objectives - caribbean dialysisprinciplesofdialysis.weebly.com/uploads/5/6/1/3/5613613/2008cc... ·...
TRANSCRIPT


ObjectivesAfter completing this module, the learner will be able to:
1. Define the basic principles of diffusion, filtration, ultrafiltration, convection, and osmosis.
2. Explain how diffusion, filtration, ultrafiltration, convection, and osmosis relate to solutetransport and fluid movement during dialysis.
3. Describe the principles of fluid dynamics and how they relate to dialysis.
Principles of Dialysis
76

IntroductionHemodialysis may seem complex, but it is basedon simple scientific principles. This modulewill help you understand these principles andhow they are used in dialysis. Dialysis replacesthree main kidney functions:
1. Removing wastes from the blood
2. Removing excess fluid from the blood
3. Keeping electrolytes (electrically chargedparticles) in balance
You will learn how these three functions arereplaced by the dialyzer.
Scientific PrinciplesUsed in Dialysis
SOLUTIONSA solution is a mixture of a solvent and a solute. The solvent is a fluid. The solute is any substance that can be dissolved into thesolvent.1 So, in salt water, water is the solventand salt is the solute.
Dialysate is the solution that is used duringdialysis. Water is the solvent. The solutes areelectrolytes (e.g., potassium, calcium, sodium,magnesium, and chloride ions) and glucose(sugar). Electrolyte levels in dialysate closelymatch the levels in human blood. This reducesthe loss of these electrolytes out of the bloodand into the dialysate during dialysis.
The patient’s blood electrolyte levels can becontrolled by changing the dialysate. Adding anelectrolyte to the dialysate at a level higher than
in the blood will allow the electrolyte to enterthe patient’s blood during a treatment.2
SEMIPERMEABLEMEMBRANE
A semipermeable membrane is a type of thin,flexible filter—a barrier that allows only particlessmaller than a certain size to pass through it.Think of the membrane as a strainer you mightuse to drain noodles. The water drains out, butthe noodles are too big to pass through the holes.In dialysis, the semipermeable membrane’sholes allow small molecules, such as water andurea, to pass through easily. Middle moleculescan also pass through, but more slowly. The smallsize of the pores keeps larger molecules andblood cells from passing through the membrane.2
DIFFUSIONDiffusion is the process by which atoms,molecules, and/or other particles move from anarea where they are in high concentration to anarea where they are in low concentration.1 Forexample, when a tea bag is placed in hot water,molecules from the tea leaves diffuse into thewater and flavor it (see Figure 1 on page 78).Diffusion can occur in solids, gases, or liquids,such as blood. Energy for the movement comesfrom the molecules themselves, and does notdepend on outside forces.
In the body, substances move into and out of cells bydiffusion through the cell membranes. In dialysis,diffusion occurs across an artificial semipermeablemembrane. This is how wastes and fluid are removedfrom the patient’s blood, and electrolytes are balanced.
The following factors affect all diffusion—fromtea bags to hemodialysis.2
377

Factors Affecting Diffusion:the Nature of the Solution1. Concentration gradients: How concentrated
is the fluid on each side of the membrane?Solutes move through a semipermeablemembrane from an area of greaterconcentration to an area of lesserconcentration. Solutes can move through amembrane in either direction, but alwaystoward the area of lesser concentration. Agradient is a difference. As the concentrationgradient—the difference in soluteconcentration—increases, solute movementincreases, too. Diffusion stops when theconcentrations on both sides of the membraneare equal. Concentration gradients allowdialysate to remove wastes from a patient’sblood and to balance electrolytes in theblood with electrolytes in the dialysate.
2. Molecular weight of the solutes: How large are the dissolved particles? Smaller moleculesdiffuse more easily and quickly than largerones. Large blood components, such as red blood cells, white blood cells, albumin,and platelets—as well as viruses andbacteria—diffuse more slowly because theyare bigger. Small molecules, such as urea and salts, diffuse faster. Middle moleculesmay pass through, but more slowly.
3. Temperature: How warm is the fluid?Molecules move faster at highertemperatures, so warmer fluids allow fasterdiffusion. This is why you’ll get tea sooner if you put your tea bag in hot water instead of cold water. Dialysate temperature iscontrolled during dialysis for patient safety,comfort, and faster diffusion.
