odontogenic keratocyst marsupialization and decompression · that can immediately impact their...
TRANSCRIPT
The Journal of Implant & Advanced Clinical Dentistry
Volume 10, No. 4 may/JuNe 2018
Odontogenic Keratocyst Marsupialization and Decompression
3D Printed Bone Scaffolds
ATTENTION PROSPECTIVE
AUTHORSJIACD wants to publish
your article!
The Journal of Implant & Advanced Clinical Dentistry
For complete details regarding publication in JIACD,
please refer to our author guidelines at the following link:
jiacd.com/author-guidelines or email us at:
The Best Things in Life Are FREE!
Subscribe now to enjoy articles free of charge that will benefit you, the actively practicing dental provider. With each JIACD issue, readers are afforded the opportunity to
assess clinical techniques, cases, literature reviews, and expert commentary that can immediately impact their daily dental practice.
Email notification when new issues are available online.
Start your FREE subscription today at www.jiacd.com
The Journal of Implant & Advanced Clinical Dentistry
Volume 8, No. 8 December 2016
Full Mouth Rehabilitation of Periodontitis Patient
Implant-Supported Milled Bar
Overdenture
The Journal of Implant & Advanced Clinical Dentistry
Volume 8, No. 1 march 2016
Treatment of the Atrophic Maxilla with Autogenous Blocks
Modified Mandibular Implant Bar Overdenture
The Journal of Implant & Advanced Clinical Dentistry
Volume 8, No. 3 may/JuNe 2016
Treatment of Mandibular Central Giant Cell Granuloma
Titanium Mesh Ridge Augmentation for Dental
Implant Placement
The Journal of Implant & Advanced Clinical Dentistry
Volume 8, No. 4 July/August 2016
Mandibular Overdentures with Mini-Implants
Augmentation of Severe Ridge Defect with rhBMP-2
and Titanium Mesh
The Journal of Implant & Advanced Clinical DentistryVolume 10, No. 4 • may/JuNe 2018
Table of Contents
6 Odontogenic Keratocyst Treatment with Marsupialization and Decompression: A Case Series Juan Gonzalez, David Malave, Dan Holtzclaw
12 3-D Printing of a Customized Bone Scaffold using Beta- Tricalcium-Phosphate, Alginate, and Cellulose Nanofibers: A Novel Test Mohamed Maksoud, Kevin Guze
2 • Vol. 10, No. 4 • May/June 2018
The Journal of Implant & Advanced Clinical Dentistry • 3
The Journal of Implant & Advanced Clinical DentistryVolume 10, No. 4 • may/JuNe 2018
Table of Contents
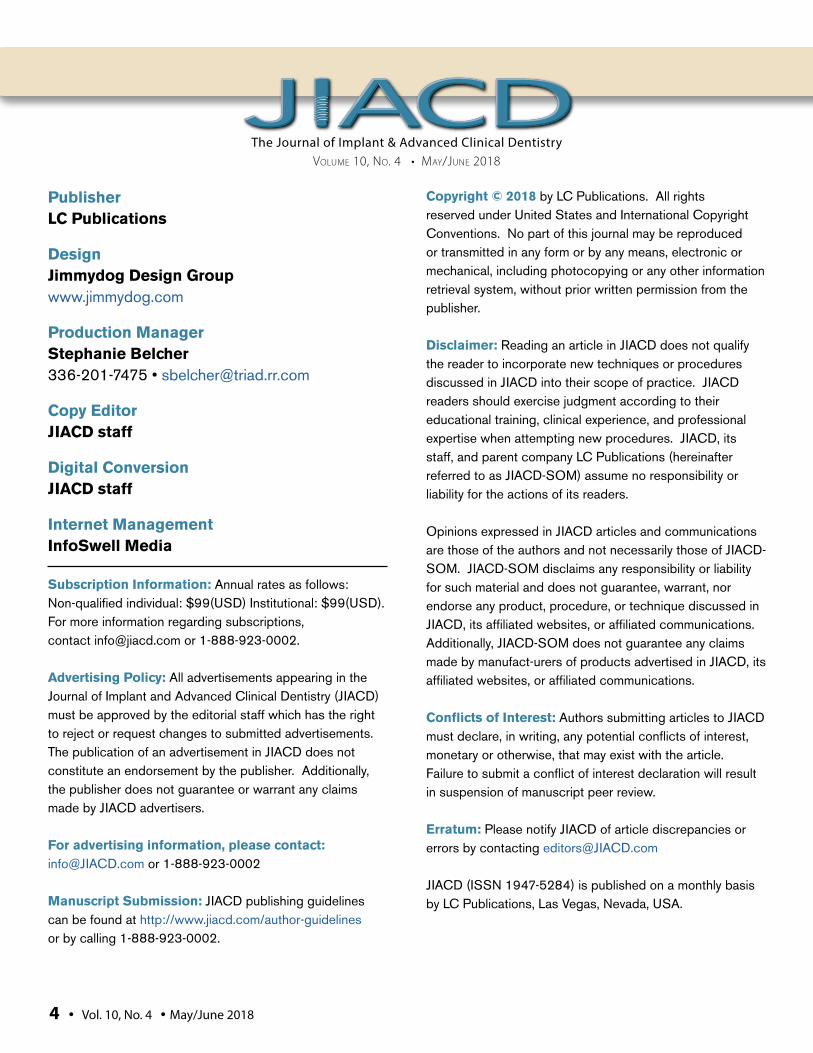
16 The Role of Antimicrobials in the Success Rate of Dental Implants Dr. Lanka Mahesh, Dr. JL Calvo Guiardo, Dr. Gregori Kurtzman, Dr. Sagrika Shukla
24 Periodontal Perspectives of Autologous Blood Preparations Pavankumar Addanki
The Journal of Implant & Advanced Clinical DentistryVolume 10, No. 4 • may/JuNe 2018
PublisherLC Publications
DesignJimmydog Design Group www.jimmydog.com
Production ManagerStephanie Belcher 336-201-7475 • [email protected]
Copy EditorJIACD staff
Digital ConversionJIACD staff
Internet ManagementInfoSwell Media
Subscription Information: Annual rates as follows: Non-qualified individual: $99(USD) Institutional: $99(USD). For more information regarding subscriptions, contact [email protected] or 1-888-923-0002.
Advertising Policy: All advertisements appearing in the Journal of Implant and Advanced Clinical Dentistry (JIACD) must be approved by the editorial staff which has the right to reject or request changes to submitted advertisements. The publication of an advertisement in JIACD does not constitute an endorsement by the publisher. Additionally, the publisher does not guarantee or warrant any claims made by JIACD advertisers.
For advertising information, please contact:[email protected] or 1-888-923-0002
Manuscript Submission: JIACD publishing guidelines can be found at http://www.jiacd.com/author-guidelines or by calling 1-888-923-0002.
Copyright © 2018 by LC Publications. All rights reserved under United States and International Copyright Conventions. No part of this journal may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopying or any other information retrieval system, without prior written permission from the publisher.
Disclaimer: Reading an article in JIACD does not qualify the reader to incorporate new techniques or procedures discussed in JIACD into their scope of practice. JIACD readers should exercise judgment according to their educational training, clinical experience, and professional expertise when attempting new procedures. JIACD, its staff, and parent company LC Publications (hereinafter referred to as JIACD-SOM) assume no responsibility or liability for the actions of its readers.
Opinions expressed in JIACD articles and communications are those of the authors and not necessarily those of JIACD-SOM. JIACD-SOM disclaims any responsibility or liability for such material and does not guarantee, warrant, nor endorse any product, procedure, or technique discussed in JIACD, its affiliated websites, or affiliated communications. Additionally, JIACD-SOM does not guarantee any claims made by manufact-urers of products advertised in JIACD, its affiliated websites, or affiliated communications.
Conflicts of Interest: Authors submitting articles to JIACD must declare, in writing, any potential conflicts of interest, monetary or otherwise, that may exist with the article. Failure to submit a conflict of interest declaration will result in suspension of manuscript peer review.
Erratum: Please notify JIACD of article discrepancies or errors by contacting [email protected]
JIACD (ISSN 1947-5284) is published on a monthly basis by LC Publications, Las Vegas, Nevada, USA.
4 • Vol. 10, No. 4 • May/June 2018
The Journal of Implant & Advanced Clinical Dentistry • 5
Tara Aghaloo, DDS, MDFaizan Alawi, DDSMichael Apa, DDSAlan M. Atlas, DMDCharles Babbush, DMD, MSThomas Balshi, DDSBarry Bartee, DDS, MDLorin Berland, DDSPeter Bertrand, DDSMichael Block, DMDChris Bonacci, DDS, MDHugo Bonilla, DDS, MSGary F. Bouloux, MD, DDSRonald Brown, DDS, MSBobby Butler, DDSNicholas Caplanis, DMD, MSDaniele Cardaropoli, DDSGiuseppe Cardaropoli DDS, PhDJohn Cavallaro, DDSJennifer Cha, DMD, MSLeon Chen, DMD, MSStepehn Chu, DMD, MSD David Clark, DDSCharles Cobb, DDS, PhDSpyridon Condos, DDSSally Cram, DDSTomell DeBose, DDSMassimo Del Fabbro, PhDDouglas Deporter, DDS, PhDAlex Ehrlich, DDS, MSNicolas Elian, DDSPaul Fugazzotto, DDSDavid Garber, DMDArun K. Garg, DMDRonald Goldstein, DDSDavid Guichet, DDSKenneth Hamlett, DDSIstvan Hargitai, DDS, MS
Michael Herndon, DDSRobert Horowitz, DDSMichael Huber, DDSRichard Hughes, DDSMiguel Angel Iglesia, DDSMian Iqbal, DMD, MSJames Jacobs, DMDZiad N. Jalbout, DDSJohn Johnson, DDS, MSSascha Jovanovic, DDS, MSJohn Kois, DMD, MSDJack T Krauser, DMDGregori Kurtzman, DDSBurton Langer, DMDAldo Leopardi, DDS, MSEdward Lowe, DMDMiles Madison, DDSLanka Mahesh, BDSCarlo Maiorana, MD, DDSJay Malmquist, DMDLouis Mandel, DDSMichael Martin, DDS, PhDZiv Mazor, DMDDale Miles, DDS, MSRobert Miller, DDSJohn Minichetti, DMDUwe Mohr, MDTDwight Moss, DMD, MSPeter K. Moy, DMDMel Mupparapu, DMDRoss Nash, DDSGregory Naylor, DDSMarcel Noujeim, DDS, MSSammy Noumbissi, DDS, MSCharles Orth, DDSAdriano Piattelli, MD, DDSMichael Pikos, DDSGeorge Priest, DMDGiulio Rasperini, DDS
Michele Ravenel, DMD, MSTerry Rees, DDSLaurence Rifkin, DDSGeorgios E. Romanos, DDS, PhDPaul Rosen, DMD, MSJoel Rosenlicht, DMDLarry Rosenthal, DDSSteven Roser, DMD, MDSalvatore Ruggiero, DMD, MDHenry Salama, DMDMaurice Salama, DMDAnthony Sclar, DMDFrank Setzer, DDSMaurizio Silvestri, DDS, MDDennis Smiler, DDS, MScDDong-Seok Sohn, DDS, PhDMuna Soltan, DDSMichael Sonick, DMDAhmad Soolari, DMDNeil L. Starr, DDSEric Stoopler, DMDScott Synnott, DMDHaim Tal, DMD, PhDGregory Tarantola, DDSDennis Tarnow, DDSGeza Terezhalmy, DDS, MATiziano Testori, MD, DDSMichael Tischler, DDSTolga Tozum, DDS, PhDLeonardo Trombelli, DDS, PhDIlser Turkyilmaz, DDS, PhDDean Vafiadis, DDSEmil Verban, DDSHom-Lay Wang, DDS, PhDBenjamin O. Watkins, III, DDSAlan Winter, DDSGlenn Wolfinger, DDSRichard K. Yoon, DDS
Founder, Co-Editor in ChiefDan Holtzclaw, DDS, MS
Co-Editor in ChiefLeon Chen, DMD, MS, DICOI, DADIA
The Journal of Implant & Advanced Clinical Dentistry
Gonzales et al
Odontogenic cysts such as the odon-togenic keratocyst are benign lesions that have the potential for
aggressive infiltrative behavior and unde-sirable comorbidities. Treatment of these lesions with conservative techniques such
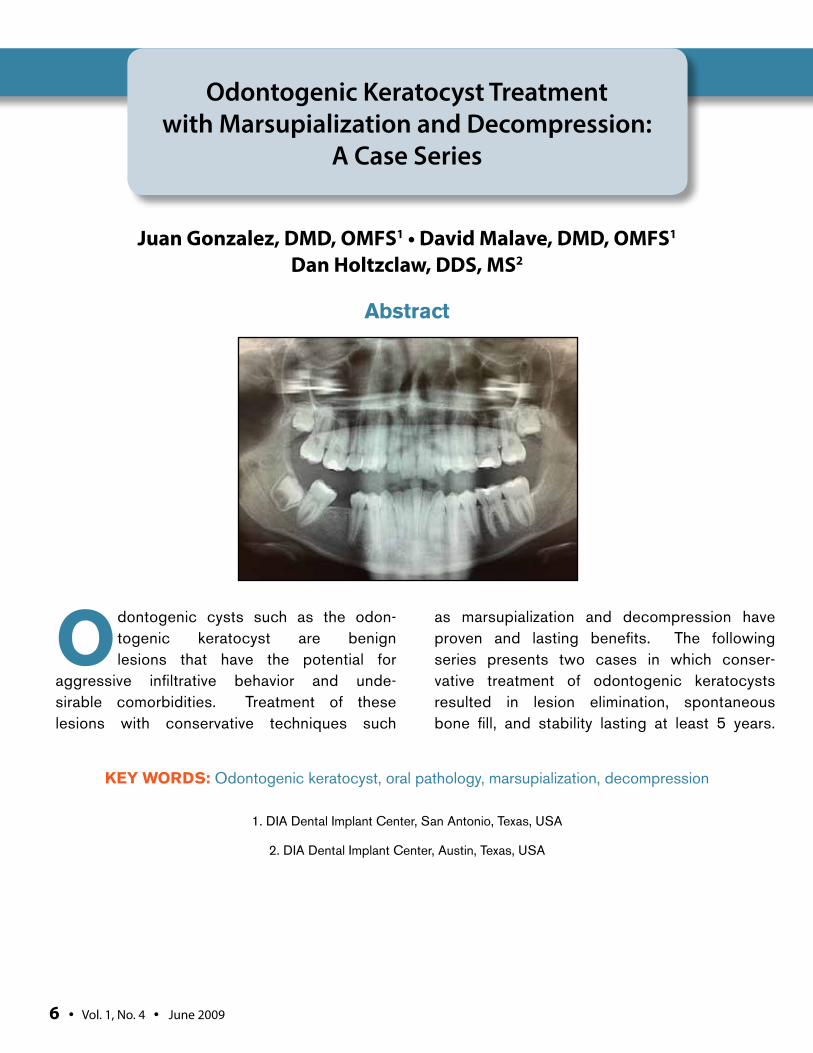
as marsupialization and decompression have proven and lasting benefits. The following series presents two cases in which conser-vative treatment of odontogenic keratocysts resulted in lesion elimination, spontaneous bone fill, and stability lasting at least 5 years.
