october 2019 medical policy update bulletin · in this issue 3 medical policy update bulletin:...
TRANSCRIPT

UnitedHealthcare respects the expertise of the physicians, health care professionals, and their staff who participate in our network. Our goal is to support you and your patients in making the most informed decisions regarding the choice of quality and cost-effective care, and to support practice
staff with a simple and predictable administrative experience. The Medical Policy Update Bulletin was developed to share important information regarding UnitedHealthcare Medical Policy, Medical Benefit Drug Policy, Coverage Determination Guideline, Utilization Review Guideline, and Quality of Care Guideline updates.* *Where information in this bulletin conflicts with applicable state and/or federal law, UnitedHealthcare follows such applicable federal and/or state law.
October 2019
medical policy update bulletin Medical Policy, Medical Benefit Drug Policy & Coverage Determination Guideline Updates
Updated Oct. 4, 2019: Implementation of the changes described in this bulletin for the following Medical Benefit Drug Policies has been delayed until further notice: Page 21: Cimzia® (Certolizumab Pegol) (New)
Page 26: Actemra® (Tocilizumab) Injection for Intravenous Infusion (Revised) Page 41: Orencia® (Abatacept) Injection for Intravenous Infusion (Revised) Page 43: Simponi Aria® (Golimumab) Injection for Intravenous Infusion (Revised)
Updated Oct. 8, 2019: Implementation of the changes described in this bulletin for the following Clinical Policy has been delayed until further notice: Page 27: Benlysta® (Belimumab) (Revised)

2 Medical Policy Update Bulletin: October 2019
Medical Policy, Medical Benefit Drug Policy & Coverage Determination Guideline Updates
Overview
Tips for using the Medical Policy Update Bulletin:
From the table of contents, click the policy title to be
directed to the corresponding policy update summary.
From the policy updates table, click the policy title to view a
complete copy of a new, updated, or revised policy.
Policy Update Classifications
New
New clinical coverage criteria and/or documentation review
requirements have been adopted for a health service (e.g., test, drug,
device or procedure)
Updated
An existing policy has been reviewed and changes have not been made
to the clinical coverage criteria or documentation review requirements;
however, items such as the clinical evidence, FDA information, and/or
list(s) of applicable codes may have been updated
Revised
An existing policy has been reviewed and revisions have been made to
the clinical coverage criteria and/or documentation review requirements
Replaced
An existing policy has been replaced with a new or different policy
Retired
The health service(s) addressed in the policy are no longer being
managed or are considered to be proven/medically necessary and are
therefore not excluded as unproven/not medically necessary services,
unless coverage guidelines or criteria are otherwise documented in
another policy
Note: The absence of a policy does not automatically indicate or imply
coverage. As always, coverage for a health service must be determined
in accordance with the member’s benefit plan and any applicable
federal or state regulatory requirements. Additionally, UnitedHealthcare
reserves the right to review the clinical evidence supporting the safety
and effectiveness of a medical technology prior to rendering a coverage
determination.
This bulletin provides complete details on UnitedHealthcare Medical
Policy, Medical Benefit Drug Policy, Coverage Determination
Guideline (CDG), Utilization Review Guideline (URG), and/or
Quality of Care Guideline (QOCG) updates. The inclusion of a
health service (e.g., test, drug, device or procedure) in this bulletin
indicates only that UnitedHealthcare has recently adopted a new
policy and/or updated, revised, replaced or retired an existing
policy; it does not imply that UnitedHealthcare provides coverage
for the health service. In the event of an inconsistency or conflict
between the information provided in this bulletin and the posted
policy, the provisions of the posted policy will prevail. Note that
most benefit plan documents exclude from benefit coverage health
services identified as investigational or unproven/not medically
necessary. Physicians and other health care professionals may not
seek or collect payment from a member for services not covered by
the applicable benefit plan unless first obtaining the member’s
written consent, acknowledging that the service is not covered by
the benefit plan and that they will be billed directly for the service.
The complete library of UnitedHealthcare Medical
Policies, Medical Benefit Drug Policies, CDGs, URGs, and
QOCGs is available at UHCprovider.com > Policies and
Protocols > Commercial Policies > Medical & Drug
Policies and Coverage Determination Guidelines.

3 Medical Policy Update Bulletin: October 2019
Medical Policy, Medical Benefit Drug Policy & Coverage Determination Guideline Updates
In This Issue
Take Note
QUARTERLY CPT® AND HCPCS CODE UPDATES
Effective Oct. 1, 2019, all applicable Medical Policies and Medical Benefit Drug Policies have been modified to reflect the quarterly Current Procedural Terminology (CPT®) and Healthcare Common Procedure Coding System (HCPCS) code additions, revisions, and deletions.
Medical Policy Updates Page
UPDATED
Electric Tumor Treatment Field Therapy – Effective Nov. 1, 2019 ......................................................................................................................... 5 Molecular Oncology Testing for Cancer Diagnosis, Prognosis, and Treatment Decisions – Effective Oct. 1, 2019 ........................................................... 5 Skin and Soft Tissue Substitutes – Effective Oct. 1, 2019 .................................................................................................................................... 5
REVISED
Apheresis – Effective Nov. 1, 2019 ................................................................................................................................................................... 5 Bariatric Surgery – Effective Dec. 1, 2019 ....................................................................................................................................................... 10 Epidural Steroid and Facet Injections for Spinal Pain – Effective Dec. 1, 2019 ....................................................................................................... 12 Genetic Testing for Hereditary Cancer – Effective Oct. 1, 2019 ........................................................................................................................... 14 Omnibus Codes – Effective Dec. 1, 2019 ......................................................................................................................................................... 17 Vagus and External Trigeminal Nerve Stimulation – Effective Dec. 1, 2019 .......................................................................................................... 18
Medical Benefit Drug Policy Updates
NEW
Cimzia® (Certolizumab Pegol) – Effective Oct. 1, 2019 TBD ............................................................................................................................... 21 Krystexxa® (Pegloticase) – Effective Oct. 1, 2019 ............................................................................................................................................. 24
UPDATED
Complement Inhibitors (Soliris® & Ultomiris™) – Effective Oct. 1, 2019 ............................................................................................................... 25 Evenity™ (Romosozumab-Aqqg) – Effective Oct. 1, 2019 .................................................................................................................................. 26 Gamifant™ (Emapalumab-Lzsg) – Effective Oct. 1, 2019 ................................................................................................................................... 26 Onpattro™ (Patisiran) – Effective Oct. 1, 2019 ................................................................................................................................................ 26
REVISED
Actemra® (Tocilizumab) Injection for Intravenous Infusion – Effective Oct. 1, 2019 TBD ........................................................................................ 26 Benlysta® (Belimumab) – Effective Oct. 1, 2019 TBD ........................................................................................................................................ 27 Clotting Factors, Coagulant Blood Products & Other Hemostatics – Effective Oct. 1, 2019 ....................................................................................... 28

4 Medical Policy Update Bulletin: October 2019
Medical Policy, Medical Benefit Drug Policy & Coverage Determination Guideline Updates
In This Issue
Infliximab (Remicade®, Inflectra™, Renflexis™) – Effective Oct. 1, 2019 ............................................................................................................. 28 Ketalar® (Ketamine) and Spravato™ (Esketamine) – Effective Oct. 1, 2019 ......................................................................................................... 33 Maximum Dosage – Effective Oct. 1, 2019 ...................................................................................................................................................... 36 Oncology Medication Clinical Coverage – Effective Oct. 1, 2019 .......................................................................................................................... 38 Orencia® (Abatacept) Injection for Intravenous Infusion – Effective Oct. 1, 2019 TBD ........................................................................................... 41 Review at Launch Medication List – Effective Oct. 1, 2019 ................................................................................................................................. 42 Self-Administered Medications List – Effective Oct. 1, 2019 ............................................................................................................................... 43 Simponi Aria® (Golimumab) Injection for Intravenous Infusion – Effective Oct. 1, 2019 TBD .................................................................................. 43 Sodium Hyaluronate – Effective Oct. 1, 2019 ................................................................................................................................................... 44 Stelara® (Ustekinumab) – Effective Oct. 1, 2019 .............................................................................................................................................. 47
Coverage Determination Guideline (CDG) Updates
REVISED
Preventive Care Services – Effective Dec. 1, 2019 ............................................................................................................................................ 51
5 Medical Policy Update Bulletin: October 2019
Medical Policy Updates
Policy Title Effective Date Summary of Changes
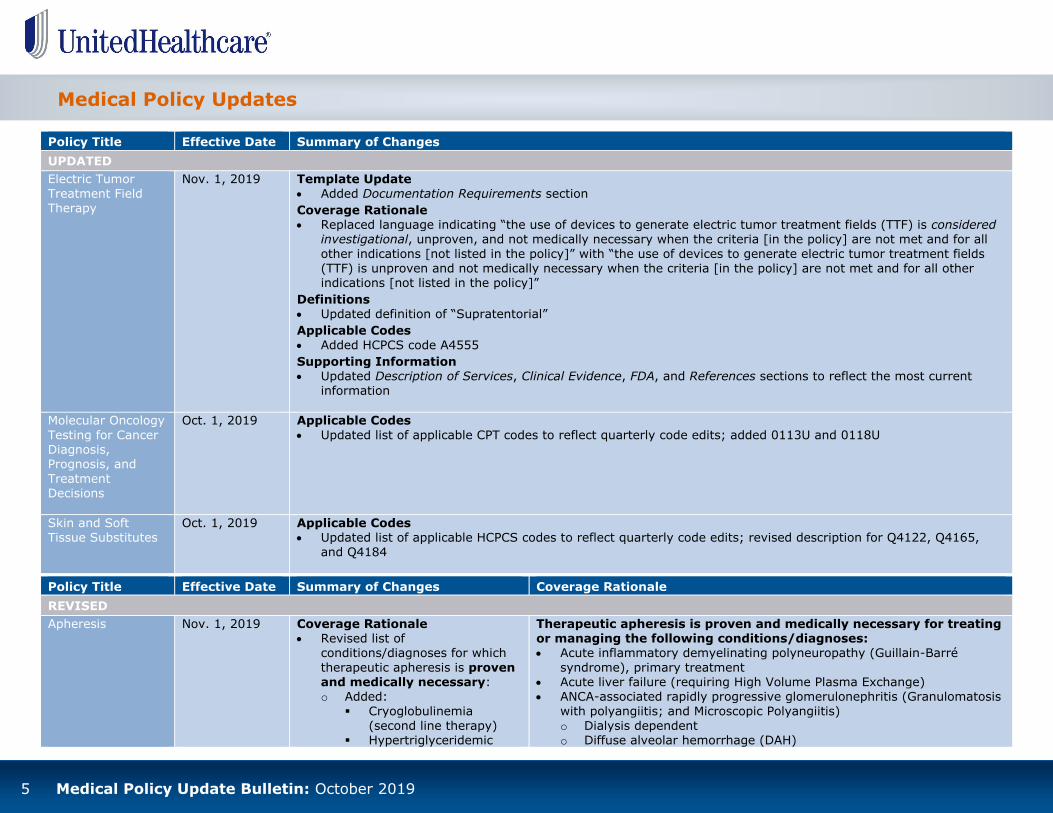
UPDATED
Electric Tumor
Treatment Field Therapy
Nov. 1, 2019 Template Update
Added Documentation Requirements section
Coverage Rationale Replaced language indicating “the use of devices to generate electric tumor treatment fields (TTF) is considered
investigational, unproven, and not medically necessary when the criteria [in the policy] are not met and for all
other indications [not listed in the policy]” with “the use of devices to generate electric tumor treatment fields (TTF) is unproven and not medically necessary when the criteria [in the policy] are not met and for all other indications [not listed in the policy]”
Definitions Updated definition of “Supratentorial”
Applicable Codes
Added HCPCS code A4555
Supporting Information Updated Description of Services, Clinical Evidence, FDA, and References sections to reflect the most current
information
Molecular Oncology
Testing for Cancer Diagnosis, Prognosis, and
Treatment Decisions
Oct. 1, 2019 Applicable Codes
Updated list of applicable CPT codes to reflect quarterly code edits; added 0113U and 0118U
Skin and Soft Tissue Substitutes
Oct. 1, 2019 Applicable Codes Updated list of applicable HCPCS codes to reflect quarterly code edits; revised description for Q4122, Q4165,
and Q4184
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Apheresis
Nov. 1, 2019
Coverage Rationale Revised list of
conditions/diagnoses for which
therapeutic apheresis is proven and medically necessary: o Added:
Cryoglobulinemia
(second line therapy) Hypertriglyceridemic
Therapeutic apheresis is proven and medically necessary for treating or managing the following conditions/diagnoses: Acute inflammatory demyelinating polyneuropathy (Guillain-Barré
syndrome), primary treatment Acute liver failure (requiring High Volume Plasma Exchange) ANCA-associated rapidly progressive glomerulonephritis (Granulomatosis
with polyangiitis; and Microscopic Polyangiitis)
o Dialysis dependent o Diffuse alveolar hemorrhage (DAH)

6 Medical Policy Update Bulletin: October 2019
Medical Policy Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Apheresis
(continued)
Nov. 1, 2019
pancreatitis, severe
Major hematopoietic stem cell transplant, ABO incompatible, second line therapy
- HPC(M) - HPC(A)
Myeloma cast
nephropathy (second line therapy)
Neuromyelitis optica
spectrum disorders (Devic’s syndrome), relapse (second line therapy)
Renal transplantation, ABO incompatible
(second line therapy)
- Antibody mediated rejection
Voltage gated potassium
channel antibodies-related conditions
o Removed: ABO incompatible major
hematopoietic stem cell/bone marrow transplant (only as
second line therapy) ABO incompatible kidney
transplantation (only as
second line therapy) - Antibody mediated
rejection, living donor (LD)
desensitization - A²/A²B into B,
deceased donor
Age-related macular
Anti-glomerular basement membrane disease (Goodpasture’s syndrome)
o Dialysis independent o DAH
Cardiac transplantation, second line therapy o Recurrent rejection
o Desensitization Chronic inflammatory demyelinating polyneuropathy Cryoglobulinemia, second line therapy
Cutaneous T-cell lymphoma; mycosis fungoides; Sezary syndrome, erythrodermic
Familial hypercholesterolemia
o Homozygous o Heterozygous, second line therapy
Focal segmental glomerulosclerosis, recurrent in transplanted kidney, second line therapy
Graft-versus-host disease o Acute
o Chronic, second line therapy
Heart transplantation in children less than 40 months of age, ABO incompatible, second line therapy
Hereditary hemochromatosis
Hyperlipoproteinemia Hypertriglyceridemic pancreatitis, severe Hyperviscosity in hypergammaglobulinemia Idiopathic dilated cardiomyopathy, NYHA class II-IV, via IA
Inflammatory bowel disease, via adsorptive cytapheresis Liver transplantation, ABO incompatible
o Desensitized ABOi
o Living donor Lung transplantation, bronchiolitis obliterans syndrome Major hematopoietic stem cell transplant, ABO incompatible, second line
therapy o HPC(M) o HPC(A)
Multiple sclerosis, second line therapy
o Acute CNS inflammatory, demyelinating o Relapsing form with steroid resistant exacerbations
Myasthenia gravis, acute
Myeloma cast nephropathy, second line therapy

