northern england strategic clinical network conference 15 th may 2015 stillbirth care bundles
TRANSCRIPT

Northern England Strategic Clinical Network Conference
15th May 2015Stillbirth Care Bundles

Saving Babies’ LivesReducing Stillbirth and early NND• SB rate in UK one of the highest in Europe
• In UK, about 33% difference between different regions
• Affects 1 in 200 – 300 babies
• About 4000 SBs every year in the UK
• SB reduction mandate from government to NHS England

Smoking cessation
CO Testing at booking and opt
out referral pathway
Identification and surveillance of
fetal growth restriction
GAP / GrowProgramme
Perinatal Institute
Reduced fetal movement
pathwayand Leaflet
Fetal monitoringStaff training and
competency assessment Fresh Eyes
Peer ReviewIn cases of stillbirth, hypoxia and early neonatal death
BME groups Vulnerable women Chronic conditions ↑BMI
WOMEN AND STAFF EXPERIENCECommunication difficulties for staff over language relating to death – “loss/sleeping baby”
Saving Babies Lives and early NNDCare Bundle Interventions

Saving babies’ lives – Care bundle (element 1)Smoking in pregnancy• Smoking in the UK is known to cause up to:
– 2,200 premature births
– 5000 miscarriages + 300 perinatal deaths
– 360 fetal losses in the NE alone
• Care bundle interventions
– Reduce smoking in pregnancy by carrying out carbon monoxide testing of all pregnant women at booking, and referring to SSS as appropriate, based on an opt out system

Saving babies’ lives – Care bundle (element 2)Identify + monitor SGA / FGR
• Strong evidence to suggest fetal growth restriction (FGR) is a major risk factor for SB
– BWs of SBs are SGA when assessed by a standard based on normal pregnancy
– Babies with FGR are usually (but not always) SGA
• Antenatal identification of SGA / FGR reduces risk significantly
• Most cases are late onset – hence, surveillance required throughout pregnancy
SB weight distribution

Saving babies’ lives – Care bundle (element 2)Fetal growth restriction
• Interventions
– Use of customised antenatal growth charts for all pregnant women by clinicians who have gained competence in their use (GROW charts)
– Use of supplied algorithm to aid decision making on classification of risk, and corresponding screening and surveillance of all pregnancies according to their risk
– Audit of SGA rates and antenatal detection rates
– Case-note audit of selected cases not detected antenatally

Yearly stillbirth rates in the 3 regions with high uptake of GROW training and protocols (‘high uptake’) vs the rest (‘low uptake’), 2008–2012 (see table 1).
Jason Gardosi et al. BMJ Open 2013;3:e003942©2013 by British Medical Journal Publishing Group

One or more risk factors
High Risk CareSerial assessment (3 weekly) of fetal weight and umbilical Doppler from 26-28 weeks until delivery; EFWs plotted on customised chart
Low Risk□ No known risk factors
Increased Risk: one or more of the following:
Maternal Risk Factors□ Maternal age >40 years□ Smoker (any)□ Drug misusePrevious Pregnancy History□ Previous SGA baby (<10th cust. centile) □ Previous stillbirthMaternal Medical History□ Chronic hypertension□ Diabetes □ Renal impairment□ Antiphospholipid syndromeUnsuitable for monitoring by fundal height- e.g.□ Large fibroids□ BMI >35
Current Pregnancy ComplicationsEarly Pregnancy□ PAPP-A <0.415 MoM□ Fetal echogenic bowelLate Pregnancy□ Severe pregnancy induced hypertension or pre-eclampsia (=PIH and proteinuria)□ Unexplained antepartum haemorrhage
Direct referral for assessment (<72 hours) for estimated fetal weight (EFW), liquor volume and umbilical artery Doppler
Low Risk CareSerial assessment (2-3 weekly) of fundal height from 26-28 weeks until delivery FH measurements plotted on customised chart
Abnormal growth: - cust EFW <10th centile and/or- Serial measurements not following curve and/or - abnormal umbilical artery pulsatility index
Suspected abnormal growth: FH <10th centile or not following curve (‘crossing centile lines’)
No risk factors
Refer to RCOG guidance on management of the SGA fetus
Normal


Saving babies’ lives – Care bundle (element 3)Reduced fetal movements Aspiration
o Raising awareness amongst pregnant women of the importance of detecting and reporting reduced fetal movement (RFM), and ensuring providers have protocols in place, based on best available evidence, to manage RFM
Interventions
o Information and advice leaflet on reduced fetal movement (RFM), based on current evidence, best practice and clinical guidelines, to be provided to all pregnant women by, at the latest, the 24th week of pregnancy and RFM discussed at every subsequent contact
o Use provided checklist to manage care of pregnant women who report reduced fetal movement, in line with RCOG Green-top Guideline 57