Odontogenic Keratocyst Treatment with Marsupialization and Decompression:
A Case Series
Juan Gonzalez, DMD, OMFS1 • David Malave, DMD, OMFS1
Dan Holtzclaw, DDS, MS2
1. DIA Dental Implant Center, San Antonio, Texas, USA
2. DIA Dental Implant Center, Austin, Texas, USA
Abstract
KEY WORDS: Odontogenic keratocyst, oral pathology, marsupialization, decompression
6 • Vol. 1, No. 4 • June 2009

Gonzalez et al
The Journal of Implant & Advanced Clinical Dentistry • 7
Gonzales et al
BACKGROUNDOdontogenic keratocyst tumors are benign devel-opmental odontogenic lesions that originate from the basal layer of oral epithelium or remnants of the dental lamina.1 The lesion was originally described in 1956 by Philipsen as keratocyst odontogenic tumor (KCOT),2 but is commonly referred to as odontogenic keratocyst in contem-porary literature.3,4 The World Health Organiza-tion (WHO) designates odontogenic keratocysts as benign unicystic, intra-osseous tumors of odontogenic origins, with a characteristic lining of parakeratinized epithelium, potential for infil-trative aggressive behavior, and a possible high recurrence rate.5 Odontogenic keratocysts are often initially recognized upon radiographic eval-uation with presentation as unilocular or multi-locular well-circumscribed radiolucent lesions surrounded by sclerotic borders.6 These lesions are most commonly seen in the posterior man-dible and/or ascending ramus in patients rang-ing in age from late teens to forties.7 Signs and
symptoms of odontogenic keratocysts include, but are not limited to, the following: pain, edema, cellulitis, purulent discharge, trismus, altered neu-ral sensation, and trigeminal neuralgia.8,9 Odon-togenic keratocysts account for up to 14% of all odontogenic cysts of the jaw and have recur-rence rates varying from 5-62%.7,10,11 The follow-ing article documents two cases in which patients who were ultimately diagnosed with odonto-genic keratocysts were successfully treated and have had no lesion recurrence to date.
MATERIALS AND METHODSThis article documents the treatment of two patients that were referred to our Oral and Maxil-lofacial Surgery Clinic for evaluation of suspicious radiolucent lesions in the posterior mandible. Patient A was a 54 year old female with an unre-markable medical history. Panoramic radiograph revealed full-bony impacted tooth #17 with a well-circumscribed radiolucent lesion encompassing the distal half of the tooth and extending into the
Figure 1: Panoramic radiograph from Patient 1 displaying well-circumscribed radiolucent lesion encompassing the distal half of the tooth and extending into the ascending ramus.
Figure 2: Decompression stent secured to Patient 1 during marsupialization and decompression treatment.
8 • Vol. 10, No. 4 • May/June 2018
ascending ramus (Figure 1). The patient reported occasional pain and pressure in the area. Upon clinical and radiographic examination, the patient was presented with a differential diagnosis of odontogenic keratocyst, dentigerous cyst, and/or ameloblastoma and treatment recommenda-tions of removal and biopsy. The patient accepted the treatment plan and following a standard his-tory and physical examination, the patient was consented for surgery. Upon the establishment of intravenous sedation and local anesthesia, the lesion at site #17 was treated with decompres-sion, marsupialization, and tooth extraction. A decompression stent was sutured into the lesion to allow for the reduction of intramural pressure and to stimulate bone formation within the lesion (Figure 2). The patient experienced no post-sur-gical complications and the stent was removed during a subsequent follow-up visit. Histological analysis of the lesion resulted in a diagnosis of odontogenic keratocyst. The patient was informed of the findings and that periodic follow-up assess-
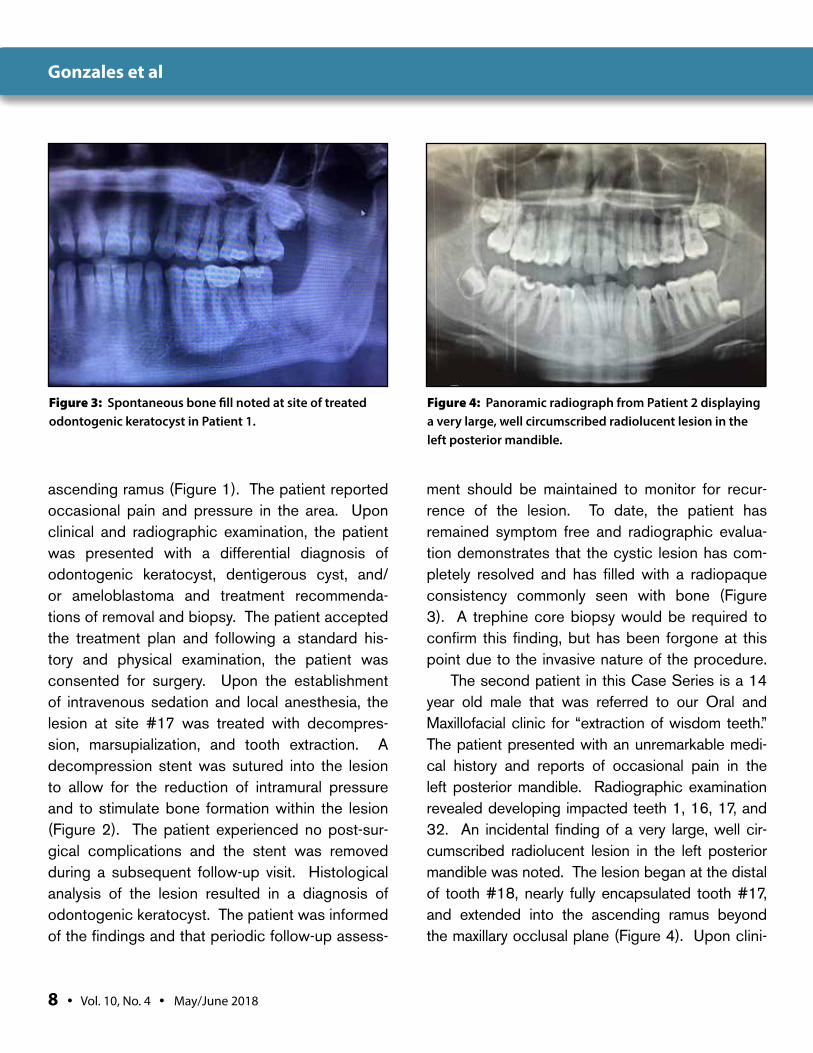
ment should be maintained to monitor for recur-rence of the lesion. To date, the patient has remained symptom free and radiographic evalua-tion demonstrates that the cystic lesion has com-pletely resolved and has filled with a radiopaque consistency commonly seen with bone (Figure 3). A trephine core biopsy would be required to confirm this finding, but has been forgone at this point due to the invasive nature of the procedure.
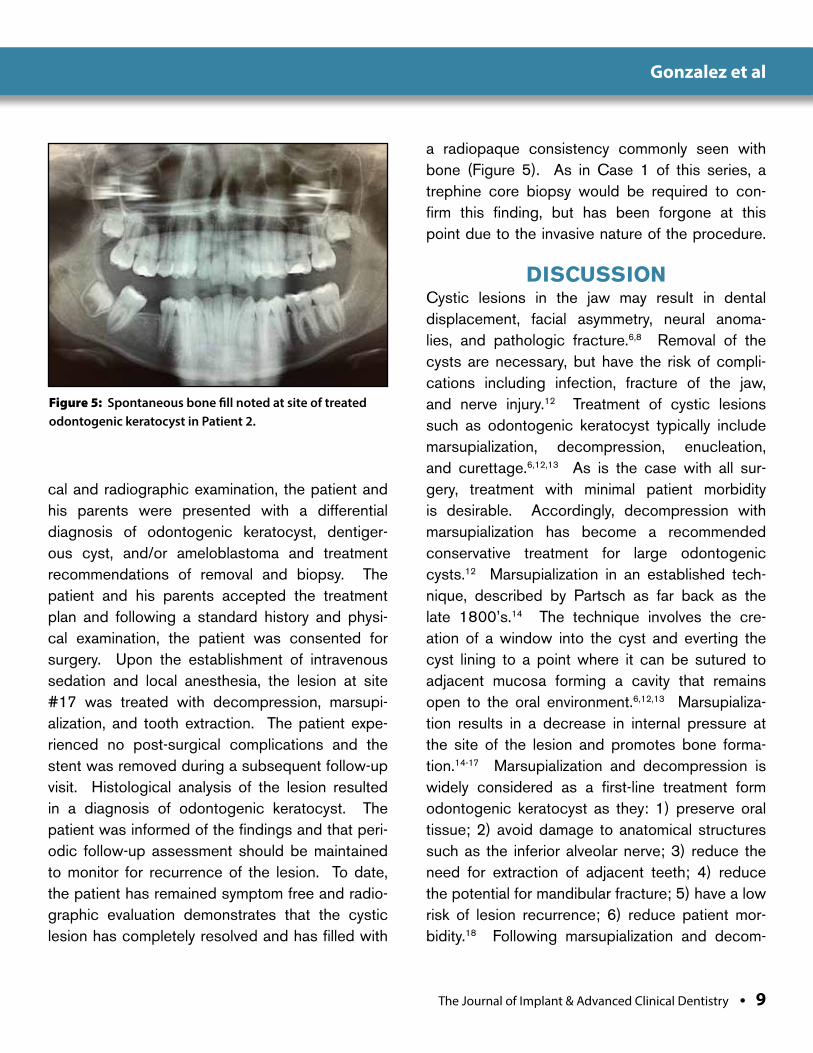
The second patient in this Case Series is a 14 year old male that was referred to our Oral and Maxillofacial clinic for “extraction of wisdom teeth.” The patient presented with an unremarkable medi-cal history and reports of occasional pain in the left posterior mandible. Radiographic examination revealed developing impacted teeth 1, 16, 17, and 32. An incidental finding of a very large, well cir-cumscribed radiolucent lesion in the left posterior mandible was noted. The lesion began at the distal of tooth #18, nearly fully encapsulated tooth #17, and extended into the ascending ramus beyond the maxillary occlusal plane (Figure 4). Upon clini-
Figure 3: Spontaneous bone fill noted at site of treated odontogenic keratocyst in Patient 1.
Figure 4: Panoramic radiograph from Patient 2 displaying a very large, well circumscribed radiolucent lesion in the left posterior mandible.
Gonzales et al
The Journal of Implant & Advanced Clinical Dentistry • 9
cal and radiographic examination, the patient and his parents were presented with a differential diagnosis of odontogenic keratocyst, dentiger-ous cyst, and/or ameloblastoma and treatment recommendations of removal and biopsy. The patient and his parents accepted the treatment plan and following a standard history and physi-cal examination, the patient was consented for surgery. Upon the establishment of intravenous sedation and local anesthesia, the lesion at site #17 was treated with decompression, marsupi-alization, and tooth extraction. The patient expe-rienced no post-surgical complications and the stent was removed during a subsequent follow-up visit. Histological analysis of the lesion resulted in a diagnosis of odontogenic keratocyst. The patient was informed of the findings and that peri-odic follow-up assessment should be maintained to monitor for recurrence of the lesion. To date, the patient has remained symptom free and radio-graphic evaluation demonstrates that the cystic lesion has completely resolved and has filled with
a radiopaque consistency commonly seen with bone (Figure 5). As in Case 1 of this series, a trephine core biopsy would be required to con-firm this finding, but has been forgone at this point due to the invasive nature of the procedure.
DISCUSSION Cystic lesions in the jaw may result in dental displacement, facial asymmetry, neural anoma-lies, and pathologic fracture.6,8 Removal of the cysts are necessary, but have the risk of compli-cations including infection, fracture of the jaw, and nerve injury.12 Treatment of cystic lesions such as odontogenic keratocyst typically include marsupialization, decompression, enucleation, and curettage.6,12,13 As is the case with all sur-gery, treatment with minimal patient morbidity is desirable. Accordingly, decompression with marsupialization has become a recommended conservative treatment for large odontogenic cysts.12 Marsupialization in an established tech-nique, described by Partsch as far back as the late 1800’s.14 The technique involves the cre-ation of a window into the cyst and everting the cyst lining to a point where it can be sutured to adjacent mucosa forming a cavity that remains open to the oral environment.6,12,13 Marsupializa-tion results in a decrease in internal pressure at the site of the lesion and promotes bone forma-tion.14-17 Marsupialization and decompression is widely considered as a first-line treatment form odontogenic keratocyst as they: 1) preserve oral tissue; 2) avoid damage to anatomical structures such as the inferior alveolar nerve; 3) reduce the need for extraction of adjacent teeth; 4) reduce the potential for mandibular fracture; 5) have a low risk of lesion recurrence; 6) reduce patient mor-bidity.18 Following marsupialization and decom-
Figure 5: Spontaneous bone fill noted at site of treated odontogenic keratocyst in Patient 2.
Gonzalez et al

10 • Vol. 10, No. 4 • May/June 2018
pression, debate exists whether or not to graft the resultant intrabony defect with bone augmenta-tion. Various studies have demonstrated sponta-neous bone regeneration following the removal of large cystic lesions in the absence of bone aug-mentation. A study by Chiapasco et al. in the year 2000 noted 48% bony defect healing at 12 months and 91% healing at 24 months via spon-taneous bone regeneration after removal of large mandibular cysts.19 A 2015 study by Chacko et al. examined 44 patients treated with removal of large jaw cysts and found a reduction in cyst size via spontaneous bone regeneration by 28.85% at 6 months, 57.13% at 9 months, 81.03% at 12 months, and 100% at 24 months.20 In the current Case Series, we noted complete and spontane-ous bone fill in the sites of the treated odonto-genic keratocysts at follow-up visits over 5 years. Recurrence rates following the removal of odon-togenic keratocysts vary greatly from 5-62% and are more common in the first 5-7 years after treat-ment.7,10,11 Accordingly, annual follow-up is recom-mended with radiographic evaluation to monitor for recurrence. To date, the patients in our Case Series have displayed no symptoms of lesion recurrence after time periods of up to 3 years.
CONCLUSIONOdontogenic keratocysts are benign developmen-tal odontogenic lesions that have the potential to create significant co-morbidities if left untreated. Conservative treatment with marsupialization and decompression offers a way to manage these lesions with minimal trauma to the patient. l
Correspondence:Dr. Juan [email protected]
DisclosureThe authors report no conflicts of interest with anything mentioned in this article.
References1. Kramer IR, Pindborg JJ, Shear M. The WHO Histological Typing
of Odontogenic Tumours. A commentary on the Second Edition. Cancer 1992; 15;70(12):2988-94.
2. Philipsen H. On keratocysts in the jaws. Tandlaegebladet. 1956;60:963-981.3. Asevedo Campos de Resende T, de Fátima Bernardes V, Carolina da Silva
J, De Marco LA, Santiago Gomez R, Cavalieri Gomes C, Gonçalves Diniz M. Loss of heterozygosity of MIR15A/MIR16-1, negative regulators of the antiapoptotic gene BCL2, is not common in odontogenic keratocysts. Oral Surg Oral Med Oral Pathol Oral Radiol 2018; 125(4):313-316.
4. Doramacı EJ, Rossi-Fedele G. Odontogenic keratocyst: the pitfalls of uncoordinated multidisciplinary care. Am J Orthod Dentofacial Orthop 2018;153(2):167.
5. de Avila ED1, de Molon RS, Massucato EM, Hochuli-Vieira E. Relationship between the prevalence of the dentigerous cyst and the odontogenic keratocyst tumor and the current etiologic hypothesis. J Craniofac Surg 2009;20(6):2036-40.
6. de Molon RS, Verzola MH, Pires LC, Mascarenhas VI, da Silva RB, Cirelli JA, Barbeiro RH. Five years follow-up of a keratocyst odontogenic tumor treated by marsupialization and enucleation: A case report and literature review. Contemp Clin Dent 2015;6(Suppl 1):106-110.
7. Titinchi F, Nortje CJ. Keratocystic odontogenic tumor: a recurrence analysis of clinical and radiographic parameters. Oral Surg Oral Med Oral Pathol Oral Radiol 2012;114(1):136-142.