7 Medical Policy Update Bulletin: October 2019
Medical Policy Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Apheresis
(continued)
Nov. 1, 2019
degeneration, dry
Coagulation factor inhibitors, autoantibody via immunoadsorption (IA)
Hyperleukocytosis, symptomatic
Systemic lupus
erythematosus nephritis o Replaced:
“ABO incompatible liver
transplantation, desensitized ABOi, deceased donor” with “liver transplantation,
ABO incompatible: desensitized ABOi, living
donor”
“Graft-versus-host disease: acute or chronic, skin and non-
skin” with “graft-versus-host disease: acute or chronic”
“Hyperviscosity in
monoclonal gammopathies” with “hyperviscosity in
hypergammaglobulinemia”
“Myasthenia gravis” with
“myasthenia gravis, acute”
“Sickle cell disease: primary or secondary
stroke prevention” with “sickle cell disease:
stroke prevention”
“Vasculitis: Behçet’s
Neuromyelitis optica spectrum disorders (Devic’s syndrome), acute or
relapse, second line therapy N-methyl D-aspartate receptor antibody encephalitis Paraproteinemic polyneuropathies via Therapeutic Plasma Exchange
(TPE)
o Anti-MAG o Multifocal motor o IgG/IgA
o IgM Pediatric autoimmune neuropsychiatric disorders associated with
streptococcal infections (PANDAS exacerbation)
Peripheral vascular diseases Polycythemia vera; erythrocytosis Progressive multifocal leukoencephalopathy associated with natalizumab Pruritus due to hepatobiliary diseases
Renal transplantation, ABO compatible o Antibody mediated rejection
o Desensitization, living donor
Renal transplantation, ABO incompatible, second line therapy o Antibody mediated rejection
Rheumatoid arthritis, refractory, second line therapy
Sickle cell disease o Acute stroke or multiorgan failure o Acute chest syndrome, severe, second line therapy o Stroke prevention
o Prevention of transfusional iron overload Thrombotic microangiopathy, complement mediated
o MCP mutations
Thrombotic microangiopathy, Shiga toxin mediated o Absence of severe neurological symptoms
Thrombotic thrombocytopenic purpura
Vasculitis o Behcet’s disease (adsorptive cytapheresis) o Idiopathic PAN (TPE)
Voltage gated potassium channel antibodies-related conditions
Wilson’s disease, fulminant
Due to insufficient evidence of efficacy, therapeutic apheresis
including plasma exchange, plasmapheresis, or photopheresis is
8 Medical Policy Update Bulletin: October 2019
Medical Policy Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
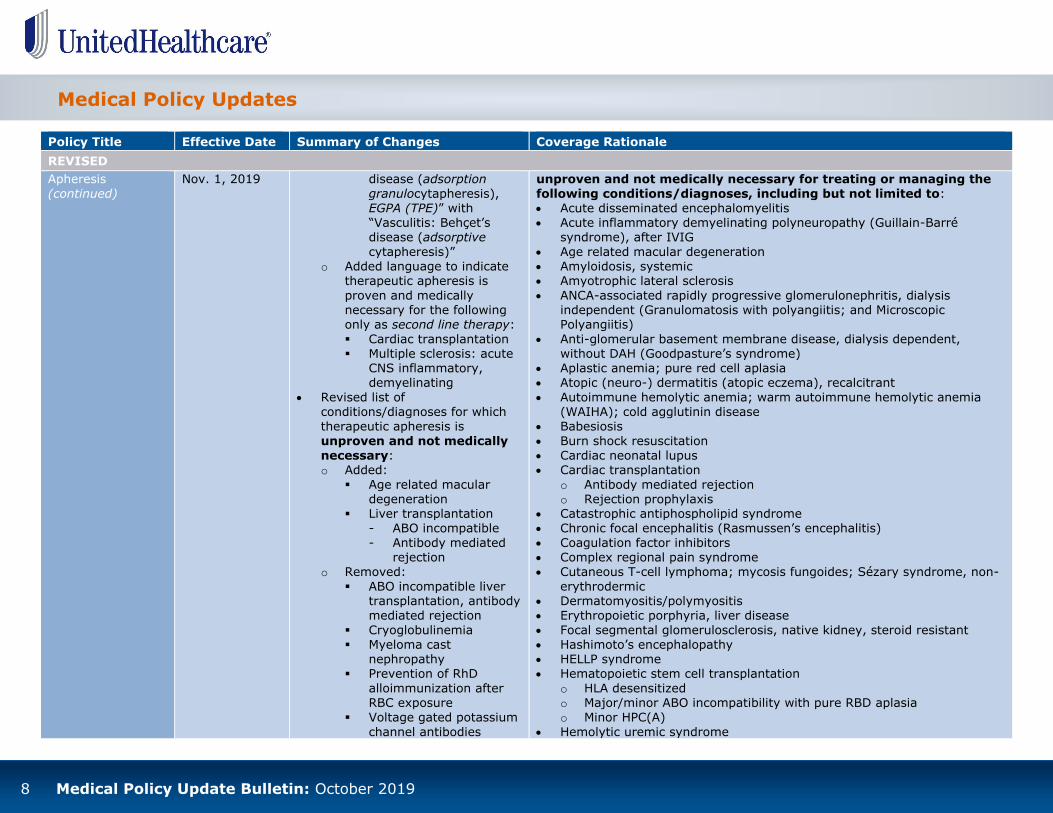
REVISED
Apheresis
(continued)
Nov. 1, 2019
disease (adsorption
granulocytapheresis), EGPA (TPE)” with “Vasculitis: Behçet’s disease (adsorptive
cytapheresis)” o Added language to indicate
therapeutic apheresis is
proven and medically necessary for the following only as second line therapy:
Cardiac transplantation Multiple sclerosis: acute
CNS inflammatory, demyelinating
Revised list of conditions/diagnoses for which
therapeutic apheresis is
unproven and not medically necessary: o Added:
Age related macular degeneration
Liver transplantation - ABO incompatible
- Antibody mediated rejection
o Removed:
ABO incompatible liver transplantation, antibody mediated rejection
Cryoglobulinemia Myeloma cast
nephropathy Prevention of RhD
alloimmunization after RBC exposure
Voltage gated potassium
channel antibodies
unproven and not medically necessary for treating or managing the
following conditions/diagnoses, including but not limited to: Acute disseminated encephalomyelitis Acute inflammatory demyelinating polyneuropathy (Guillain-Barré
syndrome), after IVIG
Age related macular degeneration Amyloidosis, systemic Amyotrophic lateral sclerosis
ANCA-associated rapidly progressive glomerulonephritis, dialysis independent (Granulomatosis with polyangiitis; and Microscopic Polyangiitis)
Anti-glomerular basement membrane disease, dialysis dependent, without DAH (Goodpasture’s syndrome)
Aplastic anemia; pure red cell aplasia Atopic (neuro-) dermatitis (atopic eczema), recalcitrant
Autoimmune hemolytic anemia; warm autoimmune hemolytic anemia (WAIHA); cold agglutinin disease
Babesiosis
Burn shock resuscitation Cardiac neonatal lupus Cardiac transplantation
o Antibody mediated rejection o Rejection prophylaxis
Catastrophic antiphospholipid syndrome Chronic focal encephalitis (Rasmussen’s encephalitis)
Coagulation factor inhibitors Complex regional pain syndrome Cutaneous T-cell lymphoma; mycosis fungoides; Sézary syndrome, non-
erythrodermic Dermatomyositis/polymyositis Erythropoietic porphyria, liver disease
Focal segmental glomerulosclerosis, native kidney, steroid resistant Hashimoto’s encephalopathy HELLP syndrome Hematopoietic stem cell transplantation
o HLA desensitized o Major/minor ABO incompatibility with pure RBD aplasia
o Minor HPC(A)
Hemolytic uremic syndrome

9 Medical Policy Update Bulletin: October 2019
Medical Policy Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Apheresis
(continued)
Nov. 1, 2019
o Replaced:
“Coagulation factor inhibitors, alloantibody (via IA), autoantibody (via TPE or IA)” with
“coagulation factor inhibitors”
“Hematopoietic stem cell
transplantation, major/minor HPC(A)” with “hematopoietic
stem cell transplantation, major/minor ABO incompatibility with pure
RBD aplasia, minor HPC(A)”
“Hyperleukocytosis,
prophylaxis” with “hyperleukocytosis”
“Hypertriglyceridemic
pancreatitis” with “hypertriglyceridemic pancreatitis, prevention”
“Immunoglobulin
nephropathy” with “IgA nephropathy (Berger’s Disease)”
“Multiple sclerosis (unless noted [in the policy] as proven)” with
“multiple sclerosis, chronic (unless noted [in the policy] as proven)”
“Red cell
alloimmunization, in pregnancy” with “red cell
alloimmunization,
prevention and
Hemophagocytic lymphohistiocytosis
Henoch-Schonlein purpura Heparin induced thrombocytopenia and thrombosis Hyperleukocytosis Hypertriglyceridemic pancreatitis, prevention
Immune thrombocytopenia IgA nephropathy (Berger’s Disease) Inflammatory bowel disease, via Extracorporeal Photopheresis
Lambert-Eaton myasthenic syndrome Liver transplantation
o ABO incompatible
o Antibody mediated rejection Lung transplantation
o Antibody mediated rejection o Desensitization
Malaria Multiple sclerosis, chronic (unless noted above as proven)
Nephrogenic systemic fibrosis
Neuromyelitis optica spectrum disorders, maintenance Overdose, venoms, and poisoning Paraneoplastic neurologic syndromes
Paraproteinemic polyneuropathy (unless noted above as proven) Pediatric autoimmune neuropsychiatric disorders associated with
streptococcal infections (Sydenham’s chorea, severe) Pemphigus vulgaris
Phytanic acid storage disease (Refsum’s disease) Post transfusion purpura Psoriasis
Red cell alloimmunization, prevention and treatment Renal transplantation, ABO compatible, desensitized, deceased donor Scleroderma (systemic sclerosis)
Sepsis with multiorgan failure Sickle cell disease (unless noted above as proven) Stiff-person syndrome Sudden sensorineural hearing loss
Systemic lupus erythematosus, severe Thrombocytosis
Thrombotic microangiopathy (unless noted above as proven)
Thyroid storm

10 Medical Policy Update Bulletin: October 2019
Medical Policy Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Apheresis
(continued)
Nov. 1, 2019 treatment”
“Sickle cell disease, non-acute (unless noted [in the policy] as proven)” with “sickle cell disease
(unless noted [in the policy] as proven)”
Supporting Information
Updated Clinical Evidence and References sections to reflect the most current information
Toxic epidermal necrolysis
Vasculitis (unless noted above as proven) Note: Refer to the Description of Services section for information regarding all apheresis-based procedures.
Bariatric Surgery
Dec. 1, 2019
Coverage Rationale Added language to indicate the
TransPyloric Shuttle (TPS) Device is unproven and not medically necessary for treating
obesity
Supporting Information Updated Description of Services,
Clinical Evidence, FDA, and References sections to reflect the most current information
The following bariatric surgical procedures are proven and medically
necessary for treating obesity: Gastric bypass (includes robotic-assisted gastric bypass)
o Laparoscopic adjustable gastric banding for individuals > 18 years of
age. Refer to the U.S. Food and Drug Administration (FDA) section
for additional information Gastric sleeve procedure
Vertical banded gastroplasty Biliopancreatic bypass Biliopancreatic diversion with duodenal switch
In adults, bariatric surgery using one of the procedures identified above for treating obesity is proven and medically necessary when ALL of the following criteria are met:
Class III obesity; or Class II obesity in the presence of one or more of the following co-
morbidities:
o Type 2 diabetes; or o Cardiovascular disease [e.g., stroke, myocardial infarction, poorly
controlled hypertension (systolic blood pressure greater than 140
mm Hg or diastolic blood pressure 90 mm Hg or greater, despite pharmacotherapy)]; or
o History of coronary artery disease with a surgical intervention such as coronary artery bypass or percutaneous transluminal coronary
angioplasty; or
o History of cardiomyopathy; or o Obstructive Sleep Apnea (OSA) confirmed on polysomnography with

11 Medical Policy Update Bulletin: October 2019
Medical Policy Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Bariatric Surgery
(continued)
Dec. 1, 2019
an AHI or RDI of >30
and The individual must also meet the following criteria:
o Both of the following: Completion of a preoperative evaluation that includes a detailed
weight history along with dietary and physical activity patterns; and
Psychosocial-behavioral evaluation to provide screening and
identification of risk factors or potential postoperative challenges that may contribute to a poor postoperative outcome
or
o Participation in a multi-disciplinary surgical preparatory regimen In Adolescents, the bariatric surgical procedures identified above are proven and medically necessary for treating obesity when ALL of the
following criteria are met: Class III obesity; or
Class II obesity in the presence of one or more of the following co-
morbidities: o Type 2 diabetes; or o Cardiovascular disease [e.g., stroke, myocardial infarction, poorly
controlled hypertension (systolic blood pressure greater than 140 mm Hg or diastolic blood pressure 90 mm Hg or greater, despite pharmacotherapy)]; or
o History of coronary artery disease with a surgical intervention such
as coronary artery bypass or percutaneous transluminal coronary angioplasty; or
o History of cardiomyopathy; or
o Obstructive Sleep Apnea confirmed on polysomnography with an AHI or RDI of >30
and
The individual must also receive an evaluation at, or in consultation with, a multidisciplinary center focused on the surgical treatment of severe childhood obesity. This may include adolescent centers that have received accreditation by the Metabolic and Bariatric Surgery
Accreditation and Quality Improvement Program (MBSAQIP) or can demonstrate similar programmatic components.
Revisional Bariatric Surgery using one of the procedures identified

12 Medical Policy Update Bulletin: October 2019
Medical Policy Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Bariatric Surgery
(continued)
Dec. 1, 2019 above is proven and medically necessary when due to a Technical
Failure or Major Complication from the initial bariatric procedure. The following procedures are unproven and not medically necessary for treating obesity due to insufficient evidence of efficacy:
Revisional Bariatric Surgery for any other indication than those listed above
Bariatric surgery as the primary treatment for any condition other than
obesity Bariatric surgical interventions for the treatment of obesity including but
not limited to:
o Transoral endoscopic surgery o Mini-gastric bypass (MGB) or laparoscopic mini-gastric bypass (LMGBP) o Gastric electrical stimulation with an implantable gastric stimulator
(IGS) o VBLOC® vagal blocking therapy
o Intragastric balloon
o Laparoscopic greater curvature plication, also known as total gastric vertical plication o Stomach aspiration therapy (AspireAssist®)
o Bariatric artery embolization (BAE) o Single-Anastomosis Duodenal Switch (also known as duodenal switch
with single anastomosis, or stomach intestinal pylorus sparing surgery [SIPS])
o TransPyloric Shuttle (TPS) Device Gastrointestinal liners (EndoBarrier®) are investigational, unproven
and not medically necessary for treating obesity due to lack of U.S. Food and Drug Administration (FDA) approval, and insufficient evidence of efficacy.
Epidural Steroid and Facet
Injections for Spinal Pain
Dec. 1, 2019
Coverage Rationale Added coverage criteria for
Epidural Steroid Injections (ESI) for treating lumbar radicular pain caused by spinal stenosis, disc
herniation or degenerative changes in the vertebrae
Note: This policy addresses Epidural Steroid Injections (ESI) of the lumbar spine only. The policy does not address Epidural Steroid Injections of the
cervical or thoracic spine, nor does it address injections for obstetrical or surgical anesthetic. The policy addresses Facet Joint Injections of multiple sites and is not limited to Facet Joint Injections of the lumbar spine.
The following are proven and medically necessary:

