observation services · why is obs important now? medicare pays a fixed amount for inpatient care...
TRANSCRIPT

Observation Services
Michael A. Granovsky, MD CPC FACEP
President LogixHealth

▪ CMS Recovery Audit Contractors (RACs) focusing on inpatient DRG payments vs. observation status
▪ Hospitals under pressure to cut costs – Global contracts/ACOs/directly insuring
communities There is opportunity!
▪ ED groups ideally suited to run efficient units with short lengths of stay – We have the throughput mindset!
Why is Obs Important Now?

▪ Medicare pays a fixed amount for inpatient care ▪ Typically a large amount
– Much more than the observation payment ▪ Recent study calculated use of Obs instead of
inpatient reduce CMS cost dramatically ▪ Average cost savings per patient = $1,572 ▪ Annual savings calculated: $3.1 Billion
DRG Economics

▪ RACs collected more than $2 billion from hospitals in 2013
▪ AHA's RACTrac Survey – 63 percent of hospitals spent at least $40,000
in 2013 for RAC-related defense costs – 46 percent > $100,000 in defense costs – 28 percent > $200,000 – 10 percent > $400,000
▪ SHORT-STAY DENIALS: Largest Area of Investigation – 62% of short-stay denials were because the care
was reported as Inpatient vs Obs
Whacked by RAC

▪ TIA 6% (DRG 69) ▪ Chest pain 8% (DRG 313) ▪ Syncope 16% (DRG 312) ▪ COPD (uncomplicated) 5% (DRG 312) ▪ Pulmonary edema 4% (DRG 189) RAC review of one-day stays: 78% of claims denied because the care was reported as Inpatient vs Obs
Top RAC DRG Targets and Denials

Observation care is a well-defined set of specific, clinically appropriate services, that are furnished while a decision is being made regarding whether patients will require further treatment as hospital inpatients.
CMS Transmittal 1745, 290.1 - Obs Services Overview
Such services are covered only when provided by order of a physician…
“The following codes are used to report encounters by the supervising physician…and performance of periodic reassessments” CPT 2015 page 17
2015 Obs CPT & CMS
▪ Timed/dated order to place in observation status ▪ A short treatment plan
regarding the goals of observation
▪ Clinically appropriate progress notes – Asthma different than chest pain
▪ A discharge summary reviewing the course in observation, findings, and plan
General Documentation Requirements

Same day admit and discharge CPT Codes: ▪ 99234 – Low severity
– Low-complexity MDM ▪ 99235 – Moderate severity
– Moderate-complexity MDM ▪ 99236 – High severity
– High-complexity MDM
Professional Observation CPT Codes
▪ Medicare requires 8 hours of Obs. on the same calendar date to bill 99234-99236 – CPT does not define a time threshold
▪ If the Obs. stay spans 2 calendar days, no time constraints for CMS or CPT payers
CMS 8 Hour Rule

▪ Admit and discharge more than one calendar day:
▪ Initial Day CPT codes: – 99218 – Low severity
• Low-complexity MDM – 99219 – Moderate severity
• Moderate-complexity MDM – 99220 – High severity
• High-complexity MDM
Professional Observation CPT Codes

Discharge day CPT Code: ▪ 99217- Discharge Day ▪ Includes final exam, discussion of
observation stay, follow-up instructions, and documentation
▪ Used with codes from the initial observation day codes series (99218/99219/99220)
Professional Observation CPT Codes

Observation Level of Care
Care All on the Same Day
Care Covers Two Calendar Days
1 99234 99218 + 99217
2 99235 99219 + 99217
3 99236 99220 + 99217
Coding Scenarios Observation Services

