okeson outline copy
DESCRIPTION
book notesTRANSCRIPT

1
Okeson: Mgmt of TMD & Occlusion
Chapter 1: Functional Anatomy and Biomechanics of Mastication .................................................. 2
Chapter 2: Functional Neuroanatomy and Physiology of Masticatory System.................................. 4
Chapter 3: Alignment and Occlusion of the Dentition...................................................................... 6
Chapter 4: Mechanics of Mandibular Movement ............................................................................. 8
Chapter 5: Criteria for Optimal Functional Occlusion...................................................................... 9
Chapter 6: Determinates of occlusal morphology........................................................................... 10
Chapter 7: Causes of functional disturbances in the masticatory system......................................... 12
Chapter 8: Signs & Symptoms of TMD......................................................................................... 13
Chapter 9: History & Examination for TMD ................................................................................. 15
Chapter 10: Diagnosis of TMD...................................................................................................... 16
Chapter 12: Treatment of Masticatory Muscle Disorders ............................................................... 21
Chapter 13: TMD and Treatments ................................................................................................. 22
Chapter 14: Tx of Chronic MN Hypomobility and Growth Disorders............................................ 23
Chapter 15: Occlusal Appliance Therapy....................................................................................... 24
Chapter 16: Treatment Sequencing................................................................................................ 26
Chapter 17: General Considerations in Occlusal Therapy .............................................................. 27
Chapter 18: Articulators in Occlusal Therapy................................................................................ 28
Chapter 19: Selective Grinding..................................................................................................... 29
Chapter 20: Restorative Considerations in Occlusal Therapy......................................................... 30
2
Chapter 1: Functional Anatomy and Biomechanics of Mastication Masticatory system – functional unit of the body primarily responsible for chewing, speaking, and
swallowing - Composed of: bones, joints, ligaments, and teeth
Maxilla: two maxillary bones are fused together at the midpalatal suture making up greater part of upper
facial skeleton.
• Superiorl border forms floor of nasal cavity and floor of each orbit
• inferiorly forms palate and alveolar ridges
Mandible: U-shaped bone supporting lower teeth and making lower facial skeleton with no bony attachments
to skull, suspended below maxilla by muscles, ligaments, and other soft tissues providing the mobility
necessary to function with maxilla.
• superior aspect- alveolar process and the teeth.
• body of the mandible - form mandibular angle and ascending ramus extending upward as two
processes - coronoid process and condyle which articulates with the cranium
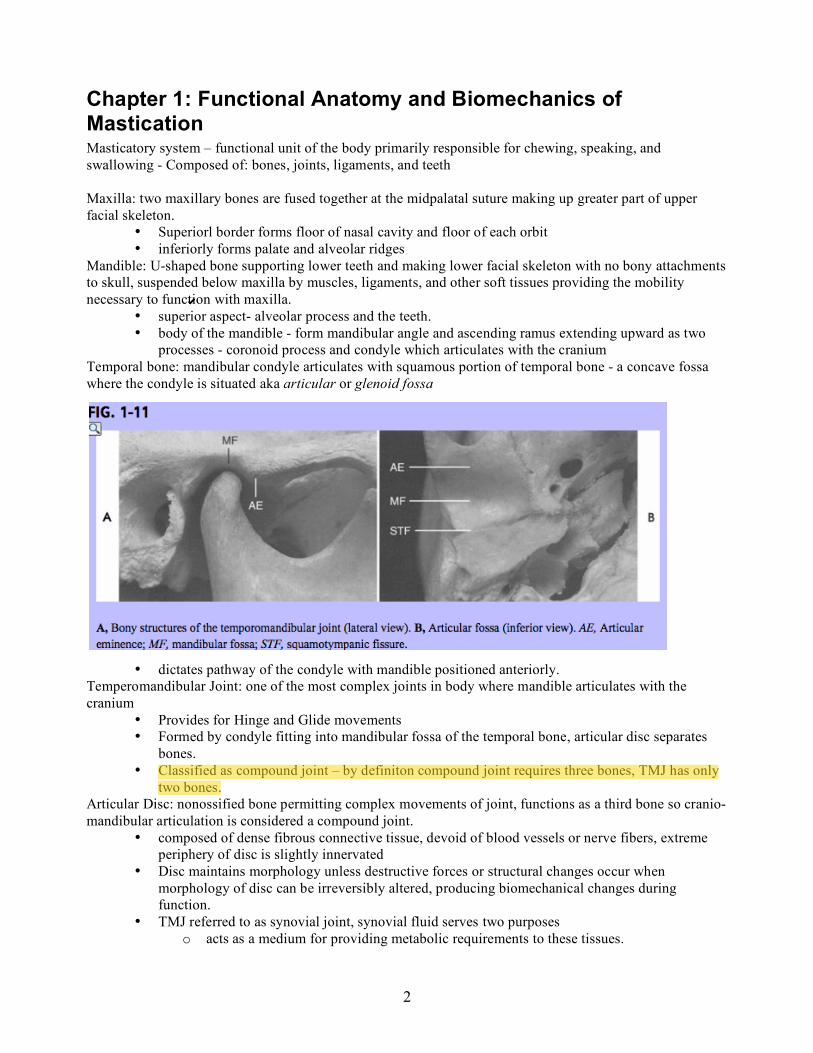
Temporal bone: mandibular condyle articulates with squamous portion of temporal bone - a concave fossa
where the condyle is situated aka articular or glenoid fossa
• Articular eminence: convex bony prominence anterior to fossa whose steepness
•
• dictates pathway of the condyle with mandible positioned anteriorly.
Temperomandibular Joint: one of the most complex joints in body where mandible articulates with the
cranium
• Provides for Hinge and Glide movements
• Formed by condyle fitting into mandibular fossa of the temporal bone, articular disc separates
bones.
• Classified as compound joint – by definiton compound joint requires three bones, TMJ has only
two bones.
Articular Disc: nonossified bone permitting complex movements of joint, functions as a third bone so cranio-
mandibular articulation is considered a compound joint.
• composed of dense fibrous connective tissue, devoid of blood vessels or nerve fibers, extreme
periphery of disc is slightly innervated
• Disc maintains morphology unless destructive forces or structural changes occur when
morphology of disc can be irreversibly altered, producing biomechanical changes during
function.
• TMJ referred to as synovial joint, synovial fluid serves two purposes
o acts as a medium for providing metabolic requirements to these tissues.

3
o lubricant between articular surfaces during function, friction during movement is
minimized
Innervation of the TMJ: same nerve (the trigeminal nerve – V3) that provides motor and sensory innervation
to TMJ also innervate muscles that control it.
• Most innervation is provided by the auriculotemporal nerve as it leaves the mandibular nerve
behind the joint,
• deep temporal and masseteric nerves provide additional innervation.
