Date
Governing Body DATE: September 2019
NHS Northumberland Clinical Commissioning Group Agenda Item 4.2Governing Body - REGISTER OF ACTIONSLog owner: Governing Body Chair

Agenda Item 6
OFFICIAL
1 20190925 UC Agenda Item 6 Finance Update Month 5
Clinicians commissioning healthcare for the people of Northumberland
Meeting title Governing Body
Date 25 September 2019
Agenda item 6
Report title Finance Update – Month 5
Report author Chief Finance Officer
Sponsor Chief Finance Officer
Private or Public agenda
Public
NHS classification Official
Purpose
Information only
Development/Discussion
Decision/Action
Links to Corporate Objectives Ensure that the CCG makes best use of all available resources
Ensure the delivery of safe, high quality services that deliver the best outcomes
Create joined up pathways within and across organisations to deliver seamless care
Deliver clinically led health services that are focused on individual and wider population needs and based on evidence.
Northumberland CCG/external meetings this paper has been discussed at:
None
QIPP Overall QIPP Programme delivery Risks Strategic Risk 946 – Financial Balance
Operational Risk 1799 – QIPP Resource implications N/A Consultation/engagement N/A

OFFICIAL
20190925 UC Agenda Item 6 Finance Update Month 5 2
Quality and Equality impact assessment
Complete report (pages 3 & 4).
Data Protection Impact Assessment
No
Research N/A Legal implications CCG Statutory Financial Duties Impact on carers N/A Sustainability implications N/A

OFFICIAL
20190925 UC Agenda Item 6 Finance Update Month 5 3
QUALITY and EQUALITY IMPACT ASSESSMENT 1. Project Name Finance Update – Month 5
2. Project Lead Director Lead Project Lead Clinical Lead Chief Finance Officer
3. Project Overview & Objective
Finance Update – Month 5
4. Quality Impact Assessment
Impact Details Pos/ Neg
C L Scores
Mitigation / Control
Patient Safety N/A Clinical Effectiveness N/A Patient Experience N/A Others including reputation, information governance and etc.
5.Equality Impact Assessment
Impact Details Pos/ Neg
C L Scores
Mitigation / Control
What is the impact on people who have one of the protected characteristics as defined in the Equality Act 2010?
N/A
What is the impact on health inequalities in terms of access to services and outcomes achieved for the population of Northumberland? (which is in line with the legal duties defined in the National Health Service Act 2006 as amended by the Health and Social Care Act 2012), for example health inequalities due to differences in socioeconomic circumstances?
N/A
6. Research Reference to relevant local and national research as appropriate.
N/A
7. Metrics Sensitive to the impacts or risks on quality and equality and can be used for
Impact Descriptors Baseline Metrics Target
OFFICIAL
20190925 UC Agenda Item 6 Finance Update Month 5 4
ongoing monitoring. 8. Completed By Signature Printed
Name Date
Chief Finance Officer
Jon Connolly
J Connolly
12/09/2019
Additional Relevant Information:
8. Clinical Lead Approval by Signature Printed Name
Date
Additional Relevant Information:
9. Reviewed By Signature Printed Name
Date
Comments

OFFICIAL
20190925 UC Agenda Item 6 Finance Update Month 5 5
Governing Body 25 September 2019 Agenda Item: 6 Finance Update – Month 5 Sponsor: Chief Finance Officer
Members of the Governance Body are asked to: 1. Consider NHS Northumberland Clinical Commissioning Group’s draft financial
position as at 31 August 2019 and provide comment. 2. Consider the forecast outturn and key risks to delivery and provide comment.
Purpose
This report presents the draft financial position for the period to 31 August 2019. The appendices show this position broken down across the relevant areas of expenditure. Background
NHS Northumberland Clinical Commissioning Group (CCG) has a control total deficit of £4m for the financial year 2019-20. As with the previous financial year, if the CCG can demonstrate that it is on track to achieve the control total it will qualify for an additional non-recurrent allocation of £4m Commissioner Sustainability Funding (CSF) in 2019-20. This will enable the CCG to report an in-year breakeven position for 2019-20. By achieving breakeven, the CCG will maintain the same level of historic debt that it started the financial year with of £57.6m. Appendix 1-5 are designed to be in line with the national reporting requirements categories used in the financial planning submissions to NHS England (NHSE) and reporting requirements through the monthly non ISFE returns and annual accounts process. Appendix 6 shows the CCG level performance for primary medical (GP) care commissioning in more detail. Financial Position Overview Appendix 1 (Income and Expenditure (I&E)) shows the financial performance of the CCG for the financial year to 31 August 2019. The ‘in year’ resource allocation is shown in the top section split between Programme, Delegated Primary Care Commissioning and Running costs allocations excluding the brought forward cumulative historic deficit (£57.6m). The middle I&E section then shows the net expenditure and budget variances as at Month 5 (£3.6m deficit forecast outturn). The bottom section in grey adjusts for the CSF allocation received to date

OFFICIAL
20190925 UC Agenda Item 6 Finance Update Month 5 6
(£0.4m) and expected (£3.6m), and shows the ‘in year’ and cumulative deficit positions forecast for the year ending 31 March 2020 (Breakeven and £57.6m respectively). Appendix 2 (Allocations) shows the total confirmed 2019-20 allocation as at 31 August 2019 of £548.8m. The allocation table in appendix 2 shows the allocation information for each allocation received by the CCG in year, who is the commissioning lead, and where required, whether the funding has been approved by board to be committed.
August 2019 (M5) Allocations £000’s Armed forces CCG OOH Allocation 8 Total Allocations received in month 8
In August 2019, the CCG received £8k in non-recurrent allocations; this allocation is for out of hours (OOH) work with armed forces patients and available to be bid for by the OOH service providers. Financial Position Detail The CCG shows the individual budget line positions on Appendix 1 net of its Quality, Innovation, Productivity and Prevention (QIPP) target. The following positions for Month 5 show the variance against these lines reflecting expected QIPP delivery achieved in 2019-20. Acute The CCG uses the latest data available in the Service Level Agreement Monitoring (SLAM) model (Month 4 flex) to show the most up to date and accurate position for its main providers. Overall for the acute sector at Month 5, the CCG has reported as an over spend of £969k. This is mainly to do with over performance in the Northumbria Healthcare NHS Foundation Trust (NHCFT) contract (£998k) for high cost drugs costs growing at a higher rate than planned for this year and some of the initial efficiency schemes not delivering as much as planned at this stage of the year. In the CCGs other main acute services contract with Newcastle Hospitals NHS Foundation Trust (NUTHFT) the position has been reported in line with plan, with most of planned care delivery being within planning assumptions made. The main ambulance contract with North East Ambulance Service NHS Foundation Trust (NEAS) is mainly a block payment arrangement; however there is now additional non recurrent investment reported in the forecast at month 5 for community paramedics that results in reporting an over spend against original plan of £39k. In the smaller acute contracts and non-recurrent lines, NHS providers are reporting a small over spend of £108k offset with an under spend in non-contracted activity (NCA’s) of £30k and non NHS acute providers of £146k.

OFFICIAL
20190925 UC Agenda Item 6 Finance Update Month 5 7
Mental Health Overall the CCG is reporting a £1m over spend against mental health budgets and there has been no movement in this forecast from the previous month. Section 117 packages of care continue to represent an expenditure risk to the CCG in 2019-20. The forecast over performance of £0.5m against the planned budget reflects the increased level of cost the CCG is seeing in month 5 data from the local authority. In the other mental health services line, there is a further £0.5m over spend reported in month 5, this is additional non recurrent expenditure incurred and forecast for temporary placement costs for learning disability patients. Also included within mental Health and currently reported to plan is the CCGs main Mental Health contract is with Northumberland, Tyne and Wear NHS Foundation Trust (NTW). This contract is a block contract and will be reported to the agreed contract value throughout the year pending any contract variations. There are also two other block contracts included under mental health that will also continue to be shown as breakeven throughout the year also pending any contract variations. They are the Talking Matters Northumberland (TMN) IAPT contract and the Mental Health Pool contract with the local authority. Community Services Overall in Community Services the CCG is forecasting a small under performance of £68k. Under the community services heading the CCG reports its main community block contract with NHCFT, there is a smaller community contract with NUTHFT, and a budget for continence products also with NHCFT in the other community contracts NHS line that is forecasting a £83k underspend. The non NHS community line includes the Joint Equipment Loan Service (JELS) block contract and smaller contracts with the Local Authority and St Oswald’s for Palliative care. All of these lines are reported breakeven at month 5 due to either being block contracts or where there is not enough data received at the stage to change the forecast from plan, with the exception of short break care St Oswald’s showing an over spend of £14k. Continuing Healthcare The data received to date for the main Continuing Healthcare (CHC) contract with the local authority at Month 5 is in line with planning assumptions. CHC is therefore reported in line with the budget agreed in the planning process. Other CHC spend includes children’s CHC package contributions and recharges from the Local Authority, Nurse Assessor payments to NHCFT and additional recharges for CHC clients outside of the main contract charge. These are also reported breakeven at Month 5 until more data is analysed in year.

OFFICIAL
20190925 UC Agenda Item 6 Finance Update Month 5 8
Prescribing and CCG funded Primary Care services Prescribing data runs two months in arrears and therefore at the time of reporting there was two month’s worth of data available from the Business Services Authority (BSA) for reporting variances in the Month 5 position. The Business Services Authority (BSA) does not provide a forecast until part way through the year to ensure volatility in early monthly prescribing evens out before the forecast is released. However, the CCG can still forecast based on the available data locally which incorporates previous years profiling and dispensing days. A national announcement on an expected increase in Category M drug prices from August data (nationally 15m a month increase) has now been included in the I&E position, the impact is expected to be in the region of £0.1m a month for the CCG and therefore the Month 5 position reflects this pressure reporting a £864k over spend. The Out of Hours contract was re-negotiated in 2018-19 and the revised contract value is being forecast at Month 5. This is lower than the planned budget and therefore the CCG is showing an under spend of £137k contributing towards in year efficiency. Commissioning schemes contain the CCG’s local enhanced services and are reported breakeven at Month 5, this forecast is reported breakeven until the annual projections on the level of achievement/participation of each of the individual schemes by each practice is determined later in the financial year. GPFV contains the allocation for extended access that is now part of the CCG recurrent baseline and is reported breakeven at Month 5. As in 2018-19 Online consultation and GP clerical training will also be reported under GPFV in future months once the non-recurrent in year allocations have been received. Primary Care Networks funding is new for 2019-20 and is expected to be fully committed in the setup of the new primary care hubs. Primary care dressings are showing an over-spend at Month 5 of £119k, further work is underway to understand the increase from the initial data received for 2019-20. Finally, the Other Primary Care line is made up of GPIT, Oxygen and the medicines management element of the NECS contract. Oxygen forecast as £58k under spend. Primary Care Commissioning The delegated primary care budgets are under more pressure than they have been in previous years with the increase in cost relating to national GP contract uplifts, increasing at a percentage of growth above the annual growth applied to the ring fenced primary care commissioning allocation. At this stage of the year, the CCG expects that this cost pressure

OFFICIAL
20190925 UC Agenda Item 6 Finance Update Month 5 9
can be managed in 2019-20 and for Month 5 the Delegated Primary care commissioning budgets are reported breakeven. The Primary Care Commissioning budgets are looked at further and in more detail at the CCGs Primary Care Operational Group (PCOG) and the Primary Care Commissioning Committee (PCCC). Other Programme Services The core Better Care Fund (BCF) social care payment the CCG makes to the local authority is an amount included by NHSE in the CCG’s baseline and is a block arrangement paid in twelfths. The 111 Contract has been agreed as part of the overall NEAS contract negotiations and is also a block contract paid in twelfths. Also included within the other services line are smaller contracts for Voluntary sector, expenditure for ad hoc private transport and expenditure for exceptional treatments. Collectively there is an overspend against the budget set of £168k at Month 5, that is mainly coming from additional expenditure and investment with NEAS for Renal transport and Additional discharge vehicles to help with the pressure at Northumbria Specialist Emergency Care Hospital (NSECH). Running costs Running cost budgets are reported as a £411k under spend at month 5. This is made up of a number of components including the release of admin reserves budget of 256k, current vacancy factor and whole time variances differences in staffing budgets (part time working) of 368k (including clinical sessions and NECS support). These are offset with a pressure of 213k against non-pay budgets which in the main is an increase in void costs for vacant property space, IT investment and Professional fees. Activity overview As mentioned above under acute, there is Month 4 flex data available for reporting activity variances this month. The CCG was able to set a robust activity plan with NHCFT and NUTH for 2019-20 and in the early data received the CCG can report that there are no significant over performance issues against activity plans set for 2019-20 that affect the CCGs financial position. The CCG is confident that activity variances should continue to be less material than seen in previous years due to a more joint up system planning approach with the main local providers during the contract alignment / agreement process for 2019-20. The introduction of the emergency care blended tariff in 2019-20 reduces the CCGs risk to emergency care over performance by applying a marginal rate of 80% to activity over plan (CCG only pays 20% of tariff on over performance).
OFFICIAL
20190925 UC Agenda Item 6 Finance Update Month 5 10
The blended tariff arrangement provides more certainty in forecasting annual outturns for the CCG and reduces volatility in reporting for 2019-20 with the blended tariff covering 46% of the contract value in NHCFT and 20% in NUTH. Underlying Position The CCG also reports on its underlying position each month to NHSE. The underlying position of the CCG is the recurrent position after any non-recurrent expenditure and allocations are removed and adjustments are made for impacts of part year effects that will then go on to be full year values in future years. At Month 5, the CCG is reporting that it will achieve its planned underlying position of breakeven. Statement of Financial Position and Cashflow Forecast Appendix 3 (Statement of Financial Position (SoFP)) shows the closing positions at the end of August 2019 in comparison to the last reported month. There have been minimal movements in the SoFP this month with small increases of £0.1m in both Debtors and Creditors leaving the net movement to the overall net current assets being mainly from the CCG carrying a lower cash balance in August than in the previous month. Appendix 5 (Cashflow forecast), the CCG is expected by NHSE to proactively manage the cash it draws down each month and the amount it actually spends. The target is to have no more than 1.25% of the monthly drawdown of cash left in the main bank account each month. The cash balance at the end of August 2019 was £0.27m which equates to 0.64% of the July drawdown, and meets the target level. Better Payment Practice Code for year to 31 August 2019 Appendix 4 (Better Payment Practice Code) requires that all valid invoices should be paid by their due date or within 30 days of receipt, whichever is later. The CCG is measured against a target of 95% achievement.
The CCGs cumulative value of NHS invoices paid within 30 days at 31 August was 99.83% as a percentage of invoice value and 99.69% by invoice count. The cumulative value of Non NHS invoices paid within 30 days at 31 August was 99.64% as a percentage of invoice value and 98.27% by invoice count. Recommendation CFC is asked to consider the financial position as at 31 August 2019 and the key risks to delivery and provide comment.

OFFICIAL
20190925 UC Agenda Item 6 Finance Update Month 5 11
Appendix 1: Income and expenditure report YTD and FOT Appendix 2: Allocation breakdown Appendix 3: Statement of financial position Appendix 4: Better payment practice code Appendix 5: Cash flow forecast Appendix 6: Primary care commissioning expenditure

APPENDIX 1
YTD Budget YTD Actual
YTD Variance (Under)/
Overspend
YTD Variance (Under)/
Overspend Annual BudgetForecast Outturn
Forecast Variance (Under)/
Overspend
Forecast Variance (Under)/
Overspend£000's £000's £000's % £000's £000's £000's %
Resource
Programme Baseline 204,795 204,795 0 495,816 495,816 0Primary Care Co-commissioning Baseline 19,432 19,432 0 46,063 46,063 0Running Costs Baseline 2,631 2,631 0 6,966 6,966 0In Year Allocation 226,858 226,858 0 548,845 548,845 0
Expenditure
Acute ServicesNorthumbria Healthcare NHS FT 81,167 81,582 416 0.51% 194,800 195,798 998 0.51%Newcastle Upon Tyne Hospitals NHS FT 27,577 27,577 0 0.00% 66,184 66,184 0 0.00%North East Ambulance Service 6,303 6,319 16 0.26% 15,127 15,165 39 0.26%Acute Contracts NHS 1,510 1,555 45 2.98% 3,624 3,732 108 2.98%Acute Contracts Non NHS 3,426 3,365 -61 -1.78% 8,223 8,077 -146 -1.78%Other Acute NCA 997 985 -12 -1.24% 2,394 2,364 -30 -1.24%Other Acute Non Rec 212 212 0 0.01% 509 509 0 0.00%Total acute services 121,192 121,595 404 290,860 291,829 969
Core Mental Health servicesNorthumberland Tyne & Wear NHS Foundation Trust 18,016 18,016 0 0.00% 43,239 43,239 0 0.00%Section 117's (LA) 3,099 3,307 208 6.72% 7,437 7,937 500 6.72%Talking Matters Northumberland 1,773 1,773 0 0.00% 4,254 4,254 0 0.00%Mental Health Pooled budget (LA) 1,124 1,124 0 0.00% 2,698 2,698 0 0.00%Mental Health Other services 966 1,178 212 21.90% 2,319 2,826 508 21.89%Total Core Mental Health 24,978 25,398 420 59,947 60,955 1,008
Community ServicesNorthumbria Healthcare NHS FT (Comm) 12,438 12,438 0 0.00% 29,851 29,851 0 0.00%Newcastle Upon Tyne Hospitals NHS FT (Comm) 117 117 0 0.00% 282 282 0 0.00%Other Community Contracts NHS 328 294 -35 -10.52% 787 705 -83 -10.52%Community Contracts Non NHS 765 771 6 0.78% 1,836 1,850 14 0.78%Total Community Services 13,648 13,620 -29 32,756 32,688 -68
Continuing HealthcareContinuing Healthcare Main contract 14,458 14,458 0 0.00% 34,700 34,700 0 0.00%Other Continuing Healthcare 973 973 0 0.00% 2,335 2,335 0 0.00%Total Continuing Healthcare 15,431 15,431 0 37,035 37,035 0
Prescribing and CCG Funded Primary Care ServicesPrescribing 22,270 22,670 400 1.79% 53,448 54,312 864 1.62%Out of Hours 966 909 -57 -5.92% 2,319 2,182 -137 -5.92%Commissioning Schemes 1,037 995 -42 -4.06% 2,490 2,490 0 0.01%GP Forward View 810 810 0 0.00% 1,943 1,943 0 0.00%Practice Transformation support 203 203 0 0.00% 488 488 0 0.00%Primary Care Dressings 691 741 50 7.18% 1,659 1,778 119 7.18%Other Primary Care 615 593 -22 -3.51% 1,476 1,418 -58 -3.93%Total Prescribing and CCG Funded Primary Care Services 26,593 26,921 328 63,823 64,610 788 152
Primary Care Commissioning (appendix 6) 19,432 19,432 0 0.00% 46,063 46,063 0 0.00%
Other Programme ServicesCore BCF (Social Care) 3,152 3,152 0 0.00% 7,564 7,564 0 0.00%111 contract 546 546 0 0.00% 1,310 1,310 0 0.00%Other Services (inc. PTS & IFR) 411 481 70 17.03% 987 1,156 168 17.03%Total Other Programme Services 4,109 4,179 70 9,861 10,029 168
Commissioning Reserves & ContingencyGeneral Reserve 0 0 0 0.00% 2,132 2,132 0 0.00%Non Recurrent Allocations 111 -911 -1,022 0.00% 266 -2,187 -2,453 0.00%Contingency 0 0 0 0.00% 2,737 2,737 0 0.00%Total Commissioning Reserves 111 -911 -1,022 5,135 2,681 -2,453
Planned Deficit Control Total -1,667 0 1,667 -4,000 0 4,000
Total Commissioned Services 223,826 225,664 1,838 541,479 545,890 4,411
Running Costs 2,631 2,460 -171 -6.50% 6,966 6,555 -411 -5.89%
Total Expenditure 226,458 228,124 1,667 548,445 552,445 4,000
Commissioner Sustainability Fund (CSF) Received 400 0 -400 400 0 -400
Revised Forecast Outturn 226,858 228,124 1,267 548,845 552,445 3,600
CSF - To be allocated 1,267 -1,267 3,600 -3,600
In year (Surplus)/Deficit 228,124 228,124 0 552,445 552,445 0
Add B/F Deficit 57,610
Cumulative Deficit 57,610
INCOME & EXPENDITURE REPORT - YTD & FOT POSITION AS AT 31 AUGUST 2019

APPENDIX 2
Recurrent Non Recurrent Total£000's £000's £000's
April Initial CCG Programme Allocation 491,193 491,193 Initial allocation - ProgrammeInitial CCG Running Cost Allocation 6,966 6,966 Initial allocation - Running CostsInitial CCG Primary Care Co-Commissioning Allocation 47,016 47,016 Initial allocation - Primary Care Co CommissioningOther Funding after Pace of Change 2,295 2,295 Baseline AdjustmentReduction for central indemnity scheme (1,353) (1,353) Baseline AdjustmentIR PELs transfer 128 128 Baseline AdjustmentAdditional Premises Support 400 400 Baseline AdjustmentNHS Property Services Voids & Subs 687 687 Baseline Adjustment
Total NHS England Allocation April 2019 547,332 0 547,332May
Deficit Carry Forward - Planned 0 (57,610) (57,610) Technical Adjustment
Total NHS England Allocation May 2019 0 (57,610) (57,610)June
Morbid Obesity Risk Share (78) (78) Technical Adjustment Excess Treatment Costs (20) (20) Technical Adjustment Cancer Quality of Life Metric Project Q1 11 11 Susan Boyd Pass through allocation to Northumbria HC FTCYP Green Paper Project Initiation Funds 125 125 Kate O'Brien TrailblazersCYP Green Paper MH Support Teams 228 228 Kate O'Brien TrailblazersCYP Green Paper Four week waiting pilot 556 556 Kate O'Brien TrailblazersImproving Access Allocations 19/20 from National Programme 6 6 Pamela Phelps GP Forward ViewAtrial Fibrillation (AF) patient optimisation 2019-20 [Q1 and Q2] 258 258 Alan Bell
Total NHS England Allocation June 2019 (78) 1,164 1,086July
Cancer Quality of Life Metric Project Q2 11 11 Susan Boyd Pass through allocation to Northumbria HC FT2019-20 Q1 Commissioner Sustainability Fund (CSF) 400 400 Technical Adjustment GPFV Other Initiatives 8 8 Pamela Phelps GP Forward View
0Total NHS England Allocation July 2019 0 419 419August
2019-20 Armed Forces CCG OOH allocation 8 8 Laurie Robson Armed Forces OOH
Total NHS England Allocation August 2019 0 8 8
Total YTD Confirmed NHS England Allocation 2019-20 547,254 (56,019) 491,235
In Year Allocation 2019-20 548,845
Commissioning Manager Lead Narrative
Board Approval
(Y/N)Board
Approval Date
NHS ENGLAND IN YEAR ALLOCATIONS ASSIGNMENT & APPROVAL STATUS

APPENDIX 3
August 2019 July 2019 Movement£000's £000's £000's
Non Current Assets Property, plant and equipment 951 973 (22)Intangible Assets 0 0 0Other Financial Assets 0 0 0
Total Non Current Assets 951 973 (22)
Current Assets Trade and other Receivables 2,637 2,545 92Cash and cash equivalents 268 388 (120)
Total Current Assets 2,905 2,933 (28)
Total Assets 3,856 3,906 (50)
Current Liabilities Trade and other payables (36,128) (36,262) 133Other liabilities 0 0 0Provisions 0 0 0Borrowings 0 0 0
Total Current Liabilities (36,128) (36,262) 133
Non-Current Assets plus/less Net Current Assets/Liabilities (32,272) (32,356) 84
Non-Current liabilities Other liabilities 0 0 0Provisions 0 0 0Borrowings 0 0 0
Total Non-Current Liabilities 0 0 0
TOTAL ASSETS EMPLOYED (32,272) (32,356) 84
Financed by Taxpayers Equity General Fund (32,272) (32,356) 84Capital & Reserves Revaluation Reserve 0 0 0
Other reserves 0 0 0TOTAL TAXPAYERS EQUITY (32,272) (32,356) 84
STATEMENT OF FINANCIAL POSITION

APPENDIX 4
Better Payment Practice Code - 30 Days NUMBER £000's
Non-NHSTotal Non-NHS Trade Invoices Paid in the Year 2,547 50,898 Total Non-NHS Trade Invoices Paid Within 30 Day Target 2,503 50,717 Percentage of Non-NHS Trade Invoices Paid Within 30 Day Target 98.27% 99.64%
NHS Total NHS Trade Invoices Paid in the Year 981 152,852 Total NHS Trade Invoices Paid Within 30 Day Target 978 152,594 Percentage of NHS Trade Invoices Paid Within 30 Day Target 99.69% 99.83%
BETTER PAYMENT PRACTICE CODEFOR THE FIVE MONTHS TO 31 AUGUST 2019

APPENDIX 5
Actual Actual Actual Actual Actual Forecast Forecast Forecast Forecast Forecast Forecast Forecast
April May June July August September October November December January February March£000's £000's £000's £000's £000's £000's £000's £000's £000's £000's £000's £000's
IncomeBalance bfwd 131 64 85 172 388 268 118 156 183 160 100 182DOH Income 38,800 42,300 40,100 41,700 41,700 41,600 40,300 40,300 40,300 40,300 40,700 40,400Supplementary /Cash Return 0 0 0 0 0 0 0 0 0 0 0 0Prescribing/Home Oxygen Therapy Charge to Cash Limit 3,761 4,042 4,021 4,195 4,011 4,084 4,131 4,012 4,271 4,126 4,064 4,042CHC Risk Pool 0 0 0 0 0 0 0 0 0 0 0 0Better Care Fund 0 0 0 0 0 0 0 0 0 0 0 0Other Income 221 47 24 113 57 200 200 200 200 200 200 200Total Income 42,913 46,453 44,230 46,180 46,156 46,152 44,749 44,668 44,954 44,786 45,064 44,824
ExpenditurePay (255) (242) (243) (247) (245) (256) (256) (256) (256) (256) (256) (256)NHS Payments including contracts (31,477) (30,023) (30,021) (30,499) (30,953) (30,220) (30,220) (30,220) (30,220) (30,144) (30,144) (30,144)Other Payments - BACS/CHAPS/CHQS (3,244) (5,095) (2,739) (5,419) (4,755) (6,582) (5,182) (5,182) (5,177) (5,270) (5,070) (5,335)Prescribing/Home Oxygen Therapy (3,761) (4,042) (4,021) (4,195) (4,011) (4,084) (4,131) (4,012) (4,271) (4,126) (4,064) (4,042)Delegated Co-Commissioning (4,020) (4,369) (5,408) (4,276) (4,395) (3,499) (3,411) (3,422) (3,477) (3,497) (3,955) (3,604)Better Care Fund 0 (2,408) (1,204) (967) (1,204) (1,204) (1,204) (1,204) (1,204) (1,204) (1,204) (1,204)Other (92) (189) (422) (189) (325) (189) (189) (189) (189) (189) (189) (189)Total Expenditure (42,849) (46,368) (44,058) (45,792) (45,888) (46,034) (44,593) (44,485) (44,794) (44,686) (44,882) (44,774)
BALANCE CFWD 64 85 172 388 268 118 156 183 160 100 182 50
2133
2019-20 CASHFLOW FORECAST

APPENDIX 6
Annual Budget YTD Budget YTD Actual
YTD Variance (Under)/
Overspend Forecast Outturn
Forecast Variance (Under)/
Overspend£000's £000's £000's £000's £000's £000's
General Practice - GMS 8,707 3,628 3,654 26 8,619 (88)General Practice - PMS 22,706 9,461 9,598 137 23,034 329QOF 5,163 2,151 2,071 (80) 5,191 28Enhanced Services 1,276 531 553 22 1,338 63Premises Cost Reimbursement 4,307 1,794 1,836 42 4,415 108Dispensing/Prescribing Drs 1,460 608 633 25 1,518 58Other GP Services 951 396 342 (54) 934 (17)PC Networks 2,069 862 744 (118) 1,567 (502)Reserves (575) 0 0 0 (554) 21Grand Total 46,063 19,431 19,431 0 46,063 0
PRIMARY CARE COMMISSIONING REPORT AT 31 AUGUST 2019

Agenda Item 7
OFFICIAL
1 20190925 UC Agenda Item 7 CMB Update Report
Clinicians commissioning healthcare for the people of Northumberland
Meeting title Governing Body
Date 25 September 2019
Agenda item 7
Report title Clinical Management Board Report
Report author Chief Operating Officer and Clinical Director of Primary Care
Sponsor Clinical Director of Primary Care
Private or Public agenda
Public
NHS classification Official
Purpose (tick one only)
Information only
Development/Discussion
Decision/Action
Links to Corporate Objectives Ensure that the CCG makes best use of all available resources
Ensure the delivery of safe, high quality services that deliver the best outcomes
Create joined up pathways within and across organisations to deliver seamless care
Deliver clinically led health services that are focused on individual and wider population needs and based on evidence.
Northumberland CCG/external meetings this paper has been discussed at:
CMB
QIPP N/A Risks Covers a range of strategic risks on the assurance framework Resource implications N/A Consultation/engagement N/A Quality and Equality impact assessment
See below

OFFICIAL
20190925 UC Agenda Item 7 CMB Update Report
2
Data Protection Impact Assessment
N/A
Research N/A Legal implications N/A Impact on carers N/A Sustainability implications N/A
OFFICIAL
20190925 UC Agenda Item 7 CMB Update Report
3
QUALITY and EQUALITY IMPACT ASSESSMENT 1. Project Name Clinical Management Board Report
2. Project Lead Director Lead Project Lead Clinical Lead Clinical Director of Primary Care
Chief Operating Officer Clinical Director of Primary care
3. Project Overview & Objective
Clinical Management Board Overview for Governing Body
4. Quality Impact Assessment
Impact Details Pos/ Neg
C L Scores
Mitigation / Control
Patient Safety NA Clinical Effectiveness NA Patient Experience NA Others including reputation, information governance and etc.
NA
5.Equality Impact Assessment
Impact Details Pos/ Neg
C L Scores
Mitigation / Control
What is the impact on people who have one of the protected characteristics as defined in the Equality Act 2010?
NA
What is the impact on health inequalities in terms of access to services and outcomes achieved for the population of Northumberland? (which is in line with the legal duties defined in the National Health Service Act 2006 as amended by the Health and Social Care Act 2012), for example health inequalities due to differences in socioeconomic circumstances?
NA
6. Research Reference to relevant local and national research as appropriate.
NA

OFFICIAL
20190925 UC Agenda Item 7 CMB Update Report
4
7. Metrics Sensitive to the impacts or risks on quality and equality and can be used for ongoing monitoring.
Impact Descriptors Baseline Metrics Target
8. Completed By Signature Printed Name
Date
Chief Operating Officer
S BROWN
19/09/2019
Additional Relevant Information:
8. Clinical Lead Approval by Signature Printed Name
Date
Additional Relevant Information:
9. Reviewed By Signature Printed Name
Date
Comments

OFFICIAL
20190925 UC Agenda Item 7 CMB Update Report
5
Governing Body 25 September 2019 Agenda Item: 7 Clinical Management Board Report Sponsor: Chief Operating Officer Members of the Governing Body are asked to: 1. Consider the Clinical Management Board exception and highlight report and provide
comment.
Purpose This report details the Clinical Management Board (CMB) performance and quality Exception Report which is the main focus of Governing Body (GB) and the board highlight report. Introduction The September 2019 CMB provided an opportunity for all Clinical Directors and Clinical Leads to reflect on NHS Northumberland Clinical Commissioning Group’s (CCG) performance, quality and workload half way through the current year; and collectively plan for the remainder of the year. Performance and Quality Headlines The CMB Quality and Performance Exception Report is at Appendix 1. GB should note: The main headline with regard to performance is the sheer volume of non-elective activity across the system which is at an unprecedented high – not only in accident and emergency, ambulatory care, ambulance conveyances (especially in Category Two), emergency admissions but also in primary care contacts. This is not unique to the Northumberland system. Local provider organisations as well as the System Transformation Board are considering the causes for this as well as potential solutions for managing non elective demand. From a Cancer perspective, there are increased numbers of people being diagnosed within 28 days (this analysis is operating in shadow form as it is not yet a mandated target nationally – each Foundation Trust is recording this locally and sometimes differently at the moment). The percentage of patients seen within 62 days is now up to 84.9% and the focus is on maintaining and improving this sustainably.
With regard to referral to treatment times (RTT) – there is an average improving reduction in wait times but numbers of patients on the waiting lists are still going up – but the CCG

OFFICIAL
20190925 UC Agenda Item 7 CMB Update Report
6
achieved the 92% threshold. There are early indications of improvement that is supported by changes to patient pathways including urology for example and detailed patient tracking. Other headlines for noting - all outlined in the attached Appendix are:
• The underperformance against the 4 hour Accident and Emergency target • The recent deterioration in delayed transfers of care • The ongoing under performance of the ambulance service both at trust wide and at
Northumberland level • The variation in waiting list sizes for patients awaiting treatment • The underperformance against the diagnostic 6 week threshold • The slight deterioration in performance against the IAPT access target within mental
health linked to the increase in performance expected in quarter 4 • The incidence of E.Coli against the provider and CCG trajectories and the recent CCG
MRSA cases.
Five Year Plan Work continues to develop the five year plan across Northumberland, the North Integrated Care Partnership (ICP) and System levels; with a draft plan developed by October followed by the final plan at the end of the calendar year. Engagement with wider local authorities has been positive at an ICP level and everyone involved will continue to build and develop positive relations within the wider system. The whole system is awaiting the financial control totals within which to operate. Clinical leads key work areas – highlights of current work All lead and directors present outlined the current and future workload illustrated in the summary table below:
Medicines Optimisation
• Meds Optimisation three meetings coming up – Medicines Management GP Leads meeting
• Consultant Connect decision for the future • Pharmaceutical organisation engagement - more formal
process and culture in the CCG, rules of engagement Workforce • Workforce Planning
• Funded training for practices for PCNs • Primary Care Development – recruitment into primary care
team, apprentices into the team Newcastle Pathways
• Tele-dermatology – paper to CMB October. Survey Monkey going out in September
• Ophthalmology including Glaucoma Cancer, Primary Care
• Cancer action plan aligned with other CCGs • Early diagnosis – aligned with other CCGs

OFFICIAL
20190925 UC Agenda Item 7 CMB Update Report
7
Quality
• Public Health and Prevention (this is wider than just cancer, Health Inequalities five year plan)
• Living with and Beyond Cancer • Patient Experience • GP Visiting programme is a priority • GP Assurance
Long Term Conditions Adult Mental Health
• MH – reconfigure head injuries service - meeting in two weeks’ time beyond Age 65
• Autism/ ADHD services – health checks, long waits • IAPT review • Respiratory • Spirometry services – how best to provide this • MyCOPD – granted licenses. Rightcare respiratory meeting • New COPD pathway – through prescribing teams for approval • Asthma guidelines with inhalers out now • Cardiology – AF demonstrator programme • Diabetes – low calorie diets, diabetes education programme –
re-commission in some way • GP Teamnet, clinical guidelines
Public Health • Relaunch of exercise referral; Active Tier 2 service offer – team going around locality meetings this week
• Health Inequalities paper to GB • Primary care event 2 October 2019 • Social prescribing – launch Directory of services in December
(maintenance will be important) • Meeting PCNs to support content of their plans • UEC strategy data and evidence
Maternity • Maternity – Local Maternity System North (1) perinatal MH – we have a model working with NHCFT – discussion on roll out to whole region (2) Continuity of carer – one midwife following through whole pathway of care – 35% of all women being under this model of care – struggling to get these numbers – NSECH is main issue not MLUs
• Smoking in pregnancy is covered in all of this – but check our rates
• Strategic direction of travel for Northumberland although measures in place for staff safety
Workforce and pharma
• Workforce development with Tony and Annie • Working with Pharma – culture of CCG and practices • Gables medical group – nursing home safeguarding issues • Education event preparation 2 October 2019
Planned Care
• IFR – VBC review is happening at the moment but not published yet

OFFICIAL
20190925 UC Agenda Item 7 CMB Update Report
8
• JMAPS implementation and assessment • Outpatient work • RTT, Diagnostics, performance • GP Teamnet guidelines • Lothian
Recommendations GB is asked to consider the quality and performance exception report and the board update and provide comment. Appendix 1: Quality and Performance Exception Report Appendix 2: Patient Impact report

OFFICIAL
20190925 UC Agenda item 7 Appendix 1 & 2 Performance and Quality Exceptions 1
Appendix 1 Performance and Quality exception report – September 2019 This section of the report details the exception reports relating to NHS Northumberland Clinical Commissioning Group (CCG) and main acute provider performance and quality. Appendix 2 Included within this section is a report that was presented to CMB members at the August 2019 meeting aiming to identify and assess the potential impact on patients as a consequence of delays or breaches against the wide range of quality and/or performance standards, which CCGs are expected to achieve as a part of the commissioning of health care within their local population.

OFFICIAL
20190925 UC Agenda item 7 Appendix 1 & 2 Performance and Quality Exceptions 2
Appendix 1 Performance and Quality exception report
Performance Area Current Position Detail Mitigating Actions and Timeframe Director
Lead Cancer 62 days Standard: 85% of patients should be treated within 62 days of referral by GP.
CCG Under performance since June 2018 2018/19 79.9% April 2019 80.2% May 2019 77.0% June 2019 74.3% July 2019 85.5% Northumbria Under performance since June 2018 2018/19 78.3% April 2019 77.3% May 2019 80.0% June 2019 75.8% July 2019 84.5% Newcastle Under performance since June 2018 2018/19 78.6% April 2019 81.3% May 2019 77.5% June 2019 70.9% July 2019 77.9%
Under performance by both local acute trusts of the standard Surge in demand within urology during first quarter of 2018/19 has contributed towards underperformance from June 2018 onwards Consistent achievement of 62 day target is not expected to be achieved until March 2020 based upon local acute provider trajectories.
Both local providers continue to focus upon improving governance, tracking patients to avoid delays in diagnosis and treatment at each stage and reviewing pathways to achieve the new 28 day target to be formally introduced next year as a threshold to diagnose cancer. Northumbria has reduced its time to diagnosis of cancer significantly across a range of procedures that has been reflected in the July performance data resulting in the CCG achieving the 62 day target for the first month for a long period of time. A joint commissioner meeting has been established involving the clinical and commissioning leads from Northumberland, North Tyneside and Newcastle/ Gateshead CCGs. The group continues to gather and share intelligence relating to the progress against the action plans that the local acute providers are making in relation to improving cancer performance and changing future pathways. The group has agreed to meet every two months.
Robin Hudson
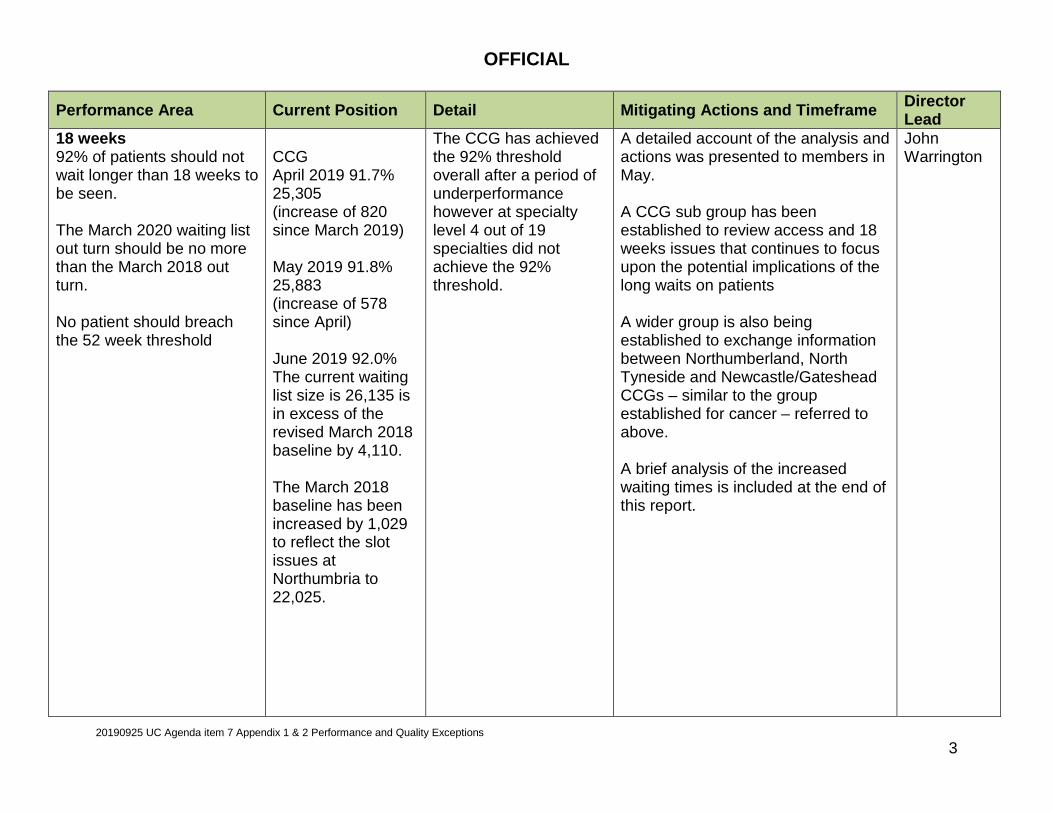
OFFICIAL
20190925 UC Agenda item 7 Appendix 1 & 2 Performance and Quality Exceptions 3
Performance Area Current Position Detail Mitigating Actions and Timeframe Director Lead
18 weeks 92% of patients should not wait longer than 18 weeks to be seen. The March 2020 waiting list out turn should be no more than the March 2018 out turn. No patient should breach the 52 week threshold
CCG April 2019 91.7% 25,305 (increase of 820 since March 2019) May 2019 91.8% 25,883 (increase of 578 since April) June 2019 92.0% The current waiting list size is 26,135 is in excess of the revised March 2018 baseline by 4,110. The March 2018 baseline has been increased by 1,029 to reflect the slot issues at Northumbria to 22,025.
The CCG has achieved the 92% threshold overall after a period of underperformance however at specialty level 4 out of 19 specialties did not achieve the 92% threshold.
A detailed account of the analysis and actions was presented to members in May. A CCG sub group has been established to review access and 18 weeks issues that continues to focus upon the potential implications of the long waits on patients A wider group is also being established to exchange information between Northumberland, North Tyneside and Newcastle/Gateshead CCGs – similar to the group established for cancer – referred to above. A brief analysis of the increased waiting times is included at the end of this report.
John Warrington

OFFICIAL
20190925 UC Agenda item 7 Appendix 1 & 2 Performance and Quality Exceptions 4
Performance Area Current Position Detail Mitigating Actions and Timeframe Director Lead
Diagnostic waits A maximum tolerance of 1% of patients should wait longer than 6 weeks for a diagnostic test
CCG March 2019 1.3% April 2019 2.5% May 2019 3.1% June 2019 1.5% Northumbria March 2019 0.4% April 2019 0.9% May 2019 2.1% June 2019 0.9% Newcastle March 2019 3.4% April 2019 5.0% May 2019 4.5% June 2019 4.1%
Newcastle hospitals’ over recent months has continued to breach the 1% threshold which is impacting upon the CCG performance. The CCG has failed to achieve the standard since March which was for the first time for a few years.
There are ongoing workforce shortages in radiology reporting although the trust is outsourcing more activity for diagnostic tests. The trust is developing a short, medium and long term plan to recover performance. There is also less capacity in sleep studies and a backlog of patients in urodynamics. At Northumbria the trust failed to achieve the target at the start of the year relating to breaches within echo cardiology, however sue to the trust increasing their staffing, recent performance has improved to enable the trust to achieve the target overall.
John Warrington
Performance Area Current Position Detail Mitigating Actions and Timeframe Director Lead
Accident and Emergency 95% of patients should be either treated or admitted within 4 hour of arrival
Northumbria April 2019 93.8% May 2019 92.8% June 2019 91.8% July 2019 95.0%
A high volume of patients whose care is amenable to primary care are attending A&E combined with a higher level of acuity in seriously ill patients are placing the trusts under considerable pressure
A wide range of region wide and local actions are in place which is being overseen by the LAEDB. These include:
• Ambulance investment to reduce conveyance into A&E (in 19/20 contract)
• Increase in same day discharge from hospital ( to
Nicole McLean

OFFICIAL
20190925 UC Agenda item 7 Appendix 1 & 2 Performance and Quality Exceptions 5
Newcastle upon Tyne April 2019 95.15 May 2019 94.2% June 2019 95.4% July 2019 94.5%
improve bed flow) • Community paramedic pilot in
Berwick (July 19 start) • Introduction of Systm 1 in
A&E to link in with primary care records / appointments (Sept 19)
• Revisiting ECIP/ RPIW actions - currently under review by LAEDB.
• Working with ECIST to improve ambulance arrival to clear times within the local system.
Performance Area Current Position Detail Mitigating Actions and Timeframe Director Lead
Health Care Acquired Infections E.Coli March 2020 end of year target 262.
June 2019 77 cases reported year to date against the year to date trajectory of 66.
The CCG continues to breach the E.Coli trajectory. It is a local, regional and national challenge particularly within the community
CCG is a part of the Regional NHSI HCAI Improvement Board, working with local CCGs and providers on a wide range of initiatives including the management of catheterised patients, hydration and fluid management. A review of the circumstances behind the cases has been undertaken by the CCG. The local health system is now reflecting on the lessons learnt from these cases.
Annie Topping

OFFICIAL
20190925 UC Agenda item 7 Appendix 1 & 2 Performance and Quality Exceptions 6
MRSA There is a zero tolerance for MRSA cases
2 cases were reported in April 1 case reported in May
Northumbria Health Care NHS Foundation Trust reported the cases in April that were to be apportioned to the CCG

OFFICIAL
20190925 UC Agenda item 7 Appendix 1 & 2 Performance and Quality Exceptions 7
Growth in waiting lists and access to services The recent increase in waiting list size combined with the deterioration in performance is of ongoing concern to the CCG. As cited in previous reports to Governing Body members, increase in demand for services, pressure within cancer services and the current workforce issues are all contributing to the changing waiting list status. Between March and May 2019 the CCG performance has not achieved the 92% threshold. The chart below however shows that the CCG in June achieved the target.
82%
84%
86%
88%
90%
92%
94%
96%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Northumberland Incomplete 18 weeks pathway performance 2018/19 to 2019/20
Northumberland 2019/20 England 19/20
Northumberland 2018/19 Target

OFFICIAL
20190925 UC Agenda item 7 Appendix 1 & 2 Performance and Quality Exceptions 8
Variation in number of patients on the waiting list
The CCG waiting list also increased by 252 in June compared with the previous month when the increase was 578. This continues to be of concern as the CCG was expected to ensure that the number of patients on the waiting lists in March 2019 does not exceed the number as at March 2018. NHS England expects the waiting lists now to return to the March 2018 position by March 2020. The CCG has been partially successful in having the March 2018 baseline adjusted for the slot issues in relation to the patients on the Northumbria waiting lists but as yet no adjustment has been made for patients on the Newcastle waiting list. As a consequence of this, the March 2018 baseline is now 22,025. The June 2019 waiting list was reported at 26,135, representing an increase of 4,110.
20000
21000
22000
23000
24000
25000
26000
27000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Comparative incomplete 18 weeks pathway 2018/19 - 2019/20
2019/20 2018/19 March 18 Baseline

OFFICIAL
20190925 UC Agenda item 7 Appendix 1 & 2 Performance and Quality Exceptions 9
Key actions A detailed account was provided to members recently as the contributing factors behind both the increase in list size and the deterioration in performance. The acute provider trusts continue to prioritise based upon clinical need with waiting list initiatives identified for cancer patients where possible. Recent actions include
• Recruitment of consultants and locums in spinal surgery, Gastro-intestinal and the upper limb specialties. • Negotiations over the pension arrangements affecting senior medical staff carrying out additional hours. This is
expected to generate additional capacity to reduce waiting lists through the delivery of waiting list initiatives. • Validation of waiting lists – to remove patients who no longer require treatment • Review of performance and reporting structures within providers to ensure better accountability for any potential
delays in treatment • Operational focus to avoid long waiters – particularly close monitoring of patients who have been on a waiting list
for 36 weeks or more to avoid breaching the 52 weeks threshold.
The CCG continues to carry out analyses of the waiting list profiles as outlined below.