▪ All but the lowest level Obs require very significant Hx and PE documentation
▪ Comprehensive Hx and PE: 99219/99220 & 99235/99236
– HPI: 4 elements – PFSHx: 3 areas (Requires Family Hx) – ROS: 10 systems – PE: 8 organ systems
Obs services typically require a family history
▪ Beware overuse of macros for ROS and PE
Physician Documentation
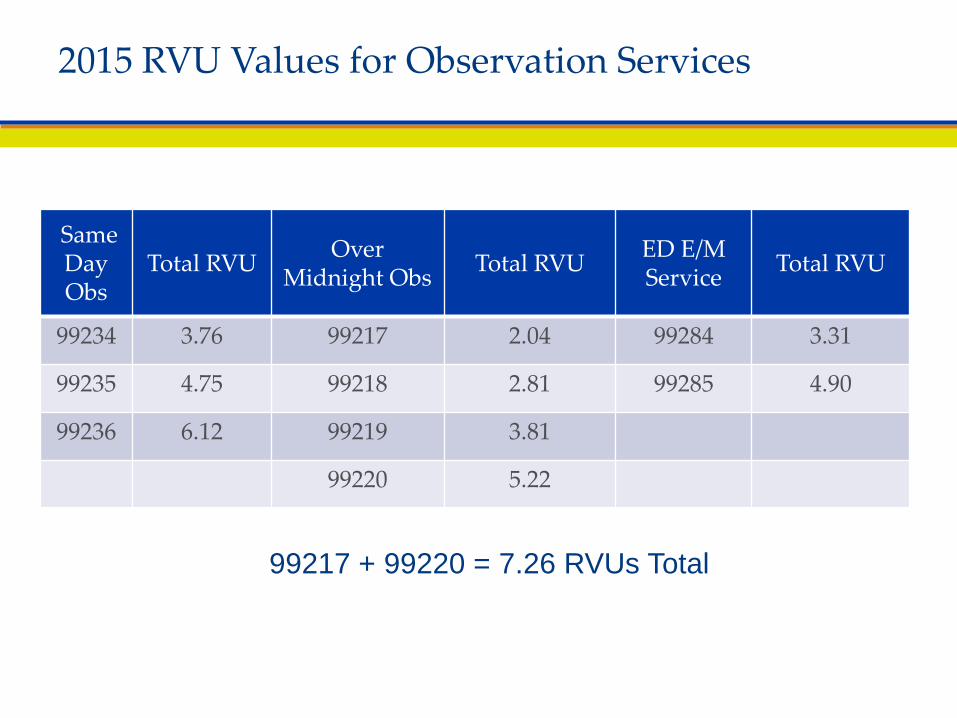
2015 RVU Values for Observation Services
Same Day Obs
Total RVU Over Midnight Obs Total RVU ED E/M
Service Total RVU
99234 3.76 99217 2.04 99284 3.31
99235 4.75 99218 2.81 99285 4.90
99236 6.12 99219 3.81
99220 5.22
99217 + 99220 = 7.26 RVUs Total

▪ 2 downcodes: 99236 99234 – Loose 4.72 RVUs. – $168.98 – 39%
Cost Of Hx and PE Downcodes
$438.20
$353.71
$269.22
$100.00
$200.00
$300.00
$400.00
$500.00
99236 x 2 1 Downcode 2 Downcodes
Obs Revenue
▪ Most ED run Observation units see higher acuity patients
▪ Chest pain or clinically equivalent
complexity is very common ▪ ED Observation E/M distribution
influenced by pre-selected complexity
Obs Coding Methodology

Clinical Benchmarks of Patient Complexity ▪ No AMA CPT Appendix C Obs code vignettes
CMS RUC data base vignettes ▪ 99234: 19 y.o . pregnant patient (9 weeks gestation) presents
to the ED with vomiting X 2 days. The patient is admitted for observation and discharged later on the same day.
▪ 99235: 48-year-old presents with an asthma exacerbation
in moderate distress.
▪ 99236: 52-year-old patient comes to the ED because of chest pain.

