oite trauma review h. pakzad wed sept 12, 2007. which of the following arteries provides the single...
TRANSCRIPT

OITE Trauma OITE Trauma ReviewReview
H. PakzadH. Pakzad
Wed Sept 12, 2007Wed Sept 12, 2007

Which of the following arteries provides Which of the following arteries provides the single dominant proximal blood the single dominant proximal blood supply to the medial head of the supply to the medial head of the gastrocnemius muscle? gastrocnemius muscle?
1- Anterior tibial 1- Anterior tibial
2- Posterior tibial2- Posterior tibial
3- Peroneal3- Peroneal
4- Genicular4- Genicular
5- Sural5- Sural
2006 – Question 12006 – Question 1

Each muscle has one dominant pedicle consisting of the sural artery and vein given off by the popliteal artery at the level of the knee joint. The sural arteries run distally with the tibial nerve branches for several centimeters before entering the muscle bellies on their anterior surfaces.
2006 – Question 82006 – Question 8
Two years following open reduction and Two years following open reduction and internal fixation of a pilon fracture, which internal fixation of a pilon fracture, which of the following parameters correlates most of the following parameters correlates most closely with a poor clinical outcome and closely with a poor clinical outcome and inability to return to work? inability to return to work?
1 - Metaphyseal comminution 1 - Metaphyseal comminution
2- Quality of reduction 2- Quality of reduction
3- Time to surgery 3- Time to surgery
4- Lower level of education 4- Lower level of education
5- Open fracture5- Open fracture

2006 – Question 132006 – Question 13
During placement of an iliosacral screw During placement of an iliosacral screw into the body of S1, what pelvic into the body of S1, what pelvic radiographic view should be obtained radiographic view should be obtained to help avoid entering the S1 to help avoid entering the S1 neuroforamen?neuroforamen?
1- AP1- AP2- Lateral 2- Lateral 3- Inlet 3- Inlet 4- Outlet4- Outlet5- Obturator oblique5- Obturator oblique
2006 – Question 162006 – Question 16
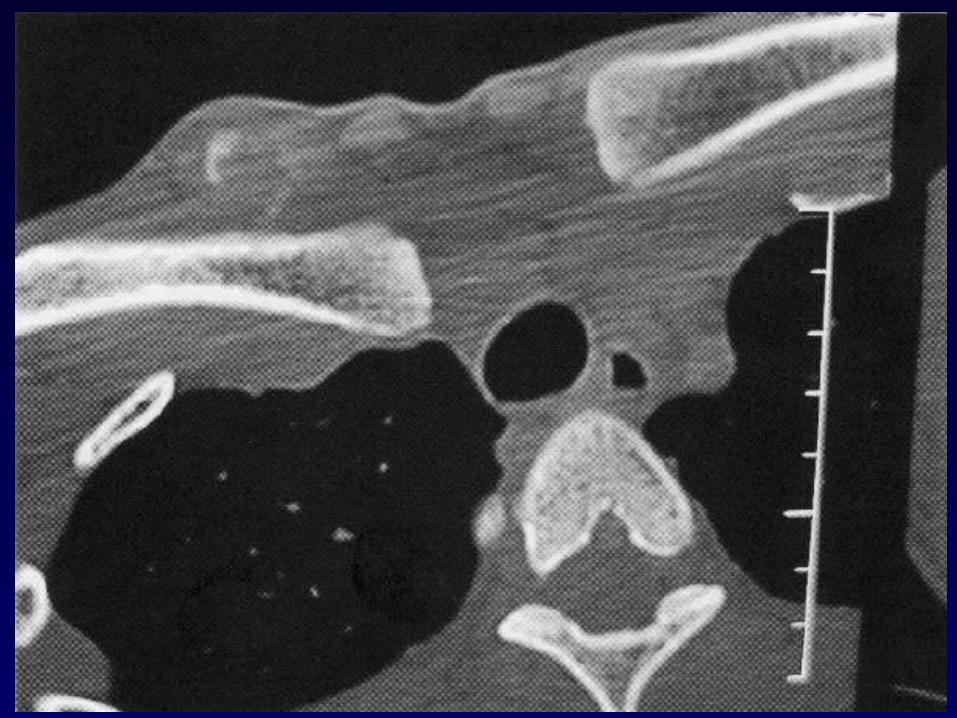
A 22-year-old woman has wrist pain after falling on A 22-year-old woman has wrist pain after falling on her outstretched hand 2 weeks ago. Examination her outstretched hand 2 weeks ago. Examination reveals tenderness in the anatomic snuffbox. A reveals tenderness in the anatomic snuffbox. A radiograph is shown. Treatment should consist of radiograph is shown. Treatment should consist of
1- open reduction and internal fixation using the 1- open reduction and internal fixation using the Russe bone graft technique via a volar approach.Russe bone graft technique via a volar approach.
2- open reduction and internal fixation with a 2- open reduction and internal fixation with a compression screw via a volar approach.compression screw via a volar approach.
3- open reduction and internal fixation with 3- open reduction and internal fixation with vascularized bone graft via a volar approach.vascularized bone graft via a volar approach.
4- open reduction and internal fixation with 4- open reduction and internal fixation with vascularized bone graft via a dorsal approach.vascularized bone graft via a dorsal approach.
5- a cast brace for 6 weeks 5- a cast brace for 6 weeks

2006 – Question 162006 – Question 16
A 22-year-old woman has wrist pain after falling on A 22-year-old woman has wrist pain after falling on her outstretched hand 2 weeks ago. Examination her outstretched hand 2 weeks ago. Examination reveals tenderness in the anatomic snuffbox. A reveals tenderness in the anatomic snuffbox. A radiograph is shown. Treatment should consist of radiograph is shown. Treatment should consist of
1- open reduction and internal fixation using the 1- open reduction and internal fixation using the Russe bone graft technique via a volar approach.Russe bone graft technique via a volar approach.
2- open reduction and internal fixation with a 2- open reduction and internal fixation with a compression screw via a volar approach.compression screw via a volar approach.
3- open reduction and internal fixation with 3- open reduction and internal fixation with vascularized bone graft via a volar approach.vascularized bone graft via a volar approach.
4- open reduction and internal fixation with 4- open reduction and internal fixation with vascularized bone graft via a dorsal approach.vascularized bone graft via a dorsal approach.
5- a cast brace for 6 weeks 5- a cast brace for 6 weeks

2006 – Question 222006 – Question 22
Following imaging show the injury a 17-year-old boy Following imaging show the injury a 17-year-old boy sustained in a recreational vehicle accident 3 weeks sustained in a recreational vehicle accident 3 weeks ago. Examination reveals mild asymmetry and ago. Examination reveals mild asymmetry and regional discomfort referable to the right regional discomfort referable to the right sternoclavicular joint. The remainder of the physical sternoclavicular joint. The remainder of the physical examination findings are unremarkable. Management examination findings are unremarkable. Management should consist ofshould consist of
1 - closed reduction.1 - closed reduction.2- open reduction and pin fixation.2- open reduction and pin fixation.3- sternoclavicular ligamentous reconstruction.3- sternoclavicular ligamentous reconstruction.4- nonsurgical treatment with resumption of 4- nonsurgical treatment with resumption of
unrestricted activity in 3 months. unrestricted activity in 3 months. 5- nonsurgical treatment with cessation of contact 5- nonsurgical treatment with cessation of contact
sports indefinitely.sports indefinitely.