OFFICIAL
20190925 UC Agenda item 7 Appendix 1 & 2 Performance and Quality Exceptions 10
Using the revised March 2018 baseline as the position to which NHS England expects both CCGs and Providers to return to by March 2020, the above table shows by specialty level the changes in waiting list size by volume of patients along with the average and 92%ile waiting times in weeks.
March 2018 v June 2019
Treatment FunctionChange in
total waiting list
% change
Change in average waiting
time
Change in waiting
times 92nd percentile
General Surgery 388 15% -1.1 -1.7Urology 445 35% 1.2 2.3Trauma & Orthopaedics 703 22% -0.4 -2.2Ear, Nose & Throat (ENT) 119 6% 1.8 2.4Ophthalmology 822 34% 1.9 3.6Oral Surgery - Neurosurgery 15 500%Plastic Surgery 23 6% -0.9 -2.3Cardiothoracic SurgeryGeneral Medicine 14 3% 0.0 -0.8Gastroenterology 87 11% 0.2 -1.2Cardiology 176 15% -0.5 0.9Dermatology 276 33% 0.9 0.5Thoracic Medicine 151 23% 2.2 3.1Neurology 22 275%Rheumatology 156 27% 1.3 5.2Geriatric Medicine 102 21% 1.2 3.6Gynaecology 188 13% 0.7 -0.4Other 423 11% 0.9 1.4Total 4,110 18.7% 0.5 0.7
Change in activity Change in waiting time
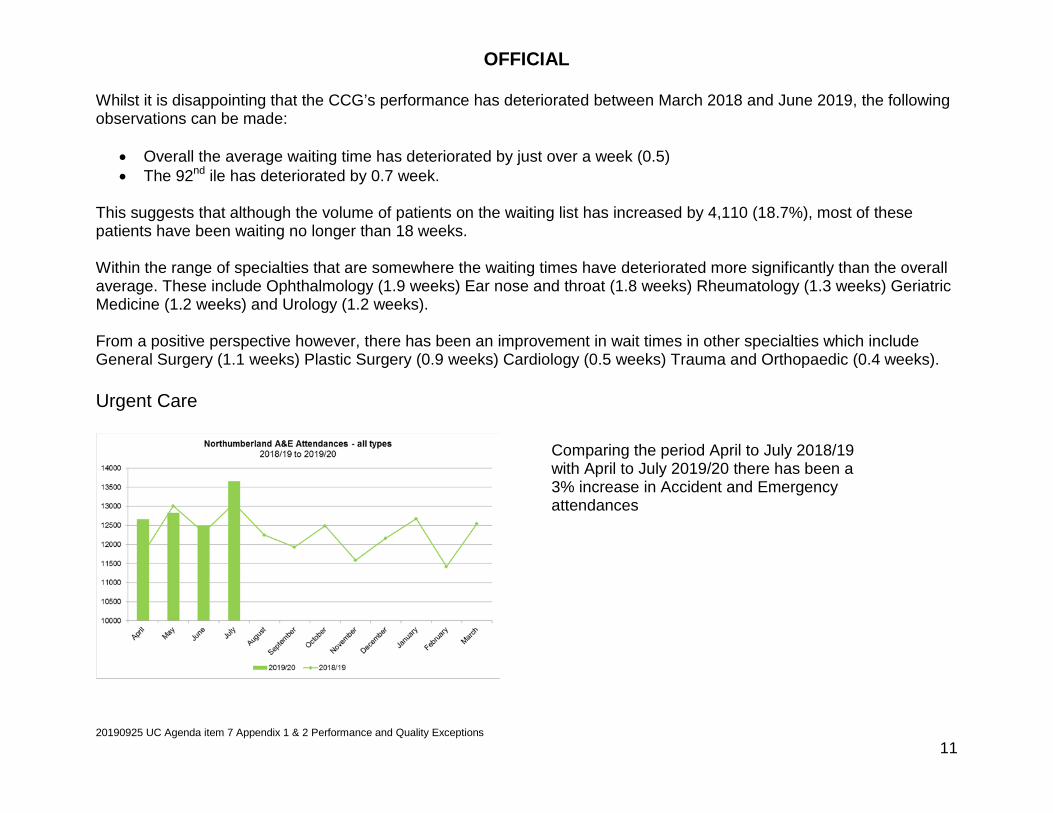
OFFICIAL
20190925 UC Agenda item 7 Appendix 1 & 2 Performance and Quality Exceptions 11
Whilst it is disappointing that the CCG’s performance has deteriorated between March 2018 and June 2019, the following observations can be made:
• Overall the average waiting time has deteriorated by just over a week (0.5) • The 92nd ile has deteriorated by 0.7 week.
This suggests that although the volume of patients on the waiting list has increased by 4,110 (18.7%), most of these patients have been waiting no longer than 18 weeks. Within the range of specialties that are somewhere the waiting times have deteriorated more significantly than the overall average. These include Ophthalmology (1.9 weeks) Ear nose and throat (1.8 weeks) Rheumatology (1.3 weeks) Geriatric Medicine (1.2 weeks) and Urology (1.2 weeks). From a positive perspective however, there has been an improvement in wait times in other specialties which include General Surgery (1.1 weeks) Plastic Surgery (0.9 weeks) Cardiology (0.5 weeks) Trauma and Orthopaedic (0.4 weeks). Urgent Care
Comparing the period April to July 2018/19 with April to July 2019/20 there has been a 3% increase in Accident and Emergency attendances

OFFICIAL
20190925 UC Agenda item 7 Appendix 1 & 2 Performance and Quality Exceptions 12
In addition to the increase volume of attendances within Accident and Emergency there was also an 8.4% increase in ambulatory care and a 5.8% increase in emergency admissions when comparing performance and activity over the same period of time (April to July). Northumbria opened its new Ambulatory care unit in July 2019. There is an expectation that there would be a reduction in emergency admissions as a consequence of increased activity within ambulatory care.

OFFICIAL
20190925 UC Agenda item 7 Appendix 1 & 2 Performance and Quality Exceptions 13
Delayed transfers of care The Better Care Fund states that within Northumberland there should not be in excess of 261 delayed transfers of care per month
050
100150200250300350400450
Northumberland delayed transfer of care against BCF target 2018/19 -2019/20
2019/20 Actual 2018/19 Actual BCF Target Revised trajectory

OFFICIAL
20190925 UC Agenda item 7 Appendix 1 & 2 Performance and Quality Exceptions 14
The above charts show a deteriorating position in terms of an increase in the number of delayed transfers of care across the system in the recent months. An investigation is being undertaken by the CCG as to causes of the recent increases before an action plan for future recovery is prepared and implemented. A particular concern is that there are increases evidenced at all the providers.
0100200300400500600
Delayed transfers of care by provider - Northumberland
April 2017 - June 2019
NHCFT NUTHFT NTW Other

OFFICIAL
20190925 UC Agenda item 7 Appendix 1 & 2 Performance and Quality Exceptions 15
Primary Care An analysis has also been undertaken in profiling the activity undertaken within primary care. The chart below shows that there continues to be an increase in activity. Comparing the period April to July 2018/19 with April to July 2019/20 there has been a 12.7% of activity. This activity includes face to face, telephone and home visits carried out by GPs.

OFFICIAL
20190925 UC Agenda item 7 Appendix 1 & 2 Performance and Quality Exceptions 16
It is interesting to note that despite the changes in activity the proportion of activity has remained the about the same across the three years. The CCG will continue to review activity across the system to identify potential pressures during the forthcoming winter period to develop actions to mitigate the consequences and implications of such changes.

OFFICIAL
20190925 UC Agenda item 7 Appendix 1 & 2 Performance and Quality Exceptions 17
Appendix Two Patient Impact report Background Members of CMB as a matter of routine, receive a monthly report outlining the performance and quality of the services provided by local providers that serve the population of Northumberland. Many of the standards are outlined in the NHS Constitution or captured in the binding contracts held between the CCG and provider based upon the standard national NHS contract. Where there are areas of underperformance, the reasons are outlined along with an overview as to the actions that the provider is taking to improve future outcomes. The reports periodically make reference to national or local surveys such as the cancer patient experience survey or the results of the friends and family test. This information is however provided in many cases at a high level, and does not offer the detail in terms of the impact on patients when performance or the quality is not at the required standard. The area of particular focus relates to potential harm or compromise to their treatment as consequence of the delay in treatment or care. This report however seeks to provide more detail to reflect the actual impact at a patient individual level. It is however recognised that there are areas of further development required due to the current assurance system and infrastructure to date not being established between local commissioner and provider. Taking a proportionate and balanced approach, the CCG will endeavour to address this in going forward through further collaboration with local providers. This report will review the year 2018/19 and where possible capture information relating to the first quarter of 2019/20. Areas of particular focus Following the recent deterioration in the CCG’s tradition of strong performance, the areas of concern reflected in the CCG and provider key performance and quality indicators summary in the monthly Joint Performance and Quality Report are:
• Cancer 62 day performance • Ambulance response times • Hospital handover delays • Accident and Emergency 4 hour waits • Waiting times against the 18 weeks referral to treatment target • MRSA incidence
With the exception of the MRSA and ambulance response times, the above data relates to breaches during 2018/19 involving Northumberland patients.
OFFICIAL
20190925 UC Agenda item 7 Appendix 1 & 2 Performance and Quality Exceptions 18
Cancer 62 day performance In 2018/19 255 patients were not treated within 62 days. Patient Harm There were no serious incidents reported by the provider trusts on STEIS or incidents reported by GP practices on SIRMS regarding these patients. The CCG had an agreement with NHCFT to enable its Cancer Project Lead to attend the Trust’s cancer multidisciplinary meeting. The aim was to allow a better understanding of a range of issues including quality impact on individual patient. Unfortunately, this did not happen as planned. At the moment, there is no ‘formal’ process in place to monitor / assess the potential harmful impact at a patient level. Actions taken by the Trust In response to the CCGs’ repeated requests for information on patient impact, high level assurance had been provided via the Quality Review Groups for patients treated at Newcastle Hospitals and Northumbria Healthcare NHSFT. The latest information received was in April and May 2019. NHCFT reported that their Executive Director of Nursing and Midwifery and Executive Medical Director are assessing potential harm of these patients, and have started to carry out a review of the notes of all patients involved. The Trust will provide an update after six months to advise what actions have been taken and the progress that has been made. NUTH has also given verbal assurance that there is an internal system in place to review patients who have breached in this area. Patient Experience The National Cancer Patient Experience Survey has been designed to monitor national progress on cancer care. The results for NHCFT show that patients have an increasingly positive view of their cancer care, scoring positively outside the expected range for 24 questions regarding the experience of care received. None of the results were in the ‘lower than expected’ range. Overall, the Trust wide cancer services have demonstrated improvement with performance rated above the national average and sustained as one of the uppermost in the Northern Cancer Alliance geography. The patients who were surveyed for NUTH rated their overall care as 9/10 and reported a positive experience in many areas including involvement in decisions about care and treatment and being treated with dignity and respect.
OFFICIAL
20190925 UC Agenda item 7 Appendix 1 & 2 Performance and Quality Exceptions 19
Ambulance Response Times In 2018/19, 12,547 Northumberland patients were not treated within the required standard:
• Category 1: 1215 patients • Category 2: 9309 patients • Category 3: 1301 patients • Category 4: 722 patients
From April 2019 to June 2019, there have been 4063 Northumberland patients who have not been treated within the required standard:
• Category 1: 340 • Category 2: 3127 • Category 3: 383 • Category 4: 213
Serious Incidents Of the 1215 patients who were not treated within the Category 1 standard in 2018/19 NEAS reported one serious incident regarding a treatment delay to a Northumberland CCG patient. The patient had chest pain and collapsed. The original address was input into the CAD system incorrectly and as a result it took 43 minutes for the crew to reach the patient. Patient Harm The patient was found to be deceased when the crew arrived at the correct address. The main contributing factor was incorrect documentation of recording patients address. However there is no conclusive evidence in the Root Cause Analysis to indicate whether the delay directly contributed to the death of this patient. Actions taken by the Trust • Refresher training via the Lamp for Health Advisors – individual training was completed in
July 2018. • New procedure on how to download a call for playback whilst a live call is still in progress to
confirm address details has been implemented. • New procedures to document correct escalation flow for contacting a team leader for time
critical information. • Cleanse performed of the Gazetteer ensuring all address details have an accurate
recording of town and district locations.

OFFICIAL
20190925 UC Agenda item 7 Appendix 1 & 2 Performance and Quality Exceptions 20
SIRMS The number of incidents reported by Northumberland GP practices has been low. However, the West locality did raise concerns to the CCG Senior Head of Commissioning in early 2019/20 regarding delays in Category 2 responses. Of the 3127 Northumberland patients who have not been treated within the required standard, five have been reported and whilst awaiting investigations from NEAS, the patient outcomes for each incident were confirmed by NHCFT with confirmation given from the reporting GP practices having reviewed the discharge summaries:
Patient Harm On all of the incidents reported, no patient harm was reported as a result of the ambulance delay. Long waits analysis As a result of the CCGs’ persistent effort to request at QRGs for further assurance on patients who had experienced long waits, NEAS agreed to explore further through a short pilot in order to review its safety measures and improvements that could be made. The criteria for this review was decided internally by NEAS, and anyone who had waited three times the expected ARP standard arrival time under each deposition criteria is classified as a ‘significant breach’. All significant breaches between the 1 February 2019 to 14 February 2019 were reviewed, and as can be seen in the below table, there was a total of 156 cases. The analysis was presented at the NEAS QRG in April 2019.
Attendance Date
Reason for attend Diagnosis Length of Stay Procedure Harm?
15/07/2019 GP Ref ?sepsis (current UTI), non productive cough, SOB, Lower back ache, unsteady of feet and feeling dizzy
Pneumonia L sided. Derranged bloods 4 days Bloods and USS
No
11/07/2019 GP ref 2 hour hx of CP, waves of pain, tightness around chest, had GTN with GP which eased pain slightly
NAD - Trop <5, ECG noemal, no MSK CP. 5hr47min Bloods incl Trop and ECG
No
09/07/2019 GP ref, known COPD, SOB over several days, SATS lower than normal. Episodes of crushing chest pain but pain free on triage, productive cough
Exacerbation of COPD 5 days Bloods, ABG and CXR
No
10/07/2019 Chest tightness/heaviness. Left arm tingling-resolved. SOB. GP sent to ED
Diagnosed with atypical chest pain and discharge home 4pm same day
13 mins in ED. 3 hours in MAC
None in ED, Bloods incl Trop and XR on MAC
No
19/06/2019 1/12 hx of CCP. GP Ref ?cardiac Transferred from A&E to coronary care at Freeman hospital with acute coronary syndrome. Angiogram revealed severe stenosis of RCA and stent was inserted and triple therapy. Discharged 24/06/2019
5 days then transfer to FRH Ward 27
Bloods incl Trop and ECG
No

OFFICIAL
20190925 UC Agenda item 7 Appendix 1 & 2 Performance and Quality Exceptions 21
Category Total dispatch Significant breaches C1 1199 0 C2 13255 55 C3 3704 61 C4 1716 40 Patient Harm Within the Category 2 response, there were 2 patients whose condition deteriorated. However, rapid response vehicles were in attendance and treatment was provided. Within the Category 3 response, one patient was identified as having low harm and this is currently under investigation. Actions taken by the Trust • The information from the audit has now been added by NEAS onto the CLERIC system so
more audits can be carried out. • Following this benchmarking exercise, the audit will now be run on a regular basis. Should
instances of harm increase, this audit would then be run on a daily basis. • A dashboard is also being developed by NEAS to show results. Patient Experience The Trust Friends & Family Test Data is consistently reported as better than the national average for See & Treat and Patient Transport Services. Hospital Handover Delays 12 patients experienced handover delays more than 2 hours when attending NSECH in 2018/19, all of which were during the winter period in December 2018 and January 2019. On the days where over 2 hour handovers were reported, performance ranged from 69.4% - 77.53%. The Trust investigates these handover delays under a local system known as Significant Learning Events (SLEs) to establish;
• Explanation and consideration of the circumstances of the 2 hour wait • Lessons which could have been learned as a result of the incident • Any harm that came to the patient as a result of the wait • Recommendations of any actions to address and prevent such a thing happening again.

OFFICIAL
20190925 UC Agenda item 7 Appendix 1 & 2 Performance and Quality Exceptions 22
Patient harm The Trust had reported that there was no detriment to all of the affected patients care reported, and there was no threat to the safe management of the 12 patients throughout this wait in both the care of NEAS and the emergency care department post-handover. However as a result of prolonged waits and handover times, this might have a negative impact on patient experience, expectations of partners (NEAS) as well as staff wellbeing in A&E. Actions taken by the Trust (on the days where delays were reported) • Bed Managers continually updated the nerve centre screens to identify any empty beds
back of house to pull from A&E. • OSMs and matrons aided timely discharges on identified wards. • Patients on wards were identified and sent to the discharge lounge to make space for
patients coming through A&E. • Senior Managers and OSMs present and active within the department and on site • Boarders had been identified as early in the day as possible and moved where possible. • Patients who were deemed appropriate to sit out of the queue were handed over and sat
out in the A&E hub to await a bay. Full hospital protocol in action with regular “decompressions” to the wards.
• Patients already in cubicles were assessed and if appropriate were sat out in the corridor or sub wait to allow new patients to be handed over in cubicles where needed.
• Additional space was utilised to see patients in the plaster room. • Diverts place where possible • Additional consultants were brought forward to see patients and base site consultants were
asked to do extra ward rounds to help with flow.
Patient Experience The latest Patient Perspective Data highlighted that “actual waiting times until triage” was an area for improvement. Patient Perspective is an external NHS approved agency. The company surveys NHCFT’s patients two weeks post discharge and provides the Trust with consultant rich data. Two weeks post discharge is when research suggests that patients are most likely to tell of their experience in the most honest way. Accident and Emergency 4 hour waits 6061 patients were not treated or admitted within 4 hours of arrival at A&E during 2018/19. Patient Harm There was one serious incident reported in 2018/19 where a patient had a treatment delay in A&E of just over 4 hours.

OFFICIAL
20190925 UC Agenda item 7 Appendix 1 & 2 Performance and Quality Exceptions 23
On 20 September 2018, a patient was brought into A&E at 05:35 with chest pain. The patient was triaged as a P2 with the ECG indicated possible STEMI but the patient was not seen until 09:44. The patient’s notes were inadvertently placed in the P3 queue, and as a result, there was a delay in the patient’s medical assessment. During the medical assessment, the patient deteriorated and had a cardiac arrest and died in the department. It is not clear whether an earlier diagnosis would have altered the outcome. Currently there is no formal system to gain assurance on other patients which are not reportable under SI. Actions taken by the Trust • As a result of these findings the department IT screens have been newly located to enable
a more cohesive overview of patients in the department. • The existing guideline for ECG sign off is being re-iterated to all staff • In addition a new SOP is being written to standardise the triage process. Patient Experience The Patient Perspective Data for NHCFT shows a consistent performance within the emergency department. Three out of 27 questions asked place the Trust outside of the top 20% threshold. However, the scores are still above the national average. These questions relate to waiting times, co-ordination and consistency of care and response to pain. Current performance is discussed at the Trust’s Executive Management Team and Safety & Quality meetings to appropriately explore with the business units possible reasons. Observations of monthly data are maintained to support improvement. The Friends and Family Test data remains steady but continue to be below the national average and require improvement. Poster vote has been introduced in high frequency areas across NHCFT with returns being collected over coming months. At NUTH, The FFT response rate remains well below the national and regional averages. However, the % of patients who would recommend the service continues to be reported above regional and national averages. Waiting times against the 18 weeks referral to treatment target 19,392 patients were not seen within 18 weeks of being referred by their GP to a Consultant. Patient Harm There were no serious incidents reported on STEIS or incidents reported by GP practices on SIRMS regarding these patients. Currently there is no formal process in place to assure other patients affected which are not reportable as SIs.
OFFICIAL
20190925 UC Agenda item 7 Appendix 1 & 2 Performance and Quality Exceptions 24
MRSA Incidence During 2018/19 there were no MRSA attributed to the CCG. As from April 2019, the rule has changed and now all pre-48 hours’ cases are attributed to the CCG and any post-48 hours cases are attributed to the providers, regardless of any gaps identified in the investigation process. Year to date in 2019/20, 3 cases have been attributed to the CCG. There is a statutory requirement for each MRSA to carry out a post infection review. Post infection reviews have been held for all of these cases. Based on the information available, it would appear that there were potential gaps in care in other settings but not primary care. Lessons learnt have been fed back to the organisations concerned. Case 1: The patient lives in sheltered housing and has a number of long term conditions. The patient had no MRSA before this episode of care and there is uncertainty as to the source of the infection. Patient Harm This patient was admitted to NESCH following a fall on 7 April 2019, and then discharged back to the community to a nursing home. Potential gaps in care The patient record showed that the patient had chronic problems with the left leg and a wound management plan was ongoing. Factor that may have contributed a MRSA bacteraemia is:
• Skin swabs were not taken despite of a chronic leg wound. This would help to identify the presence of MRSA, if any, and enable the treatment to be provided if needed.
Case 2: This patient was brought to NESCH showing signs of sepsis on admission. The patient had a history of metastatic colorectal cancer and unfortunately passed away. MRSA swabs were taken from a wound and nose in 2018 and 2019 and all tested positive at the Freeman Hospital. Patient Harm This patient was admitted to hospital on 11 April 2019 and unfortunately passed away. The MRSA bacteraemia does not appear to have been a factor in the outcome for this patient. Potential gaps in care This patient had been seen by an oncologist in Harley Street. A letter was received by the GP practice referring to the swab taken on 1 April 2019 as tested MRSA positive. Factor that may have contributed to the MRSA bacteraemia is:
• No eradication treatment was prescribed for the positive MRSA swab; this might have led to this episode of bacteraemia.
OFFICIAL
20190925 UC Agenda item 7 Appendix 1 & 2 Performance and Quality Exceptions 25
However, it is unlikely that the eradication therapy would have changed the final outcome of this patient. Case 3: This patient arrived at NSECH on 12 May 2019 with muscle spasm. Blood culture was taken and reported MRSA positive on the 15 May 2019. There was a previous episode of care shortly before this incident and this lady was admitted to the NESCH from 30 April to 3 May with suspected cellulitis. Patient Harm This patient was admitted to the hospital and then discharged back to the community to a nursing home. Potential gaps in care One factor may have contributed to the MRSA bacteraemia:
• The full MRSA routine screening had not been carried out by NHCFT on admission in April 2019. No skin or nose swabs were taken, and this would help to identify if MRSA was present and if so, the necessary treatment could have been provided. The current episode of bacteraemia might be a consequence of this.
Summary This patient impact report is a first, and it is envisaged that it will evolve to reflect the CCG’s approach in assessing the potential harm to patients over time. This report has provided a baseline and highlighted potential areas for further development. Where there is a statutory process in place to track and assess harm, e.g. SI and post infection review, the CCG is more able to measure the impact on patients as a consequence of delays or breaches against the quality and/or performance standards. However this process only covers a very small number of people when compared to the total number of patients affected. It is also worth noting that only those with significant harm are included. If the CCG wishes to receive assurance on all or more patients affected with low or medium level of harm, an additional system will need to be established locally with the providers together. However where a large number of patients are affected such as ambulance response time, the implementation of such a system would be extremely challenging and perhaps impossible. Members of the CMB are asked to discuss the approach going forward to assess the harmful impact of underperformance on residents in Northumberland. Feedback and comments will help to shape the format and inform the contents of future reports.
Agenda Item 8
OFFICIAL
1 20190925 UC Agenda Item 8 Rothbury Community Hospital Report
Clinicians commissioning healthcare for the people of Northumberland
Meeting title Governing Body
Date 25 September 2019
Agenda item 8
Report title Rothbury Community Hospital Report
Report author Senior Head of Commissioning
Sponsor Chief Operating Officer
Private or Public agenda
Public
NHS classification Official
Purpose (tick one only)
Information only
Development/Discussion
Decision/Action
Links to Corporate Objectives Ensure that the CCG makes best use of all available resources
Ensure the delivery of safe, high quality services that deliver the best outcomes
Create joined up pathways within and across organisations to deliver seamless care
Deliver clinically led health services that are focused on individual and wider population needs and based on evidence.
Northumberland CCG/external meetings this paper has been discussed at:
Various including Governing Body, OSC, Rothbury Engagement Group Meeting, meetings with providers and campaigners.
QIPP N/A but a new model will add financial pressure unless it can be mitigated by risk share and increased efficiencies.
Risks Strategic Risk 1505 – Service Commissioning and 451 Provider delivery
Resource implications TBC

OFFICIAL
2
20190925 UC Agenda Item 8 Rothbury Community Hospital Report
Consultation/engagement Engagement process already underway and will be ongoing. OSC decision in September was not to consult on the new model.
Quality and Equality impact assessment
Attached
Research Further detail on the new model will be required. Legal implications Linked to CCG’s statutory duties to involve and meet needs of
whole population included those with protected characteristics. Impact on carers New model will consider the needs of carers. Sustainability implications Depends on the new model.

OFFICIAL
3
20190925 UC Agenda Item 8 Rothbury Community Hospital Report
QUALITY and EQUALITY IMPACT ASSESSMENT 1. Project Name Rothbury Community Hospital
2. Project Lead Director Lead Project Lead Clinical Lead Chief Operating Officer
Senior Head of Commissioning Clinical Lead for pathway development
3. Project Overview & Objective
Governing Body asked to recommend the development of the new model – detailed Quality andEquality Impact analysis will be undertaken as part of the next steps.
4. Quality Impact Assessment
Impact Details Pos/ Neg
C L Scores
Mitigation / Control
Patient Safety N/A Clinical Effectiveness N/A Patient Experience N/A Others including reputation, information governance and etc.
5.Equality Impact Assessment
Impact Details Pos/ Neg
C L Scores
Mitigation / Control
What is the impact on people who have one of the protected characteristics as defined in the Equality Act 2010?
N/A
What is the impact on health inequalities in terms of access to services and outcomes achieved for the population of Northumberland? (which is in line with the legal duties defined in the National Health Service Act 2006 as amended by the Health and Social Care Act 2012), for example health inequalities due to differences in socioeconomic circumstances?
N/A
6. Research Reference to relevant local and national research as appropriate.
NA

OFFICIAL
4
20190925 UC Agenda Item 8 Rothbury Community Hospital Report
7. Metrics Sensitive to the impacts or risks on quality and equality and can be used for ongoing monitoring.
Impact Descriptors Baseline Metrics Target
8. Completed By Signature Printed Name
Date
Senior Head of Commissioning
R Mitcheson
18/7/2019
Additional Relevant Information:
8. Clinical Lead Approval by Signature Printed Name
Date
Additional Relevant Information:
9. Reviewed By Signature Printed Name
Date
Comments

OFFICIAL
5
20190925 UC Agenda Item 8 Rothbury Community Hospital Report
Governing Body 25 September 2019 Agenda Item: 8 Rothbury Community Hospital Sponsor: Chief Operating Officer
Purpose The purpose of the report is to provide an update to Governing Body (GB) on the progress made following Northumberland County Council’s (NCC) Health and Wellbeing Overview and Scrutiny Committee (OSC) held on the 3 September 2019, and confirm GB’s support regarding the development of a new model within Rothbury Community Hospital. Background Since the closure of the Rothbury Community Hospital beds in September 2016, the local population, supported by the Save Rothbury Hospital Campaign Group and local Councillors, have been consistently clear that there is an ongoing need for a vibrant hospital at Rothbury and that this needs to include a number of beds. NHS Northumberland Clinical Commissioning Group (CCG) and Northumbria Healthcare NHS Foundation Trust (NHCFT) have worked with a small group to relook at the model for the hospital considering both the judgement of the Independent Reconfiguration Panel (IRP) and the genuine challenges of care provision in this vibrant, yet very rurally isolated, area.
Members of the Governing Body are asked to:
1. Consider the outcome of the Northumberland Health and Wellbeing Overview and Scrutiny Committee (OSC) meeting on the 3 September 2019.
2. Agree to a joint letter in response to the Secretary of State (SOS) and Independent Reconfiguration Panel (IRP) from NHS England (NHSE), Northumberland Clinical Commissioning Group (CCG) and OSC.
3. Recommend that the Rothbury proposal begins its mobilisation phase including – • Agreement for the clinical senate works alongside Northumbria Healthcare
NHS Foundation Trust (NHCFT) during the mobilisation phase to independently advise on the sustainability of the model for the future including staffing; and the contracting, performance and quality metrics required for the successful delivery of the model.
• Fully developed Equality and Quality Impact Assessment of the new model. • Continued engagement with the local community.
4. Invite NHCFT to present the business case including a detailed staffing model and financial plan prior to the commencement of the new model.

OFFICIAL
6
20190925 UC Agenda Item 8 Rothbury Community Hospital Report
GB was presented with the comprehensive assessments and outcomes from the work of the CCG, the wider care system and Rothbury Engagement Group’s integrated working on the future model of care for Rothbury Community Hospital, at the August extraordinary GB meeting. The work follows the recommendations made by the Secretary of State (SoS) and IRP and which is overseen by OSC Rothbury Review Group. Following GB’s approval in August, the CCG and NHCFT presented the new model to OSC on 3 September 2019. Appendix 1 includes the report to OSC. OSC update The CCG asked OSC to consider the following points:
• To agree that the CCG and wider system has met all requirements related to the process as stated within the letter from the SoS and IRP
• To support the proposed new model presented by NHCFT to further develop the services available within Rothbury and include a new bed model for both step up and step down beds and palliative care
• To indicate whether the proposal constitutes a substantial change that requires consultation, or is not considered a substantial change.
NHCFT presented a new model of care highlighting the new model will include the following:
• A comprehensive hospital to home pathway including discharge to assess (assessments undertaken at home with agreed support packages post discharge for those that are assessed as requiring additional support
• A flexible bed model to support local people to avoid admission to acute hospitals and to offer short term rehabilitation and specialist end of life care
• Additional outpatient clinics both face to face and virtual using the most advanced and secure technology.
OSC were positive with the progress made by the Rothbury engagement group and encouraged ongoing engagement through the operationalising of the model. OSC were supportive of the new model, although requested a further update once more detail around the flexible bed model especially assurance around recruitment and sustainability of the new team. OSC agreed that the CCG had met its requirements relating to the SOS and IRP and agreed to a joint letter from both the OSC and the CCG in response. OSC finally agreed that the change was not substantial and that a consultation was therefore not required. Next Steps The CCG and NHCGT are very keen to continue to engage with the local community in the co design phase of the new model. The next steps in this process will be discussed and shared

OFFICIAL
7
20190925 UC Agenda Item 8 Rothbury Community Hospital Report
at the Rothbury engagement group at the end of September. At this meeting, NHCFT will set out their proposed action plan for operationalising of the new model in preparation for starting in April 2020. The Clinical senate has agreed to support the CCG in providing independent advice regarding the sustainability of the model for the future including staffing; contracting, performance and quality metrics required for the successful delivery of the model. NHCFT will develop the full business case for the new model in preparation for commencement in April 2010. Conclusion The next steps in this process are for NHCFT to further develop the new model of care including an action plan detailing the work to be completed which will feed into the business case in preparation to start in April 2020. The CCG will monitor progress and involve the clinical senate for assurance and advice through the mobilisation phase. The CCG and NHCFT will continue to engage with the local community and Councillors to ensure the model is codesigned and meets the needs of the community. OSC and the CCG will jointly respond by letter regarded the successful completion of the requirements set out by the SOS and IRP. Recommendation GB are asked to:
• Agree to a joint letter in response to the SOS and IRP from NHSE, CCG and OSC due to all requirements relating to the process being met and all parties in agreement.
• To recommend that the Rothbury proposal begins its mobilisation phase including: o Agreement for the clinical senate works alongside NHCFT during the mobilisation
phase to independently advise on the sustainability of the model for the future including staffing; and the contracting, performance and quality metrics required for the successful delivery of the model
o Fully developed Equality and Quality Impact Assessment of the new model o Continued engagement with the local community.
GB are asked to invite NHCFT to present the full business case prior to commencement of the new model. This will include:
o Confirmed staffing model o Contractual arrangements with partners o Finalised financial plan
Appendix 1: The Northumberland Health and Wellbeing Overview and Scrutiny Committee Report – 3 September 2019.
1
Northumberland Health and Wellbeing Overview and Scrutiny Committee Report
Rothbury Community Hospital
3rd September 2019
Purpose
The purpose of the report is to provide an update to The Health and Wellbeing Overview and Scrutiny Committee (OSC) regarding the progress made by the Rothbury Engagement Group, led by Northumberland Clinical Commissioning Group (CCG), and to request the committee’s views, guidance and comments on the following: To agree that the CCG and wider system has met all requirements related to the process
as stated within the letter from the Secretary of State (SoS) and Independent Reconfiguration Panel (IRP).
To support the proposed new model presented by Northumbria Healthcare Foundation Trust (NHCFT) to further develop the services available within Rothbury and include a new bed model for both step up and step down beds and palliative care.
To indicate whether the proposal constitutes a substantial change that requires consultation, or is not considered a substantial change.
Background
Since the closure of Rothbury Community Hospital beds in September 2016 the local population, supported by the Save Rothbury Hospital Campaign Group and local Councillors, have been consistently clear that there is an ongoing need for a vibrant hospital at Rothbury and that this needs to include a number of beds. The CCG and NHCFT have worked with a small group to relook at the model for the hospital considering both the judgement of the IRP and the genuine challenges of care provision in this vibrant, yet very rurally isolated, area. This report provides an update from the comprehensive assessments and outcomes from the work of the CCG, the wider care system and Rothbury Engagement Group’s integrated working on the future model of care for Rothbury Community Hospital. The work follows the recommendations made by the SoS and IRP and which is overseen by OSC Rothbury Review Group. Approach to engagement and the work of the Rothbury Engagement Group The CCG and its system partners, including members of the community and campaign group, have developed a robust engagement framework with the Rothbury Engagement Group and the principles of co-design wherever possible at its heart. The Group is chaired by an experienced independent Chair and is made up of the Save Rothbury Hospital Campaign Group, Healthwatch Northumberland, a county councillor, parish councillors, patient participation group members, a member of the National Community Hospital Association as well as the CCG and NHCFT. Clinical and social care experts have also joined the group.

2
The CCG has built in as much independence as possible so, in addition to the engagement group’s independent Chair, the CCG has also included the following:
Advice from the Consultation Institute on the process; this has included the last Governing Body development session delivered by the Institute as well as advice to meet our legal and statutory duties as a CCG with regard to involvement
Independent analysis of the data by Price Waterhouse Cooper (PwC)
Independent clinical audit of 150 patients by NHS England’s Clinical Senate. The work programme for the six months of the group has covered so far:
Date Focus Areas
16 April 2019 Setting principles of working, group expectations, work areas and timelines, essential background information required
20 May 2019 Discussion of data packs requested including public health, community services, bed occupancy and travel analysis
21 June 2019 Community Asset discussion and preparation for an update to OSC; also established subgroups for data analysis and community assets (if required)
31 July 2019 PwC presentation of independent data analysis, social care data analysis and discussion and a presentation on the Strategic Vision for Rothbury
27 August 2019 Clinical Senate Audit report and findings, patient experience and NHCFT proposal for the future of Rothbury Hospital. Also preparation for the 3 September OSC meeting
September 2019 date TBC
Next steps depending on the outcome of the August Rothbury Engagement Group Meeting, CCG Governing Body and the September OSC meeting outcomes
In addition to this work, individual sessions with members of the group have taken place alongside communication with parish councils and other local patient participation groups. NHCFT has also been testing ideas for the art of the possible with Rothbury Hospital Campaign Group members, prior to the full proposal development being presented to the Rothbury Engagement Group on 27 August 2019 and the CCG’s Governing Body on 28 August 2019. Both meetings were positive about the new model of care. The engagement group supported the model and agreed to continued engagement with the development of the proposal. The CCG’s Governing Body recommended the new model for approval subject to OSC’s consideration of the proposal, agreement from NHS England’s clinical senate working alongside NHCFT during the mobilisation phase to independently advise on the sustainability of the model for the future and receiving a fully developed Equality Impact Assessment of the new model. The presentation is attached as appendix 1

3
Findings from the groups work 1. Community Asset Mapping The Public Health Team based in the Local Authority produced a Community Asset map of the Rothbury area. The fundamental feeling of the engagement group was that Rothbury is already an extremely vibrant community and the community asset mapping merely proves this to be the case, although members acknowledged that it is important to assess for any gaps in provision. A subgroup to look further at this area was not deemed to be necessary. 2. PwC Independent Data Analysis
PwC, whose team was commissioned to analyse the data, presented its results in the first instance to the Data Subgroup for detailed scrutiny on 26 July 2019 and then subsequently to the wider Rothbury Engagement Group on 31 July 2019. Please note PwC used a dataset of all Northumberland residents for comparisons where possible and focused on the period of 2016 to date. The PwC scope was to independently analyse and comment on trends both before and after the Ward was suspended, in relevant data as sourced (directly or indirectly) from the CCG, NHCFT, Northumberland County Council, the Office for National Statistics, TomTom, and the Health Evaluation Data system. PwC’s conclusions relate purely to findings arising from the agreed analyses, including how the data and trends have (or have not) changed since the CCG’s original decision to suspend the Ward. The report outlined six key findings: 1. Despite the suspension of the Rothbury ward, availability at surrounding community
hospitals has not suffered – with no indication of increasing occupancy levels
2. There has been an overall 13% decrease in total admissions to community wards in Northumberland since 2016. Although there were increased admissions to Alnwick of 19%, this does not account for the level of admissions previously seen at Rothbury i.e. Alnwick would have seen a 40% increase not 19%
3. There has also been a decrease in the provision of community inpatient palliative care provision in Northumberland since 2016
4. The average rate of acute admissions per person aged 65 plus has increased by 35% across Northumberland. Rates of emergency re-admissions have increased for 65 plus except for those patients registered to the Rothbury GP practice which have decreased
5. District Nursing visits have continued to increase following the suspension of the ward (but not through increased numbers of nurses, rather each nurse doing more visits)
6. At the time of the initial decision to suspend the ward, it was noted that travel for patients local to the ward would increase to reach alternative inpatient wards and this finding remains the case.
The scrutiny given to PwC and the report at the data subgroup meeting was extremely challenging and key concerns outlined by some engagement group members related to the demographics, patient activity data, validity of midnight occupancy data, and the analysis of district nursing and travel.

4
3. Social Care and Continuing Healthcare Analysis In the 30 months before and after the suspension of the ward, there has been an increase in the number of short break stays which was a direct result of home care being unavailable until the new contract arrangements came into force. In April 2019, further funding has been allocated especially into rural areas. There was also an increase in the use of the short term support service which has now decreased as a result of the new contract. 4. Clinical Senate Report and Findings The CCG’s request of the Northern England Clinical Senate was to: “give independent clinical advice to Northumberland CCG, inform the development of a new model of care / new pathways of care for the residents of Rothbury and surrounds and provide clinical assurance on the final short-listed option(s) for the service model” The Northern England Clinical Senate agreed to provide this independent clinical advice in two stages: 1. A clinical audit of the care received by patients from the Rothbury and surrounding area during the time the inpatient beds at Rothbury Community Hospital were closed
2. Independent clinical review and / or clinical due diligence of the revised option/options for services for the patients Rothbury and surrounding that the CCG will produce, informed by the clinical audit alongside other engagement, analysis and development work carried out or commissioned by the CCG in partnership with NHCFT.
Of 155 case notes reviewed 9 (5.8%) of the patients were considered to have been suitable for a period of in-patient rehabilitation at Rothbury Community Hospital. The audit of all admissions over the age of 65 years, and only non-elective admissions aged over the age of 65, yielded similar results in terms of the number of patients who would likely have used the facility had it been available between 1 April 2018 and 30 April 2019. Rothbury Hospital Proposal NHCFT The vision is to create a vibrant, fully integrated exemplar of rural health and care provision delivering person-centred care in people’s homes and community with access to hospital beds for end of life support and short term rehabilitation for prevention of acute admission and transitioned support to independent living. The aim is to: • Improve the health and wellbeing of the population
• Find the solution to the challenges from within Coquetdale harnessing the excellent community offer already available
• Develop a flexible bed model that supports the local population at times of greatest need allocating resources in ways that promote health, wellbeing and independence
• Support the development of a fully integrated rural health and social care service model for Coquetdale through a new and innovative partnership between health and care providers, the community and wider third sector and educational partners

5
This new model will require continued engagement with local people to develop and support the delivery of a sustainable model for the future that enhances the current provision and develops a flexible bed model. The proposal is that we design this collectively over the next 3-4 months but NHCFT are confident that this model can be delivered locally. The following are proposed as part of this model: • A comprehensive hospital to home pathway including discharge to assess (assessments
undertaken at home with agreed support packages post discharge for those that are assessed as requiring additional support
• A flexible bed model to support local people to avoid admission to acute hospitals and to offer short term rehabilitation and specialist end of life care
• Additional outpatient clinics both face to face and virtual using the most advanced and secure technology.
If this proposal is supported then NHCFT, the CCG and local representatives will work together to prepare a plan of action and a business proposal that will be adopted by the CCG and NHCFT (with named partners) to ensure the funding for this proposal is secured. This planning exercise will firm up a delivery date for commencement of the new model but it is anticipated that, with early agreement, most components of this model could be operational by April 2020 allowing for staff recruitment time and detailed planning.
Meeting the Secretary of State, Independent Reconfiguration Panel and OSC Rothbury Review Group recommendations Attached in Appendix 2 is a detailed breakdown of all activity related to the delivery of the SoS and IRP recommendations and timelines. The view of the CCG is that it has met or is in the process of meeting all of the recommendations required and would like to work together with OSC to write jointly back to the SoS with the CCG once the final proposal is agreed stating that this is the case. The CCG has filed evidence for every area of action as required. NHS England also has a role in assessing that the CCG has met its responsibilities in this regard and will make its own assessment.
Conclusion The work of the Rothbury Engagement Group led by the CCG with contribution from all partners has worked well in evaluating all the assessments undertaken since the group started meeting in April 2019. NHCFT’s new model of delivering flexible beds and additional other services provided as part of the health and wellbeing centre, has been well received by all stakeholders and the local community. It is acknowledged that further details around how this model will be operationalised is needed as well as continued engagement with the local community. The new model of delivering flexible beds within Rothbury Community Hospital has been approved by both the Rothbury Engagement Group and the CCG’s Governing Body. The report covers the recommendations and timelines of the SoS and IRP and demonstrates how the CCG has met these requirements. The CCG and NHCFT are committed to continue to work with the local community and stakeholders in the further development of the model.

Agenda Item 9.1
OFFICIAL
1 20190925 UC Agenda Item 9.1 Director of Public Health Update
Clinicians commissioning healthcare for the people of Northumberland
Meeting title Governing Body
Date 25 September 2019
Agenda item 9.1
Report title Director of Public Health Update
Report author Director of Public Health
Sponsor Director of Public Health
Private or Public agenda
Public
NHS classification Official
Purpose (tick one only)
Information only
Development/Discussion
()
Decision/Action
Links to Corporate Objectives Ensure that the CCG makes best use of all available resources
()
Ensure the delivery of safe, high quality services that deliver the best outcomes
()
Create joined up pathways within and across organisations to deliver seamless care
()
Deliver clinically led health services that are focused on individual and wider population needs and based on evidence.
()
Northumberland CCG/external meetings this paper has been discussed at:
The DPH Annual Report has been discussed at Health and Wellbeing Overview and Scrutiny and the Health and Wellbeing Board
QIPP N/A Risks N/A Resource implications Accepting the recommendations in elements of this report will
result in changes in resource allocation. Consultation/engagement N/A

OFFICIAL
20190925 UC Agenda Item 9.1 Director of Public Health Update 2
Quality and Equality impact assessment
No formal quality and equality impact assessment undertaken but the report on inequalities is specifically written to provide recommendations on how inequalities can be addressed
Data Protection Impact Assessment
N/A
Research N/A Legal implications The Equality Act 2010 and the Health and Social Care Act 2012
both outline the responsibilities and duties of the CCG with respect to identifying, mitigating and addressing inequalities, the topic of one section of this report.
Impact on carers Not specifically considered but should be positively impacted by CCG work to address inequalities.
Sustainability implications A social value framework should seek to improve social value, one component of which is minimising the impact on the environment.

OFFICIAL
20190925 UC Agenda Item 9.1 Director of Public Health Update 3
QUALITY and EQUALITY IMPACT ASSESSMENT 1. Project Name DPH Update – 1. Health Inequalities in Northumberland; 2. Director of Public
Health Annual Report 2018 – Mental Wealth 2. Project Lead Director Lead Project Lead Clinical Lead
Director of Public Health
Director of Public Health
3. Project Overview & Objective
To provide an update to the Board on health inequalities in Northumberland; and a summary of the Director of Public Health’s Annual Report 2018 – focussing on mental health and wellbeing.
4. Quality Impact Assessment
Impact Details Pos/ Neg
C L Scores
Mitigation / Control
Patient Safety N/A Clinical Effectiveness N/A Patient Experience N/A Others including reputation, information governance and etc.
5.Equality Impact Assessment
Impact Details Pos/ Neg
C L Scores
Mitigation / Control
What is the impact on people who have one of the protected characteristics as defined in the Equality Act 2010?
N/A
What is the impact on health inequalities in terms of access to services and outcomes achieved for the population of Northumberland? (which is in line with the legal duties defined in the National Health Service Act 2006 as amended by the Health and Social Care Act 2012), for example health inequalities due to differences in socioeconomic circumstances?
N/A
6. Research Reference to relevant local and national research as appropriate.
7. Metrics Sensitive to the impacts or risks on quality and equality and can be used for
Impact Descriptors Baseline Metrics Target

OFFICIAL
20190925 UC Agenda Item 9.1 Director of Public Health Update 4
ongoing monitoring. 8. Completed By Signature Printed
Name Date
Director of Public Health
E R Morgan
16/09/19
Additional Relevant Information:
8. Clinical Lead Approval by Signature Printed Name
Date
Dr David Shovlin
Additional Relevant Information:
9. Reviewed By Signature Printed Name
Date
Comments
OFFICIAL
20190925 UC Agenda Item 9.1 Director of Public Health Update 5
Governing Body 25 September 2019 Agenda Item: 9.1 Director of Public Health Update – Health Inequalities in Northumberland; Director of Public Health Annual Report 2018 – ‘Mental Wealth’ Sponsor: Director of Public Health
Members of the Governing Body are asked to: 1. Consider the report on health inequalities in Northumberland and provide comment. 2. Endorse the recommendations. 3. Agree to operationalise the recommended actions within NHS Northumberland
Clinical Commissioning Group’s 2020/21 Operational Plan and other place-based plans.
4. Consider the Director of Public Health Annual Report 2018 and comment on the CCG’s contribution to the recommendations.
Health Inequalities in Northumberland
Background Health inequalities are systematic variations in health variables according to social and demographic variables. Health inequities are health inequalities that are unfair, potentially avoidable and socially produced. However, the term ‘health inequalities’ is frequently used to mean health inequities and will be used as such in this paper. Health inequalities may occur in association with differences in ‘protected characteristics’ under the Equality Act 2010 (age, disability, gender, gender assignment, pregnancy or maternity, race, religion or belief, sexual orientation, or marriage or civil partnership), or between an excluded or vulnerable group or small population (e.g. street sex workers, rough sleepers) and the rest of the population. Health inequalities also occur between different socio-economic groups (with more deprived groups experiencing worse health) and between different geographical areas (rural compared to urban, and north compared to south of England). Why are health inequalities important? In addition to the ethical principle of justice and the legal and policy imperatives (see below) to reduce health inequalities, there are four reasons why reducing health inequalities is important. First, there is a large body of evidence that, in countries with large socioeconomic inequalities, not only are there marked health inequalities, but everybody’s health is worse. Second, socioeconomic inequalities in morbidity and multimorbidity are driving demand in the NHS and social care rather than just age - see Figure 1. Third, health inequalities are associated with

OFFICIAL
20190925 UC Agenda Item 9.1 Director of Public Health Update 6
higher costs, accounting for an estimated £4.8 billion in hospital admissions alone. The higher burden of disease means that women living in the most deprived neighbourhoods cost the NHS 22% more per person than women living in the least deprived neighbourhoods, despite having shorter life expectancy (or £400 per person per year in secondary care costs). Fourth, as an economy we experience reduced productivity and wealth if people develop disabilities (that prevent work) before pension age due to their socioeconomic circumstances. The Marmot Review estimated that health inequalities cost society £31 billion in lost production, in 2010 prices. Figure 1.
CCG responsibilities and policy context Under the Public Sector Equality Duty (PSED) of the Equality Act 2010, CCGs are expected to understand the potential effect of policies and practices on people with protected characteristics (as above), especially in relation to their health outcomes and the experiences of patients, communities and the workforce, and to advance equality of opportunity between people who share a protected characteristic and those who do not. The NHS Constitution states that the NHS has a duty to “…pay particular attention to groups or sections of society where improvements in health and life expectancy are not keeping pace with the rest of the population”. This is reflected in the National Health Service Act 2006 as

OFFICIAL
20190925 UC Agenda Item 9.1 Director of Public Health Update 7
amended by the Health and Social Care Act 2012, which introduced for the first-time legal duties to reduce health inequalities, with specific duties on CCGs and NHS England. In particular, CCGs have a duty to have regard to the need to reduce inequalities between patients in access to health services and the outcomes achieved. This applies to any group experiencing health inequalities. The NHS Long Term Plan makes a commitment to base 5-year funding allocations to local areas on a more accurate assessment of health inequalities and unmet need. The Plan itself sets an expectation that CCGs will set out specific measurable goals and mechanisms by which they will contribute to narrowing health inequalities over the next five and ten years, although the Implementation Framework places this responsibility at the level of the Integrated Care System. The Industrial Strategy sets a challenge to increase Disability Free Life Expectancy by at least 5 years by 2035, while reducing the gap between the richest and poorest. The government’s recently published Prevention Green Paper focuses on improving and maintaining good health through prevention, prediction of disease and early personalised interventions. The overall aim of the Northumberland Joint Health and Wellbeing Strategy is to maximise wellbeing and health and reduce inequalities. The four strategy themes were deliberately chosen because of their impact on health inequalities:
• Giving children and young people the best start in life • Empowering people and communities • Tackling some of the wider determinants of health • Adopting a whole system approach to health and social care.
Health inequalities in Northumberland As in England, the gap in life expectancy between the most and least deprived area in Northumberland is increasing, in particular for females. A girl born to parents living in Ponteland South with Heddon can expect to live almost 14 years longer than one born in Cowpen. Figure 2 shows the causes of death and age groups which are driving the gaps in life expectancy within Northumberland, many of which are preventable.