10.9%
27.3%
61.8%
0%
10%
20%
30%
40%
50%
60%
70%
99234 99235 99236
Medicare E Med Obs Codes Reported RUC Data Base Analysis
CMS E Med Obs E/M Distribution
2013 data q4 2014 analysis
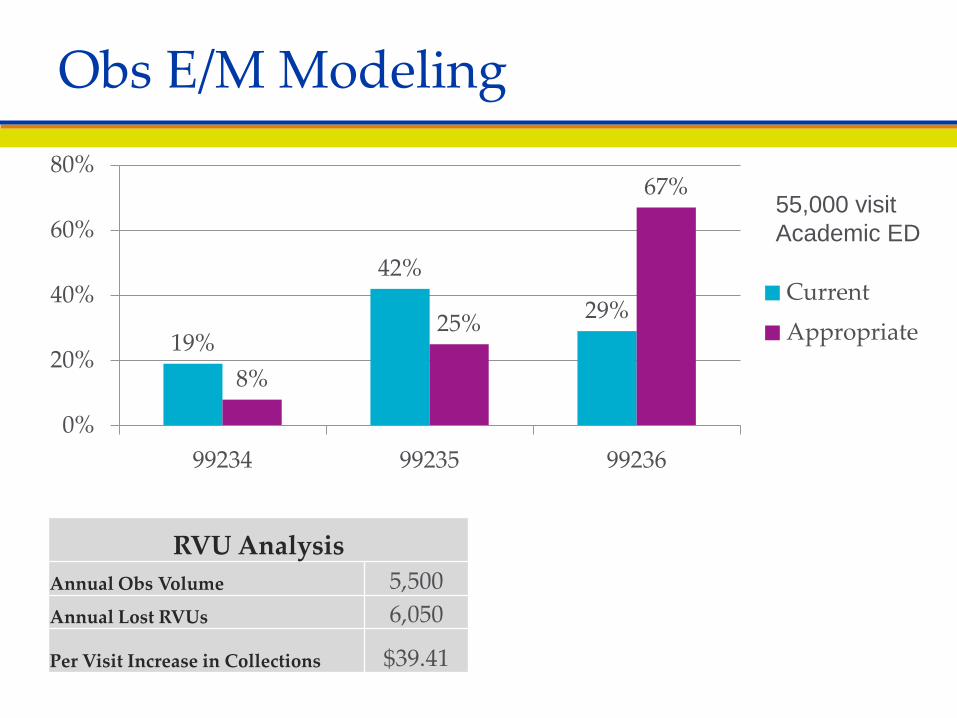
19%
42%
29%
8%
25%
67%
0%
20%
40%
60%
80%
99234 99235 99236
Current Appropriate
Obs E/M Modeling
RVU Analysis Annual Obs Volume 5,500 Annual Lost RVUs 6,050
Per Visit Increase in Collections $39.41
55,000 visit Academic ED

Which Obs patients will an ED group be successful with? ▪ Select patients with diagnoses
that have clinical protocols ▪ Expedite throughput ▪ Achieve decreased length of stay ▪ Reach a successful clinical endpoint ▪ Prolonged stays drag down RVU efficiency
Who Should Be In Obs?