2006 – Question 222006 – Question 22
Following imaging show the injury a 17-year-old boy Following imaging show the injury a 17-year-old boy sustained in a recreational vehicle accident 3 weeks sustained in a recreational vehicle accident 3 weeks ago. Examination reveals mild asymmetry and ago. Examination reveals mild asymmetry and regional discomfort referable to the right regional discomfort referable to the right sternoclavicular joint. The remainder of the physical sternoclavicular joint. The remainder of the physical examination findings are unremarkable. Management examination findings are unremarkable. Management should consist ofshould consist of
1 - closed reduction.1 - closed reduction.2- open reduction and pin fixation.2- open reduction and pin fixation.3- sternoclavicular ligamentous reconstruction.3- sternoclavicular ligamentous reconstruction.4- nonsurgical treatment with resumption of 4- nonsurgical treatment with resumption of
unrestricted activity in 3 months. unrestricted activity in 3 months. 5- nonsurgical treatment with cessation of contact 5- nonsurgical treatment with cessation of contact
sports indefinitely.sports indefinitely.

2006 – Question 272006 – Question 27
What type of nonunion is most likely What type of nonunion is most likely to unite by increasing biomechanical to unite by increasing biomechanical stability?stability?
1- Atrophic1- Atrophic
2- Oligotrophic 2- Oligotrophic
3- Hypertrophic 3- Hypertrophic
4- Infected4- Infected
5- Synovial pseudarthrosis5- Synovial pseudarthrosis

2006 – Question 282006 – Question 28
On an AP ankle radiograph, the measurement of the On an AP ankle radiograph, the measurement of the tibial clear space (the syndesmotic space) should be tibial clear space (the syndesmotic space) should be less than 5 mm if there is no syndesmotic widening. less than 5 mm if there is no syndesmotic widening. The tibial clear space is defined as theThe tibial clear space is defined as the
1- distance between the medial border of the fibula and 1- distance between the medial border of the fibula and the incisura fiibularis. the incisura fiibularis.
2- distance from the incisura fibularis to the lateral tibial 2- distance from the incisura fibularis to the lateral tibial border. border.
3- distance from the medial malleolus to the talus. 3- distance from the medial malleolus to the talus. 4- overlap of the anterior portion of the lateral tibia on 4- overlap of the anterior portion of the lateral tibia on
the fibula. the fibula. 5- overlap of the posterior portion of the lateral tibia on 5- overlap of the posterior portion of the lateral tibia on
the fibula.the fibula.

2006 – Question 332006 – Question 33
A greater trochanteric entry site for femoral A greater trochanteric entry site for femoral intramedullary nailing, compared to a piriformis intramedullary nailing, compared to a piriformis fossa starting point, is associated with:fossa starting point, is associated with:
1- more disruption of the gluteus medius tendon.1- more disruption of the gluteus medius tendon.2- more disruption of the short external rotator 2- more disruption of the short external rotator
tendons.tendons.3- more disruption of the medial femoral circumflex 3- more disruption of the medial femoral circumflex
artery. artery. 4- greater hoop stresses with an anterior starting 4- greater hoop stresses with an anterior starting
point. point. 5- greater colinearity with a long axis of the femoral 5- greater colinearity with a long axis of the femoral
shaft.shaft.

2006 – Question 392006 – Question 39
In patients with ipsilateral femoral neck In patients with ipsilateral femoral neck and shaft fractures, what percent of and shaft fractures, what percent of femoral neck fractures are significantly femoral neck fractures are significantly displaced?displaced?
1 - 5%1 - 5%
2- 20%2- 20%
3- 40% 3- 40%
4- 70%4- 70%
5- 90%5- 90%

2006 – Question 412006 – Question 41
When comparing antegrade nailing of When comparing antegrade nailing of femoral shaft fractures treated with a femoral shaft fractures treated with a fracture table versus manual traction, fracture table versus manual traction, the manual traction group had the manual traction group had significantly lesssignificantly less
1- fluoroscopy time.1- fluoroscopy time.2- shortening of the femur. 2- shortening of the femur. 3- assistants per case. 3- assistants per case. 4- exchange nailings.4- exchange nailings.5- internal rotational deformities.5- internal rotational deformities.

2006 – Question 512006 – Question 51
To minimize the risk of iatrogenic traction injury To minimize the risk of iatrogenic traction injury to the sciatic nerve during open reduction and to the sciatic nerve during open reduction and internal fixation of the acetabulum through the internal fixation of the acetabulum through the Kocher-Langenbeck exposure, the leg should Kocher-Langenbeck exposure, the leg should be in what position?be in what position?
1- Extended at the hip and extended at the knee 1- Extended at the hip and extended at the knee 2- Extended at the hip and flexed at the knee 2- Extended at the hip and flexed at the knee 3- Flexed at the hip and extended at the knee 3- Flexed at the hip and extended at the knee 4- Flexed at the hip and flexed at the knee4- Flexed at the hip and flexed at the knee5- Abducted at the hip and extended at the knee5- Abducted at the hip and extended at the knee

2006 – Question 572006 – Question 57
A lower discharge Glasgow Coma Scale A lower discharge Glasgow Coma Scale score in a patient with a femoral fracture score in a patient with a femoral fracture and a head injury has been associated and a head injury has been associated with with
1- surgery within 24 hours after injury. 1- surgery within 24 hours after injury.
2- hypotension and hypoxia. 2- hypotension and hypoxia.
3- prolonged length of stay in the ICU. 3- prolonged length of stay in the ICU.
4- major non-orthopaedic surgeries. 4- major non-orthopaedic surgeries.
5- the presence of pneumonia.5- the presence of pneumonia.
2006 – Question 642006 – Question 64
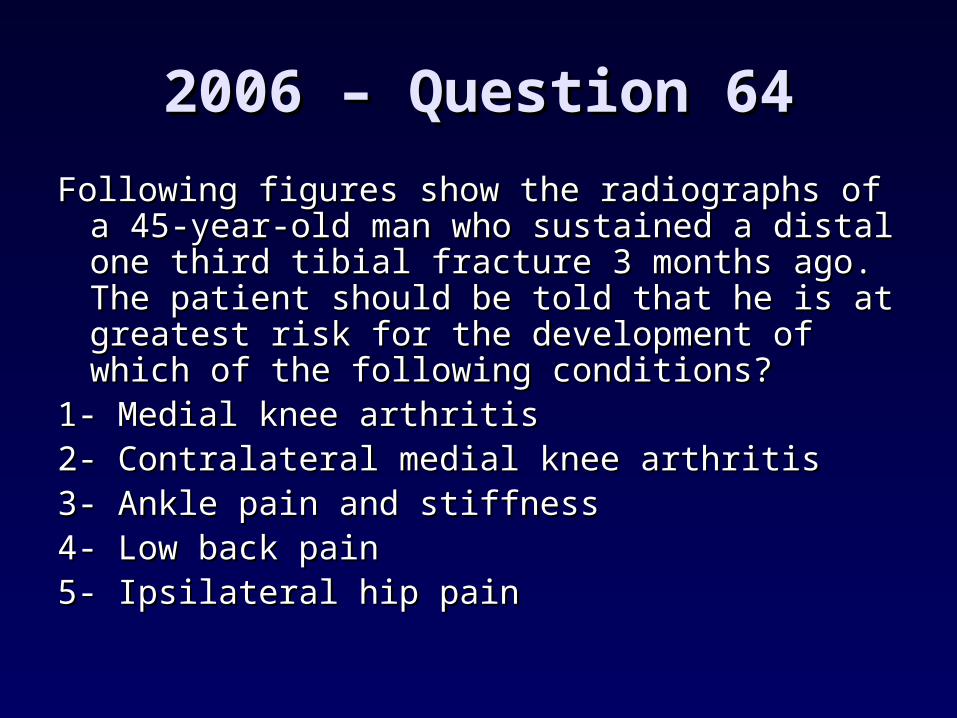
Following figures show the radiographs of a Following figures show the radiographs of a 45-year-old man who sustained a distal one 45-year-old man who sustained a distal one third tibial fracture 3 months ago. The third tibial fracture 3 months ago. The patient should be told that he is at greatest patient should be told that he is at greatest risk for the development of which of the risk for the development of which of the following conditions? following conditions?
1- Medial knee arthritis1- Medial knee arthritis2- Contralateral medial knee arthritis 2- Contralateral medial knee arthritis 3- Ankle pain and stiffness 3- Ankle pain and stiffness 4- Low back pain4- Low back pain5- Ipsilateral hip pain5- Ipsilateral hip pain