8. Forssell K, Kallioniemi H, Sainio P. Microcysts and epithelial islands in primoridal cysts.Proc Finn Dent Soc 1979;75(5-6):99-102.
9. Gopalkrishna AA, Tejasree BN, Manjunath M, Ashwin DP. Trigeminal neuralgia induced by odontogenic keratocyst associated with impacted supernumerary teeth: A rare case report. J Oral Maxillofac Pathol 2018;22(Suppl 1):135-140.
10. Kaczmarzyk T, Mojsa I, Stypulkowska J. A systematic review of the recurrence rate for keratocystic odontogenic tumour in relation to treatment modalities. Int J Oral Maxillofac Surg 2012;41(6):756-767.
11. Bhargava D, Deshpande A, Pogrel MA. Keratocystic odontogenic tumour (KCOT)--a cyst to a tumour. Oral Maxillofac Surg 2012; 16(2):163-170.
12. Sun Y, Zhang J, Qian N, Sima G, Zhang J, Zhong J, Guo Z, Chen Y, Dong W. Comparison of the osteogenic differentiation of orofacial bone marrow stromal cells prior to and following marsupialization in patients with odontogenic cyst. Mol Med Rep 2018;17(1):988-994.
13. Oliveros-Lopez L, Fernandez-Olavarria A, Torres-Lagares D, Serrera-Figallo MA, Castillo-Oyagüe R, Segura-Egea JJ, Gutierrez-Perez JL. Reduction rate by decompression as a treatment of odontogenic cysts. Med Oral Patol Oral Cir Bucal 2017;22(5):643-650.
14. Partsch C. Zur behandlung der kieferzystem. Dtsch Monatssch Zahnkeilkd 1910. 28:252-20.
15. Goyal S, Sharma S, Kotru M, Gupta N. Role of FNAC in the diagnosis of intraosseous jaw lesions. Med Oral Patol Oral Cir Bucal 2015;1;20(3):284-291.
16. Shudou H, Sasaki M, Yamashiro T, Tsunomachi S, Takenoshita Y, Kubota Y, Ninomiya T, Kawazu T, Mori Y. Marsupialisation for keratocystic odontogenic tumours in the mandible: longitudinal image analysis of tumour size using 3D visualised CT scans. Int J Oral Maxillofac Surg 2012;41(3):290-296.
17. Wushou A, Zhao YJ, Shao ZM. Marsupialization is the optimal treatment approach for keratocystic odontogenic tumour. J Craniomaxillofac Surg 2014;42(7):1540-1544.
18. Pogrel MA, Jordan RC. Marsupialization as a definitive treatment for the odontogenic keratocyst. J Oral Maxillofac Surg 2004;62(6):651-655.
19. Chiapasco M, Rossi A, Motta JJ, Crescentini M. Spontaneous bone regeneration after enucleation of large mandibular cysts: a radiographic computed analysis of 27 consecutive cases. J Oral Maxillofac Surg 2000;58(9):942-948.
20. Chacko R, Kumar S, Paul A, Arvind. Spontaneous Bone Regeneration after Enucleation of Large Jaw Cysts: A Digital Radiographic Analysis of 44 Consecutive Cases. J Clin Diag Res 2015;9(9):84-89.
Gonzales et al

The Journal of Implant & Advanced Clinical Dentistry • XX
Gonzalez et al
Maksoud et al
Background: Three-dimensional bio printing of tissues and biological structures has been pro-posed to enable precise manufacture of various biomaterials with complex 3D architectures, while being compatible with multiple cell sources and being customizable to patient-specific needs. As the fabrication of scaffolds upon which cells attach, migrate, and proliferate is already in use, printing of a bone scaffold that matches the mechanical properties of bone is still in its early stages. The binding agent or bioink binds the par-ticles as an adhesive and determines the physi-cal properties of a construct. Although different
bioinks have been introduced , the combination of cellulose nanofibers and alginate has not been tested yet with beta tricalcium phosphate (TCP).
Methods: This test will evaluate a printed bone scaffolds using beta tri cal-cium phosphate and cellulose nanofi-bers in addition to alginate as a bioink.
Results and Conclusion: The construct developed presented with mechanical stiff-ness that can be transported to an intra-oral bone defect and secured to the recipient site.
3-D Printing of a Customized Bone Scaffold using Beta- Tricalcium-Phosphate, Alginate,
and Cellulose Nanofibers: A Novel Test
Mohamed Maksoud DMD1 • Kevin Guze DMD1
1. Harvard University School of Dental Medicine, Oral Medicine Infection and Immunity, Boston, Massachusetts, USA.
Abstract
KEY WORDS: 3-D bioprinting, alveolar defects, beta-tricalcium-phosphate
12 • Vol. 10, No. 4 • May/June 2018
Maksoud et al
The Journal of Implant & Advanced Clinical Dentistry • 13
Maksoud et al
INTRODUCTIONThrough the ages, biological materials have been used to treat surgical bone defects of the maxilla and the mandible.1-5 These range from autog-enous, xenografts to allografts and other non-resorbable materials that can demonstrate wound closure. However, this closure typically occurs in a slow manner which eventually results in exposure of the bone graft mass and graft loss or infection.6
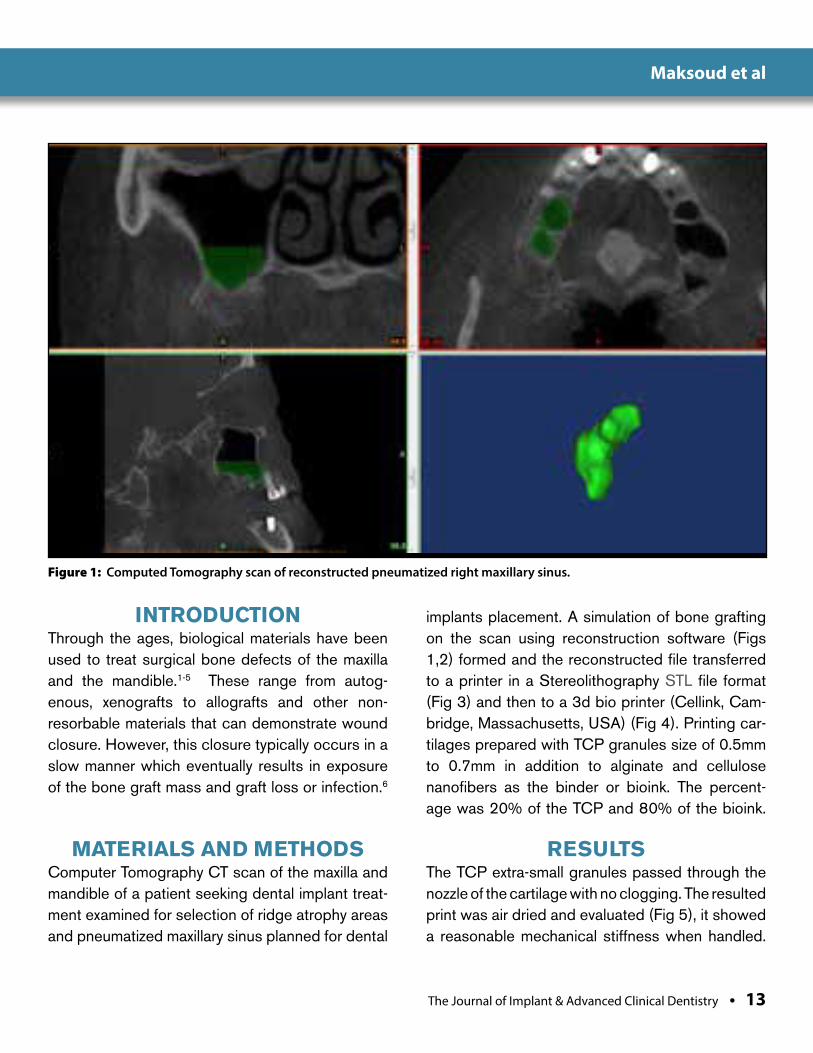
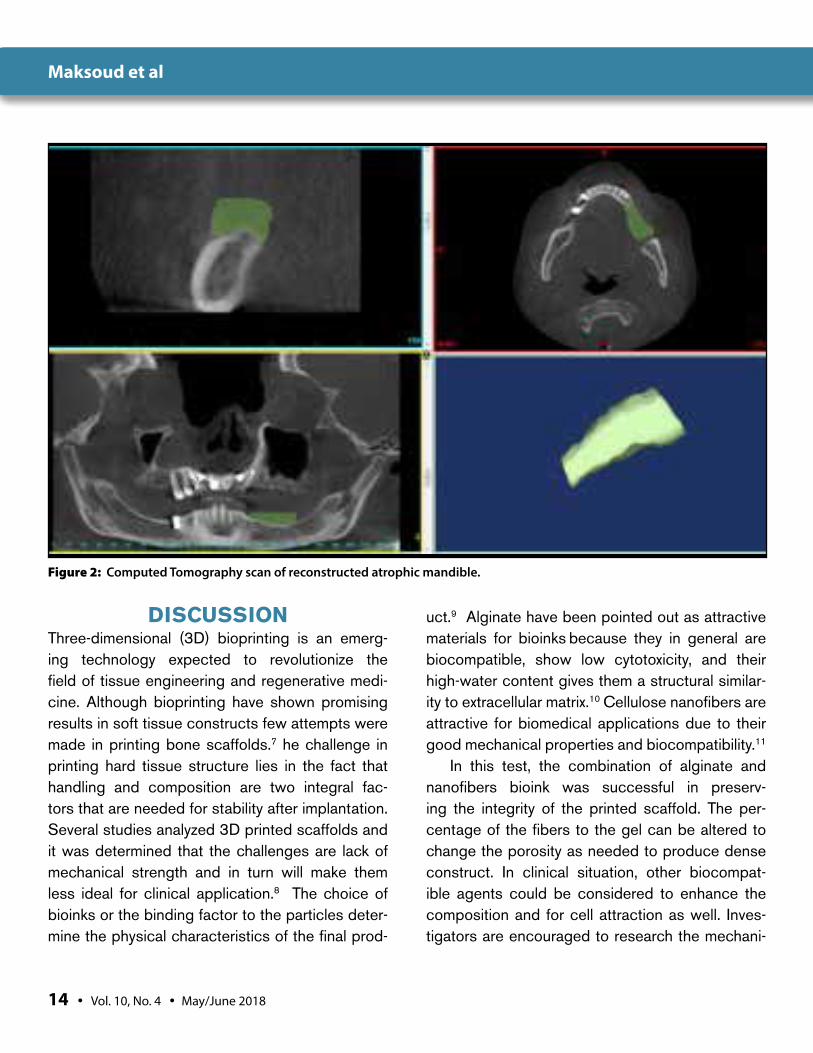
MATERIALS AND METHODSComputer Tomography CT scan of the maxilla and mandible of a patient seeking dental implant treat-ment examined for selection of ridge atrophy areas and pneumatized maxillary sinus planned for dental
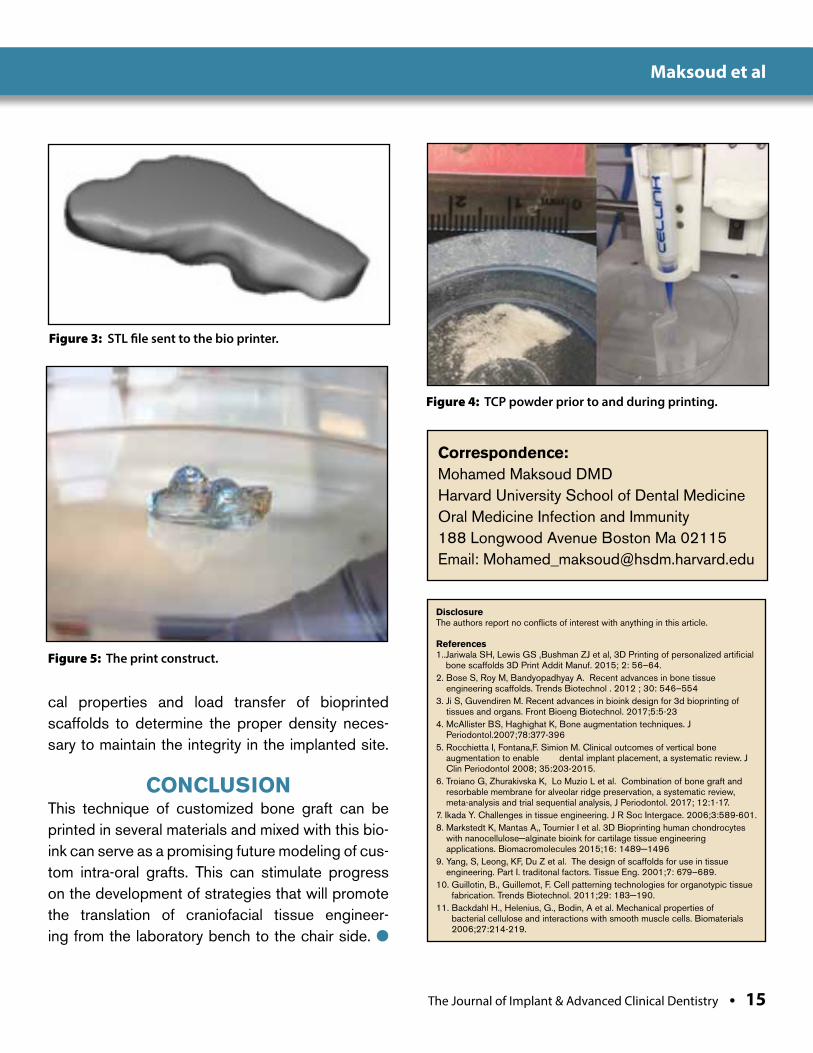
implants placement. A simulation of bone grafting on the scan using reconstruction software (Figs 1,2) formed and the reconstructed file transferred to a printer in a Stereolithography STL file format (Fig 3) and then to a 3d bio printer (Cellink, Cam-bridge, Massachusetts, USA) (Fig 4). Printing car-tilages prepared with TCP granules size of 0.5mm to 0.7mm in addition to alginate and cellulose nanofibers as the binder or bioink. The percent-age was 20% of the TCP and 80% of the bioink.
RESULTSThe TCP extra-small granules passed through the nozzle of the cartilage with no clogging. The resulted print was air dried and evaluated (Fig 5), it showed a reasonable mechanical stiffness when handled.
Figure 1: Computed Tomography scan of reconstructed pneumatized right maxillary sinus.
14 • Vol. 10, No. 4 • May/June 2018
Maksoud et al
DISCUSSIONThree-dimensional (3D) bioprinting is an emerg-ing technology expected to revolutionize the field of tissue engineering and regenerative medi-cine. Although bioprinting have shown promising results in soft tissue constructs few attempts were made in printing bone scaffolds.7 he challenge in printing hard tissue structure lies in the fact that handling and composition are two integral fac-tors that are needed for stability after implantation. Several studies analyzed 3D printed scaffolds and it was determined that the challenges are lack of mechanical strength and in turn will make them less ideal for clinical application.8 The choice of bioinks or the binding factor to the particles deter-mine the physical characteristics of the final prod-
uct.9 Alginate have been pointed out as attractive materials for bioinks because they in general are biocompatible, show low cytotoxicity, and their high-water content gives them a structural similar-ity to extracellular matrix.10
Cellulose nanofibers are attractive for biomedical applications due to their good mechanical properties and biocompatibility.11
In this test, the combination of alginate and nanofibers bioink was successful in preserv-ing the integrity of the printed scaffold. The per-centage of the fibers to the gel can be altered to change the porosity as needed to produce dense construct. In clinical situation, other biocompat-ible agents could be considered to enhance the composition and for cell attraction as well. Inves-tigators are encouraged to research the mechani-
Figure 2: Computed Tomography scan of reconstructed atrophic mandible.