Factors Affecting Diffusion:the Nature of theMembrane1. Membrane permeability: How plentiful and
large are the pores? A membrane with morepores allows faster diffusion. Larger poresallow larger molecules to pass through. The membrane’s thickness and design alsoaffect the diffusion rate (see Figure 2).
2. Surface area of the membrane: How big is the membrane? Surface area is the amount of membrane in direct contact with theblood and dialysate. Larger surface areasallow more diffusion.
3. Flow geometry: How do the fluids flow? Indialysis, blood flows one way while dialysateflows the opposite way (see Figure 3). Thiscountercurrent flow of blood to dialysatespeeds up diffusion, because with this
Principles of Dialysis
78
Figure 1: Diffusion through a
semipermeable membrane
Tea particlesdiffuse into the water
An ordinary tea bag is made of porous paper—asemipermeable membrane. Tiny holes allow the tea particlesto come out into the water, but keep the tea leaves in the bag.

arrangement, a high concentration gradientbetween the blood and dialysate can bemaintained throughout the length of thedialyzer. (A concurrent flow would occur if blood and dialysate moved in the samedirection).
OSMOSISIn diffusion, solutes move. In osmosis, thesolvent moves across the membrane. Osmosisis movement of a solvent through asemipermeable membrane from an area oflower solute concentration toward an area ofhigher solute concentration.3 The difference inconcentration is called an osmotic pressuregradient. In both diffusion and osmosis,movement goes on until the concentration ofmolecules equilibrates (becomes equal) on bothsides of the membrane.2,3
Imagine a jar divided in two by a membrane thatallows water—but not glucose molecules—topass through. If you fill one side of the jar withwater, half of the water will slowly pass throughthe membrane, until the water level on bothsides of the jar is the same. You could thendissolve sugar on one side of the jar, to create adifference in glucose concentration between thetwo sides. Osmotic pressure created by thesugar would draw water across the membraneto dilute the sugar water. In time, the level ofsugar water would rise above the level of purewater. The more sugar you added, the higherthe osmotic pressure would build, and thehigher the sugar water level would rise.
Osmotic pressure can be overcome by hydraulicpressure using a pump, gravity, or other means.The total pressure on a fluid will include both
579
Figure 2: Membrane and fiber characteristics
Figure 3: Blood and dialysate flow:Countercurrent directions
Wall thickness
Internal diameter190 to 240µ
Surface areaNumber andsize of pores
Blood
Drawing adapted with permission from Althin Academy, Miami Lakes, Florida
Blood out
Blood in
Used dialysate and excess fluidfrom the patient’s body out to drain
Each blood-filled fiberis surrounded by
dialysate
Dialysate inDirection of blood flow
Direction of dialysate flow
Single, hollow fiber

osmotic and mechanical forces.2 In our jar, hydraulic(mechanical) pressure was applied by gravity.Water would be pulled into the sugar water untilthe osmotic pressure is equal to the pressurecreated by the weight of the water. The osmoticpressure drops as the sugar water is diluted.
Hydraulic pressure can reduce or overcomeosmotic pressure. If you raised the hydraulicpressure on the sugar water in the jar, you couldovercome the osmotic pressure. This wouldcause water to move from the sugar water backinto the pure water. This principle is the basisfor reverse osmosis water treatment devices.
FILTRATION ANDULTRAFILTRATION
Filtration is movement of fluid through a filteras the result of hydraulic pressure.1 Fluid willalways move from a higher pressure to a lowerpressure. The filter traps any matter that is toolarge to pass through it.
In dialysis, ultrafiltration (UF)—water removalfrom blood due to a pressure gradient across amembrane (see Figure 4)—is used to removeexcess water that has built up. The filter used in UF is a semipermeable membrane.2
Convection is the transfer of heat and solutes by physical circulation or movement of theparts of a liquid or gas. In dialysis, convectivetransport leads to solvent drag.4 As a solventcrosses a semipermeable membrane, it dragsalong smaller solutes.5
FLUID DYNAMICSA fluid is a liquid or gas that changes shape at asteady rate when acted upon by a force.1 Thefield of “dynamics” addresses the motion andequilibrium of systems. Fluid dynamics appliesto dialysis, because it describes how two fluids—blood and dialysate—are pumped through tubing.Within the dialyzer, blood and dialysate are keptapart by the semipermeable membrane.