Vascularization of the TMJ: provided by many vessels, predominantly
• superficial temporal artery from the posterior
• middle meningeal artery from anterior
• internal maxillary artery from the inferior.
Ligaments of the TMJ: play key role in protecting the structures, collagenous connective tissues that have
particular lengths and don’t stretch. However, with force, suddenly or over a prolonged period of time, the
ligament can be elongated
• 1. Collateral Discal Ligament: responsible for dividing joint mediolaterally into the superior and
inferior joint cavities,
o true ligaments - collagenous connective tissue fibers so do not stretch.
o Restrict movement of disc away from the condyle allowing disc to move passively with
the condyle as it glides anteriorly and posteriorly.
o responsible for hinging movement of the TMJ, between condyle and articular disc.
• 2. Capsular Ligament - entire TMJ is surrounded and encompassed by the capsular ligament
o resists medial, lateral, or inferior forces that tend to separate or dislocate the articular
surfaces, retains the synovial fluid.
• 3. Temperomandibular Ligament- lateral aspect of capsular ligament of strong, tight fibers,
composed of outer oblique portion and inner horizontal portion
o oblique portion - resists excessive dropping of the condyle; limiting mouth opening.
If the jaw is opened wider, distinct change in opening movement will occur,
represents change from rotation to movement forward and down the articular
eminence as TM ligament tightens.
o Inner horizontal portion of ligament limits posterior movement of the condyle and disc
protecting retrodiscal tissues from trauma
• 4. Sphenomandibular Ligament - accessory ligament, has no significant limiting effects on
mandibular movement.
• 5. Stylomandibular Ligament - limits excessive protrusive movements of mandible.
Muscles of Mastication: have only one nerve ending near the middle of the fiber, innervates each fiber.
Higher myoglobin = deeper red & slow but sustained contraction (type I muscle fibers), well-developed
aerobic metabolism, thus resistant to fatigue. Lower concentrations of myoglobin are whiter (type II fibers),
fewer mitochondria and rely more on anaerobic activity for function, capable of quick contraction but fatigue
more rapidly.
1. Masseter: elevates mandible and teeth brought into contact.
o Powerful, provides force necessary to chew efficiently, may aid in protruding the
mandible.
2. Temporalis: elevates the mandible and the teeth are brought into contact.
3. Medial Pterygoid: with masseter, forms muscular sling supporting the mandible at mandibular angle.
• Elevates mandible and teeth are brought into contact, also active in protruding the mandible.
4. Inferior Lateral Pterygoid: functions with the mandibular depressors to lower mandible and condyles glide
forward and downward on the articular eminences.

4
5. Superior Lateral Pterygoid: active during power stroke (movements involving closure of mandible) and
when teeth are held together.
6. Digastrics:
• right and left digastrics contract to help depress mandible and teeth brought out of contact.
• along with suprahyoid and infrahyoid muscles, elevate the hyoid bone, necessary function for
swallowing
Chapter 2: Functional Neuroanatomy and Physiology of Masticatory System Central Pattern Generator (CPG): pool of neurons controlling rhythmic muscle activities like
chewingEfficient pattern minimizes damage to structures, learned and repeated pattern called muscle
engram.
The three major functions of the masticatory system are:
(1) mastication
(2) swallowing
(3) speech.
• Secondary functions aid in respiration and expression of emotions.
Mastication: rhythmic and well-controlled separation and closure of maxillary and mandibular teeth, via
CPG in brainstem.
• chewing stroke is tear-shaped, divided into opening & closing movement.
o Closing further divided: crushing phase and grinding phase.
Early studies: teeth do not actually contact during mastication. Speculated food between teeth, along with the
acute response of the neuromuscular system, prohibits tooth contacts.
Other studies: have revealed that tooth contacts occur during mastication.
• New Food - few contacts initially,
• bolus broken down - frequency of tooth contacts increases.
• final stages of mastication contacts occur during every stroke.
• Two types of contact have been identified:
o gliding contact - cuspal inclines pass by each other
o single contact - occurs in the maximum intercuspal position.
Average contact time during mastication: 194 msec.
• contacts influence/dictate initial opening and final grinding phase
5
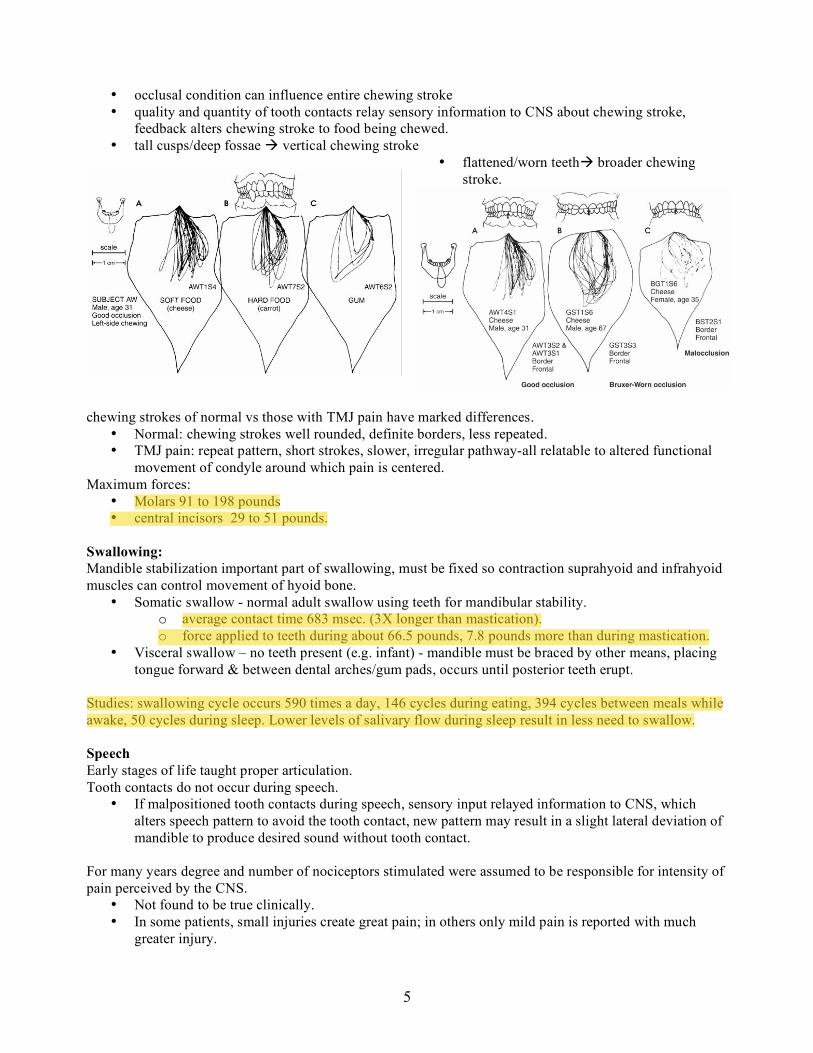
• occlusal condition can influence entire chewing stroke
• quality and quantity of tooth contacts relay sensory information to CNS about chewing stroke,
feedback alters chewing stroke to food being chewed.