The Journal of Implant & Advanced Clinical Dentistry • 15
Maksoud et al
Figure 3: STL file sent to the bio printer.
Figure 4: TCP powder prior to and during printing.
Figure 5: The print construct.
cal properties and load transfer of bioprinted scaffolds to determine the proper density neces-sary to maintain the integrity in the implanted site.
CONCLUSIONThis technique of customized bone graft can be printed in several materials and mixed with this bio-ink can serve as a promising future modeling of cus-tom intra-oral grafts. This can stimulate progress on the development of strategies that will promote the translation of craniofacial tissue engineer-ing from the laboratory bench to the chair side. l
Correspondence:Mohamed Maksoud DMDHarvard University School of Dental MedicineOral Medicine Infection and Immunity188 Longwood Avenue Boston Ma 02115Email: [email protected]
DisclosureThe authors report no conflicts of interest with anything in this article.
References1.. Jariwala SH, Lewis GS ,Bushman ZJ et al, 3D Printing of personalized artificial
bone scaffolds 3D Print Addit Manuf. 2015; 2: 56–64.2. Bose S, Roy M, Bandyopadhyay A. Recent advances in bone tissue
engineering scaffolds. Trends Biotechnol . 2012 ; 30: 546–5543. Ji S, Guvendiren M. Recent advances in bioink design for 3d bioprinting of
tissues and organs. Front Bioeng Biotechnol. 2017;5:5-234. McAllister BS, Haghighat K, Bone augmentation techniques. J
Periodontol.2007;78:377-396 5. Rocchietta I, Fontana,F. Simion M. Clinical outcomes of vertical bone
augmentation to enable dental implant placement, a systematic review. J Clin Periodontol 2008; 35:203-2015.
6. Troiano G, Zhurakivska K, Lo Muzio L et al. Combination of bone graft and resorbable membrane for alveolar ridge preservation, a systematic review, meta-analysis and trial sequential analysis, J Periodontol. 2017; 12:1-17.
7. Ikada Y. Challenges in tissue engineering. J R Soc Intergace. 2006;3:589-601.8. Markstedt K, Mantas A,, Tournier I et al. 3D Bioprinting human chondrocytes
with nanocellulose−alginate bioink for cartilage tissue engineering applications. Biomacromolecules 2015;16: 1489−1496
9. Yang, S, Leong, KF, Du Z et al. The design of scaffolds for use in tissue engineering. Part I. traditonal factors. Tissue Eng. 2001;7: 679–689.
10. Guillotin, B., Guillemot, F. Cell patterning technologies for organotypic tissue fabrication. Trends Biotechnol. 2011;29: 183−190.
11. Backdahl H., Helenius, G., Bodin, A et al. Mechanical properties of bacterial cellulose and interactions with smooth muscle cells. Biomaterials 2006;27:214-219.
Mahesh et al
Aim: To observe role of antibiot-ics in the success of 860 implant cases.Materials and Methods: Single tooth replace-ment implants were placed following two-staged implant placement protocol under aseptic condi-tions. In the test group, 430 patients were ran-domly prescribed with an antibiotic, whereas in the control group 430 patients were randomly pre-scribed with a non-steroidal anti-inflammatory drug after implant procedure. Patients were scheduled for a regular check-up every 6 months. At the end of three years, 8 implants were lost from test group and 11 implants from the control group.
Results: Both the test and control groups showed the same results dur-ing healing and implant success. Conclusion: Prescribing antibiotics does not affect or assure implant successClinical Significance: The use of antibiotics has been largely mishandled by dental professionals, creating resistant strains and complicating the situation, which can be checked upon, as every procedure does not require an antibiotic dosage.
The Role of Antimicrobials in the Success Rate of Dental Implants
Dr. Lanka Mahesh1 • Dr. JL Calvo Guiardo2 Dr. Gregori Kurtzman3 • Dr. Sagrika Shukla4
1. Private practice, New Delhi, India
2. Full professor of Oral Surgery, UCAM, SPAIN
3. Private Practice, Silver Spring, Maryland, USA
Abstract
KEY WORDS: Antibiotics, drug resistance, implants, implant success, NSAID
16 • Vol. 10, No. 4 • May/June 2018
Mahesh et al
The Journal of Implant & Advanced Clinical Dentistry • 17
Mahesh et al
INTRODUCTIONSuccessful implant therapy constitutes all the aspects of a surgical procedure defining the process of osseointegration which implies “cell-friendly” materials to provide long last-ing esthetic and functional reliability.1 However, due to various reasons, implants fail and infec-tion is one of the main reasons causing peri-implantitis and ultimately failure of the implant. According to the consensus report of the sixth European workshop on periodontology there is limited data providing prevalence on Peri-implantitis.2 The authors stated that there are only three cross-sectional reports available, presenting information on only one implant system including six hundred and sixty-two subjects (3,413 implants) in one publication and 216 (987 implants) in another one. In two reports on the basis of bleeding upon probing and bone loss (after 1 year in function) repre-senting only one implant system, peri-implan-titis was identified in between 28% - 56% of subjects and in 12% to 43% of implant sites.2
In general, to prevent any infection, antibiot-icsare prescribed to the patient following dental implant surgery. Selman Waksman first used the word antibiotics as a noun in 1941 to describe any small molecule made by a microbe that antagonizes the growth of other microbes.3 But in the oral cavity with more than 700 microbes,4 will any antibiotic, if not specific will work in preventing any infection? When these should be prescribed? Usually peri-implantitis sets in after 1 year of implant placement but the pro-cess of destruction starts much earlier than the actual clinical presentation. The proper dose of a drug is the amount that produces the maxi-mum benefit with the least attendant harm.5,6
The correct dose should be sufficient enough in eliminating the infecting pathogens with mini-mal adverse effects. Blood concentration of the antibiotic should exceedthe minimal inhibitory concentration by a factor of 2-8 times to off-set tissue barriers that restrict the accessof the drug to the infected site.7 Currently, antimicro-bial therapy is given by a vigorous dosage for a short time till the clinical situation permits.5 Such a regimen is desirable since a major fac-tor in the success of most antimicrobial agents isthe height of the serum concentration of the drug and, by inference, the concentra-tion in the infectedtissue,8 reducing the patient risk for antibiotic-induced toxicity, allergy and selection of resistant microorganisms.
But will placing an implant in aseptic con-ditions will create infection? Important thing to understand here is that when an implant is placed in the alveolar bone, the body recog-nizes it as a foreign body and inflammation is initiated as a protective response, characterized by vascular dilatation, enhanced permeability of capillaries and leukocyte recruitment.9 In the late 19th century, Robert Koch and Louis Pas-teur proposed the germ theory, which identified microorganisms as major inducers of the acute inflammatory response.9 Even a small oral activ-ity such as tooth brushing/flossing/chewing is capable of inducing transient bacteremia so a wound and implant placement stands a stron-ger chance of causing it.10 More recently, acute inflammation has been accepted being as a physiological response that occurs in vascular-ized tissues to defend the host and to maintain homeostasis.9 It is only when this inflammatory mechanism fails to remove noxious materials, chronic disease and fibrosis develops.11 Recent
18 • Vol. 10, No. 4 • May/June 2018
advances show that this defense mechanism is an active and highly regulated biochemi-cal process that comprises a genus of endog-enous molecules, including resolvins, lipoxins, protectins and maresins, which actively drive the termination of inflammation.9 However the question still remains unanswered, that is if the body is capable enough of fighting an infection then do antibiotics play a role or no role at all in implant dentistry. For the same reason authors conducted a study with a sample size of 860 patients, where 430 patients were included in test group and 430 patients in control group.
SETTINGS AND DESIGNThis was a multi-centre study and the patients chosen were healthy without any signs and symptoms of systemic condition and/or under-going bone grafting and other ancillary pro-cedures. 860 patients were enrolled for the study where 430 were randomly prescribed with an antibiotic after the implant therapy and considered as test group whereas in control group 430 patients were randomly prescribed with a non-steroidal anti-inflammatory drug.
METHOD AND MATERIALSSurgical therapy of the patients was started after complete prophylaxis. Drugs used were Cap. Amoxicillin 500 mg TDS for 5 days after meals, patients who were allergic to Cap. Amox-icillin was prescribed one Tab. Ciprofloxicin 500 mg BD, after meals for 5 days and for pain con-trol Tab. Ibuprofen 400 mg TDS was prescribed.
Single tooth replacements Implants were placed following two-staged implant place-ment protocol under aseptic conditions. Patients were scheduled for a regular check-up in every 6 months. At the end of three years 8 implants were lost from test group and 11 implants from the control group.
STATISTICAL ANALYSIS Patients were randomly assigned for the statis-tical analysis. Pearson Chi-square value Statisti-cal analysis was done for the implants placed.
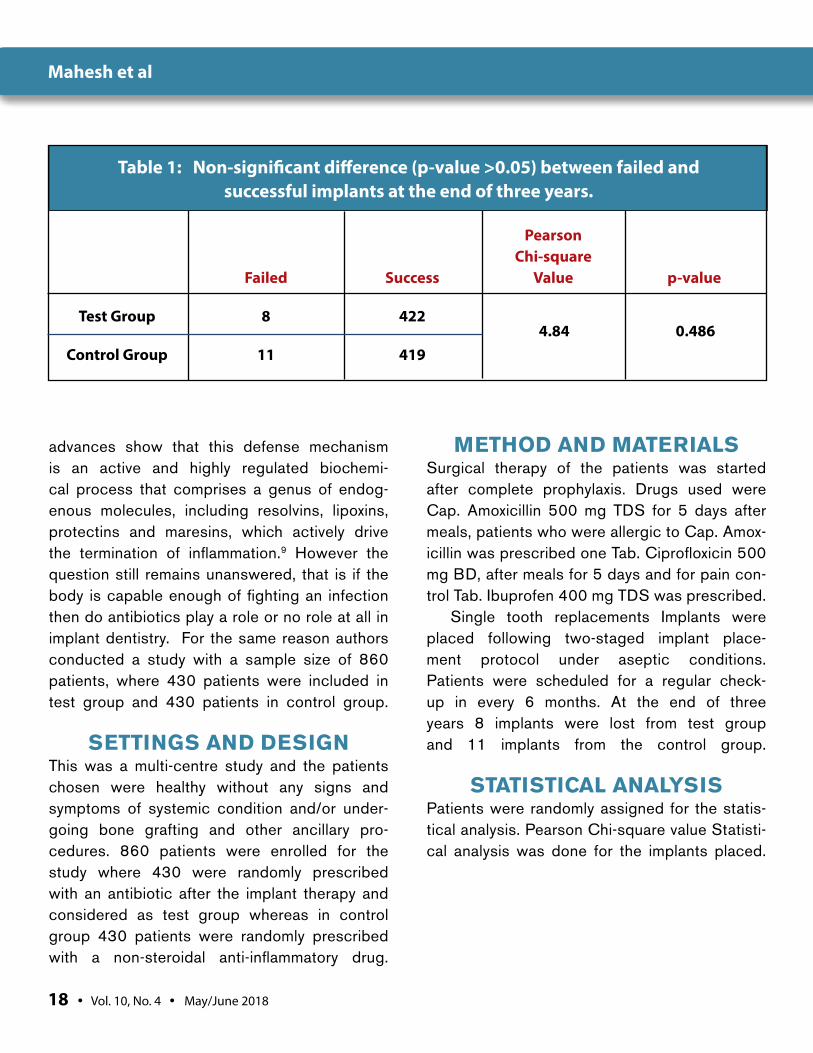
Table 1: Non-significant difference (p-value >0.05) between failed and successful implants at the end of three years.
Pearson Chi-square Failed Success Value p-value
Test Group 8 422
Control Group 11 419 4.84 0.486
Mahesh et al
The Journal of Implant & Advanced Clinical Dentistry • 19
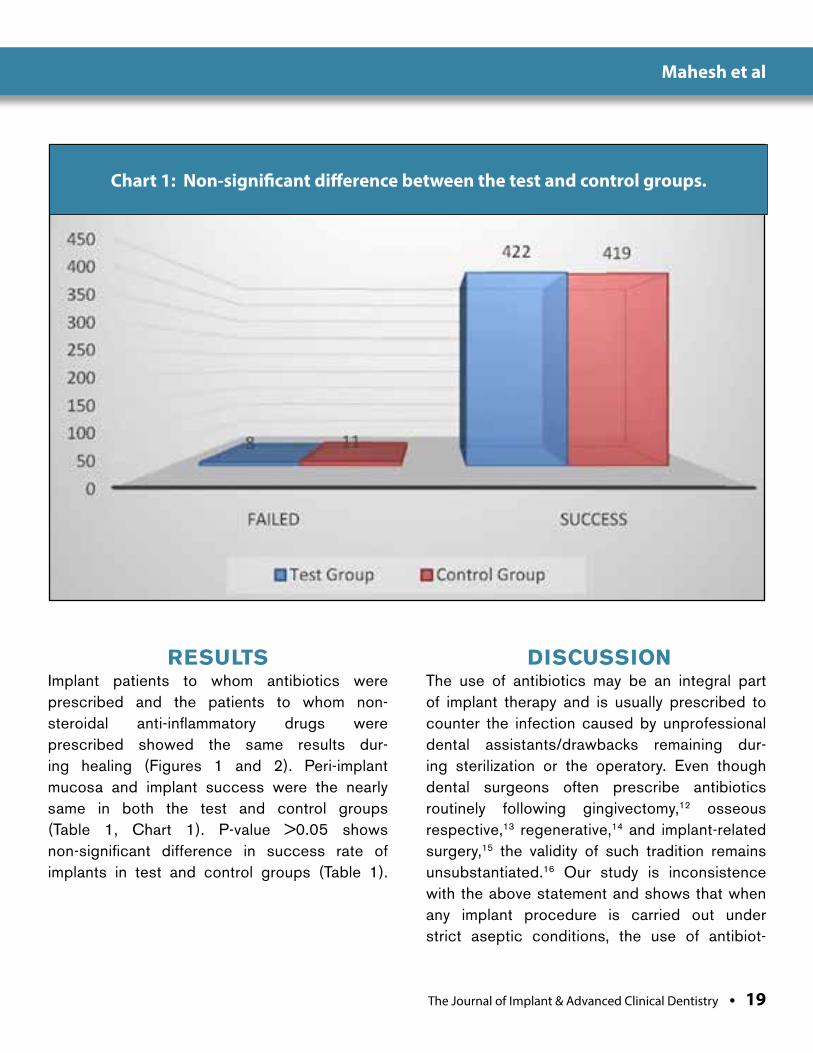
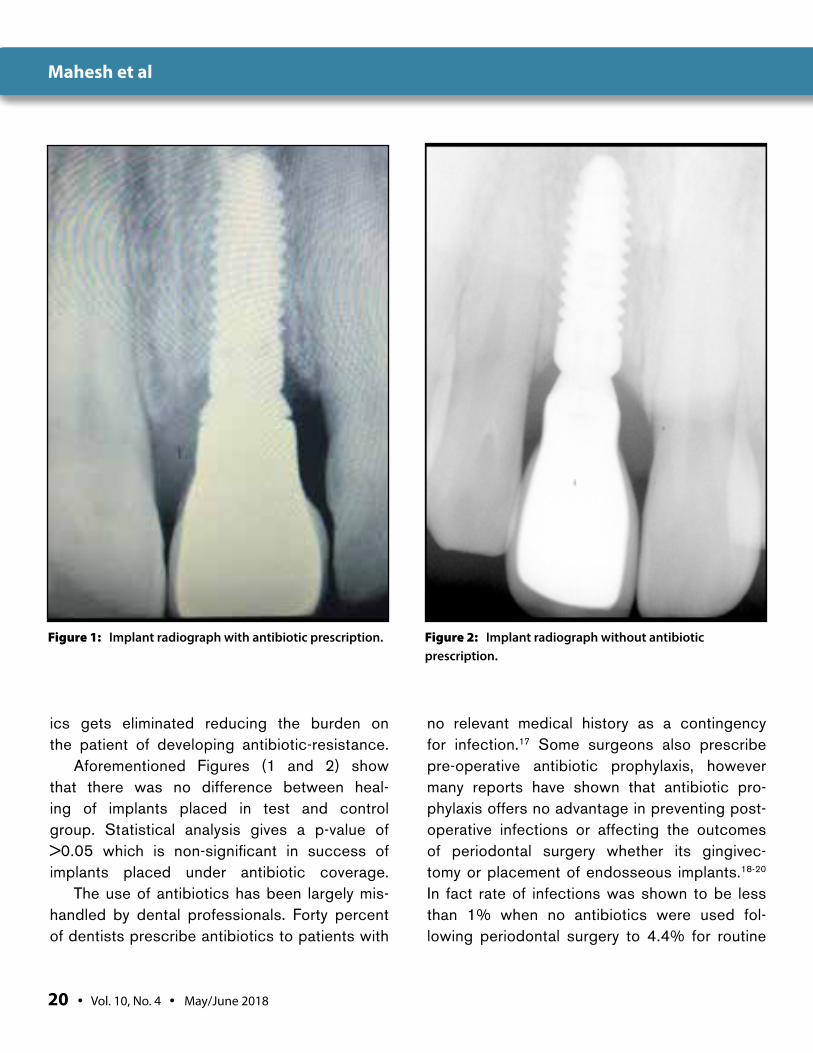
RESULTSImplant patients to whom antibiotics were prescribed and the patients to whom non-steroidal anti-inflammatory drugs were prescribed showed the same results dur-ing healing (Figures 1 and 2). Peri-implant mucosa and implant success were the nearly same in both the test and control groups (Table 1, Chart 1). P-value >0.05 shows non-significant difference in success rate of implants in test and control groups (Table 1).