▪ Chest pain ▪ Abdominal pain ▪ Headache ▪ Cellulitis ▪ Pyelonephritis ▪ Asthma ▪ Dehydration ▪ Renal colic ▪ Hypoglycemia ▪ Allergic reaction ▪ Pharyngitis
▪ Closed head injury ▪ Vertigo ▪ Hematuria ▪ Pancreatitis ▪ SOB ▪ CHF/COPD ▪ Back pain
– non ambulatory ▪ Extremes of age ▪ Mental Health
– Substance abuse
The Spectrum of Complexity
Easier Harder
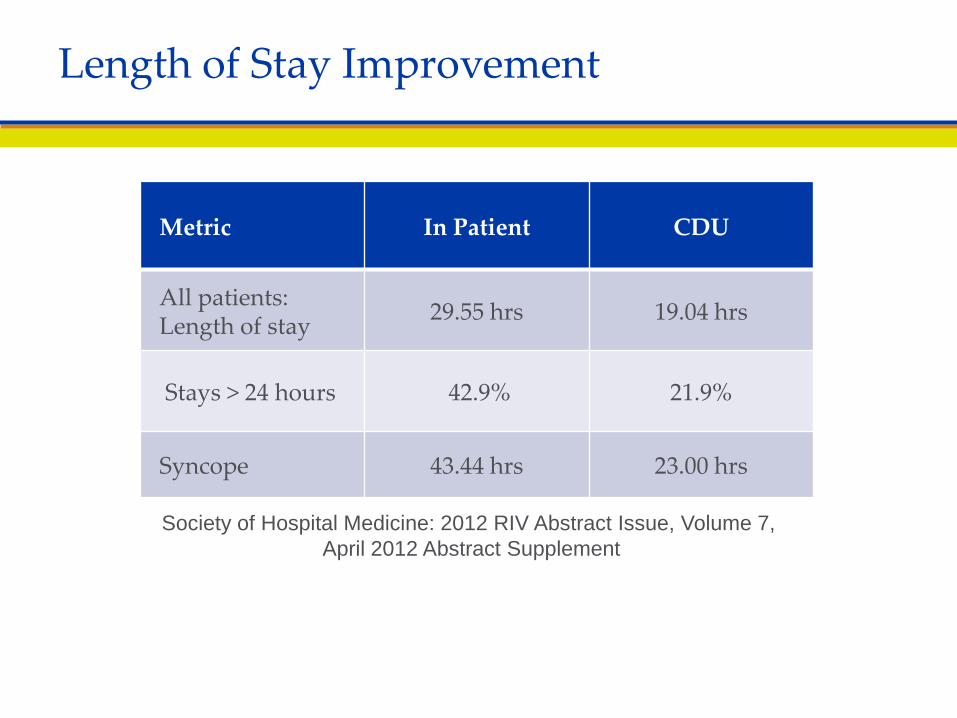
Metric In Patient CDU
All patients: Length of stay 29.55 hrs 19.04 hrs
Stays > 24 hours 42.9% 21.9%
Syncope 43.44 hrs 23.00 hrs
Length of Stay Improvement
Society of Hospital Medicine: 2012 RIV Abstract Issue, Volume 7, April 2012 Abstract Supplement
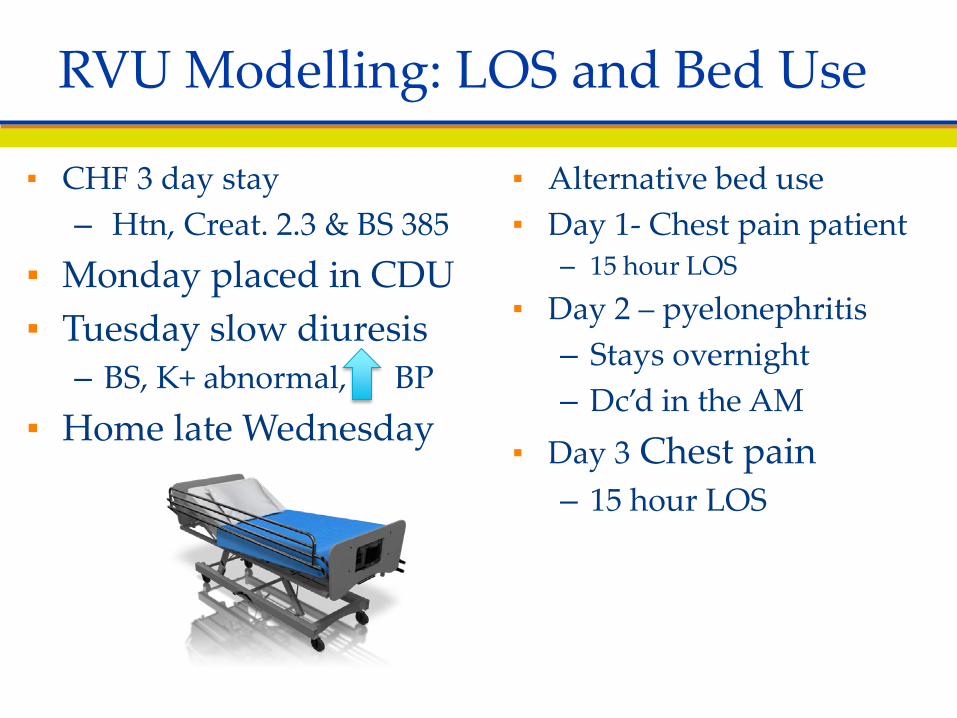
▪ CHF 3 day stay – Htn, Creat. 2.3 & BS 385
▪ Monday placed in CDU ▪ Tuesday slow diuresis
– BS, K+ abnormal, BP ▪ Home late Wednesday
▪ Alternative bed use ▪ Day 1- Chest pain patient
– 15 hour LOS ▪ Day 2 – pyelonephritis
– Stays overnight – Dc’d in the AM
▪ Day 3 Chest pain – 15 hour LOS
RVU Modelling: LOS and Bed Use
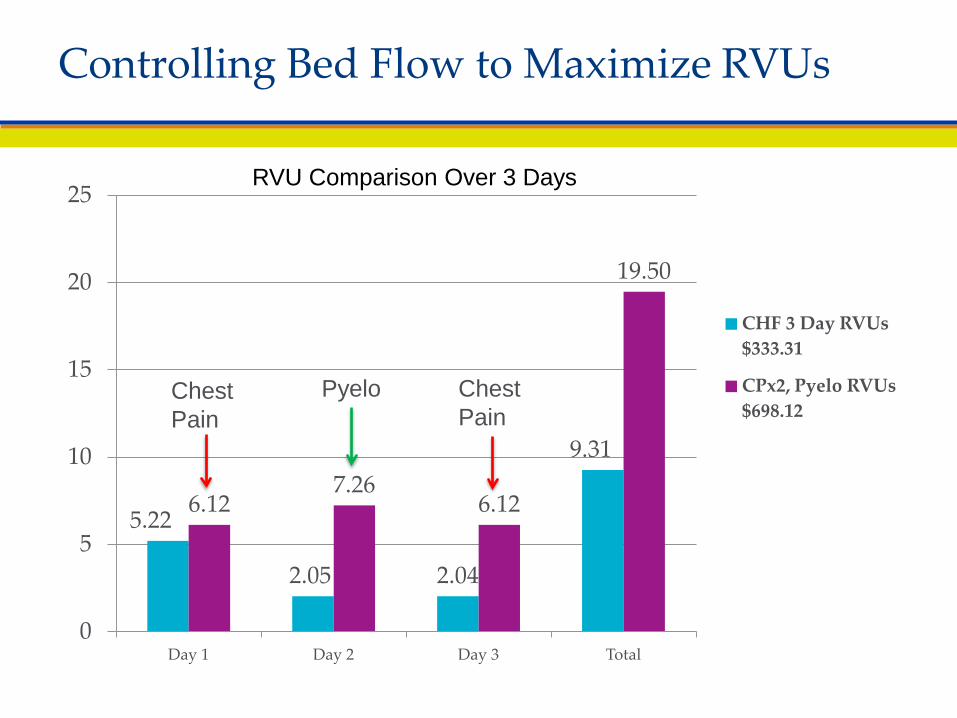
Controlling Bed Flow to Maximize RVUs
5.22
2.05 2.04
9.31
6.12 7.26
6.12
19.50
0
5
10
15
20
25
Day 1 Day 2 Day 3 Total
CHF 3 Day RVUs $333.31
CPx2, Pyelo RVUs $698.12
RVU Comparison Over 3 Days
Chest Pain
Chest Pain
Pyelo