13 Medical Policy Update Bulletin: October 2019
Medical Policy Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Epidural Steroid
and Facet Injections for Spinal Pain (continued)
Dec. 1, 2019 requiring:
o The pain is associated with symptoms of nerve root irritation and/or low back pain due to disc extrusions
and/or contained herniations; and
o The pain is unresponsive to
Conservative Treatment, including but not limited to pharmacotherapy, exercise
or physical therapy Replaced language indicating
“therapeutic Facet Joint Injection (FJI) is unproven and not
medically necessary for treating chronic spinal pain” with
“therapeutic Facet Joint Injection
(FJI) and/or facet nerve block (i.e., medial branch block) are unproven and not medically
necessary for treating chronic spinal pain”
Definitions Added definition of:
o Facet Joint Injections (FJIs) o Facet Nerve Block o Medial Branch Block
Supporting Information Updated Clinical Evidence and
References sections to reflect the
most current information
Epidural Steroid Injections (ESI) for treating lumbar radicular pain
caused by spinal stenosis, disc herniation, degenerative changes in the vertebrae or for the short-term management of low back pain when the following criteria are met: o The pain is associated with symptoms of nerve root irritation and/or
low back pain due to disc extrusions and/or contained herniations; and
o The pain is unresponsive to Conservative Treatment, including but
not limited to pharmacotherapy, exercise or physical therapy Diagnostic Facet Joint Injection (FJI) and/or facet nerve block (i.e.,
medial branch block) to localize the source of pain to the facet joint in
persons with spinal pain The following are unproven and not medically necessary due to insufficient evidence of efficacy:
The use of ultrasound guidance for ESIs and FJIs ESI for all other indications of the lumbar spine not included above
Therapeutic Facet Joint Injection (FJI) and/or facet nerve block (i.e.,
medial branch block) for treating chronic spinal pain Epidural Steroid Injection Limitations
A maximum of three (3) ESI (regardless of level, location, or side) in a year will be considered medically necessary when criteria (indications for coverage) are met for each injection
A session is defined as one date of service in which ESI injection(s) are performed
A year is defined as the 12-month period starting from the date of
service of the first approved injection

14 Medical Policy Update Bulletin: October 2019
Medical Policy Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Genetic Testing for
Hereditary Cancer
Oct. 1, 2019
Notice of Revision: The following
summary of changes has been modified. Revisions to the previous policy update announcement are outlined in red below. Please take
note of the additional updates implemented on Oct. 1, 2019.
Coverage Rationale Simplified content
Hereditary Breast and Ovarian
Cancer (BRCA1/BRCA2) Revised list of proven and
medically necessary indications for:
o Men with a personal history of prostate cancer
o Women with a personal
history of Breast Cancer o Individuals without a
personal history of a related
cancer
Multi-Gene Hereditary Cancer Panel Testing Criteria Revised coverage
guidelines/criteria for individuals: o With an indication for testing
for hereditary Breast and Ovarian Cancer
o With an indication for testing
for hereditary colorectal cancer
o Without an indication for testing for hereditary Breast
and Ovarian cancer or colorectal cancer
Documentation Requirements
Removed 0104U from the list of
Genetic counseling is strongly recommended prior to these tests in order to
inform persons being tested about the advantages and limitations of the test as applied to a unique person. Hereditary Breast and Ovarian Cancer (BRCA1/BRCA2)
Genetic testing for BRCA1 and BRCA2 for individuals with a personal history of a related cancer is proven and medically necessary in the
following situations: Individuals with a BRCA 1/2 pathogenic mutation detected in tumor
tissue; or
Individuals with a personal history of pancreatic cancer; or Men with a personal history of Breast Cancer; or Men with a personal history of prostate cancer in any of the following
situations:
o At least one Close Blood Relative who has a BRCA1 or BRCA2 mutation; or
o Metastatic prostate cancer; or
o High risk prostate cancer (Gleason Score at least 7) with at least one Close Blood Relative with a BRCA-Related Cancer; or
o At least two Close Blood Relatives with BRCA-Related Cancer; or
o Ashkenazi Jewish ancestry; or o An unknown or Limited Family History
Women with a personal history of Ovarian Cancer; or Women with a personal history of Breast Cancer in any of the following
situations: o Metastatic Breast Cancer; or o Breast Cancer diagnosed at age 45 or younger; or
o An additional Breast Cancer primary (prior diagnosis or bilateral cancer); or
o Triple-Negative Breast Cancer diagnosed at age 60 or younger; or
o At least one Close Blood Relative who has a BRCA1 or BRCA2 mutation; or
o Ashkenazi Jewish ancestry; or o At least one Close Blood Relative with a BRCA-Related Cancer; or
o An unknown or Limited Family History Genetic testing for BRCA1 and BRCA2 for individuals without a
personal history of a related cancer is proven and medically necessary in the following situations:

15 Medical Policy Update Bulletin: October 2019
Medical Policy Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Genetic Testing for
Hereditary Cancer (continued)
Oct. 1, 2019
CPT codes with associated
documentation requirements (quarterly code edit)
Applicable Codes Updated list of applicable CPT
codes for multi-gene panel to reflect quarterly code edits: o Added 0129U, 0130U,
0131U, 0132U, 0133U, 0134U, 0135U, and 0138U
o Removed 0104U
Definitions Added definition of:
o BRCA-Related Cancers o Multi-Gene Panel
o Panel Modified definition of:
o Lynch Syndrome-Associated
Cancer
Supporting Information Updated Description of Services,
Clinical Evidence, CMS, and References sections to reflect the most current information
A known BRCA1/BRCA2 mutation in a Close Blood Relative; or
At least two Close Blood Relatives with a BRCA-Related Cancer; or Ashkenazi Jewish ancestry and at least one Close Blood Relative with a
BRCA-Related Cancer
Genetic testing for BRCA1 and/or BRCA2 is unproven and not medically necessary for all other indications including: Screening for cancer risk for individuals not listed in the proven
indications above; or Risk assessment of other cancers; or Confirmation of direct to consumer genetic testing without meeting any
of the proven indications above Multi-Gene Hereditary Cancer Panel Testing Criteria
Genetic testing with a Multi-Gene hereditary cancer Panel in individuals with an indication for testing for hereditary Breast and Ovarian cancer is proven and medically necessary if all of the
following criteria are met: The suspected hereditary cancer syndromes can be diagnosed by testing
of two or more genes included in the specific hereditary cancer Panel;
and The individual meets at least one of the criteria for Hereditary Breast and
Ovarian Cancer (BRCA1/BRCA2) (see above section); and The individual has a family history or personal history that is strongly
suggestive of more than one hereditary cancer syndrome including at least one of the following: o A personal history of at least two different cancers (e.g., Breast and
Ovarian); or o A personal history of cancer diagnosed at age 40 or younger; or o A personal history of cancer and at least one Close Blood Relative
with a cancer associated with Lynch Syndrome; or o At least one Close Blood Relative diagnosed with a BRCA-Related
Cancer at age 40 or younger; or o At least three Close Blood Relatives diagnosed with any cancer
Genetic testing with a Multi-Gene hereditary cancer Panel in individuals with an indication for testing for hereditary colorectal
cancer is proven and medically necessary in the following situations: The suspected hereditary cancer syndromes can be diagnosed by testing
16 Medical Policy Update Bulletin: October 2019
Medical Policy Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
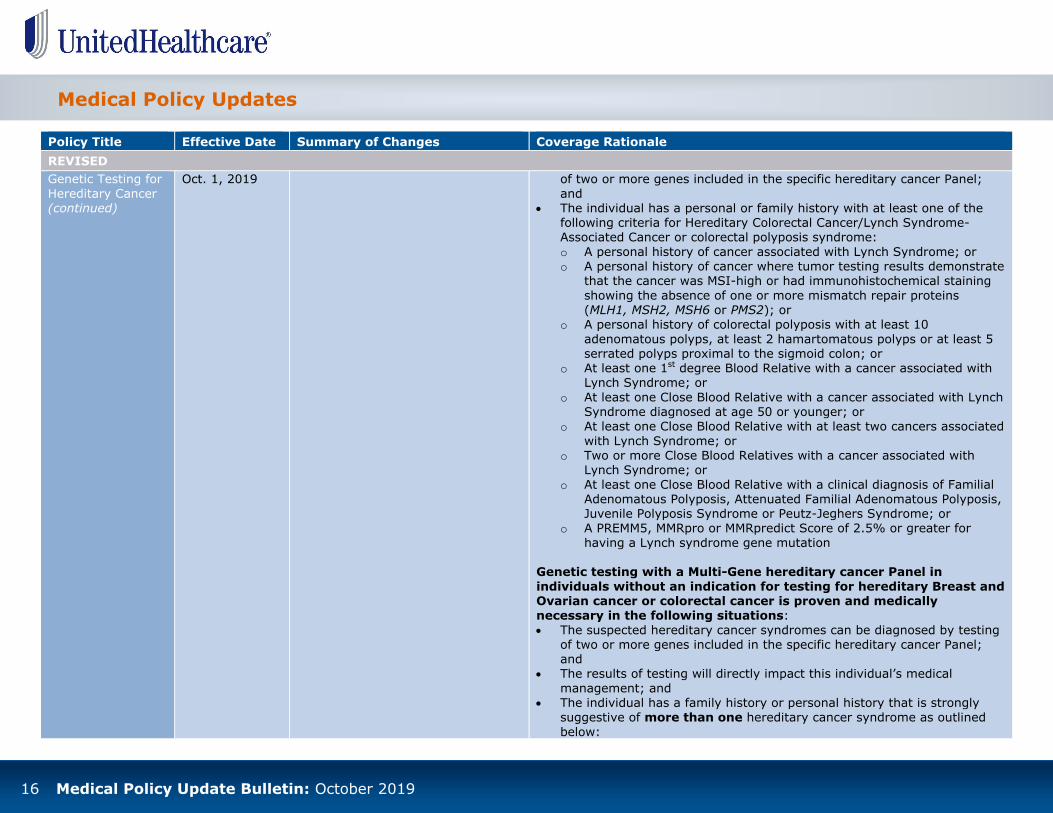
REVISED
Genetic Testing for
Hereditary Cancer (continued)
Oct. 1, 2019
of two or more genes included in the specific hereditary cancer Panel;
and The individual has a personal or family history with at least one of the
following criteria for Hereditary Colorectal Cancer/Lynch Syndrome-Associated Cancer or colorectal polyposis syndrome:
o A personal history of cancer associated with Lynch Syndrome; or o A personal history of cancer where tumor testing results demonstrate
that the cancer was MSI-high or had immunohistochemical staining
showing the absence of one or more mismatch repair proteins (MLH1, MSH2, MSH6 or PMS2); or
o A personal history of colorectal polyposis with at least 10
adenomatous polyps, at least 2 hamartomatous polyps or at least 5 serrated polyps proximal to the sigmoid colon; or
o At least one 1st degree Blood Relative with a cancer associated with Lynch Syndrome; or
o At least one Close Blood Relative with a cancer associated with Lynch Syndrome diagnosed at age 50 or younger; or
o At least one Close Blood Relative with at least two cancers associated
with Lynch Syndrome; or o Two or more Close Blood Relatives with a cancer associated with
Lynch Syndrome; or
o At least one Close Blood Relative with a clinical diagnosis of Familial Adenomatous Polyposis, Attenuated Familial Adenomatous Polyposis, Juvenile Polyposis Syndrome or Peutz-Jeghers Syndrome; or
o A PREMM5, MMRpro or MMRpredict Score of 2.5% or greater for
having a Lynch syndrome gene mutation Genetic testing with a Multi-Gene hereditary cancer Panel in
individuals without an indication for testing for hereditary Breast and Ovarian cancer or colorectal cancer is proven and medically necessary in the following situations:
The suspected hereditary cancer syndromes can be diagnosed by testing of two or more genes included in the specific hereditary cancer Panel; and
The results of testing will directly impact this individual’s medical
management; and The individual has a family history or personal history that is strongly
suggestive of more than one hereditary cancer syndrome as outlined
below:

17 Medical Policy Update Bulletin: October 2019
Medical Policy Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Genetic Testing for
Hereditary Cancer (continued)
Oct. 1, 2019
o A personal history of at least two different cancers (e.g., Breast and
colon); or o A personal history of cancer diagnosed at age 40 or younger; or o A personal history of cancer and at least one Close Blood Relative
with a cancer associated with Lynch Syndrome; or
o At least one Close Blood Relative diagnosed with a BRCA-Related Cancer at age 40 or younger; or
o At least three Close Blood Relatives diagnosed with any cancer
Genetic testing with a Multi-Gene hereditary cancer Panel in individuals diagnosed with cancer at age 18 or younger is proven and
medically necessary. Multi-Gene hereditary cancer Panels are unproven and not medically necessary for all other indications.
Omnibus Codes
Dec. 1, 2019
Coverage Rationale
Revised coverage guidelines for:
Sinus tarsi implant (CPT code 0335T and HCPCS code
S2117) o Updated list of applicable
codes; added S2117
Electroretinogram (CPT codes
0509T and 92274) o Added language to indicate
multifocal electroretinogram
(mfERG) is proven and medically necessary for chloroquine (CQ) and
hydroxychloroquine (HCQ) retinopathy screening
o Replaced language indicating “multifocal electroretinogram
(mfERG) is unproven and not medically necessary due to insufficient evidence of
safety and/or efficacy” with “multifocal electroretinogram
Refer to the policy for complete details on the coverage guidelines for
Omnibus Codes.

18 Medical Policy Update Bulletin: October 2019
Medical Policy Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Omnibus Codes
(continued)
Dec. 1, 2019 (mfERG) is unproven and not
medically necessary for all other indications [not listed as proven and medically necessary] due to
insufficient evidence of safety and/or efficacy”
Instrument-based ocular
photoscreening (CPT codes 99174 and 99177) o Updated language pertaining
to age requirements to indicate instrument-based ocular photoscreening is proven and medically
necessary for one of the following:
As a mass screening
instrument for children 1-5 years of age (ends on 6th birthday)
In individuals 6 years of age and older who are developmentally delayed and are unable or
unwilling to cooperate with routine visual acuity screening
Supporting Information Updated Clinical Evidence and
References sections to reflect the
most current information
Vagus and External
Trigeminal Nerve Stimulation
Dec. 1, 2019
Title Change
Previously titled Vagus Nerve Stimulation
Coverage Rationale
Revised coverage criteria for proven and medically necessary
Implantable vagus nerve stimulators are proven and medically
necessary for treating epilepsy in individuals with ALL of the following (see below for implants that allow detection and stimulation of increased heart rate):
Medically refractory epileptic seizures with failure of two or more trials of single or combination antiepileptic drug therapy or intolerable side effects

19 Medical Policy Update Bulletin: October 2019
Medical Policy Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Vagus and External
Trigeminal Nerve Stimulation (continued)
Dec. 1, 2019
use of implantable vagus nerve
stimulators for treating epilepsy; replaced criterion requiring “the individual is not a surgical candidate or has failed a surgical
intervention” with “the individual is not a candidate for epilepsy surgery or has failed epilepsy
surgery” Revised list of unproven and not
medically necessary indications:
o Added external or transcutaneous (nonimplantable) trigeminal nerve stimulation devices
(e.g., Monarch® eTNS System, Cefaly®) for
preventing or treating all
conditions, including but not limited to: Attention deficit
hyperactivity disorder (ADHD)
Depression Epilepsy
Headache o Updated list of examples of
vagus nerve stimulation
implants that allow detection and stimulation of increased heart rate; added “SenTiva™
Model 1000”
Supporting Information Updated Description of Services,
Clinical Evidence, FDA, CMS, and
References sections to reflect the most current information
of antiepileptic drug therapy; and
The individual is not a candidate for epilepsy surgery or has failed epilepsy surgery; and
No history of left or bilateral cervical vagotomy. The U.S. Food and Drug Administration (FDA) identifies a history of left or bilateral cervical
vagotomy as a contraindication to vagus nerve stimulation Implantable vagus nerve stimulators are unproven and not medically necessary for treating ALL other conditions due to insufficient
evidence of efficacy. These conditions include but are not limited to: Alzheimer's disease
Anxiety disorder Autism spectrum disorder Back and neck pain Bipolar disorder
Bulimia Cerebral palsy
Chronic pain syndrome
Cluster headaches Depression Fibromyalgia
Heart failure Migraines Morbid obesity Narcolepsy
Obsessive-compulsive disorder Paralysis agitans Sleep disorders
Tourette's syndrome The following are unproven and not medically necessary due to
insufficient evidence of efficacy: Vagus nerve stimulation implants that allow detection and stimulation of
increased heart rate (e.g., AspireSR™ Model 106, SenTiva™ Model 1000) for treating epilepsy
Transcutaneous (nonimplantable) vagus nerve stimulation (e.g., gammaCore® for headaches) for preventing or treating all indications
External or transcutaneous (nonimplantable) trigeminal nerve stimulation
devices (e.g., Monarch® eTNS System, Cefaly®) for preventing or

20 Medical Policy Update Bulletin: October 2019
Medical Policy Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Vagus and External
Trigeminal Nerve Stimulation (continued)
Dec. 1, 2019 treating all conditions including but not limited to:
o Attention deficit hyperactivity disorder (ADHD) o Depression o Epilepsy o Headache
Note: For vagus nerve blocking for the treatment of obesity, refer to the Medical Policy titled Bariatric Surgery.