DISCUSSIONThe use of antibiotics may be an integral part of implant therapy and is usually prescribed to counter the infection caused by unprofessional dental assistants/drawbacks remaining dur-ing sterilization or the operatory. Even though dental surgeons often prescribe antibiotics routinely following gingivectomy,12 osseous respective,13 regenerative,14 and implant-related surgery,15 the validity of such tradition remains unsubstantiated.16 Our study is inconsistence with the above statement and shows that when any implant procedure is carried out under strict aseptic conditions, the use of antibiot-
Chart 1: Non-significant difference between the test and control groups.
Mahesh et al
20 • Vol. 10, No. 4 • May/June 2018
ics gets eliminated reducing the burden on the patient of developing antibiotic-resistance.
Aforementioned Figures (1 and 2) show that there was no difference between heal-ing of implants placed in test and control group. Statistical analysis gives a p-value of >0.05 which is non-significant in success of implants placed under antibiotic coverage.
The use of antibiotics has been largely mis-handled by dental professionals. Forty percent of dentists prescribe antibiotics to patients with
no relevant medical history as a contingency for infection.17 Some surgeons also prescribe pre-operative antibiotic prophylaxis, however many reports have shown that antibiotic pro-phylaxis offers no advantage in preventing post-operative infections or affecting the outcomes of periodontal surgery whether its gingivec-tomy or placement of endosseous implants.18-20 In fact rate of infections was shown to be less than 1% when no antibiotics were used fol-lowing periodontal surgery to 4.4% for routine
Figure 1: Implant radiograph with antibiotic prescription. Figure 2: Implant radiograph without antibiotic prescription.
Mahesh et al

The Journal of Implant & Advanced Clinical Dentistry • 21
periodontal surgery and 4.5% when endos-seous implants were placed.18-20 Side-effects of antibiotics include severe anaphylaxis and development of drug resistant bacteria. Initially drug resistance was observed only in hospitals where antibiotics were used in large quantity, however, drug resistance is no more a local-ized entity and has extended beyond the con-fines of the hospital which can be traced from community to hospital and vice-versa.21 Resis-tant strains double the duration of hospital stay, double mortality and morbidity rates and also affect the cost of the treatment.21 Drug resis-tance genes can spread from one bacterium to another and is continuously evolving into new virulence toxin posing a threat on patient’s health.21 Due to these reasons it should not be considered as a choice of drug for signs of inflammation specially pain and edema.
Canadian Dental Association states that, “All dental procedures where significant oral bleeding and/or exposure to potentiallycon-taminated tissue occurs typically (will) require antibiotic prophylaxis.”22 The American Dental Association(ADA) also suggests similar guide-lines.23 Also, the American College of Surgeons and the AmericanHeart Association (AHA) guidelines24 suggests that complex oral sur-geries like implant placement will benefit from prophylactic antibiotic coverage; however, as of 2007, these associations currently suggest that only high and some moderate risk category patients should receive antibiotics.25 As afore-mentioned oral cavity inhabitants more than 700 species of bacteria, but out of these only few known cause infection and most of them have still not been isolated and cultured. Thus keep-ing side-effects of antimicrobials into account,
some leniency should be considered as one-stage, full mouth disinfection should be car-ried according to Quirynen et al.’s26 protocols. To further reduce the chance of infection, peri-oral structures should be disinfected with beta-dine solution. However Abu-Ta’a et al.27 stated that there is no correlation between peri-oral microbiology and post-operative infections. Uses of two independent suction tips decrease the chances of wound contamination through saliva.28 During surgery a meshed nose guard can be used which prevents contact with the highly contaminated nares, however it was dem-onstrated that the surrounding air of the oper-ating room contains more bacteria than the expired air.28 These methods including regular check-ups will prevent chances of peri-implan-titis and enhance success rate of implants.
CONCLUSIONThis study shows that antibiotics do not have any role in the implant success. Also stud-ies by various authors have shown that giv-ing prophylactic antimicrobial treatment or perioral disinfection does not play any role in post-operative treatment success. Thus the practice of prescribing unneces-sary antibiotics should be checked and other treatment options considered. l
Correspondence:Dr. Lanka [email protected]
Mahesh et al
22 • Vol. 10, No. 4 • May/June 2018
DisclosureThe authors report no conflicts of interest with anything mentioned in this article.
References1.1. Mahesh L, Narayan TV, Kurtzman G, Shukla S.
Microbiology of Peri-Implant Infections. Smile Dent J 2011;6:54-7.
2. Lindhe J, Meyle J. Peri-implant diseases: Consensus Report of the Sixth European Workshop on Periodontology. J ClinPeriodontol 2008;35:282–5.
3. Clardy J, Fischbach M, Currie C. The natural history of antibiotics. Curr Biol 2009;19:437–41.
4. Armellini D, Reynolds MA, Harro JM, Molly L. Biofilm formation on natural teeth and dental implants: what is the difference? In, Shirtliff M, Leid JG, Role of Biofilms in Device-Related Infections, Volume 3 of the series Springer Series on Biofilms, Berlin Heidelberg, 2009 Pp109-22.
5. Pallasch TJ. Pharmacokinetic principles of antimicrobial therapy. Periodontal 2000 1996;10:5-11.
6. Council Conference. Notes on the package insert. J Am Med Ass 1969:207:1335.
7. Neu HC. Current practices in antimicrobial dosing. Rev Infect Dis 1981:3:12-8.
8. Weinstein L. Some principles of antimicrobial therapy. Rational Drug Ther 1977;11:1-4.
9. Freire MO, Dyke TEV. Natural resolution of inflammation. Periodontol 2000 2013;63:149-64.
10. Bhanji S, Williams B, Sheller B, Elwood T, Mancl L. transient bacteremia induced by tooth brushing: a comparison of the Soni care toothbrush with a conventional toothbrush. Pediatr Dent 2002;24:295-99.
11. Van Dyke TE. Cellular and molecular susceptibility determinants for periodontitis. Periodontol 2000. 2007; 45:10–13.
12. Stahl SS, Soberman A, de Cesare A. Gingival healing. V. The effects of antibiotics administered during the early stages of repair. J Periodontol1969;40:521–3.
13. Kidd EA, WadeAB. Penicillin control of swelling and pain after periodontal osseous surgery. J ClinPeriodontol 1974;1:52–7.
14. Cortellini P, Bowers GM. Periodontal regeneration of intrabony defects: an evidence-based treatment approach. Int J Perio Rest Den1995;15:128–45.
15. Dent CD, Olson JW, Farish SE, Bellome J, Casino AJ, Morris HF, Ochi S. The influence of preoperative antibiotics on success of endosseous implants up to and including stage II surgery: a study of 2,641 implants. J Oral Maxillofac Surg 1997;55:19–24.
16. Abu-Ta’a M, Quirynen M, Teughels W, van Steenberghe D. Asepsis during periodontal surgery involving oral implants and the usefulness of peri-operative antibiotics: a prospective, randomized, controlled clinical trial. J Clin Periodontol 2008;35:58–63.
17. Ahmad N, Saad N. Effects of Antibiotics on Dental Implants: A Review. J Clin Med Res 2012;4:1-6.
18. Pack PD, Haber J. The incidence of clinical infection after periodontal surgery. A retrospective study. J Periodontol1983;54:441–3.
19. Checchi L,Trombelli L, Nonato M. Postoperative infections and tetracycline prophylaxis in periodontal surgery: a retrospective study. Quintessence Int1992;23:191–5.
20. Gynther GW, Kondell PA, Moberg LE, Heimdahl A. Dental implant installation without antibiotic prophylaxis. Oral Surg, Oral Med, Oral Path, Oral Radiol, Endodontics1998;85,509–11.
21. Levy SB, Marshall B. antibacterial resistance worldwide: cause, challenges and responses. Nature med 2004;10:122-9.
22. Canadian Dental Association. CDA Position on antibiotic prophylaxis for dental patients at risk. CDA-ADC Journal 2005.
23. Advisory statement. Antibiotic prophylaxis for dental patients with total joint replacements. American Dental Association; American Academy of Orthopaedic Surgeons. J Am Dent Assoc 1997;128:1004-8.
24. Dajani AS, Taubert KA, Wilson W, Bolger AF, Bayer A, Ferrieri P, Gewitz MH, et al. Prevention of bacterial endocarditis. Recommendations by the American Heart Association. J Am Med Ass 1997;277:1794-1801.
25. Ahmad N, Saad N. effects of antibiotics of dental implants: Areview. J clin med res 2012;4:1-6.
26. Quirynen M, Bollen CM, Vandekerckhove BN, Dekeyser C, Papaioannou W, Eyssen H. Full vs. partial–mouth disinfection in the treatment of periodontal infection: short term clinical and micribiological observation. J dent res 1995;74:1459-67.
27. Abu-Ta’a M, Quirynen M, Teughels W, van Steenberghe D. Asepsis during periodontal surgery involving oral implants and the usefulness of peri-operative antibiotics: a prospective, randomized, controlled clinical trial. J Clin Periodontol 2008;35:58–63.
28. Van Steenberghe D, Yoshida K, Papaioannou W, Bollen CM, Reybrouck G, Quirynen M. Complete nose coverage to prevent airborne contamination via nostrils is unnecessary. Clin Oral Implants Res 1997;8:512–16.
Mahesh et al
The Journal of Implant & Advanced Clinical Dentistry • XX
Mahesh et al
The Journal of Implant and Advanced Clinical Dentistry has been providing high quality, peer reviewed dental journals since 2007. We take pride in knowing that tens of thousands of readers around the world continue to read and contribute articles to JIACD. As you can imagine, there is a lot of expense involved in managing a top quality dental journal and we sincerely appreciate our advertisers purchasing ad space in both the journal and on the website which allows our monthly journals to continue to be free to all of our readers. In an e�ort to streamline our business practice and continue to provide no-fee, open access journals, JIACD is now sponsored exclusively by Osseofuse International Inc., a cutting edge dental implant company that provides exceptional implants and prosthetics and believes in the free distribution of information towards clinical advancements to dentists in the U.S. and around the world.
This generous sponsorship, which provides funding towards our operating expenses, allows JIACD to focus on the more important aspects of our journal; monthly publishing of relevant clinical practices.
As a reader or author of JIACD, nothing will change. In fact, readers will see less advertisements overall and authors can continue to submit articles relating to any clinical topic. We here at JIACD sincerely appreciate the continued �nancial support by Osseofuse International Inc., and are excited about the opportunity it a�ords. Thank you once again for your generous support.
Sincerely,
Leon Chen MD, MS, Co-Editor-in-Chief | Dave Beller, Director |The JIACD Team
International Inc.
Addanki
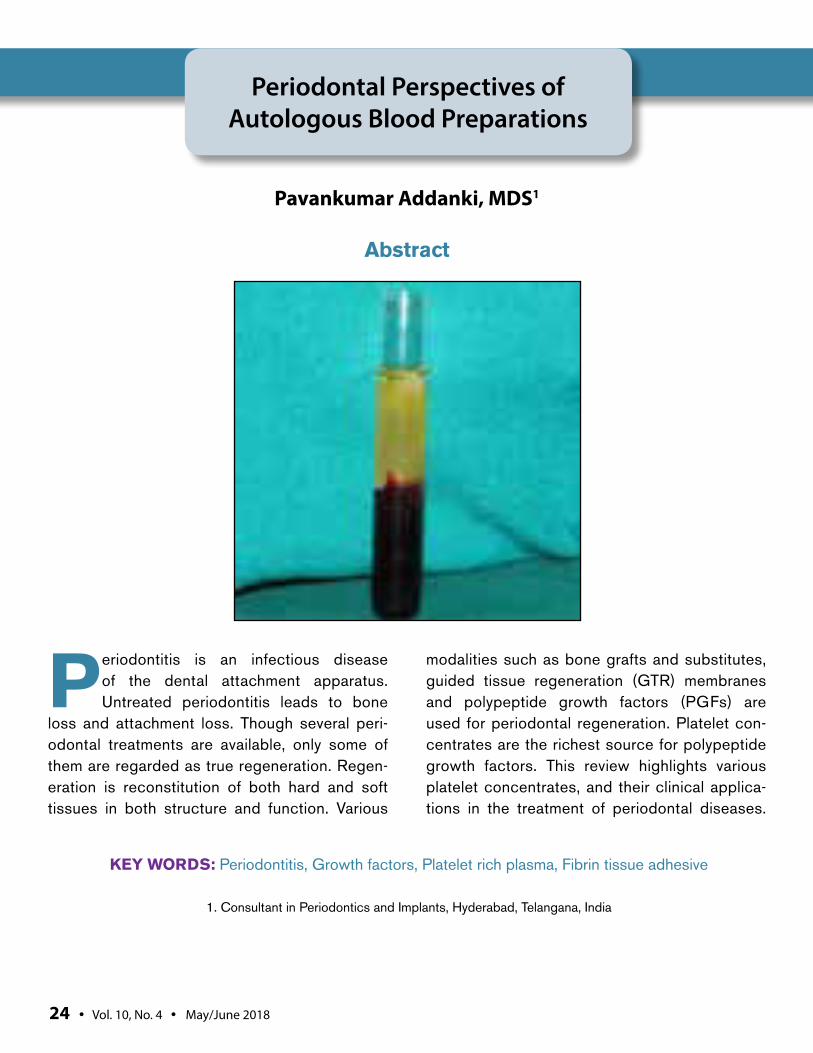
Periodontitis is an infectious disease of the dental attachment apparatus. Untreated periodontitis leads to bone
loss and attachment loss. Though several peri-odontal treatments are available, only some of them are regarded as true regeneration. Regen-eration is reconstitution of both hard and soft tissues in both structure and function. Various
modalities such as bone grafts and substitutes, guided tissue regeneration (GTR) membranes and polypeptide growth factors (PGFs) are used for periodontal regeneration. Platelet con-centrates are the richest source for polypeptide growth factors. This review highlights various platelet concentrates, and their clinical applica-tions in the treatment of periodontal diseases.