OPPS Definitions ▪ Direct supervision: during the initiation
of observation ▪ General Supervision: once the patient is
deemed stable ▪ CMS further stated: the provider could be
an MD or NP/PA Original citation OPPS 2011 no 2015 change
Who Mans The Unit
“When observation status is initiated in the course of an encounter in
another site of service (e.g., hospital emergency department) all evaluation and management services provided by
the supervising physician in conjunction with initiating the
observation status are considered part of the initial observation care when
provided on the same date.” CPT 2015
The Observation Roll Up

▪ 10 bed unit…turned 1.3 times daily – Blend of moderate and high ….5.5 RVUs per case – 74 RVUs….$34/RVU….$2,400 daily Cost: salary, benefits,
overhead…?tough to cover costs Innovative Profit Solutions ▪ MD coverage in the morning and evening ▪ PA/NP interim coverage ▪ Creep up volume to be profitable
– Expand beyond chest pain to include protocol driven complaints such as Dehydration, Pyelonephritis, Asthma, Cellulitis
Observation Unit Staffing for Profit

▪ CMS and members of Congress concerns: – Beneficiaries spending long periods of time in Obs
without being admitted as inpatients – Obs is an outpatient status – Concerned beneficiaries may pay more as outpatients
than if they were admitted as inpatients • If not inpatient then responsible for SNF charges
– In 2012, 11% of Obs was > 3 days • 80/20 co-insurance under part B • Self administered (P.O.) medications not covered
OIG Report and HHS Letter The 2 Midnight Rule
▪ SNF Obs stay…no qualifying SNF Medicare coverage Patient may be entirely responsible - $5,000 Typical stay starts at roughly $250 per day
Qualifying inpatient stay spanning 3 nights No patient SNF cost sharing for first 20 days After 20 days co-payment is $145 per day
▪ 20% co pays add up for longer complex Obs stays Inpatient expense: Part A inpatient deductible $1,260
▪ Self administered meds- “uncovered service” - gross hospital charges are in play (average bill $528)
Patient Financial Considerations