Attendance with reduced Fetal Movements Please initial when
Ask Is there maternal perception of reduced fetal movements? □
Assess Are there risk factors for Fetal Growth Restriction or Stillbirth? □
Consider - multiple consultations for RFM, known FGR, maternal hypertension, diabetes, extremes of maternal age, primiparity, smoking, obesity, racial/ethnic factors, past obstetric history of FGR or stillbirth) and issues with access to care
Act Auscultate fetal heart (hand-held Doppler / Pinnard)Perform CTG to assess fetal heart rate in accordance with national guidelinesIf risk factors for FGR/Stillbirth, perform ultrasound scan for fetal growth, liquor volume and umbilical artery Doppler within 24 hours.
□□□
Advise Convey results of investigations to the mother.Mother should re-attend if further reductions in fetal movements at anytime
□□
Act Act upon abnormal results promptly □
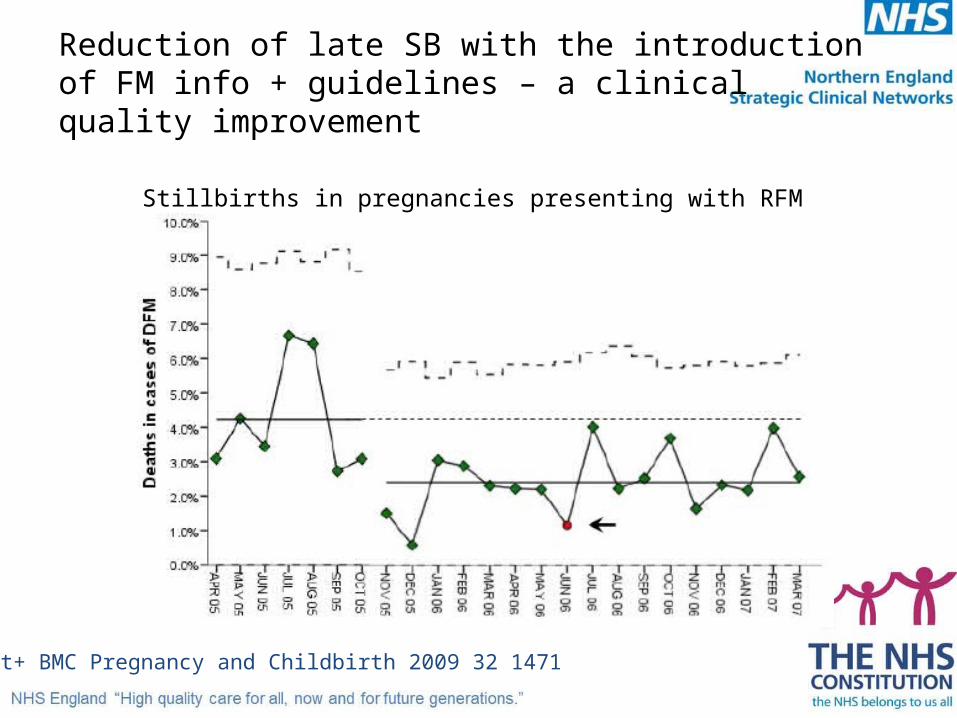
Reduction of late SB with the introduction of FM info + guidelines – a clinical quality improvement
Tveit+ BMC Pregnancy and Childbirth 2009 32 1471
Stillbirths in pregnancies presenting with RFM

Saving babies’ lives – Care bundle (element 4)Effective fetal monitoring in labour Aim
Effective fetal monitoring during labour Interventions
All staff who care for women in labour are required to undertake an annual training and competency assessment on CTG interpretation.
No member of staff should care for women in a birth setting without evidence of training and competence within the last year
Buddy system in place for review of CTG interpretation and auscultation, with a
Protocol for escalation if concerns are raised. All staff to be trained in the review system and escalation protocol

Saving Babies’s Lives
• Conclusions / discussion points
– Comprehensive and thorough series of care bundles
– Inconsistent evidence base, but plausible
– National priority
– Ongoing resource / education issues
– Innovative solutions – CTG / USS?
– Local opportunities for implementation
Reduction of late SB with the introduction of FM info + guidelines – a clinical quality improvement
• Guideline– Standard clinical evaluation– NST– Ultrasound scan for size, AFV, activity
• Information for women– Primary indicator: maternal perception of major and lasting reduction in the
normal activity of her baby– Never to wait to the next day if no kicks in one day– Contact midwife if baby kicks “less and less” in course of a day / days– Contact midwife if < 10 FM in 2 hours at a time of day when baby usually
active
Tveit+ BMC Pregnancy and Childbirth 2009 32 1471