Principles of Dialysis
80
Figure 4: Diffusion, osmosis,and ultrafiltration
Semipermeablemembrane Pressure
Diffusion is the movement ofsolutes from an area of higherconcentration to an area oflower concentration.
Osmosis is the movement of asolvent across a semipermeablemembrane from a lowerconcentration of solutes to ahigher concentration of solutes.
Ultrafiltration is the removal of extra fluid through themembrane using additionalpressure.
Several forces affect the movement, or flow, offluid through tubing. Flow rate is the amount of fluid that flows through the tubing in a givenperiod of time (e.g., 10 milliliters per minute, ormL/min). Flow velocity is the speed at whichthe fluid moves through a given length oftubing. Velocity is based on the rate of flow andthe area of a cross section of the tube. So, if theflow rate is held constant but the cross sectionof the tube is reduced by half, the flow velocitywill double.
Imagine that one gallon of water must movethrough a tube with a one-square-inch crosssection in one minute. If you reduce the crosssection of the tube by half, to 1/2 square inch,the fluid will have to go twice as fast to move agallon of water in one minute; flow velocitywould need to double. Adding a piece of tubingwith a 1/2-square-inch cross section to the endof a tube with a one-square-inch cross sectionwill have the same effect: doubling flow velocity.Because all the water must pass through thenarrowest part of the tube, the narrowest part ofany tubing limits the maximum flow velocity.
Adding a second, narrower, piece of tubing alsoincreases resistance to the flow—another forcethat affects the movement of fluid in a tube. In any tubing, simple friction creates someresistance to the flow of fluid. But a restriction,such as a narrowing of the tube, will greatlyincrease resistance and so will increase thepressure of the fluid in the tube.
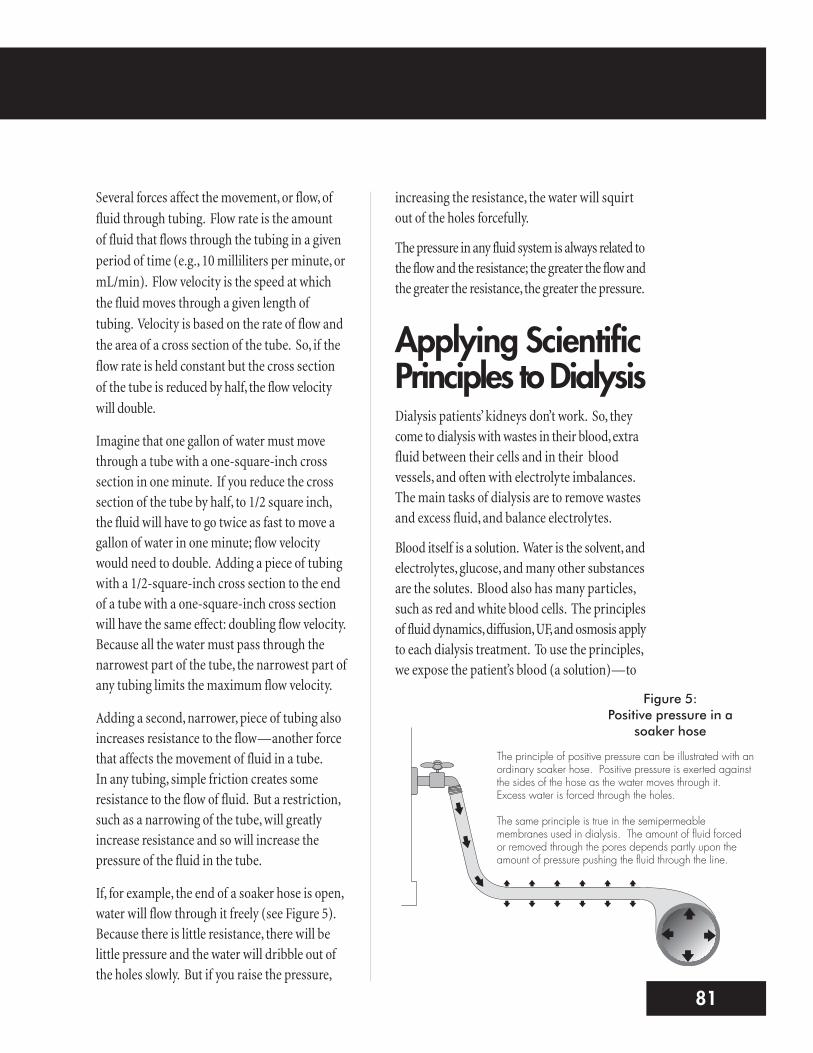
If, for example, the end of a soaker hose is open,water will flow through it freely (see Figure 5).Because there is little resistance, there will belittle pressure and the water will dribble out ofthe holes slowly. But if you raise the pressure,
increasing the resistance, the water will squirtout of the holes forcefully.