2006 – Question 642006 – Question 64
Following figures show the radiographs of a Following figures show the radiographs of a 45-year-old man who sustained a distal one 45-year-old man who sustained a distal one third tibial fracture 3 months ago. The third tibial fracture 3 months ago. The patient should be told that he is at greatest patient should be told that he is at greatest risk for the development of which of the risk for the development of which of the following conditions? following conditions?
1- Medial knee arthritis1- Medial knee arthritis2- Contralateral medial knee arthritis 2- Contralateral medial knee arthritis 3- Ankle pain and stiffness 3- Ankle pain and stiffness 4- Low back pain4- Low back pain5- Ipsilateral hip pain5- Ipsilateral hip pain

Long-term effects of tibial angular malunion on the knee and ankle Long-term effects of tibial angular malunion on the knee and ankle joints.joints.
PunoPuno RM RM, , Vaughan JJVaughan JJ, , StettenStetten ML ML, , Johnson JRJohnson JR.. Department of Orthopaedic Surgery, University of Louisville, Kentucky Department of Orthopaedic Surgery, University of Louisville, Kentucky
40292.40292.
Twenty-seven patients with 28 tibial fractures were evaluated for an Twenty-seven patients with 28 tibial fractures were evaluated for an average of 8.2 years (range 6.0-12.3 years) following their injuries. average of 8.2 years (range 6.0-12.3 years) following their injuries. There were 16 closed and 12 open fractures, all of which healed There were 16 closed and 12 open fractures, all of which healed uneventfully. Overall, 50% of the ankles and 75% of the knees were uneventfully. Overall, 50% of the ankles and 75% of the knees were rated good to excellent. The patients' knee and ankle joint rated good to excellent. The patients' knee and ankle joint malalignments were extrapolated using a method previously malalignments were extrapolated using a method previously published. This was made possible by knowing both the degree and published. This was made possible by knowing both the degree and site of angular deformity. Correlation between joint malalignments site of angular deformity. Correlation between joint malalignments and clinical outcome were performed. and clinical outcome were performed. Analysis showed that greater Analysis showed that greater degrees of ankle malalignment produce poorer clinical results (p = degrees of ankle malalignment produce poorer clinical results (p = 0.001).0.001). Conversely, the patients with lesser degrees of ankle joint Conversely, the patients with lesser degrees of ankle joint malalignment had a higher percentage of good to excellent results (p malalignment had a higher percentage of good to excellent results (p = 0.006, p = 0.003, p = 0.03). The knee results did not correlate with = 0.006, p = 0.003, p = 0.03). The knee results did not correlate with the degree of joint malalignment (p = 0.82).the degree of joint malalignment (p = 0.82). The findings in this The findings in this study show that there is merit in reducing tibial fractures as close to study show that there is merit in reducing tibial fractures as close to anatomical configuration as possible to lessen the chance of early anatomical configuration as possible to lessen the chance of early degenerative arthritis.degenerative arthritis.
PMID: 1941305 [PubMed - indexed for MEDLINE]PMID: 1941305 [PubMed - indexed for MEDLINE]

2006 – Question 702006 – Question 70
A 25-year-old man has right knee pain after being A 25-year-old man has right knee pain after being involved in a motor vehicle accident. Radiographs involved in a motor vehicle accident. Radiographs reveal a distal femoral fracture with metaphyseal reveal a distal femoral fracture with metaphyseal comminution. What is the most common missed comminution. What is the most common missed injury diagnosed by CT? injury diagnosed by CT?
1- Coronal fracture of the medial femoral condyle 1- Coronal fracture of the medial femoral condyle 2- Coronal fracture of the lateral femoral condyle 2- Coronal fracture of the lateral femoral condyle 3- Sagittal fracture of the medial femoral condyle 3- Sagittal fracture of the medial femoral condyle 4- Sagittal fracture of the lateral femoral condyle 4- Sagittal fracture of the lateral femoral condyle 5- Anterior cruciate ligament tear5- Anterior cruciate ligament tear

2006 – Question 772006 – Question 77
Femoral nailing through the piriformis Femoral nailing through the piriformis fossa is contraindicated in adolescents fossa is contraindicated in adolescents with open physes because of the risk with open physes because of the risk of? of?
1- osteonecrosis1- osteonecrosis
2- rotational malalignment2- rotational malalignment
3- shortening 3- shortening
4- coxa vara4- coxa vara
5- increased intramedullary pressure5- increased intramedullary pressure

2006 – Question 812006 – Question 81
A terrible triad elbow injury that includes a comminuted A terrible triad elbow injury that includes a comminuted non-reconstructable radial head fracture and a type non-reconstructable radial head fracture and a type III coronoid fracture associated with an elbow III coronoid fracture associated with an elbow dislocation is best treated with acute radial head dislocation is best treated with acute radial head
1- resection and lateral collateral ligament repair1- resection and lateral collateral ligament repair2- resection, coronoid open reduction and internal 2- resection, coronoid open reduction and internal
fixation, and medial collateral ligament repairfixation, and medial collateral ligament repair3- arthroplasty alone3- arthroplasty alone4- arthroplasty and coronoid open reduction and 4- arthroplasty and coronoid open reduction and
internal fixationinternal fixation5- arthroplasty, coronoid open reduction and internal 5- arthroplasty, coronoid open reduction and internal
fixation, and lateral collateral ligament repairfixation, and lateral collateral ligament repair
2006 – Question 852006 – Question 85
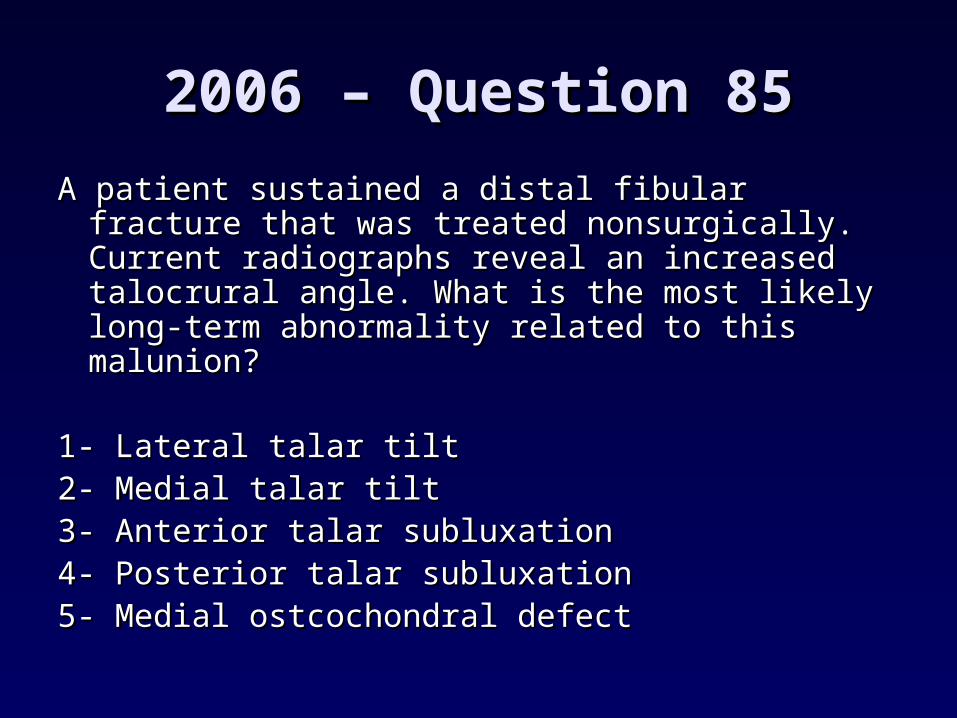
A patient sustained a distal fibular fracture that A patient sustained a distal fibular fracture that was treated nonsurgically. Current was treated nonsurgically. Current radiographs reveal an increased talocrural radiographs reveal an increased talocrural angle. What is the most likely long-term angle. What is the most likely long-term abnormality related to this malunion?abnormality related to this malunion?
1- Lateral talar tilt1- Lateral talar tilt2- Medial talar tilt2- Medial talar tilt3- Anterior talar subluxation 3- Anterior talar subluxation 4- Posterior talar subluxation 4- Posterior talar subluxation 5- Medial ostcochondral defect5- Medial ostcochondral defect