OFFICIAL
20190925 UC Agenda Item 9.1 Director of Public Health Update 8
Figure 2.
Health is not just about length of life, but also quality of life. The gap in healthy life expectancy (years lived in good health) at birth for females is even higher between these two wards at 21 years. People living in more deprived areas of Northumberland suffer the double disadvantage of not only living shorter lives, but also living longer in poor health (see Figure 3). For many, this means poor health before the rising pension age, resulting in poor productivity and compounding inequalities.

OFFICIAL
20190925 UC Agenda Item 9.1 Director of Public Health Update 9
Figure 3. Scatterplot ‘Marmot’ graph of index of multiple deprivation (IMD) rank (x axis) and life expectancy and healthy life expectancy at birth (y axis) by electoral ward in Northumberland. Socioeconomic inequalities are not only seen in health outcomes but also in smoking prevalence, uptake of cancer screening, stage at diagnosis of lung cancer, and specialist referral for some conditions. Despite considerably higher burden of disease and consultation rates in general practices in more deprived areas, practice funding is not distributed to take this into account in England or Scotland. Northumberland also has one of the highest socioeconomic inequalities in unplanned hospital admissions in England as illustrated in Figures 4 and 5.
Figure 4.

OFFICIAL
20190925 UC Agenda Item 9.1 Director of Public Health Update 10
Figure 5. Reducing health inequalities is possible An evaluation of the English health inequalities strategy concluded that “a comprehensive strategy characterised by an increase in social investment targeted at the most deprived parts of the country, in conjunction with high level commitment from across government departments backed up by national targets, could be effective at reducing geographical health inequalities.” The strategy was associated with a decline in geographical inequalities in life expectancy, reversing a previously increasing trend. Whilst this was a national strategy which coincided with a period of economic prosperity (1997 to 2010), it demonstrates that system leadership and disproportionate investment can be effective. Actions and approaches by the CCG and NHS to reduce health inequalities Focus on the wider determinants of health and ‘place’ To effectively reduce health inequalities, it is important to start with a clear conceptual framework which analyses the causes, and opportunities for action. Figure 6 (adapted from Labonte models) encapsulates the different factors that impact our health, where they stem from (the wider determinants of health), how they interact, multiply, reinforce and act both in sequence and simultaneously. Acting on one factor is likely to provide only a partial and incomplete response to the situation.

OFFICIAL
20190925 UC Agenda Item 9.1 Director of Public Health Update 11
Figure 6. Patterns of risk affecting health and wellbeing
Interventions to address the wider determinants of health require a focus on place as well as people. Crucially, interventions that solely rely on individual behaviour change are likely to widen inequalities. While action on behaviours and conditions is a necessary part of the solution to reduce health inequalities, these need to be addressed within the context of their root causes in the wider determinants of health. Although healthcare may contribute as little as 10% to population health and wellbeing, the NHS has a huge role to play in addressing both behavioural risk factors and the wider determinants of health. The population intervention triangle and system leadership and planning Because of the complexity of health inequalities, a place-based approach requires system leadership and planning across civic (local authority), service (NHS and social care) and community sectors. However, it is joint working across the interfaces between the civic, service and community sectors that enables “the whole to become more than the sum of its parts” - see Figure 7. Place-based approaches therefore not only need senior representation from local authority, health and related services, and the voluntary, community and social enterprise (VCSE) sector, but also strengthening of the ‘seams’ between different sectors:
• Strengthening community action: supporting local communities to become more empowered and resilient, and to enable them to support individuals and families to take more control of their own wellbeing and health.

OFFICIAL
20190925 UC Agenda Item 9.1 Director of Public Health Update 12
• Service engagement with communities: building on the structures, relationships and links of partners to engage the seldom-heard, vulnerable groups and break down barriers to participation.
• Civic and service integration: clear but shared responsibility and accountability with integrated commissioning, integrated care (including shared electronic records), clear ambitions and goals with consequences.
Figure 7.
Use of scarce resource As illustrated above, current funding formulas for primary care fail to adequately resource areas with higher levels of deprivation that have higher demand for primary care and unplanned secondary care. Although the NHS Long Term Plan makes a commitment to review funding, the Northumberland system should identify alternative mechanisms to shift resources to address the levels of need for specific communities or populations and achieve more equitable outcomes for all. In addition to this, in order to reduce health inequalities, the Northumberland system will need to move care out of hospital; invest more in prevention; and invest more in primary care. In keeping with the focus on wider determinants, resources should be maximised to support early years (including for maternity health improvement interventions and child development) and support for good employment.

OFFICIAL
20190925 UC Agenda Item 9.1 Director of Public Health Update 13
Using data and evidence effectively Reallocation of resources to reduce health inequalities requires that we obtain and use data on health inequalities. This includes data on existing communities and segmented populations with higher risk of disease, poorer health or higher healthcare usage; and also, data on communities or populations that are less likely to access services or experience poor quality or worse outcomes from services. Combined with evidence of effectiveness of specific interventions, these can be resourced and targeted effectively (when combined with effective community engagement as described above). For example, alcohol brief interventions have been shown to have modestly positive impacts on health and health inequalities when socially targeted. Numerous data sources are available, including PHE Fingertips profiles, Local Health, and Right Care Equality and Health Inequalities Packs as well as routine data sources such as SUS, RAIDR and IAPT data. The current consensus is that universal action is needed (as opposed to a narrow-targeted approach), but with a scale and intensity that is proportionate to the level of disadvantage (proportionate universalism). Asset-based, community-centred approaches Community life, social connections, supportive relationships and having a voice in local decisions are all factors that underpin good health. The assets within communities, including the skills and knowledge, social networks, local groups and community organisations, are building blocks for good health. The ‘family of community-centred approaches’ includes four pillars:
• Strengthening communities: building community capacity to act on health - people coming together to identify local issues, devise solutions, and build sustainable non-service solutions. The Locality Coordinators are currently fulfilling this role as part of the Empowering Communities project.
• Volunteer and peer roles: this includes health trainers as well as health champions and befriending and volunteer schemes such as Health Walks.
• Collaborations and partnerships: involving communities in planning and agreeing priorities. The Locality Coordinators are working with communities to identify priorities for grant funding.
• Access to community resources: connecting individuals to community resources, groups activities, volunteering opportunities and practical support (e.g. benefits advice). This is a key role of the new social prescribing link workers within Primary Care Networks and is also undertaken by a range of other roles such as Support Planners in Adult Social Care.
Social prescribing is a key activity through which commissioner and frontline healthcare professionals can support individuals to address the social and economic determinants of health such as poor housing, poor or under-employment, low income or loneliness. The CCG role goes beyond supporting the PCNs to supporting the VCSE in building capacity in terms of the community resources that individuals can be connected to.
OFFICIAL
20190925 UC Agenda Item 9.1 Director of Public Health Update 14
Health, wealth and social value As well as facilitating social prescribing and sources of benefits and employment advice, the NHS and the local authority as the largest employers in Northumberland, can support the local economy by maximising workplace health and wellbeing (to reduce sickness absence and maintain people in good work); procuring and investing locally; paying living wages; and working collaboratively to increase the employment opportunities for certain groups such as formerly looked after children and people with learning differences or disabilities. The Northumberland Joint Health and Wellbeing Strategy 2018-28 says: “Social Value is about how we spend public funds to produce a wider benefit to the community, be it the social, environmental or economic wellbeing of the people we serve. We think we should develop a social value framework and embed social value considerations into all policies, decisions and public procurement.” The Public Services (Social Value) Act requires public bodies to consider the social good that could come from the procurement of services, before they embark upon the process. These can be measured using the national social value measurement framework. Examples of social value include increasing local employment; preservation of the local high street; promotion of local business; facilitating apprenticeships; and reducing air pollution and burning of fossil fuels. A Joseph Rowntree Foundation analysis of the Leeds City Region found that if ten anchor institutions (including clinical commissioning groups and hospitals) shifted an additional 10% of their total spend locally, this could drive an additional £168–£196 million into the Leeds economy. Advocacy As well as having considerable influence at an individual level with patients in relation to behaviours (e.g. smoking), healthcare professionals and other leaders often underestimate the impact they could have on populations and policy. This could include advocating for increased primary care funding and (re)allocation in favour of more deprived areas; supporting local campaigns to protect green spaces, reject takeaways or promote cycle lanes and active travel to appointments; or lobbying at a national level in favour of alcohol minimum unit pricing or increased investment in public health and child development, or against marketing of high calorie food. GPs in the Scottish Deep End group (a network of GP surgeries which cover the 100 most deprived patient populations) have demonstrated the impact that collaboration and advocacy can achieve. Recommendations Governing Body are asked to:
1. Recognises the role that the NHS should play in addressing the wider determinants of health and as an anchor institution.
2. Strengthens community action, service engagement with communities and collaboration and integration between the NHS, social care, local authority and the VCSE.

OFFICIAL
20190925 UC Agenda Item 9.1 Director of Public Health Update 15
3. Identifies and commits to mechanisms to enable unequal, higher per head NHS funding in more deprived areas.
4. Where possible, invest an increasing proportion of the CCG budget in primary care and prevention, including funding for community-centred approaches (for example, the Locality Coordinators) and the VCSE to build capacity.
5. Systematically collect, share and act on data on health inequalities within the Northumberland population (including inequalities in access, quality and outcomes of services) and use the best available evidence to apply a proportionate universalism approach.
6. Recognise poor housing, financial insecurity, debt and unemployment as determinants of health and prioritise the work of social prescribing link workers accordingly.
7. Work with the other parts of the public sector in Northumberland to develop a social value framework and embed social value considerations into all policies, decisions and public procurement, contributing to the Northumberland economy through local procurement and investment.
8. Become even greater advocates locally and nationally for public health interventions to reduce health inequalities.
DPH Annual Report 2018 – ‘Mental Wealth’ Background Directors of Public Health in England have a statutory duty to write an Annual Public Health Report on the health of the local population; the Local Authority has a duty to publish it. The DPH Annual Report is a vehicle for informing local people about the health of their community, as well as providing necessary information for commissioners and providers of services on health and wellbeing issues and priorities that need to be addressed. This year’s report focuses on mental health and wellbeing. It explains the link between psychology and biology and the pathway that links stress in childhood to poorer health and wellbeing outcomes in the longer term. It takes a life course approach to mental health, exploring some of the protective and risk factors at each stage; where some of the inequalities lie; and what interventions are and could be put in place to protect and promote good mental health and wellbeing. The report concludes with a small number of recommendations on how the Northumberland system can protect and promote mental health and wellbeing. The report is available at: https://www.northumberland.gov.uk/NorthumberlandCountyCouncil/media/Health-and-social-care/Public%20Health/2018-Director-of-Public-Health-Annual-Report-Mental-Wealth.pdf Key issues
• Mental health and wellbeing are critical elements of good health. Those with good mental health and wellbeing are likely to live 10 - 20 years longer than people with a significant mental illness and are less likely to smoke, experience problem drug and alcohol use, be unemployed or have to take time off work. Poor mental health is one of

OFFICIAL
20190925 UC Agenda Item 9.1 Director of Public Health Update 16
the biggest contributors to disability and ill health and in some groups, is a significant cause of early deaths.
• About 1 in 4 people in the UK will experience a mental health problem each year; in England, about 1 in 6 people report experiencing a common mental health problem (such as anxiety and depression) in any given week. Poor mental health imposes a significant cost to society in terms of public services (such as housing, health and social care), the criminal justice system and the economy so there is a social, economic and ethical argument to support good mental health and wellbeing.
• The foundations for good mental health and wellbeing are laid down in the first few months and years after birth. Infant and childhood stress affects physical development which can have health consequences along the whole of the life course. The consequences of Adverse Childhood Experiences on longer term health can now be quantified. Protective factors for good mental health in the early years include secure attachment, family structure, early literacy and access to high quality pre-school education and good maternal health. These are supported by a variety of programmes across the county such as targeted home visiting and parenting programmes, supporting breastfeeding and early identification and support for mothers who may have mental health issues. The importance of the father’s voice and the challenges for new fathers are also highlighted.
• Good mental health and wellbeing in young people is vital for physical wellbeing, educational attainment, successful transition, supporting health promoting behaviours, skills development and employment. Half of all mental disorders are diagnosed before the age of 14; three-quarters by the time a person reaches 25 years; many are undiagnosed until a crisis is reached. Good mental health is promoted by a supportive school environment, supportive families and parenting, and access to a trusted adult. Promoting a whole school approach to good mental health and wellbeing; the Mental Health Trailblazer programme; and the county’s Early Help hubs all contribute to improving mental health and wellbeing in the county’s young people.
• Last year’s annual report highlighted the links between employment and health. Work is increasingly being seen as a health outcome, providing people with a sense of purpose, self-confidence, independence, fulfilment, and social networks as well as an income. Mental ill health is the second highest identifiable reason for sickness absence; 1 in 6 employees in the UK have reported having a mental illness. Supporting people back into work is a priority in Northumberland’s Joint Health and Wellbeing Strategy along with promoting wellbeing interventions in the workplace which reduce sickness absence, improve productivity and reduce staff turnover.
• In older people, mental wellbeing continues to be important and protective factors include retirement (in some people), remaining connected, keeping active and accessing outdoor spaces. Conversely, the risks to poorer mental health and wellbeing also include retirement (in some other people), a decline in physical health, organic disease such as dementia, providing unpaid care and financial stress. Many voluntary and statutory support mechanisms exist across the county to support healthy ageing; the council’s Ageing Well Programme exists to promote health and wellbeing in older people whilst also valuing the skills, experience and energy that older people have to offer.

OFFICIAL
20190925 UC Agenda Item 9.1 Director of Public Health Update 17
• Social connectedness has a key role in achieving good mental health and wellbeing and is estimated to have the same wellbeing benefits as not smoking. In Northumberland, there is plenty of evidence of strong and connected communities and about 1 in 4 residents are involved in formal voluntary work which in itself is associated with better mental wellbeing. Community centred approaches to improving mental and physical wellbeing are already embedded across the county but are being further supported by the Public Health team’s Empowering Communities projects and a commitment in the NHS Plan to make social prescribing more routinely available as an alternative/additional approach to improving wellbeing.
• The report makes a number of recommendations:
o Develop a plan to make Northumberland a county which is more aware of the impact of Adverse Childhood Experiences across the life course;
o Support all schools to adopt a whole-school approach to promoting mental health and wellbeing;
o Prioritise mental wellbeing in the workplace as part of the North East Better Health at Work Award;
o Grow initiatives which increase social connectedness; o Make a cross sector commitment to prevention through the Prevention Concordat
for Better Mental Health. Recommendations Governing Body is asked to consider the Public Health Annual Report 2018 and comment on its contributions to the recommendations.
AGENDA ITEM 9.2
OFFICIAL
1 20190925 UC Agenda Item 9.2 Urgent Care Design Principles
Clinicians commissioning healthcare for the people of Northumberland
Meeting title Governing Body
Date 25 September 2019
Agenda item 9.2
Report title Urgent Care Design Principles
Report author Director of Commissioning
Sponsor Chief Operating Officer
Private or Public agenda
Public
NHS classification Official
Purpose (tick one only)
Information only
Development/Discussion
Decision/Action
Links to Corporate Objectives Ensure that the CCG makes best use of all available resources
Ensure the delivery of safe, high quality services that deliver the best outcomes
Create joined up pathways within and across organisations to deliver seamless care
Deliver clinically led health services that are focused on individual and wider population needs and based on evidence.
Northumberland CCG/external meetings this paper has been discussed at:
None
QIPP Not related to a particular QIPP scheme at this present time Risks Strategic Risk 1178 – System Resilience and Escalation Planning

OFFICIAL
20190925 UC Agenda Item 9.2 Urgent Care Design Principles 2
Resource implications None additional at this time, however, further discussion is required in relation to CCG resources available to deliver the engagement work and strategy development and consideration will be given as to whether additional funding may be required for staffing or engagement materials/venues etc.
Consultation/engagement Informal discussions have taken place with CCG clinical leads, primary care staff in localities, current providers of urgent care services in Northumberland
Quality and Equality impact assessment
Completed
Data Protection Impact Assessment
No
Research https://www.england.nhs.uk/publication/urgent-treatment-centres-principles-and-standards/
Legal implications None Impact on carers Potential positive impact on carers due to improved access and
reduced travel. Sustainability implications None

OFFICIAL
20190925 UC Agenda Item 9.2 Urgent Care Design Principles 3
QUALITY and EQUALITY IMPACT ASSESSMENT 1. Project Name Urgent Care Design Principles
2. Project Lead Director Lead Project Lead Clinical Lead
Chief Operating Officer Director of Commissioning Clinical Lead – Urgent Care
3. Project Overview & Objective
Urgent Care Design Principles
4. Quality Impact Assessment
Impact Details Pos/ Neg
C L Scores
Mitigation / Control
Patient Safety Patient safety will be taken into account throughout the engagement phase and when considering any future service configuration proposals
NA
Clinical Effectiveness Clinical effectiveness will be taken into account throughout the engagement phase and when considering any future service configuration proposals
NA
Patient Experience Patient experience will be taken into account throughout the engagement phase and when considering any future service configuration proposals
NA
Others including reputation, information governance and etc.
5.Equality Impact Assessment
Impact Details Pos/ Neg
C L Scores
Mitigation / Control
What is the impact on people who have one of the protected characteristics as defined in the Equality Act 2010?
The impact on individuals with protected characteristics will be taken into account throughout the engagement phase and when considering any future service configuration proposals
What is the impact on health inequalities in terms
The impact on health inequalities will be

OFFICIAL
20190925 UC Agenda Item 9.2 Urgent Care Design Principles 4
of access to services and outcomes achieved for the population of Northumberland? (which is in line with the legal duties defined in the National Health Service Act 2006 as amended by the Health and Social Care Act 2012), for example health inequalities due to differences in socioeconomic circumstances?
taken into account throughout the engagement phase and when considering any future service configuration proposals
6. Research Reference to relevant local and national research as appropriate.
https://www.england.nhs.uk/publication/urgent-treatment-centres-principles-and-standards/
7. Metrics Sensitive to the impacts or risks on quality and equality and can be used for ongoing monitoring.
Impact Descriptors Baseline Metrics Target Patient experience Satisfaction with service
delivery Positive patient experience ratings
Further metrics will be developed as part of the service configuration proposals and future service specifications
8. Completed By Signature Printed Name
Date
Director of Commissioning
Ailsa Nokes 11/9/19
Additional Relevant Information:
8. Clinical Lead Approval by Signature Printed Name
Date
Additional Relevant Information:
9. Reviewed By Signature Printed Name
Date
Comments

OFFICIAL
20190925 UC Agenda Item 9.2 Urgent Care Design Principles 5
Governing Body 25 September 2019 Agenda Item: 9.2 Urgent Care Design Principles Sponsor: Chief Operating Officer
Members of the Governing Body are asked to: 1. Consider the updated draft of the Urgent Care Strategic Direction and in particular
the proposed Design Principles for future service configuration and provide comment.
2. Approve commencement for wider engagement with patients and partners across localities.
Purpose This report provides a summary of the key themes emerging from the first phase of engagement with partners on the Urgent Care Strategic direction which have been incorporated into a refreshed. It also sets out the proposed Design Principles for future service configuration, which will guide the next phase of engagement and conversations with patients and partners across localities. Background The draft Strategic Direction for Urgent Care in Northumberland has been developed in the context of the overarching vision and strategic objectives of NHS Northumberland Clinical Commissioning Group (CCG). It sets out a vision for a future model of urgent care, which will better meet the needs of the local population, helping reduce some of the complexity and confusion our residents have told us is inherent within the current model. Furthermore it outlines the process that will guide the development of this future model for Urgent Care provision across the county. Central to this is a commitment to collaborative working with stakeholders from across our system in order design the optimal model for urgent care delivery. In the document urgent care (UC) means: A range of health services that people access when they need medical care that cannot wait for a routine appointment with a GP but is not so serious or life-threatening that they require emergency care from the Accident and Emergency (A&E) Department. Accident and Emergency (A&E) also known as the Emergency Department (ED) is not included in this definition as it is a service for immediate or life threatening conditions, or serious injuries or illnesses.

OFFICIAL
20190925 UC Agenda Item 9.2 Urgent Care Design Principles 6
Development of the Urgent Care Strategic Direction The CCG will develop and implement its UC Strategic Direction by working jointly with its system stakeholders. Within this definition we are referring to; individuals and organisations who may be affected by changes which may emerge from the implementation of this strategy. This includes both patients and professionals working in health and social care across the county. The development and implementation of the Strategic Direction will be clinically led throughout. In particular we will ensure that it aligns with the commissioning strategy for General Practice and the emerging development of Primary Care Networks across the county. Key themes from initial engagement work The following are some of the high level themes that have emerged for the early engagement with partners, in light of which we have amended the first draft document:
• Information and self care - Ensure people have access to good quality information that enables them to self manage rather than seeking urgent advice when appropriate.
• NHS 111 and Directory of Service (DOS)- Patients to access urgent care services via NHS111 and appropriate clinical triage, with use of the DOS as an enabler to drive pathways and ensure patients get to the right place, right time, first time.
• Managing expectations - Managing patient’s expectations of what the services are there to provide which conditions requiring urgent same day care.
• Realistic medicine - Health and social care staff to adopt a realistic medicine approach putting the person receiving care at the centre of decisions made about their care.
• Continuity of care - Understanding when same day access in primary care can be used to support patients with urgent care needs, and ensuring wherever a patient presents that there is appropriate access to the patient record and communication regarding care between professionals
• Workforce - Development of a workforce strategy to support the new delivery models of delivery, linking this to the developing Primary Care Strategy for Northumberland. Recognition of the increasing pressure on scarce resources and look to utilise an increasing skill mix through the inclusion of other a range of professionals.
• Role of primary care - Consider the opportunities that Primary Care Networks bring to support the development of primary care hubs and increasing skill mix of professionals to meet locality needs. Build on the new Community Pharmacist contract and Consultation Service to extend further the role of community pharmacy, and consider pathways to community dentists and optometrists.
• Use of technology - Using technology to improve access to services such as through NHS 111 or online patient consultations; to support patients to manage their own condition; enabling care to be patient-centric, not limited by care settings and

OFFICIAL
20190925 UC Agenda Item 9.2 Urgent Care Design Principles 7
organisational boundaries and enabling shared access to the patient care record. Key is direct booking from NHS 111 and between service providers to improve patient flow.
Vision and Design Principles Our overall vision is An integrated urgent care delivery model which is simple for patients and professionals to access, which delivers safe, sustainable, responsive and high quality care meeting national best practice standards, and promotes and supports patients return to health and independence The aim is that within three years the CCG will have commissioned fully integrated, 24/7, seamless urgent care provision across Northumberland. Our vision is simple, for those people with urgent but non-life threatening needs, we must provide accessible, responsive, effective and personalised services, outside of a hospital environment when clinically appropriate. These services should deliver care to the highest standards, and quality of care will be based on nationally and locally agreed outcomes. The urgent care model has primary care at the heart of the service; GP leadership will be central to the development and delivery of this model. Taking the learning from national best practice and evidence, and feeding in the key themes from our engagement work; we propose the following five principles to guide the redesign of urgent care services across Northumberland: 1. Increase self-care through access to good quality information and appropriate clinical
advice 2. Ensure service delivery is appropriate to needs, accessible and responsive 3. Simplify access by improving integration across health and social care and reducing
duplication of services 4. Be safe, sustainable, and provide high quality, care 5. Meet mandated requirements
The following draft objectives of the new model have been developed in light of our engagement and review work to date which will be tested as part of our further engagement work:
• The public will have access to good quality information and guidance in the event of them needing urgent or emergency care
• Patients will be encouraged to use NHS 111 as the central point of access for urgent care advice and triage so that patients can ‘talk before they walk’
• Patients will be seen at the right time, in the right place, by a person with the appropriate skills to manage their needs
• Only patients requiring emergency care will navigate into our emergency care services • Urgent care services will be accessible and responsive

OFFICIAL
20190925 UC Agenda Item 9.2 Urgent Care Design Principles 8
• We will ensure an evidence based approach to commissioning services • Services will be joined up, seamless and co-ordinated • Services will be safe, responsive and a high quality • Real time information, essential to patient care, will be available to professionals
involved in a patients care • We will monitor the quality and experience of urgent care services and ensure
continuing improvement
Next steps The next step is to continue with our engagement programme with patients and partners, to further understand what matters to local people, what the evidence and partners tell us works well and areas for improvement. We are developing a ‘Listening Document’ based on the strategic direction, which incorporates the views and evidence from this first stage, and we will use this to undertake further engagement and ‘listening’, holding open and honest conversations, explaining the challenges the CCG has around urgent care and asking a series of questions the CCG would like to explore. Following consideration of the views heard in the engagement and listening phases, we aim to co-produce proposals for future service configuration in each locality. The results of the above will inform the CCG’s urgent care commissioning intentions and any subsequent procurement required. The previously agreed outline timeline is provided below.
Recommendations Governing Body is asked to consider the updated draft of the Urgent Care Strategic Direction and in particular the proposed design principles for future service configuration and provide comment. Approve commencement for wider engagement with patients and partners across localities. Appendix 1: Draft Strategic Direction for Urgent Care in Northumberland 2019 – 2022.

Strategic Direction for Urgent Care in
Northumberland 2019 - 2022
Clinicians commissioning healthcare for the people of Northumberland

1
Document Version Control
Version Changes Author Date Issued
Status
0.1 Draft document to begin discussions with partners
Ailsa Nokes 18/6/19 Draft
0.2 Diagrams for STB governance and outcome metrics made clearer
Ailsa Nokes 27/6/19 Draft
0.3 Updated to include initial comments made during informal engagement with EMG, CMB and LADB members
Ailsa Nokes 18/7/19 Draft
0.4 Updated to include further comments made during informal engagement with EMG, CMB and LADB members
Ailsa Nokes 10/9/19 Draft
2
CONTENTS
No. Section Page
1 Introduction 3
2 Development of the Urgent Care Strategic Direction 4
3 National Context and Drivers for Change 5
4 Regional Context and Drivers for Change 8
5 Local Context and Drivers for Change 9
6 Vision and Future Service Model 18
7 Enablers and Interdependencies 23
8 Leadership and Governance Arrangements 24
9 Performance Management Framework 26
10 Conclusion 27

3
1. Introduction Northumberland CCG’s (NCCG) Vision is: To ensure that the highest quality integrated care is provided, in the most efficient and sustainable way, by the most appropriate professional to meet the needs of the people in Northumberland. The four strategic objectives that support the achievement of the vision are to:
Ensure that the CCG makes best use of all available resources
Ensure the delivery of safe, high quality services that deliver the best outcomes
Create joined up pathways within and across organisations to deliver seamless care
Deliver clinically led health services that are focused on individual and wider population needs and based on evidence.
This draft Strategic Direction for Urgent Care in Northumberland has been developed in the context of this overarching vision and strategic objectives. It sets out a vision for a future model of urgent care, which will better meet the needs of the local population, helping reduce some of the complexity and confusion our residents have told us is inherent within the current model. Furthermore it outlines the process that will guide the development of this future model for Urgent Care provision across the county. Central to this is a commitment to collaborative working with stakeholders from across our system in order design the optimal model for urgent care delivery. In this document urgent care (UC) means: A range of health services that people access when they need medical care that cannot wait for a routine appointment with a GP but is not so serious or life-threatening that they require emergency care from the Accident and Emergency (A&E) Department. Examples of UC services:
NHS 111
Community Pharmacy
GP Out of Hours
Clinical Hub (Clinical Assessment Service)
Urgent Care Centres and Minor Injuries Units Accident and Emergency (A&E) also known as the Emergency Department (ED) is not included in this definition as it is a service for immediate or life threatening conditions, or serious injuries or illnesses.

4
2. Development of the Urgent Care Strategic Direction NCCG will develop and implement its UC Strategic Direction by working jointly with its system stakeholders. Within this definition we are referring to; individuals and organisations who may be affected by changes which may emerge from the implementation of this strategy. This includes both patients and professionals working in health and social care across the county. The development and implementation of the Strategic Direction will be clinically led throughout. In particular we will ensure that it aligns with the commissioning strategy for General Practice and the emerging development of Primary Care Networks across the county. The following organisations have been, and will continue to be, involved in the development of this draft UC Strategic Direction:
Northumberland CCG
Northumbria Healthcare NHS Foundation Trust
Newcastle Hospitals NHS Foundation Trust
Northumberland, Tyne and Wear NHS Foundation Trust
North East Ambulance Service NHS Foundation Trust (inc NHS 111 & CAS service)
Vocare
Northumberland County Council
GP Practices in Northumberland
Health Watch
North Tyneside CCG
North Tyneside Council
Newcastle Gateshead CCG
North of England Commissioning Support (inc DOS team)
NHS England / Improvement The CCG will continue to engage with these stakeholders individually and formally as part of the following boards:
Northumberland Health and Well Being Board
Northumberland System Transformation Board
Northumberland and North Tyneside Local A&E Delivery Board The Strategic Direction will also continue to be developed in line with relevant national guidance and best practice. Due consideration will continue to be given to the various interdependencies with additional local strategies and programmes, which as an example include:
Northumberland CCG’s Operational Plan 2019/20
Northumberland Joint Health and Well Being Strategy 2018-2028
Northumberland System Transformation Board Health and Care Strategy 2019/20

5
3. National Context and Drivers for Change Across the NHS, staff work 24/7 to deliver the best possible care to more patients than ever before, however, the urgent and emergency care (UEC) system is under real pressure as demand continues to rise. Over recent years there have been a number of national publications re the future direction of UEC in an attempt to help relieve current pressures. All publications have encouraged a move towards simplifying models for UEC in order to reduce confusion inherent within current models. They advocate a move towards responsive and flexible services which are available seven days a week and ensure people who need care get to the right place at the right time. NHS ‘Five Year Forward View’ (NHSE, 2014)1 This set out the need to re-design urgent care services: For those people with urgent but non-life threatening needs we must provide highly responsive, effective and personalised services outside of hospital. These services should deliver care in or as close to people’s homes as possible, minimising disruption and inconvenience for patients and their families The Five Year Forward View vision was for NHS 111 to be embedded within the UC system, providing access to telephone, primary, and community care services which meet peoples’ UC needs as close to home as possible. Most UC will be provided by out of hospital and general practice services, including evening and weekend access to GPs or nurses working from community bases. Services will be integrated and patient centred. Diagram 1 sets out the national shape and structure for a future urgent and emergency care system: Diagram 1:
1 NHS Five Year Forward View. NHS England October 2014

6
Safer, faster, better: good practice document (2015)2 This publication developed the Five Year Forward View making the following distinction:
For adults and children with urgent care needs, we should provide a highly responsive service that delivers care as close to home as possible, minimising disruption and inconvenience for patients, carers and families.
For those people with more serious or life-threatening emergency care needs, we should ensure they are treated in centres with the right expertise, processes and facilities to maximise the prospects of survival and a good recovery.
It highlighted five changes to deliver the Five Year Forward View:
Providing better support for people and their families to self-care or care for their dependants
Helping people who need urgent care to get the right advice in the right place, first time
Providing responsive, urgent physical and mental health services outside of hospital every day of the week, so people no longer choose to queue in hospital emergency departments
Ensuring that adults and children with more serious or life threatening emergency needs receive treatment in centres with the right facilities, processes and expertise in order to maximise their chances of survival and a good recovery
Connecting all urgent and emergency care services together so the overall physical and mental health and social care system becomes more than just the sum of its parts
Integrated Urgent Care Commissioning Standards (2015)3 This sets out the requirements to deliver Integrated Urgent Care (IUC) aiming to:
Deliver a functionally integrated 24/7 urgent care service that is the ‘front door’ of the NHS and which provides the public with access to both treatment and clinical advice. This will include NHS 111 providers and GP Out of Hours services, community services, ambulance services, emergency departments and social care”
For patients unable to access their own GP, because the practice is closed or they are away from home for example, NHS 111 will be the primary route to UC services.
The Directory of Service (DoS) for NHS 111 will hold accurate information across all commissioned acute, primary care and community services and be expanded to include social care. The DoS should reflect locally commissioned schemes and services, especially those intended to utilise independent contractors such as community pharmacists as appropriate alternatives for minor ailments and urgent repeat medication. Health advisers need to be confident in referring or signposting callers to these services, where available.
2 Transforming urgent and emergency care services in England Safer, faster, better: good practice in delivering
urgent and emergency care A guide for local health and social care communities. NHS England 2015 3 Commissioning Standards Integrated Urgent Care. NHS England 2015

7
IUC will have a ‘Clinical Hub’4 offering patients who require it access to generalist and specialist clinicians. It will also offer advice to community health professionals including paramedics, so that no decision is taken in isolation.
The Clinical Hub will be able to access patients’ clinical records. Over time IT system interoperability will support direct appointment booking into other services.
Next Steps on the NHS Five Year Forward View (2017)5
This publication directed the roll out of new Urgent Treatment Centres (UTCs) as an integral part of local urgent care services. The overarching aim of the new UTCs was to standardise the confusing range of options available to the public such as: Walk in Centres, Urgent Care Centres, Minor Injury Units which all have differing levels of service, and simplify the system so that the public and patients are clear on which service is best suits their needs. Since its publication the NHS has:
Rolled out evening and weekend GP appointments nationally, ahead of schedule, so that accessing primary care is easier and more convenient for all patients
Enhanced NHS 111, so over 50% of people calling the service now receive a clinical assessment and can be offered immediate advice or referred to the right clinician for a face-to-face consultation
Achieved 100% of the population now able to access urgent and emergency care advice through the NHS 111 online service
Begun rolling out UTCs across the country, offering a consistent service to patients at 110 locations and introducing the ability to book appointments in UTCs through
The Long Term Plan (LTP) (2019) This plan sets a target for full implementation of the UTC model by Autumn 2020, so that all localities have a consistent offer for out-of-hospital urgent care. This model will include the option of appointments being booked directly through NHS 111. UTCs will work alongside other parts of the urgent care network including primary care, community pharmacists, ambulance and other community-based services to provide a locally accessible and convenient alternative to A&E for patients who do not need to attend hospital. At the same time the LTP maintains investment in primary care, aimed at promoting sustainability in general practice and improving patient care and access. CCGs will continue to commission extra capacity to ensure that everyone has access to GP services, including sufficient pre-bookable and same day appointments at evenings and weekends to meet locally determined demand, as well as access to urgent primary care when GP surgeries are closed.
4 In the North East region the ‘Clinical Hub’ is referred to as the ‘Clinical Assessment Service’ (CAS)
5 Next steps on the NHS Five year forward view. NHS England March 2017
8
4. Regional Context and Drivers for Change Regionally, implementation of the relevant elements of the Five Year Forward View have been taken forward via the Cumbria and North East (CNE) Urgent and Emergency Care Network (UECN). The Network has 4 strategic aims:
System leadership, with an overarching framework to address fragmentation
Promoting self-care among patients
Improving general practice access through GP bookings
Improvements and integration to out-of-hospital care Key areas of focus over the last three years include:
Clinical hub development, including: o clinical advice to members of the public calling NHS 111 o clinical support to paramedics and emergency technicians o clinical support to other health and social care professionals
Digital Care (Information Sharing & Information Governance), including: o sharing patient care records through the Medical Interoperability
Gateway (MIG) o deploying Information Sharing Gateway tool regionally
GP Direct Booking through NHS 111: o direct booking of GP appointments from NHS 111 o accessing general practice data from GP practices to identify trends in
illness
Supporting Self-Care for under 5’s: o develop a smart device application targeted at parents of children aged
under five featuring a body map where users can click parts of the body to reveal a list of symptoms relating to that area and information about common childhood illnesses and the recommended actions signposts parents to the most appropriate health service
o includes a list of NHS services which will be geo-targeted to the user.
Region Wide Communications Plan o development of a system wide social marketing approach o developing activities aimed at changing or maintaining people’s
behaviour o identifying what the public perceive to be key issues around urgent and
emergency care o insight into the experiences of those who have recently accessed
specific health services o understanding the behaviours and motivations which govern how and
why people use specific services

9
5. Local Context and drivers for change Population Need Northumberland’s population is approximately 319,000 (Mid-2017 population estimate, Northumberland County Council JSNA). The map in Diagram 2 below shows the Index of multiple deprivation in Northumberland which includes income, employment, crime, education skills and training, health and disability, barriers to housing and services, living environment. 96.7% of the Northumberland geography is classified as rural. Nationally, only about 19% of the population live in areas classified as rural, nearly 50% in Northumberland live in areas classified as rural. Conversely, the other 50% of the population are in the 3% of the geography in the south east corner. Disproportionately the older population are more likely to live in rural communities. Rurality can affect safe staffing models, recruitment, costs, access; and time and location sensitive care. Diagram 2: Index of Multiple Deprivation in Northumberland

10
Northumberland CCG and its partners through the Health and Well Being Board have continually demonstrated the ability to overcome traditional barriers between organisations and use innovative approaches to improve the quality of care. We want to get to a position where people in Northumberland are living independently for as long as possible with the best health possible, not because that may make our health and care system sustainable, but because it’s the right thing to do for our residents. Over the last few years though there has been an unprecedented increase in the demand on health and social care. Here are a few key facts:
There were almost 114,000 hospital admissions for NHS Northumberland CCG patients in 2018/19
Northumberland County Council currently provides services to 3170 people aged 18-64 years of age and 8175 people 65 years of age or older.
People living in the least deprived areas of Northumberland can expect to spend 16.6 years longer living in good health than people living in the most deprived areas.
Smoking continues to be the biggest cause of preventable ill health but although smoking prevalence in Northumberland is the lowest in the North East, 30% of adults in routine and manual occupations (25.5% in England) and 37.1% of adults with serious mental illness (40.5% in England) still smoke. And 12.9% of pregnant women were reported to be still smoking at time of delivery during 2016/17
Both the rate of hospital admissions for alcohol-related conditions and the total volume of alcohol sold (off-trade) per adult are significantly higher in Northumberland than in England
More than two-thirds (69.8%) of adults living in Northumberland are overweight or obese (2013-15) compared to 64.8% in England; in 2015/16, a third of children in year 6 (10-11 years of age) were overweight or obese.
A quarter (24.3%) of adults in Northumberland are inactive, compared to 22.3% in England.
Current Urgent Care Provision Within Northumberland patients with urgent and emergency care needs can currently access support through a range of services including: NHS 111 and its Clinical Hub (the Clinical Assessment Service (CAS)), two UCCs, four MIUs, the Emergency Department (ED) at Northumbria Specialist Emergency Care Hospital (NSECH), 41 GP practices, Extended Hours in Primary Care, GP Out of Hours service, and 75 community pharmacies. Diagram 3 highlights the spectrum of current provision across

11
Diagram 3: Current services accessed for Urgent and Emergency care needs in Northumberland
Community Pharmacies There are 75 pharmacies in Northumberland, including six 100 hour pharmacies and one internet/distance selling pharmacy. Access to community pharmacies across Northumberland is well provided for Monday to Friday, 9am to 5pm. Hexham, Morpeth and Ashington have an over-provision of pharmacies during these hours; however, this provides additional patient choice, and extra capacity to provide enhanced services.
NHS 111 and Clinical Assessment Service
The NHS 111 and Clinical Assessment Service (CAS) for Northumberland is part of a regionally commissioned service for the CCGs in the North East. Patients calling NHS 111 who need clinical input can now be transferred to the CAS and speak directly to a clinician who will seek to complete the call there and then without the need to transfer the patient elsewhere. The aim is for NHS 111 and the CAS team to be able to directly book patients into an appointment at an Urgent Treatment Centre if needed, following a clinical assessment over the phone. This service also has the opportunity to direct to self-care if clinically appropriate. Work is currently underway to implement SystmOne within the two existing UCCs in Northumberland, which will enable pre-bookable appointments into these services. This is a nationally specified requirement of any future UTC.
General Practice Northumberland has 41 practices in four localities (East, West, North and Central) that are also now forming into 6 Primary Care Networks across the county. NCCG, as the direct commissioner of general practice, has agreed a strategy to enable the sustainability and transformation of general practice and this aligns with the NHS GP Five Year Forward View and NHS Long Term Plan.

12
NCCG also commissions locality based Extended Hours in Primary Care which aims to improve seven day access to general practice. Extended Hours in Primary Care offers additional appointments with GPs during the evenings and at weekends and the service is delivered on a locality basis from one location on behalf of a number of practices in that locality. Whilst Extended Hours appointments are aimed at patients requiring routine care, the availability of increased numbers of appointments and the potential to be seen either the same day or within a 24 hour period can often avoid people self-presenting at ED because they have been unable to secure such an appointment. GP Out of Hours Service The Northumberland GP Out of Hours (OOHs) service is provided by GPs and Advanced Nurse Practitioners/ Emergency Nurse Practitioners, and is accessed outside of normal surgery hours via NHS111. Patients are triaged and provided with advice, which can then be followed up with a home visit or a centre- based visit, where appropriate. Where a centre visit is required, these patients are booked directly into the GP OOHs service following assessment by NHS 111 through the NHS Pathways triage system. The patient is advised of the time and location of their appointment and given advice on what to do should their condition worsen in the intervening period. The GP OOHs service in Northumberland is currently co-located in the two UCCs and Alnwick and Berwick MIUs. Urgent Care Centres and Minor Injury Units
The urgent care needs of Northumberland residents are served from a number of locations, for the assessment and treatment of minor illness and minor injury. There are two UCCs in Northumberland with diagnostics available at the following sites:
Hexham General Hospital
Wansbeck General Hospital There are also two MIUs with diagnostics available at:
Alnwick Infirmary
Berwick Infirmary Additionally there are two other services that provide minor injury management for walk in patients in:
Blyth Community Hospital
Haltwhistle War Memorial Hospital These two services have reduced opening hours as compared to the UCCs and MIUs, with Blyth also being a weekday service only. The differing scope of services, naming and designation, and the staffing model for each, has led to confusion for patients.