The pressure in any fluid system is always related tothe flow and the resistance; the greater the flow andthe greater the resistance, the greater the pressure.
Applying ScientificPrinciples to DialysisDialysis patients’ kidneys don’t work. So, theycome to dialysis with wastes in their blood, extrafluid between their cells and in their bloodvessels, and often with electrolyte imbalances.The main tasks of dialysis are to remove wastesand excess fluid, and balance electrolytes.
Blood itself is a solution. Water is the solvent, andelectrolytes, glucose, and many other substancesare the solutes. Blood also has many particles,such as red and white blood cells. The principlesof fluid dynamics, diffusion, UF, and osmosis applyto each dialysis treatment. To use the principles,we expose the patient’s blood (a solution)—to
781
Figure 5: Positive pressure in a
soaker hose
The principle of positive pressure can be illustrated with anordinary soaker hose. Positive pressure is exerted againstthe sides of the hose as the water moves through it.Excess water is forced through the holes.
The same principle is true in the semipermeablemembranes used in dialysis. The amount of fluid forced or removed through the pores depends partly upon theamount of pressure pushing the fluid through the line.

the dialysate (another solution)—with asemipermeable membrane between them.
FLUID COMPARTMENTSTo understand how dialysis removes fluid, youmust know how fluids work inside the body(see Figure 6). The human body is made mostlyof fluids. Fluids are found inside the cells,tissues, and vasculature (blood vessels). Eachof these three sites is a “compartment:”
n The intracellular compartment is fluidinside the cells.
n The interstitial compartment is fluid inbetween cells.
n The intravascular compartment is bloodinside the blood vessels.
Differences in the level of sodium andelectrolytes between compartments (gradients)cause water to move. The body tries to keepequilibrium—to have the same level ofosmotically-active solutes in all threecompartments. If the level is different, waterwill move from one compartment to anotheruntil they are equal. During dialysis, only fluidfrom the intravascular compartment—thebloodstream—can be removed.6
FLUID DYNAMICS IN DIALYSIS
Fluid dynamics create changes in pressure asblood is pumped out of the patient’s body andthrough tubing and the dialyzer. Together, the tubing and dialyzer are called theextracorporeal (outside of the body) circuit.
When the dialysis machine is switched on andtreatment starts, the blood pump speeds theflow of blood from the patient. Blood passesthrough the needle—the first restriction in thecircuit. Because the blood pump is pulling—rather than pushing—blood through thisrestriction, the pressure created is usuallynegative: less than zero. The amount of flow and restriction determine negative pressure,just as with positive pressure (see Figure 7). As the flow or the restriction increases, thepressure will decrease.2 (The dialysis machinechecks this pressure in the blood tubing beforethe blood pump [pre-pump arterial pressure].)