The talocrural angle is the superior and medial angle formed by the intersection of a line joining the tips of both malleoli and of a line perpendicular to the distal tibial articular surface.
The difference in the talocrural angle between the injured and normal sides was the only statistically significant radiographic indicator of a good prognosis.
A prospective, randomized study of the management of severe ankle fractures
J Bone Joint Surg Am. 1985;67:67-78.WA Phillips, HS Schwartz, CS Keller, HR Woodward, WS Rudd
78.4 degrees (range 74 to 83)

2006 – Question 872006 – Question 87
The inhibitory effect of quinolone-class The inhibitory effect of quinolone-class antimicrobials on early fracture healing antimicrobials on early fracture healing is most directly linked to toxic effects is most directly linked to toxic effects on which of the following structures?on which of the following structures?
1- Vascular endothelial cells 1- Vascular endothelial cells 2- Osteoblasts 2- Osteoblasts 3- Ostcoclasts 3- Ostcoclasts 4- Chondrocytes 4- Chondrocytes 5- Macrophages5- Macrophages

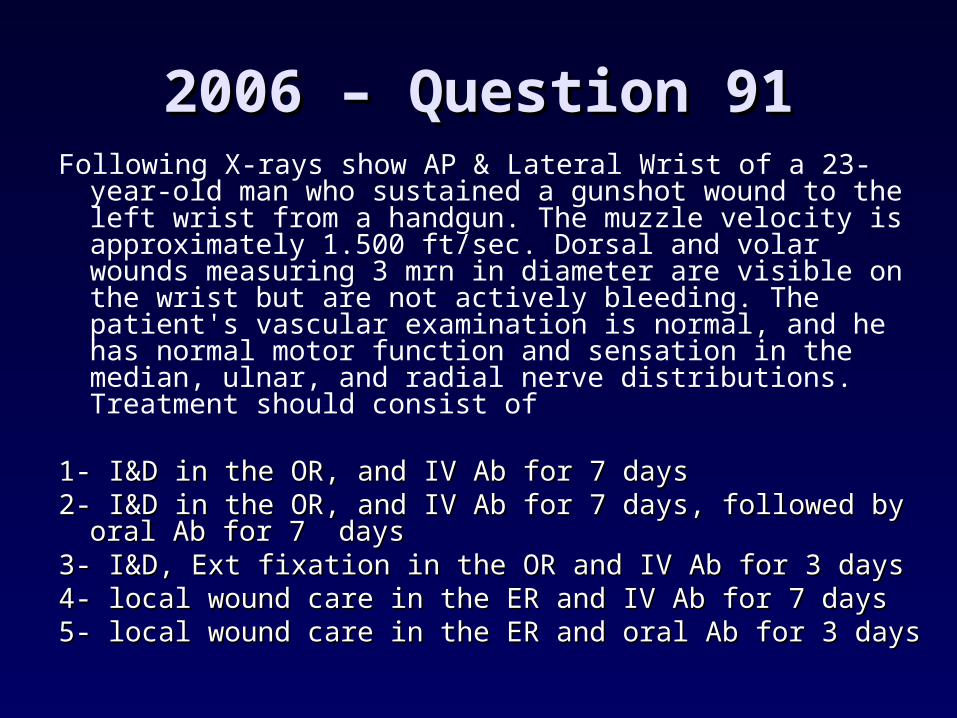
2006 – Question 912006 – Question 91Following X-rays show AP & Lateral Wrist of a 23-year-
old man who sustained a gunshot wound to the left wrist from a handgun. The muzzle velocity is approximately 1.500 ft/sec. Dorsal and volar wounds measuring 3 mrn in diameter are visible on the wrist but are not actively bleeding. The patient's vascular examination is normal, and he has normal motor function and sensation in the median, ulnar, and radial nerve distributions. Treatment should consist of
1- I&D in the OR, and IV Ab for 7 days1- I&D in the OR, and IV Ab for 7 days2- I&D in the OR, and IV Ab for 7 days, followed by oral 2- I&D in the OR, and IV Ab for 7 days, followed by oral
Ab for 7 daysAb for 7 days3- I&D, Ext fixation in the OR and IV Ab for 3 days3- I&D, Ext fixation in the OR and IV Ab for 3 days4- local wound care in the ER and IV Ab for 7 days 4- local wound care in the ER and IV Ab for 7 days 5- local wound care in the ER and oral Ab for 3 days5- local wound care in the ER and oral Ab for 3 days

2006 – Question 912006 – Question 91Following X-rays show AP & Lateral Wrist of a 23-year-
old man who sustained a gunshot wound to the left wrist from a handgun. The muzzle velocity is approximately 1.500 ft/sec. Dorsal and volar wounds measuring 3 mrn in diameter are visible on the wrist but are not actively bleeding. The patient's vascular examination is normal, and he has normal motor function and sensation in the median, ulnar, and radial nerve distributions. Treatment should consist of
1- I&D in the OR, and IV Ab for 7 days1- I&D in the OR, and IV Ab for 7 days2- I&D in the OR, and IV Ab for 7 days, followed by oral 2- I&D in the OR, and IV Ab for 7 days, followed by oral
Ab for 7 daysAb for 7 days3- I&D, Ext fixation in the OR and IV Ab for 3 days3- I&D, Ext fixation in the OR and IV Ab for 3 days4- local wound care in the ER and IV Ab for 7 days 4- local wound care in the ER and IV Ab for 7 days 5- local wound care in the ER and oral Ab for 3 days5- local wound care in the ER and oral Ab for 3 days