• tall cusps/deep fossae vertical chewing stroke
• flattened/worn teeth broader chewing
stroke.
chewing strokes of normal vs those with TMJ pain have marked differences.
• Normal: chewing strokes well rounded, definite borders, less repeated.
• TMJ pain: repeat pattern, short strokes, slower, irregular pathway-all relatable to altered functional
movement of condyle around which pain is centered.
Maximum forces:
• Molars 91 to 198 pounds
• central incisors 29 to 51 pounds.
Swallowing:
Mandible stabilization important part of swallowing, must be fixed so contraction suprahyoid and infrahyoid
muscles can control movement of hyoid bone.
• Somatic swallow - normal adult swallow using teeth for mandibular stability.
o average contact time 683 msec. (3X longer than mastication).
o force applied to teeth during about 66.5 pounds, 7.8 pounds more than during mastication.
• Visceral swallow – no teeth present (e.g. infant) - mandible must be braced by other means, placing
tongue forward & between dental arches/gum pads, occurs until posterior teeth erupt.
Studies: swallowing cycle occurs 590 times a day, 146 cycles during eating, 394 cycles between meals while
awake, 50 cycles during sleep. Lower levels of salivary flow during sleep result in less need to swallow.
Speech
Early stages of life taught proper articulation.
Tooth contacts do not occur during speech.
• If malpositioned tooth contacts during speech, sensory input relayed information to CNS, which
alters speech pattern to avoid the tooth contact, new pattern may result in a slight lateral deviation of
mandible to produce desired sound without tooth contact.
For many years degree and number of nociceptors stimulated were assumed to be responsible for intensity of
pain perceived by the CNS.
• Not found to be true clinically.
• In some patients, small injuries create great pain; in others only mild pain is reported with much
greater injury.

6
• As pain has been studied, become increasingly clear that degree of suffering does not relate well to
amount of tissue damage. Instead the degree of suffering relates more closely to the patient's
perceived threat of injury and amount of attention given to injury.
Pain terminology:
• Nociception - noxious stimulus originating from sensory receptor, carried into the CNS by the
primary neuron.
• Pain is unpleasant sensation perceived in the cortex
• Suffering - how human reacts to perception of pain.
• Pain behavior - individual's audible and visible actions that communicate suffering to others.
• source of pain is where the pain originates.
• site of pain is where the patient perceives the pain to be coming from.
The experience of pain (and eventually suffering) may be the most important consideration in caring for
patients.
Types of Pain:
• Central pain - When a tumor or other disturbance is present in the CNS, the pain is often felt in
peripheral structures.
• Projected pain - neurologic disturbances causing pain sensations down the peripheral distributions of
same nerve root that is involved in disturbance.
3. Referred pain. sensations are felt in other branches of nerve
• Referred pain is not a haphazard occurrence but seems to follow three clinical rules:
o most frequently within a single nerve root, passing from one branch to another (e.g., a
mandibular molar referring pain to a maxillary molar).
o can be felt outside the nerve responsible for it, generally moves cephalad (i.e., upward,
toward the head) and not caudal.
o In trigeminal area, referred pain never crosses midline unless it originates at midline, e.g.
pain in right TMJ will not cross over to left side of face. (not true for cervical region or
below)
Local provocation of pain source increase in symptoms
Local provocation of site of pain generally does not increase symptoms
Chapter 3: Alignment and Occlusion of the Dentition Occlusion- static relationship of teeth, basic to all aspects of dentistry
Neutral position – tooth position with equal labio-lingual & bucco-lingual forces
• Tooth stability: tooth too far lingual & tongue moves it buccally & vice versa
• Tongue & lip forces constant – can move teeth (as can muscular forces)
o Large active tongue get open bite
• Proximal contacts also help maintain tooth alignment
o Loss of tooth struct or extraction mesial tipping
• Occlusal contacts – prevent super-eruption/extrusion