As the blood passes through the blood pump, it is pushed against the resistance of:
Principles of Dialysis
82
Figure 6: Intake and Output
Fluid in:• Food• Beverages• Intravenous fluids (if any)
Fluid out:• Respiration• Stool• Perspiration and skin water loss• Dialysate loss• Residual urine• Vomiting
1. The tubing
2. The tiny hollow fibers in the dialyzer
3. The small opening of the (venous) blood-return needle (or catheter)
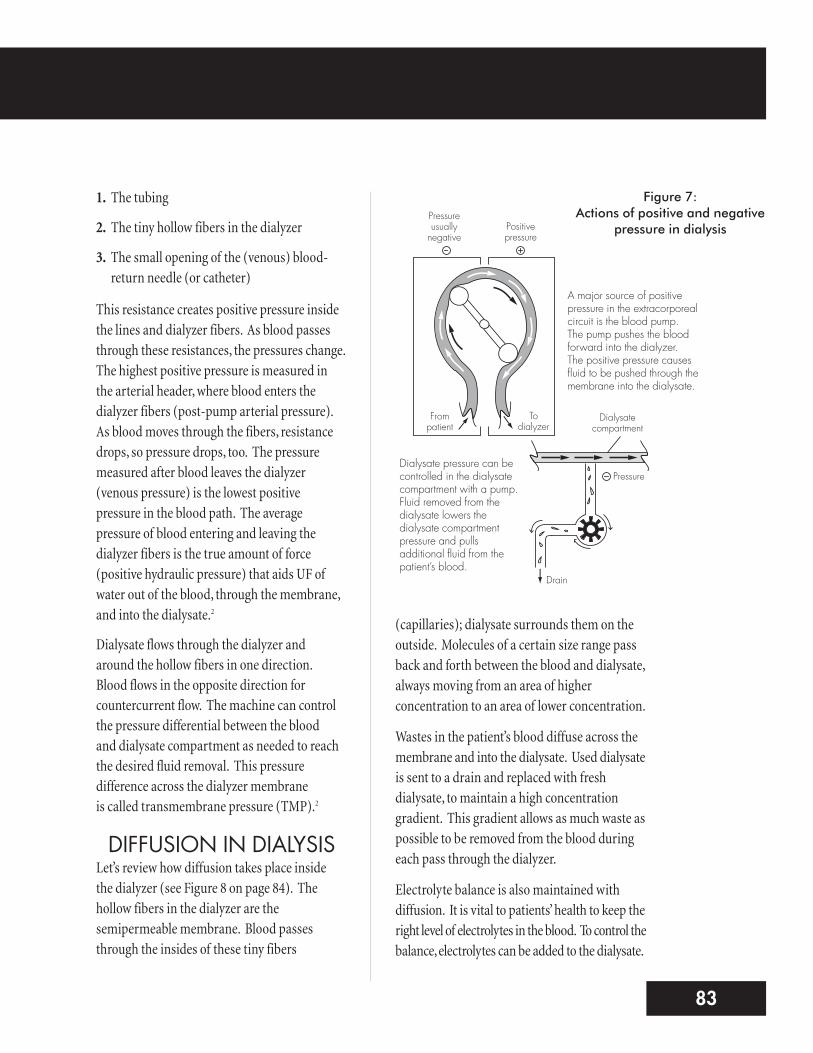
This resistance creates positive pressure inside the lines and dialyzer fibers. As blood passesthrough these resistances, the pressures change.The highest positive pressure is measured in the arterial header, where blood enters thedialyzer fibers (post-pump arterial pressure).As blood moves through the fibers, resistancedrops, so pressure drops, too. The pressuremeasured after blood leaves the dialyzer(venous pressure) is the lowest positivepressure in the blood path. The averagepressure of blood entering and leaving thedialyzer fibers is the true amount of force(positive hydraulic pressure) that aids UF ofwater out of the blood, through the membrane,and into the dialysate.2
Dialysate flows through the dialyzer and around the hollow fibers in one direction.Blood flows in the opposite direction forcountercurrent flow. The machine can controlthe pressure differential between the blood and dialysate compartment as needed to reachthe desired fluid removal. This pressuredifference across the dialyzer membrane is called transmembrane pressure (TMP).2
DIFFUSION IN DIALYSISLet’s review how diffusion takes place inside the dialyzer (see Figure 8 on page 84). Thehollow fibers in the dialyzer are thesemipermeable membrane. Blood passesthrough the insides of these tiny fibers
(capillaries); dialysate surrounds them on theoutside. Molecules of a certain size range passback and forth between the blood and dialysate,always moving from an area of higherconcentration to an area of lower concentration.
Wastes in the patient’s blood diffuse across themembrane and into the dialysate. Used dialysateis sent to a drain and replaced with freshdialysate, to maintain a high concentrationgradient. This gradient allows as much waste aspossible to be removed from the blood duringeach pass through the dialyzer.
Electrolyte balance is also maintained withdiffusion. It is vital to patients’ health to keep theright level of electrolytes in the blood. To control thebalance, electrolytes can be added to the dialysate.
983
Figure 7: Actions of positive and negative
pressure in dialysis
Drain
Pressure
Dialysatecompartment
Todialyzer
Frompatient
Positivepressure
Pressureusually
negative
A major source of positivepressure in the extracorporealcircuit is the blood pump. The pump pushes the bloodforward into the dialyzer. The positive pressure causesfluid to be pushed through themembrane into the dialysate.
Dialysate pressure can becontrolled in the dialysatecompartment with a pump.Fluid removed from thedialysate lowers thedialysate compartmentpressure and pullsadditional fluid from thepatient’s blood.