13
Same Day Emergency Care Sometimes called ‘ambulatory emergency care’, same day emergency care is a transformational change in care delivery similar to that seen in elective day surgery. It is a way of managing a significant proportion of emergency patients on the same day without admission to a hospital bed. Patients are managed in a timely and clinically appropriate way with rapid access to diagnostics and robust clinical assessment. Same day emergency care gives the opportunity to better manage patient flow, improve patient experience and reduce acute hospital admissions. Patients may be referred to SDEC by their GP, A&E or other route. The Northumberland SDEC vision is to facilitate clinical discussion between key partners to ensure appropriate patients access SDEC, with patients receiving the right care, in the right place, at the right time. Currently access to SDEC is within dedicated facilities at NSECH.
Emergency Department
Currently patients are conveyed by Ambulance to A&E (also known as the Emergency Department) at NSECH for their emergency care needs, however, a large number of patients also self-present, which was not the original intention of the department when it was developed. The department does not currently turn away any patients or stream to other facilities and all are treated on site. Analysis has shown that a significant proportion of presenting patients do not have emergency care needs and could be dealt with by primary care, which could be on site or in either a primary care setting or at an alternate urgent care facilities. Diagram 4 below shows the locations of all the UCCs, MIUs, and the SDEC unit and A&E at NSECH. Diagram 4: Locations of Urgent Care facilities in Northumberland

14
Out of Hospital reform In Northumberland work is ongoing to review clinical pathways to embed prevention, assessment and intervention across the pathway, and to reshape health and community teams to maximise the skills in the workforce, to understand the role of specialists in support of generalist colleagues, and to maximise care provision in community settings, preventing admissions and actively ‘pulling’ patients out of hospital where admission has been required. New ways of working, and new roles are being explored along with opportunities to use technology to enhance capacity in community integrated care. In line with the NHS Long Term Plan, additional national investment will flow into primary and community health services in Northumberland from 2019 - 2023 to expand the workforce and fund new services. A key requirement is the establishment of Primary Care Networks (PCNs) of which there will be 6 in Northumberland, bringing together local GP practices with multidisciplinary community teams to support the provision of integrated health and social care in communities. Pharmacists, physios, paramedics, physician associates and social prescribers will form part of these expanded community teams providing tailored care for patients and allowing GPs to focus more on patients with complex needs. These new roles and enhanced teams will also need to consider how they work alongside existing community professionals such as community nursing, therapists and social care staff, plus nurse practitioners and advanced nurse practitioners working in practices and out of hours services. The new advanced service specification for Community Pharmacists, the NHS Community Pharmacist Consultation Service, aims to connect patients who have a minor illness, or a need for urgent supply of previously prescribed urgent medicines, with a community pharmacy which should rightly be their first port of call. This will begin with referrals from NHS 111 followed by the piloting of expansion to referrals from GP practices, 111 online, UTCs and ED, with aim of appropriately relieving pressure elsewhere in the urgent care system. There is also a need to consider how we expand pathways and support from dentists and optometrists in community settings for specific urgent care needs that can be dealt with more appropriately. In Northumberland, partners under the auspices of the System Transformation Board are considering the opportunities to introduce these new roles in the community taking into account the full health and care system, so that the workforce needs and interdependencies across all pathways and services are acknowledged, including those of the urgent care system. Why local urgent care services need to change A gap analysis has been undertaken on the way urgent care services are currently provided for patients across Northumberland. Feedback from patients tells us that it can be confusing due to the different settings, variable service offers and opening times. We know from discussions with professionals that services are not as joined up as they could be, and the overall fragmentation of the system means that many patients may not be able to access the most appropriate urgent care service to suit their needs. This can lead to duplication and over-use of the most expensive services, at significant cost to the NHS. As shown in the diagram 5 below from 2014 to 2019 we have seen an overall increasing trend in A&E activity year on year (Type 1 – 4). There has been an increase

15
by 23% when comparing the activity overall between 2014/15 with 2018/19. This data includes patients presenting at the ED at NESCH along with the UCCs and MIUs Diagram 5: A&E activity 2014 - 2019
A Type 1 A&E department is a consultant led 24 hour service with full resuscitation facilities and designated accommodation for the reception of accident and emergency patients. Type 2 is the same but for specialist patients such as ophthalmology or dental. A Type 3 and Type 4 A&E department could be any other type of A&E, Urgent Care Centre and Minor Injuries Unit / Walk in Centre which can be doctor led or nurse led. It may be co-located with a major A&E or sited in the community. A defining characteristic of a service qualifying as a type 3 department is that it treats at least minor injuries and illnesses (sprains for example) and can be routinely accessed without appointment. On average there were 8,042 Types 1 and 2 patients seen per month in 2014/15 compared with 6,818 in 2018/19, although in recent years there has been a steady increase in activity since a low point in 2016/17 of a monthly average of 6,138. Types 3 and 4 have seen a more significant increase per month. An average of 1,932 patients per month seen during 2014/15 compared with 5,450 per month in 2018/19. UCCs were originally envisaged as more appropriate care provision than ED for people accessing ED for non-life-threatening care. It was originally hypothesised that patients would access UCCs instead of ED resulting in less people overall accessing ED however we can see that this is not the case as attendances at ED have increased year on year despite the additional activity seen in the UCCs.
0
1,000
2,000
3,000
4,000
5,000
6,000
7,000
8,000
9,000
10,000
11,000
12,000
13,000
14,000
Ap
r-14
Jun
-14
Au
g-1
4
Oct-
14
Dec-1
4
Fe
b-1
5
Ap
r-15
Jun
-15
Au
g-1
5
Oct-
15
Dec-1
5
Fe
b-1
6
Ap
r-16
Jun
-16
Au
g-1
6
Oct-
16
Dec-1
6
Fe
b-1
7
Ap
r-17
Jun
-17
Au
g-1
7
Oct-
17
Dec-1
7
Fe
b-1
8
Ap
r-18
Jun
-18
Au
g-1
8
Oct-
18
Dec-1
8
Fe
b-1
9
Northumberland A&E attendances by A&E department type 2014/15 - 2018/19
Type 1 Type 2 Type 3/4 unknown

16
The graph in Diagram 6 shows the A&E attendances that were amenable to primary care, with a year on year increase in attendances amenable to primary care and a 4% increase over period (2014/15 (10.1%) to 2018/19 (14.1%)). Diagram 6: A&E attendances amenable to primary care
This correlates with national research which found that of first time attendances to EDs, 15.1% were defined as non-urgent. The study also found that non-urgent attendances were significantly more likely to present out of hours than in hours and odds of a non-urgent attendance were significantly higher for younger patients (aged 16–44) compared to those aged 45–64 and the over 65’s.6 Across the North East health economy the proportion of ambulance turnarounds conducted within 30 minutes has also deteriorated between 2014/15 and 2018/19.. The average in 2014/15 was 90.3% compared to 39.4% in 2018/19 although data collection has improved significantly during this period. Engagement
Over the past few years NCCG has engaged with partners and stakeholders across Northumberland, including members of the public, patients, statutory and voluntary organisations and providers of both health and social care. Some key things that patients and the public have told us include:
They want us to make it easier to access primary care services
They sometimes find it difficult to get a same day appointment at their practice
They find the range of names and terminology for urgent and emergency care confusing
They are unsure what services and facilities are available at various locations
They don’t think that services are as joined up as they could be and that communication between GPs and hospitals could be improved
People with long term conditions told us they want tailored advice to manage their condition and easier access to a GP appointment
6 Characterising non-urgent users of the emergency department (ED): A retrospective analysis of routine ED data,
Colin O’Keeffe , Suzanne Mason, Richard Jacques, Jon Nicholl February 23, 2018
0%2%4%6%8%
10%12%14%16%18%
Ap
r-14
Jun
-14
Au
g-1
4
Oct-
14
De
c-1
4
Fe
b-1
5
Ap
r-15
Jun
-15
Au
g-1
5
Oct-
15
De
c-1
5
Fe
b-1
6
Ap
r-16
Jun
-16
Au
g-1
6
Oct-
16
De
c-1
6
Fe
b-1
7
Ap
r-17
Jun
-17
Au
g-1
7
Oct-
17
De
c-1
7
Fe
b-1
8
Ap
r-18
Jun
-18
Au
g-1
8
Oct-
18
De
c-1
8
Fe
b-1
9
Northumberland A&E % attendances amenable to primary care 2014/15 - 2018/19

17
From engagement activities we know that: 1. The current system is too complicated to navigate effectively. We know this because:
In previous engagement exercises the public have said they find the UC system confusing, and they don’t know where best to go to get their health care needs met
Research has found that staff are nearly as confused over the definitions of urgent and emergency care as the public which adds to the overall complexity for patients and the public.
Patients attending NSECH report feeling unsure about which facilities and testing was available from other services such as, Urgent Care being unable to provide x-rays or blood tests, therefore either being informed by other services or having the perception that NSECH was the only hospital to provide the particular services they needed.
2. The current system does not provide the UC service that the people of Northumberland would prefer. We know this because:
People attending at NSECH have told us they would prefer to be treated at a location closer to where they live
Local data shows us that people in Northumberland continue to access ED for nonlife-threatening needs despite the provision of GP led UCCs and nurse led MIUs across the county
Local data show us that the number of people going into ED has increased year on year
People have told us that access to primary care is not always easy and therefor the default option is to walk-in to a facility where you know that you will be seen
Regional research found that services are not as responsive to the needs of people with mental health problems and those with a learning disability.
3. People are not getting their urgent care needs met effectively in the current system. We know this because:
On average 14% of people attending ED had and ailment or injury that was amenable to treatment in primary care
Over one fifth of patients who attend ED and UCCs do not require any investigate or significant treatment
A significant number of patients who call NHS 111 and are referred to a service other than ED or UCC, ultimately end up presenting there
When people are seen by their GP practice or in primary care hubs, the GP can see their whole medical history, but in ED or the UCCs/MIUs, while they have access to diagnosis, medications and details of hospital admissions and treatments, they don’t have access to the whole patient case notes including End of Life care preferences (for example DNACPR, ADRT) and other critical information that will impact on decisions of how to respond during encounters with the treating service.

18
Patients and professionals tell us that they are happy for their information to be shared to enable delivery of joined up care but report that this does not often happen
UCC and MIU providers have issues with recruitment of GPs and Emergency Nurse Practitioners to work in the centres
4. Northumberland residents have an overreliance on hospital care. We know this because:
The amount of people accessing ED has not reduced despite the provision of two UCCs and 4 MIUs
A significant proportion of people attending ED in Northumberland leave the department without receiving any treatment or are discharged requiring no follow up or follow up by their GP
National engagement work as part of the 5YFV highlights the need for services to keep pace with societal and technological changes, particularly the use of online services which have led to a culture of immediacy and rising expectations. Regional behavioural insight work has highlighted that the public are concerned about the potential misuse of urgent and emergency care. Speed of access and quality of service were cited as the main factors that would avoid patients seeking or escalating to another service. Patients felt that if they could get speedy access they would use their surgery as the first port of call, however, participants felt that if access to a GP could not meet the ‘speedy’ criteria care then patients would access elsewhere as the default position.
6. Vision and Future Service Model Vision and Design Principles The model for urgent care in Northumberland must:
Be easily understood
Provide services than can meet the demand of urgent care conditions in and out of hours, providing timely, accessible and appropriate care.
Our overall vision is An integrated urgent care delivery model which is simple for patients and professionals to access, which delivers safe, sustainable, responsive and high quality care meeting national best practice standards, and promotes and supports patients return to health and independence The aim is that within three years the CCG will have commissioned fully integrated, 24/7, seamless urgent care provision across Northumberland. Our vision is simple, for those people with urgent but non-life threatening needs, we must provide accessible, responsive, effective and personalised services, outside of a hospital environment when clinically appropriate. These services should deliver care to

19
the highest standards, and quality of care will be based on nationally and locally agreed outcomes. The urgent care model has primary care at the heart of the service; GP leadership will be central to the development and delivery of this model. Urgent care provision must be aligned to changes within primary care, taking into account changes in the GP contract as well as the emerging Primary Care Networks (PCNs) and the developing out of hospital agenda. There is also an ideal opportunity now, both with the start of a new community pharmacy contract, and the development of PCNs to try and extend further the role of community pharmacy in dealing with pressures in the system. In 2013, NHS England (NHSE)7 set out the following principles for a new system of urgent and emergency care:
Provides consistently high quality and safe care, across all seven days of the week
Is simple and guides good, informed choices by patients, their carers and clinicians
Provides access to the right care in the right place, by those with the right skills, the first time
Is efficient and effective in the delivery of care and services for patients. Taking the learning from national best practice and evidence, and feeding in the key themes from our engagement work; we propose the following five principles to guide the redesign of UC services across Northumberland:
1. Increase self-care through access to good quality information and appropriate clinical advice
2. Ensure service delivery is appropriate to needs, accessible and responsive
3. Simplify access by improving integration across health and social care and reducing duplication of services
4. Be safe, sustainable, and provide high quality, care 5. Meet mandated requirements
Increase self-care through access to good quality information and appropriate clinical advice
What does this mean?
people will able to access good quality information that enables them to self manage rather than seeking urgent advice when appropriate, and understand the conditions requiring urgent same day attention
people will be able to access clinical advice to meet their needs in a timely way
advice will be tailored to individuals to meet their specific needs
health and social care staff will adopt a realistic medicine approach putting the
7 Principles for urgent and emergency care in England - Transforming urgent and emergency care services in
England -Urgent and Emergency Care Review - End of Phase 1 Report- NHS England 2013

20
person receiving care at the centre of decisions made about their care
we will encourage health and social care staff to find out what matters most to you so that the care of your condition fits your needs and situation
people will not need to attend a service just to be given advice on how to care for themselves
What could success look like?
people will be empowered to take responsibility for their own minor health needs
people will know where to go to access evidence based clinical advice
people will receive consistent evidence based advice
people will trust the advice, and this will give them confidence
people will have a greater understanding of what conditions require an urgent response
people will access the right level of service for their needs
shared decision making between health and social care staff and patients
we will ask stakeholders what they want success to look like
Ensure service delivery is appropriate to needs, accessible and responsive
What does this mean?
for simpler health care requirements people will seek telephone advice first, and use appropriate local services such as pharmacies and general practice
services that do not need to be provided in a hospital but could not effectively be provided by general practice care, will be provided in either locality primary care hubs or in county wide community services
we aim to ensure appropriate and accessible locations to reduce travel time for simpler and easy to treat urgent care needs, with people only needing to travel longer distances to access more specialist services
we will ensure appropriate and accessible transport options are in place
people will receive timely care where they require it
What could success look like?
patients present appropriately at the right place ensuring their health needs are met in a timely way, thus improving their longer term health outcomes which will support long term system sustainability
people self-present to ED only when they have life threatening conditions
people who require advice are able to access alternatives to attending at urgent and emergency care services
general practices are supported by their local primary care hub
we will ask stakeholders what they want success to look like
Simplify access by improving integration across health and social care and reducing duplication of services
What does this mean?
there will be fewer, but more improved, ways of accessing UC services
NHS 111 will be integrated with UC services
seamless pathways across services and transfer of information to support patient care

21
What could success look like?
people will know who to contact to get their health needs met
people will access the appropriate service for their needs
people will get their needs met at the service they access
people who require it (for example people with long term conditions) will receive continuity of care
people with complex needs will have agreed care plans in place to meet all their health needs including UC
we will ask stakeholders what they want success to look like
Be safe, sustainable, and provide high quality, care
What does this mean?
our aim is that there are no serious incidents
all clinicians and services meet required quality standards of care
services meet best practice and are evidence based
patients are asked about their experience of services, and any concerns are listened to and where possible acted upon
resources are used to maximise the health of the population
What could success look like?
patients receive high quality care
people live longer and with more years of good health
people value the system and their behaviour reflects this
patients are seen as partners in their care
we will ask stakeholders what they want success to look like
Meet mandated requirements
What does this mean?
access to clinical advice as appropriate via NHS 111
24 hours/7 days a week access to appropriate services via NHS 111
7 day extended access to General Practice (evenings and weekends)
access to community pharmacy consultation services via NHS 111 and other professional referrals
implementation of national UTC specification
consistent use of regional DoS profiles to ensure equity of access
rebranding of UC facilities to A&E, UTC or primary care hubs
What could success look like?
people will be empowered to manage self-limiting health needs
people access the most appropriate service for their needs by phoning NHS 111
people will be able to access General Practice in a timely way
only people who need specialist care will need to access the ED
we will ask stakeholders what they want success to look like
22
What will the future UC model in Northumberland look like? There is a need for the CCG to review existing urgent care provision in light of national policy, and the regional and local context and drivers for change, in order to set out the changes that need to be made to ensure high quality urgent care can be delivered to meet local needs whilst making best use of existing resources. This UC Strategic Direction is the start of a work programme to develop the Northumberland wide UC model. The future UC model has not yet been defined as we wish to co-produce this with patients and partners across the county. Further documents will be produced by NCCG as this work develops. The following draft objectives of the new model have been developed in light of our engagement and review work to date which will be tested as part of our further engagement work:
The public will have access to good quality information and guidance in the event of them needing urgent or emergency care
Patients will be encouraged to use NHS 111 as the central point of access for urgent care advice and triage so that patients can ‘talk before they walk’
Patients will be seen at the right time, in the right place, by a person with the appropriate skills to manage their needs
Only patients requiring emergency care will navigate into our emergency care services
Urgent care services will be accessible and responsive
We will ensure an evidence based approach to commissioning services
Services will be joined up, seamless and co-ordinated
Services will be safe, responsive and a high quality
Real time information, essential to patient care, will be available to professionals involved in a patients care
We will monitor the quality and experience of urgent care services and ensure continuing improvement
The next step is to continue with our engagement programme with patients and partners, to further understand what matters to local people, what the evidence and partners tell us works well and areas for improvement. We are developing a ‘Listening Document’ based on the strategic direction, which incorporates the views and evidence from this first stage, and we will use this to undertake further engagement and ‘listening’, holding open and honest conversations, explaining the challenges the CCG has around urgent care and asking a series of questions the CCG would like to explore. Following consideration of the views heard in the engagement and listening phases, we aim to co-produce proposals for future service configuration in each locality. The results of the above will inform the CCG’s urgent care commissioning intentions and any subsequent procurement required. An outline timeline for is provided in Diagram 7 below.

23
Diagram 7: Outline timeline for engagement and proposal development
7. Enablers and Interdependencies Enablers Clinical leadership The principal of having clinical leaders at the forefront of progressing the vision provides a strong basis for taking forward the reconfiguration of urgent care services in Northumberland. Service developments that arise from the Strategic Direction will be based on clinical best practice and learning from national and local reviews. Patient and Public Engagement The CCG is committed to engaging with the residents of Northumberland to inform service redesign and development, which includes commissioning urgent care services. To take the urgent care strategy forward we will need to develop a communication and engagement strategy supporting the continued involvement and engagement of patients. By listening to the experiences and views of our patients we can redesign urgent care in line with local needs. Workforce Development Delivering the Strategic Direction is dependent on having suitably competent staff. Development of a workforce strategy to support the new delivery models will be key to our success and linking this to the developing Primary Care Strategy for Northumberland. The requirements for UTCs to be GP led will place increasing pressure on the GP workforce and as such implementation will look to utilise an increasing skill mix through the inclusion of other professionals such as; Emergency Care Practitioners and Community Paramedics Data and Digital Technology Better use of data and digital technology has the power to support people to live healthier lives and use care services less. This may be through using technology to improve access to services such as through NHS 111 or online patient consultations; to support patients to manage their own condition; enabling care to be patient-centric, not limited by care settings and organisational boundaries and enabling shared access to the patient care record. Key is direct booking into ED, SDEC, UTCs and primary care hubs, from NHS 111 and between service providers to improve patient flow. Implementation of this Strategic Direction will embed shared access to data and use of digital technology as key components of future service requirements.

24
Utilising Estate Urgent care services are delivered from a number of facilities and locations across the county. Within this process our estates provision will be reviewed to ensure we make best use of the available facilities to support the delivery of urgent care provision and that these are appropriate and fit for purpose to meet the requirement of national and local service specifications. Interdependencies Throughout the development and delivery of this Strategic Direction due consideration will continue to be given to the various interdependencies with other local strategies and programmes, including:
Northumberland CCG’s Operational Plan 2019/20
Northumberland Joint Health and Well Being Strategy 2018-2028
Northumberland System Transformation Board Health and Care Strategy 2019/20
Specifically the Strategic Direction will take into account the synergies and interdependencies with the following system transformation workstreams:
Whole Systems Approach to Improving Health and Care
Children and Young People
Mental Health, Learning Disabilities and Autism
Primary Care and Community Services
Elective Care and Outpatients 8. Leadership and Governance Arrangements Northumberland CCG is both responsible and accountable for urgent care services for the local population and anyone present in Northumberland. However the CCG recognises that urgent care cannot be commissioned or delivered in isolation and is therefore working with system partners through the following Boards to discharge their statutory responsibilities with regards to urgent care:
Northumberland Health and Wellbeing Board
Northumberland System Transformation Board
Northumberland and North Tyneside Local A&E Delivery Board Specifically the Health and Wellbeing Board (HWBB) aims to transform the way health and social care services are commissioned and provided to promote integration, improve the health and wellbeing of the population of Northumberland and reduce health inequalities. This Strategic Direction will be aligned to the Joint Health and Wellbeing Strategy 2018-2028. The System Transformation Board (STB) is responsible for leading and enabling the delivery of clinically and financially stable care services across Northumberland, connecting the health and social care system to deliver care focused on an outcomes

25
framework, and enabling a shift from secondary to primary and community care, in the best interests of the person. This Strategic Direction will be aligned to the aims and underpinning principles of the STB and sits within the Urgent and Emergency Care workstream of the STB. The Board will oversee the development and implementation of the Strategic Direction, receiving progress reports on progress of the transformation work and ensuring that implementation takes into account synergies and interdependencies across all system transformation workstreams. On overview of the supporting governance structure is shown in Diagram 6 below. Diagram 6: Northumberland System Transformation Governance
The Local A&E Delivery Board (LADB) covering Northumberland and North Tyneside has a number of key roles in relation to leading and overseeing system planning and resilience in relation to UEC and specifically delivering national, regional and local UEC Strategy. The LADB will support delivery of specific actions arising from the development of the Strategic Direction as determined by the STB. Throughout the process of developing this Strategic Direction, Northumberland Overview and Scrutiny Committee (OSC) and NHS England will be informed of the ongoing process regarding the significance of any emerging proposals for service reconfiguration. Consideration as to the needs for a formal consultation process will be given in collaboration with both of the above.

26
9. Performance Management Framework
The CCG is currently monitored nationally against the following Key Performance Indicators (KPIs) that relate to the provision of UEC.
A&E performance against the 4 hour target for patients to be either treated or admitted from arrival within the department,
GP Extended access – to ensure that there are appointments available outside normal hours of GP surgery opening
Provision of access to online consultations
Ambulance response time performance
Proportion of ambulance calls that are managed through hear and treat, see and treat or transported to an alternative site other than an A&E department.
Emergency hospital admissions activity along with average length of stay.
Turnaround times for ambulance measuring the time spent from arrival with a patient to being clear to respond to another call. (This is a local measure however is a valuable indicator as to the performance of UEC system)
The CCG with its partners on the System Transformation Board (STB) are developing an Outcomes Framework that will support the delivery of the ambition and strategy of the local system to which this Urgent Care Strategic Direction is aligned. Diagram 7 shows outcomes and metrics being considered by the STB which relate to UEC: Diagram 7: STB UEC Outcome Measures A1: The health and care system works to improve the overall health of the population
Priority Indicator
First Order Excess Winter Deaths (persons)
Second Order Mortality rate from causes considered preventable (persons)
A2: People are supported to lead healthy lifestyle and are protected from illness
Priority Indicator
First Order Smoking Prevalence (adults)
Second Order Alcohol related hospital admissions (persons)
A3: The health and care system works with others
Priority Indicator
First Order Proportion of older people (65 and over) who were still at home 91 days after discharge from hospital into reablement / rehabilitation services (persons)
Second Order Social isolation: proportion of people who use services who reported that they had as much social contact as they would like
B4: People have access to services when they need them
Priority Indicator
First Order The ability to get an appointment or speak to someone in primary care
Second Order Common surgical procedure rates
B5: The health and care system works to reduce unplanned hospital admissions and the time people spend in hospital
Priority Indicator
First Order Inequity in avoidable emergency admissions / for urgent care sensitive conditions
Second Order Emergency admissions for acute conditions that should not usually require hospital admission (persons)
B6: people are supported to recover from illness or injury and stay healthy after treatment
Priority Indicator
First Order One year survival from all cancers (persons)
Second Order Leaving hospital, did the doctors or nurses give your family or someone close to you all the information they needed to help care for you?
B7: People receive services which are coordinated and person-centred
Priority Indicator
First Order Were you involved as much as you wanted to be in decisions about your care and treatment
Second Order Delayed transfers of care
B8: People are supported to maintain their independence and manage their own health
Priority Indicator
First Order Long term support needs met by admission to residential and nursing care homes (age 65 and over)
Second Order Proportion of people who use services have control over their daily life

27
10. Conclusion
Like many areas, the current model for UC in Northumberland is made up of a number of different services, provided from different locations providing differing levels of care. As such, the system can be confusing for patients to navigate and is failing to have the desired impact of freeing up capacity at A&E to respond to the most complex patients with the highest emergency needs. This Strategic Direction document outlines the start of a journey for Northumberland, moving towards a more cohesive, simplified model for UC for our residents. We are committed to achieving this not in isolation but through a collaborative approach whereby our system partners, most importantly the residents of Northumberland, co-produce the new model. By doing this we will ensure best use of the Northumberland pound but most importantly we will ensure urgent care services enable people to be seen in the right place by the right person, first time and every time.

Agenda Item 10.1
OFFICIAL
1 20190925 UC Governing Body Agenda Item 10.1 Annual Audit Letter 2018/19
Clinicians commissioning healthcare for the people of Northumberland
Meeting title Governing Body
Date 25 September 2019
Agenda item 10.1
Report title Annual Audit Letter 2018/19
Report author Senior Manager - Public Services, Mazars
Sponsor Chief Finance Officer
Private or Public agenda
Public
NHS classification Official
Purpose (tick one only)
Information only
Development/Discussion
Decision/Action
Links to Corporate Objectives Ensure that the CCG makes best use of all available resources
Ensure the delivery of safe, high quality services that deliver the best outcomes
Create joined up pathways within and across organisations to deliver seamless care
Deliver clinically led health services that are focused on individual and wider population needs and based on evidence.
Northumberland CCG/external meetings this paper has been discussed at:
None
QIPP N/A Risks N/A Resource implications N/A Consultation/engagement N/A

OFFICIAL
20190925 UC Governing Body Agenda Item 10.1 Annual Audit Letter 2018/19 2
Quality and Equality impact assessment
Completed.
Data Protection Impact Assessment
N/A
Research N/A Legal implications N/A Impact on carers N/A Sustainability implications N/A

OFFICIAL
20190925 UC Governing Body Agenda Item 10.1 Annual Audit Letter 2018/19 3
QUALITY and EQUALITY IMPACT ASSESSMENT 1. Project Name Annual Audit Letter 2018/19
2. Project Lead Director Lead Project Lead Clinical Lead
Chief Finance Officer
3. Project Overview & Objective
Not applicable – no schemes.
4. Quality Impact Assessment
Impact Details Pos/ Neg
C L Scores
Mitigation / Control
Patient Safety NA Clinical Effectiveness NA Patient Experience NA Others including reputation, information governance and etc.
NA
5.Equality Impact Assessment
Impact Details Pos/ Neg
C L Scores
Mitigation / Control
What is the impact on people who have one of the protected characteristics as defined in the Equality Act 2010?
NA
What is the impact on health inequalities in terms of access to services and outcomes achieved for the population of Northumberland? (which is in line with the legal duties defined in the National Health Service Act 2006 as amended by the Health and Social Care Act 2012), for example health inequalities due to differences in socioeconomic circumstances?
NA
6. Research Reference to relevant local and national research as appropriate.
NA
7. Metrics Sensitive to the impacts or risks on quality and equality and can be used for
Impact Descriptors Baseline Metrics Target NA

OFFICIAL
20190925 UC Governing Body Agenda Item 10.1 Annual Audit Letter 2018/19 4
ongoing monitoring. 8. Completed By Signature Printed
Name Date
Senior Manager, Mazars
Jim Dafter
J Dafter
18/09/2019
Additional Relevant Information:
8. Clinical Lead Approval by Signature Printed Name
Date
Additional Relevant Information:
9. Reviewed By Signature Printed Name
Date
Comments

OFFICIAL
20190925 UC Governing Body Agenda Item 10.1 Annual Audit Letter 2018/19 5
Governing Body 25 September 2019 Agenda Item: 10.1 External Audit Annual Audit Letter 2018/19 Sponsor: Chief Finance Officer
Members of the Governing Body are asked to: 1. Consider the External Audit Annual Audit Letter 2018/19 and provide comment.
Purpose This report provides the Governing Body of NHS Northumberland Clinical Commissioning Group (CCG) with the Annual Audit Letter 2018/19 produced by Mazars. Recommendation Governing Body is asked to consider the Annual Audit Letter 2018/19 and provide comment. Appendix 1: Annual Audit Letter 2018/19

Annual Audit LetterNHS Northumberland Clinical Commissioning GroupYear ending 31 March 2019

CONTENTS
1. Executive summary
2. Audit of the financial statements
3. Value for money conclusion
4. Other reporting responsibilities
5. Our fees
6. Forward look
Reports and letters prepared by the auditor and addressed to the CCG are prepared for the sole use of the CCG and we
take no responsibility to any member or officer in their individual capacity or to any third party.
1

Purpose of the Annual Audit LetterOur Annual Audit Letter summarises the work we have undertaken as the auditor for NHS Northumberland Clinical Commissioning Group (the CCG) for the year ended 31 March 2019. Although this letter is addressed to the CCG, it is designed to be read by a wider audience including members of the public and other external stakeholders.
Our responsibilities are defined by the Local Audit and Accountability Act 2014 (the 2014 Act) and the Code of Audit Practice issued by the National Audit Office (the NAO). The detailed sections of this letter provide details on those responsibilities, the work we have done to discharge them, and the key findings arising from our work. These are summarised below:
1. EXECUTIVE SUMMARY
2
1. Executive summary2. Audit of the
financial statements3. Value for money
conclusion 4. Other reporting
responsibilities5. Our fees 6. Forward look
Area of responsibility Summary
Audit of the financial statements
Our auditor’s report issued on 24 May 2019 included our opinion that: • the financial statements give a true and fair view of the CCG’s financial
position as at 31 March 2019 and of its financial performance for the year then ended; and
• income and expenditure has, in all material respects, been applied for the purposes intended by Parliament.
Value for Money conclusionOur auditor’s report stated that we had matters to report in respect of the CCG’s arrangements to secure economy, efficiency and effectiveness in its
use of resources.
Reporting to the group auditorIn line with group audit instructions issued by the NAO, on 21 April 2019 we reported that we identified one difference of over £300k between the CCG’s
consolidation schedules and the audited financial statements.
Statutory reporting Not applicable.

The scope of our audit and the results of our workThe purpose of our audit is to provide reasonable assurance to users that the financial statements are free from material error. We do this by expressing an opinion on whether the statements are prepared, in all material respects, in line with the financial reporting framework applicable to the CCG and whether they give a true and fair view of the CCG’s financial position as at 31 March 2019 and of its financial performance for the year then ended.
Our audit was conducted in accordance with the requirements of the Code of Audit Practice issued by the NAO, and International Standards on Auditing (ISAs). These require us to consider whether:
the accounting policies are appropriate to the CCG’s circumstances and have been consistently applied and adequately disclosed;
the significant accounting estimates made by management in the preparation of the financial statements are reasonable; and
the overall presentation of the financial statements provides a true and fair view.
Our auditor’s report, issued to the CCG on 24 May 2019, stated that, in our view, the financial statements give a true and fair view of the CCG's financial position as at 31 March 2019 and of its financial performance for the year then ended.
The Code of Audit Practice also requires us to form and express an opinion on whether the CCG’s expenditure has been, in
all material respects, applied for the purposes intended by Parliament (our regularity opinion). Our auditor’s report also
confirmed that, in our view, income and expenditure has, in all material respects, been applied for the purposes intended by Parliament.
2. AUDIT OF THE FINANCIAL STATEMENTS
3
Opinion on the financial statements Unqualified
Opinion on regularity Unqualified
1. Executive summary2. Audit of the
financial statements3. Value for money
conclusion 4. Other reporting
responsibilities5. Our fees 6. Forward look

Our approach to materialityWe apply the concept of materiality when planning and performing our audit, and when evaluating the effect of misstatements identified as part of our work. We consider the concept of materiality at numerous stages throughout the audit process, in particular when determining the nature, timing and extent of our audit procedures, and when evaluating the effect of uncorrected misstatements. An item is considered material if its misstatement or omission could reasonably be expected to influence the economic decisions of users of the financial statements.
Judgements about materiality are made in the light of surrounding circumstances and are affected by both qualitative and quantitative factors. As a result we have set materiality for the financial statements as a whole (financial statement materiality) and a lower level of materiality for specific items of account (specific materiality) due to the nature of these items or because they attract public interest. We also set a threshold for reporting identified misstatements to the Audit Committee. We call this our trivial threshold.
The table below provides details of the materiality levels applied in the audit of the financial statements for the year ended 31 March 2019:
2. AUDIT OF THE FINANCIAL STATEMENTS
4
Financial statement materiality Our financial statement materiality is based on1.5% of gross operating expenditure £8.009 million
Trivial threshold Our trivial threshold is based on 3% of financialstatement materiality. £0.240 million
Specific materiality
We have applied a lower level of materiality to the following areas of the accounts:
• Remuneration and staff report £5k banding
1. Executive summary2. Audit of the
financial statements3. Value for money
conclusion 4. Other reporting
responsibilities5. Our fees 6. Forward look

2. AUDIT OF THE FINANCIAL STATEMENTS
Our response to significant risksAs part of our continuous planning procedures we considered whether there were risks of material misstatement in the CCG’s financial statements that required special audit consideration. We reported significant and enhanced risks identified at the planning stage to the Audit Committee within our Audit Strategy Memorandum and provided details of how we responded to those risks in our Audit Completion Report. The table below outlines the identified significant and enhanced risks and the work we carried out on those risks and our conclusions.
5
Identified significant and enhanced risks Our response Our findings and
conclusions
Significant risk - management override of controls
Management at various levels within anorganisation are in a unique position toperpetrate fraud because of their abilityto manipulate accounting records andprepare fraudulent financial statementsby overriding controls that otherwiseappear to be operating effectively. Dueto the unpredictable way in which suchoverride could occur there is a risk ofmaterial misstatement due to fraud onall audits.
We addressed this risk by:
• reviewing the key areas within the financialstatements where management has usedjudgement and estimation techniques andconsider whether there is evidence ofunfair bias;
• examining any accounting policies thatvary from the Government AccountingManual;
• testing the appropriateness of journalentries recorded in the general ledger andother adjustments made in preparing thefinancial statements; and
• undertaking cut-off testing around theyear-end on receipts and payments.
Our work provided us with the assurance we sought and did not highlight any material issues to bring to the CCG’s attention. We
highlighted one low priority internal control recommendation in relation to journals. This issue has been identified at all NHS Shared Business Services (SBS) users and is not isolated to this CCG.
Significant risk - Expenditure recognition
There is a risk of fraud in financialreporting relating to expenditurerecognition due to the potential toInappropriately record expenditure in thewrong period. This is not to imply wesuspect actual fraud, but that weapproach our audit maintaining dueprofessional scepticism.
We addressed this risk by:
• undertaking cut-off testing around theyear-end on payments;
• sample testing expenditure transactionsthroughout the year;
• sample testing material year-end payablesand provisions; and
• reviewing inter-NHS reconciliations anddata matches provided by the Departmentof Health.
This work also informed our conclusion on theregularity element of the audit opinion.
Our work provided us with the assurance sought and did not highlight any material issues to bring to the CCG’s attention.
1. Executive summary2. Audit of the
financial statements3. Value for money
conclusion 4. Other reporting
responsibilities5. Our fees 6. Forward look
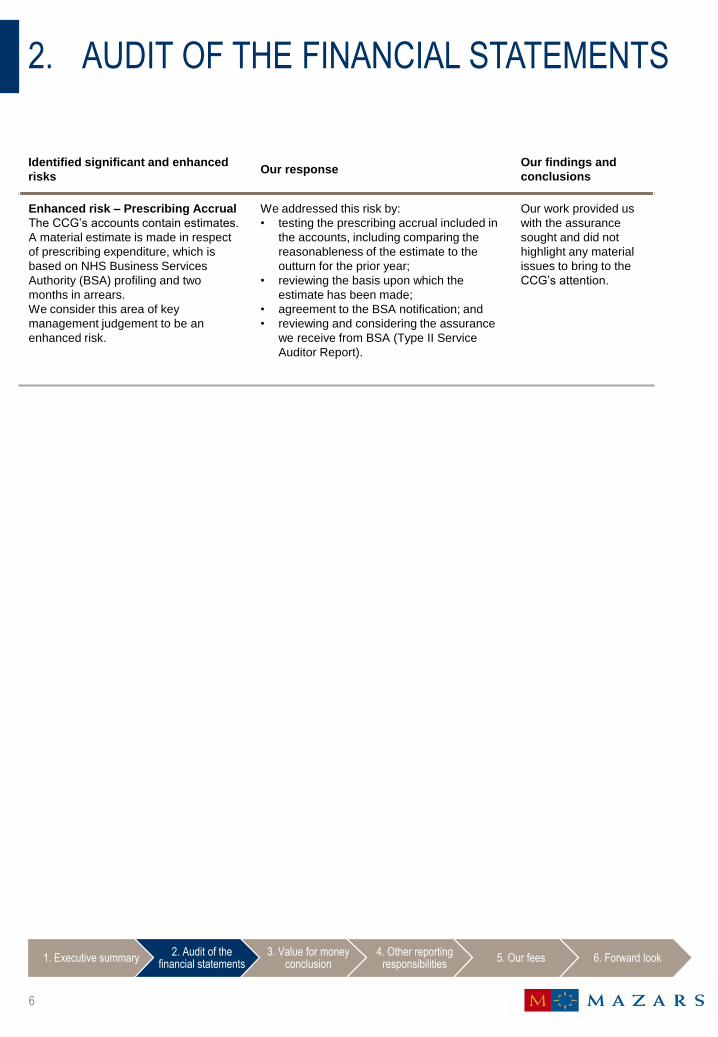
2. AUDIT OF THE FINANCIAL STATEMENTS
6
Identified significant and enhanced risks Our response Our findings and
conclusions
Enhanced risk – Prescribing AccrualThe CCG’s accounts contain estimates.
A material estimate is made in respect of prescribing expenditure, which is based on NHS Business Services Authority (BSA) profiling and two months in arrears.We consider this area of key management judgement to be an enhanced risk.
We addressed this risk by:• testing the prescribing accrual included in
the accounts, including comparing the reasonableness of the estimate to the outturn for the prior year;
• reviewing the basis upon which the estimate has been made;
• agreement to the BSA notification; and• reviewing and considering the assurance
we receive from BSA (Type II Service Auditor Report).
Our work provided us with the assurance sought and did not highlight any material issues to bring to the CCG’s attention.
1. Executive summary2. Audit of the
financial statements3. Value for money
conclusion 4. Other reporting
responsibilities5. Our fees 6. Forward look

2. AUDIT OF THE FINANCIAL STATEMENTS
Internal control recommendationsAs part of our audit we considered the internal controls in place that are relevant to the preparation of the financial statements. We did this to design audit procedures that allow us to express our opinion on the financial statements, but this did not extend to us expressing an opinion on the effectiveness of internal controls.
We did not identify any significant deficiencies in internal control.
During the audit, we followed-up the low priority recommendation that we raised last year, as set out below.
7
Description of deficiency including follow-up for 2018/19
Testing of journals identified a small number of journals which had been prepared and authorised by the same officers within NHS Shared Business Services (SBS) on behalf of the CCG. These were all of a clearly trivial value and we obtained assurance there were no other journals prepared and authorised by the same officer.
Potential effects Journal controls are key controls for the prevention of misstatement due to fraud or error. The lack of segregation of duties could result in fraud or error.
Recommendation The CCG should again escalate this control failure to SBS to ensure that journals are not prepared and authorised by the same officer.
2018/19 Update Testing showed this remains an issue in 2018/19. However the CCG put in place compensating controls during the year and it is hoped that SBS will resolve this control issue in the coming year to avoid the need for compensating controls going forward.
1. Executive summary2. Audit of the
financial statements3. Value for money
conclusion 4. Other reporting
responsibilities5. Our fees 6. Forward look
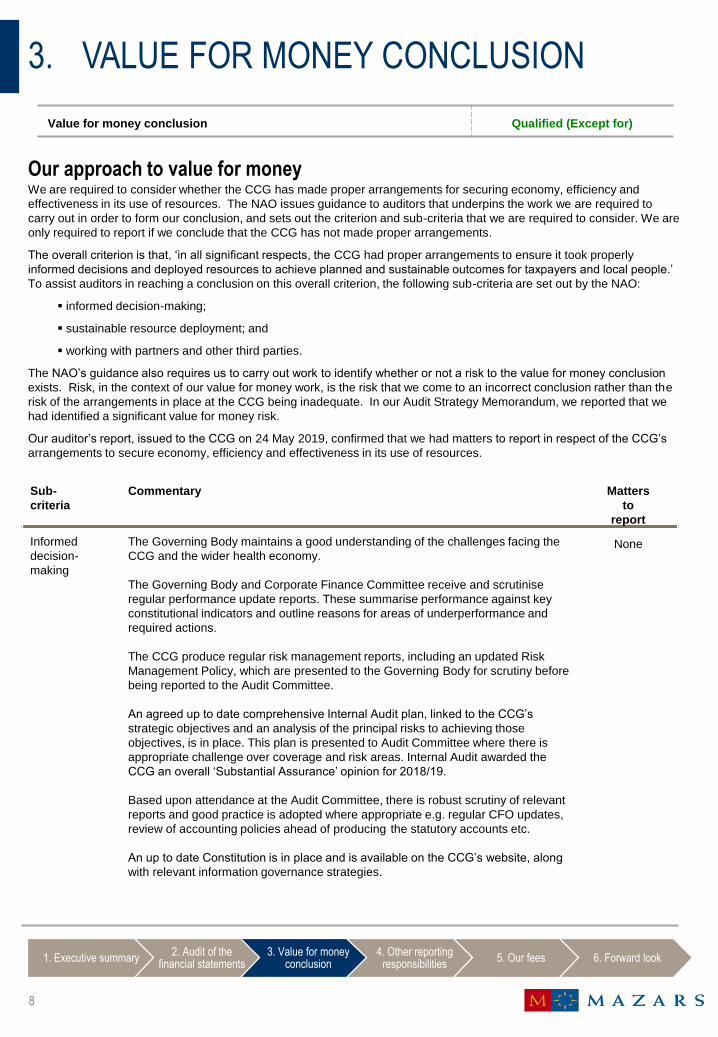
Our approach to value for moneyWe are required to consider whether the CCG has made proper arrangements for securing economy, efficiency and effectiveness in its use of resources. The NAO issues guidance to auditors that underpins the work we are required to carry out in order to form our conclusion, and sets out the criterion and sub-criteria that we are required to consider. We are only required to report if we conclude that the CCG has not made proper arrangements.
The overall criterion is that, ‘in all significant respects, the CCG had proper arrangements to ensure it took properly informed decisions and deployed resources to achieve planned and sustainable outcomes for taxpayers and local people.’
To assist auditors in reaching a conclusion on this overall criterion, the following sub-criteria are set out by the NAO:
informed decision-making;
sustainable resource deployment; and
working with partners and other third parties.
The NAO’s guidance also requires us to carry out work to identify whether or not a risk to the value for money conclusion
exists. Risk, in the context of our value for money work, is the risk that we come to an incorrect conclusion rather than the risk of the arrangements in place at the CCG being inadequate. In our Audit Strategy Memorandum, we reported that we had identified a significant value for money risk.
Our auditor’s report, issued to the CCG on 24 May 2019, confirmed that we had matters to report in respect of the CCG’s
arrangements to secure economy, efficiency and effectiveness in its use of resources.
8
3. VALUE FOR MONEY CONCLUSION
Sub-criteria
Commentary Matters to
report
Informed decision-making
The Governing Body maintains a good understanding of the challenges facing the CCG and the wider health economy.
The Governing Body and Corporate Finance Committee receive and scrutinise regular performance update reports. These summarise performance against key constitutional indicators and outline reasons for areas of underperformance and required actions.
The CCG produce regular risk management reports, including an updated Risk Management Policy, which are presented to the Governing Body for scrutiny before being reported to the Audit Committee.
An agreed up to date comprehensive Internal Audit plan, linked to the CCG’s
strategic objectives and an analysis of the principal risks to achieving those objectives, is in place. This plan is presented to Audit Committee where there is appropriate challenge over coverage and risk areas. Internal Audit awarded the CCG an overall ‘Substantial Assurance’ opinion for 2018/19.
Based upon attendance at the Audit Committee, there is robust scrutiny of relevant reports and good practice is adopted where appropriate e.g. regular CFO updates, review of accounting policies ahead of producing the statutory accounts etc.
An up to date Constitution is in place and is available on the CCG’s website, along
with relevant information governance strategies.
None
Value for money conclusion Qualified (Except for)
1. Executive summary2. Audit of the
financial statements3. Value for money
conclusion 4. Other reporting
responsibilities5. Our fees 6. Forward look

9
3. VALUE FOR MONEY CONCLUSION
Sub-criteria
Commentary Matters to
report
Sustainable resource deployment
The CCG has reported an in year surplus of £197,000 when taking into account the £8 million of non-recurrent Commissioner Sustainability Fund (CSF) support it has received during the year. The above has resulted in small reduction in the cumulative deficit to £57.610 million at 31 March 2019.
In our Audit Strategy Memorandum, presented to the Audit Committee in January 2019, we identified a significant risk in relation to the CCG failing to achieve the level of QIPP (quality, innovation, productivity and prevention) required in this and future years.
In order to assess the robustness of QIPP, we identified that we would complete sample testing of the achievement of the CCG’s 2018/19 QIPP plans. We also
undertook testing in relation to the CCG’s arrangements for achieving the 2019/20
QIPP plan requirement along with a high level review of the 2020/21 QIPP target.
Achievement of 2018/19 QIPP programmeThe CCG’s QIPP target was £21.6 million. This target was made up of a number of
individual projects, each having an individual savings target. Our work identified that processes were in place to develop, scrutinise and monitor QIPP schemes, overseen by the Corporate Finance Committee.
Based on the Month 12 tracker, the CCG achieved QIPP savings of £19.457 million, representing over 90% achievement of targeted savings opportunities, with slippage being offset by other mitigations together with favourable performance across the CCG’s commissioning and running costs budgets.
Arrangements for achievement of 2019/20 QIPP programmeThe CCG’s 2019/20 agreed budget identifies a £4 million deficit projected outturn
for which, if achieved, it will receive £4 million of CSF support thereby reporting a planned break even position.
Included in the CCG’s 2019/20 budget is a QIPP target of £10.394 million. Officers
have carried out detailed work in this area and have identified savings plans for a number of individual projects to achieve this target.
The CCG will continue with formal arrangements in place for the production and monitoring of QIPP schemes. As in previous year, the monthly QIPP tracker will allow project managers to be aware of financial achievements/issues as the year progresses.
The CCG has recently implemented a Portfolio Management approach which will provide a system of Programme and Project Governance & Assurance with oversight of the whole Operational Plan. In addition, the CCG have further strengthened arrangements with the addition of a ‘QIPP pipeline’ system which
allows additional projects to be brought on board in-year to supplement the QIPP programme and address any shortfall as a result of slippage.
Review of 2020/21 QIPP targetThe CCG’s medium term financial planning has identified the need to achieve QIPP
savings of £4.686 million. Work is ongoing to identify schemes to deliver this saving.
Yes
1. Executive summary2. Audit of the
financial statements3. Value for money
conclusion 4. Other reporting
responsibilities5. Our fees 6. Forward look

10
3. VALUE FOR MONEY CONCLUSION
Sub-criteria
Commentary Matters to
report
Working with partners and other third parties
A number of policy documents and frameworks are in place, including a Policy and Framework for Partnership Governance and available on its website.
Partnership working remains a corporate risk for the CCG i.e. Corporate Risk Objective 3 is to Create joined up pathways within and across organisations to deliver seamless care.
As part of the 2018/19 internal audit plan, AuditOne carried out a review of the Quality of Commissioned Services and also a review of arrangements for delivering Outsourced Services. Both of these reviews were given ‘Substantial Assurance’.
A detailed Procurement Policy is in place which includes the scheme of delegation, standing orders and detailed financial policies of the CCG.
The CCG continues to play an active role in the Northern CCG Joint Committee set up in late 2017.
It is also part of the North East and North Cumbria Urgent and Emergency Care Network, which aims to take a ‘whole system’ approach.
None
1. Executive summary2. Audit of the
financial statements3. Value for money
conclusion 4. Other reporting
responsibilities5. Our fees 6. Forward look

Significant Value for Money risksThe NAO’s guidance requires us to carry out work to identify whether or not a risk to the Value for Money conclusion exists.
Risk, in the context of our Value for Money work, is the risk that we come to an incorrect conclusion rather than the risk ofthe arrangements in place at the CCG being inadequate. In our Audit Strategy Memorandum, we reported that we had identified one significant Value for Money risk. The work we carried out in relation to significant risks is outlined below.
11
5. VALUE FOR MONEY CONCLUSION
Risk Work undertaken Conclusion
Failing to achieve the level of QIPP savings required
On-going financial pressures, along with a very challenging QIPP plan, represent a significant risk to sustainable resource deployment.
The CCG is projecting a planned in year deficit of £8m which, if achieved, it will qualify for £8m of non-recurrent Commissioner Sustainability Fund (CSF) support, which will give an in-year break-even position. This will result in a cumulative deficit of £57.807 million. However this is reliant on the CCG achieving QIPP savings of £21.600 million or making other compensating savings elsewhere within their annual budget.
We reviewed:
• the current year QIPP plan and progress being made;
• the robustness of the 2019/20 and 2020/21 QIPP plans; and
• budget monitoring
We outline in the sub criteria sections above, the financial performance of the CCG along with commentary on the achievement of the 2018/19 QIPP target and details of the robustness of the planned QIPP targets for 2019/20 and 2020/21.
The CCG has reported an in year surplus of £197,000 when taking into account the £8m of non-recurrent Commissioner Sustainability Fund (CSF) support it has received during the year, along with the delivery of 2018/19 QIPP savings of £19.457 million.
The above has resulted in a cumulative deficit of £57.610 million at the end of 2018/19 financial year.
Our overall conclusion is therefore that, ‘except for’ the CCG’s significant
cumulative deficit position, which current plans do not eliminate until 2025/26, there are no matters on which we are required to report.
Executive summary Significant findingsInternal control
recommendationsSummary of
misstatementsValue for Money
conclusionAppendices