21 Medical Policy Update Bulletin: October 2019
Medical Benefit Drug Policy Updates
Policy Title Effective Date Coverage Rationale
NEW
Cimzia®
(Certolizumab Pegol)
Oct. 1, 2019
TBD
Notice of Implementation Delay: This policy will not be effective on Oct. 1, 2019, as previously announced.
Implementation of the new Medical Benefit Drug Policy has been postponed until further notice; complete details will be provided in a future edition of the Medical Policy Update Bulletin. This policy refers to Cimzia (certolizumab pegol) injection. Cimzia (certolizumab pegol) for self-administered
subcutaneous injection is obtained under the pharmacy benefit. Cimzia is proven and/or medically necessary for the treatment of:
Crohn’s Disease (CD) when all of the following criteria are met: For initial therapy, all of the following:
o Diagnosis of moderately to severely active Crohn’s disease; and o Patient has had an inadequate response to conventional therapies (examples include anti-inflammatory
drugs, corticosteroids, or oral immunosuppressive agents); and o Physician attestation that the patient or caregiver are not competent to administer Cimzia FDA labeled for
self-administration; physician must submit explanation; and o Cimzia is initiated and titrated according to US Food and Drug Administration labeled dosing for CD; and
o Patient is not receiving Cimzia in combination with either of the following:
Biologic DMARD [e.g., Actemra (tocilizumab), Enbrel (etanercept), Rituxan (rituximab), Orencia (abatacept)]
Janus kinase inhibitor [e.g., Xeljanz (tofacitinib)]
and o Initial authorization will be issued for 12 months.
For continuation of therapy, all of the following: o Documentation of positive clinical response; and
o Physician attestation that the patient or caregiver are not competent to administer Cimzia FDA labeled for self-administration; physician must submit explanation; and
o Cimzia is initiated and titrated according to US Food and Drug Administration labeled dosing for CD; and
o Patient is not receiving Cimzia in combination with either of the following: Biologic DMARD [e.g., Actemra (tocilizumab), Enbrel (etanercept), Rituxan (rituximab), Orencia
(abatacept)]
Janus kinase inhibitor [e.g., Xeljanz (tofacitinib)] and
o Authorization will be issued for 12 months.
Rheumatoid Arthritis (RA) when all of the following criteria are met: For initial therapy, all of the following:
o Diagnosis of moderately to severely active rheumatoid arthritis; and
o Physician attestation that the patient or caregiver are not competent to administer Cimzia FDA labeled for

22 Medical Policy Update Bulletin: October 2019
Medical Benefit Drug Policy Updates
Policy Title Effective Date Coverage Rationale
NEW
Cimzia®
(Certolizumab Pegol) (continued)
Oct. 1, 2019
TBD
self-administration; physician must submit explanation; and
o Cimzia is initiated and titrated according to US Food and Drug Administration labeled dosing for RA; and o Patient is not receiving Cimzia in combination with either of the following:
Biologic DMARD [e.g., Actemra (tocilizumab), Enbrel (etanercept), Rituxan (rituximab), Orencia (abatacept)]
Janus kinase inhibitor [e.g., Xeljanz (tofacitinib)] and
o Initial authorization will be issued for 12 months.
For continuation of therapy, all of the following: o Documentation of positive clinical response; and o Physician attestation that the patient or caregiver are not competent to administer Cimzia FDA labeled for
self-administration; physician must submit explanation; and o Cimzia is initiated and titrated according to US Food and Drug Administration labeled dosing for RA; and o Patient is not receiving Cimzia in combination with either of the following:
Biologic DMARD [e.g., Actemra (tocilizumab), Enbrel (etanercept), Rituxan (rituximab), Orencia
(abatacept)] Janus kinase inhibitor [e.g., Xeljanz (tofacitinib)]
and
o Authorization will be issued for 12 months. Psoriatic Arthritis (PsA) when all of the following criteria are met:
For initial therapy, all of the following: o Diagnosis of active psoriatic arthritis; and o Physician attestation that the patient or caregiver are not competent to administer Cimzia FDA labeled for
self- administration; physician must submit explanation; and
o Cimzia is initiated and titrated according to US Food and Drug Administration labeled dosing for PsA; and o Patient is not receiving Cimzia in combination with either of the following:
Biologic DMARD [e.g., Actemra (tocilizumab), Enbrel (etanercept), Rituxan (rituximab), Orencia
(abatacept)] Janus kinase inhibitor [e.g., Xeljanz (tofacitinib)] Phosphodiesterase 4 (PDE4) inhibitor [e.g., Otezla (apremilast)]
and o Initial authorization will be issued for 12 months.
For continuation of therapy, all of the following: o Documentation of positive clinical response; and
o Physician attestation that the patient or caregiver are not competent to administer Cimzia FDA labeled for self- administration; physician must submit explanation; and
o Cimzia is initiated and titrated according to US Food and Drug Administration labeled dosing for PsA; and
o Patient is not receiving Cimzia in combination with either of the following:

23 Medical Policy Update Bulletin: October 2019
Medical Benefit Drug Policy Updates
Policy Title Effective Date Coverage Rationale
NEW
Cimzia®
(Certolizumab Pegol) (continued)
Oct. 1, 2019
TBD
Biologic DMARD [e.g., Actemra (tocilizumab), Enbrel (etanercept), Rituxan (rituximab), Orencia
(abatacept)] Janus kinase inhibitor [e.g., Xeljanz (tofacitinib)] Phosphodiesterase 4 (PDE4) inhibitor [e.g., Otezla (apremilast)] and
o Authorization will be issued for 12 months.
Ankylosing Spondylitis (AS) and non-radiographic Axial Spondyloarthritis (nr-axSpA) when all of the
following criteria are met: For initial therapy, all of the following:
o Diagnosis of active ankylosing spondylitis or non-radiographic axial spondyloarthritis; and
o Physician attestation that the patient or caregiver are not competent to administer Cimzia FDA labeled for self- administration; physician must submit explanation; and
o Cimzia is initiated and titrated according to US Food and Drug Administration labeled dosing for AS or nr-axSpA; and
o Patient is not receiving Cimzia in combination with either of the following: Biologic DMARD [e.g., Actemra (tocilizumab), Enbrel (etanercept), Rituxan (rituximab), Orencia
(abatacept)]
Janus kinase inhibitor [e.g., Xeljanz (tofacitinib)] Phosphodiesterase 4 (PDE4) inhibitor [e.g., Otezla (apremilast)] and
o Initial authorization will be issued for 12 months. For continuation of therapy, all of the following:
o Documentation of positive clinical response; and o Physician attestation that the patient or caregiver are not competent to administer Cimzia FDA labeled for
self- administration; physician must submit explanation; and o Cimzia is initiated and titrated according to US Food and Drug Administration labeled dosing for AS or nr-
axSpA; and
o Patient is not receiving Cimzia in combination with either of the following: Biologic DMARD [e.g., Actemra (tocilizumab), Enbrel (etanercept), Rituxan (rituximab), Orencia
(abatacept)]
Janus kinase inhibitor [e.g., Xeljanz (tofacitinib)] Phosphodiesterase 4 (PDE4) inhibitor [e.g., Otezla (apremilast)] and
o Authorization will be issued for 12 months.
Plaque Psoriasis (PS) when all of the following criteria are met:
For initial therapy, all of the following:
o Diagnosis of moderate to severe plaque psoriasis; and

24 Medical Policy Update Bulletin: October 2019
Medical Benefit Drug Policy Updates
Policy Title Effective Date Coverage Rationale
NEW
Cimzia®
(Certolizumab Pegol) (continued)
Oct. 1, 2019
TBD
o Physician attestation that the patient or caregiver are not competent to administer Cimzia FDA labeled for
self- administration; physician must submit explanation; and o Cimzia is initiated and titrated according to US Food and Drug Administration labeled dosing for PS; and o Patient is not receiving Cimzia in combination with either of the following:
Biologic DMARD [e.g., Actemra (tocilizumab), Enbrel (etanercept), Rituxan (rituximab), Orencia
(abatacept)] Janus kinase inhibitor [e.g., Xeljanz (tofacitinib)] Phosphodiesterase 4 (PDE4) inhibitor [e.g., Otezla (apremilast)]
and o Initial authorization will be issued for 12 months.
For continuation of therapy, all of the following:
o Documentation of positive clinical response; and o Physician attestation that the patient or caregiver are not competent to administer Cimzia FDA labeled for
self- administration; physician must submit explanation; and o Cimzia is initiated and titrated according to US Food and Drug Administration labeled dosing for PS; and
o Patient is not receiving Cimzia in combination with either of the following: Biologic DMARD [e.g., Actemra (tocilizumab), Enbrel (etanercept), Rituxan (rituximab), Orencia
(abatacept)]
Janus kinase inhibitor [e.g., Xeljanz (tofacitinib)] Phosphodiesterase 4 (PDE4) inhibitor [e.g., Otezla (apremilast)] and
o Authorization will be issued for 12 months.
Krystexxa®
(Pegloticase)
Oct. 1, 2019
Krystexxa (pegloticase) is proven for the treatment of chronic gout refractory to conventional therapy.
Krystexxa (pegloticase) is medically necessary for the treatment of chronic gout when all of the following criteria are met:
For initial therapy, all of the following:
o One of the following:
History of at least 2 gout flares in the previous 12 months At least 1 gouty tophus Chronic gouty arthropathy and
o History of contraindication, intolerance, or treatment failure after 3 months of therapy (at the maximally medically appropriate dose) with both of the following: Zyloprim (allopurinol)
Uloric (febuxostat) and

25 Medical Policy Update Bulletin: October 2019
Medical Benefit Drug Policy Updates
Policy Title Effective Date Coverage Rationale
NEW
Krystexxa®
(Pegloticase) (continued)
Oct. 1, 2019 o One of the following:
Patient has a confirmed baseline serum uric acid of 6 mg/dL or greater prior to initiating Krystexxa despite conventional therapy; or
Both of the following: - Patient has a baseline serum uric acid less than 6 mg/dL
- Patient has at least 1 gouty tophus and
o Member has undertaken appropriate life style modifications (e.g., limiting of alcohol consumption and diet
modifications, discontinuing or changing medications known to cause gout attacks); and o Patient does not have glucose‐6‐phosphate dehydrogenase (G6PD) deficiency; and
o Prescribed by a rheumatologist; and o Dosing is in accordance with the United States Food and Drug Administration approved labeling; and
o Initial authorization will be for no more than 12 months.
For continuation therapy, all of the following:
o Patient has previously received treatment with Krystexxa; and o Patient has experienced a positive clinical response to Krystexxa (e.g., serum uric acid levels < 6mg/dL,
tophus reduction, etc); and o Patient has not experienced one of the following:
Pre-infusion serum uric acid concentration of > 6 mg/dL accompanied by an infusion reaction Pre-infusion serum uric acid concentration of > 6 mg/dL on two consecutive occasions and
o Member has undertaken appropriate life style modifications (e.g., limiting of alcohol consumption and diet modifications, discontinuing or changing medications known to cause gout attacks); and
o Prescribed by a rheumatologist; and
o Dosing is in accordance with the United States Food and Drug Administration approved labeling; and o Reauthorization will be for no more than 12 months.
Krystexxa (pegloticase) is unproven and not medically necessary for the treatment of asymptomatic
hyperuricemia.
Policy Title Effective Date Summary of Changes
UPDATED
Complement
Inhibitors (Soliris® & Ultomiris™)
Oct. 1, 2019 Applicable Codes
Updated list of applicable HCPCS codes to reflect quarterly code edits: o Replaced J3590 with J1303
o Removed C9052
26 Medical Policy Update Bulletin: October 2019
Medical Benefit Drug Policy Updates
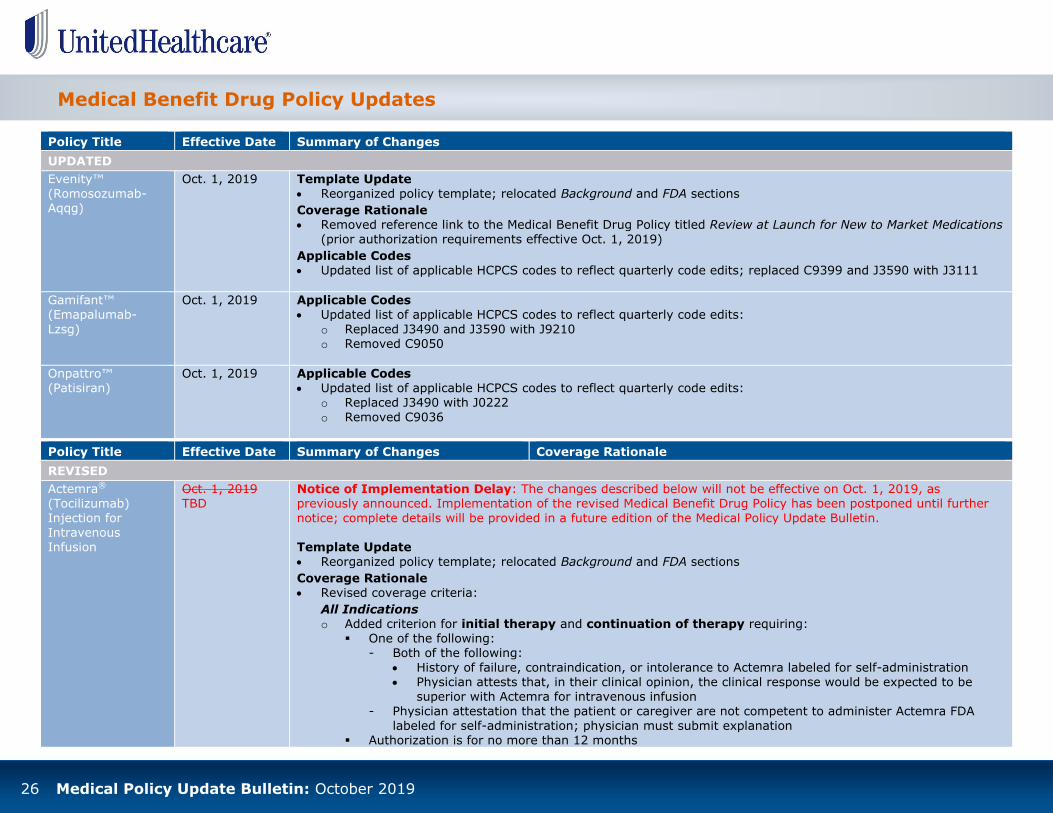
Policy Title Effective Date Summary of Changes
UPDATED
Evenity™
(Romosozumab-Aqqg)
Oct. 1, 2019
Template Update
Reorganized policy template; relocated Background and FDA sections
Coverage Rationale Removed reference link to the Medical Benefit Drug Policy titled Review at Launch for New to Market Medications
(prior authorization requirements effective Oct. 1, 2019)
Applicable Codes Updated list of applicable HCPCS codes to reflect quarterly code edits; replaced C9399 and J3590 with J3111
Gamifant™ (Emapalumab-
Lzsg)
Oct. 1, 2019 Applicable Codes Updated list of applicable HCPCS codes to reflect quarterly code edits:
o Replaced J3490 and J3590 with J9210 o Removed C9050
Onpattro™ (Patisiran)
Oct. 1, 2019 Applicable Codes Updated list of applicable HCPCS codes to reflect quarterly code edits:
o Replaced J3490 with J0222
o Removed C9036
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Actemra®
(Tocilizumab)
Injection for Intravenous Infusion
Oct. 1, 2019 TBD
Notice of Implementation Delay: The changes described below will not be effective on Oct. 1, 2019, as previously announced. Implementation of the revised Medical Benefit Drug Policy has been postponed until further
notice; complete details will be provided in a future edition of the Medical Policy Update Bulletin. Template Update
Reorganized policy template; relocated Background and FDA sections
Coverage Rationale Revised coverage criteria:
All Indications o Added criterion for initial therapy and continuation of therapy requiring:
One of the following: - Both of the following:
History of failure, contraindication, or intolerance to Actemra labeled for self-administration Physician attests that, in their clinical opinion, the clinical response would be expected to be
superior with Actemra for intravenous infusion
- Physician attestation that the patient or caregiver are not competent to administer Actemra FDA
labeled for self-administration; physician must submit explanation Authorization is for no more than 12 months