Principles of Dialysis
84
Electrolytes will move until the concentration isequal on both sides of the membrane. Keeping aconstant low level of an electrolyte in the dialysateensures that the excess is removed withoutallowing the levels in the blood to drop too low.
Diffusion occurs continuously in the patient’sbody. As cleansed blood is returned to thepatient, it slowly dilutes the rest of the blood.The drop in the concentration of solutes in theblood creates a gradient between the bloodplasma (liquid portion of blood) and the fluidin the cells and tissues. Because these cells havetheir ownmembranes, solutes—such as wastesand certain electrolytes—slowly pass out of the
patient’s cells and into the bloodstream. From there, they are dialyzed. This processallows some of the wastes from other bodycompartments to be cleared from the body bydialysis. This slow process of diffusion is whydialysis treatments require more than one passof blood through the dialyzer to clear wastesfrom the blood.
The nephrologist factors in diffusion whenprescribing a treatment. He or she can choose alarge or small dialyzer, based on the patient’s bodysize, the length of the treatment needed, and thesize of molecules to be removed. The only thingthat cannot be chosen is the size of the patient.To get an adequate treatment in a large patient, thedoctor can increase treatment time and/ordialyzer size (clearance) to remove more wastes.2
UF IN DIALYSISUF requires pressure to force fluid through themembrane. The dialysis machine can create ahydraulic pressure difference, with higher pressurein the blood compartment than in the dialysatecompartment. This TMP pushes excess waterout of the blood and into the dialysate.
A dialysis prescription calls for taking off enoughfluid to bring a patient to an estimated dry weight(EDW) by the end of the treatment. To figureout how much fluid you need to remove, justsubtract a patient’s EDW from the predialysisweight. Then add the amount of any fluids thepatient will receive during the treatment.
CONVECTION IN DIALYSISAs water (a solvent) moves from the bloodcompartment to the dialysate compartment,molecules of dissolved solute are dragged alongtoo (solvent drag). This process of solvent
Figure 8: Diffusion inside the dialyzer
Dialysate Dialysate
Blood
Hollow fibers
Blood compartment
Dialysate compartment
Blood
Solutes move betweendialysate and blood tomaintain equilibrium
Excess fluid movesinto dialysate
Cleansed bloodis returned tothe patient
Blood flowsthrough hollowfiber; wastes areremoved withexcess water
Urea andother wastesmove into thedialysate

movement is called convection. The ease withwhich the solute is dragged along by the solventis determined by the size of the solute moleculecompared to the size of the membrane pores.Smaller solutes move easily, so the solution cansieve across the membrane without any changein concentration. But larger solutes move moreslowly and the rate of convective transport isalso slower. Thus, the convective transport of asolute depends on how porous (both size andnumbers of holes) the membrane is. Thismeasurement of porosity is known as thesieving coefficient (SC) of the membrane.7,8
An SC of 1.0 means that, barring other clinicalfactors, the membrane could allow 100% of agiven solute to pass. An SC of 0.4 means thatonly 40% of a solute would pass and 60% wouldbe kept in the blood.
OSMOSIS IN DIALYSISOsmosis also plays a key role in dialysis. Thepressure of UF pushes fluid out of the blood andinto the dialysate. But osmotic forces decidewhich way water will move from one bodycompartment to another. In hemodialysis,diffusion lowers the solute concentration in the
blood. Higher solute concentration in thetissues and cells then pulls water out of theblood. Rapid drops in blood volume can occur,which causes drops in blood pressure and othersymptoms. Often, sodium is added to thedialysate, so it diffuses into the blood. Thehigher blood sodium draws water from otherbody compartments into the blood, so it can beremoved by UF. The sodium in the dialysate isthen lowered towards the end of the dialysistreatment2 to pull the sodium back out of thebloodstream.
ConclusionUnderstanding the principles of dialysis is keyto knowing how the patient’s blood is cleanedby dialysis. Diffusion, filtration, UF, convection,and osmosis must occur in the right amounts ateach treatment.
If you understand dialysis well, you will see howthe treatment can be tailored to meet the needsof each patient. You can play a crucial role indelivering the best dialysis treatment eachpatient can receive.