The NAO’s Code of Audit Practice and the 2014 Act place wider reporting responsibilities on us, as the CCG’s external auditor. We set out below, the context of these reporting responsibilities and our findings for each.
Matters which we report by exceptionThe 2014 Act provides us with specific powers where matters come to our attention that, in our judgement, require reporting action to be taken. We have the power to:
issue a report in the public interest
make a referral to the Secretary of State where we believe that as decision has led to, or would lead to, unlawful expenditure, or an action has been, or would be unlawful and likely to cause a loss or deficiency; and
make written recommendations to the CCG which must be responded to publically.
We have not exercised any of these statutory reporting powers.
We are also required to report if, in our opinion, the governance statement does not comply with the guidance issued by the NHSE or is inconsistent with our knowledge and understanding of the CCG. We did not identify any matters to report in this regard.
Reporting to the NAO in respect of consolidation dataThe NAO, as group auditor, requires us to report to them whether consolidation data that the CCG has submitted is consistent with the audited financial statements. We have concluded and reported that we identified one difference of over £300k between the CCG’s consolidation schedules and the audited financial statements. This related to an amount of £2.253 million and was a result of payments that should have charged to Services from foundation trusts being incorrectly charged against Purchase of healthcare from non-NHS bodies. This resulted in an amendment between lines of the operating expenses disclosure note only (Note 4) and had no impact on the CCG’s total operating expenditure .
Other information published alongside the financial statements The Code of Audit Practice requires us to consider whether information published alongside the financial statements is consistent with those statements and our knowledge and understanding of the CCG. In our opinion, the information in the Annual Report is consistent with the audited financial statements.
12
4. OTHER REPORTING RESPONSIBILITIES
Exercise of statutory reporting powers No matters to report
Governance Statement No matters to report
Consistency of consolidation data with the audited financial statements
One difference of over £300k identified
Other information published alongside the audited financial statements
Consistent
1. Executive summary2. Audit of the
financial statements3. Value for money
conclusion 4. Other reporting
responsibilities5. Our fees 6. Forward look

Fees for work as the CCG’s auditorWe reported our proposed fees for the delivery of our work in the Audit Strategy Memorandum, presented to the Audit Committee in January 2019.
Having completed our work for the 2018/19 financial year, we can confirm that our final fees are as follows:
Fees for other work
We confirm that we have not undertaken any non-audit services for the CCG in the year.
We anticipate being engaged by the CCG to carry out work mandated by NHSE in respect of the Mental Health Investment Standard for 2018/19. The review will be completed following on from this year-end accounts and audit process and will be conducted according to a standard scope that has been agreed by NHSE. Whilst the engagement has not yet been formally agreed, the fee is expected to be £7,500 (excluding VAT). The final fee is dependent on any potential changes to the scope of the work following national consideration of the outcomes from pilot sites.
13
5. OUR FEES
Area of work 2018-19 proposed fee 2018-19 final fee
Delivery of audit work under the NAO Code of Audit Practice £43,900 £43,900
1. Executive summary2. Audit of the
financial statements3. Value for money
conclusion 4. Other reporting
responsibilities5. Our fees 6. Forward look

Financial outlookThe CCG’s cumulative deficit now stands at £57.610 million at the end of 2018/19 financial year. The 2019/20 agreed budget identifies a £4 million deficit projected outturn for which, if achieved, it will receive £4 million of CSF support thereby reporting a planned break even position. However, this is reliant upon the achievement of a QIPP target of £10.394 million or compensating savings being made elsewhere within the CCG’s budget.
Processes are in place to develop QIPP (Quality, Innovation, Productivity and Prevention) schemes and each is subject to regular monitoring and scrutiny, overseen by the Corporate Finance Committee. Officers recognise the challenges associated with delivering its 2019/20 budget and considers the risks associated with delivering its QIPP programme to be manageable.
Operational challengesWhilst the CCG achieved a number of its 2018/19 performance targets and was placed in the top quartile of all CCGs in the England comparison table in a number of areas, it still, along with partners, faces a number of operational challenges that have been considered in developing the CCG’s 2019/20 Operational Plan, including:
Ambulance response times.
Cancer Treatment.
Reducing falls in people over age 65
The CCG recognises the need to work collaboratively with its partners to deliver plans developed to address these issues. Progress made against these challenges will be reported to the Governing Body.
Legislative / environmental changesThe North East and North Cumbria are working towards the development of an Integrated Care System (ICS) with several local Integrated Care Partnerships (ICPs) to succeed the existing STP approach. This CCG is part of the North East and North Cumbria (NENC) ICS which aims to bring together local organisations to redesign care and improve population health, creating shared leadership and action, integrating primary and specialist care, physical and mental health services, and health with social care.
The challenges and risks associated with these changes reinforce the need for the implementation of robust governance arrangements at both an ICS and ICP level.
How we will work with the CCGWe are grateful to the CCG, its Members, officers and NECS colleagues for the cooperation and open dialogue during the year. We look forward to continuing to work closely with the CCG in delivering our Code of Audit Practice responsibilities infuture years.
We are committed to supporting the CCG as its external auditor. We will meet with the CCG and NECS staff to identify any learning from the 2018/19 audit and will continue to share our insights from across the NHS and relevant knowledge from the wider public and private sector.
Our added value offer In the coming year we will continue to support the CCG by:
continued liaison with AuditOne (the CCG’s Internal Auditors) to minimise duplication of work;
attending Audit Committee meetings, presenting Progress Reports that include updates on regional and national developments; and
hosting events for staff, such as our CCG Accounts Workshop.
14
6. FORWARD LOOK
1. Executive summary2. Audit of the
financial statements3. Value for money
conclusion 4. Other reporting
responsibilities5. Our fees 6. Forward look
Partner: Cameron Waddell
Phone: 0191 383 6300
Mobile: 0781 375 2053
Email: [email protected]
Senior Manager: Jim Dafter
Phone: 0191 383 6300
Mobile: 07815 876 042
Email: [email protected]
CONTACT
Agenda Item: 10.2 OFFICIAL
1 20190925 UC Agenda Item 10.2 2019-20 Assurance Framework and Risk Register Six Month Review
Clinicians commissioning healthcare for the people of Northumberland
Meeting title Governing Body
Date 25 September 2019
Agenda item 10.2
Report title 2019-20 Assurance Framework and Risk Register Six Month
Review
Report author Deputy Head of Governance
Sponsor Deputy Head of Governance
Private or Public agenda
Public
NHS classification Official
Purpose (tick one only)
Information only
Development/Discussion
Decision/Action
Links to Corporate Objectives Ensure that the CCG makes best use of all available resources
Ensure the delivery of safe, high quality services that deliver the best outcomes
Create joined up pathways within and across organisations to deliver seamless care
Deliver clinically led health services that are focused on individual and wider population needs and based on evidence.
Northumberland CCG/external meetings this paper has been discussed at:
Governance Group Discussions between COO DOF
QIPP All QIPP risks on the framework and register Risks Full Assurance Framework and Corporate Risk Register Resource implications NA Consultation/engagement NA

OFFICIAL
20190925 UC Agenda Item 10.2 2019-20 Assurance Framework and Risk Register Six Month Review 2
Quality and Equality impact assessment
Completed.
Data Protection Impact Assessment
NA
Research NA Legal implications NA Impact on carers NA Sustainability implications NA

OFFICIAL
20190925 UC Agenda Item 10.2 2019-20 Assurance Framework and Risk Register Six Month Review 3
QUALITY and EQUALITY IMPACT ASSESSMENT 1. Project Name 2019-20 Assurance Framework and Risk Register Six Month Review
2. Project Lead Director Lead Project Lead Clinical Lead Chief Operating Officer
Deputy Head of Governance
3. Project Overview & Objective
2019-20 Assurance Framework and Risk Register
4. Quality Impact Assessment
Impact Details Pos/ Neg
C L Scores
Mitigation / Control
Patient Safety NA Clinical Effectiveness NA Patient Experience NA Others including reputation, information governance and etc.
NA
5.Equality Impact Assessment
Impact Details Pos/ Neg
C L Scores
Mitigation / Control
What is the impact on people who have one of the protected characteristics as defined in the Equality Act 2010?
NA
What is the impact on health inequalities in terms of access to services and outcomes achieved for the population of Northumberland? (which is in line with the legal duties defined in the National Health Service Act 2006 as amended by the Health and Social Care Act 2012), for example health inequalities due to differences in socioeconomic circumstances?
NA
6. Research Reference to relevant local and national research as appropriate.
AuditOne benchmarking report for 2017
7. Metrics Impact Descriptors Baseline Metrics Target NA

OFFICIAL
20190925 UC Agenda Item 10.2 2019-20 Assurance Framework and Risk Register Six Month Review 4
Sensitive to the impacts or risks on quality and equality and can be used for ongoing monitoring.
8. Completed By Signature Printed Name
Date
Deputy Head of Governance
D Elliott 17/09/2019
Additional Relevant Information:
8. Clinical Lead Approval by Signature Printed Name
Date
Additional Relevant Information:
9. Reviewed By Signature Printed Name
Date
Comments

OFFICIAL
20190925 UC Agenda Item 10.2 2019-20 Assurance Framework and Risk Register Six Month Review 5
Governing Body 25 September 2019 Agenda Item: 10.2 2019/20 Assurance Framework and Risk Register Sponsor: Deputy Head of Governance
Members of the Governing Body are asked to: 1. Consider NHS Northumberland Clinical Commissioning Group’s Assurance
Framework, Corporate Risk Register and provide comment. 2. Approve the new strategic risks 2134 and 2182. 3. Note the closure of operational risks 1504 and 1797. 4. Approve the 2019/20 Assurance Framework six month review. Purpose This report seeks approval of the half year review of the 2019/20 Assurance Framework. Introduction This report provides the current risk status of NHS Northumberland Clinical Commissioning Group (CCG) and outlines risk management progress, and changes to the overall risk profile, since the last report to Governing Body (GB) in May 2019. Governing Body responsibility GB is responsible for assuring the CCG that risks are appropriately managed and consequently consider the assurance framework and corporate risk register on a quarterly basis (it is also a standing agenda item at the bi-monthly Governance Group). Members are required to consider all strategic risks on the assurance framework, together with operational risks on the corporate risk register above the GB Risk Tolerance Line (RTL) (set at a risk rating of 12 and above). A risk distribution matrix (Appendix 1) will be presented by the Deputy Head of Governance to focus GB risk discussions on the most important areas of strategic and operational risk. As a guide to assessing CCG risk, the risk matrix, as detailed in the approved Risk Management Policy, is reproduced below:

OFFICIAL
20190925 UC Agenda Item 10.2 2019-20 Assurance Framework and Risk Register Six Month Review 6
Likelihood score Consequence score 1 2 3 4 5
Rare Unlikely Possible Likely Almost certain
5 Catastrophic 5 10 15 20 25 4 Major 4 8 12 16 20 3 Moderate 3 6 9 12 15 2 Minor 2 4 6 8 10 1 Negligible 1 2 3 4 5
Scoring = Consequence x Likelihood (C x L) Audit Committee responsibility The Audit Committee (AC) is required, under its terms of reference, to report to GB annually on its work in support of the Annual Governance Statement, specifically commenting on the fitness for purpose of the Assurance Framework, the completeness and embeddedness of risk management in the organisation and the integration of governance arrangements. AC consider risk quarterly after GB and are presented with the GB paper and minutes. Development of Assurance Framework and Risk Register Safeguard Incident and Risk Management System (SIRMS) has been updated as follows:
• Assurance Framework and Corporate Risk Register adjusted to reflect the current risk landscape
• Full review of all risks • Full audit of outstanding actions
Assurance Framework The assurance framework for 2019-20 (Appendix 2) incorporates the CCG’s strategic plan and corporate objectives. Its purpose is to:
• Identify the strategic risks to the delivery of the CCG’s corporate objectives • Identify the controls and assurances in place • Identify and manage any gaps in controls and assurance.
The assurance framework drives the internal audit plan and associated outcomes are detailed in the relevant section of both the assurance framework and the corporate risk register. The assurance framework has been regularly reviewed by the risk owners and the Deputy Head of Governance; it has also been comprehensively reviewed to ensure that the 2019/20

OFFICIAL
20190925 UC Agenda Item 10.2 2019-20 Assurance Framework and Risk Register Six Month Review 7
risk profile has been updated to reflect all potential risks that could be experienced. There are 18 risks above the RTL (an increase of one since May 2019) with the following key changes:
Risk No (Page of AF)
Title Movement
2134 (11)
Quality and continuity of patient service – New strategic risk relating to potential impact on patient services in Laburnum surgery. The risk is currently rated as amber with a score of 12.
N/A
2182 (14)
CCG responsibilities for implementation of Liberty Protection Safeguards – New strategic risk that highlights proposed changes in legislation. The risk has a current score of 12 (amber).
N/A
Although the assurance framework printout is in current risk rating descending order, GB should note that the inherent risk (the initial risk rating) is equally important on the assurance framework and therefore should consider all risks in this respect. All risks and associated actions are in date for review. Risk Register The corporate risk register (Appendix 3) lists operational risks above the GB RTL and has been regularly reviewed by the risk owners. The complete risk register is reviewed by the Deputy Head of Governance and risk owners as required, on a monthly basis. Like the Assurance Framework the register was also reviewed to adjust to the start of 2019/20 position. There are 5 risks (the same number as in May 2019) identified on the corporate risk register that are above the GB RTL and there has been no key movement in the period. All risks and associated actions are in date for review. New Risks/Closed Risks Two new risks (Strategic Risk 2134 – Quality and continuity of patient services at Laburnum surgery and Strategic Risk 2182 – Potential impact of proposed change in legislation with the introduction of Liberty Protection Safeguards (LPS)) have been added; Appendix 4 refers. Two risks have been closed; Appendix 5 refers. The closed risks fall below the GB RTL. There are 40 risks experienced by the CCG (no change from May 2019).
OFFICIAL
20190925 UC Agenda Item 10.2 2019-20 Assurance Framework and Risk Register Six Month Review 8
Further Work The Assurance Framework and the Corporate Risk Register detail the full range of risks likely to be experienced, however ongoing work is required to ensure that each one is realistically scored and the controls, actions and assurances are fully articulated. Recommendation GB is asked to consider the 2019/20 Assurance Framework and Corporate Risk Register Six Month Review and provide comment. GB is also asked to approve new Strategic Risks 2134 and 2182. Appendix 1 – Risk Distribution Matrix Appendix 2 – Assurance Framework Appendix 3 – Operational risks above the GB RTL Appendix 4 – New Risks added since May 2019 Appendix 5 – Risks closed since May 2019

Northumberland CCG - Risk Analysis on a page
Consequence/ Severity
Rare 1
Unlikely 2
Possible 3
Likely 4
Almost Certain 5
Likelihood
Catastrophic 5
Major 4
Moderate 3
Minor 2
Negligible 1
1505, 1178, 945, 946
744, 1190
1374, 1181, 1981, 399, 1435, 1064, 1985, 1856
451, 2134, 1980, 1800, 1492, 2182, 407, 1447, 1894, 2019, 1799, 1506, 1385
403, 1390, 401, 1503
853, 1027, 1508, 1191
2125, 1983
1507, 733
805
To
lera
nce
line
NLAND MAT8
17/09/2019

Risk RefRisk directorRisk owner L
Risk description Risk effect Initial
C L Score
Controls InternalAssurance
Current
C L Score
Gaps in controls Gaps in assurances Actions Target dateLead Officer
Acceptable
ScoreC
Risk title
NHS Northumberland CCG
Assurance Framework 17/09/2019
CorpObj
ExternalAssurance
403
Siobhan Brown
CCG memberengagement
There is a risk that afailure to engage theCCG's membershipmeans that vitalintelligence is nottaken into accountwhen developingfuture deliverystrategy.
This could result inservices not beingevidence based ormeeting patientneeds, legalchallenge,reputational damageand memberpractices leaving theCCG, ultimatelyleading to the breakup of the CCG.
4 5 20 Communicationsand engagementstrategy.
GB monitoring ofCCG strategy
Stakeholder360 Survey.Internal auditreport onstrategicplanning Sept2018substantialassurance
Monthly localitymeetings with CCGclinical directorrepresentation andsenior management
Locality meetingkey pointsdiscussed atCMB andadditionalguidance/feedback provided asrequired.
Bi-annual membersmeeting
Governing BodymemberengagementAttendancelevels monitored
Lack of regularcontact betweensenior CCGmanagers andpractices
Memberengagementscheme
COO annualoversight of thescheme
StakeholderEngagementIA Oct 2017 -SubstantialAssurance
CCG 360 Feedbackreport
GB monitoring ClinicalEngagementIA Oct 2017 -Substantialassurance
Engagementimprovement planto be developed
OD - Clinical LeadsDevelopmentSessions quarterlysupported bymentoring andcoaching
CMB reporting -exceptionsreported to GB
Primary CareSustainability Plan -led by clinical leadsproviderdevelopment andCOO
GB reporting NHS EnglandNew Models ofCare teamquarterlyreviews
Practice Updateprovides currentinformation
New Comms andEngagement Planto go to OctoberGB that willaddress CCGreputation andengagementgoing forward
31/10/2019SiobhanBrown
Wide range ofactions plannedincluding Visit Schedule topractices, LindenHall County Wideevent, fullengagement withPCNs, refresh ofLocality Meetings,LMC monthlyengagement
31/10/2019SiobhanBrown
4 244 16 8
4. D
eliv
er C
linic
ally
Le
d H
ea
lth S
erv
ice
s T
ha
tA
re F
ocu
se
d O
n In
div
idu
al A
nd
Wid
er
Siobhan Brown
1Page

Risk RefRisk directorRisk owner L
Risk description Risk effect Initial
C L Score
Controls InternalAssurance
Current
C L Score
Gaps in controls Gaps in assurances Actions Target dateLead Officer
Acceptable
ScoreC
Risk title
NHS Northumberland CCG
Assurance Framework 17/09/2019
CorpObj
ExternalAssurance
401
Siobhan Brown
StakeholderEngagement
There is a risk that alack of appropriateengagement with keystakeholders,including the publicand patients, willmean that the CCGwill fail to takefeedback andevidence intoaccount whendesigning andcommissioning newservices.
This could result inpotential legalchallenge, deliveredservices not meetingpatient expectationsand diminishing carequality that ultimatelyaffects the CCG'sreputation.
4 4 16 Participation inHealth andWellbeing Board
Governing Body Internal Audit
Communicationsand engagementstrategy approvedby GB in May 2018
Governing Bodyto monitorprogress againststrategy
Internal auditreviews: StakeholderEngagementInternal Audit2017/18 -SubstantialAssurance
2019/20 commsand engagementstrategy
Regular stakeholderupdates by CCG
GB IA No CCGstakeholderupdates
Empowering Peopleand Communitiesstrategy and workinggroup
2017/18 StakeholderIA SubstantialAssurance
SystemTransformationBoard
Governing Body Internal AuditNHS EnglandAssurancemeetings
360 StakeholderSurvey
Governing Body Internal AuditNHS England
2019/20 360stakeholderimprovement plan
ICS, ICP andSystemTransformation Boardgovernancestructure, clinicalstrategy andsystem-wideengagementresponsibility tobe fully definedand implemented
30/11/2019SiobhanBrown
Communicationand managementroutes fordeveloping ICPsand engaging onthe wider footprintof NT,NorthumberlandNewcastle andGateshead aswell as full ICSfootprint - launchof CommsAutumn 2019
30/11/2019SiobhanBrown
Develop 360responseimprovement plan
30/11/2019SiobhanBrown
Develop andimplementquarterlystakeholderupdates as part ofnew Comms andEngagement Plan
30/11/2019SiobhanBrown
Develop Commsand Engagement2019/20 strategy- will go toOctober GB
31/10/2019SiobhanBrown
4 344 16 12
4. D
eliv
er C
linic
ally
Le
d H
ea
lth S
erv
ice
s T
ha
tA
re F
ocu
se
d O
n In
div
idu
al A
nd
Wid
er
Siobhan Brown
1503
Siobhan Brown
Primary CareResilience
There is a risk thatworkforce shortagesand increasingdemand combine atpractice level andresult in practiceclosures, patientsbeing dispersed andadditional pressuresbeing experiencedby other practices.This could lead to anunsustainablenumber of practiceclosures andultimately an inabilityto deliver primarycare at scale inNorthumberland.
This will result aderogation of patientcare at the primarycare level, additionalpressures beingexperienced acrossthe wider healtheconomy and theassociatedreputational damageto the CCG.
4 4 16 NorthumberlandPrimary CareCommissioningCommittee
Governing Bodyreceive minutes
NHS England,LMC, HWBandHealthWatchare committeemember.
Internal Auditon PCCommissioning SubstantialAssurance(April 2019)
Additional CCGcapacity allocated tosupport COO andthe Strategic Headof Corporate Affairs
CCG LineManagement
NHS England
Primary care PCCC Minutes
Primary CareEarly WarningDashboard to befully implemented- aligned withRAIDR and thedevelopingdashboards forPrimary careNetworks
30/11/2019PamelaPhelps
Two year majorprogramme ofwork to createsustainableprimary care forthe future
31/03/2020SiobhanBrown
Primary CareNetworks - initial2019/20 deliveryplan to be
30/11/2019PamelaPhelps
4 244 16 8
2. E
nsu
re T
he
De
live
ry O
f Sa
fe, H
igh
Qu
ality
Se
rvic
es T
ha
t De
live
r Th
e B
est O
utc
om
es
Pamela Phelps
2Page

Risk RefRisk directorRisk owner L
Risk description Risk effect Initial
C L Score
Controls InternalAssurance
Current
C L Score
Gaps in controls Gaps in assurances Actions Target dateLead Officer
Acceptable
ScoreC
Risk title
NHS Northumberland CCG
Assurance Framework 17/09/2019
CorpObj
ExternalAssurance
workforcedevelopmentscheme
GP Forward Viewoperational plansupported byTransformationFunding
PCCC NHS England
Merger ApprovalProcess
Process testedand fit forpurpose
Delivery of locumagency, communityeducation providernetwork and carenavigation
CMB, Gov Bodyand PCCC
NHS EnglandLMC
Primary CareDevelopment ActionPlan
PCCC Internal AuditMay 2019SubstantialAssurance
Clinical Leadership ClinicalManagementBoardGoverning Body
GP STP Submission CMB PCCC Additional fundingrequests will berequired to obtainNHS E approvalprior toimplementation
Sustainableprovision of GPservices in localities
PCCC NHS E Systematicprogrammerequired tosupport practiceswith early warningsignals
Primary Care EarlyWarning Dashboard
PCCC NHS E Primary CareEarly WarningDashboard to befully developedand implemented
developed bypractices
3Page

Risk RefRisk directorRisk owner L
Risk description Risk effect Initial
C L Score
Controls InternalAssurance
Current
C L Score
Gaps in controls Gaps in assurances Actions Target dateLead Officer
Acceptable
ScoreC
Risk title
NHS Northumberland CCG
Assurance Framework 17/09/2019
CorpObj
ExternalAssurance
1505
Siobhan Brown
ServiceCommissioning
There is a risk thatthe CCG fails tocommission the righthigh quality, costeffective services tomeet the needs ofthe population itserves.
This could result inpoor healthoutcomes, increasedpressure across theNorthumberlandhealth economy andassociated financialpressure andreputational damageto the CCG.
5 4 20 Adherence to theNHS ConstitutionalStandards
CMBPerformanceReport andminutes
NHS Englandassurance
Adherence to thenational and localrequirements in the2019/20 planningrefresh
CMBperformancereport andminutes
NHS Englandassurance
2019/20 operationalplan and detaileddelivery plan withtimelines andmetrics for impact ofdelivery
CMB andGoverning Body
NHS Englandquarterlyassurance andlegaldirections/specialmeasuresmeetings,StrategicPlanningInternal Audit
2019/20 Contractssigned with all keyproviders
CFC and GB NHS EAssurance
Improvement andAssessmentFramework
CMB andGoverning Body
NHS EnglandQuarterlyassurancemeetings
SystemTransformationBoard withstrengthenedgovernance
CMB and GoverningBody
Health andWellbeingBoardNHS England
CommissioningIntentions & Strategy2019/20
CMB Internal AuditNHS E
Every delivery groupin the CCG sightedand focused onpriority performanceareas.
PMO processwill generatehighlight reportsform CCGcommittees
5 235 15 10
4. D
eliv
er C
linic
ally
Le
d H
ea
lth S
erv
ice
s T
ha
tA
re F
ocu
se
d O
n In
div
idu
al A
nd
Wid
er
Paul Turner
4Page

Risk RefRisk directorRisk owner L
Risk description Risk effect Initial
C L Score
Controls InternalAssurance
Current
C L Score
Gaps in controls Gaps in assurances Actions Target dateLead Officer
Acceptable
ScoreC
Risk title
NHS Northumberland CCG
Assurance Framework 17/09/2019
CorpObj
ExternalAssurance
1178
Siobhan Brown
System Resilienceand EscalationPlanning
There is a risk that alack of robustplanning for surgesin demand forfrontline servicesthroughout the year,mean that urgentand emergency carepressures increase,resulting in rises inA&E activity andmultiple demands onambulance,community, acuteand primary careservices. There isalso a risk that EUExit could affectfrontline services.
This could lead toinsufficient resourcebeing available,potentially resultingin increased CCGcosts due toduplication of servicedelivery andinsufficient capacityto meet demand andan inability to meetnational targets (4hour A&E, 18 weeksRTT and ambulanceperformance). Thiswill lead to impact onorganisationalperformance atprovider level andreputational impacton the CCG.Workforce,ReciprocalHealthcare andResearch andClinical Trials couldbe affected as aresult of the UKexiting the EU.
5 5 25 Internal Audit onEmergency Planningand BusinessContinuityManagement - GoodAssurance March2019
Internal Audit
A&E Delivery Boardchaired by NHCFTCEO - nowconfigured with aseparate Executiveand Operationalfunction
All CCG boardsreceive regularupdates.Management ofdemand andthen escalationas requiredacross thesystem
Urgent andEmergencyCare NetworkRegional A&EDelivery BoardChairs GroupHWBBscrutinyOSC scrutiny
A&E demandpressures inSummer and riskfor WinterUEC performanceoverall
NHS I and NHS Einvolvement insystem wide deliveryplans
Local A&E DeliveryBoard action plan inplace, also reshapedLADB with executiveboard andoperational group fordelivery
Workforce - DHSCguidance states thecurrent expectationis that there will notbe a significantdegree of health andcare staff leavingaround EU exit day,also affectingaccess to supplies.
Ongoing issueswill be escalatedto the CCG bymemberpractices asdeemednecessary
Health andcareprofessionalswhosequalificationhas beenrecognisedand who areregistered inthe UK willcontinue to beregistered.
ReciprocalHealthcare - UKcitizens mayexperience limitedaccess to healthcareservices whilst onholiday
Ongoing issueswill be escalatedto the CCG bymemberpractices asdeemednecessary
Thegovernment isseeking toprotect currentreciprocalhealthcarerights throughbilateralagreementsand will issueadvice
It is not possibleto quantify howmany peoplemight return dueto changes inreciprocalhealthcare
Monitoring ofConsultantConnect; reset ofNSECH with mostseniorconsultantsseeing thepatients first;ambulatory carejoint investigationwork; review ofprimary carestreaming at frontdoor andSystmOne atinterface ; NEASDOS and modelof caredevelopment forcommunityparamedics
31/12/2019SiobhanBrown
Development ofUTCs/ hubs forconsistency andpre-bookableappts; SystmOneas interface atfront door ofNSECH andUTCs
31/10/2019SiobhanBrown
Devp of pilot forcommunityparamedic inBerwick
31/07/2019SiobhanBrown
5 335 15 15
2. E
nsu
re T
he
De
live
ry O
f Sa
fe, H
igh
Qu
ality
Se
rvic
es T
ha
t De
live
r Th
e B
est O
utc
om
es
Ailsa Nokes
5Page

Risk RefRisk directorRisk owner L
Risk description Risk effect Initial
C L Score
Controls InternalAssurance
Current
C L Score
Gaps in controls Gaps in assurances Actions Target dateLead Officer
Acceptable
ScoreC
Risk title
NHS Northumberland CCG
Assurance Framework 17/09/2019
CorpObj
ExternalAssurance
945
Jon Connolly
Contract overperformance
There is a risk ofover-activity, beyondthe CCG's control,on acute/secondarycare contracts, whichcould ultimately leadto the provision ofinadequate patientcare pathways whichwould necessitatecorrective actionbeing taken.
This would result inincreased CCGfinancial pressureand reputationaldamage to the CCG.
5 5 25 Monthly monitoringof contracts in yearand raising anyissues with the FT'sin accordance withour agreed timetableas part of contractmeetings, -or viacommissioningarrangements asassociate.
Minutes ofcontractmeetings andissue logsmaintained.CorporateFinanceCommittee andGoverning Bodyreporting ofSLAM contractFinance andActivitypositions.
Contract andPerformanceMonitoring IAMarch 2019 -SubstantialAssurance,next IAplanned forMarch 2020.
NECS producethe finance andactivityreconciliationreports andanalysis thatcomes from theSLAM model.Relies on thatanalysis beingdone in Accurateand timely manoron a monthlybasis in order forCCG to raisechallenges andissues at thecontract meetings.
Monthly internalBudget managerreview meetings forthe 3 main workstreams (MentalHealth, LearningDisabilities andChildren, Plannedcare and Communityservices, andPrimary and Urgentcare involving headsof commissioningand localitymanagers. Outcomeof which feeds intoprovider contractmonitoring meetingsand financialposition.
Signed budgetmanagermeeting notesand actions, partof key financialsystems audit.IA on keyFinancialcontrols March2019 substantialassurance. NextIA due March2020.
Signed ServiceLevel Agreements inplace with allproviders whichspecify finance andactivity plans.
All contracts for2019-20 signedas part of thecontractalignmentprocess.Contractperformancediscussed atmonthly contractmeetings withproviders andinternally at theCorporateFinanceCommittee.
Monthly monitoringand reporting;Corporate financecommittee, ActivityPlanning
CorporateFinanceCommitteereview offinancial
BI to producemonthly activityand financereports fromSUS/SLAM forthe CCG financeteam so the CCGcan assure itselfthat the contractdata beingreceived byNECS is in linewith plannedactivity and costlevels in the2019-20 contract.
31/03/2020RichardTurnbull
5 235 15 10
1. E
nsu
re T
ha
t Th
e C
CG
Ma
ke
s B
est U
se
Of A
llA
va
ilab
le R
eso
urc
es
Jon Connolly
6Page

Risk RefRisk directorRisk owner L
Risk description Risk effect Initial
C L Score
Controls InternalAssurance
Current
C L Score
Gaps in controls Gaps in assurances Actions Target dateLead Officer
Acceptable
ScoreC
Risk title
NHS Northumberland CCG
Assurance Framework 17/09/2019
CorpObj
ExternalAssurance
Assumptions,contract analysis oflarger and smallercontracts to feed intobudget managermeetings.
pressures andQIPP delivery
Agreement of ablended tariffapproach foremergency care asper the 2019-20planning guidance.
Blended tariff atmarginal rate of20% on allemergency PbRoverperformanceagreed betweenCCG and MainFoundationTrusts.Significantlyreduces in yearrisk on c100m ofactivity acrossboth trusts.
Financial Recoveryplan developed toget the CCG to asustainable in yearposition.
FRP deliveredfor 2018-19,2019-20 Longterm FRPsubmitted toNHSE at end ofQ1. Full PMOembedded innew CCGstructure,Portfoliomanagementgroup (PMG) setup to ensureQIPP/efficiencyis part ofbusiness asusual.
NHS EnglandArea teamexternalassuranceover Recoveryplan. PWCExternalreviewhighlightedgoodgovernanceand financialstewardship.NHSE Ratingimproved fromrequiresimprovementto good. CCGout of legaldirections andspecialmeasures July2019.
Project managementoffice put in place tohelp monitor andimplement financialrecovery planrequired savingsand schemes.Report on risks andmitigation to NHSEngland.
CorporateFinanceCommittee toreview andimplement newQIPP schemes,and review risksand mitigationsoutside thereported I&Eposition.
NHSEreviewing risksandmitigations ofthe CCG on amonthly basisas part of thenon ISFEfinancereturns.
7Page

Risk RefRisk directorRisk owner L
Risk description Risk effect Initial
C L Score
Controls InternalAssurance
Current
C L Score
Gaps in controls Gaps in assurances Actions Target dateLead Officer
Acceptable
ScoreC
Risk title
NHS Northumberland CCG
Assurance Framework 17/09/2019
CorpObj
ExternalAssurance
946
Jon Connolly
Financial Balance Currentcommissioningarchitecture remainsand there is a riskthat the mediumterm financial plan(including delivery ofQIPP) will beadversely affectedby contractperformance leadingto a failure toachieve financialbalance and abreach of statutoryduty. This wouldresult in reducedfunds for futureimprovements topatient outcomesand NHS Englandrevoking the CCG'scommissioningauthority.
Leading to increasedfinancial pressureand reputationaldamage to the CCG
5 5 25 1. Monthly financialclose down withreview of positionagainst budgets andmonthly boardreport.
Detailed reviewof financialposition andforecasts takenplace with CFOor deputy everymonth (premonth endmeeting).Detailedvalidation workand testing ofledgertransactions isundertaken eachmonth byfinancialmanagementteam. Workingpapers updatedeach month indetail forProgramme andrunning costs.
Internal Auditreview -contractmonitoring(March 2019 -substantialassurance).Internal Auditreview - keyfinancialcontrols (April2019 -substantialassurance).Internal Auditreview -Financial andstrategicplanning (July2019 -substantialassurance).
2. Procedure notesupdated routinely forrecurring tasks, andindividual task listsproduced to ensurecapacity for coveringabsence in financeteam.
Internal Auditreview - keyfinancialcontrols (Apr2019 -substantialassurance)
3. Detailed review ofgeneral ledger andupdate workingpapers
Updated reviewof general ledger- transactionsand trial balancereconciliations.This is ongoingand undertakenon a regularbasis andreviewed indetail at monthend. Workingpaperscompleted aspart ofmonth-endclosedown.
Internal Auditreview - keyfinancialcontrols (Apr2019 -substantialassurance)
4. Monthly budgetreports anddiscussion withbudget managers atmonthly meetings.
Monthlymeetings withbudgetmanagers onfinance position,QIPP within theirdelegatedbudgetresponsibility.
Internal Auditreview - keyfinancialcontrols (Apr2019 -substantialassurance)
5. Projectmanagement office
QIPP assurancereporting withProject delivery
NHS EnglandArea team
Medium to LongTerm Plansubmitted toNHSE and to bedeveloped andrefined further.
30/11/2019RichardTurnbull
5 235 15 10
1. E
nsu
re T
ha
t Th
e C
CG
Ma
ke
s B
est U
se
Of A
llA
va
ilab
le R
eso
urc
es
Jon Connolly
8Page

Risk RefRisk directorRisk owner L
Risk description Risk effect Initial
C L Score
Controls InternalAssurance
Current
C L Score
Gaps in controls Gaps in assurances Actions Target dateLead Officer
Acceptable
ScoreC
Risk title
NHS Northumberland CCG
Assurance Framework 17/09/2019
CorpObj
ExternalAssurance
established afterrecommendation inPWC capability andcapacity report,PMO tasked withhelping ensure thatindividual projectsare delivering therecovery plantargets.
and financialRAG ratingsdiscussed at theCorporateFinanceCommittee andGoverning Body.
externalassuranceover financialposition. Nowjoint meetingwith NorthTyneside CCGas the CFO isjointappointment.
6. Monthly contractmonitoring throughNECS and contractmeetings with mainproviders.
Attendance atcontractmeetings todiscussperformance andrisks on amonthly basis forthe main PbRacute providers.
Contract andPerformancemonitoringInternal auditreview -Fieldwork ongoing,Previoussubstantialassurance
NECS fail toidentify issuespromptly andchallengewindows aremissed.
7. Budget approvalprocess/ Budgetmanager Meetings
Managers haveto get relevantapproval viaappropriateCommitteeand/orGoverning Bodyfor newinvestment/allocations. Budgetmanagerreviews withsigned actionsand reviews.Increasingawareness ofneed forPurchase ordersto approvespending.
Internal Auditreview -Financial andStrategicPlanning (July2019substantialassurance)Internal Auditreview - KeyFinancialControls (April2019substantialassurance)
8. Additional nonrecurrent resource inform ofCommissionerSupport fund toachieve financialbalance in 2019-20.
CCG will need tomonitor progressagainst thecontrol totalthroughout theyear.
Notification of£4mCommissionerSustainabilityFundconfirmed fromNHSE as partof the planningprocess. Q1achieved.
The CCG needsto achieve 4mdeficit plannedcontrol total to beeligible for theCSF funding.
9Page

Risk RefRisk directorRisk owner L
Risk description Risk effect Initial
C L Score
Controls InternalAssurance
Current
C L Score
Gaps in controls Gaps in assurances Actions Target dateLead Officer
Acceptable
ScoreC
Risk title
NHS Northumberland CCG
Assurance Framework 17/09/2019
CorpObj
ExternalAssurance
1507
Annie Topping
Learning DisabilitiesTransformationProgramme
There is a risk thatthere is insufficientsystem capacity tocare for patients whoare transferred to thecommunity setting asa result of thenational requirementto deliver the bedclosure trajectory.This could result indelayed transfers ofcare,over-commissionedcare packages andpatient's care beingtransferred out ofNorthumberland.An emerging risk asa result oftransforming care isthe insufficientprovision of NHSassessment andtreatment beds forpeople with a LD and/ or Autism.
This could result inderogated patientcare and pooroutcomes, increasedfinancial pressure onthe CCG andreputational damage.More independentprivate sector bedswould have to becommissioned toaccommodate MHArequired admissions.
3 5 15 Community care andtreatment reviews
TransformingCare Meeting
Audited byNHS England
In-patient trackingsystem
TransformingCare Group
Regional LDTransformation BoardThis has beenreviewed andthe CCG isperformingwell againstthe target
Enhanced Models ofCare delivery
TransformingCare Meeting
OSCNHS EnglandAssurancemeeting takenplace
Business Casedevelopment
Mental HealthStrategic meeting
Cross CCGmeeting
NTW FT monthlycontract meeting
Chaired byNECS
Northern RegionalImplementationGroup
Chaired byNewcastleGateshead CCGDirector ofNursing
NorthumberlandCCG leadingdevelopment ofbusiness plan onbehalf of NorthCCGs
29/11/2019Kate O'Brien
Additional fundingto support a shortterm waiting listinitiative fundedthrough MHInvestmentStandard.Further workbeing undertakento considermedium termactions required.
31/10/2019Kate O'Brien
3 143 12 3
2. E
nsu
re T
he
De
live
ry O
f Sa
fe, H
igh
Qu
ality
Se
rvic
es T
ha
t De
live
r Th
e B
est O
utc
om
es
Kate O'Brien
451
Jon Connolly
Provider Delivery There is a risk thatproviders fail to meetkey performanceoutcomes and ceaseoperations leading tocompromised patientcare and the CCGhaving to introducepotentially expensiveshort term measuresin response. NHSEngland couldrevoke the CCG'scommissioningauthority if foundnegligent.
This could lead toincreased financialpressure andreputational damageto the CCG
4 4 16 Signed contracts inplace with allproviders.NECS provide amonthly report forsmaller providerscovering finance andperformance.
CMB and GBreporting
Non FinancialPerformanceManagementIA March 2017- SubstantialAssurance.QualityMonitoring andImprovementIA March 2016- SignificantAssuranceNHS EnglandQuarterlyReviewupdates
Monthlyperformance reportsto CMB andexception reports toGB. Also monthlyanalysis of activityagainst plan onrelease of SLAMand SUS data
NHS Englandquarterly assurancemeetings & weeklyfinancial recoverymeetings,highlighting risks theCCG is facing.
Internal Audit -SubstantialAssurance (nofindings)March 2018
Robust actionplans in place inareas of concernsuch as spinal,Cancer and otherspecialties.Working with FTfor triggers, earlywarning andsolutions to theissues includingcross FT to FTpathways
31/12/2019SiobhanBrown
4 234 12 8
2. E
nsu
re T
he
De
live
ry O
f Sa
fe, H
igh
Qu
ality
Se
rvic
es T
ha
t De
live
r Th
e B
est O
utc
om
es
David Lea
10Page
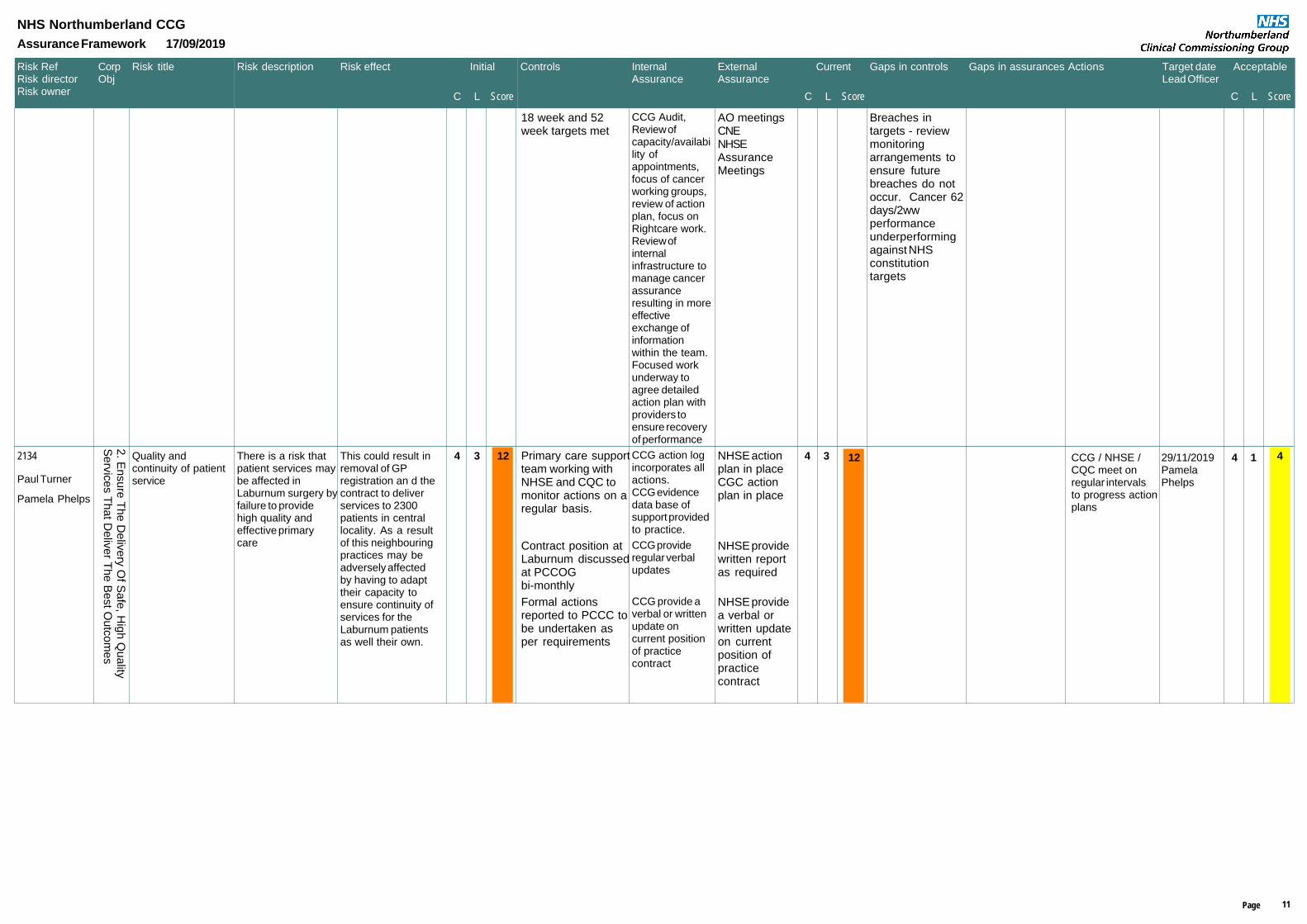
Risk RefRisk directorRisk owner L
Risk description Risk effect Initial
C L Score
Controls InternalAssurance
Current
C L Score
Gaps in controls Gaps in assurances Actions Target dateLead Officer
Acceptable
ScoreC
Risk title
NHS Northumberland CCG
Assurance Framework 17/09/2019
CorpObj
ExternalAssurance
18 week and 52week targets met
CCG Audit,Review ofcapacity/availability ofappointments,focus of cancerworking groups,review of actionplan, focus onRightcare work.Review ofinternalinfrastructure tomanage cancerassuranceresulting in moreeffectiveexchange ofinformationwithin the team.Focused workunderway toagree detailedaction plan withproviders toensure recoveryof performance
AO meetingsCNENHSEAssuranceMeetings
Breaches intargets - reviewmonitoringarrangements toensure futurebreaches do notoccur. Cancer 62days/2wwperformanceunderperformingagainst NHSconstitutiontargets
2134
Paul Turner
Quality andcontinuity of patientservice
There is a risk thatpatient services maybe affected inLaburnum surgery byfailure to providehigh quality andeffective primarycare
This could result inremoval of GPregistration an d thecontract to deliverservices to 2300patients in centrallocality. As a resultof this neighbouringpractices may beadversely affectedby having to adapttheir capacity toensure continuity ofservices for theLaburnum patientsas well their own.
4 3 12 Primary care supportteam working withNHSE and CQC tomonitor actions on aregular basis.
CCG action logincorporates allactions.CCG evidencedata base ofsupport providedto practice.
NHSE actionplan in placeCGC actionplan in place
Contract position atLaburnum discussedat PCCOGbi-monthly
CCG provideregular verbalupdates
NHSE providewritten reportas required
Formal actionsreported to PCCC tobe undertaken asper requirements
CCG provide averbal or writtenupdate oncurrent positionof practicecontract
NHSE providea verbal orwritten updateon currentposition ofpracticecontract
CCG / NHSE /CQC meet onregular intervalsto progress actionplans
29/11/2019PamelaPhelps
4 134 12 4
2. E
nsu
re T
he
De
live
ry O
f Sa
fe, H
igh
Qu
ality
Se
rvic
es T
ha
t De
live
r Th
e B
est O
utc
om
es
Pamela Phelps
11Page
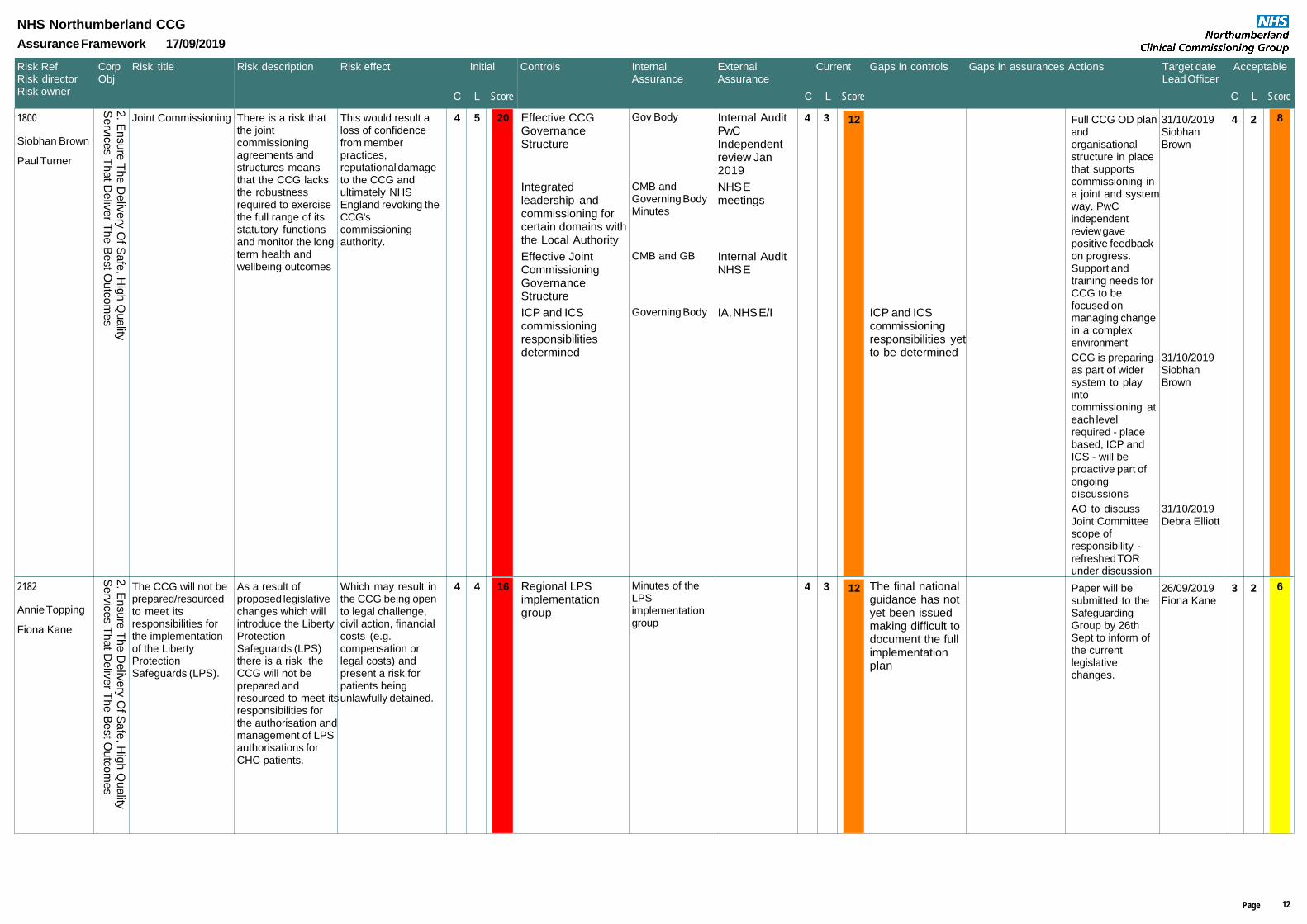
Risk RefRisk directorRisk owner L
Risk description Risk effect Initial
C L Score
Controls InternalAssurance
Current
C L Score
Gaps in controls Gaps in assurances Actions Target dateLead Officer
Acceptable
ScoreC
Risk title
NHS Northumberland CCG
Assurance Framework 17/09/2019
CorpObj
ExternalAssurance
1800
Siobhan Brown
Joint Commissioning There is a risk thatthe jointcommissioningagreements andstructures meansthat the CCG lacksthe robustnessrequired to exercisethe full range of itsstatutory functionsand monitor the longterm health andwellbeing outcomes
This would result aloss of confidencefrom memberpractices,reputational damageto the CCG andultimately NHSEngland revoking theCCG'scommissioningauthority.
4 5 20 Effective CCGGovernanceStructure
Gov Body Internal AuditPwCIndependentreview Jan2019
Integratedleadership andcommissioning forcertain domains withthe Local Authority
CMB andGoverning BodyMinutes
NHS Emeetings
Effective JointCommissioningGovernanceStructure
CMB and GB Internal Audit NHS E
ICP and ICScommissioningresponsibilitiesdetermined
Governing Body IA, NHS E/I ICP and ICScommissioningresponsibilities yetto be determined
Full CCG OD planandorganisationalstructure in placethat supportscommissioning ina joint and systemway. PwCindependentreview gavepositive feedbackon progress.Support andtraining needs forCCG to befocused onmanaging changein a complexenvironment
31/10/2019SiobhanBrown
CCG is preparingas part of widersystem to playintocommissioning ateach levelrequired - placebased, ICP andICS - will beproactive part ofongoingdiscussions
31/10/2019SiobhanBrown
AO to discussJoint Committeescope ofresponsibility -refreshed TORunder discussion
31/10/2019Debra Elliott
4 234 12 8
2. E
nsu
re T
he
De
live
ry O
f Sa
fe, H
igh
Qu
ality
Se
rvic
es T
ha
t De
live
r Th
e B
est O
utc
om
es
Paul Turner
2182
Annie Topping
The CCG will not beprepared/resourcedto meet itsresponsibilities forthe implementationof the LibertyProtectionSafeguards (LPS).
As a result ofproposed legislativechanges which willintroduce the LibertyProtectionSafeguards (LPS)there is a risk theCCG will not beprepared andresourced to meet itsresponsibilities forthe authorisation andmanagement of LPSauthorisations forCHC patients.
Which may result inthe CCG being opento legal challenge,civil action, financialcosts (e.g.compensation orlegal costs) andpresent a risk forpatients beingunlawfully detained.
4 4 16 Regional LPSimplementationgroup
Minutes of theLPSimplementationgroup
The final nationalguidance has notyet been issuedmaking difficult todocument the fullimplementationplan
Paper will besubmitted to theSafeguardingGroup by 26thSept to inform ofthe currentlegislativechanges.
26/09/2019Fiona Kane
3 234 12 6
2. E
nsu
re T
he
De
live
ry O
f Sa
fe, H
igh
Qu
ality
Se
rvic
es T
ha
t De
live
r Th
e B
est O
utc
om
es
Fiona Kane
12Page