27 Medical Policy Update Bulletin: October 2019
Medical Benefit Drug Policy Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Actemra®
(Tocilizumab) Injection for Intravenous Infusion
(continued)
Oct. 1, 2019
TBD
For continuation of therapy: Patient has previously received Actemra injection for intravenous infusion
Rheumatoid Arthritis o Added criterion for initial therapy requiring history of failure, contraindication, or intolerance to two of the
following preferred products (document drug, date, and duration of trial): Cimzia (certolizumab)
Humira (adalimumab) Simponi (golimumab) Olumiant (baricitinib)
Rinvoq (upadacitinib) Xeljanz/Xeljanz XR (tofacitinib)
Supporting Information
Updated References section to reflect the most current information
Benlysta® (Belimumab)
Oct. 1, 2019 TBD
Notice of Implementation Delay: The changes described below will not be effective on Oct. 1, 2019, as previously announced. Implementation of the revised Medical Benefit Drug Policy has been postponed until further notice; complete details will be provided in a future edition of the Medical Policy Update Bulletin.
Template Update Reorganized policy template; relocated Background and FDA sections
Coverage Rationale
Replaced language indicating “Benlysta (belimumab) is proven and medically necessary for the treatment of systemic lupus erythematosus when all of the [listed] criteria are met” with “Benlysta (belimumab) is proven and medically necessary for the treatment of active systemic lupus erythematosus when all of the [listed]
criteria are met” Revised criteria for initial therapy:
o Added criterion requiring: One of the following:
- Both of the following: History of failure, contraindication, or intolerance to Benlysta labeled for self-administration Physician attests that, in their clinical opinion, the clinical response would be expected to be
superior with Benlysta for intravenous infusion - Physician attestation that the patient or caregiver is not competent to administer Benlysta FDA
labeled for self-administration; physician must submit explanation
Initial authorization is for no more than 12 months o Replaced criterion requiring:
“Diagnosis of active systemic lupus erythematosus” with “diagnosis of active systemic lupus
erythematosus without severe active lupus nephritis or severe active central nervous system lupus”
“Currently receiving at least one standard of care treatment for active systemic lupus erythematosus”
28 Medical Policy Update Bulletin: October 2019
Medical Benefit Drug Policy Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Benlysta®
(Belimumab) (continued)
Oct. 1, 2019
TBD
with “currently receiving at least one standard of care treatment for active systemic lupus
erythematosus that is not a biologic or intravenous cyclophosphamide” Added criteria for continuation of therapy
Clotting Factors, Coagulant Blood Products & Other
Hemostatics
Oct. 1, 2019 Coverage Rationale Revised list of applicable long-
acting Factor VIII (recombinant)
products; added Esperoct® [antihemophilic factor (recombinant), glycopegylated-
exei] Added language to indicate
Esperoct [antihemophilic factor (recombinant), glycopegylated-
exei] is not medically necessary for treatment of hemophilia A for the following:
o Routine prophylactic treatment
o Perioperative management
of surgical bleeding o Treatment of bleeding
episodes
Supporting Information
Updated Clinical Evidence, FDA, CMS, and References sections to reflect the most current
information
Refer to the policy for complete details on the coverage guidelines for Clotting Factors, Coagulant Blood Products & Other Hemostatics.
Infliximab (Remicade®, Inflectra™,
Renflexis™)
Oct. 1, 2019
Template Update Reorganized policy template;
relocated Background and FDA
sections
Coverage Rationale Added language to indicate
Inflectra™ (infliximab-dyyb) is a
preferred infliximab product;
coverage will be provided for Inflectra™ (infliximab-dyyb)
This policy refers to the following infliximab products: Remicade® (infliximab) Inflectra™ (infliximab-dyyb)
Renflexis™ (infliximab-abda) Preferred Product
Medical Necessity Plans
Remicade® (infliximab) and Inflectra™ (infliximab-dyyb) are the preferred
infliximab products. Coverage will be provided for Remicade® or Inflectra™ (infliximab-dyyb) contingent on the coverage criteria in the Diagnosis-
29 Medical Policy Update Bulletin: October 2019
Medical Benefit Drug Policy Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Infliximab
(Remicade®, Inflectra™, Renflexis™) (continued)
Oct. 1, 2019
contingent on the coverage
criteria in the Diagnosis-Specific Criteria section of the policy
Revised preferred product criteria to indicate treatment
with Renflexis™ (infliximab-abda) or another infliximab biosimilar is medically necessary
for the indications specified in the policy when treatment with Remicade and Inflectra is
contraindicated or has failed
Applicable Codes Added ICD-10 diagnosis codes
H20.10, H20.11, H20.12,
H20.13, H20.821, H20.822, H20.823, H20.829, H30.001,
H30.002, H30.003, H30.009,
H30.011, H30.012, H30.013, H30.019, H30.021, H30.022, H30.023, H30.029, H30.031,
H30.032, H30.033, H30.039, H30.041, H30.042, H30.043, H30.049, H30.101, H30.102, H30.103, H30.109, H30.111,
H30.112, H30.113, H30.119, H30.121, H30.122, H30.123, H30.129, H30.131, H30.132,
H30.133, H30.139, H30.20, H30.21, H30.22, H30.23, H30.811, H30.812, H30.813,
H30.819, H30.891, H30.892, H30.893, H30.899, H30.90, H30.91, H30.92, H30.93, H35.021, H35.022, H35.023,
H35.029, H35.061, H35.062, H35.063, H35.069, H44.111,
H44.112, H44.113, and H44.119
Specific Criteria section.
Coverage for Renflexis™ (infliximab-abda) will be provided contingent on the criteria in this section and the coverage criteria in the Diagnosis-Specific Criteria section. In order to continue coverage, members already on
Renflexis™ (infliximab-abda) will be required to change therapy to Remicade® or Inflectra™ unless they meet the criteria in this section.
Preferred Product Criteria
Treatment with Renflexis™ (infliximab-abda), or other infliximab
biosimilar is medically necessary for the indications specified in this policy when BOTH the following criteria are met: One of the following:
o Both of the following:
History of a trial of at least 14 weeks of Remicade and Inflectra resulting in minimal clinical response to therapy and residual disease activity.
Physician attests that in their clinical opinion, the clinical response would be expected to be superior with Renflexis or other infliximab biosimilar product, than experienced with
Remicade or Inflectra. or
o Both of the following: History of intolerance, contraindication, or adverse event to
Remicade and Inflectra. Physician attests that in their clinical opinion, the same
intolerance, contraindication, or adverse event would not be
expected to occur with Renflexis or other infliximab biosimilar product.
and
Both of the following o Patient has not had a loss of a favorable response after established
maintenance therapy with Remicade or other infliximab biosimilar product.
o Patient has not developed neutralizing antibodies to any infliximab biosimilar product that has led to an attenuation of efficacy of therapy.
Non-Medical Necessity Plans

30 Medical Policy Update Bulletin: October 2019
Medical Benefit Drug Policy Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Infliximab
(Remicade®, Inflectra™, Renflexis™) (continued)
Oct. 1, 2019
Any infliximab product is to be approved contingent on the coverage criteria
in the Diagnosis-Specific Criteria section. Diagnosis-Specific Criteria
“Infliximab” will be used to refer to all infliximab products. Infliximab is proven and medically necessary for the treatment of:
Ankylosing spondylitis when the following criterion is met:
o Diagnosis of ankylosing spondylitis (AS).
Crohn’s disease when ONE of the following criteria is met:
o Diagnosis of fistulizing Crohn’s disease (Crohn’s Disease Activity Index (CDAI) ≥ 220 and ≤ 400); or
o Both of the following: Diagnosis of moderately to severely active Crohn’s disease; and History of failure, contraindication, or intolerance to at least one
conventional therapy (e.g., corticosteroids, 6-mercaptopurine, azathioprine, methotrexate, etc.).
Noninfectious uveitis when BOTH of the following criteria are met: o Diagnosis of refractory noninfectious uveitis that is causing or
threatening vision loss (e.g., noninfectious uveitis associated with Behçet’s or Reiter’s syndromes); and
o History of failure, contraindication, or intolerance to all of the following: Topical corticosteroids; and
Systemic corticosteroids; and Immunosuppressive drugs (e.g., azathioprine, cyclosporine, or
methotrexate).
Plaque psoriasis when BOTH of the following criteria are met:
o Diagnosis of chronic severe plaque psoriasis (i.e., extensive and/or disabling); and
o Patient is a candidate for systemic therapy. Psoriatic arthritis when the following criterion is met:
o Diagnosis of psoriatic arthritis (PsA).
Rheumatoid arthritis when BOTH of the following criteria are met:

31 Medical Policy Update Bulletin: October 2019
Medical Benefit Drug Policy Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Infliximab
(Remicade®, Inflectra™, Renflexis™) (continued)
Oct. 1, 2019
o Diagnosis of moderately to severely active rheumatoid arthritis (RA);
and o One of the following:
Patient is receiving concurrent therapy with methotrexate. History of contraindication or intolerance to methotrexate.
Sarcoidosis when ALL of the following criteria are met:
o Diagnosis of sarcoidosis; and
o History of failure, contraindication, or intolerance to corticosteroids (e.g., prednisone, methylprednisolone); and
o History of failure, contraindication, or intolerance to one
immunosuppressant (e.g., methotrexate, cyclophosphamide, azathioprine).
Ulcerative colitis when BOTH of the following criteria are met:
o Diagnosis of moderately to severely active ulcerative colitis (UC); and
o History of failure, contraindication, or intolerance to at least one
conventional therapy (e.g., 6-mercaptopurine, aminosalicylate, azathioprine, corticosteroids).
Immune checkpoint inhibitor-related toxicities when BOTH of the following criteria are met: o Patient has recently received checkpoint inhibitor therapy [e.g.,
Keytruda (Pembrolizumab), Opdivo (Nivolumab)];and
o One of the following: Both of the following:
- Diagnosis of moderate (G2) or severe (G3-4)
immunotherapy-related diarrhea or colitis; and - History of failure, contraindication, or intolerance to
corticosteroids (e.g. methylprednisolone).
or Both of the following:
- Diagnosis of severe (G3-4) immunotherapy-related pneumonitis; and
- History of failure, contraindication, or intolerance to corticosteroids (e.g. methylprednisolone).
or
Both of the following:

32 Medical Policy Update Bulletin: October 2019
Medical Benefit Drug Policy Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Infliximab
(Remicade®, Inflectra™, Renflexis™) (continued)
Oct. 1, 2019
- Diagnosis of severe (G3) or life-threatening (G4)
immunotherapy-related acute renal failure/elevated serum creatinine; and
- Toxicity remains >G2 after 1 week of corticosteroids. or
Both of the following: - Diagnosis of severe (G3-4) immunotherapy-related uveitis;
and
- Toxicity remains after 1 week of high dose systemic corticosteroids.
or
Both of the following: - Diagnosis of life threatening (G4) immunotherapy-related
myocarditis, pericarditis, arrhythmias, or impaired ventricular function; and
- No improvement of toxicity within 24 hours of starting pulse-dose methylprednisolone.
or
Both of the following: - Diagnosis of severe immunotherapy-related inflammatory
arthritis; and
- No symptom improvement within 2 weeks of starting high-dose corticosteroids.
There may be other conditions that qualify as serious, rare diseases for
which the use of infliximab may be appropriate. Refer to the Benefit Considerations section of the policy for additional information.
Infliximab is unproven and not medically necessary for the treatment of: Still’s disease
Sjögren’s syndrome Graft-vs-host disease Myelodysplastic syndromes Undifferentiated spondyloarthropathy
Reiter’s syndrome Hidradenitis suppurativa
Wegener’s granulomatosis
Juvenile idiopathic arthritis (juvenile rheumatoid arthritis)

33 Medical Policy Update Bulletin: October 2019
Medical Benefit Drug Policy Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Infliximab
(Remicade®, Inflectra™, Renflexis™) (continued)
Oct. 1, 2019 Infliximab is unproven for the treatment of the above conditions because
statistically robust randomized controlled trials are needed to address the issue of whether infliximab has sufficient superiority in clinical efficacy compared to other available treatments to justify the inherent clinical risk in the use of a monoclonal antibody anti-tumor necrosis factor agent.
Ketalar®
(Ketamine) and Spravato™ (Esketamine)
Oct. 1, 2019
Coverage Rationale
Revised medical necessity criteria for the treatment of treatment-resistant depression
(TRD) with Spravato; replaced initial therapy criterion requiring “Spravato will be used in combination with a newly
initiated daily oral antidepressant that has not previously been tried” with
“Spravato will be initiated at the same time the member starts a new daily oral antidepressant
(one that has not previously been tried)”
This policy refers to the following ketamine products:
Ketalar (ketamine) Spravato (esketamine)
Spravato (Esketamine) Nasal Spray
Spravato is proven for the treatment of treatment-resistant
depression (TRD) when ALL of the following criteria are met:
Initial Therapy
Diagnosis for major depressive disorder (treatment-resistant) according to the current DSM (i.e., DSM-5), by a mental health professional; and
Patient has not experienced a clinically meaningful improvement after treatment with at least two different antidepressants of adequate dose, duration (at least 6 weeks), and adherence in the current depressive
episode (must document medications, doses, and durations); and Patient is to receive Spravato therapy in conjunction with another oral
antidepressant; and Provider and/or the provider’s healthcare setting is certified in the
Spravato REMS program; and Spravato dosing is in accordance with the United States Food and Drug
Administration approved labeling; and
Initial authorization will be for no longer than 12 weeks.
Continuation of Therapy
Patient has previously been treated with Spravato; and
Documentation demonstrating a positive clinical response from baseline (e.g., improved Montgomery-Asberg Depression Rating Scale [MADRS], clinical remission, response, etc.), as defined by the provider; and
Patient is to receive Spravato therapy in conjunction with another oral
antidepressant; and Provider and/or the provider’s healthcare setting is certified in the
Spravato REMS program; and
Spravato dosing is in accordance with the United States Food and Drug