2006 – Question 1002006 – Question 100
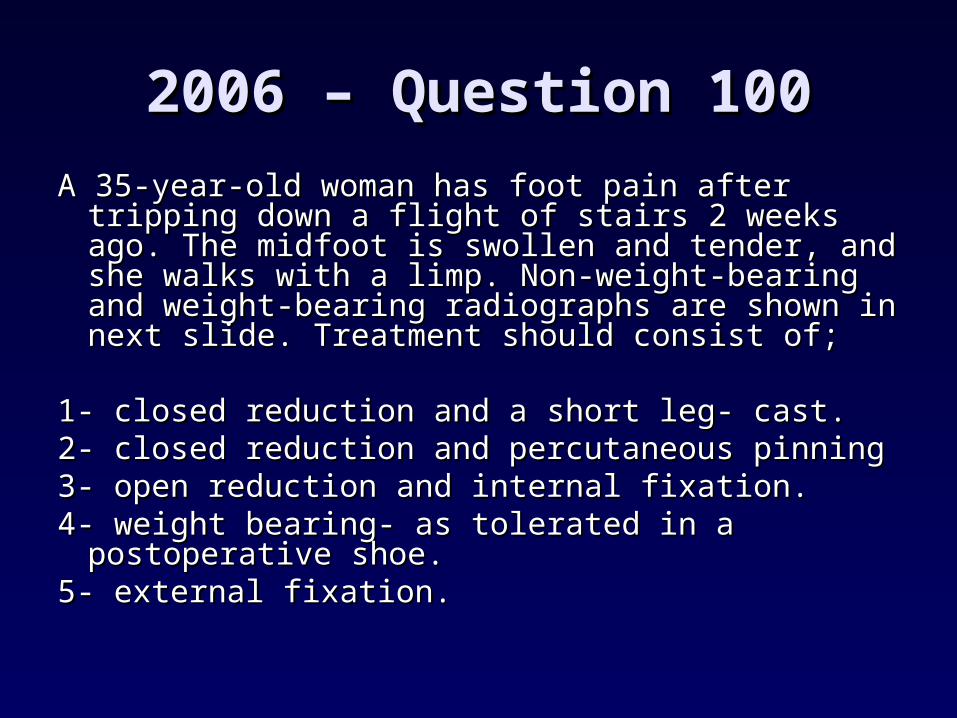
A 35-year-old woman has foot pain after tripping A 35-year-old woman has foot pain after tripping down a flight of stairs 2 weeks ago. The midfoot down a flight of stairs 2 weeks ago. The midfoot is swollen and tender, and she walks with a is swollen and tender, and she walks with a limp. Non-weight-bearing and weight-bearing limp. Non-weight-bearing and weight-bearing radiographs are shown in next slide. Treatment radiographs are shown in next slide. Treatment should consist of; should consist of;
1- closed reduction and a short leg- cast.1- closed reduction and a short leg- cast.2- closed reduction and percutaneous pinning2- closed reduction and percutaneous pinning3- open reduction and internal fixation.3- open reduction and internal fixation.4- weight bearing- as tolerated in a postoperative 4- weight bearing- as tolerated in a postoperative
shoe. shoe. 5- external fixation.5- external fixation.

2006 – Question 1002006 – Question 100
A 35-year-old woman has foot pain after tripping A 35-year-old woman has foot pain after tripping down a flight of stairs 2 weeks ago. The midfoot down a flight of stairs 2 weeks ago. The midfoot is swollen and tender, and she walks with a is swollen and tender, and she walks with a limp. Non-weight-bearing and weight-bearing limp. Non-weight-bearing and weight-bearing radiographs are shown in next slide. Treatment radiographs are shown in next slide. Treatment should consist of; should consist of;
1- closed reduction and a short leg- cast.1- closed reduction and a short leg- cast.2- closed reduction and percutaneous pinning2- closed reduction and percutaneous pinning3- open reduction and internal fixation.3- open reduction and internal fixation.4- weight bearing- as tolerated in a postoperative 4- weight bearing- as tolerated in a postoperative
shoe. shoe. 5- external fixation.5- external fixation.

2 time Grand Slam Champion 2 time Grand Slam Champion (Wimbledon 2004 & US Open 2006) (Wimbledon 2004 & US Open 2006)
Birth date: April 19,1987Birth date: April 19,1987 Birthplace: Siberia, RussiaBirthplace: Siberia, Russia Ht./Wt.: 6'2/130 lbs.Ht./Wt.: 6'2/130 lbs. Plays Right-handedPlays Right-handed Sustained shoulder injury recentlySustained shoulder injury recently
Sport QuestionSport Question

Maria Sharapova

2006 – Question 1102006 – Question 110
Which of the following is considered the most Which of the following is considered the most common problem that limits active common problem that limits active overhead shoulder motion after overhead shoulder motion after hemiarthroplasty performed for a four-part hemiarthroplasty performed for a four-part proximal humeral fracture?proximal humeral fracture?
1- Retroversion of the prosthesis1- Retroversion of the prosthesis
2- Varus alignment of the prosthesis 2- Varus alignment of the prosthesis
3- Acromioclavicular arthritis 3- Acromioclavicular arthritis
4- Greater tuberosity nonunion 4- Greater tuberosity nonunion
5- Use of a cemented stem 5- Use of a cemented stem

2006 – Question 1152006 – Question 115
Which of the following is considered the most Which of the following is considered the most common disadvantage of using posterior anti-common disadvantage of using posterior anti-glide plating in the treatment of lateral malleolar glide plating in the treatment of lateral malleolar fractures compared to lateral neutralization fractures compared to lateral neutralization plating?plating?
1- Intra-articular penetration of the distal screws1- Intra-articular penetration of the distal screws2- Inability to stabilize the syndesmosis2- Inability to stabilize the syndesmosis3- Peroneal irritation if the plate is placed too 3- Peroneal irritation if the plate is placed too
distally distally 4- Poor distal fixation4- Poor distal fixation5- A biomechanically weaker construct5- A biomechanically weaker construct

2006 – Question 1292006 – Question 129
When using hyperbaric oxygen treatment When using hyperbaric oxygen treatment for a crush injury to the extremity, which for a crush injury to the extremity, which of the following mechanisms of action is of the following mechanisms of action is present?present?
1- Increased hydrostatic pressures1- Increased hydrostatic pressures
2- Increased tissue edema2- Increased tissue edema
3- Increased gradient for diffusion 3- Increased gradient for diffusion
4- Decreased leukocyte function4- Decreased leukocyte function
5- Decreased arteriolar vasoconstriction5- Decreased arteriolar vasoconstriction

2006 – Question 1322006 – Question 132
A 66-year-old woman reports persistent pain after A 66-year-old woman reports persistent pain after falling and being diagnosed with a foot sprain 1 year falling and being diagnosed with a foot sprain 1 year ago. She also notes that she is becoming "flatfooted" ago. She also notes that she is becoming "flatfooted" on that side. Radiographs are shown in the following on that side. Radiographs are shown in the following slides. Surgical management should consist ofslides. Surgical management should consist of
1- medial displacement calcaneal osteotomy.1- medial displacement calcaneal osteotomy.2- lateral column lengthening, through the 2- lateral column lengthening, through the
calcaneocuboid joint. calcaneocuboid joint. 3- lateral column lengthening through the calcaneus. 3- lateral column lengthening through the calcaneus. 4- tarsometatarsal arthrodesis.4- tarsometatarsal arthrodesis.5- subtalar fusion 5- subtalar fusion



2006 – Question 1322006 – Question 132
A 66-year-old woman reports persistent pain after A 66-year-old woman reports persistent pain after falling and being diagnosed with a foot sprain 1 year falling and being diagnosed with a foot sprain 1 year ago. She also notes that she is becoming "flatfooted" ago. She also notes that she is becoming "flatfooted" on that side. Radiographs are shown in the following on that side. Radiographs are shown in the following slides. Surgical management should consist ofslides. Surgical management should consist of
1- medial displacement calcaneal osteotomy.1- medial displacement calcaneal osteotomy.2- lateral column lengthening, through the 2- lateral column lengthening, through the
calcaneocuboid joint. calcaneocuboid joint. 3- lateral column lengthening through the calcaneus. 3- lateral column lengthening through the calcaneus. 4- tarsometatarsal arthrodesis.4- tarsometatarsal arthrodesis.5- subtalar fusion 5- subtalar fusion