Risk RefRisk directorRisk owner L
Risk description Risk effect Initial
C L Score
Controls InternalAssurance
Current
C L Score
Gaps in controls Gaps in assurances Actions Target dateLead Officer
Acceptable
ScoreC
Risk title
NHS Northumberland CCG
Assurance Framework 17/09/2019
CorpObj
ExternalAssurance
407
Siobhan Brown
National and localagreed outcomes
There is a risk thatthe CCG falls belowthe IntegratedAssessmentFramework targetsand fails to identifyand address qualityissues in services orproviders orproviders fail toprovide the requisiteinformation to enableeffective monitoringof performance,leading tocompromised patientcare and a loss ofincome from theCCG's qualitypremium
This could result inderogated patientcare, increasedreputational risk andfinancial pressureand ultimately NHSEngland revoking theCCG'scommissioningauthority.
4 4 16 Signed contracts inplace with allproviders
Minutes of GBand CMBCFC minutes
ContractMonitoring IA(Feb 2018) -SubstantialAssurance Key FinancialControls IA(Apr 2017) -SignificantAssurancewith no issuesof note.Qualitymonitoring &improvementIA (Apr 2016) -SignificantAssurancewith no issuesof note.
Regional escalationprocess if requredwhere outcomes notbeing met
RegionalQualitySurveillanceGroup.
New contract signedwith clearperformancerequirements andwithholding offunding if underperforming. Contractand commissioningmanagers closelyworking with NEAson improvements
Exceptionreporting isprovided to GovBody and CMBvia the Perf andQuality Reports
Progressagainst actionplan ismonitored byNEAS 999 and111 contractreviewmeeting andQRG (qualityimpact).
Monthlyperformance reportsto CMB and GovBody Meetings
Area Team quarterlyassurance meetings
Minutes ofNHS Emeetings
QRGs in place
Programme ofunannounced visitsto providers, theoutcome of whichare reported toQuality SafetyGroup.
Minutes ofQuality andSafety Group
HCAI root causeanalysis undertakenmonthly by HCAIclinical domain lead
HCAI bi monthlyworkstreammeetingconsiders rootcause analysis
HCAI recovery plan HCAIworkstream
CCG quarterlyassurance
4 334 12 12
2. E
nsu
re T
he
De
live
ry O
f Sa
fe, H
igh
Qu
ality
Se
rvic
es T
ha
t De
live
r Th
e B
est O
utc
om
es
Paul Turner
13Page

Risk RefRisk directorRisk owner L
Risk description Risk effect Initial
C L Score
Controls InternalAssurance
Current
C L Score
Gaps in controls Gaps in assurances Actions Target dateLead Officer
Acceptable
ScoreC
Risk title
NHS Northumberland CCG
Assurance Framework 17/09/2019
CorpObj
ExternalAssurance
meeting meeting.
RAIDR informationvalidated by NECS.
Local A&E DeliveryBoard
GB and CMBupdates
A&E deliveryboardHWBBUrgent andEmergencyCare network
IntegratedAssuranceFramework
Quarterly reportto GB and CMB
Progressreviewmeetings withNHSE localarea team.
1894
Siobhan Brown
Primary CareProvider Influence
There is a risk thatthe CCG fails toensure that theprimary care issufficiently engagedand offered ODsupport to operateas an equal partnerin the wider system,
This could result inreputational damageto Primary Care withthe consequentimpact on bothprimary caredevelopment andsystemdevelopments/implementation
4 5 20 Membership ofSystemTransformationBoard
CCG managementsupport
PCCCCMBGB
NHSEAssuranceSystemTransformation Board
Regular updatesprovided on CCGstrategic andoperational issues
Primary CareDevelopment Events
CMB and GB IA
PCNs PCCC and GB Not yet fullydeveloped
Series of primarycare events andprogramme ofwork initiated on3 October 2018 toidentify solutionsto primary caresustainability,create aleadership groupto steer actionplan and potentialinvestment fund.Supported bynational leadersin primary care
28/06/2019SiobhanBrown
Detailed actionand supportingOD plan for theestablishmentand priorities ofPCNs - workingwith the widersystem
31/12/2019SiobhanBrown
4 234 12 8
4. D
eliv
er C
linic
ally
Le
d H
ea
lth S
erv
ice
s T
ha
tA
re F
ocu
se
d O
n In
div
idu
al A
nd
Wid
er
Pamela Phelps
2019
Siobhan Brown
Access There is a risk thatpatients are unableto accessappropriate andtimely primary andsecondary care.
This could result inderogated patientcare, an increase inthe level ofcomplaints andreputational damageto the CCG.
4 5 20 NHS ConstitutionalStandards
CMB and GBperformancereporting
Internal Audit,NHS England
Variation inaccess/ waits bypractices andsecondary careproviders
Local A&E DeliveryBoard
Patient Choice andSatisfaction Surveys
Access timesreported to CMB ona monthly basiswhere areas ofconcern areescalated to GB
SystemTransformationBoard oversight ofsystem performance
Patient leveltracking of patientreferrals, waits,RTT and othertreatment times,diagnostics andespecially acrosscancer andsurgicalspecialties
31/12/2019SiobhanBrown
Review of urgentcare services andGB agreement toprocure the threerelevant servicesto ensure accessfor patients.NECSprocurementteam has beenappointed to work
31/07/2019PamelaPhelps
4 234 12 8
2. E
nsu
re T
he
De
live
ry O
f Sa
fe, H
igh
Qu
ality
Se
rvic
es T
ha
t De
live
r Th
e B
est O
utc
om
es
Pamela Phelps
14Page

Risk RefRisk directorRisk owner L
Risk description Risk effect Initial
C L Score
Controls InternalAssurance
Current
C L Score
Gaps in controls Gaps in assurances Actions Target dateLead Officer
Acceptable
ScoreC
Risk title
NHS Northumberland CCG
Assurance Framework 17/09/2019
CorpObj
ExternalAssurance
with CCG todevelop theprocurementstrategy
Programme toreduce variationin primary careincluding accessissues; alsoprogramme ofsustainability forthe future forprimary care -reducing accessproblems
31/07/2019PamelaPhelps
1506
Siobhan Brown
StrategicPartnerships
There is a risk thatthe CCG's strategicpartnerships failleading to abreakdown inrelationships andassociated shortterm capability gapsemerging.
This could lead to aderogation of patientcare and an impacton patient safety andthe CCG futurefinancial plansleading toreputational damageto the CCG
4 4 16 SystemTransformationBoard reports toH&WBB quarterly
Governing Body,CMB
HWBB
Register ofPartnershipAgreement
CFCGov Body
Formal S75agreements in placeas necessary
Internal auditSignificantAssuranceBCF 2019
Joint working asSection 117s andother complex carepackages
Joint Appointments -AO, CFO,permanent apptswith LA - SENDDCO and Children'sCommissioner roles
GB IA Consistentcommunicationlines
CCG has confirmedwith all partners thatdelivery will be thecurrentcommissioningarchitecture with theadded dimension ofspecial measures
CMBCFCGov Body
NHSEAssuranceSystemTransformation BoardH&WBB
Change instrategiclandscape
ICS and ICPworkingarrangements fullydetermined andCCG decisionmaking interestsfully protected
Governing BodyICS WorkstreamWorkshops
Internal Audit,NHS E/I
ICS and ICPgovernance yet tobe determined
ICP CCG Executiveto Executivemeetings
Governing Body Two Initialmeetings held butdevelopments andcohesion stillrequired
SystemTransformationBoard tasked byregulators withdelivering asystem financialplan, strategy andsystem leadershipproposition for asustainablesystem
30/11/2019SiobhanBrown
Chief OperatingOfficers of allthree CCGstasked withoutline proposalfor developmentacross ICP.Three CCG ExecMeetings nowtaking placemonthly.
30/11/2019SiobhanBrown
4 234 12 8
3. C
rea
te J
oin
ed
Up
Pa
thw
ays W
ithin
An
dA
cro
ss O
rga
nis
atio
ns T
o D
eliv
er S
ea
mle
ss C
are
Paul Turner
15Page

Risk RefRisk directorRisk owner L
Risk description Risk effect Initial
C L Score
Controls InternalAssurance
Current
C L Score
Gaps in controls Gaps in assurances Actions Target dateLead Officer
Acceptable
ScoreC
Risk title
NHS Northumberland CCG
Assurance Framework 17/09/2019
CorpObj
ExternalAssurance
1385
Annie Topping
Deprivation ofLiberty Safeguards(DOLS).
Due to a SupremeCourt ruling that hassignificantly loweredthe threshold fordeprivation of libertythere is a risk thatmany people whonow receive healthfunded care at homewill needauthorisation fromthe court ofprotection which theCCG are required toconsider. The CCGcould either fail toconsider and depriveliberty unlawfully ormake an incorrectjudgement.
This could lead to arisk of legalchallenge resulting inboth reputational andfinancial damage tothe CCG andincreased care costsoverall.
4 4 16 MCA/DOL'S trainingdelivered by theLDU to CCG andPrimary Care staff.
Annual CCGtraining auditreported to SG.Exceptionreporting to CMBand Governing Body.
Potentially staffunwilling toengage withtraining.
lA/CHC teamidentify potentialcases which need tobe referred torelevant SupervisoryBody for DOL'S.
LA DOL'sDashboardreport discussedat theSafeguardingGroup.
Internal auditDeprivation ofLiberty2016/17substantialassurance.Quarterly CHCreports andcommissioningteammonitoring andassurance. DOL'SDashboardreported toNSAB/PerformanceandGovenancesub groupquarterly.
LA/CHC teamidentify potentialcases of deprivationof liberty that needauthorisation fromthe Court ofProtection.
CCGrepresentation atthe quarterlyNSABPerformanceand Govenancesub groupmeetings,assurancesought from LAre currentposition ofjudicial DOL's.
Quarterly CHCreports andcommissioning/quality andsafeguardingteamsmonitoring andassurance.Dashboard forrecording COPDOL'S inplace.
MCA DOL's Forthcominginternal audit tobe carried out tolook at howmany cases areCHC funded andhow many jointlyfunded via 117.All informationhas beenrequested fromthe LA. Oncecomplete reportwill be provided.
All outstandingcases to bemade priorityfor completion.
LA /ContinuingHealthcare Teamto review carepackages of CHCfunded patients,independantsupported livingor foster/adultplacements. Toexplore lessrestrictive ways ofdelivering care tonegate the risk ofa deprivation ofliberty occurring.
31/03/2020Fiona Kane
4 234 12 8
2. E
nsu
re T
he
De
live
ry O
f Sa
fe, H
igh
Qu
ality
Se
rvic
es T
ha
t De
live
r Th
e B
est O
utc
om
es
Fiona Kane
16Page

Risk RefRisk directorRisk owner L
Risk description Risk effect Initial
C L Score
Controls InternalAssurance
Current
C L Score
Gaps in controls Gaps in assurances Actions Target dateLead Officer
Acceptable
ScoreC
Risk title
NHS Northumberland CCG
Assurance Framework 17/09/2019
CorpObj
ExternalAssurance
1980
Jon Connolly
Procurement There is a risk thatthe CCG fails tofollow correct legalprocurementprocesses or hasinsufficient capacityto ensure this occursand leading to alegal challenge fromsuppliers
This would result inreputational damageto the CCG, a failureto deliver value formoney and improvedpatient services.
4 5 20 Legal advice takenfrom Hill DickensonSolicitors asappropriate
Sign off fromGoverning Body
Additional postshave been recruitedto CCG structure
Internal meetingto formalisestrategy forprocurement
29/11/2019Paul Turner
4 234 12 8
1. E
nsu
re T
ha
t Th
e C
CG
Ma
ke
s B
est U
se
Of A
llA
va
ilab
le R
eso
urc
es
Paul Turner
2125
Annie Topping
Implications ofInspection results onthe reputation of theCCG and quality ofprovision
There is a risk thatthe CCG as a keypartner will fail toaddress the findingsof the inspection anddeliver the WrittenStatement of Action.A re-inspection isdue to take placesometime in thefuture. Failure toaddress the gapsidentified in theinspection could leadto poor qualityservices andthereforereputational damageto the CCG.
This could result inpoor service qualitywhich leads to poorhealth outcomes ofchildren with SEND,and the CCG beingplaced in specialmeasures byregulators.
3 3 9 Strategic SENDBoard to monitorprogress on SENDWSOA
Reporting toGoverning Body
NHS Englandmonitoring forthe next 12months
LSR CQCCommittee in placeto monitor readinessfor area review
Governing Bodyreporting
These are newinspections andas it is an areainspection noteverything iswithin the gift ofthe CCG
WrittenStatement ofAction monitoredby SENDStrategic Group
31/12/2020AnnieTopping
LSR PID 31/03/2020SiobhanBrown
3 233 9 6
2. E
nsu
re T
he
De
live
ry O
f Sa
fe, H
igh
Qu
ality
Se
rvic
es T
ha
t De
live
r Th
e B
est O
utc
om
es
Sam Barron
1181
Graham Syers
Prescribing There is a risk thatpoor qualityprescribing or drugshortages could leadto patient safety andexperience issuesand unnecessaryprecribing costs.
This could ultimatelyresult in reputationaldamage, legalchallenge andunsustainableprescribing costgrowth to the CCG.
4 4 16 NECS horizonscanning documentsand cost growthprojections.
The MedicinesOptimisationGroup evaluatesregular NECSreports andaction plans areproduced asnecessary.
Internal auditreview onmedicinesmanagementApril 2019-substantialassurance).ServiceAuditor Reportfrom PwC onNHS BSAPrescriptionsPaymentsProcess2018/19.
The Departmentof Healthsometimesconsults with thePharmaceuticalServicesNegotiatingCommittee toadjust the amountcommissionerspay topharmacies. Thiscan result inadjustment ofCategory M(generic drugs)prices the CCGpay which cannegatively impact
4 224 8 8
2. E
nsu
re T
he
De
live
ry O
f Sa
fe, H
igh
Qu
ality
Se
rvic
es T
ha
t De
live
r Th
e B
est O
utc
om
es
RachelMitcheson
17Page

Risk RefRisk directorRisk owner L
Risk description Risk effect Initial
C L Score
Controls InternalAssurance
Current
C L Score
Gaps in controls Gaps in assurances Actions Target dateLead Officer
Acceptable
ScoreC
Risk title
NHS Northumberland CCG
Assurance Framework 17/09/2019
CorpObj
ExternalAssurance
drug spend.These changesare difficult toanticipate.
QIPP precribingplanning.
MOG membersmonitor of QIPPaction planprogressmonthly.CCG 14 daymeetingmonitors CFC monitorQIPP progressmonthly
NHSE monitorQIPP progresswith COO andCFO.
NECS MedicineManagementFunction
MedicinesOptimisationGroup
Proposedintroduction ofOptimiseRx - thissystem suggest themost cost andquality effective drugat the point ofprescription. Thisallows alternativemedication to besuggested whenthere are knownshortages.
The system willbe monitoredquarterly by theMedicinesOptimisationGroup
OptimiseRxintroduced Jun 16and data monitoredon a monthly basis
MedicinesOptimisationGroup (MOG)consider monthlydata. MOG minutesconsidered byJLEB
Internal Audit onMedicinesOptimisationNovember 2016
SubstantialAssurance
Quarterly prescribingreport: OverarchingReport, High CostDrugs Report,Controlled DrugsReport,AntimicrobialReport.
Ensures theMedicinesOptimisationGroup is awareof prescribingquality andperformanceissues. Allmanagement ofthese issues totake place.
There is a6-8week time lagwhen receivingmonthlyprescribing datawhich limits howquickly action canbe taken ifperformanceissues arise.
Practice MedicinesManagementworkplanachievement data
The workplanachievementdata givesoverview ofperformance
Some of theprescribing datahas a 6-8 weektime delay which
18Page
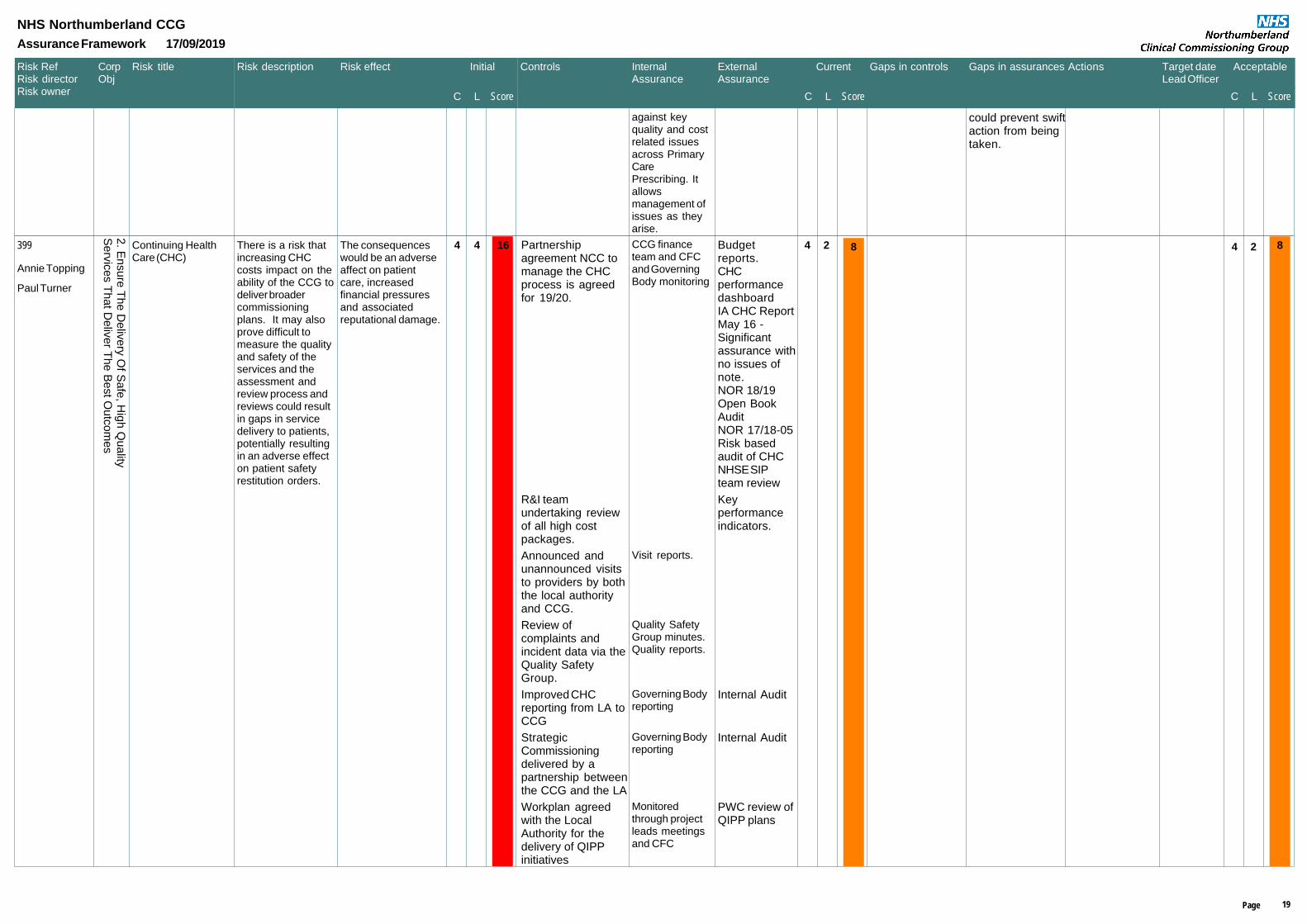
Risk RefRisk directorRisk owner L
Risk description Risk effect Initial
C L Score
Controls InternalAssurance
Current
C L Score
Gaps in controls Gaps in assurances Actions Target dateLead Officer
Acceptable
ScoreC
Risk title
NHS Northumberland CCG
Assurance Framework 17/09/2019
CorpObj
ExternalAssurance
against keyquality and costrelated issuesacross PrimaryCarePrescribing. Itallowsmanagement ofissues as theyarise.
could prevent swiftaction from beingtaken.
399
Annie Topping
Continuing HealthCare (CHC)
There is a risk thatincreasing CHCcosts impact on theability of the CCG todeliver broadercommissioningplans. It may alsoprove difficult tomeasure the qualityand safety of theservices and theassessment andreview process andreviews could resultin gaps in servicedelivery to patients,potentially resultingin an adverse effecton patient safetyrestitution orders.
The consequenceswould be an adverseaffect on patientcare, increasedfinancial pressuresand associatedreputational damage.
4 4 16 Partnershipagreement NCC tomanage the CHCprocess is agreedfor 19/20.
CCG financeteam and CFCand GoverningBody monitoring
Budgetreports.CHCperformancedashboardIA CHC ReportMay 16 -Significantassurance withno issues ofnote.NOR 18/19Open BookAuditNOR 17/18-05Risk basedaudit of CHCNHSE SIPteam review
R&I teamundertaking reviewof all high costpackages.
Keyperformanceindicators.
Announced andunannounced visitsto providers by boththe local authorityand CCG.
Visit reports.
Review ofcomplaints andincident data via theQuality SafetyGroup.
Quality SafetyGroup minutes.Quality reports.
Improved CHCreporting from LA toCCG
Governing Bodyreporting
Internal Audit
StrategicCommissioningdelivered by apartnership betweenthe CCG and the LA
Governing Bodyreporting
Internal Audit
Workplan agreedwith the LocalAuthority for thedelivery of QIPPinitiatives
Monitoredthrough projectleads meetingsand CFC
PWC review ofQIPP plans
4 224 8 8
2. E
nsu
re T
he
De
live
ry O
f Sa
fe, H
igh
Qu
ality
Se
rvic
es T
ha
t De
live
r Th
e B
est O
utc
om
es
Paul Turner
19Page

Risk RefRisk directorRisk owner L
Risk description Risk effect Initial
C L Score
Controls InternalAssurance
Current
C L Score
Gaps in controls Gaps in assurances Actions Target dateLead Officer
Acceptable
ScoreC
Risk title
NHS Northumberland CCG
Assurance Framework 17/09/2019
CorpObj
ExternalAssurance
1435
Siobhan Brown
CCG OperatingResilience
There is a risk thatexternal or internalevents could occurwhich could impacton the CCG's abilityto conduct routinebusiness (property orIT infrastructure,staffing levels) whichlead to capacity oroperational deliverygaps.
This could result inreduced operationaloutput, a potentialreduction in qualityof clinical services,and ultimatelydamage to theCCG's reputation.
4 3 12 Business ContinuityPlan approved byGoverning Body
Internal auditreview onbusinesscontinuity andemergencyplanningFebruary 2019(goodassurance)
EPRR returnsare submittedto NHSEngland forassurance onan annualbasis
Regional ITresilience group setup as required.
Regional EPRRteams and LADB
4 224 8 8
1. E
nsu
re T
ha
t Th
e C
CG
Ma
ke
s B
est U
se
Of A
llA
va
ilab
le R
eso
urc
es
Debra Elliott
1064
Annie Topping
SafeguardingVulnerable People
There is a risk thatfailure to comply withgood clinicalpractice, policies andprocedures,ineffectivemulti-agency andmulti-disciplinaryworking and notimplementing CaseReview action planswill result invulnerable people'ssafety beingcompromised andnon-compliance withstatutory regulations.
This could result in aderogation of patientcare with associatedreputational damageto the CCG andlitigation financialpressures.
4 4 16 SafeguardingChildren/adultPolicies andProcedures ofproviderorganisations andother agencies.
AnnualsafeguardingChildren andadult reportsreviewed SG.
Quarterlyperformancedashboardfrom providers.
Representation ofCCG onLSCB/NSAB CaseReview Groups.
SG standingagenda item.Regular audit ofGP practices.
Quarterlyproviderassurance.
CCG's own internalstatutoryarrangements
InternalgovernancearrangementsSG / CMB
Internal AuditFinal Report -NOR 1718/03:Safeguarding -LessonsLearntFebruary 2018Significantassurance.
4 224 8 8
2. E
nsu
re T
he
De
live
ry O
f Sa
fe, H
igh
Qu
ality
Se
rvic
es T
ha
t De
live
r Th
e B
est O
utc
om
es
Margaret Tench
20Page
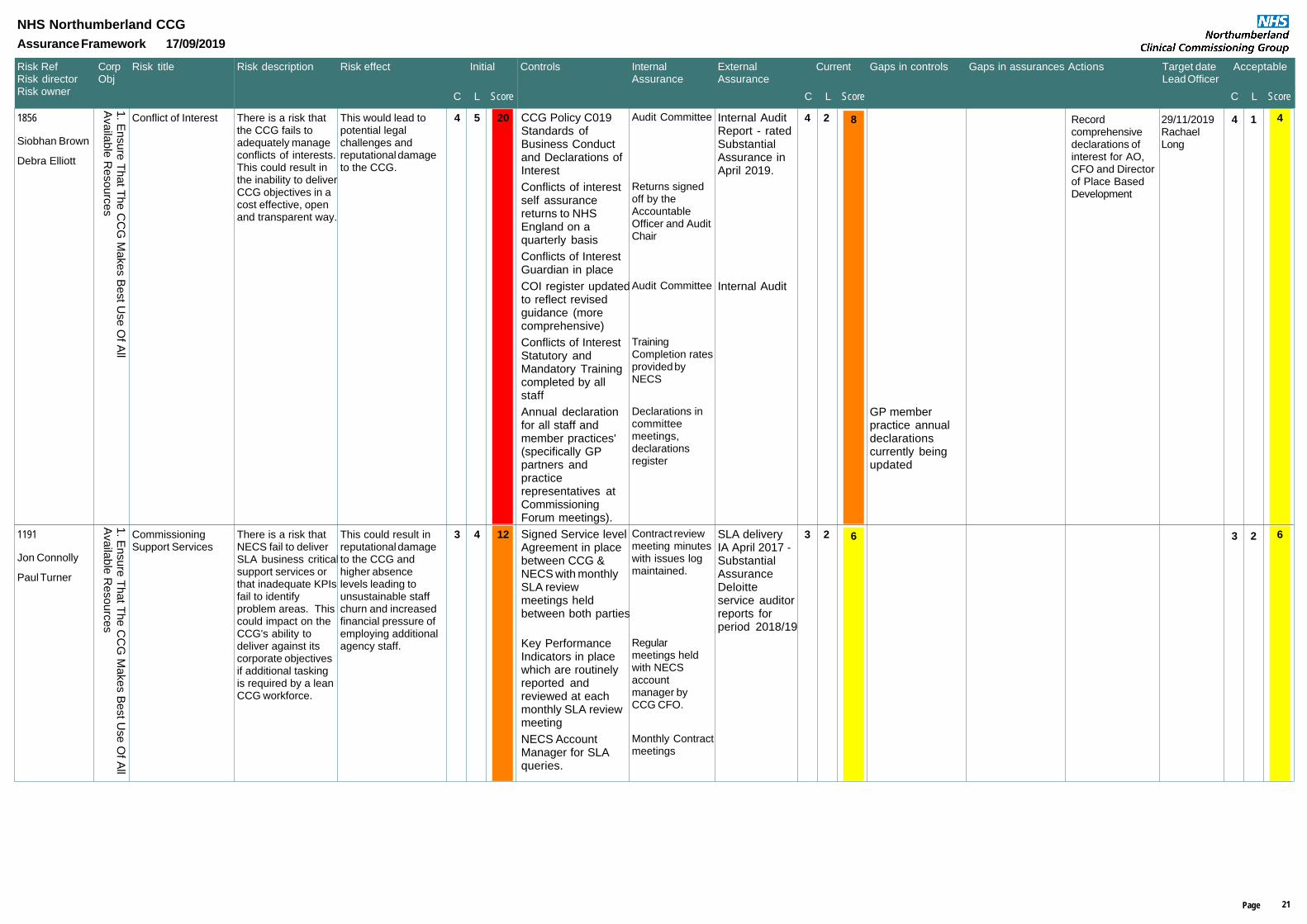
Risk RefRisk directorRisk owner L
Risk description Risk effect Initial
C L Score
Controls InternalAssurance
Current
C L Score
Gaps in controls Gaps in assurances Actions Target dateLead Officer
Acceptable
ScoreC
Risk title
NHS Northumberland CCG
Assurance Framework 17/09/2019
CorpObj
ExternalAssurance
1856
Siobhan Brown
Conflict of Interest There is a risk thatthe CCG fails toadequately manageconflicts of interests.This could result inthe inability to deliverCCG objectives in acost effective, openand transparent way.
This would lead topotential legalchallenges andreputational damageto the CCG.
4 5 20 CCG Policy C019Standards ofBusiness Conductand Declarations ofInterest
Audit Committee Internal AuditReport - ratedSubstantialAssurance inApril 2019.
Conflicts of interestself assurancereturns to NHSEngland on aquarterly basis
Returns signedoff by theAccountableOfficer and AuditChair
Conflicts of InterestGuardian in place
COI register updatedto reflect revisedguidance (morecomprehensive)
Audit Committee Internal Audit
Conflicts of InterestStatutory andMandatory Trainingcompleted by allstaff
TrainingCompletion ratesprovided byNECS
Annual declarationfor all staff andmember practices'(specifically GPpartners andpracticerepresentatives atCommissioningForum meetings).
Declarations incommitteemeetings,declarationsregister
GP memberpractice annualdeclarationscurrently beingupdated
Recordcomprehensivedeclarations ofinterest for AO,CFO and Directorof Place BasedDevelopment
29/11/2019RachaelLong
4 124 8 4
1. E
nsu
re T
ha
t Th
e C
CG
Ma
ke
s B
est U
se
Of A
llA
va
ilab
le R
eso
urc
es
Debra Elliott
1191
Jon Connolly
CommissioningSupport Services
There is a risk thatNECS fail to deliverSLA business criticalsupport services orthat inadequate KPIsfail to identifyproblem areas. Thiscould impact on theCCG's ability todeliver against itscorporate objectivesif additional taskingis required by a leanCCG workforce.
This could result inreputational damageto the CCG andhigher absencelevels leading tounsustainable staffchurn and increasedfinancial pressure ofemploying additionalagency staff.
3 4 12 Signed Service levelAgreement in placebetween CCG &NECS with monthlySLA reviewmeetings heldbetween both parties
Contract reviewmeeting minuteswith issues logmaintained.
SLA deliveryIA April 2017 -SubstantialAssuranceDeloitteservice auditorreports forperiod 2018/19
Key PerformanceIndicators in placewhich are routinelyreported andreviewed at eachmonthly SLA reviewmeeting
Regularmeetings heldwith NECSaccountmanager byCCG CFO.
NECS AccountManager for SLAqueries.
Monthly Contractmeetings
3 223 6 6
1. E
nsu
re T
ha
t Th
e C
CG
Ma
ke
s B
est U
se
Of A
llA
va
ilab
le R
eso
urc
es
Paul Turner
21Page

Risk RefRisk directorRisk owner L
Risk description Risk effect Initial
C L Score
Controls InternalAssurance
Current
C L Score
Gaps in controls Gaps in assurances Actions Target dateLead Officer
Acceptable
ScoreC
Risk title
NHS Northumberland CCG
Assurance Framework 17/09/2019
CorpObj
ExternalAssurance
1508
Annie Topping
MentalHealthTransformation Programme
There is a risk thatthe programme failsto deliver therequired reduction inthe mental healthbed base resulting infinances unable tobe released toimprove communityservices. This willlead to additionalnon-elective activity.
This will resultderogated patientcare, variations inquality by localityand increasedfinancial pressure onthe CCG.
3 4 12 Monthly contractsmanagementmeeting with NTW
Mental HealthStrategic Meeting
Chaired byNECS
STP MH workstream CMB andGoverning Body
HWBBNHS Englandquarterlyassurancemeeting
MH TransformationPlan now beingdelivered
SystemTransformationBoard
Internal AuditOSC
Completedevelopment ofMHTransformationPlan
01/07/2019Kate O'Brien
MH Investmentfunding to supportthe developmentof a universalcrisis team whichwill work toprevent hospitaladmissionwherever possibleand providesupport to thoseclients residing athome or in a carehome setting.
31/12/2019Kate O'Brien
3 223 6 6
2. E
nsu
re T
he
De
live
ry O
f Sa
fe, H
igh
Qu
ality
Se
rvic
es T
ha
t De
live
r Th
e B
est O
utc
om
es
Kate O'Brien
744
Jon Connolly
Anti-FraudArrangements
There is a risk thatineffective anti-fraudarrangements, orstaff failing to adhereto comprehensiveinstructions orundertake mandatorytraining, will notprevent bribery andcorruption leading toa breach of nationalstandards and CCGliability under theBribery Act 2010.
This would result inreputational damageto the CCG.
4 3 12 CO19- Standards ofBusiness ConductPolicy - April 2019
Standards ofBusinessConduct Policyhas beenupdated toincludereference to theBribery Act 2010
Internal Auditreview ondeclarations ofinterest - April2019substantialassurance thatthe CCG isgenerallycompliant withtherequirementsof the Health &Social CareAct 2012 inrelation todeclarations ofinterest.
Procurementprocedures in placewithin NECS / SBS
ISAE Reportissued byDeloitte onoperation ofNECS incertain areasfor the period1/4/18 to31/3/19.Covered underongoingServiceAuditor reporttesting byDeloitte newyear reportdue in April aspart of annualaccountsprocess.
4 114 4 4
1. E
nsu
re T
ha
t Th
e C
CG
Ma
ke
s B
est U
se
Of A
llA
va
ilab
le R
eso
urc
es
Jon Connolly
22Page

Risk RefRisk directorRisk owner L
Risk description Risk effect Initial
C L Score
Controls InternalAssurance
Current
C L Score
Gaps in controls Gaps in assurances Actions Target dateLead Officer
Acceptable
ScoreC
Risk title
NHS Northumberland CCG
Assurance Framework 17/09/2019
CorpObj
ExternalAssurance
Inclusion in CCGAnnual Accounts ofrelated third partytransactions.
IndependentAuditorsReport issuedby Mazars LLPMay 2019.Included withinthe annualreport, nomaterial issuesfound.
Annual Review ofDeclaration ofInterests Register bythe CCG AuditCommittee.
Minutes of theAudit Committeemeeting.
Anti-fraudarrangements inplace which include:Local Counter FraudSpecialist (LCFS) inplace Approved Anti-fraudpolicyAnnual anti-fraudplan approved byAudit CommitteeCounter fraudawarenessmandatory trainingand InformationGovernance relatedto Cyber Crime
Audit CommitteeminutesQuarterlytraining report toGovernanceGroupAssessment ofanti-fraudarrangementsundertaken.
Regularupdate reportsfrom LCFS toAuditCommittee.Annual Reporton anti-fraudawarenessreport to AuditCommittee.Carried out byPaul Bevan.SRT inattachments.
Budget approvalprocess, PurchaseOrder requirementsfor payments.Scheme ofdelegation andapproval hierarchy inplace.
Finance policyfor budgetaryapprovaldeveloped redetailed financialPolicies, 'nocontract, no PO,no Payment'policy for budgetmanagers.Limits set anagreed byCorporateFinanceCommittee andGoverning Body.(New limitsgoing to SeptCFC and GB)
23Page

Risk RefRisk directorRisk owner L
Risk description Risk effect Initial
C L Score
Controls InternalAssurance
Current
C L Score
Gaps in controls Gaps in assurances Actions Target dateLead Officer
Acceptable
ScoreC
Risk title
NHS Northumberland CCG
Assurance Framework 17/09/2019
CorpObj
ExternalAssurance
1190
Siobhan Brown
InformationGovernance
A failure to embedinformation riskmanagement intoCCG business andto comply withinformationgovernance policiescould lead toinformationinefficiencies andrisks not beingidentified andassessed.
This could result inconfidentialitybreaches or a failureto embrace a spirit ofopenness andhonesty which maylead to litigation andconsequent financialand reputational riskto the CCG.
4 3 12 InformationGovernanceFramework in placewhich includespolicies andInformationGovernanceStrategy
NHS DigitalData Securityand ProtectionSelfAssessmentToolkit.NECs ServiceAuditor Report2018/19IG Toolkit IAMarch 2019 -SubstantialAssurance
InformationGovernancemandatory trainingfor all CCG staffCompliance is beingmonitoredthroughout 2018/19.100% completionrates achieved forIG. Next year reviewafter 31 December2019.
Compliance withIG training ismonitored by theGoveranceGroup
Caldicott Guardianand SIRO in place inCCG. Both requiredto undertake annualtraining specific totheir roles.
Completion ofannual trainingmonitored byGovernanceGroup
No patientidentifiable data ishandled by the CCG- patient dataprovided by NECS isroutinelypseudonymised.
DeloitteService auditorreport covering1-4-18 to31-3-19. Nextannual reportfor 2018-19 tobe publishedin May 2019as part ofannualaccountsprocess.
Implementation ofGDPR requirements
Part of theNECS SLA
DeloitteService auditorreport covering1-4-17 to31-3-18. Nextannual reportfor 2018-19 tobe released inMay 2019 aspart of annualaccountsprocess.
New SIRO in place
4 114 4 4
2. E
nsu
re T
he
De
live
ry O
f Sa
fe, H
igh
Qu
ality
Se
rvic
es T
ha
t De
live
r Th
e B
est O
utc
om
es
Siobhan Brown
24Page

Risk RefRisk directorRisk owner L
Risk description Risk effect Initial
C L Score
Controls InternalAssurance
Current
C L Score
Gaps in controls Gaps in assurances Actions Target dateLead Officer
Acceptable
ScoreC
Risk title
NHS Northumberland CCG
Assurance Framework 17/09/2019
CorpObj
ExternalAssurance
from July 2019 -Chief OperatingOfficer
25Page
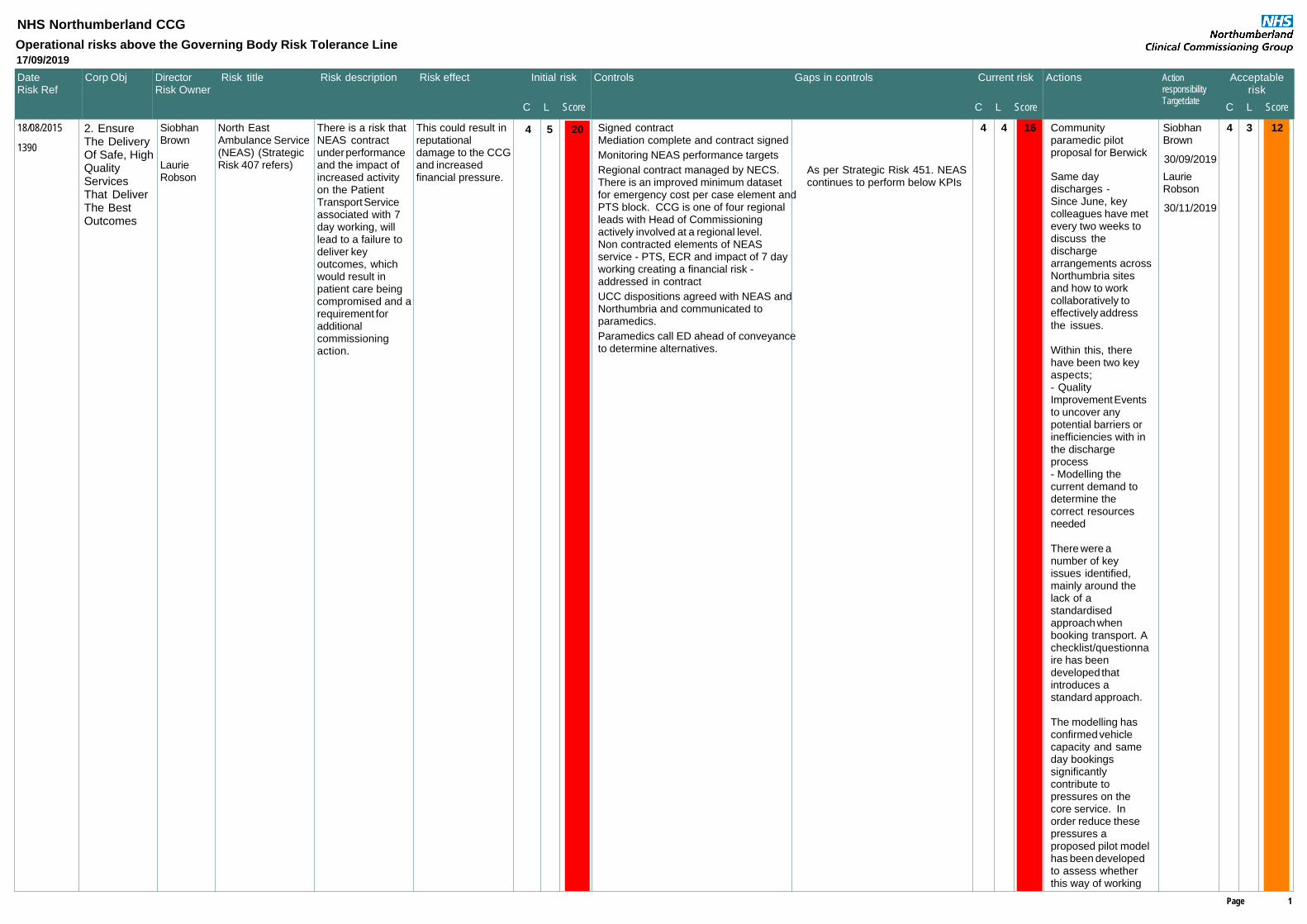
L
DirectorRisk Owner
Risk title Risk description Risk effect Initial risk
C L Score
Controls Gaps in controls Actions ActionresponsibilityTarget date
Acceptablerisk
Score
DateRisk Ref
NHS Northumberland CCG
Operational risks above the Governing Body Risk Tolerance Line
17/09/2019
C
Corp Obj Current risk
C L Score
18/08/2015
1390
SiobhanBrown
LaurieRobson
North EastAmbulance Service(NEAS) (StrategicRisk 407 refers)
There is a risk thatNEAS contractunder performanceand the impact ofincreased activityon the PatientTransport Serviceassociated with 7day working, willlead to a failure todeliver keyoutcomes, whichwould result inpatient care beingcompromised and arequirement foradditionalcommissioningaction.
This could result inreputationaldamage to the CCGand increasedfinancial pressure.
4 4 16Signed contractMediation complete and contract signed
Monitoring NEAS performance targets
Regional contract managed by NECS.There is an improved minimum datasetfor emergency cost per case element andPTS block. CCG is one of four regionalleads with Head of Commissioningactively involved at a regional level.Non contracted elements of NEASservice - PTS, ECR and impact of 7 dayworking creating a financial risk -addressed in contract
As per Strategic Risk 451. NEAScontinues to perform below KPIs
UCC dispositions agreed with NEAS andNorthumbria and communicated toparamedics.
Paramedics call ED ahead of conveyanceto determine alternatives.
Communityparamedic pilotproposal for Berwick
SiobhanBrown
30/09/2019
Same daydischarges - Since June, keycolleagues have metevery two weeks todiscuss thedischargearrangements acrossNorthumbria sitesand how to workcollaboratively toeffectively addressthe issues.
Within this, therehave been two keyaspects; - QualityImprovement Eventsto uncover anypotential barriers orinefficiencies with inthe dischargeprocess- Modelling thecurrent demand todetermine thecorrect resourcesneeded
There were anumber of keyissues identified,mainly around thelack of astandardisedapproach whenbooking transport. Achecklist/questionnaire has beendeveloped thatintroduces astandard approach.
The modelling hasconfirmed vehiclecapacity and sameday bookingssignificantlycontribute topressures on thecore service. Inorder reduce thesepressures aproposed pilot modelhas been developedto assess whetherthis way of working
LaurieRobson
30/11/2019
4 3 1254 202. EnsureThe DeliveryOf Safe, HighQualityServicesThat DeliverThe BestOutcomes
Page 1