Occlusal table – between buccal and lingual cusps, major mastication forces applied here
Intra-arch tooth alignment 0 relationship of teeth in one arch to those in other
• Arch lengths – Mx 128mm, Mn 126mm (distal surface of 3rds to 3rds)
• Arch width – distance across arch Mx > Mn
Non-centric (aka Guiding cusp) – Mx buccal, Mn lingual cusps
• Provide stability: guide teeth in & out of full occlusion (mx intercuspation)
Centric cusps – Mx lingual & Mn buccal (aka supporting, holding, occluding cusps)
7
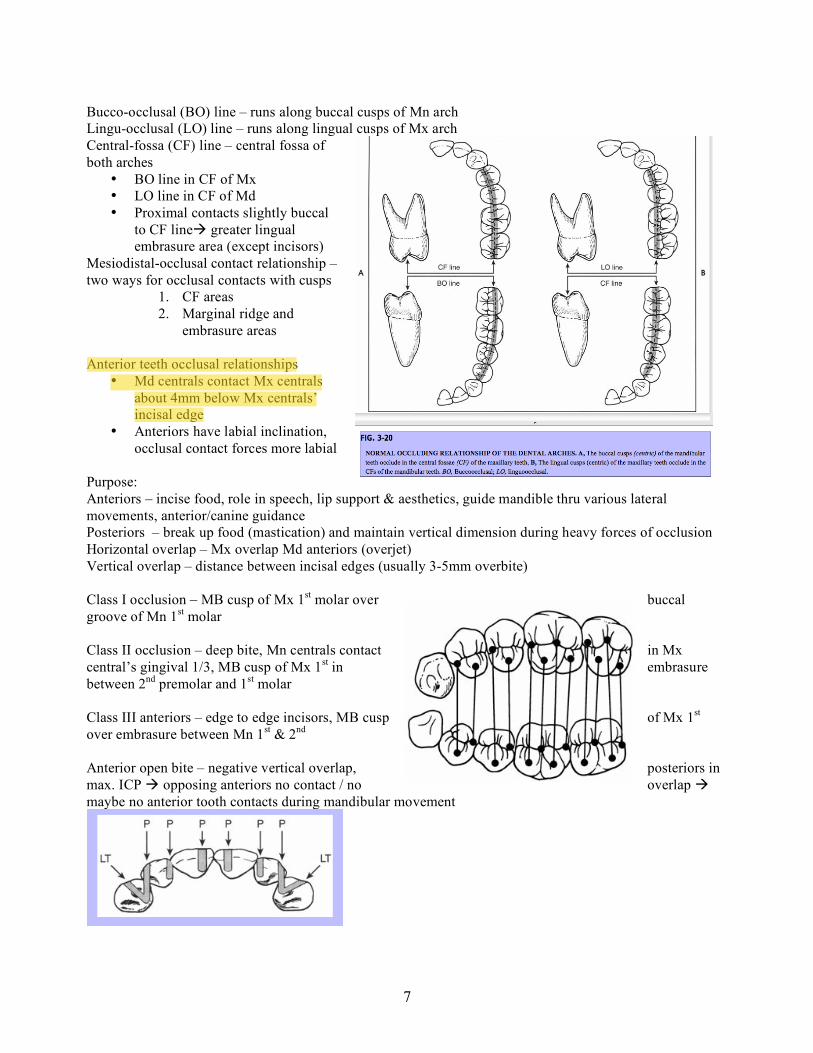
Bucco-occlusal (BO) line – runs along buccal cusps of Mn arch
Lingu-occlusal (LO) line – runs along lingual cusps of Mx arch
Central-fossa (CF) line – central fossa of
both arches
• BO line in CF of Mx
• LO line in CF of Md
• Proximal contacts slightly buccal
to CF line greater lingual
embrasure area (except incisors)
Mesiodistal-occlusal contact relationship –
two ways for occlusal contacts with cusps
1. CF areas
2. Marginal ridge and
embrasure areas
Anterior teeth occlusal relationships
• Md centrals contact Mx centrals
about 4mm below Mx centrals’
incisal edge
• Anteriors have labial inclination,
occlusal contact forces more labial
Purpose:
Anteriors – incise food, role in speech, lip support & aesthetics, guide mandible thru various lateral
movements, anterior/canine guidance
Posteriors – break up food (mastication) and maintain vertical dimension during heavy forces of occlusion
Horizontal overlap – Mx overlap Md anteriors (overjet)
Vertical overlap – distance between incisal edges (usually 3-5mm overbite)
Class I occlusion – MB cusp of Mx 1st molar over buccal
groove of Mn 1st molar
Class II occlusion – deep bite, Mn centrals contact in Mx
central’s gingival 1/3, MB cusp of Mx 1st in embrasure
between 2nd
premolar and 1st molar
Class III anteriors – edge to edge incisors, MB cusp of Mx 1st
over embrasure between Mn 1st & 2
nd
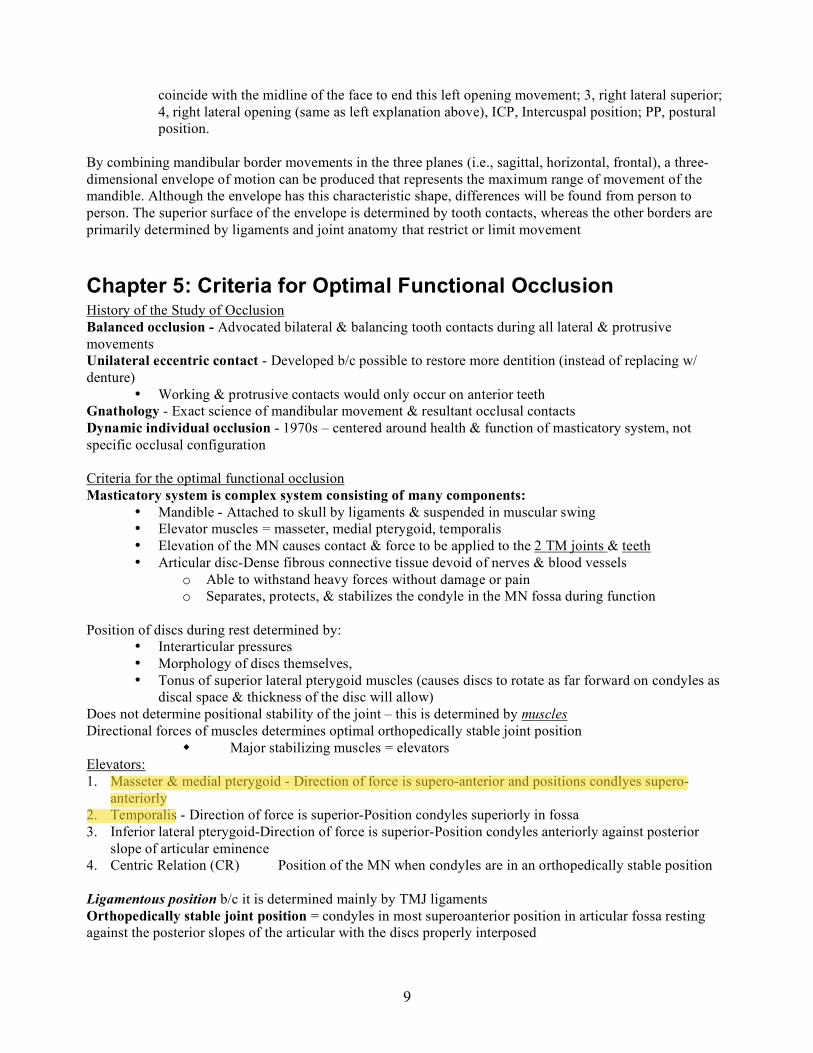
Anterior open bite – negative vertical overlap, posteriors in
max. ICP opposing anteriors no contact / no overlap
maybe no anterior tooth contacts during mandibular movement

8
Chapter 4: Mechanics of Mandibular Movement MN movement is determined by the combined and simultaneous activities of both TMJs, which cannot
function entirely independently of each other and rarely function with identical concurrent movements
Two types of movement (during most movements, both occur simultaneously):
• Rotational – movement between the superior surface of the condyle and the inferior surface of
the articular disc
o Can occur in three reference planes around the axis:
o (1) horizontal – opening/closing, called hinge movement, only example of “pure”
rotational movement
o (2) frontal (vertical) – one condyle moves anteriorly out of terminal hinge position with
the opposite condyle remaining in terminal hinge position (this isolated movement does
not occur naturally – need other movements as well)
o (3) sagital – one condyle moves inferiorly while the other remains in the terminal hinge
position; ligaments/muscles prevent inferior displacement of condyle so this movement
must occur in conjunction with other movements
• Translational – occurs when MN moves forward, as in protrusion, within the superior cavity of
the joint, between the superior surface of the articular disc and the inferior surface of the
articular fossa
Sagittal Plane Border and Functional Movements - The range of posterior
and anterior opening border movements is determined, or limited, primarily by
ligaments and the morphology of the TMJs. Superior contact border
movements are determined by the occlusal and incisal surfaces of the teeth.
1, Posterior opening border -> TM ligament (upper part) then
sphenomandibular ligament (lower part); 2, anterior opening border -> lateral
pterygoids; 3, superior contact border -> occluding sufaces of teeth; 4, typical
functional.
Postural position (MN at rest) – 2-4mm below ICP
MN Border Movements in Horizontal Plane
1, Left lateral -> caused by contraction of rt lateral
pterygoid (left condyle is rotating/working and rt
condyle is orbiting/non-working); 2, continued
left lateral with protrusion -> rt & left lat
pterygoid; 3, right lateral -> left lat ptrerygoid; 4,
continued right lateral with protrusion -> rt & left
lat pterygoid. CR, Centric relation; ICP, intercuspal position.