2006 – Question 1402006 – Question 140
According to the Lauge-Hansen According to the Lauge-Hansen classification. what is the mechanism of classification. what is the mechanism of injury for the fracture shown in next injury for the fracture shown in next slide?slide?
1- Supination external rotation 1- Supination external rotation
2- Supination adduction 2- Supination adduction
3- Pronation abduction 3- Pronation abduction
4- Pronation external rotation 4- Pronation external rotation
5- Pronation dorsiflexion 5- Pronation dorsiflexion


2006 – Question 1402006 – Question 140
According to the Lauge-Hansen According to the Lauge-Hansen classification. what is the mechanism of classification. what is the mechanism of injury for the fracture shown in next injury for the fracture shown in next slide?slide?
1- Supination external rotation 1- Supination external rotation
2- Supination adduction 2- Supination adduction
3- Pronation abduction 3- Pronation abduction
4- Pronation external rotation 4- Pronation external rotation
5- Pronation dorsiflexion 5- Pronation dorsiflexion

2006 – Question 1402006 – Question 140
1- Supination External Rotation: 1- Supination External Rotation: - Spiral fracture of the fibula AT the level of the syndesmosis - Spiral fracture of the fibula AT the level of the syndesmosis
2- Supination adduction:2- Supination adduction:
- Transverse fracture of the fibula below the syndesmosis- Transverse fracture of the fibula below the syndesmosis- Vertically, oriented medial malleolar fracture - Vertically, oriented medial malleolar fracture
3- Pronation abduction:3- Pronation abduction:
- Short, oblique fracture of the fibula AT or ABOVE the level of - Short, oblique fracture of the fibula AT or ABOVE the level of the syndesmosis the syndesmosis
4- Pronation external rotation4- Pronation external rotation
- Spiral fracture of the fibula ABOVE the syndesmosis- Spiral fracture of the fibula ABOVE the syndesmosis
Hallmark:Hallmark:

Pronation-Abduction
Supination External Rotation
Supination-Adduction
Pronation External Rotation

2006 – Question 1432006 – Question 143
What subset of patients is expected to have a What subset of patients is expected to have a poorer outcome following open reduction poorer outcome following open reduction and internal fixation of a displaced intra-and internal fixation of a displaced intra-articular calcaneal fracture?articular calcaneal fracture?
1- Younger men1- Younger men2- Women2- Women3- Patients with a lower post-fracture Bohler 3- Patients with a lower post-fracture Bohler
angleangle4- Patients not receiving workers' 4- Patients not receiving workers'
compensation compensation 5- Patients with a lighter workload5- Patients with a lighter workload
2006 – Question 1512006 – Question 151
What is the most common malalignment What is the most common malalignment after intramedullary nailing of the tibia'?after intramedullary nailing of the tibia'?
1- Varus with proximal one third fractures1- Varus with proximal one third fractures2- Apex posterior with proximal one third 2- Apex posterior with proximal one third
fractures fractures 3- Rotational with distal one third fractures 3- Rotational with distal one third fractures 4- Rotational with proximal one third 4- Rotational with proximal one third
fracturesfractures5- Valgus with distal one third fractures 5- Valgus with distal one third fractures
with an intact fibulawith an intact fibula
2006 – Question 1572006 – Question 157
An 84-year-old woman has an An 84-year-old woman has an intertrochanteric hip fracture. What intertrochanteric hip fracture. What is the best predictor of mortality risk?is the best predictor of mortality risk?
1- American Society of 1- American Society of Anesthesiologists (ASA) classification Anesthesiologists (ASA) classification
2- Patient age2- Patient age3- Fracture type3- Fracture type4- Pre-fracture mobility4- Pre-fracture mobility5- Type of implant used5- Type of implant used

2006 – Question 1592006 – Question 159
What is the preferred method of treatment for What is the preferred method of treatment for the isolated injury shown in next slide?the isolated injury shown in next slide?
1- Sling and swathe for 6 weeks followed by 1- Sling and swathe for 6 weeks followed by motionmotion
2- A sling for 2 weeks, followed by early motion2- A sling for 2 weeks, followed by early motion
3- Open reduction and internal fixation through 3- Open reduction and internal fixation through a posterior approach a posterior approach
4- Open reduction and internal fixation through 4- Open reduction and internal fixation through an anterior approach an anterior approach
5- Percutaneous screw fixation alone 5- Percutaneous screw fixation alone


2006 – Question 1592006 – Question 159
What is the preferred method of treatment for What is the preferred method of treatment for the isolated injury shown in next slide?the isolated injury shown in next slide?
1- Sling and swathe for 6 weeks followed by 1- Sling and swathe for 6 weeks followed by motionmotion
2- A sling for 2 weeks, followed by early motion2- A sling for 2 weeks, followed by early motion
3- Open reduction and internal fixation through 3- Open reduction and internal fixation through a posterior approach a posterior approach
4- Open reduction and internal fixation through 4- Open reduction and internal fixation through an anterior approach an anterior approach
5- Percutaneous screw fixation alone 5- Percutaneous screw fixation alone

Ada and Miller retrospectively reviewed 16 displaced glenoid neck fractures characterized by translational displacement greater than or equal to 1 cm or angulatory deformity greater than or equal to 40 degrees in either the transverse or the coronal plane. The average post-injury follow-up period was 36 months. They found that 20% of patients had decreased range of motion, 50% had pain (of whom 75% had night pain), 40% had weakness with exertion, and 25% noted popping. In particular, they found that these individuals frequently had shoulder abductor weakness and subacromial pain due at least in part to rotator cuff dysfunction. They recommended ORIF for glenoid neck fractures with this degree of displacement.

2006 – Question 1632006 – Question 163
Next slide shows the radiograph of a patient Next slide shows the radiograph of a patient who has medial knee pain. What is the most who has medial knee pain. What is the most likely cause of the pain?likely cause of the pain?
1- Iatrogenic anterior cruciate ligament 1- Iatrogenic anterior cruciate ligament injury?injury?
2- Iatrogenic posterior cruciate ligament 2- Iatrogenic posterior cruciate ligament injury injury
3- Medial collateral ligament injury 3- Medial collateral ligament injury
4- Nail is too distal4- Nail is too distal
5- Distal interlock is too long 5- Distal interlock is too long

2006 – Question 1632006 – Question 163
Next slide shows the radiograph of a patient Next slide shows the radiograph of a patient who has medial knee pain. What is the most who has medial knee pain. What is the most likely cause of the pain?likely cause of the pain?
1- Iatrogenic anterior cruciate ligament 1- Iatrogenic anterior cruciate ligament injury?injury?
2- Iatrogenic posterior cruciate ligament 2- Iatrogenic posterior cruciate ligament injury injury
3- Medial collateral ligament injury 3- Medial collateral ligament injury
4- Nail is too distal4- Nail is too distal
5- Distal interlock is too long 5- Distal interlock is too long
2006 – Question 1662006 – Question 166
What anatomic region or landmark is What anatomic region or landmark is best seen on the iliac oblique best seen on the iliac oblique radiograph of the pelvis?radiograph of the pelvis?
1- Posterior column 1- Posterior column
2- Sacroiliac joint2- Sacroiliac joint
3- Iliopectineal line3- Iliopectineal line
4- Profile of the obturator foramen 4- Profile of the obturator foramen
5- Posterior all of the acetabular 5- Posterior all of the acetabular

Iliac obliqueIliac oblique Ilioischial line Ilioischial line
Posterior Posterior columncolumn
Anterior wallAnterior wall
Obturator obliqueObturator oblique Iliopectineal line Iliopectineal line
Anterior columnAnterior column
Posterior wallPosterior wall