L
DirectorRisk Owner
Risk title Risk description Risk effect Initial risk
C L Score
Controls Gaps in controls Actions ActionresponsibilityTarget date
Acceptablerisk
Score
DateRisk Ref
NHS Northumberland CCG
Operational risks above the Governing Body Risk Tolerance Line
17/09/2019
C
Corp Obj Current risk
C L Score
meets current andforecast demand.
05/11/2013
733
AnnieTopping
AnnieTopping
HealthcareAssociatedInfections (StrategicRisk 407 refers).
The numbers ofhealthcareassociatedinfections e.g. c.diff,MRSA, Norovirusand Gram -ve bloodstream infectionparticularly in thecommunity,continue toincrease. Thiswould also lead to afailure in meetingthe nationalambition andachieving qualitypremium for CCG.
Adverse impact onpatient care andservice quality Potential risk toother patients Failing to meetquality standardsFailing to securefinancial incentives (Strategic Risk 407refers)
3 4 12Bi-monthly HCAI Workstream meetingallowing focused discussion with acutetrusts' clinicians and microbiologists andmedicine optimisation leads. Onwardreporting to the Quality and Safety Group(QSG) and CMB.
Bi-monthly monitoring and scrutinythrough QRGs, and ad hoc deep dive.
Monitoring amd evaluation of antibioticprescribing data (monthly at CCG leveland quarterly at practice level) by NECSpharmacist and feed into HCAIworkstream meetings.
RCAs for all MRSA and C.Diff incidentsand reviewed at bi monthly HCAIWorstream to identify lessons to be learntand monitor progress.
Collaborative working and share learningat North of Tyne level through the HCAIReduction Partnership.
WInter SITREP reports to monitorincidents and identify potential outbreaksfor futher actions
Development of a HCAI workplan for2019/20
Northumberland GNBSI action plan. No robust evidence base onreduction of GNBSI.
Monitoring and sharing learning at CNElevel through the HCAI ImprovementBoard (formerly the GNBSI CollaborativeBoard)
Limited system wide actionsagreed.
Regular review toensure newevidence is includedwhen it is available.
AnnieTopping
31/03/2020
3 2 633 92. EnsureThe DeliveryOf Safe, HighQualityServicesThat DeliverThe BestOutcomes
01/03/2016
1492
AnnieTopping
AnnieTopping
Maternity staffshortages atNESCH and MLUs.(Strategic Risk 407refers)
High levels ofsickness andvacancy at NESCHmaternity serviceshave resulted in alarge number ofunfilled shifts andunable to meet theincreasing demand.
Ongoingrecruitment issuesat MLUs haveimpacted on theability to releasemidwives onto therotation programmeto NESCH to keepup skills andcompetencies, andmaintain the currentlevel of service.
Adverse impact onpatient safety andquality of services.Reputationaldamage to theCCG.Litigation andfinancial loss.
4 3 12Trust has put in place maternityescalation plan if there is an increase indemand or staffing issues. Actions are inplace to mitigate by drawing in staffingfrom midwifery management / matronsroles and specialist midwifery posts tosupport the unit and ensure safestandards of care are maintained.
Trust has recruited additional band 6 staffto meet with increasing demand.
Monitor maternity services at NSECH andMLUs to ensure patient safety.
The Trust has implemented temporaryovernight closure at Alnwick MLU as fromNov 2016 to reduce overall staffingrequirement.
A strategic decision on the futureprovision of MLU is yet to bemade.
21/05/2019
4 2 844 162. EnsureThe DeliveryOf Safe, HighQualityServicesThat DeliverThe BestOutcomes
Page 2

L
DirectorRisk Owner
Risk title Risk description Risk effect Initial risk
C L Score
Controls Gaps in controls Actions ActionresponsibilityTarget date
Acceptablerisk
Score
DateRisk Ref
NHS Northumberland CCG
Operational risks above the Governing Body Risk Tolerance Line
17/09/2019
C
Corp Obj Current risk
C L Score
24/11/2015
1447
SiobhanBrown
PamelaPhelps
Low AcuityActivity(StrategicRisk 945 refers)
There is a risk thatincreasednon-elective activitywhich results inadditional resourcebeing requiredeither to fundNHCFT (above thecurrent cap) orNUFT
This could result inunsustainable costpressures, therelated failure todeliver othercommissioning planobjectives, with theassociated patientcare derogation,and reputationaldamage to theCCG. (StrategicRisk 945 refers).
4 3 12Chief Officer level meetings to identifysystem wide actions.STP and FRP actions include redesign ofemergency care post-NSECH.Contract negotiated back to PbR onurgent care centres and reclassification totype 3.
UEC delivery plan has been updated andCCG Planning and Operational deliveryteams in place. Controls linked to Risk945
Controls linked to Risk 945
Emergency activity monitored on monthlybasis at internal finance and activitymeetings.
Procurement ofurgent andemergency careincluding out ofhours with a view toestablishing UTCsand primary carehubs with reducedduplication
SiobhanBrown
29/11/2019
Negotiated blendedtariff for UEC andclose contract andclinical monitoring ofactivity type and itsclinicalappropriateness inthe settings - newambulatory spaceopens at NSECH 18June 2019
SiobhanBrown
31/10/2019
4 2 854 204. DeliverClinically LedHealthServicesThat AreFocused OnIndividualAnd WiderPopulationNeeds AndBased OnEvidence
18/01/2017
1799
JonConnolly
JonConnolly
QIPP (StrategicRisk 946 refers)
There is a risk thatthe 2019-20 QIPPplan is underdelivered, andsufficient pipelineschemes areidentified to offset inyear under delivery.
This will result inincreased financialpressure andreputationaldamage to theCCG.
4 3 12QIPP tracker monitoring and QIPPassurance reported to Corporate FinanceCommittee and Governing Body.
Development of detailed QIPP includingproject milestones.
PMO and portfolio management in CCGstructure.
Joint QIPP/CIPunderstandingacross allorganisations in thesystem, developedas part of theTransformationBoard
RichardTurnbull
31/03/2020
4 2 854 201. EnsureThat TheCCG MakesBest Use OfAll AvailableResources
Page 3

NHS Northumberland CCG
New risks added from: 14/05/2019 to 17/09/2019
DateRisk RefReview FreqRisk type
DirectorOwner
Details Current score
C L Score
Controls AssurancesGaps in controls Gaps in assurance
2134
15/05/2019 PaulTurner
PamelaPhelps
Quality and continuity of patientserviceThere is a risk that patient servicesmay be affected in Laburnumsurgery by failure to provide highquality and effective primary careThis could result in removal of GPregistration an d the contract todeliver services to 2300 patients incentral locality. As a result of thisneighbouring practices may beadversely affected by having toadapt their capacity to ensurecontinuity of services for theLaburnum patients as well their own.
4 3 12
(3). Monthly
Primary care support teamworking with NHSE and CQC tomonitor actions on a regularbasis.
CCG action logincorporates all actions.CCG evidence data baseof support provided topractice.NHSE action plan in placeCGC action plan in place
Contract position at Laburnumdiscussed at PCCOG bi-monthly
CCG provide regularverbal updatesNHSE provide writtenreport as required
Formal actions reported to PCCCto be undertaken as perrequirements
CCG provide a verbal orwritten update on currentposition of practicecontract NHSE provide a verbal orwritten update on currentposition of practicecontract
Strategic -
2182
05/09/2019 AnnieTopping
FionaKane
The CCG will not beprepared/resourced to meet itsresponsibilities for theimplementation of the LibertyProtection Safeguards (LPS).As a result of proposed legislativechanges which will introduce theLiberty Protection Safeguards (LPS)there is a risk the CCG will not beprepared and resourced to meet itsresponsibilities for the authorisationand management of LPSauthorisations for CHC patients. Which may result in the CCG beingopen to legal challenge, civil action,financial costs (e.g. compensation orlegal costs) and present a risk forpatients being unlawfully detained.
4 3 12
(5). Quarterly
Regional LPS implementationgroup
The final nationalguidance has not yetbeen issued makingdifficult to document thefull implementation plan
Minutes of the LPSimplementation group
Strategic -
Page 1

Risk RefRisk Type
Date closedCurrent Score
AcceptableScore
Reason for closureDescription of risk
NHS Northumberland CCG - risks closed from 14/05/2019 to 17/09/2019
1504
Operational -
Primary Care Delegated Commissioning There is a risk that conflicts of interest are notdeclared, or once they are, they reach a level thatprecludes the delivery of the operational business ofthe Northumberland Primary Care CommissioningCommittee.This could lead to delays in decision making,potential derogation to patient care and a lack ofconfidence in the CCG by member practices leadingto reputational damage to the CCG
Risk No Longer Applies
Risk merged into risk 1856
8 4 10/09/2019
1797
Operational -
Conflicts of InterestThere is a risk that the CCG's governance structurewill result in additional Conflicts of Interest beingdeclared. This could result in the CCG's decisionmaking process being adversely affected. Leading to sub-optimal strategic commissioningdecisions and resultant reputational damage to theCCG.
Risk No Longer Applies
Risk merged into risk 1856
8 8 10/09/2019

Agenda Item: 10.3
OFFICIAL
1 20190925 UC Agenda Item 10.3 EPRR Core Standards Self-Assessment
Clinicians commissioning healthcare for the people of Northumberland
Meeting title Governing Body
Date 25 September 2019
Agenda item 10.3
Report title Emergency Preparedness, Resilience and Response
(EPRR) Core Standards Self Assessment
Report author NECS Senior Governance Officer
Sponsor Deputy Head of Governance
Private or Public agenda
Public
NHS classification Official
Purpose (tick one only)
Information only
Development/Discussion
Decision/Action
Links to Corporate Objectives Ensure that the CCG makes best use of all available resources
Ensure the delivery of safe, high quality services that deliver the best outcomes
Create joined up pathways within and across organisations to deliver seamless care
Deliver clinically led health services that are focused on individual and wider population needs and based on evidence.
Northumberland CCG/external meetings this paper has been discussed at:
None
QIPP N/A

OFFICIAL
20190925 UC Agenda Item 10.3 EPRR Core Standards Self-Assessment
2
Risks Strategic Risk 1178 System Resilience and Escalation Planning (current score 15), Strategic Risk 1435 CCG Operating Resilience (current score 8).
Resource implications N/A Consultation/engagement N/A Quality and Equality impact assessment
Completed.
Research N/A Legal implications N/A Impact on carers N/A Sustainability implications N/A

OFFICIAL
20190925 UC Agenda Item 10.3 EPRR Core Standards Self-Assessment
3
QUALITY and EQUALITY IMPACT ASSESSMENT
1. Project Name EPPR Core Standards Self Assessment
2. Project Lead Director Lead Project Lead Clinical Lead Siobhan Brown Deputy Head of
Governance
3. Project Overview & Objective
Not applicable – no schemes.
4. Quality Impact Assessment
Impact Details Pos/ Neg
C L Scores
Mitigation / Control
Patient Safety There is a risk that a lack of robust planning for surges in demand for frontline services mean that urgent and emergency care pressures increase, resulting in rises in A&E activity and multiple demands on ambulance, community, acute and primary care services. This could lead to insufficient resource being available. This will lead to impact on organisational performance at provider level and reputation impact on the CCG There is a risk that external or internal events could occur which could impact on the CCG’s
5 4 Internal Audit on Emergency Planning and Business Continuity A&E Delivery Board chaired by NHCFT CEO - delivering 5 mandated areas; now configured with a separate Executive and Operational function NHS I and NHS E involvement in system wide delivery plans Local A&E Delivery Board action plan in place, also reshaped LADB with executive board and operational group for delivery The CCG has a business continuity plan in place. The CCG has an absence management policy in place

OFFICIAL
20190925 UC Agenda Item 10.3 EPRR Core Standards Self-Assessment
4
ability to conduct routine business which could lead to capacity or operational delivery gaps. This could result in a reduced operational output, a potential reduction in quality of clinical services, and ultimately damage to the CCG’s reputation.
NECS IT manage the IT and telephone system Regional IT resilience group set up as required.
Clinical Effectiveness As above Patient Experience As above Others including reputation, information governance and etc.
As above
5.Equality Impact Assessment
Impact Details Pos/ Neg
C L Scores
Mitigation / Control
What is the impact on people who have one of the protected characteristics as defined in the Equality Act 2010?
NA
What is the impact on health inequalities in terms of access to services and outcomes achieved for the population of Northumberland?
NA
6. Research Reference to relevant local and national research as appropriate.
NA
7. Metrics Sensitive to the impacts or risks on quality and equality and can be used for ongoing monitoring.
Impact Descriptors
Baseline Metrics Target
NA

OFFICIAL
20190925 UC Agenda Item 10.3 EPRR Core Standards Self-Assessment
5
8. Completed By Signature Printed Name
Date
Wendy Marley Governance Officer
Wendy Marley
21/08/2019
Additional Relevant Information:
8. Clinical Lead Approval by Signature Printed Name
Date
Additional Relevant Information:
9. Reviewed By Signature Printed Name
Date
Deputy Head of Governance
Debra Elliott
21.08.19
Comments

OFFICIAL
20190925 UC Agenda Item 10.3 EPRR Core Standards Self-Assessment
6
Governing Body 25 September 2019 Agenda Item: 10.3 Emergency Preparedness, Resilience and Response Core Standards Self-Assessment Sponsor: Chief Operating Officer
Members of the Governing Body are asked to: 1. Consider the content of the Emergency Preparedness, Resilience and Response
(EPRR) Self-Assessment. 2. Ratify the submission of the 2019/20 EPRR Self-Assessment.
Purpose This report outlines the EPRR Core Standards Template and Assurance Statement requirement and seeks NHS Northumberland Clinical Commissioning Group’s (CCG) Governing Body’s ratification of the submission. Background NHS England (NHSE) is required to be able to plan for and respond to a wide range of emergencies and business continuity incidents that could affect health or patient safety. Under the Civil Contingencies Act (2004), NHS organisations and providers of NHS funded care must show that they can effectively respond to emergencies and business continuity incidents while maintaining services to patients. CCGs are responsible for co-operating and sharing relevant information with other responders in the event of an emergency. NHS funded providers are required to carry out a self-assessment against the EPRR core standards and provide evidence that their Boards are sighted on the level of compliance achieved. The CCG is a category 2 responder and as such, is required by NHSE to complete a self-assessment against these standards. Process Once organisations have completed the assessment the Local Health Resilience Partnership (LHRP) will assess the submission and undertake a peer review. The LHRP Co-Chairs will submit their reports to the NHS Regional Teams who will undertake a regional consolidation process. NHSE Regional Teams will coordinate a submission to evidence their level of assurance and inform the national assurance assessment.

OFFICIAL
20190925 UC Agenda Item 10.3 EPRR Core Standards Self-Assessment
7
NHSE business continuity assurance will be undertaken once and in conjunction with the NHSE Business Continuity Team, via the NHS EPRR Core Standards template. Assurance Ratings Organisations will be expected to state an overall assurance rating as to whether they are Fully, Substantially, Partially or Non-Compliant with the NHS EPRR Core Standards.
CCG Self-Assessment
The CCG’s self-assessment is green (fully compliant) as set out in Table 1 below. This is mirrored by neighbouring CCGs. Table 1 core standards 2019/20
The CCG’s self-assessment (Appendix 1) was submitted, subject to Governing Body’s ratification, to NHSE on 10 September (the submission deadline). Adverse Weather Deep Dive The self-assessment tool includes a deep dive section. CCGs are asked to provide assurance on eight deep dive statements although these do not contribute to the organisation’s overall EPRR assurance rating. The deep dive into adverse weather focuses on the CCG’s readiness in relation to:
Adverse weather response, Long term adaptation planning.
The CCG is fully compliant with 12 of the 19 deep dive standards. Table 2 sets out the CCG’s compliance with applicable adverse weather standards.
Core StandardsTotal
standards applicable
Fully compliant
Partially compliant
Non compliant
Governance 6 6 0 0Duty to risk assess 2 2 0 0Duty to maintain plans 9 9 0 0Command and control 2 2 0 0Training and exercising 3 3 0 0Response 5 5 0 0Warning and informing 3 3 0 0Cooperation 4 4 0 0Business Continuity 9 9 0 0CBRN 0 0 0 0Total 43 43 0 0

OFFICIAL
20190925 UC Agenda Item 10.3 EPRR Core Standards Self-Assessment
8
Table 2 deep dive standards
Action plans are being developed for the six areas where the CCG is partially compliant. There is one standard where the CCG is non-compliant. This relates to the inclusion of a climate change risk on the CCG’s risk register. While there are two existing risks that are linked to adverse weather (risk ref 1178 relates to surge management and risk ref 1435 relates to infrastructure), the CCG will need to carry out a risk assessment using based on HM Government Climate Change Risk Assessment (2017). Recommendation Governing Body is asked to ratify the submission of the CCG’s EPRR 2019/20 self-assessment. Appendix 1: EPRR 2019/20 self-assessment Appendix 2: 2019 EPRR statement of compliance

Ref Domain Standard DetailClinical
Commissioning Group
Evidence - examples listed below Organisational Evidence
Self assessment RAG
Red (not compliant) = Not compliant with the core standard. The organisation’s EPRR work programme shows compliance will not be
reached within the next 12 months.
Amber (partially compliant) = Not compliant with core standard. However, the organisation’s EPRR work programme demonstrates sufficient evidence of progress and an action plan to achieve full
compliance within the next 12 months.
Green (fully compliant) = Fully compliant with core standard.
Action to be taken Lead Timescale Comments
1 Governance Senior Leadership
The organisation has appointed an Accountable Emergency Officer (AEO) responsible for Emergency Preparedness Resilience and Response (EPRR). This individual should be a board level director, and have the appropriate authority, resources and budget to direct the EPRR portfolio.
A non-executive board member, or suitable alternative, should be identified to support them in this role.
Y
• Name and role of appointed individual
The Chief Operating Officer is the appointed AEO Fully compliant N/A Siobhan Brown, Chief Operating Officer
2 Governance EPRR Policy Statement
The organisation has an overarching EPRR policy statement.
This should take into account the organisation’s:• Business objectives and processes• Key suppliers and contractual arrangements• Risk assessment(s)• Functions and / or organisation, structural and staff changes.
The policy should: • Have a review schedule and version control• Use unambiguous terminology• Identify those responsible for ensuring policies and arrangements are updated, distributed and regularly tested• Include references to other sources of information and supporting documentation.
Y
Evidence of an up to date EPRR policy statement that includes:• Resourcing commitment• Access to funds• Commitment to Emergency Planning, Business Continuity, Training, Exercising etc.
Included in Business Continuity PlanRisks reviewed regularly at:Governance GroupAudit CommitteeGoverning Body
Fully compliant N/A Debra Elliott, Deputy Head of Governance
3 Governance EPRR board reports
The Chief Executive Officer / Clinical Commissioning Group Accountable Officer ensures that the Accountable Emergency Officer discharges their responsibilities to provide EPRR reports to the Board / Governing Body, no less frequently than annually.
These reports should be taken to a public board, and as a minimum, include an overview on:• training and exercises undertaken by the organisation• summary of any business continuity, critical incidents and major incidents experienced by the organisation• lessons identified from incidents and exercises• the organisation's compliance position in relation to the latest NHS England EPRR assurance process.
Y
• Public Board meeting minutes• Evidence of presenting the results of the annual EPRR assurance process to the Public Board
Annual Bord Reports Fully compliant N/A Chilef Operating Officer
4 Governance EPRR work programme
The organisation has an annual EPRR work programme, informed by:• lessons identified from incidents and exercises • identified risks • outcomes of any assurance and audit processes.
Y
• Process explicitly described within the EPRR policy statement• Annual work plan
Included in Business Continuity Plan Fully compliant N/A Deputy Head of Governance
5 Governance EPRR Resource
The Board / Governing Body is satisfied that the organisation has sufficient and appropriate resource, proportionate to its size, to ensure it can fully discharge its EPRR duties.
Y
• EPRR Policy identifies resources required to fulfill EPRR function; policy has been signed off by the organisation's Board• Assessment of role / resources• Role description of EPRR Staff• Organisation structure chart • Internal Governance process chart including EPRR group
Annual Bord Reports Fully compliant N/A Chilef Operating Officer
6 Governance Continuous improvement process
The organisation has clearly defined processes for capturing learning from incidents and exercises to inform the development of future EPRR arrangements.
Y• Process explicitly described within the EPRR policy statement There is a CCG LHRP representative. BCP is developed in
conjunction with local authority, Newcastle Gateshead CCG and North Tyneside CCG
Fully compliant N/A Chilef Operating Officer
7 Duty to risk assess Risk assessment
The organisation has a process in place to regularly assess the risks to the population it serves. This process should consider community and national risk registers. Y
• Evidence that EPRR risks are regularly considered and recorded• Evidence that EPRR risks are represented and recorded on the organisations corporate risk register
BCP/EPRR implemented in the CCG. Risks are recorded on the risk register and discussed at Governing Body and Audit Committee on a quarterly basis.Business impact analysis carried out on all CCG activities
Fully compliant N/A Deputy Head of Governance
8 Duty to risk assess Risk Management
The organisation has a robust method of reporting, recording, monitoring and escalating EPRR risks.
Y
• EPRR risks are considered in the organisation's risk management policy • Reference to EPRR risk management in the organisation's EPRR policy document
Risk management policy is updated regularly and describes the escalation process for all risks which includes any EPRR risks.
Fully compliant N/A Deputy Head of Governance
9 Duty to maintain plans Collaborative planningPlans have been developed in collaboration with partners and service providers to ensure the whole patient pathway is considered. Y
Partners consulted with as part of the planning process are demonstrable in planning arrangements
Consultation takes place with relevant internal and external stakeholders during risk evaluation and analysis stages. Managed by the CCG LHRP representative
Fully compliant N/A CCG LHRP representative
11 Duty to maintain plans Critical incident
In line with current guidance and legislation, the organisation has effective arrangements in place to respond to a critical incident (as defined within the EPRR Framework).
Y
Arrangements should be: • current• in line with current national guidance• in line with risk assessment • tested regularly• signed off by the appropriate mechanism• shared appropriately with those required to use them• outline any equipment requirements • outline any staff training required
NECS service user reportBusiness Continuity PlanSLA with NECS
Fully compliant N/A Chief Operating Officer
12 Duty to maintain plans Major incident
In line with current guidance and legislation, the organisation has effective arrangements in place to respond to a major incident (as defined within the EPRR Framework).
Y
Arrangements should be: • current• in line with current national guidance• in line with risk assessment • tested regularly• signed off by the appropriate mechanism• shared appropriately with those required to use them• outline any equipment requirements • outline any staff training required
NECS service user reportBusiness Continuity PlanSLA with NECS
Fully compliant N/A Chief Operating Officer
13 Duty to maintain plans Heatwave
In line with current guidance and legislation, the organisation has effective arrangements in place to respond to the impacts of heatwave on the population the organisation serves and its staff.
Y
Arrangements should be: • current• in line with current national guidance• in line with risk assessment • tested regularly• signed off by the appropriate mechanism• shared appropriately with those required to use them• outline any equipment requirements • outline any staff training required
Business Continuity PlanNHS England guidancePublic Health England guidanceSLA with NECS
Fully compliant N/A Chief Operating Officer
14 Duty to maintain plans Cold weather
In line with current guidance and legislation, the organisation has effective arrangements in place to respond to the impacts of snow and cold weather (not internal business continuity) on the population the organisation serves.
Y
Arrangements should be: • current• in line with current national guidance• in line with risk assessment • tested regularly• signed off by the appropriate mechanism• shared appropriately with those required to use them• outline any equipment requirements • outline any staff training required
Business Continuity PlanNHS England guidancePublic Health England guidanceSLA with NECS
Fully compliant N/A Chief Operating Officer
15 Duty to maintain plans Pandemic influenza
In line with current guidance and legislation, the organisation has effective arrangements in place to respond to pandemic influenza.
Y
Arrangements should be: • current• in line with current national guidance• in line with risk assessment • tested regularly• signed off by the appropriate mechanism• shared appropriately with those required to use them• outline any equipment requirements • outline any staff training required
Business Continuity PlanNHS England guidancePublic Health England guidanceSLA with NECS
Fully compliant N/A Chief Operating Officer
16 Duty to maintain plans Infectious disease
In line with current guidance and legislation, the organisation has effective arrangements in place to respond to an infectious disease outbreak within the organisation or the community it serves, covering a range of diseases including High Consequence Infectious Diseases such as Viral Haemorrhagic Fever. These arrangements should be made in conjunction with Infection Control teams; including supply of adequate FFP3 and PPE trained individuals commensurate with the organisational risk.
Y
Arrangements should be: • current• in line with current national guidance• in line with risk assessment • tested regularly• signed off by the appropriate mechanism• shared appropriately with those required to use them• outline any equipment requirements • outline any staff training required
Business Continuity PlanNHS England guidancePublic Health England guidanceSLA with NECS
Fully compliant N/A Chief Operating Officer

18 Duty to maintain plans Mass Casualty
In line with current guidance and legislation, the organisation has effective arrangements in place to respond to mass casualties. For an acute receiving hospital this should incorporate arrangements to free up 10% of their bed base in 6 hours and 20% in 12 hours, along with the requirement to double Level 3 ITU capacity for 96 hours (for those with level 3 ITU bed).
Y
Arrangements should be: • current• in line with current national guidance• in line with risk assessment • tested regularly• signed off by the appropriate mechanism• shared appropriately with those required to use them• outline any equipment requirements • outline any staff training required
Business Continuity PlanAs a commissioner, the CCG will be directed by guidance from NHSE
Fully compliant N/A Chief Operating Officer
20 Duty to maintain plans Shelter and evacuation
In line with current guidance and legislation, the organisation has effective arrangements in place to shelter and/or evacuate patients, staff and visitors. This should include arrangements to shelter and/or evacuate, whole buildings or sites, working in conjunction with other site users where necessary. Y
Arrangements should be: • current• in line with current national guidance• in line with risk assessment • tested regularly• signed off by the appropriate mechanism• shared appropriately with those required to use them• outline any equipment requirements • outline any staff training required
Business Continuity PlanAs a commissioner, the CCG will be directed by guidance from NHSE
Fully compliant N/A Chief Operating Officer
24 Command and control On-call mechanism
A resilient and dedicated EPRR on-call mechanism is in place 24 / 7 to receive notifications relating to business continuity incidents, critical incidents and major incidents.
This should provide the facility to respond to or escalate notifications to an executive level.
Y
• Process explicitly described within the EPRR policy statement• On call Standards and expectations are set out• Include 24 hour arrangements for alerting managers and other key staff. Details included in BC plan. Rota in place across 12 regional CCGs Fully compliant N/A Chief Operating Officer
25 Command and control Trained on-call staff
On-call staff are trained and competent to perform their role, and are in a position of delegated authority on behalf of the Chief Executive Officer / Clinical Commissioning Group Accountable Officer.
The identified individual: • Should be trained according to the NHS England EPRR competencies (National Occupational Standards)• Can determine whether a critical, major or business continuity incident has occurred• Has a specific process to adopt during the decision making • Is aware who should be consulted and informed during decision making • Should ensure appropriate records are maintained throughout.
Y
• Process explicitly described within the EPRR policy statement
Details included in BC plan. Training provided by NHS England Fully compliant Deputy Head of Governance
26 Training and exercising EPRR Training
The organisation carries out training in line with a training needs analysis to ensure staff are competent in their role; training records are kept to demonstrate this.
Y
• Process explicitly described within the EPRR policy statement• Evidence of a training needs analysis• Training records for all staff on call and those performing a role within the ICC • Training materials• Evidence of personal training and exercising portfolios for key staff
Details included in BC plan. Training provided by NHS England Fully compliant Deputy Head of Governance
27 Training and exercising EPRR exercising and testing programme
The organisation has an exercising and testing programme to safely test major incident, critical incident and business continuity response arrangements.
Organisations should meet the following exercising and testing requirements: • a six-monthly communications test• annual table top exercise • live exercise at least once every three years• command post exercise every three years.
The exercising programme must:• identify exercises relevant to local risks• meet the needs of the organisation type and stakeholders• ensure warning and informing arrangements are effective.
Lessons identified must be captured, recorded and acted upon as part of continuous improvement.
Y
• Exercising Schedule• Evidence of post exercise reports and embedding learning
Exercises and training provided by NHS England Fully compliant CCG LHRP representative
28 Training and exercising Strategic and tactical responder training
Strategic and tactical responders must maintain a continuous personal development portfolio demonstrating training in accordance with the National Occupational Standards, and / or incident / exercise participation
Y
• Training records• Evidence of personal training and exercising portfolios for key staff
Details included in BCM plan. Training is provided by NHS England Fully compliant Deputy Head of Governance
30 Response Incident Co-ordination Centre (ICC)
The organisation has a preidentified Incident Co-ordination Centre (ICC) and alternative fall-back location(s).
Both locations should be annually tested and exercised to ensure they are fit for purpose, and supported with documentation for its activation and operation.
Y
• Documented processes for establishing an ICC• Maps and diagrams• A testing schedule• A training schedule• Pre identified roles and responsibilities, with action cards• Demonstration ICC location is resilient to loss of utilities, including telecommunications, and external hazards
Details in Business Continuity Plan Fully compliant Deputy Head of Governance
31 Response Access to planning arrangements
Version controlled, hard copies of all response arrangements are available to relevant staff at all times. Staff should be aware of where they are stored and should be easily accessible.
YPlanning arrangements are easily accessible - both electronically and hard copies Details in Business Continuity Plan Fully compliant Deputy Head of Governance
32 Response Management of business continuity incidents
In line with current guidance and legislation, the organisation has effective arrangements in place to respond to a business continuity incident (as defined within the EPRR Framework).
Y• Business Continuity Response plans
Details in Business Continuity Plan Fully compliant Deputy Head of Governance
33 Response Loggist
The organisation has 24 hour access to a trained loggist(s) to ensure decisions are recorded during business continuity incidents, critical incidents and major incidents. Key response staff are aware of the need for keeping their own personal records and logs to the required standards.
Y
• Documented processes for accessing and utilising loggists• Training records
Details in Business Continuity Plan Fully compliant Deputy Head of Governance
34 Response Situation Reports
The organisation has processes in place for receiving, completing, authorising and submitting situation reports (SitReps) and briefings during the response to business continuity incidents, critical incidents and major incidents.
Y
• Documented processes for completing, signing off and submitting SitReps• Evidence of testing and exercising Details in Business Continuity Plan Fully compliant Chief Operating Officer
37 Warning and informingCommunication with partners and stakeholders
The organisation has arrangements to communicate with partners and stakeholder organisations during and after a major incident, critical incident or business continuity incident.
Y
• Have emergency communications response arrangements in place • Social Media Policy specifying advice to staff on appropriate use of personal social media accounts whilst the organisation is in incident response• Using lessons identified from previous major incidents to inform the development of future incident response communications• Having a systematic process for tracking information flows and logging information requests and being able to deal with multiple requests for information as part of normal business processes• Being able to demonstrate that publication of plans and assessments is part of a joined-up communications strategy and part of your organisation's warning and informing work
Details in Business Continuity PlanSocial media policy NECS BCPNHSE
Fully compliant Deputy Head of Governance
38 Warning and informing Warning and informing
The organisation has processes for warning and informing the public (patients, visitors and wider population) and staff during major incidents, critical incidents or business continuity incidents.
Y
• Have emergency communications response arrangements in place • Be able to demonstrate consideration of target audience when publishing materials (including staff, public and other agencies)• Communicating with the public to encourage and empower the community to help themselves in an emergency in a way which compliments the response of responders• Using lessons identified from previous major incidents to inform the development of future incident response communications• Setting up protocols with the media for warning and informing
Details in Business Continuity PlanDetails in Business Continuity PlanSocial media policy NECS BCPNHSE
Fully compliant Deputy Head of Governance
39 Warning and informing Media strategy
The organisation has a media strategy to enable rapid and structured communication with the public (patients, visitors and wider population) and staff. This includes identification of and access to a trained media spokespeople able to represent the organisation to the media at all times. Y
• Have emergency communications response arrangements in place • Using lessons identified from previous major incidents to inform the development of future incident response communications• Setting up protocols with the media for warning and informing• Having an agreed media strategy which identifies and trains key staff in dealing with the media including nominating spokespeople and 'talking heads'
Details in Business Continuity PlanNECS BCP
Fully compliant Deputy Head of Governance
40 Cooperation LRHP attendance The Accountable Emergency Officer, or an appropriate director, attends (no less than 75% annually) Local Health Resilience Partnership (LHRP) meetings.
Y• Minutes of meetings CCG LHRP Representative attends meetings
Fully compliant CCG LHRP Representative
41 Cooperation LRF / BRF attendance
The organisation participates in, contributes to or is adequately represented at Local Resilience Forum (LRF) or Borough Resilience Forum (BRF), demonstrating engagement and co-operation with partner responders.
Y
• Minutes of meetings• Governance agreement if the organisation is represented
CCG LHRP Representative attends meetings
Fully compliant CCG LHRP Representative

42 Cooperation Mutual aid arrangements
The organisation has agreed mutual aid arrangements in place outlining the process for requesting, coordinating and maintaining mutual aid resources. These arrangements may include staff, equipment, services and supplies.
These arrangements may be formal and should include the process for requesting Military Aid to Civil Authorities (MACA) via NHS England.
Y
• Detailed documentation on the process for requesting, receiving and managing mutual aid requests• Signed mutual aid agreements where appropriate
Details included in Business Continuity Plan
Fully compliant Chief Operating Officer
46 Cooperation Information sharing
The organisation has an agreed protocol(s) for sharing appropriate information with stakeholders, during major incidents, critical incidents or business continuity incidents. Y
• Documented and signed information sharing protocol• Evidence relevant guidance has been considered, e.g. Freedom of Information Act 2000, General Data Protection Regulation and the Civil Contingencies Act 2004 ‘duty to communicate with the public’.
Details included in Business Continuity Plan and Communications StrategyNECS BCPNHSE guidanceNE Mutli Agency Sharing Agreement
Fully compliant Deputy Head of Governance
47 Business Continuity BC policy statement
The organisation has in place a policy which includes a statement of intent to undertake business continuity. This includes the comitmement to a Business Continutiy Management System (BCMS) in alignment to the ISO standard 22301.
Y
Demonstrable a statement of intent outlining that they will undertake BC - Policy Statement
Details included in Business Continuity Plan
Fully compliant Deputy Head of Governance
48 Business Continuity BCMS scope and objectives
The organisation has established the scope and objectives of the BCMS in relation to the organisation, specifying the risk management process and how this will be documented.
Y
BCMS should detail: • Scope e.g. key products and services within the scope and exclusions from the scope• Objectives of the system• The requirement to undertake BC e.g. Statutory, Regulatory and contractual duties• Specific roles within the BCMS including responsibilities, competencies and authorities.• The risk management processes for the organisation i.e. how risk will be assessed and documented (e.g. Risk Register), the acceptable level of risk and risk review and monitoring process• Resource requirements• Communications strategy with all staff to ensure they are aware of their roles• Stakeholders
Details included in Business Continuity Plan
Fully compliant Deputy Head of Governance
49 Business Continuity Business Impact Assessment
The organisation annually assesses and documents the impact of disruption to its services through Business Impact Analysis(s).
Y
Documented process on how BIA will be conducted, including:• the method to be used• the frequency of review• how the information will be used to inform planning • how RA is used to support.
Details included in Business Continuity Plan
Fully compliant Deputy Head of Governance
50 Business Continuity Data Protection and Security Toolkit
Organisation's Information Technology department certify that they are compliant with the Data Protection and Security Toolkit on an annual basis.
YStatement of compliance DSP toolkit submission March 2020 - service commissioned from
NECS. Fully compliant North of England CSU
51 Business Continuity Business Continuity Plans
The organisation has established business continuity plans for the management of incidents. Detailing how it will respond, recover and manage its services during disruptions to:• people• information and data• premises• suppliers and contractors• IT and infrastructure
These plans will be reviewed regularly (at a minimum annually), or following organisational change, or incidents and exercises.
Y
• Documented evidence that as a minimum the BCP checklist is covered by the various plans of the organisation
Details included in Business Continuity Plan
Fully compliant Deputy Head of Governance
52 Business Continuity BCMS monitoring and evaluation
The organisation's BCMS is monitored, measured and evaluated against established Key Performance Indicators. Reports on these and the outcome of any exercises, and status of any corrective action are annually reported to the board.
Y
• EPRR policy document or stand alone Business continuity policy• Board papers
Details included in Business Continuity Plan
Fully compliant Chief Operating Officer
53 Business Continuity BC auditThe organisation has a process for internal audit, and outcomes are included in the report to the board. Y
• EPRR policy document or stand alone Business continuity policy• Board papers• Audit reports
Internal audit conduct an annual audit on EPRRFully compliant Deputy Head of Governance
54 Business Continuity BCMS continuous improvement process
There is a process in place to assess the effectivness of the BCMS and take corrective action to ensure continual improvement to the BCMS.
Y• EPRR policy document or stand alone Business continuity policy• Board papers• Action plans
Details included in Business Continuity PlanFully compliant Chief Operating Officer
55 Business ContinuityAssurance of commissioned providers / suppliers BCPs
The organisation has in place a system to assess the business continuity plans of commissioned providers or suppliers; and are assured that these providers business continuity arrangements work with their own.
Y
• EPRR policy document or stand alone Business continuity policy• Provider/supplier assurance framework• Provider/supplier business continuity arrangements
Details included in SLAsCCG is assured by NHSE process for NHS providers
Fully compliant Chief Operating Officer

Ref Domain Standard DetailClinical
Commissioning Group
Evidence - examples listed below Organisational Evidence
Self assessment RAG
Red (not compliant) = Not compliant with the core standard. The organisation’s EPRR work
programme shows compliance will not be reached within the next 12 months.
Amber (partially compliant) = Not compliant with core standard. However, the
organisation’s EPRR work programme demonstrates sufficient evidence of progress and an action plan to achieve full compliance
within the next 12 months.
Green (fully compliant) = Fully compliant with core standard.
Action to be taken Lead Timescale Comments
Deep Dive - Severe WeatherDomain: Severe Weather Response
1 Severe Weather response Overheating
The organisation's heatwave plan allows for the identification and monitoring of inpatient and staff areas that overheat (For community and MH inpatient area may include patients own home, or nursing/care home facility) Y
The monitoring processes is explicitly identified in the organisational heatwave plan. This includes staff areas as well as inpatient areas. This process clearly identifies relevant temperature triggers and subsequent actions.
CCG uses Department of Health and Social Care annual 'Heatwave plan for England'
Partially compliant
Confirm Heatwave plan is sighted at GB or relevant committee.Is the heatwave plan cascaded to GP member practices?The plan is not uploaded to the CCG's website but there is some guidance for public on websiteDid the CCG circulate guidance from NECS H&S team to staff?
Debra Elliott
2 Severe Weather response Overheating
The organisation has contingency arrangements in place to reduce temperatures (for example MOUs or SLAs for cooling units) and provide welfare support to inpatients and staff in high risk areas (For community and MH inpatient area may include patients own home, or nursing/care home facility)
Y
Arrangements are in place to ensure that areas that have been identified as overheating can be cooled to within reasonable temperature ranges, this may include use of cooling units or other methods identified in national heatwave plan.
Office areas have access to fansWindow blinds can be closed to lower temperatures
Fully compliant Debra Elliott
3 Severe Weather response Staffing
The organisation has plans to ensure staff can attend work during a period of severe weather (snow, flooding or heatwave), and has suitable arrangements should transport fail and staff need to remain on sites. (Includes provision of 4x4 where needed)
Y
The organisations arrangements outline:- What staff should do if they cannot attend work- Arrangements to maintain services, including how staff may be brought to site during disruption- Arrangements for placing staff into accommodation should they be unable to return home
Businss impact analysis identifies key staff for high priority servicsKey staff able to work remotelyCCG staff work normal office hours and in adverse weather the situation would be monitored closely with staff sent home early if the situation looked to be worsening.
Partially compliant
To confirm through BIAsNeed to confirm that key staff can work remotely (BIAs) Debra Elliott
4 Severe Weather response Service provision
Organisations providing services in the community have arrangements to allow for caseloads to be clinically prioritised and alterative support delivered during periods of severe weather disruption. (This includes midwifery in the community, mental health services, district nursing etc)
The organisations arrangements identify how staff will prioritise patients during periods of severe weather, and alternative delivery methods to ensure continued patient care
5 Severe Weather response Discharge
The organisation has polices or processes in place to ensure that any vulnerable patients (including community, mental health, and maternity services) are discharged to a warm home or are referred to a local single point-of-contact health and housing referral system if appropriate, in line with the NICE Guidelines on Excess Winter Deaths
Y
The organisations arrangements include how to deal with discharges or transfers of care into non health settings. Organisation can demonstrate information sharing regarding vulnerability to cold or heat with other supporting agencies at discharge
CCG monitors pressures throughout the year through performance management, contract management and quality management. Additionally intelligence from reported discharge incidents would also alert staff of any trends. CCG safeguarding team and CHC staff also able to escalate issues they become aware of
Partially compliant Debra Elliott
6 Severe Weather response Access
The organisation has arrangements in place to ensure site access is maintained during periods of snow or cold weather, including gritting and clearance plans activated by predefined triggers
Y
The organisation arrangements have a clear trigger for the pre-emptive placement of grit on key roadways and pavements within the organisations boundaries. When snow / ice occurs there are clear triggers and actions to clear priority roadways and pavements. Arrangements may include the use of a third party gritting or snow clearance service.
CCG is co-located with local authority who are responsible for facilities management and have arrangements in place
Fully compliant
7 Severe Weather response Assessment
The organisation has arrangements to assess the impact of National Severe Weather Warnings (including Met Office Cold and Heatwave Alerts, Daily Air Quality Index and Flood Forecasting Centre alerts) and takes predefined action to mitigate the impact of these where necessary
Y
The organisations arrangements are clear in how it will assesses all weather warnings. These arrangements should identify the role(s) responsible for undertaking these assessments and the predefined triggers and action as a result.
PMO Manager has been identified to lead on this area of work
Partially compliant
HR 19 Other Leave Policy includes a section on adverse weather. CCG will also produce a supporting design process to describe how to monitor the weather and when to escalate for a decision & to trigger a communication cascade
Richard Hay
8 Severe Weather response Flood prevention
The organisation has planned preventative maintenance programmes are in place to ensure that on site drainage is clear to reduce flooding risk from surface water, this programme takes into account seasonal variations.
Y
The organisation has clearly demonstratable Planned Preventative Maintenance programmes for its assets. Where third party owns the drainage system there is a clear mechanism to alert the responsible owner to ensure drainage is cleared and managed in a timely manner
CCG is co-located with local authority who are responsible for facilities management and have arrangements in place.
IT assets are provided by North of England CSU who have a disaster recovery plan that covers physical IT assets.
Fully compliant Debra Elliott
9 Severe Weather response Flood response
The organisation is aware of, and where applicable contributed to, the Local Resilience Forum Multi Agency Flood Plan. The organisation understands its role in this plan. Y
The organisation has reference to its role and responsibilities in the Multi Agency Flood Plan in its arrangements. Key on-call/response staff are clear how to obtain a copy of the Multi Agency Flood Plan
Northumberland County Council produces multi agency Flood Plan which is available on their website: https://www.northumberland.gov.uk Partially compliant
Probably worth ensuring this is uploaded to intranetCheck whether CCG has any defined role in the Flood Plan
Debra Elliott