34 Medical Policy Update Bulletin: October 2019
Medical Benefit Drug Policy Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Ketalar®
(Ketamine) and Spravato™ (Esketamine) (continued)
Oct. 1, 2019
Administration approved labeling; and
Authorization will be for no longer than 6 months.
Spravato is medically necessary for the treatment of treatment-resistant depression (TRD) when ALL of the following criteria are met:
Initial Therapy
Diagnosis of major depressive disorder (treatment-resistant), according to the current DSM (i.e., DSM-5), by a mental health professional; and
Prescribed by or in consultation with a psychiatrist; and Attestation of baseline scoring (prior to starting Spravato) on at least
one of the following clinical assessments has been completed:
o Baseline score on the 17-item Hamilton Rating Scale for Depression (HAMD17)
o Baseline score on the 16-item Quick Inventory of Depressive Symptomatology (QIDS-C16)
o Baseline score on the 10-item Montgomery-Asberg Depression Rating
Scale (MADRS) and
Patient has not experienced a clinically meaningful improvement after treatment with at least three different antidepressants or treatment regimens of adequate dose (maximally tolerated), duration (at least 8
weeks), and adherence in the current depressive episode o An antidepressant or treatment regimen would include any of the
following classes or combinations (document medication, dose, and duration):
Selective serotonin reuptake inhibitors (e.g., citalopram, fluoxetine, paroxetine, sertraline)
Serotonin norepinephrine reuptake inhibitors (e.g., duloxetine,
venlafaxine, etc.) Bupropion Tricyclic antidepressants (e.g., amitriptyline, clomipramine,
nortriptyline, etc.) Mirtazapine Monoamine oxidase inhibitors (e.g., selegiline, tranylcypromine,
etc.)
Serotonin modulators (e.g., nefazodone, trazodone, etc.)
Augmentation with lithium, Cytomel (liothyronine), antipsychotics, or anticonvulsants

35 Medical Policy Update Bulletin: October 2019
Medical Benefit Drug Policy Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Ketalar®
(Ketamine) and Spravato™ (Esketamine) (continued)
Oct. 1, 2019
and
Spravato will be initiated at the same time the member starts a new daily oral antidepressant (one that has not previously been tried); and
Provider and/or the provider’s healthcare setting is certified in the Spravato REMS program; and
Spravato dosing is in accordance with the United States Food and Drug Administration (FDA) approved labeling; and
Initial authorization will be for no longer than 12 weeks.
Continuation of Therapy
Patient has previously been treated with Spravato; and Documentation of remission or a positive clinical response to Spravato;
and Submission of baseline and recent (within the last month) scoring on at
least one of the following assessments demonstrating remission or clinical response (e.g., score reduction from baseline) as defined by the:
o Hamilton Rating Scale for Depression (HAMD17; remission defined as
a score of ≤7) o Quick Inventory of Depressive Symptomatology (QIDS-C16;
remission defined as a score of ≤5) o Montgomery-Asberg Depression Rating Scale (MADRS; remission
defined as a score of ≤12)
and Patient is to receive Spravato therapy in conjunction with an oral
antidepressant; and Provider and/or the provider’s healthcare setting is certified in the
Spravato REMS program; and Prescribed by or in consultation with a psychiatrist; and Spravato dosing is in accordance with the United States FDA approved
labeling; and Authorization will be for no longer than 6 months.
Spravato is unproven and not medically necessary for the following: Anesthetic agent Chronic pain (including but not limited to nonmalignant pain,
Fibromyalgia, neuropathic pain, Complex Regional Pain Syndrome, Reflex
Sympathetic Dystrophy)
Migraine headaches

36 Medical Policy Update Bulletin: October 2019
Medical Benefit Drug Policy Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Ketalar®
(Ketamine) and Spravato™ (Esketamine) (continued)
Oct. 1, 2019 Ketalar (Ketamine) Injection
Ketamine injection is considered medically necessary and may be covered for the following: Anesthesia for diagnostic and surgical procedures that do not require
skeletal muscle relaxation The induction of anesthesia prior to administration of other anesthesia
agents
As supplemental anesthesia for low-potency agents, such as nitrous oxide
Ketamine injection is investigational, and therefore not proven or medically necessary for the following: Psychiatric disorders (including, but not limited to depression, bipolar
disorder, & posttraumatic stress disorder)
Chronic pain (including but not limited to nonmalignant pain, Fibromyalgia, neuropathic pain, Complex Regional Pain Syndrome, Reflex Sympathetic Dystrophy)
Migraine headaches
Maximum Dosage
Oct. 1, 2019
Related Policies Added reference link to the
Medical Benefit Drug Policy
titled: o Cimzia® (Certolizumab Pegol) o Onpattro™ (Patisiran)
Coverage Rationale
Added language to clarify the use of medications included in this policy, when given within
the maximum dosage based upon body surface area or patient weight or a set of
maximal dosage independent of patient body size, are proven when used according to labeled indications or when otherwise
supported by published clinical
evidence Revised list of applicable drug
This policy provides information about the maximum dosage per administration for certain medications administered by a medical professional. Most medications have a maximum dosage based upon body
surface area or patient weight or a set maximal dosage independent of patient body size. Drug Products:
bevacizumab (Avastin®) bevacizumab-awwb (Mvasi™) bevacizumab-bvzr (Zirabev™)
certolizumab pegol (Cimzia®) denosumab (Prolia® & Xgeva®) eculizumab (Soliris®)
infliximab (Remicade®) infliximab-dyyb (Inflectra™) infliximab-abda (Renflexis™) nivolumab (Opdivo®)
omalizumab (Xolair®)
patisiran (Onpattro™) pegfilgrastim (Neulasta®)

37 Medical Policy Update Bulletin: October 2019
Medical Benefit Drug Policy Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Maximum Dosage
(continued)
Oct. 1, 2019
products; added:
o bevacizumab-awwb (Mvasi™)
o bevacizumab-bvzr (Zirabev™)
o certolizumab pegol (Cimzia®) o patisiran (Onpattro™) o ravulizumab-cwvz
(Ultomiris™) o rituximab-abbs (Truxima®) o trastuzumab-anns
(Kanjinti™) o trastuzumab-dkst (Ogivri™) o trastuzumab-dttb
(Ontruzant™)
o trastuzumab-pkrb (Herzuma®)
o trastuzumab-qyyp
(Trazimera™) Revised Maximum Allowed
Quantities by HCPCS Units and
Maximum Allowed Quantities for National Drug Code (NDC) Billing
Applicable Codes Added HCPCS codes J0222,
J0717, J1303, Q5107, Q5112, Q5113, Q5114, Q5115, Q5116, Q5117, and Q5118
Updated National Drug Codes (NDCs): o Added 00006-5033-02,
00069-0305-01, 00069-0315-01, 00069-0342-01, 25682-0022-01, 50242-0214-01, 50242-0215-01,
50474-0700-62, 50474-0710-79, 50474-0710-81,
55513-0132-01, 55513-
0206-01, 55513-0207-01,
pegfilgrastim-cbqv (Udenyca™)
pegfilgrastim-jmdb (Fulphila™) ravulizumab-cwvz (Ultomiris™) rituximab (Rituxan®) rituximab-abbs (Truxima®)
trastuzumab (Herceptin®) trastuzumab-anns (Kanjinti™) trastuzumab-dkst (Ogivri™)
trastuzumab-dttb (Ontruzant™) trastuzumab-pkrb (Herzuma®) trastuzumab-qyyp (Trazimera™)
ustekinumab (Stelara®) vedolizumab (Entyvio®) zoledronic acid (zoledronic acid, Reclast® and Zometa®)
The use of medications included in this policy when given within the maximum dosage based upon body surface area or patient weight or
a set of maximal dosage independent of patient body size are proven
when used according to labeled indications or when otherwise supported by published clinical evidence.
The medications included in this policy when given beyond maximum dosages based upon body surface area or patient weight or a set maximal dosage independent of patient body size are not supported by package labeling or published clinical evidence and are unproven.
This policy creates an upper dose limit based on the clinical evidence and the 95th percentile for adult body weight (128 kg) and body surface area (2.59
meters2) in the U.S. (adult male, 30 to 39 years, Fryar, 2016). In some cases, the maximum allowed units and/or vials may exceed the upper level limit as defined within this policy due to an individual patient body weight >
128 kg or body surface area > 2.59 meters2. Maximum Allowed Quantities by HCPCS Units
Refer to the policy for complete details on the Maximum Allowed Quantities by HCPCS Units for the drug products listed above.
Maximum Allowed Quantities for National Drug Code (NDC) Billing
Refer to the policy for complete details on the Maximum Allowed

38 Medical Policy Update Bulletin: October 2019
Medical Benefit Drug Policy Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Maximum Dosage
(continued)
Oct. 1, 2019 63459-0103-10, 63459-
0104-50, 63459-0303-43, 63459-0305-47, 67457-0847-44, 67457-0991-15, and 71336-1000-01
o Removed 50242-0056-56 and 50242-0134-68
Supporting Information
Updated CMS and References sections to reflect the most current information
Quantities for NDC Billing for the drug products listed above.
Oncology Medication Clinical
Coverage
Oct. 1, 2019
Related Policies Added reference link to the
Medical Policy titled Therapeutic Radiopharmaceuticals
Coverage Rationale
Removed language pertaining to “select ancillary and supportive care medications for oncology
conditions” Added language to indicate:
o Coverage of White Blood Cell Colony Stimulating Factors is
addressed in a separate policy
Medical Necessity Plans
o The Oncology Products table lists the UnitedHealthcare preferred oncology products
and respective non-preferred products; coverage will be provided for the UnitedHealthcare preferred
oncology product contingent on the coverage criteria in the Diagnosis-Specific
Criteria section of the policy o Coverage for any respective
Description
This policy provides parameters for coverage of injectable oncology medications (J9000-J9999) [including, but not limited to octreotide acetate (J2353 and J2354), leuprolide acetate (J1950), leucovorin (J0640) and
levoleucovorin (J0641)] covered under the medical benefit based upon the
National Comprehensive Cancer Network (NCCN) Drugs & Biologics Compendium® (NCCN Compendium®). The Compendium lists the appropriate
drugs and biologics for specific cancers using US Food and Drug Administration (FDA)-approved disease indications and specific NCCN panel recommendations. Each recommendation is supported by a level of evidence
category. Coverage of White Blood Cell Colony Stimulating Factors is addressed in a separate policy. This policy does not provide coverage criteria for Chimeric Antigen Receptor (CAR)-T Cell products. Coverage determinations are based on the member’s benefits and the OptumHealth
Transplant Solutions criteria for covered transplants; refer to the Clinical Guideline titled Transplant Review Guidelines: Hematopoietic Stem Cell Transplantation.
Coverage Rationale
Medical Necessity Plans
The Oncology Products table below lists the UnitedHealthcare preferred oncology products and respective non-preferred products. Coverage will be
provided for the UnitedHealthcare preferred oncology product contingent on the coverage criteria in the Diagnosis-Specific Criteria section.
Coverage for any respective non-preferred oncology product will be provided

39 Medical Policy Update Bulletin: October 2019
Medical Benefit Drug Policy Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Oncology
Medication Clinical Coverage (continued)
Oct. 1, 2019
non-preferred oncology
product will be provided contingent on the criteria in the Medical Necessity Criteria and the Diagnosis-
Specific Criteria sections of the policy; members new to therapy will be required to
utilize the UnitedHealthcare preferred oncology product unless they meet the
[following] criteria: Treatment with the
respective non-preferred product specified in the
Oncology Products table is medically necessary
for oncology indications
when both of the following are met: - History of intolerance
or contraindication to the UnitedHealthcare preferred oncology product; and
- Physician attests that, in their clinical opinion, the same
intolerance, contra-indication, or adverse event would not be
expected to occur with the respective non-preferred product
o The Oncology Products table
lists the UnitedHealthcare preferred oncology products
with therapeutically
equivalent and/or biosimilar
contingent on the criteria in the Medical Necessity Criteria and the Diagnosis-
Specific Criteria sections. Members new to therapy will be required to utilize the UnitedHealthcare preferred oncology product unless they meet the criteria in this section.
Medical Necessity Criteria
Treatment with the respective non-preferred product specified in the
Oncology Products table is medically necessary for oncology indications when BOTH of the following are met: History of intolerance or contraindication to the UnitedHealthcare
preferred oncology product; and Physician attests that, in their clinical opinion, the same intolerance,
contraindication, or adverse event would not be expected to occur with the respective non-preferred product.
Oncology Products
Below are UnitedHealthcare preferred oncology products with therapeutically
equivalent and/or biosimilar* non-preferred products as determined by the United Helathcare P&T Committee:
UnitedHealthcare Preferred
Oncology Product Non-Preferred Product
Mvasi (bevacizumab-awwb) Avastin (bevacizumab)
Zirabev (bevacizumab-bvzr)
Kanjinti (trastuzumab-anns)
Herceptin (trastuzumab)
Herceptin Hylecta (trastuzumab and hyaluronidase-oysk)
Herzuma (trastuzumab-pkrb)
Ogivri (trastuzumab-dkst)
Ontruzant (trastuzumab-dttb)
Trazimera (trastuzumab-qyyp)
Leucovorin Levoleucovorin
*Biosimilar means that the biological product is FDA-approved based on data demonstrating that it is highly similar to an already FDA-approved biological
product, known as a reference product, and that there are no clinically
meaningful differences between the biosimilar product and the reference product.