2006 – Question 1702006 – Question 170
To decrease morbidity and mortality in an elderly To decrease morbidity and mortality in an elderly ambulatory patient with a displaced femoral ambulatory patient with a displaced femoral neck fracture. Optimal management should neck fracture. Optimal management should include:include:
1- Surgical intervention within 4 days of injury.1- Surgical intervention within 4 days of injury.
2- Open reduction and internal fixation. 2- Open reduction and internal fixation.
3- A delay in surgery of 7 days.3- A delay in surgery of 7 days.
4- Early surgery irrespective of medical 4- Early surgery irrespective of medical comorbidities. comorbidities.
5- Transfer to a level 1 trauma center 5- Transfer to a level 1 trauma center

2006 – Question 1722006 – Question 172
What is the proper order for screw What is the proper order for screw insertion to obtain fracture insertion to obtain fracture compression and lag screw fixation compression and lag screw fixation through the dynamic compression plate through the dynamic compression plate shown in the picture?shown in the picture?
1- B, E, C 1- B, E, C 2- C, D, A 2- C, D, A 3- C, B, E 3- C, B, E 4- D, B, C 4- D, B, C 5- D, A, C5- D, A, C

2006 – Question 1762006 – Question 176
Compared to harvesting of cancellous Compared to harvesting of cancellous bone from the outer table of the bone from the outer table of the anterior pelvis. Retrieval from the anterior pelvis. Retrieval from the posterior pelvis is associated withposterior pelvis is associated with
1- a similar overall complication rate1- a similar overall complication rate
2- greater blood loss2- greater blood loss
3- greater duration of pain3- greater duration of pain
4- greater level of pain4- greater level of pain
5- less mean graft volume5- less mean graft volume

2006 – Question 1852006 – Question 185
In which of the following situations would In which of the following situations would locked plating offer the greatest theoretical locked plating offer the greatest theoretical advantage?advantage?
1- A 37-year-old woman with a segmentally 1- A 37-year-old woman with a segmentally transverse radial fracturetransverse radial fracture
2- A 37-year-old woman with an oblique radial 2- A 37-year-old woman with an oblique radial fracturefracture
3- A 65-year-old woman with a humeral 3- A 65-year-old woman with a humeral nonunion treated previously with a plate nonunion treated previously with a plate
4- A 40-year-old man with a segmentally 4- A 40-year-old man with a segmentally comminuted humeral fracture comminuted humeral fracture
5- A 65-year-old man with a segmentally 5- A 65-year-old man with a segmentally comminuted humeral fracturecomminuted humeral fracture
2006 – Question 1882006 – Question 188
What soft-tissue structure is most likely What soft-tissue structure is most likely to be injured in association with low to be injured in association with low energy tibial plateau fracture shown in energy tibial plateau fracture shown in next slide?next slide?
1- Medial collateral ligament1- Medial collateral ligament
2- Lateral collateral ligament 2- Lateral collateral ligament
3- Anterior cruciate ligament 3- Anterior cruciate ligament
4- Posterior cruciate ligament 4- Posterior cruciate ligament
5- Lateral meniscus 5- Lateral meniscus


2006 – Question 1882006 – Question 188
What soft-tissue structure is most likely What soft-tissue structure is most likely to be injured in association with low to be injured in association with low energy tibial plateau fracture shown in energy tibial plateau fracture shown in next slide?next slide?
1- Medial collateral ligament1- Medial collateral ligament
2- Lateral collateral ligament 2- Lateral collateral ligament
3- Anterior cruciate ligament 3- Anterior cruciate ligament
4- Posterior cruciate ligament 4- Posterior cruciate ligament
5- Lateral meniscus 5- Lateral meniscus

2006 – Question 1932006 – Question 193
Nonunion of a surgically treated tibial Nonunion of a surgically treated tibial diaphyseal fracture correlates most diaphyseal fracture correlates most closely withclosely with
1- fracture comminution1- fracture comminution
2- gapping at the fracture site2- gapping at the fracture site
3- a nonsurgically treated fibular 3- a nonsurgically treated fibular fracturefracture
4- a mid-diaphyseal location4- a mid-diaphyseal location
5- a closed section nail5- a closed section nail

2006 – Question 1962006 – Question 196
The injury shown in next slide is The injury shown in next slide is classified as what type of acetabular classified as what type of acetabular fracture?fracture?
1- T-shaped1- T-shaped
2- Posterior wall 2- Posterior wall
3- Transverse3- Transverse
4- Posterior column 4- Posterior column
5- Both column5- Both column

2006 – Question 1962006 – Question 196
The injury shown in next slide is The injury shown in next slide is classified as what type of acetabular classified as what type of acetabular fracture?fracture?
1- T-shaped1- T-shaped
2- Posterior wall 2- Posterior wall
3- Transverse3- Transverse
4- Posterior column 4- Posterior column
5- Both column5- Both column

Fracture Type
ObturatorRingFracture
IlioischialLineDisrupted
IliopectinealLineDisrupted
IliacWing #
PosteriorWall #
PelvisIntoHalves
SpurSign
CT ScanFractureOrientation
Both-column Yes Yes Yes Yes No Front/back Yes Horizontal
Anterior column Yes No Yes Yes No Front/back No Horizontal
Posteriorcolumn
Yes Yes No No No Front/back No Horizontal
Posteriorcolumn withposterior wall
Yes Yes No No Yes Front/back No Horizontal
T-shaped Yes Yes Yes No NoTop/
bottomNo Vertical
Transverse withposterior wall
No Yes Yes No YesTop/
bottomNo Vertical
Transverse No Yes Yes No NoTop/
bottomNo Vertical
Posterior wall No No No No Yes No No Oblique
Anterior wall No No Yes No No No No Oblique
Anterior columnwith posteriorhemitransverse
No Yes Yes Yes No N/A* No N/A

2006 – Question 2012006 – Question 201When treating a tibial fracture with the long lateral plate When treating a tibial fracture with the long lateral plate
shown in next slide, what structure is at greatest risk of' shown in next slide, what structure is at greatest risk of' iatrogenic injury during percutaneous screw insertion?iatrogenic injury during percutaneous screw insertion?
1- Common peroneal nerve with placement of the proximal 1- Common peroneal nerve with placement of the proximal posterior screw posterior screw
2- Posterior tibial nerve with placement of the proximal 2- Posterior tibial nerve with placement of the proximal posterior screw posterior screw
3- Peroneal nerve with placement of the middle screw 3- Peroneal nerve with placement of the middle screw 4- Superficial peroneal nerve with placement of the middle 4- Superficial peroneal nerve with placement of the middle
screw screw 5- Superficial peroneal nerve with placement of the distal 5- Superficial peroneal nerve with placement of the distal
screwscrew


2006 – Question 2012006 – Question 201When treating a tibial fracture with the long lateral plate When treating a tibial fracture with the long lateral plate
shown in next slide, what structure is at greatest risk of' shown in next slide, what structure is at greatest risk of' iatrogenic injury during percutaneous screw insertion?iatrogenic injury during percutaneous screw insertion?
1- Common peroneal nerve with placement of the proximal 1- Common peroneal nerve with placement of the proximal posterior screw posterior screw
2- Posterior tibial nerve with placement of the proximal 2- Posterior tibial nerve with placement of the proximal posterior screw posterior screw
3- Peroneal nerve with placement of the middle screw 3- Peroneal nerve with placement of the middle screw 4- Superficial peroneal nerve with placement of the middle 4- Superficial peroneal nerve with placement of the middle
screw screw 5- Superficial peroneal nerve with placement of the distal 5- Superficial peroneal nerve with placement of the distal
screwscrew