10 Severe Weather response Warning and informin
The organisation's communications arrangements include working with the LRF and multiagency partners to warn and inform, before and during, periods of Severe Weather, including the use of any national messaging for Heat and Cold.
Y
The organisation has within is arrangements documented roles for its communications teams in the event of Severe Weather alerts and or response. This includes the ability for the organisation to issue appropriate messaging 24/7. Communications plans are clear in what the organisations will issue in terms of severe weather and when.
Communication & engagement service provided by North of England CSU. The CCG has social media accouunts which can be operated 24/7 if necessary
Partially compliantCommunication strategy currently makes no specific mention of severe weather
Debra Elliott
11 Severe Weather response Flood response
The organisation has plans in place for any preidentified areas of their site(s) at risk of flooding. These plans include response to flooding and evacuation as required.
Y
The organisation has evidence that it regularly risk assesses its sites against flood risk (pluvial, fluvial and coastal flooding). It has clear site specific arrangements for flood response, for known key high risk areas. On-site flood plans are in place for at risk areas of the organisations site(s).
CCG is co-located with local authority who are responsible for facilities management and have arrangements in place.
Fully compliant To confirm Debra Elliott
12 Severe Weather response Risk assess
The organisation has identified which severe weather events are likely to impact on its patients, services and staff, and takes account of these in emergency plans and business continuity arrangements.
Y
The organisation has documented the severe weather risks on its risk register, and has appropriate plans to address these.
CCG has documented a risk relating to system reslience(Ref 1178)Risk relating to operational resilience (Ref 1435)Both risks have well documented controls and assurances.The CCG's risk management process would ensure that any emerging risks are captured and monitored through the risk management process.
Fully compliant To confirm Debra Elliott
13 Severe Weather response Supply chain
The organisation is assured that its suppliers can maintain services during periods of severe weather, and periods of disruption caused by these.
Y
The organisation has a documented process of seeking risk based assurance from suppliers that services can be maintained during extreme weather events. Where these services can't be maintain the organisation has alternative documented mitigating arrangements in place.
Preparations for EU Exit ensured that supplier resilience was reviewed. NHS England carried out this assurance check for large national suppliers and CCG carried out local checks. This information will be utilised in a severe weather event.
Fully compliant
To confirmMight be worth considering having something like this in a battle box or an appendix to BCP.
Debra Elliott
14 Severe Weather response Exercising
The organisation has exercised its arrangements (against a reasonable worst case scenario), or used them in an actual severe weather incident response, and they were effective in managing the risks they were exposed to. From these event lessons were identified and have been incorporated into revised arrangements.
Y
The organisation can demonstrate that its arrangements have been tested in the past 12 months and learning has resulted in changes to its response arrangements.
BCP test undertaken in August 2019
Fully compliant Debra Elliott
15 Severe Weather response ICT BC
The organisations ICT Services have been thoroughly exercised and equipment tested which allows for remote access and remote services are able to provide resilience in extreme weather e.g. are cooling systems sized appropriately to cope with heatwave conditions, is the data centre positioned away from areas of flood risk.
Y
The organisations arrangements includes the robust testing of access services and remote services to ensure the total number of concurrent users meets the number that may work remotely to maintain identified critical services
CCG commissions North of England CSU to deliver ICT services. NECS undertakes regular BCP tests and also tested disaster recovery plan in 2018 which will be repeated in 2019.
Fully compliant To confirm Debra Elliott
Domain: long term adaptation planning
16 Long term adaptation planning Risk assess
Are all relevant organisations risks highlighted in the Climate Change Risk Assessment are incorporated into the organisations risk register.
YEvidence that the there is an entry in the organiations risk register detailing climate change risk and any mitigating actions
Not currentlyNon compliant To develop a risk for inclusion on risk
register. Debra Elliott
17 Long term adaptation planning Overheating risk
The organisation has identified and recorded those parts of their buildings that regularly overheat (exceed 27 degrees Celsius) on their risk register. The register identifies the long term mitigation required to address this taking into account the sustainable development commitments in the long term plan. Such as avoiding mechanical cooling and use of cooling higherachy.
Y
The organisation has records that identifies areas exceeding 27 degrees and risk register entries for these areas with action to reduce risk
CCG is co-located with local authority who are responsible for facilities management and have arrangements in place.
Fully compliant Debra Elliott
18 Long term adaptation planning Building adaptations
The organisation has in place an adaptation plan which includes necessary modifications to buildings and infrastructure to maintain normal business during extreme temperatures or other extreme weather events.
Y
The organisation has an adaptation plan that includes suggested building modifications or infrastructure changes in future
CCG is co-located with local authority who are responsible for facilities management and have arrangements in place.
Fully compliant Debra Elliott
19 Long term adaptation planning Flooding
The organisations adaptation plans include modifications to reduce their buildings and estates impact on the surrounding environment for example Sustainable Urban Drainage Systems to reduce flood risks.
Y
Areas are identified in the organisations adaptation plans that might benefit drainage surfaces, or evidence that new hard standing areas considered for SUDS
CCG is co-located with local authority who are responsible for facilities management and have arrangements in place.
Fully compliant Debra Elliott
20 Long term adaptation planning New build
The organisation considers for all its new facilities relevant adaptation requirements for long term climate change Y
The organisation has relevant documentation that it is including adaptation plans for all new builds
NHS Property Services will be responsible for ensuring any new CCG facilities have incorporated long-term adaptation planning
Fully compliant
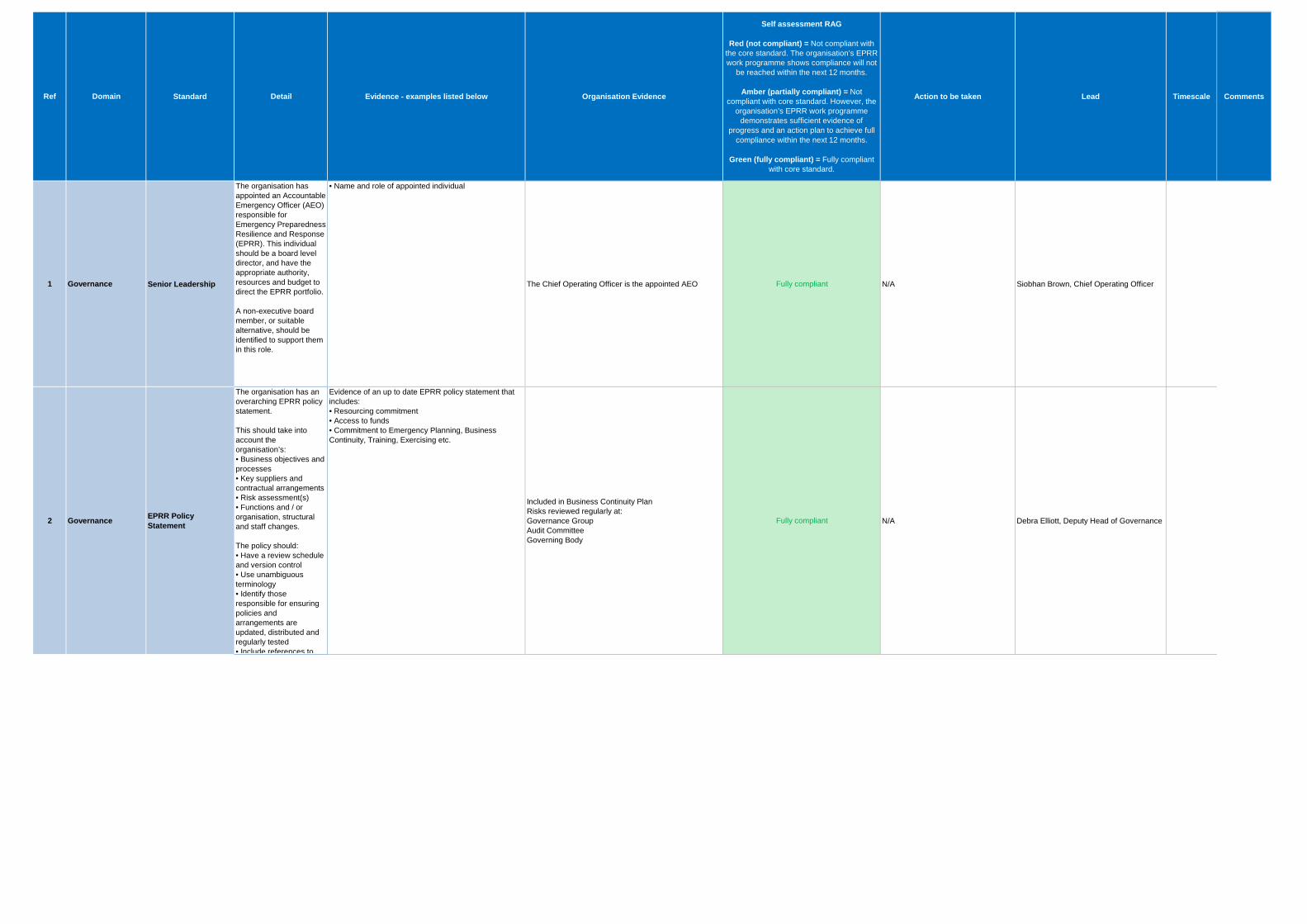
Ref Domain Standard Detail Evidence - examples listed below Organisation Evidence
Self assessment RAG
Red (not compliant) = Not compliant with the core standard. The organisation’s EPRR work programme shows compliance will not
be reached within the next 12 months.
Amber (partially compliant) = Not compliant with core standard. However, the
organisation’s EPRR work programme demonstrates sufficient evidence of
progress and an action plan to achieve full compliance within the next 12 months.
Green (fully compliant) = Fully compliant with core standard.
Action to be taken Lead Timescale Comments
1 Governance Senior Leadership
The organisation has appointed an Accountable Emergency Officer (AEO) responsible for Emergency Preparedness Resilience and Response (EPRR). This individual should be a board level director, and have the appropriate authority, resources and budget to direct the EPRR portfolio.
A non-executive board member, or suitable alternative, should be identified to support them in this role.
• Name and role of appointed individual
The Chief Operating Officer is the appointed AEO Fully compliant N/A Siobhan Brown, Chief Operating Officer
2 Governance EPRR Policy Statement
The organisation has an overarching EPRR policy statement.
This should take into account the organisation’s:• Business objectives and processes• Key suppliers and contractual arrangements• Risk assessment(s)• Functions and / or organisation, structural and staff changes.
The policy should: • Have a review schedule and version control• Use unambiguous terminology• Identify those responsible for ensuring policies and arrangements are updated, distributed and regularly tested• Include references to
Evidence of an up to date EPRR policy statement that includes:• Resourcing commitment• Access to funds• Commitment to Emergency Planning, Business Continuity, Training, Exercising etc.
Included in Business Continuity PlanRisks reviewed regularly at:Governance GroupAudit CommitteeGoverning Body
Fully compliant N/A Debra Elliott, Deputy Head of Governance

3 Governance EPRR board reports
The Chief Executive Officer / Clinical Commissioning Group Accountable Officer ensures that the Accountable Emergency Officer discharges their responsibilities to provide EPRR reports to the Board / Governing Body, no less frequently than annually.
These reports should be taken to a public board, and as a minimum, include an overview on:• training and exercises undertaken by the organisation• summary of any business continuity, critical incidents and major incidents experienced by the organisation• lessons identified from incidents and exercises
• Public Board meeting minutes• Evidence of presenting the results of the annual EPRR assurance process to the Public Board
Annual Bord Reports Fully compliant N/A Chilef Operating Officer

4 Governance EPRR work programme
The organisation has an annual EPRR work programme, informed by:• lessons identified from incidents and exercises • identified risks • outcomes of any assurance and audit processes.
• Process explicitly described within the EPRR policy statement• Annual work plan
Included in Business Continuity Plan Fully compliant N/A Deputy Head of Governance
5 Governance EPRR Resource
The Board / Governing Body is satisfied that the organisation has sufficient and appropriate resource, proportionate to its size, to ensure it can fully discharge its EPRR duties.
• EPRR Policy identifies resources required to fulfill EPRR function; policy has been signed off by the organisation's Board• Assessment of role / resources• Role description of EPRR Staff• Organisation structure chart • Internal Governance process chart including EPRR group
Annual Bord Reports Fully compliant N/A Chilef Operating Officer
6 Governance Continuous improvement process
The organisation has clearly defined processes for capturing learning from incidents and exercises to inform the development of future EPRR arrangements.
• Process explicitly described within the EPRR policy stat
There is a CCG LHRP representative. BCP is developed in conjunction with local authority, Newcastle Gateshead CCG and North Tyneside CCG
Fully compliant N/A Chilef Operating Officer
7 Duty to risk assess Risk assessment
The organisation has a process in place to regularly assess the risks to the population it serves. This process should consider community and national risk registers.
• Evidence that EPRR risks are regularly considered and recorded• Evidence that EPRR risks are represented and recorded on the organisations corporate risk register
BCP/EPRR implemented in the CCG. Risks are recorded on the risk register and discussed at Governing Body and Audit Committee on a quarterly basis.Business impact analysis carried out on all CCG activities
Fully compliant N/A Deputy Head of Governance
8 Duty to risk assess Risk Management
The organisation has a robust method of reporting, recording, monitoring and escalating EPRR risks.
• EPRR risks are considered in the organisation's risk management policy • Reference to EPRR risk management in the organisation's EPRR policy document
Risk management policy is updated regularly and describes the escalation process for all risks which includes any EPRR risks.
Fully compliant N/A Deputy Head of Governance

Emergency Preparedness, Resilience and Response (EPRR) Assurance 2019-20
STATEMENT OF COMPLIANCE
NHS Northumberland Clinical Commissioning Group has undertaken a self-assessment against the NHS England Core Standards (v2.3). Following the self-assessment, and in line with the definitions of compliance stated below, the organisation declares itself as demonstrating the following level of compliance against the 2019-20 standards as: Fully compliant
Overall EPRR assurance rating
Criteria
Fully The organisation is 100% compliant with all core standards they are required to achieve.
Substantial The organisation is 89-99% compliant with the core standards they are required to achieve.
Partial The organisation is 77-88% compliant with the core standards they are required to achieve.
Non-compliant The organisation compliant with 76% or less of the core standards they are required to achieve.
Where areas require further action, this is detailed in the organisations EPRR Work Plan and will be reviewed in line with the organisation’s governance arrangements. I confirm that the above level of compliance with the EPRR Core Standards has been or will be confirmed to the organisation’s board / governing body.
Signed by the organisation’s Accountable Emergency Officer
25/09/2019 10/09/2019
Date of board / governing body meeting Date signed

Agenda Item 10.4
OFFICIAL
1 20190925 UC Agenda Item 10.4 Workforce Race & Equalities Standard Submission
Clinicians commissioning healthcare for the people of Northumberland
Meeting title Governing Body
Date 25 September 2019
Agenda item Workforce Race Equality Standard (WRES) Submission
Report title Workforce Race Equality Standard (WRES) submission
Report author NECS Senior Governance Officer (E&D)
Sponsor Deputy Head of Governance
Private or Public agenda
Public
NHS classification Official
Purpose (tick one only)
Information only
Development/Discussion
Decision/Action ()
Links to Corporate Objectives Ensure that the CCG makes best use of all available resources
()
Ensure the delivery of safe, high quality services that deliver the best outcomes
Create joined up pathways within and across organisations to deliver seamless care
Deliver clinically led health services that are focused on individual and wider population needs and based on evidence.
Northumberland CCG/external meetings this paper has been discussed at:
N/A
QIPP N/A
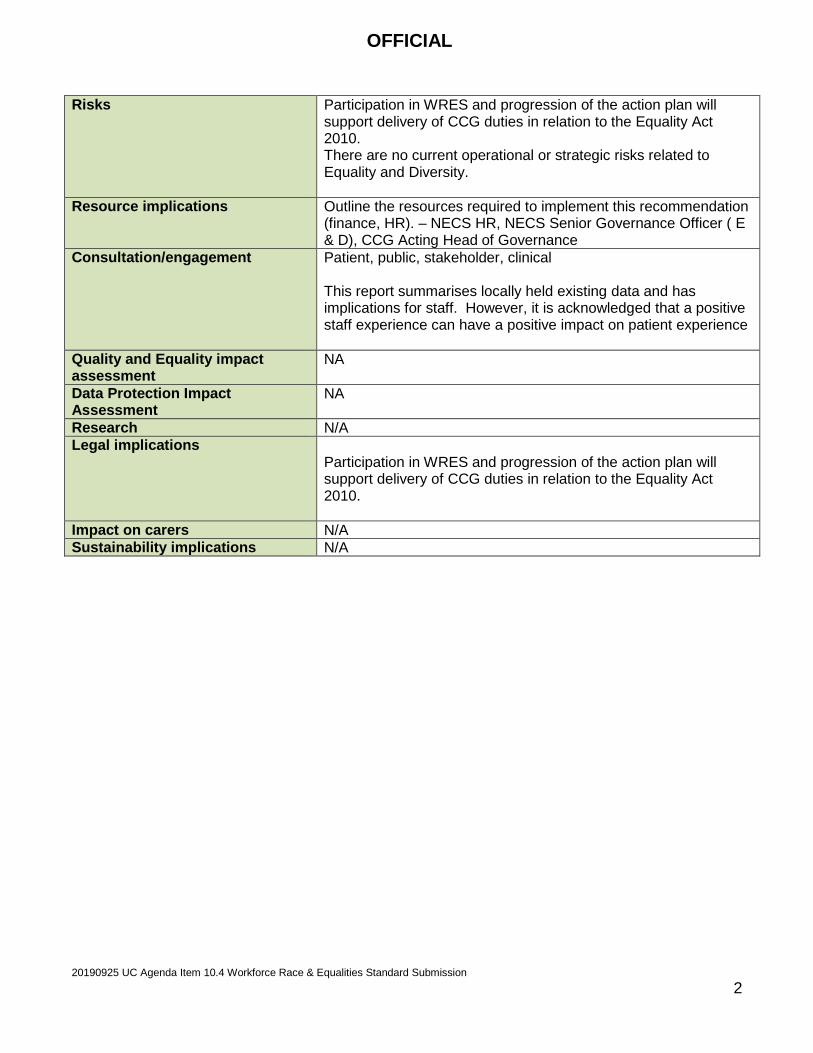
OFFICIAL
20190925 UC Agenda Item 10.4 Workforce Race & Equalities Standard Submission 2
Risks Participation in WRES and progression of the action plan will support delivery of CCG duties in relation to the Equality Act 2010. There are no current operational or strategic risks related to Equality and Diversity.
Resource implications Outline the resources required to implement this recommendation (finance, HR). – NECS HR, NECS Senior Governance Officer ( E & D), CCG Acting Head of Governance
Consultation/engagement Patient, public, stakeholder, clinical This report summarises locally held existing data and has implications for staff. However, it is acknowledged that a positive staff experience can have a positive impact on patient experience
Quality and Equality impact assessment
NA
Data Protection Impact Assessment
NA
Research N/A Legal implications
Participation in WRES and progression of the action plan will support delivery of CCG duties in relation to the Equality Act 2010.
Impact on carers N/A Sustainability implications N/A

OFFICIAL
20190925 UC Agenda Item 10.4 Workforce Race & Equalities Standard Submission 3
QUALITY and EQUALITY IMPACT ASSESSMENT 1. Project Name Workforce Race Equality Standard (WRES) submission
2. Project Lead Director Lead Project Lead Clinical Lead Chief Operating Officer
Deputy Head of Governance
N/A
3. Project Overview & Objective
The NHS Workforce Race Equality Standard (WRES) was made available to the NHS from April 2015 and this year Clinical Commissioning Groups have been asked to participate in the data return. The main purpose of the WRES is as outlined by NHS England is to • help local, and national, NHS organisations (and other organisations
providing NHS services) to review their data against the nine WRES indicators
• produce action plans to close the gaps in workplace experience between white and Black and Ethnic Minority (BME) staff, and,
• improve BME representation at the Board level of the organisation The nine indicators cover recruitment and pay; access to training; disciplinary; discrimination, bullying and harassment and Governing Body membership. By 31 August 2019 the data must be submitted to NHS England and by Friday 27 September 2019, all organisations must publish their WRES data on their corporate website.
4. Quality Impact Assessment
Impact Details Pos/ Neg
C L Scores
Mitigation / Control
Patient Safety Clinical Effectiveness Patient Experience Others including reputation, information governance and etc.
5.Equality Impact Assessment
Impact Details Pos/ Neg
C L Scores
Mitigation / Control
What is the impact on people who have one of the protected characteristics as defined in the Equality Act 2010?
The report itself analyses data with regards to equality and can support future equality impact analyses.
Positive
What is the impact on health inequalities in terms of access to services and
NA

OFFICIAL
20190925 UC Agenda Item 10.4 Workforce Race & Equalities Standard Submission 4
outcomes achieved for the population of Northumberland? 6. Research Reference to relevant local and national research as appropriate.
NA
7. Metrics Sensitive to the impacts or risks on quality and equality and can be used for ongoing monitoring.
Impact Descriptors Baseline Metrics Target
8. Completed By Signature Printed Name
Date
Governance Officer E&D
Lisa Wooton
Lisa Wooton
07.09.19
Additional Relevant Information:
8. Clinical Lead Approval by Signature Printed Name
Date
Additional Relevant Information:
9. Reviewed By Signature Printed Name
Date
Debra Elliott
Debra Elliott 07.09.19
Comments
OFFICIAL
20190925 UC Agenda Item 10.4 Workforce Race & Equalities Standard Submission 5
Governing Body 25 September 2019 Agenda Item: 10.4 Workforce Race Equality Standard (WRES) submission Sponsor: Deputy Head of Governance
Members of the Governing Body are asked to: 1. Review the workforce profiles for Northumberland CCG in relation to the nine
indicators of the Workforce Race Equality Standard (WRES) which was submitted to NHS England on the 27 August 2019, (Appendix 1).
2. Agree the CCG WRES Action Plan 2019/20 (Appendix 2) to enable the upload to the CCG’s website by the deadline of 27 September 2019 along with the WRES submission data.
Purpose This report presents the workforce profiles for NHS Northumberland Clinical Commissioning Group (CCG) Governing Body’s (GB) in relation to the nine indicators of NHS Workforce Race Equality Standards (WRES). Background The CCG assesses itself against the WRES annually to ensure that:
• data is collected and review against the nine WRES indicators • an action plan is produced to close any gaps in workplace experience between white
and Black and Ethnic Minority (BME) staff, and • Board membership includes BME representation.
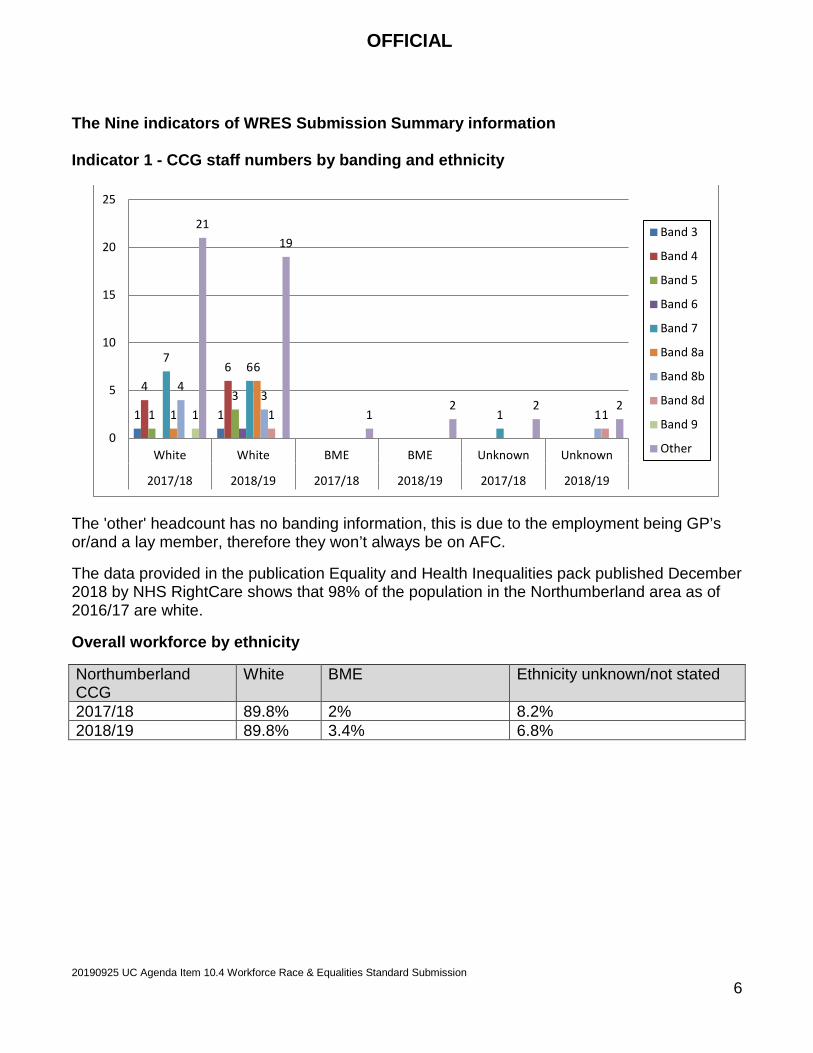
OFFICIAL
20190925 UC Agenda Item 10.4 Workforce Race & Equalities Standard Submission 6
The Nine indicators of WRES Submission Summary information Indicator 1 - CCG staff numbers by banding and ethnicity
The 'other' headcount has no banding information, this is due to the employment being GP’s or/and a lay member, therefore they won’t always be on AFC.
The data provided in the publication Equality and Health Inequalities pack published December 2018 by NHS RightCare shows that 98% of the population in the Northumberland area as of 2016/17 are white.
Overall workforce by ethnicity
Northumberland CCG
White BME Ethnicity unknown/not stated
2017/18 89.8% 2% 8.2% 2018/19 89.8% 3.4% 6.8%
1 1
4 6
1 3
7 6
1 1
6 4
3 1 1 1 1
21 19
1 2 2 2
0
5
10
15
20
25
White White BME BME Unknown Unknown
2017/18 2018/19 2017/18 2018/19 2017/18 2018/19
Band 3
Band 4
Band 5
Band 6
Band 7
Band 8a
Band 8b
Band 8d
Band 9
Other

OFFICIAL
20190925 UC Agenda Item 10.4 Workforce Race & Equalities Standard Submission 7
Indicator 2 - Relative likelihood of staff being appointed from shortlisting across all posts
The above chart shows that for 2018/19 the relative likelihood of appointment from shortlisting for white staff is 25% based on the data provided. Only three BME applicants were shortlisted but none were appointed to post.
It is also noted that for 2017/18 the appointed to post figures are not available due to GDPR regulations and NHS jobs remove data that is more than 18 months old, also not all appointments to post are noted as complete on NHS jobs.
An action has been created to pull data from NHS jobs on an annual basis to ensure that data is not lost.
Indicator 3 - Relative Likelihood of staff entering the formal disciplinary process
In the period 2017/18 and 2018/19 there have been no staff who have entered the formal disciplinary process.
Indicator 4 - Relative Likelihood of staff accessing non-mandatory training and CPD
There is no data available for this submission, an action has been created in the plan to start gathering this data. The WRES submission team were consulted and were happy for an action to be put in place going forward.
Indicators 5 to 8 were taken from the annual NHS staff survey
The NECS HR team confirmed that there is no data available for questions five to eight as the NHS staff survey was not undertaken.
An action has been created recommend the completion of the NHS staff survey going forward.
Shortlistedapplicants 2017/18
number appointedfrom Shortlisting
2017/18
Shortlistedapplicants 2018/19
number appointedfrom Shortlisting
2018/19White 48 0 51 13BME 4 0 3 0Unknown 1 0 0 0
48
0
51
13
4 0 3 0 1 0 0 0
0
10
20
30
40
50
60

OFFICIAL
20190925 UC Agenda Item 10.4 Workforce Race & Equalities Standard Submission 8
2017 2018 Indicator 5 Percentage of staff experiencing harassment, bullying or abuse from patients, relatives or the public in last 12 months.
Indicator 6 Percentage of staff experiencing harassment, bullying or abuse from staff in last 12 months.
Indicator 7 Percentage believing that trust provides equal opportunities for career progression or promotion.
Indicator 8 In the last 12 months have you personally experienced discrimination at work from any of the following? Manager/team leader or other colleagues.
Indicator 9 - Percentage difference between the organisations’ Board Membership by ethnicity disaggregated: 1) by voting membership of the Board 2) by executive membership of the Board.
2017/18 White BME Ethnicity Unknown/not
stated
Total Board Members
% by ethnicity
7
87.5%
1
12.5%
0
of which are:
White BME
Ethnicity Unknown/not stated
Voting Member 7 1 0
Exec Board members 7 1 0

OFFICIAL
20190925 UC Agenda Item 10.4 Workforce Race & Equalities Standard Submission 9
2018/19 White BME Ethnicity Unknown/not
stated
Total Board Members
% by Ethnicity
12
92.3%
1
7.7%
0
of which are:
White BAME Ethnicity Unknown/not
stated
Voting Member 12 1 0
Exec Board members 8 0 0
The results show that there are no board members who do not have their ethnicity stated which is positive for the WRES submission as organisations are encouraged to report the ethnicity of their board members.
Conclusion The CCG annual self - assessment against the NHS Workforce Race Equality Standard (WRES) to ensure that:
• data is collected and review against the nine WRES indicators
• an action plan is produced to close any gaps in workplace experience between white and Black and Ethnic Minority (BME) staff, and
• Board membership includes BME representation.
Recommendation GB is asked to:
• Review the workforce profiles for Northumberland CCG in relation to the nine indicators of the Workforce Race Equality Standard (WRES) which was submitted to NHS England on the 27 August 2019, (Appendix 1).
• Agree the CCG WRES Action Plan 2019/20 (Appendix 2) to enable the upload to the CCG’s website by the deadline of 27 September 2019 along with the WRES submission data.

OFFICIAL
20190925 UC Agenda Item 10.4 Workforce Race & Equalities Standard Submission 10
Appendix 1 - Workforce Race Equality Standard (WRES) submission Appendix 2 - CCG WRES Action Plan 2019/20

Workforce Race Equality Standards annual collection as at March-2019
For any technical queries or additional clarification relating to the collection please contact:
For any queries or additional clarification relating to submissions please contact: [email protected]

Workforce Race Equality Standards
Validations
Please correct all issues listed within the table below. If the issues are not corrected then the pro forma will fail the validation stage in SDCS.
Trust - Frontsheet

SubmissionTemplateWorkforce Race Equality Standards 2018/19 template
Answer RequiredAuto PopulatedN/A
1a) Non Clinical workforce ESR figures Verified figures ESR figures Verified figures ESR figures Verified figures ESR figures Verified figures ESR figures Verified figures ESR figures Verified figures
1 Under Band 1 Headcount 0 0 0 0 0 0 0 0 0 0 0 02 Band 1 Headcount 0 0 0 0 0 0 0 0 0 0 0 03 Band 2 Headcount 1 1 0 0 0 0 0 0 0 0 0 04 Band 3 Headcount 1 1 0 0 0 0 1 1 0 0 0 05 Band 4 Headcount 4 4 0 0 0 0 6 6 0 0 0 06 Band 5 Headcount 1 1 0 0 0 0 3 3 0 0 0 07 Band 6 Headcount 0 0 0 0 0 0 1 1 0 0 0 08 Band 7 Headcount 7 7 0 0 1 1 6 6 0 0 0 09 Band 8A Headcount 1 1 0 0 0 0 6 6 0 0 0 010 Band 8B Headcount 4 4 0 0 0 0 3 3 0 0 1 111 Band 8C Headcount 3 3 0 0 1 1 7 7 0 0 0 012 Band 8D Headcount 0 0 0 0 0 0 1 1 0 0 1 113 Band 9 Headcount 1 1 0 0 0 0 0 0 0 0 0 014 VSM Headcount 0 0 0 0 0 0 0 0 0 0 0 0
15 Under Band 1 Headcount 0 0 0 0 0 0 0 0 0 0 0 016 Band 1 Headcount 0 0 0 0 0 0 0 0 0 0 0 017 Band 2 Headcount 0 0 0 0 0 0 0 0 0 0 0 018 Band 3 Headcount 0 0 0 0 0 0 0 0 0 0 0 019 Band 4 Headcount 0 0 0 0 0 0 0 0 0 0 0 020 Band 5 Headcount 0 0 0 0 0 0 0 0 0 0 0 021 Band 6 Headcount 0 0 0 0 0 0 0 0 0 0 0 022 Band 7 Headcount 0 0 0 0 0 0 0 0 0 0 0 023 Band 8A Headcount 0 0 0 0 0 0 0 0 0 0 0 024 Band 8B Headcount 0 0 0 0 0 0 0 0 0 0 0 025 Band 8C Headcount 0 0 0 0 0 0 0 0 0 0 0 026 Band 8D Headcount 0 0 0 0 0 0 0 0 0 0 0 027 Band 9 Headcount 0 0 0 0 0 0 0 0 0 0 0 028 VSM Headcount 0 0 0 0 0 0 0 0 0 0 0 0
29 Consultants Headcount 0 0 0 0 0 0 0 0 0 0 0 0
30 of which Senior medical manager
Headcount 0 0 0 0 0 0
31 Non-consultant career grade Headcount 0 0 0 0 0 0 0 0 0 0 0 032 Trainee grades Headcount 0 0 0 0 0 0 0 0 0 0 0 0
33 Other Headcount 21 21 1 1 2 2 19 19 2 2 2 2
The 'other' headcount has no banding information, this is due to the employment being GP’s or/and a lay member, therefore they won’t always be on AFC.
34 Number of shortlisted applicants Headcount 48 4 1 51 3 0
35Number appointed from shortlisting
Headcount 0 0 0 13 0 0
Appointments to post are unknown for 2018 as due to GDPR NHS jobs remove data that is more than 18 months old and not all appointments to post are noted on NHS jobs
36Relative likelihood of appointment from shortlisting
Auto calculated 0.0000000000 0.0000000000 0.0000000000 0.2549019608 0.0000000000
37Relative likelihood of White staff being appointed from shortlisting compared to BME staff
Auto calculated
38 Number of staff in workforce Auto calculated 44 1 4 53 2 4
39Number of staff entering the formal disciplinary process
Headcount 0 0 0 0 0 0
40Likelihood of staff entering the formal disciplinary process
Auto calculated 0.0000000000 0.0000000000 0.0000000000 0.0000000000 0.0000000000 0.0000000000
41Relative likelihood of BME staff entering the formal disciplinary process compared to White staff
Auto calculated
INDICATOR MEASURE Notes
2
1
3
ETHNICITY UNKNOWN/NULLBMEBMEWHITE ETHNICITY UNKNOWN/NULLDATA ITEM
Of which Medical & Dental
31st MARCH 2018
WHITE
Relative likelihood of staff entering the formal disciplinary process, as measured by entry into a formal disciplinary investigation
Note: This indicator
Relative likelihood of staff being appointed from shortlisting across all posts
Percentage of staff in each of the AfC Bands 1-9 OR Medical and Dental subgroups and VSM (including executive Board members) compared with the percentage of staff in the overall workforce
1b) Clinical workforceof which Non Medical
31st MARCH 2019

SubmissionTemplateWorkforce Race Equality Standards 2018/19 template
Answer RequiredAuto PopulatedN/A
INDICATOR MEASURE NotesETHNICITY UNKNOWN/NULLBMEBMEWHITE ETHNICITY UNKNOWN/NULLDATA ITEM
31st MARCH 2018
WHITE
31st MARCH 2019
42 Number of staff in workforce Auto calculated 44 1 4 53 2 4
43Number of staff accessing non-mandatory training and CPD:
Headcount 0 0 0 0 0 0
Data was not available for this submission, an action plan has been created to ensure the data is collated going forward.
44Likelihood of staff accessing non-mandatory training and CPD
Auto calculated 0.0000000000 0.0000000000 0.0000000000 0.0000000000 0.0000000000 0.0000000000
45Relative likelihood of White staff accessing non-mandatory training and CPD compared to BME staff
Auto calculated
5
Percentage of staff experiencing harassment, bullying or abuse from patients,
46
% of staff experiencing harassment, bullying or abuse from patients, relatives or the public in last 12 months
Percentage 0.00% 0.00% 0.00% 0.00%There was no staff survey was undertaken in 2017 or 2018
6
Percentage of staff experiencing harassment, bullying or abuse from staff in
47% of staff experiencing harassment, bullying or abuse from staff in last 12 months
Percentage 0.00% 0.00% 0.00% 0.00%There was no staff survey was undertaken in 2017 or 2018
7
Percentage believing that trust provides equal opportunities for career progression or
48
% staff believing that trust provides equal opportunities for career progression or promotion
Percentage 0.00% 0.00% 0.00% 0.00%There was no staff survey was undertaken in 2017 or 2018
8
In the last 12 months have you personally experienced discrimination at work from any of the
49
% staff personally experienced discrimination at work from Manager/team leader or other colleague
Percentage 0.00% 0.00% 0.00% 0.00%There was no staff survey was undertaken in 2017 or 2018
50 Total Board members Headcount 7 1 0 12 1 0
51 of which: Voting Board members Headcount 7 1 0 12 1 0
52 : Non Voting Board members
Auto calculated 0 0 0 0 0 0
53 Total Board members Auto calculated 7 1 0 12 1 0
54 of which: Exec Board members Headcount 7 1 0 8 0 0
55 : Non Executive Board members
Auto calculated 0 0 0 4 1 0
56Number of staff in overall workforce
Auto calculated 44 1 4 53 2 4
57Total Board members - % by Ethnicity
Auto calculated 87.5% 12.5% 0.0% 92.3% 7.7% 0.0%
58Voting Board Member - % by Ethnicity
Auto calculated 87.5% 12.5% 0.0% 92.3% 7.7% 0.0%
59Non Voting Board Member - % by Ethnicity
Auto calculated
60Executive Board Member - % by Ethnicity
Auto calculated 87.5% 12.5% 0.0% 100.0% 0.0% 0.0%
61Non Executive Board Member - % by Ethnicity
Auto calculated 80.0% 20.0% 0.0%
62 Overall workforce - % by Ethnicity Auto calculated 89.8% 2.0% 8.2% 89.8% 3.4% 6.8%
63Difference (Total Board -Overall workforce )
Auto calculated -2.3% 10.5% -8.2% 2.5% 4.3% -6.8%
9
4
Percentage difference between the organisations’ Board voting membership and its overall workforce
Note: Only voting members of the Board should be included when considering this indicator
Relative likelihood of staff accessing non-mandatory training and CPD
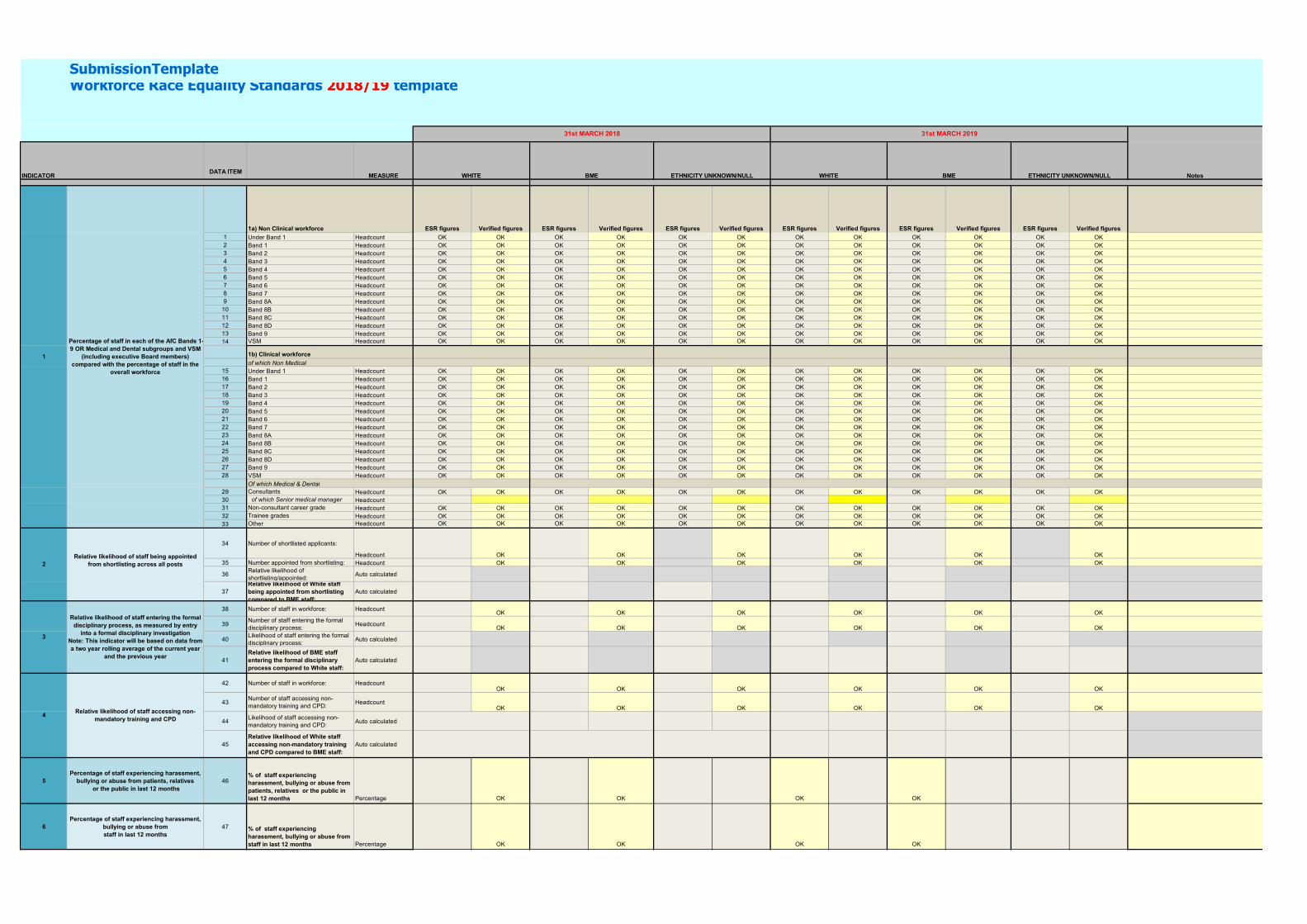
SubmissionTemplateWorkforce Race Equality Standards 2018/19 template
DATA ITEM
1a) Non Clinical workforce ESR figures Verified figures ESR figures Verified figures ESR figures Verified figures ESR figures Verified figures ESR figures Verified figures ESR figures Verified figures 1 Under Band 1 Headcount OK OK OK OK OK OK OK OK OK OK OK OK2 Band 1 Headcount OK OK OK OK OK OK OK OK OK OK OK OK3 Band 2 Headcount OK OK OK OK OK OK OK OK OK OK OK OK4 Band 3 Headcount OK OK OK OK OK OK OK OK OK OK OK OK5 Band 4 Headcount OK OK OK OK OK OK OK OK OK OK OK OK6 Band 5 Headcount OK OK OK OK OK OK OK OK OK OK OK OK7 Band 6 Headcount OK OK OK OK OK OK OK OK OK OK OK OK8 Band 7 Headcount OK OK OK OK OK OK OK OK OK OK OK OK9 Band 8A Headcount OK OK OK OK OK OK OK OK OK OK OK OK
10 Band 8B Headcount OK OK OK OK OK OK OK OK OK OK OK OK11 Band 8C Headcount OK OK OK OK OK OK OK OK OK OK OK OK12 Band 8D Headcount OK OK OK OK OK OK OK OK OK OK OK OK13 Band 9 Headcount OK OK OK OK OK OK OK OK OK OK OK OK14 VSM Headcount OK OK OK OK OK OK OK OK OK OK OK OK
1b) Clinical workforce
of which Non Medical15 Under Band 1 Headcount OK OK OK OK OK OK OK OK OK OK OK OK16 Band 1 Headcount OK OK OK OK OK OK OK OK OK OK OK OK17 Band 2 Headcount OK OK OK OK OK OK OK OK OK OK OK OK18 Band 3 Headcount OK OK OK OK OK OK OK OK OK OK OK OK19 Band 4 Headcount OK OK OK OK OK OK OK OK OK OK OK OK20 Band 5 Headcount OK OK OK OK OK OK OK OK OK OK OK OK21 Band 6 Headcount OK OK OK OK OK OK OK OK OK OK OK OK22 Band 7 Headcount OK OK OK OK OK OK OK OK OK OK OK OK23 Band 8A Headcount OK OK OK OK OK OK OK OK OK OK OK OK24 Band 8B Headcount OK OK OK OK OK OK OK OK OK OK OK OK25 Band 8C Headcount OK OK OK OK OK OK OK OK OK OK OK OK26 Band 8D Headcount OK OK OK OK OK OK OK OK OK OK OK OK27 Band 9 Headcount OK OK OK OK OK OK OK OK OK OK OK OK28 VSM Headcount OK OK OK OK OK OK OK OK OK OK OK OK
Of which Medical & Dental29 Consultants Headcount OK OK OK OK OK OK OK OK OK OK OK OK30 of which Senior medical manager Headcount31 Non-consultant career grade Headcount OK OK OK OK OK OK OK OK OK OK OK OK32 Trainee grades Headcount OK OK OK OK OK OK OK OK OK OK OK OK33 Other Headcount OK OK OK OK OK OK OK OK OK OK OK OK
34 Number of shortlisted applicants:
Headcount OK OK OK OK OK OK35 Number appointed from shortlisting: Headcount OK OK OK OK OK OK
36Relative likelihood of shortlisting/appointed:
Auto calculated
37Relative likelihood of White staff being appointed from shortlisting compared to BME staff:
Auto calculated
38 Number of staff in workforce: HeadcountOK OK OK OK OK OK
39Number of staff entering the formal disciplinary process:
HeadcountOK OK OK OK OK OK
40Likelihood of staff entering the formal disciplinary process:
Auto calculated
41Relative likelihood of BME staff entering the formal disciplinary process compared to White staff:
Auto calculated
42 Number of staff in workforce: HeadcountOK OK OK OK OK OK
43Number of staff accessing non-mandatory training and CPD:
HeadcountOK OK OK OK OK OK
44Likelihood of staff accessing non-mandatory training and CPD:
Auto calculated
45Relative likelihood of White staff accessing non-mandatory training and CPD compared to BME staff:
Auto calculated
5Percentage of staff experiencing harassment,
bullying or abuse from patients, relatives or the public in last 12 months
46% of staff experiencing harassment, bullying or abuse from patients, relatives or the public in last 12 months Percentage OK OK OK OK
6Percentage of staff experiencing harassment,
bullying or abuse from staff in last 12 months
47 % of staff experiencing harassment, bullying or abuse from staff in last 12 months Percentage OK OK OK OK
BME
2Relative likelihood of staff being appointed
from shortlisting across all posts
3
Relative likelihood of staff entering the formal disciplinary process, as measured by entry
into a formal disciplinary investigationNote: This indicator will be based on data from a two year rolling average of the current year
and the previous year
4Relative likelihood of staff accessing non-
mandatory training and CPD
WHITE
1
Percentage of staff in each of the AfC Bands 1-9 OR Medical and Dental subgroups and VSM
(including executive Board members) compared with the percentage of staff in the
overall workforce
INDICATOR MEASURE WHITE
31st MARCH 2018 31st MARCH 2019
ETHNICITY UNKNOWN/NULL NotesBME ETHNICITY UNKNOWN/NULL

SubmissionTemplateWorkforce Race Equality Standards 2018/19 template
DATA ITEMBMEWHITEINDICATOR MEASURE WHITE
31st MARCH 2018 31st MARCH 2019
ETHNICITY UNKNOWN/NULL NotesBME ETHNICITY UNKNOWN/NULL
7Percentage believing that trust provides equal
opportunities for career progression or promotion
48 % staff believing that trust provides equal opportunities for career progression or promotion Percentage OK OK OK OK
8
In the last 12 months have you personally experienced discrimination at work from any
of the following? b) Manager/team leader or other colleagues
49 % staff personally experienced discrimination at work from Manager/team leader or other colleague Percentage OK OK OK OK
Percentage difference between the organisations’ Board voting membership and
its overall workforceNote: Only voting members of the Board
50Total Board members Headcount OK OK OK OK OK OK
51 of which: Voting Board members Headcount OK OK OK OK OK OK
52 : Non Voting Board members Autocalculated
53Total Board members Headcount OK OK OK OK OK OK
54 of which: Exec Board members Headcount OK OK OK OK OK OK
55 : Non Executive Board members Autocalculated
56Number of staff in overall workforce Headcount OK OK OK OK OK OK
57Total Board members - % by Ethnicity Auto calculated
58Voting Board Member - % by Ethnicity Auto calculated
59Non Voting Board Member - % by Ethnicity Auto calculated
60Executive Board Member - % by Ethnicity Auto calculated
61Non Executive Board Member - % by Ethnicity Auto calculated
62Overall workforce - % by Ethnicity Auto calculated
63Difference (Total Board -Overall workforce ) Auto calculated
9

Workforce Race Equality Standards (WRES) Action Plan 2019/20
Ref Indicator (s) Summary Action Owner Deadline Action Updates Status
WRES1 Indicator 1 Percentage of staff in each of the AFC bands 1-9 or Medical and Dental Subgroups and VSM (including executive board members) broken down by ethnicity. Indicator 9 Percentage difference between the organisations’ Board Membership by ethnicity disaggregated:
By voting membership of the Board
By executive membership of the Board
Data Reporting Procedures
Develop a data reporting engagement exercise following review to increase staff knowledge and awareness of providing ethnicity detail and improve on the workforce data we currently hold. Encourage all staff to update and populate their personal data for diversity purposes when asked applications, surveys etc.
CCG - OD Lead Manager for CCG
April 2020

WRES2 Indicator 2 Relative likelihood of staff being appointed from shortlisting across all posts (internal and external recruitment activity) broken down by ethnicity
Recruitment Process
Run report from NHS jobs on an annual basis (31st March) to ensure that shortlisting and appointments to post data is not lost due to GDPR rules where data is removed from NHS jobs after 18 months.
CCG HR Business Partner – NECS
End of March 2020
WRES3 Indicator 4
Non- mandatory training data monitoring
Develop a process to provide non mandatory training & CPD information so that the CCG can monitor equal opportunities in the organisation and also for future WRES returns.
CCG - OD Lead Manager for CCG
December 2019
WRES4 Indicator 5 Percentage of staff experiencing harassment, bullying or abuse from patients, relatives or the public in last 12 months. Indicator 6 Percentage of staff experiencing harassment, bullying or abuse from staff in last 12 months.
Staff Survey Undertake the NHS staff survey or develop and implement internal staff survey as equivalent to obtain data and staff feedback for Equality monitoring and future WRES returns.
CCG - OD Lead Manager for CCG CCG HR Business Partner – NECS
October 2019

Indicator 7 Percentage believing that trust provides equal opportunities for career progression or promotion. Indicator 8 In the last 12 months have you personally experienced discrimination at work from any of the following? B) Manager/team leader or other colleagues.

Agenda Item 12 OFFICIAL
1 20190925 UC Agenda Item 12 Public GB Public Forward Plan 2019/20
Governing Body - Forward Plan 2019/20 Standing items Lead
• Accountable Officer and Chief Operating Officer’s Report • Finance Report • Clinical Management Board (including Quality & Performance exceptions) • Health & Wellbeing Board minutes • Governing Body Forward Plan
Mark Adams/Siobhan Brown Jon Connolly Graham Syers
October 2019
• Quarterly Commissioning Plan Progress Update • Communications & Engagement Strategy 2019/20
Siobhan Brown
November 2019
• Assurance Framework & Risk Register (Quarterly) • Mental Health S117 Forecasting • Communications & Engagement Report (Quarterly)
Debra Elliott Jon Connolly/Kate O’Brien
December 2019 (Meeting held in public)
• Public Health Update (Quarterly) Liz Morgan
January 2020
• Quarterly Commissioning Plan Progress Update Siobhan Brown

2 20190925 UC Agenda Item 12 Public GB Public Forward Plan 2019/20
• Communications & Engagement Report (Quarterly)
February 2020
• Assurance Framework & Risk Register (Quarterly)
March 2020 (Meeting held in public)
• Public Health Update (Quarterly)
Liz Morgan