1185

Learning ActivitiesINSTRUCTOR TOOLS
n Potassium permanganate (available fromthe lab or pharmacy)
n Sheets of cellophane (to make bag)n 3-cc syringe (without needle, to fill bag)n Clear glass beaker, large jar, or a bowln Soft rubber or silastic tubing or hose that will fit on end of faucet
n Tea bagn Sodium chloride (table salt)
ACTIVITIESn Select a patient dialysis record and reviewthe principles of dialysis as seen in the chart.
n Demonstrate the principles of flow, pressure,and resistance by attaching a 12-inch segmentof soft rubber tubing to a faucet. Hold therubber tubing perpendicular to the faucetand turn the water on until water flows slowlyout the end of the hose. Do not adjust theflow, but lower the hose into the sink or abucket. You will notice that the flow of wateris faster, because resistance to the flow hasbeen decreased. By increasing the flow, thepressure of the water coming out is alsoincreased. Now, gently pinch the tubingcloser together, increasing the resistanceto the flow. You will notice an increase in thepressure as the water comes out the end of thetubing. Flow, pressure, and resistance areclosely related, and each has an effect on theothers. This is also true in the hemodialysiscircuit. An obstruction at the venous needleincreases resistance to the blood flow,increasing the venous pressure reading.
n Demonstrate diffusion and filtration byplacing a tea bag in a glass of hot water.
Tea coloring will slowly diffuse throughthe glass of water. Meanwhile, thesemipermeable membrane of the tea baghas filtered the tea leaves, preventingthem from passing across the membrane.
n Demonstrate filtration and UF by soakinga sponge in water. Hold the sponge over thebucket of water and watch the sponge filterthe water. Now apply positive pressure to the sponge (squeeze it) and see howmuch more water can be removed, orultrafiltered, by applying pressure.
n Demonstrate diffusion and osmosis bymaking a bag out of a piece of cellophane.(Be sure to wet the membrane so that it doesnot tear as easily.) Into this bag, place 1 ccof potassium permanganate solution andsuspend the bag in a beaker or glass of water.Very quickly, the potassium permanganatewill diffuse into the water. At the same time,osmosis will take place. The volume insidethe bag will increase as water enters thebag to equalize the concentration on bothsides of the membrane. This process canalso be demonstrated with salt water in thebag instead of potassium permanganate.The water in the glass will become salty,while the volume in the bag will increaseas water moves into the bag in an attemptto equilibrate the concentrations of salton both sides of the bag.
n Diagram the extracorporeal blood circuit;label compartments, direction of flow ofblood and dialysate, and points of resistance.
n Observe the calculation and applicationof TMP to dialysis.
n Note patient predialysis and postdialysisweight.
Principles of Dialysis
86

References1. Dorland WAN: Dorland’s Illustrated Medical Dictionary. Philadelphia, PA, W.B. Saunders Co.,1988, pp 470, 632, 641, 1196, 1541, 1546.
2. Salai PB: Hemodialysis, in Parker J (ed): Contemporary Nephrology Nursing. Pitman, NJ,American Nephrology Nurses’ Association, 1998, pp 527-574.
3. Pickett JP (ed): Compact American Medical Dictionary. Boston, MA, Houghton MifflinCompany, 1998, p 317.
4. Sweeny J, Hajko B, Womack B, Cobb T, Lesher KM: Required basic knowledge, in Curtis J,Varughese P (eds):Dialysis Technology: A Manual for Dialysis Technicians (3rd ed). Dayton, OH,National Association of Nephrology Technicians/Technologists, 2003, p 196.
5. Daugirdas JT, Van Stone JC: Physiological principles and urea kinetic modeling, in DaugirdasJT, Blake PG, Ing TS: Handbook of Dialysis (3rd ed). Philadelphia, PA, Lippincott, Williams &Wilkins, 2001, p 15-45.
6. Purcell W, Manias E, Williams A, Walker R: Accurate dry weight assessment: reducing theincidence of hypertension and cardiac disease in patients on hemodialysis. Nephrol Nurs J31(6):631-636, 2004.
7. Ahmad S: Brief history and general principles of dialysis, in: Manual of Clinical Dialysis.London, UK, Current Medicine Group Ltd., 1999, p 3.
8. Price CA: Continuous renal replacement therapy, in Lancaster LE (ed): ANNA Core Curriculum forNephrology Nursing (3rd ed). Pitman, NJ, American Nephrology Nurses’ Association, 1995, p 330.
1387