40 Medical Policy Update Bulletin: October 2019
Medical Benefit Drug Policy Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Oncology
Medication Clinical Coverage (continued)
Oct. 1, 2019
non-preferred products as
determined by the UnitedHealthcare Pharmacy and Therapeutics (P&T) Committee; biosimilar
means that the biological product is FDA-approved based on data demonstrating
that it is highly similar to an already FDA-approved biological product, known as
a reference product, and that there are no clinically meaningful differences between the biosimilar
product and the reference product
Diagnosis-Specific Criteria
o Refer to the Medical Necessity Criteria section of the policy for the UnitedHealthcare
preferred oncology products that have therapeutically equivalent and/or biosimilar products available
Additional Information o Modified language to indicate
the NCCN Clinical Practice
Guidelines in Oncology (NCCN Guidelines®) are comprehensive guidelines
documenting management decisions and interventions and interventions that apply to malignancies which apply
to more than 97% of cancers affecting U.S. patients
Supporting Information
Updated References section to
Diagnosis-Specific Criteria
Injectable Oncology Medications
UnitedHealthcare recognizes indications and uses of injectable oncology medications listed in the NCCN Drugs and Biologics Compendium with Categories of Evidence and Consensus of 1, 2A, and 2B as proven and medically necessary, and Categories of Evidence and Consensus of 3 as
unproven and not medically necessary. UnitedHealthcare will cover all chemotherapy agents for individuals under the
age of 19 years for oncology indications. The majority of pediatric patients receive treatments on national pediatric protocols that are quite similar in concept to the NCCN patient care guidelines.
Refer to the Medical Necessity Criteria for the UnitedHealthcare preferred oncology products that have therapeutically equivalent and/or biosimilar products available.
Additional Information
The NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) are comprehensive guidelines documenting management decisions and interventions and interventions that apply to malignancies which apply to
more than 97% of cancers affecting U.S. patients. NCCN Categories of Evidence and Consensus
Category 1: The recommendation is based on high-level evidence (i.e., high-powered randomized clinical trials or meta-analyses), and the panel has reached uniform consensus that the recommendation is indicated. In
this context, uniform means near unanimous positive support with some possible neutral positions.
Category 2A: The recommendation is based on lower level evidence,
but despite the absence of higher level studies, there is uniform consensus that the recommendation is appropriate. Lower level evidence is interpreted broadly, and runs the gamut from phase II to large cohort studies to case series to individual practitioner experience. Importantly,
in many instances, the retrospective studies are derived from clinical experience of treating large numbers of patients at a member institution,
so panel members have first-hand knowledge of the data. Inevitably,
some recommendations must address clinical situations for which limited

41 Medical Policy Update Bulletin: October 2019
Medical Benefit Drug Policy Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Oncology
Medication Clinical Coverage (continued)
Oct. 1, 2019 reflect the most current
information
or no data exist. In these instances the congruence of experience-based
opinions provides an informed if not confirmed direction for optimizing patient care. These recommendations carry the implicit recognition that they may be superseded as higher level evidence becomes available or as outcomes-based information becomes more prevalent.
Category 2B: The recommendation is based on lower level evidence, and there is nonuniform consensus that the recommendation should be made. In these instances, because the evidence is not conclusive,
institutions take different approaches to the management of a particular clinical scenario. This nonuniform consensus does not represent a major disagreement, rather it recognizes that given imperfect information,
institutions may adopt different approaches. A Category 2B designation should signal to the user that more than one approach can be inferred from the existing data.
Category 3: The recommendation has engendered a major
disagreement among the panel members. Several circumstances can cause major disagreements. For example, if substantial data exists about
two interventions but they have never been directly compared in a
randomized trial, adherents to one set of data may not accept the interpretation of the other side's results. Another situation resulting in a Category 3 designation is when experts disagree about how trial data can
be generalized. A Category 3 designation alerts users to a major interpretation issue in the data and directs them to the manuscript for an explanation of the controversy.
Orencia® (Abatacept)
Injection for Intravenous Infusion
Oct. 1, 2019 TBD
Notice of Implementation Delay: The changes described below will not be effective on Oct. 1, 2019, as previously announced. Implementation of the revised Medical Benefit Drug Policy has been postponed until further
notice; complete details will be provided in a future edition of the Medical Policy Update Bulletin. Template Update
Reorganized policy template; relocated Background and FDA sections
Coverage Rationale Added language to indicate Orencia (abatacept) for self-administered subcutaneous injection is obtained under
the pharmacy benefit
Replaced language indicating “Orencia is proven and medically necessary for the treatment of [the listed indications]” with “Orencia is proven and/or medically necessary for the treatment of [the listed indications]
Revised coverage criteria:
All Indications o Added criterion for initial therapy and continuation of therapy requiring:

42 Medical Policy Update Bulletin: October 2019
Medical Benefit Drug Policy Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Orencia®
(Abatacept) Injection for Intravenous Infusion
(continued)
Oct. 1, 2019
TBD
One of the following:
- Both of the following: History of failure, contraindication, or intolerance to Orencia labeled for self-administration Physician attests that, in their clinical opinion, the clinical response would be expected to be
superior with Orencia for intravenous infusion
- Physician attestation that the patient or caregiver is not competent to administer Orencia FDA labeled for self-administration; physician must submit explanation
Authorization is for no more than 12 months
For continuation of therapy: Patient has previously received Orencia injection for intravenous infusion
Rheumatoid Arthritis o Added criterion for initial therapy requiring history of failure, contraindication, or intolerance to two of the
following preferred products (document drug, date, and duration of trial): Cimzia (certolizumab) Humira (adalimumab) Simponi (golimumab)
Olumiant (baricitinib) Rinvoq (upadacitinib)
Xeljanz/Xeljanz XR (tofacitinib)
Psoriatic Arthritis o Added criterion for initial therapy requiring history of failure, contraindication, or intolerance to two of the
following preferred products (document drug, date, and duration of trial):
Cimzia (certolizumab) Humira (adalimumab) Simponi (golimumab) Stelara (ustekinumab)
Review at Launch Medication List
Oct. 1, 2019 Removed Cutaquig® [Immune Globulin Subcutaneous (Human) – hipp], Evenity™ (romosozumab-
aqqg), and Zolgensma® (ona-semnogene abeparvovec-xioi); prior authorization requirements effective Oct. 1, 2019
Refer to the Review at Launch Medication List for complete details. Refer to the Medical Benefit Drug Policy titled Review at Launch for New to
Market Medications for additional information.

43 Medical Policy Update Bulletin: October 2019
Medical Benefit Drug Policy Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Self-Administered
Medications List
Oct. 1, 2019
Applicable Codes
Added Fasenra (benralizumab) autoinjector, prefilled syringe labeled for self-administration (HCPCS code J0517)
Removed Hemlibra (emicizumab)
Updated list of applicable HCPCS
codes for:
Ajovy (fremanezumab-vfrm) o Replaced J3590 with J3031*
o Removed C9040*
Cimzia (certolizumab pegol) Revised description for J0717
Takhzyro (lanadelumab-flyo)
o Replaced J3590 with J0593* (*quarterly code edit)
Refer to the Self-Administered Medications List for complete details.
Refer to the Medical Benefit Drug Policy titled Self-Administered Medications for additional information.
Simponi Aria®
(Golimumab)
Injection for Intravenous Infusion
Oct. 1, 2019 TBD
Notice of Implementation Delay: The changes described below will not be effective on Oct. 1, 2019, as previously announced. Implementation of the revised Medical Benefit Drug Policy has been postponed until further
notice; complete details will be provided in a future edition of the Medical Policy Update Bulletin. Template Update Reorganized policy template; relocated Background and FDA sections
Coverage Rationale Revised coverage criteria for initial therapy and continuation of therapy for all indications; added criterion
requiring:
o One of the following: Both of the following:
- History of failure, contraindication, or intolerance to Simponi labeled for self-administration
- Physician attests that, in their clinical opinion, the clinical response would be expected to be superior with Simponi Aria for intravenous infusion
Physician attestation that the patient or caregiver are not competent to administer Simponi FDA labeled for self-administration; physician must submit explanation
o Authorization is for no more than 12 months o For continuation of therapy: Patient has previously received Simponi Aria injection for intravenous infusion

44 Medical Policy Update Bulletin: October 2019
Medical Benefit Drug Policy Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Sodium
Hyaluronate
Oct. 1, 2019
Notice of Revision: The following
summary of changes has been modified. Revisions to the previous policy update announcement are outlined in red below. Please take
note of the additional updates implemented on Oct. 1, 2019.
Template Update Changed policy type
classification from “Medical
Policy” to “Medical Benefit Drug Policy”
Added Documentation
Requirements section
Coverage Rationale Added language to indicate:
Medical Necessity Plans
o Coverage for Durolane, Euflexxa, and Gelsyn-3 is contingent on criteria in the
Diagnosis-Specific Criteria section of the policy; prior authorization is not required
o Coverage for GenVisc 850, Hyalgan, Supartz, Visco-3, Hymovis, Orthovisc, Synvisc
or Synvisc-One, Gel-One, Monovisc, Triluron, TriVisc, or Synojoynt is contingent on the Medical Necessity
Criteria and Diagnosis-Specific Criteria sections of the policy
In order to continue coverage, members already on these
products will be required to change therapy to
Medical Necessity Plans
Coverage for Durolane, Euflexxa, and Gelsyn-3 is contingent on criteria in the Diagnosis-Specific Criteria section. Prior authorization is not required.
Coverage for GenVisc 850, Hyalgan, Supartz, Visco-3, Hymovis, Orthovisc, Synvisc or Synvisc-One, Gel-One, Monovisc, Triluron,
TriVisc, or Synojoynt is contingent on the Medical Necessity Criteria and Diagnosis-Specific Criteria. In order to continue coverage, members already on these products will be required to change therapy to Durolane,
Euflexxa, or Gelsyn-3 unless they meet the criteria below.
Medical Necessity Criteria
Treatment with GenVisc 850, Hyalgan, Supartz, Visco-3, Hymovis, Orthovisc, Synvisc or Synvisc-One, Gel-One, Monovisc, Triluron, TriVisc, or Synojoynt is
medically necessary for the indications specified in this policy when one the criteria below are met:
Both of the following:
o History of a trial of adequate dose and duration of Durolane, Euflexxa, and Gelsyn-3, resulting in minimal clinical response; and
o Physician attests that, in their clinical opinion, the clinical response
would be expected to be superior than experienced with Durolane, Euflexxa, and Gelsyn-3.
or Both of the following:
o History of failure, contraindication, or intolerance to Durolane, Euflexxa, and Gelsyn-3; and
o Physician attests that, in their clinical opinion, the same failure,
contraindication, or intolerance would not be expected to occur with GenVisc 850, Hyalgan, Supartz, Visco-3, Hymovis, Orthovisc, Synvisc or Synvisc-One, Gel-One, Monovisc, Triluron, TriVisc, or Synojoynt.
Non-Medical Necessity Plans
Any sodium hyaluronate product is to be approved contingent on the
coverage criteria in the Diagnosis-Specific Criteria section.
Diagnosis-Specific Criteria
Initial Authorization (sodium hyaluronate naïve patients)

45 Medical Policy Update Bulletin: October 2019
Medical Benefit Drug Policy Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Sodium
Hyaluronate (continued)
Oct. 1, 2019
Durolane, Euflexxa, or
Gelsyn-3 unless they meet the Medical Necessity Criteria listed in the policy
o Treatment with GenVisc 850, Hyalgan, Supartz, Visco-3, Hymovis, Orthovisc, Synvisc
or Synvisc-One, Gel-One, Monovisc, Triluron, TriVisc, or Synojoynt is medically
necessary for the indications specified in this policy when one of the criteria below are met:
Both of the following: - History of a trial of
adequate dose and
duration of Durolane, Euflexxa, and Gelsyn-3, resulting
in minimal clinical response
- Physician attests that, in their clinical
opinion, the clinical response would be expected to be
superior than experienced with Durolane, Euflexxa,
and Gelsyn-3 or
Both of the following: - History of failure,
contraindication, or intolerance to
Durolane, Euflexxa,
and Gelsyn-3
Intra-articular injections of sodium hyaluronate are proven and
medically necessary when all of the following are met: Diagnosis of one of the following:
o Hip osteoarthritis o Knee osteoarthritis
o Temporomandibular joint osteoarthritis o Temporomandibular joint disc displacement and
The member has not responded adequately to conservative therapy which may include physical therapy or pharmacotherapy (e.g., non-steroidal anti-inflammatory drugs [NSAIDs], acetaminophen and/or
topical capsaicin cream) or injection of intra-articular steroids and such therapy has not resulted in functional improvement after at least 3 months, or the member is unable to tolerate conservative therapy because of adverse side effects; and
The member reports pain which interferes with functional activities (e.g., ambulation, prolonged standing); and
The pain cannot be attributed to other forms of osteoarthritis; and
There are no contraindications to the injections (e.g., active joint infection, bleeding disorder); and
Dosing is in accordance with the US FDA approved labeling as shown in
the table below; and Initial authorization is for a single injection course once per joint for 6
months.
Reauthorization/Continuation
Repeated courses of intra-articular hyaluronan injections may be considered when ALL of the following are met: Documentation of positive clinical response to therapy (e.g., significant
pain relief was achieved with the prior course of injections); and Pain has recurred; and At least 6 months have passed since the prior course of treatment for the
respective joint; and Dosing is in accordance with the US FDA approved labeling as shown in
the table below; and Continuing authorization is for a single injection course once per joint for
6 months.
The table below shows the FDA approved sodium hyaluronate products and

46 Medical Policy Update Bulletin: October 2019
Medical Benefit Drug Policy Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Sodium
Hyaluronate (continued)
Oct. 1, 2019
- Physician attests
that, in their clinical opinion, the same failure, contraindication, or
intolerance would not be expected to occur with GenVisc
850, Hyalgan, Supartz, Visco-3, Hymovis, Orthovisc,
Synvisc or Synvisc-One, Gel-One, Monovisc, Triluron, TriVisc, or Synojoynt
Non-Medical Necessity Plans o Any sodium hyaluronate
product is to be approved
contingent on the coverage criteria in the Diagnosis-Specific Criteria section of
the policy Revised Diagnosis-Specific
Criteria
Applicable Codes
Updated list of applicable HCPCS codes to reflect quarterly code edits; added J7331 and J7332
Added ICD-10 diagnosis codes M16.0, M16.10, M16.11, M16.12, M16.2, M16.30,
M16.31, M16.32, M16.4, M16.50, M16.51, M16.52, M16.6, M16.7, and M16.9
Supporting Information
Updated FDA and References sections to reflect the most
current information
their respective FDA labeled dosage per treatment course per joint:
Sodium Hyaluronate Product Course of Treatment per Joint
Durolane 1 injection
Euflexxa 3 injections
Gel One 1 injection
Sodium Hyaluronate Product Course of Treatment per Joint
Gelsyn-3 3 injections
GenVisc 850 3 to 5 injections
Hyalgan 5 injections
Hymovis 2 injections
Monovisc 1 injection
Orthovisc 3 to 4 injections
Supartz 3 to 5 injections
Synvisc 3 injections
Synvisc One 1 injection
TriVisc 3 injections
Visco-3 3 injections
Synojoynt 3 injections
Intra-articular injections of sodium hyaluronate are unproven and not medically necessary for treating any other indication due to insufficient evidence of efficacy.
Hyaluronic acid gel preparations to improve the skin's appearance, contour and/or reduce depressions due to acne, scars, injury or
wrinkles are considered cosmetic and are not covered.