Periodontal Perspectives of Autologous Blood Preparations
Pavankumar Addanki, MDS1
1. Consultant in Periodontics and Implants, Hyderabad, Telangana, India
Abstract
KEY WORDS: Periodontitis, Growth factors, Platelet rich plasma, Fibrin tissue adhesive
24 • Vol. 10, No. 4 • May/June 2018

Addanki
The Journal of Implant & Advanced Clinical Dentistry • 25
Addanki
INTRODUCTIONPeriodontitis is an infectious disease causing destruction to periodontal tissues.1 The goal of periodontal therapy is the reconstitution of the periodontium in structure and function. Peri-odontal regeneration requires a series of bio-logic events including migration, proliferation and differentiation of cells in the process of wound healing.2 Platelets play a crucial role in hemosta-sis and wound healing. The Alpha granules of platelets release platelet-derived growth factor (PDGF), transforming growth factor (TGF-β),and insulin-like growth factor (IGF-I). During activa-tion, Alpha granules fuse with platelet cell mem-branes causing the release of growth factors. These growth factors bind to transmembrane receptors of target cells (Osteoblasts, fibroblasts, endothelial cells, and epithelial cells) leading to the expression of various genes, cell proliferation, collagen synthesis and osteoid formation.2 The combination of these actions results in the forma-tion of soft and hard tissues of periodontium.2
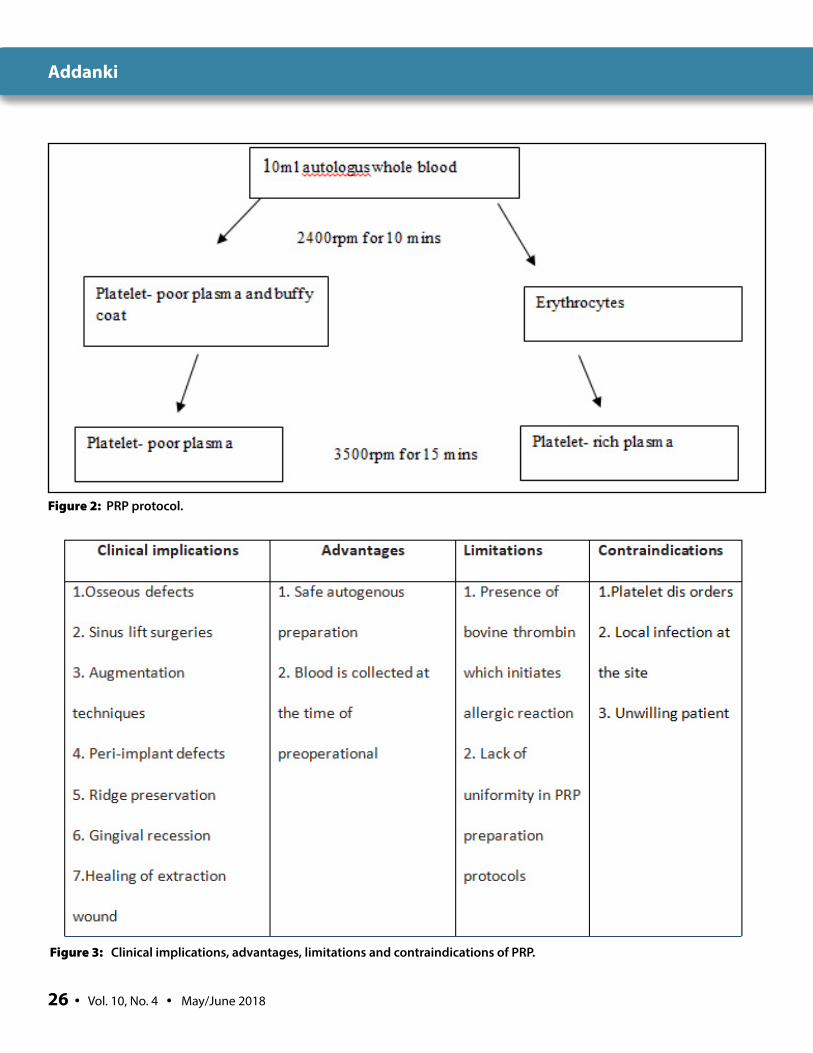
Platelet rich plasma (PRP)Marx first reported on the use of platelet rich plasma (PRP) in mandibular reconstruction defects.3 PRP is a first generation platelet con-centrate by-product of blood that is rich in plate-lets.4 It contains platelets, coagulation factors and plasma proteins (Fig. 1). Human blood clots contain 95% red blood cells (RBCs), 5% plate-lets, less than 1% white blood cells (WBCs), whereas a PRP blood clot contains 4% RBCs, 95% platelets, and 1% WBCs.4 PRP con-tains the maximum amount of platelets that can release desired growth factors (platelet derived growth factor (PDGF), transforming growth factors-β1 and -β2 (TGF-β1 and -β2) and insulin-like growth factor-1.5,6 The increased amount of growth factors enhance soft and hard tissue healing processes.5 The maturation rate dur-ing bone regenerative procedure is increased up to 2.16-times by PRP.6 PRP production requires blood collection with anticoagulant, 2 steps of centrifugation, and use of calcium chloride and bovine thrombin for polymerization (Fig. 2).7
Platelet Rich Fibrin (PRF) PRF is a second generation platelet concentrate
developed by Choukroun. 26 It is devoid of bovine thrombin which is seen in PRP preparation.26,27
The interaction between leukocytic cytokines and fibrin complex play a vital role in the regeneration. A physiological enriched fibrin complex matrix (PRF) releases growth factors in a controlled man-ner for longtime when compared to fibrin glue enriched with cytokines. The preparation of PRF is simple. A blood sample is taken in 10 ml tube without anticoagulant and centrifuged at 3,000 rpm for 10 mins. The coagulation process is natu-ral in a test tube as it is devoid of thrombin.27 It consists of 3 layers, upper layer-platelet poor
Figure 1: Platelet rich plasma.
26 • Vol. 10, No. 4 • May/June 2018
Addanki
Figure 2: PRP protocol.
Figure 3: Clinical implications, advantages, limitations and contraindications of PRP.
The Journal of Implant & Advanced Clinical Dentistry • 27
Addanki
plasma, middle layer- Fibrin clot with platelet, bot-tom layer-RBC (Figs. 5a, 5b). PRF contains cyto-kines such as IL-1, -4, -6, and growth factors such as Transforming Growth Factor beta 1 (TGF-β1), Platelet Derived Growth Factor (PDGF), and Vas-cular Endothelial Growth Factor (VEGF).28,29 PRF acts as a powerful scaffold with an integrated reservoir of growth factors for tissue regenera-tion. The fibrin matrix in PRF acts as natural guide for angiogenesis, natural support to immunity and guides the coverage of wounds (Fig. 5b). 27
Titanium-Prepared Platelet-Rich Fibrin (T-PRF)Some authors are worried about glass-evacuated blood collection tubes with silica particles as these particles may cause health hazards.53 Only a small fraction of these silica particles are sedi-mented with red blood cells. A majority of silica
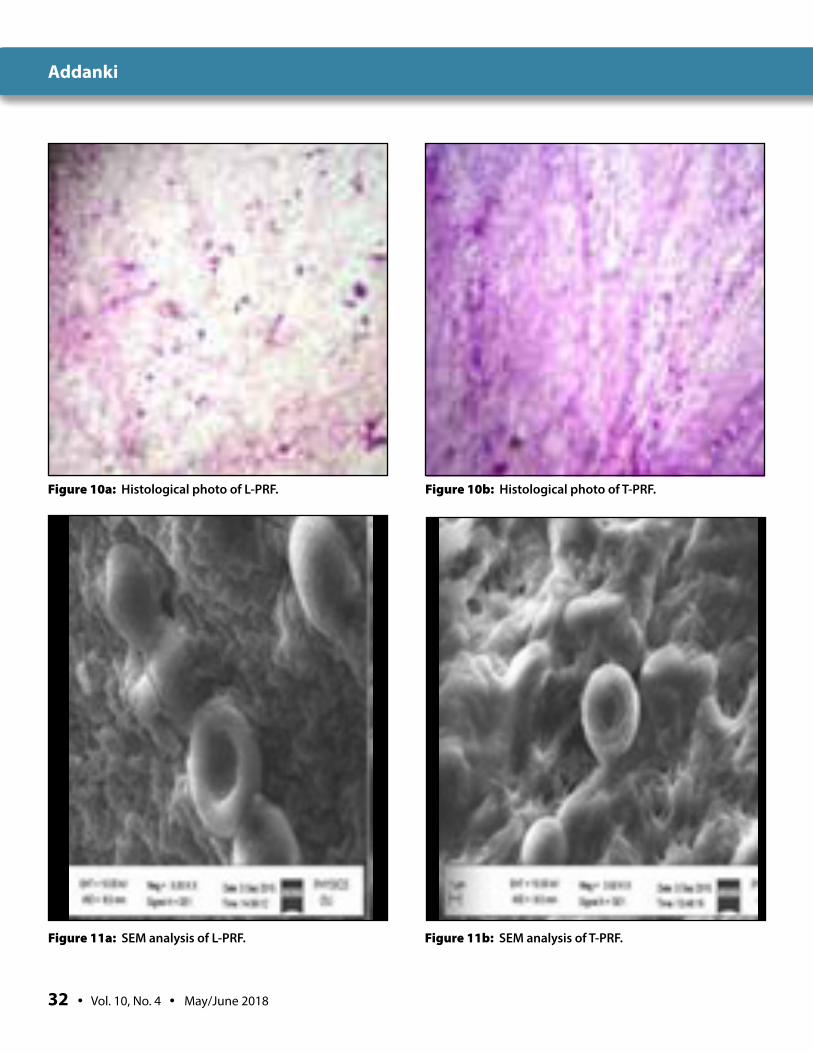
particles suspend in a buffy coat so that these particles reach may the patient when these prod-ucts are used for treatment.54 Although this is not practically concluded (the architecture of L-PRF change with type of material used for its prepara-tion), some authors have used more biocompat-ible material titanium for PRF preparation (Fig. 9). 55. Although basic histological structure simi-lar between T-PRF and L-PRF, there is some dif-ference in fibrin structure in T-PRF. The fibrin of T-PRF is more woven and thicker when compare with L-PRF. The difference may be due to the bio-compatibility and hemocompatibility of titanium, which led to the formation of a more polymerized fibrin (Figs. 10a, 10b, 11a, 11b).55 More research is required on T-PRF in terms of absorption time in body and clinical advantage over L-PRF.
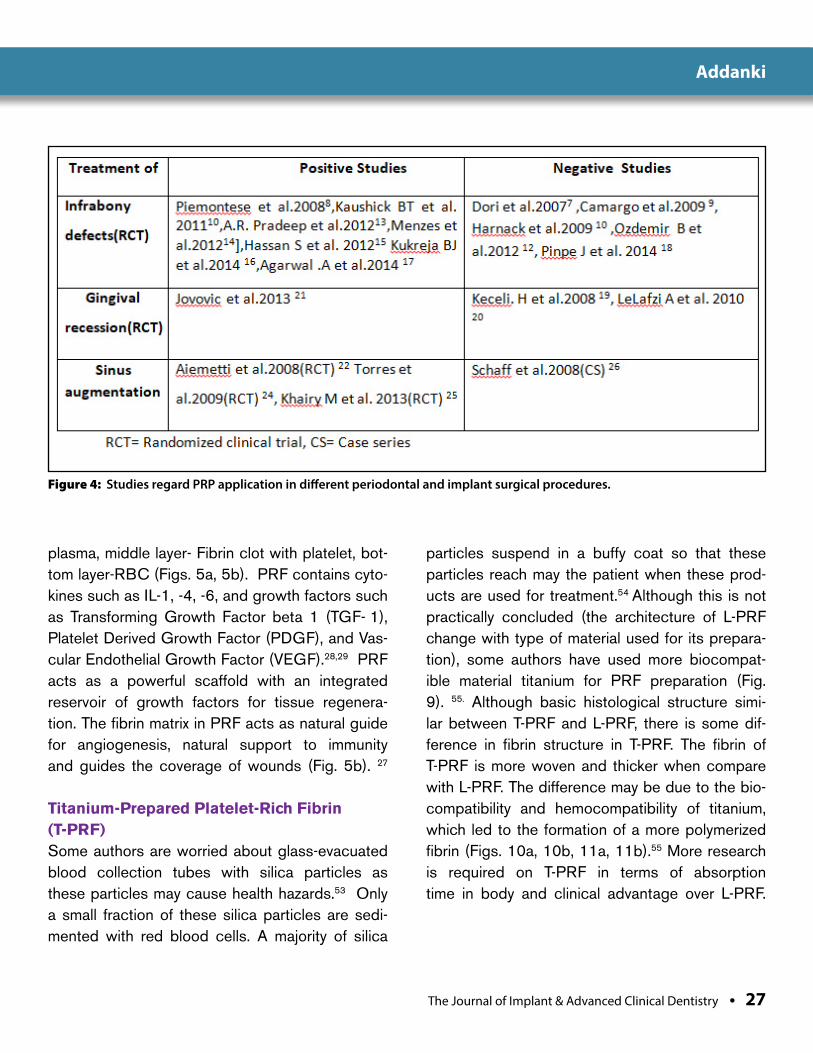
Figure 4: Studies regard PRP application in different periodontal and implant surgical procedures.

28 • Vol. 10, No. 4 • May/June 2018
Addanki
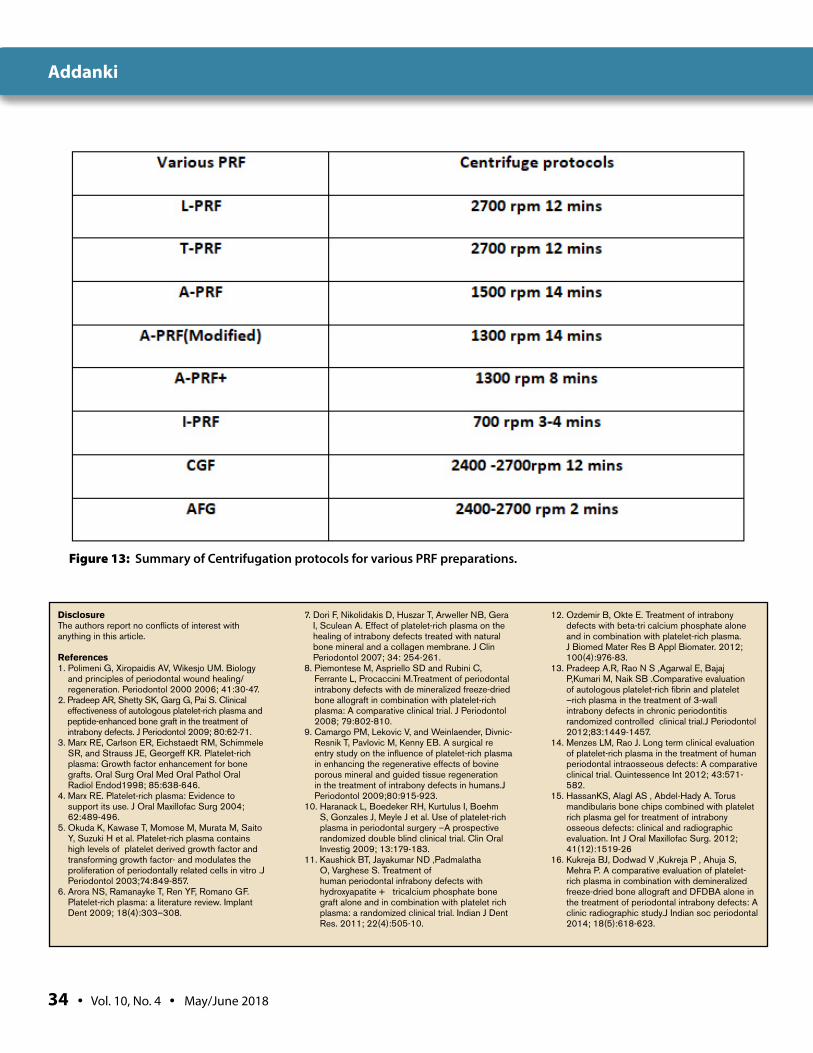
Advanced Platelet rich fibrin (A-PRF) and A-PRF+
A-PRF is a third generation platelet concentrate. The centrifugation protocol for advanced platelet rich fibrin (A-PRF) is 1500 rpm 14 mins. Later it was modified to 1300 rpm 14 mins. With the slower centrifugation protocol, it proved that presence of macrophages in Advanced plate-let rich fibrin. PRF clots formed with A-PRF cen-trifugation protocol showed a loose structure with more interfibrous space, and more cells in distal part of fibrin clot (Figs. 12a, 12b). More research is needed to find the effect of APRF on Periodontal Regeneration.56 Another varia-tion of A-PRF is called A-PRF+ which has a cen-trifugation protocol of 1300 rpm for 8 mins. Like A-PRF, it is also based on lower centrifugation protocol. More research is needed to find the effect of APRF+ on periodontal regeneration.57
Figure 5a: Platelet rich fibrin in test tube. Figure 5b: Platelet rich fibrin.