MN Movements in Frontal Plane
• Mandibular border movements in the frontal plane. 1, Left lateral superior; 2, left
lateral opening - As maximum opening is approached, ligaments tighten and
produce a medially directed movement that causes a shift back in the mandibular midline to
9
coincide with the midline of the face to end this left opening movement; 3, right lateral superior;
4, right lateral opening (same as left explanation above), ICP, Intercuspal position; PP, postural
position.
By combining mandibular border movements in the three planes (i.e., sagittal, horizontal, frontal), a three-
dimensional envelope of motion can be produced that represents the maximum range of movement of the
mandible. Although the envelope has this characteristic shape, differences will be found from person to
person. The superior surface of the envelope is determined by tooth contacts, whereas the other borders are
primarily determined by ligaments and joint anatomy that restrict or limit movement
Chapter 5: Criteria for Optimal Functional Occlusion History of the Study of Occlusion
Balanced occlusion - Advocated bilateral & balancing tooth contacts during all lateral & protrusive
movements
Unilateral eccentric contact - Developed b/c possible to restore more dentition (instead of replacing w/
denture)
• Working & protrusive contacts would only occur on anterior teeth
Gnathology - Exact science of mandibular movement & resultant occlusal contacts
Dynamic individual occlusion - 1970s – centered around health & function of masticatory system, not
specific occlusal configuration
Criteria for the optimal functional occlusion
Masticatory system is complex system consisting of many components:
• Mandible - Attached to skull by ligaments & suspended in muscular swing
• Elevator muscles = masseter, medial pterygoid, temporalis
• Elevation of the MN causes contact & force to be applied to the 2 TM joints & teeth
• Articular disc-Dense fibrous connective tissue devoid of nerves & blood vessels
o Able to withstand heavy forces without damage or pain
o Separates, protects, & stabilizes the condyle in the MN fossa during function
Position of discs during rest determined by:
• Interarticular pressures
• Morphology of discs themselves,
• Tonus of superior lateral pterygoid muscles (causes discs to rotate as far forward on condyles as
discal space & thickness of the disc will allow)
Does not determine positional stability of the joint – this is determined by muscles
Directional forces of muscles determines optimal orthopedically stable joint position
Major stabilizing muscles = elevators
Elevators:
1. Masseter & medial pterygoid - Direction of force is supero-anterior and positions condlyes supero-
anteriorly
2. Temporalis - Direction of force is superior-Position condyles superiorly in fossa
3. Inferior lateral pterygoid-Direction of force is superior-Position condyles anteriorly against posterior
slope of articular eminence
4. Centric Relation (CR) Position of the MN when condyles are in an orthopedically stable position
Ligamentous position b/c it is determined mainly by TMJ ligaments
Orthopedically stable joint position = condyles in most superoanterior position in articular fossa resting
against the posterior slopes of the articular with the discs properly interposed

10
• Occurs when elevator muscles are activated with NO occlusal influences musculoskeletally
stable position
There can be some anterior-posterior movement of the position if the joint is not healthy –
• In a healthy joint, the inner horizontal fibers of the TM ligament do not allow much posterior
movement
• Movement is generally < 1mm during intercuspal position
• If an unhealthy joint, the inner horizontal fibers of the TML are stretched & DO allow posterior
movement
• The posterior movement of the joint during function can cause force to be applied to the
posterior aspect of the disc, inferior retrodiscal lamina, and/or retrodiscal tissues damage to
the retrodiscal tissues can result in PAIN and/or breakdown.
o It can thus be seen that CR and the MS position are the same.
Intercuspal position (ICP) - Muscle stabilized position, NOT musculoskeletal position b/c the inferior
lateral pterygoid prevents the condyles from moving back into the most superoanterior position
Electrical stimulation - Some practitioners have suggested finding CR through use of electrical stimulation
which is supposed to relax muscles until MN goes from ICP to physiologic position
Summary of optimal functional occlusion
1. When the mouth closes, the condyles are in their most superoanterior position (i.e., MS position), resting
on the posterior slopes of the articular eminences with the discs properly interposed. In this position, even
and simultaneous contact of all posterior teeth exists. The anterior teeth also contact, but they do so more
lightly than do the posterior teeth.
2. All tooth contacts provide axial loading of occlusal forces.
3. When the mandible moves into laterotrusive positions, adequate tooth-guided contacts on the laterotrusive
(i.e., working) side are present to disocclude the mediotrusive (i.e., nonworking) side immediately. The most
desirable guidance is provided by the canines (i.e., canine guidance). Mediotrusive contacts should be
avoided in developing optimal functional occlusion.
4. When the mandible moves into a protrusive position, adequate tooth-guided contacts on the anterior teeth
are present to disocclude all posterior teeth immediately.
5. In the upright-head position and alert feeding position, posterior tooth contacts are heavier than anterior
tooth contacts. (mutually protected occlusion)
Chapter 6: Determinates of occlusal morphology. To maintain occlusal harmony posterior teeth must pass close but not contact opposing teeth during
mandibular movement. Two structures controlling mandibular movement:
(1) those that influence the movement of the posterior portion of the mandible
(2) those that influence the movement of the anterior portion of the mandible.
TMJs are posterior controlling factors (PCFs)
Anterior teeth the anterior controlling factors (ACFs).
Posterior controlling factors:
• Condyle descends articular eminence.
• Condylar guidance angle - angle condyle moves away from horizontal reference plane, fixed factor –
unalterable in healthy patient.
• TMJs provide guidance for posterior mandible, determine character of mandibular movement
posteriorly.
Anterior controlling factors:
• incisal edges of mandibular teeth occlude with lingual surfaces of maxillary anterior teeth in protrusion
or lateral movement.
11
• Steepness of lingual surfaces determines amount of vertical movement of the mandible.
• Anterior guidance is variable & can be altered by dental procedures, such as restorations, orthodontia,
and extractions and pathologic conditions (caries, habits, and tooth wear).
Understanding the controlling factors:
• Mandibular movement determined by anatomy of TMJs posteriorly & anterior teeth anteriorly
• Mandibular movement both vertical & horizontal component, relationship between components is
significant in study of mandibular movement.
• vertical component is a function of the supero-inferior movement
• horizontal component a function of the antero-posterior movement.