2006 – Question 2292006 – Question 229A 24-year-old man hits a deer while driving unrestrained. On arrival at the A 24-year-old man hits a deer while driving unrestrained. On arrival at the
emergency department his cervical spine is cleared, a CT of the head is normal, emergency department his cervical spine is cleared, a CT of the head is normal, and he has a blood pressure of 90/60 mm Hg. He has no intra-abdominal and he has a blood pressure of 90/60 mm Hg. He has no intra-abdominal injuries. After administration of 3 L of crystalloid, his blood pressure rises to injuries. After administration of 3 L of crystalloid, his blood pressure rises to 120/90 mm Hg. In addition to a pneumothorax and a chest tube examination 120/90 mm Hg. In addition to a pneumothorax and a chest tube examination reveals a right, closed midshaft femoral fracture and a left open both bone reveals a right, closed midshaft femoral fracture and a left open both bone forearm fracture with a 1.5 cm dorsal wound and visible bone. Treatment forearm fracture with a 1.5 cm dorsal wound and visible bone. Treatment should consist of:should consist of:
1- External fixation of 'the femoral fracture, irrigation and debridement, and 1- External fixation of 'the femoral fracture, irrigation and debridement, and external fixation of the forearm fractureexternal fixation of the forearm fracture
2- External fixation of the 1'enloral fracture, irrigation and debridement, and 2- External fixation of the 1'enloral fracture, irrigation and debridement, and plating of the forearm fractureplating of the forearm fracture
3- Intramedullary nailing of the femur, irrigation and debridement, and external 3- Intramedullary nailing of the femur, irrigation and debridement, and external fixation of the forearm fracturefixation of the forearm fracture
4- Intramedullary nailing of the femur, irrigation and debridement and plating of 4- Intramedullary nailing of the femur, irrigation and debridement and plating of the forearm fracturethe forearm fracture
5- Femoral traction, irrigation and debridement, and casting of the forearm fracture5- Femoral traction, irrigation and debridement, and casting of the forearm fracture

2006 – Question 2372006 – Question 237
Submuscular plating technique, when compared to Submuscular plating technique, when compared to conventional plating techniques, offerconventional plating techniques, offer
1- less compromise to medullary and periosteal 1- less compromise to medullary and periosteal perfusion.perfusion.
2- greater compromise to medullary and periosteal 2- greater compromise to medullary and periosteal perfusion. perfusion.
3- no difference with regard to periosteal perfusion 3- no difference with regard to periosteal perfusion only. only.
4- no difference with regard to medullary perfusion 4- no difference with regard to medullary perfusion only.only.
5- no difference with regard to periosteal and 5- no difference with regard to periosteal and medullary perfusion medullary perfusion

2006 – Question 2452006 – Question 245
Early regional osteopenia beneath a Early regional osteopenia beneath a plate after dynamic compression plate after dynamic compression plating is a direct result ofplating is a direct result of
1 - stress shielding1 - stress shielding
2- implant-bone contact2- implant-bone contact
3- implant material3- implant material
4- circumferential periosteal stripping4- circumferential periosteal stripping
5- quiescent infection5- quiescent infection
2006 – Question 2462006 – Question 246
Next slide show the injury a 26-year-old man Next slide show the injury a 26-year-old man sustained in a motor vehicle accident 12 sustained in a motor vehicle accident 12 days ago. The soft-tissue envelope is and has days ago. The soft-tissue envelope is and has been unremarkable, and no neurovascular been unremarkable, and no neurovascular deficits exist. Definitive treatment should deficits exist. Definitive treatment should consist ofconsist of
1- hybrid external fixation.1- hybrid external fixation.2- transarticular external fixation.2- transarticular external fixation.3- dual plate fixation with two surgical 3- dual plate fixation with two surgical
approaches.approaches.4- lateral locking plate fixation with a single 4- lateral locking plate fixation with a single
surgical approach. surgical approach. 5- dual plating with a single surgical approach.5- dual plating with a single surgical approach.


2006 – Question 2462006 – Question 246
Next slide show the injury a 26-year-old man Next slide show the injury a 26-year-old man sustained in a motor vehicle accident 12 days sustained in a motor vehicle accident 12 days ago. The soft-tissue envelope is and has been ago. The soft-tissue envelope is and has been unremarkable, and no neurovascular deficits unremarkable, and no neurovascular deficits exist. Definitive treatment should consist ofexist. Definitive treatment should consist of
1- hybrid external fixation1- hybrid external fixation2- transarticular external fixation2- transarticular external fixation3- dual plate fixation with two surgical 3- dual plate fixation with two surgical
approachesapproaches4- lateral locking plate fixation with a single 4- lateral locking plate fixation with a single
surgical approachsurgical approach5- dual plating with a single surgical approach5- dual plating with a single surgical approach

2006 – Question 2512006 – Question 251
What is the most appropriate treatment method for What is the most appropriate treatment method for a displaced vertical medial malleolus fracture?a displaced vertical medial malleolus fracture?
1- Casting in supination1- Casting in supination
2- Casting in pronation2- Casting in pronation
3- Two oblique screws from the tip of the medial 3- Two oblique screws from the tip of the medial malleolusmalleolus
4- Tension hand fixation with two oblique Kirschner 4- Tension hand fixation with two oblique Kirschner wires from the medial malleolus and I8-gauge wires from the medial malleolus and I8-gauge WireWire
5- Medial antiglide plate5- Medial antiglide plate
2006 Question 256 2006 Question 256
Which of the following, associated injuries is Which of the following, associated injuries is most commonly noted during arthroscopy most commonly noted during arthroscopy after acute shoulder dislocation?after acute shoulder dislocation?
1 - Anterior labral tears1 - Anterior labral tears2- Posterior labral tears2- Posterior labral tears3- Complete rotator cuff tear3- Complete rotator cuff tear4- Hill-Sach lesions4- Hill-Sach lesions5- Superior labrum anterior and posterior 5- Superior labrum anterior and posterior
(SLAP) lesions(SLAP) lesions
2006 Question 258 2006 Question 258
The working, length of a bicortical screw is The working, length of a bicortical screw is defined as thedefined as the
1- pitch of the screw.1- pitch of the screw.
2- sum of thickness of the near and far bone 2- sum of thickness of the near and far bone cortices cortices
3- intratmedullary distance traversed by the 3- intratmedullary distance traversed by the screwscrew
4- length of screw projecting beyond the far 4- length of screw projecting beyond the far cortexcortex
5- diameter of bone traversed by the screw5- diameter of bone traversed by the screw
2006 Question 2692006 Question 269
Factors contributing to an apex anterior Factors contributing to an apex anterior sagittal plane deformity when sagittal plane deformity when introducing an intramedullary nail to introducing an intramedullary nail to manage a proximal tibial fracture manage a proximal tibial fracture include all of the following include all of the following EXCEPTEXCEPT
1- anterior starting hole1- anterior starting hole2- interlocking, in flexion2- interlocking, in flexion3- posterior cortical comminution 3- posterior cortical comminution 4- posteriorly directed tibial nail4- posteriorly directed tibial nail5- posteriorly placed blocking screw5- posteriorly placed blocking screw

2006 Question 2692006 Question 269
The advantage of using blocking screws The advantage of using blocking screws during intramedullary nailing of during intramedullary nailing of metaphyseal tibial fractures include all of metaphyseal tibial fractures include all of the following EXCEPTthe following EXCEPT
1- facilitate reduction1- facilitate reduction
2- maintain reduction2- maintain reduction
3- enhance construct stiffness3- enhance construct stiffness
4- neutralize translation forces4- neutralize translation forces
5- diminish the risk of nail failure5- diminish the risk of nail failure