47 Medical Policy Update Bulletin: October 2019
Medical Benefit Drug Policy Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Stelara®
(Ustekinumab)
Oct. 1, 2019
Template Update
Reorganized policy template; relocated Background and FDA sections
Coverage Rationale
Added language to indicate Stelara (ustekinumab) for self-administered subcutaneous
injection is obtained under the pharmacy benefit
Replaced language indicating
“Stelara is proven and medically necessary for the treatment of [the listed indications]” with “Stelara is proven and/or
medically necessary for the treatment of [the listed
indications]
Revised coverage criteria for:
Crohn’s Disease o Replaced criterion for initial
therapy requiring: “History of failure,
contraindication, or intolerance to at least
one tumor necrosis factor (TNF) blocker” with “history of
inadequate response or failure, contraindication, or intolerance to at least
one tumor necrosis factor (TNF) blocker”
“History of failure, contraindication, or
intolerance to at least one immunomodulator
or corticosteroid” with
“history of inadequate
This policy refers to Stelara (ustekinumab) injection. Stelara
(ustekinumab) for self-administered subcutaneous injection is obtained under the pharmacy benefit. Stelara is proven and/or medically necessary for the treatment of:
Crohn’s disease when ALL of the following criteria are met: Diagnosis of moderately to severely active Crohn’s disease; and
One of the following: o History of inadequate response or failure, contraindication, or
intolerance to at least one tumor necrosis factor (TNF) blocker [e.g.,
infliximab, Humira (adalimumab), Cimzia (certolizumab)]; or o Both of the following:
History of inadequate response or failure, contraindication, or intolerance to at least one immunomodulator or corticosteroid
(e.g., corticosteroids, 6-mercaptopurine, azathioprine, methotrexate, etc.); and
Patient has never failed a TNF blocker [e.g., infliximab, Humira
(adalimumab), Cimzia (certolizumab)] and
o One of the following:
Initial Therapy - Stelara is to be administered as an intravenous induction
dose; and - Stelara induction dosing is in accordance with the United
States Food and Drug Administration approved labeled dosing for Crohn’s disease: 260mg for patients weighing ≤55kg
390mg for patients weighing >55kg to ≤85kg 520mg for patients weighing >85kg and
- Patient is not receiving Stelara in combination with any of the following: Biologic DMARD [e.g., infliximab, Humira (adalimumab),
Cimzia (certolizumab), Simponi (golimumab)]
Janus kinase inhibitor [e.g., Xeljanz (tofacitinib)] Phosphodiesterase 4 (PDE4) inhibitor [e.g., Otezla
(apremilast)]
and

48 Medical Policy Update Bulletin: October 2019
Medical Benefit Drug Policy Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Stelara®
(Ustekinumab) (continued)
Oct. 1, 2019
response or failure,
contraindication, or intolerance to at least one immunomodulator or corticosteroid”
o Updated criteria for continuation of therapy: Added criterion
requiring: - Physician attestation
that the patient or
caregiver are not competent to administer Stelara FDA labeled for self-
administration; physician must
submit explanation
- Authorization is for no more than 12 months
Removed criterion requiring patient is unable to self-administer subcutaneous doses
Plaque Psoriasis o Updated criteria for initial
therapy:
Added criterion requiring: - Physician attestation
that the patient or caregiver are not competent to administer Stelara
FDA labeled for self-administration;
physician must
submit explanation
- Authorization will be for one induction dose.
Continuation of Therapy - Physician attestation that the patient or caregiver is not
competent to administer Stelara FDA labeled for self-administration; physician must submit explanation; and
- Stelara is to be subcutaneously administered 8 weeks after the initial intravenous dose; and
- Stelara continuation dosing is in accordance with the United
States Food and Drug Administration approved labeled dosing for Crohn’s disease: 90mg every 8 weeks subcutaneously; and
- Patient is not receiving Stelara in combination with any of the following: Biologic DMARD [e.g., infliximab, Humira (adalimumab),
Cimzia (certolizumab), Simponi (golimumab)]
Janus kinase inhibitor [e.g., Xeljanz (tofacitinib)] Phosphodiesterase 4 (PDE4) inhibitor [e.g., Otezla
(apremilast)]
- Authorization is for no more than 12 months.
Plaque psoriasis when ALL of the following criteria are met:
For initial therapy, all of the following: o Diagnosis of moderate to severe plaque psoriasis; and o Patient is a candidate for systemic therapy; and o Physician attestation that the patient or caregiver is not competent to
administer Stelara FDA labeled for self-administration; physician must submit explanation; and
o Stelara is initiated and titrated according to US Food and Drug
Administration labeled dosing for plaque psoriasis up to a maximum of (or equivalent dose and interval schedule): 45mg every 12 weeks for patients weighing ≤100kg
subcutaneously 90mg every 12 weeks for patients weighing >100kg
subcutaneously and
o Patient is not receiving Stelara in combination with any of the following:
Biologic DMARD [e.g., Enbrel (etanercept), Humira
(adalimumab), Cimzia (certolizumab), Simponi (golimumab)]

49 Medical Policy Update Bulletin: October 2019
Medical Benefit Drug Policy Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Stelara®
(Ustekinumab) (continued)
Oct. 1, 2019
- Initial authorization
is for no more than 12 months
Removed criterion requiring patient is
unable to self-administer subcutaneous doses
o Added criteria for
continuation of therapy
Psoriatic Arthritis o Updated criteria for initial
therapy: Added criterion
requiring: - Physician attestation
that the patient or caregiver are not
competent to
administer Stelara FDA labeled for self-administration;
physician must submit explanation
- Initial authorization is for no more than
12 months Removed criterion
requiring patient is
unable to self-administer subcutaneous doses
o Added criteria for
continuation of therapy
Janus kinase inhibitor [e.g., Xeljanz (tofacitinib)]
Phosphodiesterase 4 (PDE4) inhibitor [e.g., Otezla (apremilast)] o Initial authorization is for no more than 12 months.
For continuation of therapy, all of the following: o Documentation of positive clinical response; and
o Physician attestation that the patient or caregiver is not competent to administer Stelara FDA labeled for self-administration; physician must submit explanation; and
o Stelara is initiated and titrated according to US Food and Drug Administration labeled dosing for plaque psoriasis up to a maximum of (or equivalent dose and interval schedule):
45mg every 12 weeks for patients weighing ≤100kg subcutaneously
90mg every 12 weeks for patients weighing >100kg subcutaneously
and o Patient is not receiving Stelara in combination with any of the
following:
Biologic DMARD [e.g., infliximab, Humira (adalimumab), Cimzia (certolizumab), Simponi (golimumab)]
Janus kinase inhibitor [e.g., Xeljanz (tofacitinib)]
Phosphodiesterase 4 (PDE4) inhibitor [e.g., Otezla (apremilast)] o Authorization is for no more than 12 months.
Psoriatic arthritis when ALL of the following criteria are met:
For initial therapy, all of the following: o Diagnosis of psoriatic arthritis; and o Stelara is initiated and titrated according to US Food and Drug
Administration labeled dosing for psoriatic arthritis up to a maximum of 90mg every 12 weeks subcutaneously (or equivalent dose and interval schedule); and
o Physician attestation that the patient or caregiver is not competent to administer Stelara FDA labeled for self-administration; physician must submit explanation; and
o Patient is not receiving Stelara in combination with any of the
following: Biologic DMARD [e.g., Enbrel (etanercept), Humira
(adalimumab), Cimzia (certolizumab), Simponi (golimumab)]
Janus kinase inhibitor [e.g., Xeljanz (tofacitinib)]
50 Medical Policy Update Bulletin: October 2019
Medical Benefit Drug Policy Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Stelara®
(Ustekinumab) (continued)
Oct. 1, 2019
Phosphodiesterase 4 (PDE4) inhibitor [e.g., Otezla (apremilast)]
o Initial authorization is for no more than 12 months. For continuation of therapy, all of the following:
o Documentation of positive clinical response; and o Physician attestation that the patient or caregiver is not competent to
administer Stelara FDA labeled for self-administration; physician must submit explanation; and
o Stelara is initiated and titrated according to US Food and Drug
Administration labeled dosing for psoriatic arthritis up to a maximum of 90mg every 12 weeks subcutaneously (or equivalent dose and interval schedule); and
o Patient is not receiving Stelara in combination with any of the following: Biologic DMARD [e.g., infliximab, Humira (adalimumab), Cimzia
(certolizumab), Simponi (golimumab)]
Janus kinase inhibitor [e.g., Xeljanz (tofacitinib)] Phosphodiesterase 4 (PDE4) inhibitor [e.g., Otezla (apremilast)]
o Authorization is for no more than 12 months.
Stelara is unproven and not medically necessary for the treatment of multiple sclerosis.
In available studies, Stelara does not demonstrate efficacy in the treatment of multiple sclerosis.

51 Medical Policy Update Bulletin: October 2019
Coverage Determination Guideline (CDG) Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Preventive Care Services
Dec. 1, 2019
Applicable Codes: Preventive Care Services
Hepatitis B Virus Infection Screening
Updated service description for Pregnant Women: o Removed June 2009 USPSTF
“A” rating o Added July 2019 USPSTF “A”
rating to indicate the USPSTF
recommends screening for hepatitis B virus (HBV) infection in pregnant women at their first prenatal visit
Newborn Screenings Updated service description;
removed July 2008 USPSTF “B”
rating Removed list of applicable
CPT/HCPCS codes for Hearing
Screening: 92551, 92558, 92585, 92586, 92587, 92588, and V5008
Osteoporosis Screening
Updated list of applicable CPT codes; removed 77078
Screening for Visual Impairment
in Children Updated service
description/Bright Futures
recommendation to indicate: o Visual acuity screening is
recommended for age 4 and 5 years, as well as in
cooperative 3 year olds o Instrument-based screening
is recommended for age 12
and 24 months, in addition to the well visits at age 3
Indications for Coverage
Introduction
UnitedHealthcare covers certain medical services under the preventive care services benefit. The federal Patient Protection and Affordable Care Act (PPACA) requires non-grandfathered health plans to cover certain
“recommended preventive services” as identified by PPACA under the preventive care services benefit, without cost sharing to members when provided by network physicians. This includes:
Evidence-based items or services that have in effect a rating of “A” or “B” in the current recommendations of the United States Preventive Services Task Force.
Immunizations for routine use in children, adolescents and adults that
have in effect a recommendation from the Advisory Committee on Immunization Practices of the Centers for Disease Control and Prevention.
With respect to infants, children and adolescents, evidence-informed preventive care and screenings provided for in the comprehensive
guidelines supported by the Health Resources and Services
Administration. With respect to women, such additional preventive care and screenings
as provided for in comprehensive guidelines supported by the Health Resources and Services Administration.
Member Cost-Sharing
Non-Grandfathered Plans: o Non-grandfathered plans provide coverage for preventive care
services with no member cost sharing (i.e., covered at 100% of Allowed Amounts without deductible, coinsurance or copayment) when services are obtained from a Network provider.
o Under PPACA, services obtained from an out-of-network provider are not required to be covered under a plan’s preventive benefit, and may be subject to member cost sharing. Refer to the member specific benefit plan document for out-of-network benefit
information, if any. Grandfathered Plans:
o Plans that maintain grandfathered status under PPACA are not
required by law to provide coverage for these preventive services without member cost sharing; although a grandfathered plan may

52 Medical Policy Update Bulletin: October 2019
Coverage Determination Guideline (CDG) Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Preventive Care
Services (continued)
Dec. 1, 2019
through 5 years
Revised preventive benefit instructions/age limit guidelines to indicate: o Visual acuity screening
(CPT code 99173): Up to age 21 years (ends on 22nd birthday); does not have
diagnosis code requirements for preventive benefits to apply
o Instrument-based screening (CPT codes 99174 and 99177): Age 1 to 5 (ends on 6th
birthday); does not have diagnosis code
requirements for
preventive benefits to apply
Age 6 to 21 years (ends
on 22nd birthday); refer to the Medical Policy titled Omnibus Codes for allowable diagnoses
Hearing Tests (Bright Futures) Updated list of applicable codes:
o Added CPT/HCPCS codes
92558, 92585, 92586, 92587, 92588, and V5008
o Added ICD-10 diagnosis
codes Z00.00 and Z00.01
choose to voluntarily amend its plan document to include these
preventive benefits. o Except where there are state mandates, a grandfathered plan might
include member cost sharing, or exclude some of the preventive care services identified under PPACA.
o Refer to the member specific benefit plan document for details on how benefits are covered under a grandfathered plan.
Preventive vs. Diagnostic Services
Certain services can be done for preventive or diagnostic reasons. When a service is performed for the purpose of preventive screening and is appropriately reported, it will be considered under the preventive care
services benefit. This includes services directly related to the performance of a covered preventive care service (see the Frequently Asked Questions section of the policy for additional information.)
Preventive services are those performed on a person who:
has not had the preventive screening done before and does not have symptoms or other abnormal studies suggesting abnormalities; or
has had screening done within the recommended interval with the findings considered normal; or
has had diagnostic services results that were normal after which the
physician recommendation would be for future preventive screening studies using the preventive services intervals.
When a service is done for diagnostic purposes it will be considered under the
applicable non-preventive medical benefit. Diagnostic services are done on a person who: had abnormalities found on previous preventive or diagnostic studies that
require further diagnostic studies; or had abnormalities found on previous preventive or diagnostic studies that
would recommend a repeat of the same studies within shortened time
intervals from the recommended preventive screening time intervals; or had a symptom(s) that required further diagnosis; or does not fall within the applicable population for a recommendation or
guideline
Covered Breastfeeding Equipment
Personal-use electric breast pump:
53 Medical Policy Update Bulletin: October 2019
Coverage Determination Guideline (CDG) Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Preventive Care
Services (continued)
Dec. 1, 2019
The purchase of a personal-use electric breast pump (HCPCS code
E0603). o This benefit is limited to one pump per birth. In the case of a birth
resulting in multiple infants, only one breast pump is covered. o A breast pump purchase includes the necessary supplies for the
pump to operate. Replacement breast pump supplies necessary for the personal-use
electric breast pump to operate. This includes: standard power adaptor,
tubing adaptors, tubing, locking rings, bottles specific to breast pump operation, caps for bottles that are specific to the breast pump, valves, filters, and breast shield and/or splash protector for use with the breast
pump. Coverage Limitations and Exclusions
Services not covered under the preventive care benefit may be covered under another portion of the medical benefit plan.
The coverage outlined in this guideline does not address certain
outpatient prescription medications, tobacco cessation drugs and/or over the counter items, as required by PPACA. These preventive benefits are administered by the member’s pharmacy plan administrator. For details
on coverage, refer to the member-specific pharmacy plan administrator. A vaccine (immunization) is not covered if it does not meet company
vaccine policy requirements for FDA labeling and if it does not have explicit ACIP recommendations for routine use published in the Morbidity
and Mortality Weekly Report (MMWR) of the Centers for Disease Control and Prevention (CDC).
Examinations, screenings, testing, or vaccines (immunizations) are not
covered when: o required solely for the purposes of career or employment, school or
education, sports or camp, travel (including travel vaccines
(immunizations)), insurance, marriage or adoption; or o related to judicial or administrative proceedings or orders; or o conducted for purposes of medical research; or o required to obtain or maintain a license of any type.
Services that are investigational, experimental, unproven or not medically necessary are not covered.
Breastfeeding equipment and supplies not listed above. This includes, but
is not limited to: o Manual breast pumps and all related equipment and supplies.

54 Medical Policy Update Bulletin: October 2019
Coverage Determination Guideline (CDG) Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Preventive Care
Services (continued)
Dec. 1, 2019 o Hospital-grade breast pumps and all related equipment and supplies.
o Equipment and supplies not listed in the Covered Breastfeeding Equipment section above, including but not limited to: Batteries, battery-powered adaptors, and battery packs. Electrical power adapters for travel.
Bottles which are not specific to breast pump operation. This includes the associated bottle nipples, caps and lids.
Travel bags, and other similar travel or carrying accessories.
Breast pump cleaning supplies including soap, sprays, wipes, steam cleaning bags and other similar products.
Baby weight scales.
Garments or other products that allow hands-free pump operation.
Breast milk storage bags, ice-packs, labels, labeling lids, and other similar products.
Nursing bras, bra pads, breast shells, nipple shields, and other similar products.
Creams, ointments, and other products that relieve breastfeeding
related symptoms or conditions of the breasts or nipples.