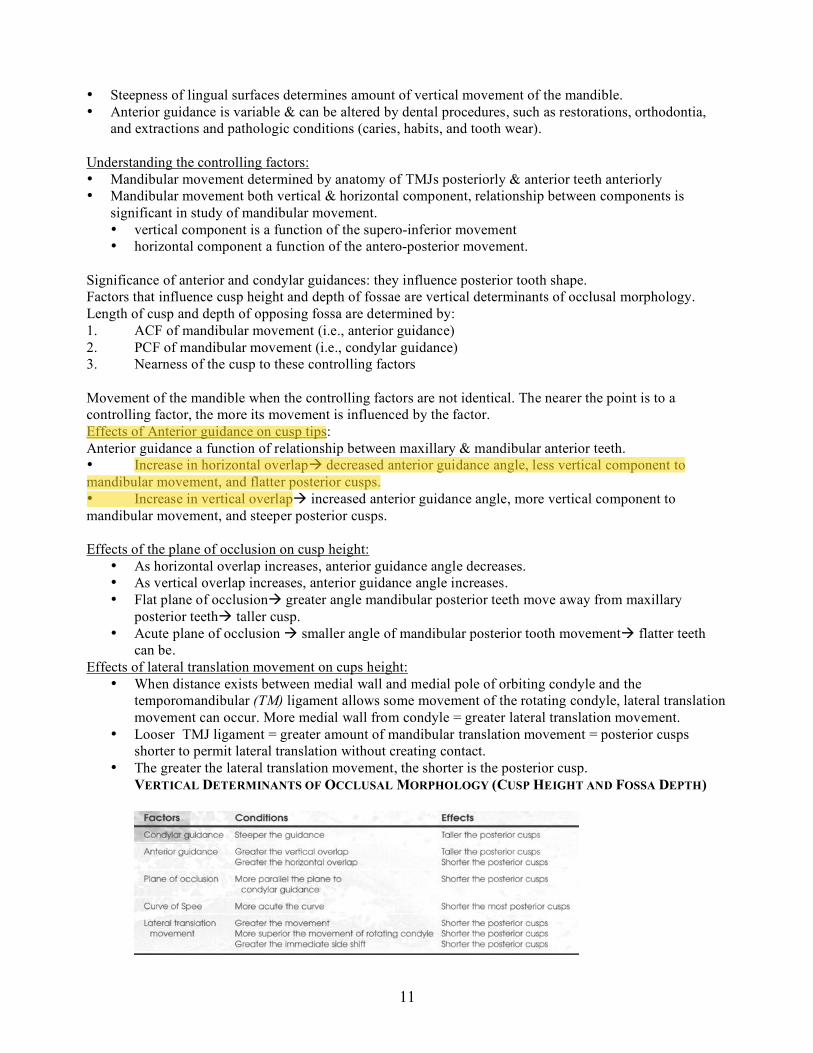
Significance of anterior and condylar guidances: they influence posterior tooth shape.
Factors that influence cusp height and depth of fossae are vertical determinants of occlusal morphology.
Length of cusp and depth of opposing fossa are determined by:
1. ACF of mandibular movement (i.e., anterior guidance)
2. PCF of mandibular movement (i.e., condylar guidance)
3. Nearness of the cusp to these controlling factors
Movement of the mandible when the controlling factors are not identical. The nearer the point is to a
controlling factor, the more its movement is influenced by the factor.
Effects of Anterior guidance on cusp tips:
Anterior guidance a function of relationship between maxillary & mandibular anterior teeth.
• Increase in horizontal overlap decreased anterior guidance angle, less vertical component to
mandibular movement, and flatter posterior cusps.
• Increase in vertical overlap increased anterior guidance angle, more vertical component to
mandibular movement, and steeper posterior cusps.
Effects of the plane of occlusion on cusp height:
• As horizontal overlap increases, anterior guidance angle decreases.
• As vertical overlap increases, anterior guidance angle increases.
• Flat plane of occlusion greater angle mandibular posterior teeth move away from maxillary
posterior teeth taller cusp.
• Acute plane of occlusion smaller angle of mandibular posterior tooth movement flatter teeth
can be.
Effects of lateral translation movement on cups height:
• When distance exists between medial wall and medial pole of orbiting condyle and the
temporomandibular (TM) ligament allows some movement of the rotating condyle, lateral translation
movement can occur. More medial wall from condyle = greater lateral translation movement.
• Looser TMJ ligament = greater amount of mandibular translation movement = posterior cusps
shorter to permit lateral translation without creating contact.
• The greater the lateral translation movement, the shorter is the posterior cusp.
VERTICAL DETERMINANTS OF OCCLUSAL MORPHOLOGY (CUSP HEIGHT AND FOSSA DEPTH)

12
HORIZONTAL DETERMINANTS OF OCCLUSAL MORPHOLOGY (RIDGE AND GROOVE DIRECTION)
Chapter 7: Causes of functional disturbances in the masticatory system 1 of 4 people report awareness of TMD, less than 10% of these people get help—most patients between 20 & 40 years old No simple cause and effect relationship between occlusion and TMD
• either the disorder has multiple causes, and no single treatment can affect all the causes • disorder not a single problem, umbrella term grouping multiple disorders.
Mandible closes condyles in most supero-anterior position with even simultaneous contacts directing forces through long axes Mandible moves eccentricallyanterior teeth contact and disocclude posterior teeth. Lack of occlusal stability may be:
• genetic, developmental, or iatrogenic causes, alterations of normal anatomic form. • lack of harmony between stable intercuspal position (ICP) of teeth and musculoskeletally stable
(MS) position of joints.
TMD Development Masticatory system structures tolerate some functional change, but if it exceeds a critical level, alteration of tissues beginsknown as the structural tolerance Numerous factors can contribute to TMD.
• predisposing factors increase risk of TMD • initiating factors cause the onset of TMD • perpetuating factors interfere with healing or enhance the progression of TMD
In some instances a single factor may serve one or all of these roles. Major factors associated with TMD:
• occlusal condition • trauma • emotional stress • deep pain input • parafunctional activities
These vary from patient to patient Occlusal features in TMD patients but rare in normal subjects:
• presence of a skeletal anterior open bite • retruded contact position (RCP) and ICP slides of greater than 2 mm • overjets of greater than 4 mm

13
• five or more missing and unreplaced posterior teeth. Not only rare in healthy individuals, also in patient populations, limited diagnostic usefulness. For functional relationship between mandible and cranium, occlusal condition affects some TMDs:.
• occlusal condition affects orthopedic stability of mandible as it loads against cranium. • acute occlusal changes can influence mandibular functionTMD symptoms
Orthopedic instability & teeth not in occlusion condyles maintained in MS positions by elevator muscles. Orthopedic instability and teeth brought into contactonly one tooth may contact Individual chooses to maintain stable joint position & occlude on one tooth or bring teeth into a more stable occlusal position compromising joint stability. Problems arise when orthopedically unstable condition is loaded by elevator muscles or extrinsic forces
• loading occurs when a joint is not in a stable relationship with disc and fossaunusual movement can occur in attempt to gain stability.
• This small movement a translatory shift between disc and condyle can lead to strain to discal ligaments and eventually elongation of ligaments and thinning of disc.