2 Midnight Rule The Benchmark: We are specifying that for those hospital stays in
which the physician expects the beneficiary to require care that crosses 2 midnights and admits the beneficiary based upon that
expectation, Medicare Part A payment is generally appropriate. 2014 IPPS Final Rule 60/2225
The Presumption- “Inpatient hospital claims with lengths of stay greater than 2 midnights after the formal admission following the order will be presumed generally appropriate for Part A payment and will not be the focus of medical review efforts.” IPPS Final Rule 1726/2225
OIG Concerns: The 2 Midnight Rule Is Born

“The final rule clarifies that the benchmark used in determining the expectation of a stay of at least two midnights begins when the beneficiary starts receiving services in the hospital. This would include outpatient care received while the beneficiary is in observation or is receiving services in the emergency department, operating room, or other treatment area.“
How to Calculate The 2 days
▪ RAC Audit backlog 800,000 RAC appeals in backlog; 2-3 years 68% settlement offer
▪ RAC audits fines delayed ▪ H.R. 4302: “probe and educate” program to assess
compliance with the “two-midnight rule,” on a pre payment basis through March 31, 2015
▪ Nov 25th Hospital Improvement for Payment Act of 2014 Discussion Draft – interim per diem system through 2020
The 2 Midnight Rule On The Books: In Flux
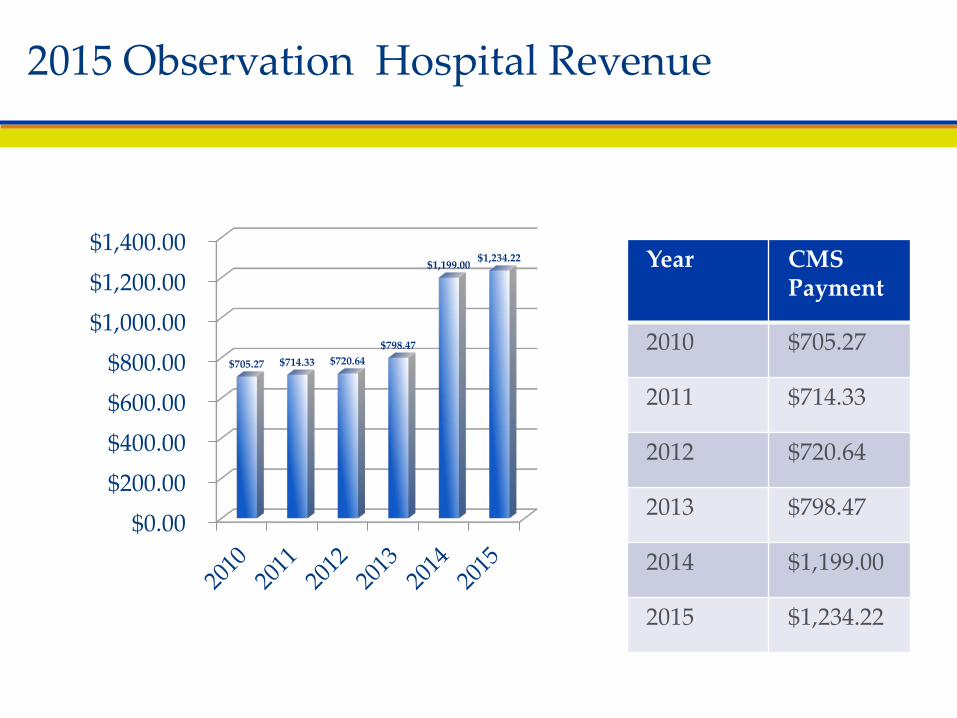
Year CMS Payment
2010 $705.27
2011 $714.33
2012 $720.64
2013 $798.47
2014 $1,199.00
2015 $1,234.22
2015 Observation Hospital Revenue
$0.00 $200.00 $400.00 $600.00 $800.00
$1,000.00 $1,200.00 $1,400.00
$705.27 $714.33 $720.64 $798.47
$1,199.00 $1,234.22
▪ 2014 status indicator X ancillary packaged Typical ED lab studies, some U/S services
▪ 2015 OPPS Final Rule further packaging increase Items w/geometric mean cost < $100 Status Indicator (S.I.) X deleted Q1-packages w/ S.I. S/T/V Q2- packaged w/ S.I. T Q3- packaged as part of a composite
99284/99285/99291 Q3- composite within APC 8009
Drug administration codes generally not packaged Documentation and Coding still really matters Q1 S.I. packages most plain films, some US, splint/strapping,
many minor procedures such as simple laceration
Observation Increased Payments in 2014 and 2015 What's The Catch?