Figure 5c: Platelet rich fibrin mixed with bone graft.
The Journal of Implant & Advanced Clinical Dentistry • 29
Addanki
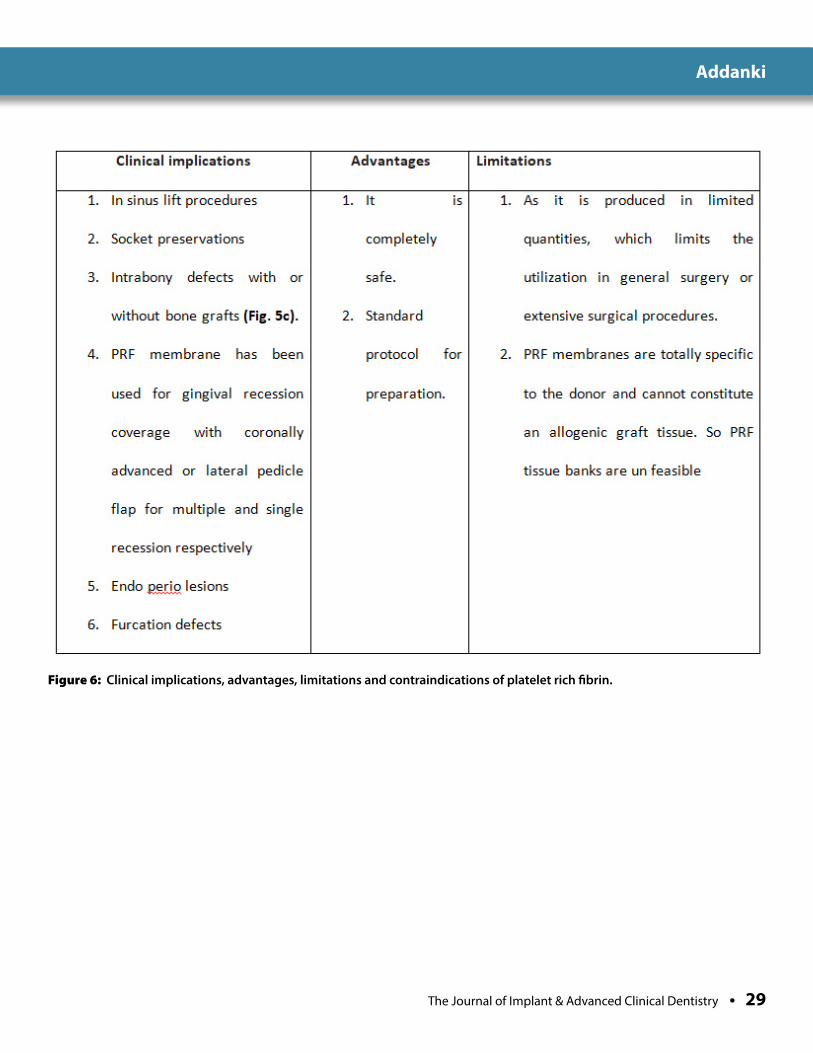
Figure 6: Clinical implications, advantages, limitations and contraindications of platelet rich fibrin.
30 • Vol. 10, No. 4 • May/June 2018
Addanki
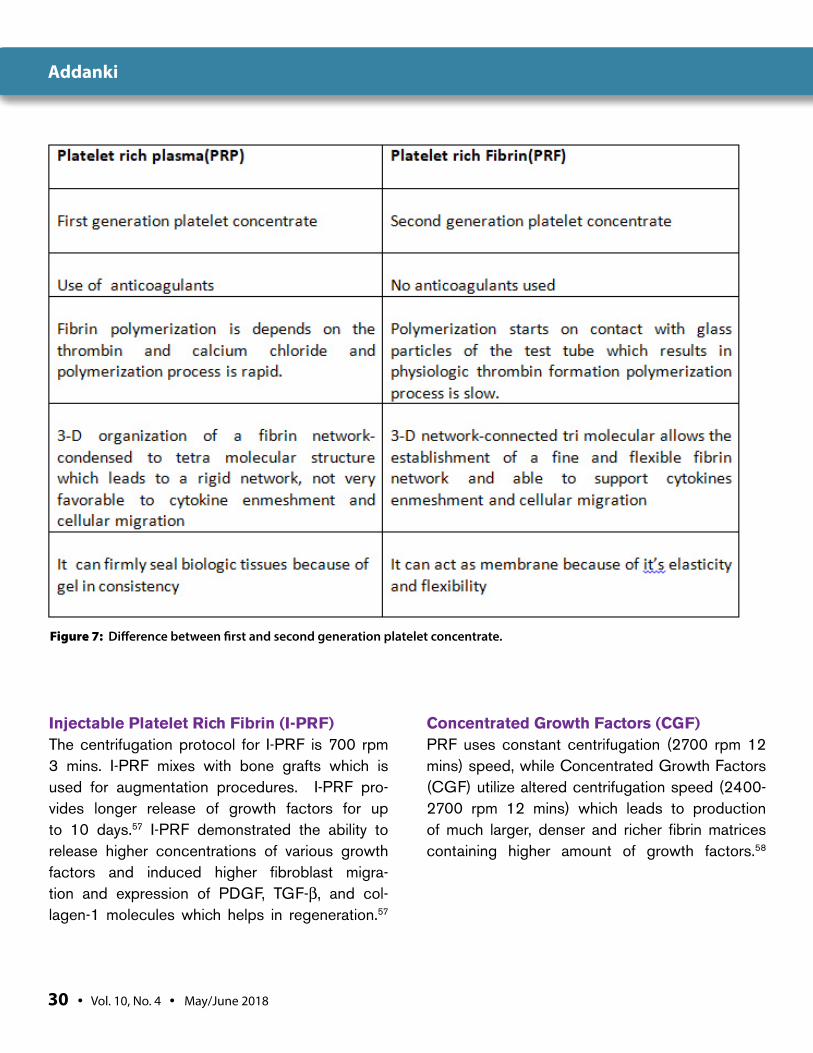
Figure 7: Difference between first and second generation platelet concentrate.
Injectable Platelet Rich Fibrin (I-PRF)The centrifugation protocol for I-PRF is 700 rpm 3 mins. I-PRF mixes with bone grafts which is used for augmentation procedures. I-PRF pro-vides longer release of growth factors for up to 10 days.57 I-PRF demonstrated the ability to release higher concentrations of various growth factors and induced higher fibroblast migra-tion and expression of PDGF, TGF-β, and col-lagen-1 molecules which helps in regeneration.57
Concentrated Growth Factors (CGF) PRF uses constant centrifugation (2700 rpm 12 mins) speed, while Concentrated Growth Factors (CGF) utilize altered centrifugation speed (2400-2700 rpm 12 mins) which leads to production of much larger, denser and richer fibrin matrices containing higher amount of growth factors.58
The Journal of Implant & Advanced Clinical Dentistry • 31
Addanki
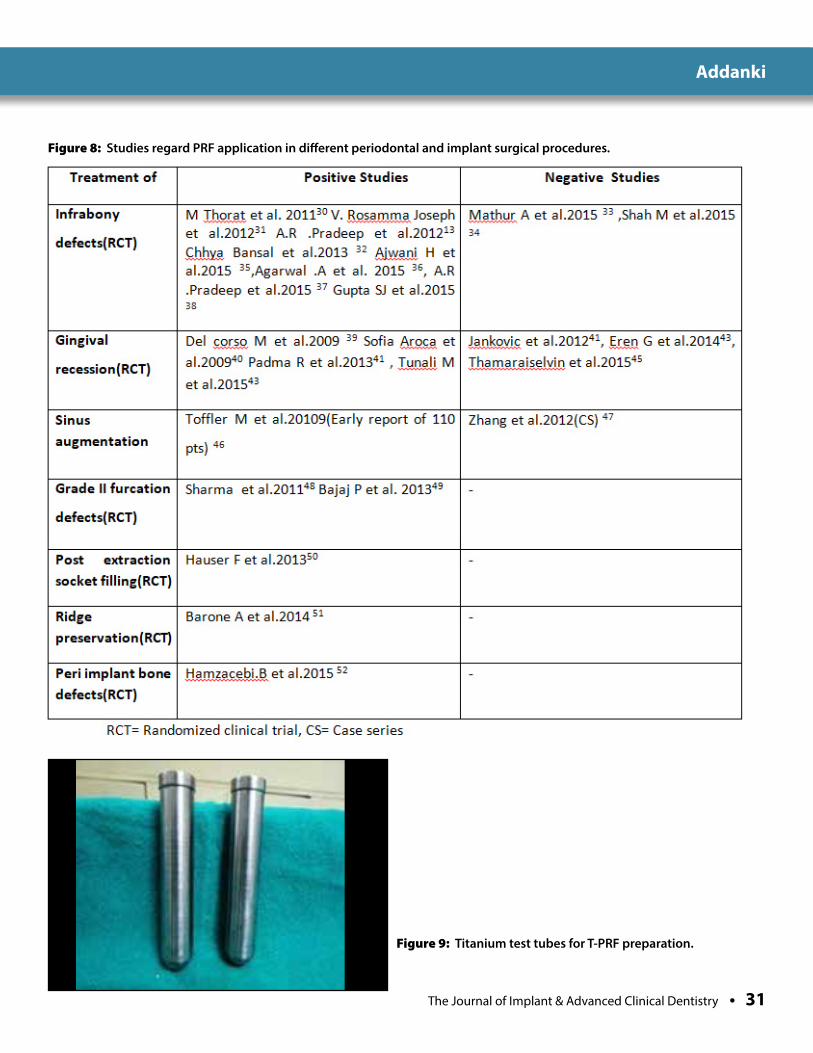
Figure 8: Studies regard PRF application in different periodontal and implant surgical procedures.
Figure 9: Titanium test tubes for T-PRF preparation.
32 • Vol. 10, No. 4 • May/June 2018
Addanki
Figure 10a: Histological photo of L-PRF. Figure 10b: Histological photo of T-PRF.
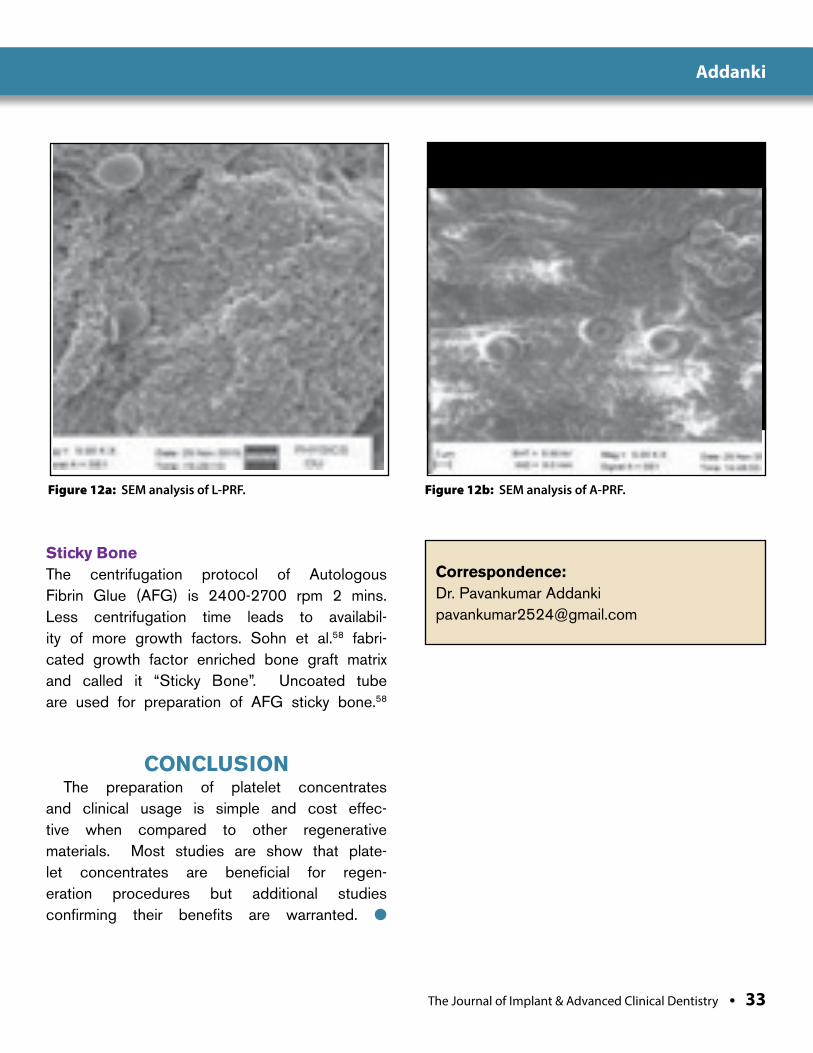
Figure 11a: SEM analysis of L-PRF. Figure 11b: SEM analysis of T-PRF.
The Journal of Implant & Advanced Clinical Dentistry • 33
Addanki
Figure 12a: SEM analysis of L-PRF. Figure 12b: SEM analysis of A-PRF.
Sticky BoneThe centrifugation protocol of Autologous Fibrin Glue (AFG) is 2400-2700 rpm 2 mins. Less centrifugation time leads to availabil-ity of more growth factors. Sohn et al.58 fabri-cated growth factor enriched bone graft matrix and called it “Sticky Bone”. Uncoated tube are used for preparation of AFG sticky bone.58
CONCLUSION The preparation of platelet concentrates and clinical usage is simple and cost effec-tive when compared to other regenerative materials. Most studies are show that plate-let concentrates are beneficial for regen-eration procedures but additional studies confirming their benefits are warranted. l
Correspondence:Dr. Pavankumar [email protected]
34 • Vol. 10, No. 4 • May/June 2018
Addanki
DisclosureThe authors report no conflicts of interest with anything in this article.
References1. Polimeni G, Xiropaidis AV, Wikesjo UM. Biology
and principles of periodontal wound healing/regeneration. Periodontol 2000 2006; 41:30-47.
2. Pradeep AR, Shetty SK, Garg G, Pai S. Clinical effectiveness of autologous platelet-rich plasma and peptide-enhanced bone graft in the treatment of intrabony defects. J Periodontol 2009; 80:62-71.