• changes can lead to a group of intracapsular disorders (chapter 18) Two factors determine whether an intracapsular disorder will develop:
• degree of orthopedic instability • amount of loading.
Orthopedic instabilities with discrepancies of 1 or 2 mm are probably not significant enough to create a problem.
• as discrepancy between MS position of condyles and maximum intercuspation of teeth becomes greater, the risk of intracapsular disorders increases.
Bruxing patients with orthopedic instability represent a higher risk for developing problems than nonbruxers with same orthopedic instability.
• forceful unilateral chewing can provide the mechanics that lead to sudden intracapsular disorders • more significant malocclusion may not always be patient who develops the disorder
Dental malocclusion: specific relationship of teeth to each other, does not necessarily reflect risk factors for development of functional disturbances in the masticatory system
Chapter 8: Signs & Symptoms of TMD Three categories of TMD signs and symptoms: Muscles, TMJ, Dentition
Dysfunction: common clinical symptom associated with muscle disorders usually seen as a decrease in the
range of mandibular movement
Acute malocclusion: is the result of the muscle disorder, not the cause
Masticatory muscle model:
If local muscle soreness does not resolve, changes in
the muscle tissues may develop, resulting in
prolonged pain input
CNS influenced pain disorders:
Myofascial pain – local areas of firm hypersensitive
bands of tissuetrigger points, trigger point has
select group of motor units contracting, no overall
shortening of the muscle results (no jaw positional

14
change), trigger points often refer pain to other areas of the head
• E.g. a TP in neck causes pain in temple…so treat TP!
• TP may be active or latent (not sensitive to palpation at that time)…look for them when
symptoms present
• TP DO NOT resolve w/o treatment
Myospasm – a CNS induced tonic muscle contraction
• Jaw positional changes can occur due to muscles in spasm
• Firm mucles upon palpation indicate spasm
As muscle pain progresses from acute to chronic, effectiveness of local treatment diminishes…catch it early
How pain gets chronic
• Protracted cause – fail to eliminate cause
• Recurrent cause – recurrent episodes ( bruxism, trauma)
• Theraputic mismanagement – misdiagnosis – incorrect treatment
Patients with fibromyalgia, systemic muscle pain, often misdiagnosed & treated for TMD.
Emotional stress most common systemic factor which can interrupt normal muscle function.
Protective co-contraction is a CNS response to injury or threat of injury. This response has also been called
protective muscle splinting
• Essentially this means that your TMJ automatically braces itself using antagonistic muscle
groups which are normally not active during their opposers function.
o Co-contraction immediately follows an event…take a good history
CNS makes pain worse when one of three things happens
• Ongoing deep pain input
• Increased emotional stress
• Changes in inhibitory system to
counteract afferent input
Discal and capsular ligaments and retrodiscal
tissues have pain receptors – normal articular
surfaces do not click (short), pop (louder than
click), crepitation (multiple rough gravel like
sounds)
When the mandible is protruded the major
directional pull of the muscle is medial, not
anterior
Functional displacement of the disc –
condyle on posterior border, disck displaced
anterior
• Click is felt as condyle moves over the posterior border into the intermediate zone of the
disk…upon opening
Reciprocal click (not always there) – heard as condyle moves from intermediate zone onto the posterior
border of the disk…upon closing
Functionally disocated disk – joint space has narrowed and disk is trapped completely anteriorly to condyle
• The dislocation without reduction has also been termed a closed lock (without reduction – person
is unable to return disk to normal position…mouth opening is lessened)
• Dislocation with reduction – disk can still slide over the condyle allowing more normal opening
and excursive movements
Macrotrauma to the joint can cause structural alterations, primarily through elongation of the discal ligaments
• Direct trauma – blow to the chin
• Indirect trauma – whiplash in car wreck, VERY LITTLE evidence that indirect affects TMJ
Microtrauma – basically bruxing with Jaw in an unstable orthopedic position. MUST have both bruxer and
orthopedically unstable jaw

15
Ortho does not cause or treat TMD
Adherence is a temporary sticking of articular surfaces over time can become an Adhesion, which is a more
permanent sticking
• Breaking of adhesion is heard as a click during function
Subluxation – hypermobility. Sounds like a thud, condyles “jump” open at the end of normal opening after a
pause
• Condyle ends in front of disk, caused by structural disk problem, not pathologic
Spontaneous dislocation – not pathologic, normal joint moved beyond normal limits, disk trapped forward
when the mouth is opened too wide
• Disk can also be trapped posteriorly
Steeper articular eminence = greater condyle-disk movement
Womens joints are more flexible than mens due to estrogen, PMS is associated with increased TMD pain
Osteoarthritis commonly affects TMJ
• End point of TMJ problems if they progress
Not all patients with joint sounds need treatment, presence of pain is important
Primary traumatic occlusion – mobility due to unusually heavy forces on teeth
Secondary “ - mobility due to normal forces on perio compromised teeth
Mandibular tori has an association with TMD, maxillary does not
Pulpitis can be caused by occlusion…only consider when more obvious factors are ruled out
Tooth wear not strongly associated with TMD symptoms
Migraines have no real connection to TMD…tension type hedaches are related to TMD
Correlation between ear symptoms and TMD is not well proven, very contoversial
Chapter 9: History & Examination for TMD 50% to 60% of the general population has a sign of some functional disturbance of the masticatory system
The purpose of a history and examination is to identify any area or structure of the masticatory system that
shows breakdown or pathologic change.
The history begins with a complete medical questionnaire identifying any major medical problems of the
patient.
A complete history obtains information in the following specific areas.
• Chief Complaint
• Pain
• Onset of Pain
• Location of Pain
• Characteristic of Pain
o Quality and Behavior of Pain
• Temporal Behavior
• Pain duration and localization
• Aggravating and alleviating factors
Clinical Exam
• Cranial nerve exam
• Eye and ear exam
• Cervical exam
• Muscle exam
o Muscle palpation, masseter, temporalis, SCM, posterior cervical muscles, functional
manipulation of the pterygoids
• Measureing mouth opening
o Maximum comfortable mouth opening vs. maximum mouth opening
o Alterations in opening pathways
o Lateral movement of pathways
• TMJ exam

16
o Palpate the joints both stationary and in movement
o Looking for joint sounds and joint restricitons
Clicks – single sound/short duration
Crepitating - multiple gravel-like sound
Dental examination
• Mobility – from bone loss or heavy occlusal forces
o Movement >0.5mm is recorded
• Widening of PDL space
o Osteosclerosis, Hypercementosis, Pupitis
• Tooth wear: most common sign of breakdown in the dentition
o Functional or parafunctional?
• Abfractions
o Abfractions are noncarious cervical lesions or wedge-shaped defects in a tooth
• Occlusal exam
o Occlusal contact pattern is examined in CR, ICP, protrusive, left and right laterotrusive
movements
• CR Contacts: when condyles in optimum functional relationship,
o Musculoskeletally stable, most superioranterior in the mandibular fossae and braced
against post slopes of articular eminences, discs interposed.