▪ Risks: overuse of observation – Financial- lower payment to hospital vs. inpatient
• $5,142 vs. $1,741 (looking at top 10 diags.) – Loss of 3 day qualifying stay for SNF coverage – Potential higher out-of-pocket expense for patients
▪ Risks: underuse of observation – Inappropriate inpatient admissions - RAC target – Short inpatient stays:
• decrease CMI • hospital payment denials
The Obs Pendulum: Facility Financial Risk/Reward
▪ Observation services will be an expanding determinant of our financial success
▪ Documentation and correct coding methodology drive the revenue per patient
▪ Focused patient selection, throughput and protocols optimize RVUs/day
▪ Packaging of services will lead to resource use pressure and efficiency pressure!
▪ The ED throughput culture is ideally suited to maximize Observation financial success
Conclusions
Contact Information
Michael A. Granovsky, MD CPC FACEP
President LogixHealth
www.logixhealth.com
Appendix
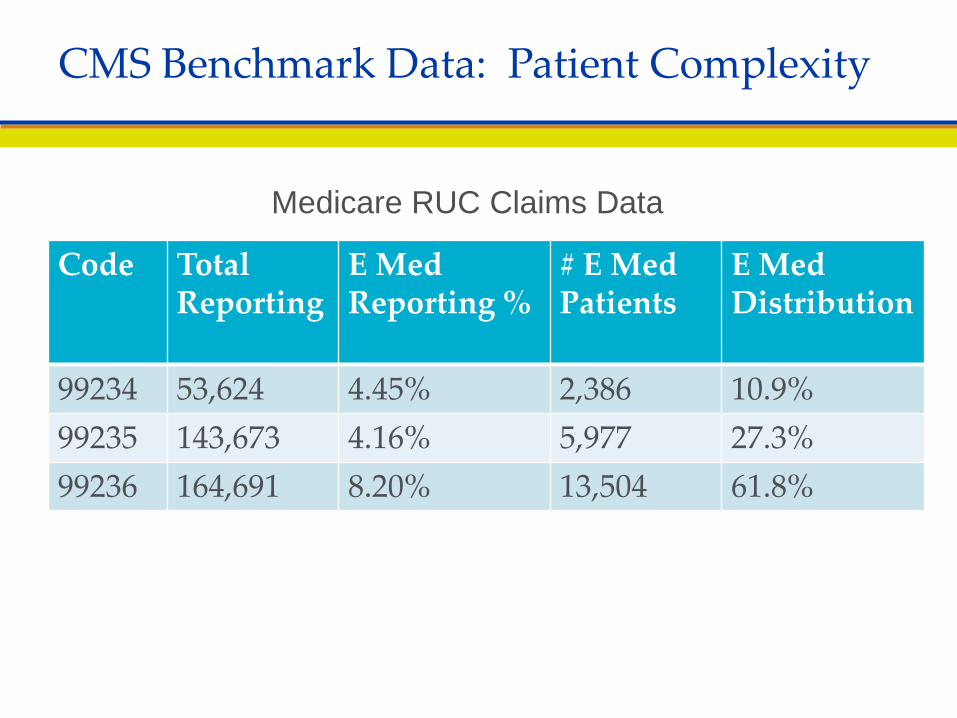
Code Total Reporting
E Med Reporting %
# E Med Patients
E Med Distribution
99234 53,624 4.45% 2,386 10.9% 99235 143,673 4.16% 5,977 27.3% 99236 164,691 8.20% 13,504 61.8%
CMS Benchmark Data: Patient Complexity
Medicare RUC Claims Data

▪ Facility Observation is a composite APC (8009) Combines specifically required visit type with
a minimum # of Observation hours 99284/99285/99291 Level 5 Type B ED visit (G0384) An outpatient clinic visit (G0463)
8 Hours reported as units of G0378 (in the units field) There must be a physician order for observation No T status procedure
2015 Observation Composite APC
▪ CMS requires that comprehensive observation histories have 3 of 3 PFSH elements rather than the 2 of 3 requirement for ED E/M codes
Medicare 1995 DGs page 6
– May utilize the nurse’s notes but beware • Rarely document a Family Hx
“A review of all three history areas is required for services that by their nature include a comprehensive assessment
or reassessment of the patient.”
CMS PFSHx Observation Requirement
Contact Information
Michael A. Granovsky, MD CPC FACEP
President LogixHealth
www.logixhealth.com