3. Marx RE, Carlson ER, Eichstaedt RM, Schimmele SR, and Strauss JE, Georgeff KR. Platelet-rich plasma: Growth factor enhancement for bone grafts. Oral Surg Oral Med Oral Pathol Oral Radiol Endod1998; 85:638-646.
4. Marx RE. Platelet-rich plasma: Evidence to support its use. J Oral Maxillofac Surg 2004; 62:489-496.
5. Okuda K, Kawase T, Momose M, Murata M, Saito Y, Suzuki H et al. Platelet-rich plasma contains high levels of platelet derived growth factor and transforming growth factor- and modulates the proliferation of periodontally related cells in vitro .J Periodontol 2003;74:849-857.
6. Arora NS, Ramanayke T, Ren YF, Romano GF. Platelet-rich plasma: a literature review. Implant Dent 2009; 18(4):303–308.
7. Dori F, Nikolidakis D, Huszar T, Arweller NB, Gera I, Sculean A. Effect of platelet-rich plasma on the healing of intrabony defects treated with natural bone mineral and a collagen membrane. J Clin Periodontol 2007; 34: 254-261.
8. Piemontese M, Aspriello SD and Rubini C, Ferrante L, Procaccini M.Treatment of periodontal intrabony defects with de mineralized freeze-dried bone allograft in combination with platelet-rich plasma: A comparative clinical trial. J Periodontol 2008; 79:802-810.
9. Camargo PM, Lekovic V, and Weinlaender, Divnic-Resnik T, Pavlovic M, Kenny EB. A surgical re entry study on the influence of platelet-rich plasma in enhancing the regenerative effects of bovine porous mineral and guided tissue regeneration in the treatment of intrabony defects in humans.J Periodontol 2009;80:915-923.
10. Haranack L, Boedeker RH, Kurtulus I, Boehm S, Gonzales J, Meyle J et al. Use of platelet-rich plasma in periodontal surgery –A prospective randomized double blind clinical trial. Clin Oral Investig 2009; 13:179-183.
11. Kaushick BT, Jayakumar ND ,Padmalatha O, Varghese S. Treatment of human periodontal infrabony defects with hydroxyapatite + β tricalcium phosphate bone graft alone and in combination with platelet rich plasma: a randomized clinical trial. Indian J Dent Res. 2011; 22(4):505-10.
12. Ozdemir B, Okte E. Treatment of intrabony defects with beta-tri calcium phosphate alone and in combination with platelet-rich plasma. J Biomed Mater Res B Appl Biomater. 2012; 100(4):976-83.
13. Pradeep A.R, Rao N S ,Agarwal E, Bajaj P,Kumari M, Naik SB .Comparative evaluation of autologous platelet-rich fibrin and platelet –rich plasma in the treatment of 3-wall intrabony defects in chronic periodontitis randomized controlled clinical trial.J Periodontol 2012;83:1449-1457.
14. Menzes LM, Rao J. Long term clinical evaluation of platelet-rich plasma in the treatment of human periodontal intraosseous defects: A comparative clinical trial. Quintessence Int 2012; 43:571-582.
15. HassanKS, Alagl AS , Abdel-Hady A. Torus mandibularis bone chips combined with platelet rich plasma gel for treatment of intrabony osseous defects: clinical and radiographic evaluation. Int J Oral Maxillofac Surg. 2012; 41(12):1519-26
16. Kukreja BJ, Dodwad V ,Kukreja P , Ahuja S, Mehra P. A comparative evaluation of platelet-rich plasma in combination with demineralized freeze-dried bone allograft and DFDBA alone in the treatment of periodontal intrabony defects: A clinic radiographic study.J Indian soc periodontal 2014; 18(5):618-623.
Figure 13: Summary of Centrifugation protocols for various PRF preparations.
The Journal of Implant & Advanced Clinical Dentistry • 35
Addanki
17. Agarwal A, Gupta ND. Platelet-rich plasma combined with decalcified freeze-dried bone allograft for the treatment of non contained human intrabony periodontal defects: a randomized controlled split-mouth study. Int J Periodontics Restorative Dent. 2014; 34(5):705-11.
18. Pinipe J, Mandalapu NB and Manchala SR, Mannem S, Gottumukkala S, Koneru S .Comparative evaluation of clinical efficacy of β-tri calcium phosphate (Septodont-RTR) alone and in combination with platelet rich plasma for treatment of intrabony defects in chronic periodontitis. J Indian Soc Periodontol. 2014; 18(3):346-51.
19. Keceli HG, Sengun D ,Berberoglu A ,Karabulut E. Use of platelet gel with connective tissue grafts for root coverage: A randomized-controlled trial. J Clin Periodontol 2008; 35:255-262.
20. Lafzi A, Chitsazi MT and Farahani RM ,Faramarzi M .Comparative clinical study of coronally advanced flap with and without use of plasma rich in growth factors in the treatment of gingival recession. Am J Dent. 2011; 24 (3):143-7.
21. Jovovic B, Lazic Z and Nedic M , Matijevic S, Gostovic-Spadijer A. Therapeutic efficacy of connective tissue auto transplants with periosteum and platelet rich plasma in the management of gingival recession. Vojnosanit Pregl. 2013; 70(7):664-9.
22. Aimetti M, Romano F, and Deliava C et al.Sinus grafting using autogenous bone and platelet-rich plasma: Histological outcomes in humans. Int J Periodontics Restorative Dent 2008; 28: 585-591.
23. Schaff H, Streckbien P, and Lendeckel S, Heidinger K S, Rehmann P, Bodeker RH et al.Sinus lift augmentation using autogenous bone grafts and platelet-rich plasma. Radiographic results. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008; 106:673-678.
24. Torres J, Tamimi F, Martinez PP, Alkhraisat MH, Linares R, Hernandez G et al. Effect of platelet-rich plasma on Sinus lifting: A randomized clinical trial. J Clin Periodontol 2009; 36: 677-687.
25. Khairy NM, Shendy EE, Askar NA , El-Rouby DH. Effect of platelet rich plasma on bone regeneration in maxillary sinus augmentation (randomized clinical trial). Int J Oral Maxillofac Surg. 2013; 42(2):249-55.
26. Sunitha Raja V, Munirathnam Naidu E. Platelet rich fibrin: evolution of a second generation platelet concentrate. Indian J Dent Res 2008; 19:42–46.
27. Dohan DM, Choukroun J, Diss A, Dohan SL, Dohan AJ, Mouhyi J et al .Platelet-rich fibrin (PRF): a second-generation platelet concentrate. Part I: technological concepts and evolution. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006; 101: e37–e44.
28. Dohan DM, Choukroun J, Diss A, Dohan SL, Dohan AJ, Mouhyi J et al. Platelet-rich fibrin (PRF): a second-generation platelet concentrate. Part III: leucocyte activation: a new feature for platelet concentrates? Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006; 101:e51–e55.
29. Choukroun J, Diss A, Simonpieri A, Girard MO, Schoeffler C, Dohan SL et al. Platelet-rich fibrin (PRF): a second-generation platelet concentrate. Part IV: clinical effects on tissue healing. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006; 101:e56–e60.
30. Thorat M, Pradeep AR, Pallavi B. Clinical effect of autologous platelet-rich fibrin in the treatment of intra-bony defects: a controlled clinical trial. J Clin Periodontol 2011; 38 (10):925-32.
31. Rosamma Joseph V, Raghunath A ,Sharma N. Clinical effectiveness of autologous platelet rich fibrin in the management of infrabony periodontal defects. Singapore Dent J 2012; 33(1):5-12.
32. Bansal C, Bharti V. Evaluation of efficacy of autologous platelet-rich fibrin with demineralized-freeze dried bone allograft in the treatment of periodontal intrabony defects. J Indian Soc Periodontol. 2013; 17(3):361-6.
33. Mathur A, Bains VK, and Gupta V ,Jhingran R, Singh G.P. Evaluation of intrabony defects treated with platelet-rich fibrin or autogenous bone graft: A comparative analysis. Eur J Dent. 2015; 9(1):100-8.
34. Shah M, Patel J, and Dave D , Shah S. Comparative evaluation of platelet-rich fibrin with demineralized freeze-dried bone allograft in periodontal infrabony defects: A randomized controlled clinical study. J Indian Soc Periodontol. 2015; 19(1):56-60.
35. Ajwani H, Shetty S, Gopalakrishnan D. Comparative evaluation of platelet-rich fibrin biomaterial and open flap debridement in the treatment of two and three wall intrabony defects. Int Oral Health. 2015; 7(4):32-7.
36. Agarwal A, Gupta ND, Jain A. Platelet rich fibrin combined with decalcified freeze-dried bone allograft for the treatment of human intrabony periodontal defects: a randomized split mouth clinical trial. Acta Odontol Scand. 2015; 14:1-8.
37. Pradeep A.R. , Nagpal K, Karvekar S , Patanaik K, Naik SB, Guru Prasad CN. Platelet rich fibrin with 1%Metformin for the treatment of intrabony defects in chronic periodontitis: A randomized clinical trial. J Periodontol 2015; 86(6):729-737.
38. Gupta SJ, Jhingran R, Gupta V , Bains VK, Madan R, Rizvi I. Efficacy of platelet-rich fibrin vs. enamel matrix derivative in the treatment of periodontal intrabony defects: a clinical and cone beam computed tomography study. J Int Acad Periodontol. 2014; 16(3):86-96.
39. Del Corso M, Sammartino G, Dohan Ehrenfest DM. Clinical evaluation of a modified coronally advanced flap alone or in combination with a platelet-rich fibrin membrane for the treatment of adjacent multiple gingival recessions: a 6-month study”. J Periodontol. 2009; 80(11):1694-7
40. Sofia Aroca, Tibor Keglevich , Bruno Barbieri et al. Clinical evaluation of modified coronally advanced flap alone or in combination with a platelet-rich fibrin membrane for the treatment of adjacent multiple gingival recessions: A 6-month study. J Periodontol 2009;80(2):244-252.
41. Jankovic S, Aleksic Z, Klokkvold P ,Lekovic V, Dimitrijevic B, Kenny EB, Camargo P.Use of platelet-rich fibrin membrane following treatment of gingival recession: A randomized clinical trial. Int J Periodontics Restorative Dent 2012; 32:e41-e50.
42. Padma R, Shilpa A , Kumar PA ,Naga sri M, Kumar C, Sreedhar A. A split mouth randomized controlled study to evaluate the adjunctive effect of platelet-rich fibrin to coronally advanced flap in Miller’s class-I and II recession defects. J Indian Soc Periodontol. 2013; 17(5):631-637
43. Eren G, Atilla G. Platelet-rich fibrin in the treatment of localized gingival recessions: a split-mouth randomized clinical trial. Clin Oral Investig. 2014; 18(8):1941-8.
44. Tunali M, Ozdemir H , Arabaci T , Gurbuzer B, Pikdoken L, Firatli E. Clinical evaluation of autologous platelet-rich fibrin in the treatment of multiple adjacent gingival recession defects: a 12-month study. Int J Periodontics Restorative Dent. 2015; 35(1):105-14
45. Thamaraiselvin, Elavarasu S , Thangakumaran S ,Gadgi JS, Arthie T. Comparative clinical evaluation of coronally advanced flap with or without platelet rich fibrin membrane in the treatment of isolated gingival recession. J Indian Soc Periodontol. 2015; 19(1):66-71.
46. Toffler M, Toscano N , Holtzclaw D .Osteotome-mediated sinus floor elevation using only platelet-rich fibrin: an early report on 110 patients. Implant Dent. 2010; 19(5):447-56.
47. Zhang Y, Tangl S , Huber CD ,Lin Y, Qiu L, Rausch-Fan X. Effect of Choukroun’s platelet rich fibrin on bone regeneration in combination with deprotienzed bovine bone material in maxillary sinus augmentation: A histological and histomorphometric study. J Crainomaxillofac Surg 2012; 40(4):321-8.
48. Sharma A, Pradeep A.R.. Autologous Platelet-rich fibrin in the treatment of mandibular degree II furcation defects: A randomized clinical trial. J Periodontol 2011; 82:1396-1403.
49. Bajaj P, Pradeep AR and Agarwal E , Rao NS, Naik SB , Priyanka N et al. Comparative evaluation of autologous platelet-rich fibrin and platelet-rich plasma in the treatment of mandibular degree II furcation defects: a randomized controlled clinical trial. J Periodontal Res. 2013; 48(5):573-81.
50. Hauser F, Gaydarov Nand Badoud I et al. Clinical and histological evaluation of post extraction platelet-rich fibrin socket filling: a prospective randomized controlled study. Implant Dent. 2013; 22(3):295-303.
51. Barone A, Ricci M and Romanos GE et al. Buccal bone deficiency in fresh extraction sockets: a prospective single cohort study. Clin Oral Implants Res. 2014; 31:45-49
52. Hamzacebi.B, Oduncuoglu B , Alaaddinoglu EE. Treatment of Peri-implant Bone Defects with Platelet-Rich Fibrin. Int J Periodontics Restorative Dent. 2015; 35(3):415-22.
53. M. Tunali, H. Ozdemir, Z. Kuçukodaci, S. Akman, E. Yaprak, E. Firatli et al. “In vivo evaluation of titanium-prepared platelet-rich fibrin (T-PRF): a new platelet concentrate” .Br J Oral Maxillofac Surg 2012; 51(5): 438–443.
54. S. Takemoto, T. Yamamoto, K. Tsuru, S. Hayakawa, A. Osaka, S. Takashima et al. “Platelet adhesion on titanium oxide gels: effect of surface oxidation”. Biomaterials 2004; 25(17); 3485–3492.
55. M. Tunali, H. Ozdemir, Z. Kuçukodaci, S. Akman, E. Yaprak, E. Firatli et al. A Novel Platelet Concentrate: Titanium-Prepared Platelet-Rich Fibrin. Biomed research international 2014; 1; 1-7.
56. Ghanaati S, Booms P, Orlowska A, Kubesch A, Lorenz J, Rutkowski J et al. Advanced Platelet-rich fibrin: A new concept for cell based tissue engineering by means of inflammatory cells. J Oral Implant 2014; 40; 680-689
57. Reduction of relative centrifugation force within injectable platelet-rich-fibrin (PRF) concentrates advances patients’ own inflammatory cells, platelets and growth factors: the first introduction to the low speed centrifugation concept. Eur J Trauma Emerg Surg. 2018 Feb; 44(1):87-95.
58. Sohn DK, Huang B, Kim J, Park W.E, Park CC. Utilization of Autologous concentrated growth factors (GGF) enriched bone graft matrix (Sticky bone) and CGF-Enriched membrane in implant dentistry. The J Implant Adv Clin Dent 2015; 7:11-27.
The Best Things in Life Are FREE!
Subscribe now to enjoy articles free of charge that will benefit you, the actively practicing dental provider. With each JIACD issue, readers are afforded the opportunity to
assess clinical techniques, cases, literature reviews, and expert commentary that can immediately impact their daily dental practice.
Email notification when new issues are available online.
Start your FREE subscription today at www.jiacd.com
The Journal of Implant & Advanced Clinical Dentistry
Volume 9, No. 4 may/JuNe 2017
Xenograft Socket Preservation
The MIMS Technique for Gingival Grafting
The Journal of Implant & Advanced Clinical Dentistry
Volume 9, No. 2 February 2017
Updated Primer on Amnion-Chorion Allografts
Computer Guided Full Arch Immediately Loaded
Dental Implants
The Journal of Implant & Advanced Clinical Dentistry
Volume 9, No. 6 August 2017
Impacted Canine Replacement
6 Year Multi-Center Study onOsseofuse Dental Implants
The Journal of Implant & Advanced Clinical Dentistry
Volume 9, No. 7 September 2017
Biotype Tissue Change at Second Stage Implant Surgery
Immediate vs. Early Loading of Short Implants