• ICP, MIP stability vs. joint stability , arch integraty, VDO, Eccentric Occlusal contacts
(protrusive, laterotrusive, mediotrusive)
• Imaging of TMJ
o 4 useful radiographs
panoramic, transpharyngeal, transcranial, anteroposterior (AP) or transmaxillary
• Tomography
o uses controlled movement of the head of the radiograph tube and the film to obtain a
radiograph of the desired structures that deliberately blurs out other structures
• Arthrography: Contrast medium is injected into the joint spaces to outline important soft tissue
structures because routine radiographic techniques only show bony structure (not soft tissue).
• MRI and Bone scanning
• Mounted Casts
• Remodeling of the condyle or fossa can occur from mild forces applied over a long period of
time
o destructive changes associated with osteoarthritis can occur if forces become too great
• Electromyography, Songraphy, Vibration Analysis, Thermography
Chapter 10: Diagnosis of TMD Identifying common functional disturbances of masticatory system.
Rules to differentiate primary pain from referred pain:
1. Local provocation of the site of pain does not increase the pain.
2. Local provocation at the source of pain not only increases the pain at the source but also the pain at
the site.
3. Local anesthetic blocking of the site of pain does not decrease the pain.
4. Local anesthetic blocking of the source of the pain decreases the pain at the source and at the site.
These seven keys in making a differential diagnosis are:
1. History
2. mandibular restriction
3. mandibular interference
4. acute malocclusion

17
5. loading of the joint
6. functional manipulation
7. diagnostic anesthetic blockade.
Classification System used for diagnosing TMD
I. Masticatory muscle disorders – myoalgia most common complaint with TMD
1. Protective co-contraction – CNS response to injury/threat of injury, appropriate muscle action altered
to protect from injury
2. Local muscle soreness – change in local environment, e.g. prolonged contraction, fatigue
3. Myofascial pain – regional pain caused by hyper-sensitive muscle bands called trigger points
4. Myospasm – involuntary CNS induced tonic contraction
5. Centrally mediated myalgia – chronic muscle pain from CNS felt peripherally
II. Temporomandibular joint disorders – altered condyle-disc function
1. Derangement of the condyle-disc complex – breakdown of normal rotational function of disc on the
condyle
• Disc displacements – thinning of posterior border of disc displaces anteriorly
• Disc dislocation with reduction – disc forces through discal space, no articulation w/condlyle
• Disc dislocation without reduction – forward translation of the condyle forces disc in front of
condyle
2. Structural incompatibility of the articular surfaces
• Deviation in form - – change to smooth articular surface that alters normal condylar movement
o Disc
o Condyle
o Fossa
• Adhesions - adherence = temporary sticking of joint, adhesion more permanent fibrous
attachment to articular surface, caused by prolonged joint loading.
o Disc to condyle
o Disc to fossa
• Subluxation (hypermobility) - condyle moves past articular eminence, this is variation of normal,
not pathology
• Spontaneous dislocation – ‘open lock’, both condyle and disc dislocated
3. Inflammatory disorders of the TMJ - by continous joint area pain made worse by function
• Synovitis/capsulitis – inflammation of synovial tissue & capsular ligament
a. can’t be differentiated clinically
• Retrodiscitis - inflammation of retrodiscal tissue
• Arthritides - inflammation of articular surfaces of joint caused by joint overloading
a. Osteoarthritis – one of most common affecting TMJ
b. Osteoarthrosis – bony changes are actively occurring, adaptive process
c. Polyarthritides - a group of arthritic conditions, rarely occurs in TMJ
• Inflammatory disorders of associated structures
a. Temporal tendonitis - hyperactive temporalis muscle can cause soreness at
insertion to coronoid process
b. Stylomandibular ligament inflammation - pain at angle of mandible radiating
towards TMJ and ear
III. Chronic mandibular hypomobility – long term painless restriction of mandible
1. Ankylosis – intracapsular adhesions that prevent normal movement
a. Fibrous
b. Bony
2. Muscle contracture – shortening of muscle w/o interfering ability to contract further
a. Myostatic – muscle kept from relaxing (stretching) for a long time
b. Myofibrotic – tissue adhesions in muscle
3. Coronoid impedance – fibrotic or long coronoid process prevents normal movement

18
IV. Growth disorders – growth disturbance in bone or muscles
1. Congenital and developmental bone disorders -
a. Agenesis – no growth
b. Hypoplasia – insufficient growth
c. Hyperplasia – too much growth
d. Neoplasia – destructive growth
2. Congenital and developmental muscle disorders
a. Hypotrophy – weakened muscle
b. Hypertrophy – increased size & strength of muscle
c. Neoplasia – destructive growth
If patient’s problem does not fall into one of these categories, more extensive exam procedures required.
Chapter 11: General Considerations Treating TMD
All the treatment methods being used for TMDs can be categorized one of two types: Definitive
treatment those methods that control or eliminate the causes of the disorder. Supportive therapy treatment
methods that are directed toward altering the symptoms.
Revesible Occlusal Therapy: Temporarily alters patients occlusal condition, best done with an occlusal
splint. This creates occlusal contact pattern in harmony with optimum condyle-disc-fossa relationship for the
patient—providing orthopedic stability

19
stops parafunctional habits, and decrease symptoms of TMJ
• reversible treatment since once it is removed, the preexisting condition returns
• An occlusal appliance that uses musculoskeletally stable (MS) (i.e., centric relation [CR]) position of
the condyles is a stabilization appliance.
Irreversible Occlusal therapy: therapy that alters the occlusal condition, mandibular position or both.
• Reversible therapy always indicated for initial treatment of patients with TMD
Definitive Treatment considerations for emotional stress
• Excess emotional stress can affect muscle function by increasing the resting activity
• can activate the sympathetic nervous system, which may be a source of muscle pain
• Activation of autonomic nervous system may be associated with other psychophysiologic
disorders commonly associated with TMD, e.g. Irritable bowl syndrome or PMS
Common Emotional States: high levels of anxiety common - not determined if anxiety was cause or result of
TMD. Apprehension, frustration, hostility, anger and fear other reported states. Studies do not show a clear
relationship between altered emotional state and increased parafunctional habits.
• Depression and sexual abuse lead to TMD occasionally
o Relaxation therapy: behavior modification substituting enjoyable activities
o Exercise for those patients that enjoy it to reduce stress
o Active relaxation :train patient to relax symptomatic muscles, encouraging blood flow
muscles, and metabolic wastes that stimulate nociceptors are eliminated
o Modification of Jacobson’s technique: tense and relax the muscles until relaxed state
recognized.
o Contraction of masticatory muscles to passively stretch and relax the muscles.
Progressive relaxation techniques most common method of promoting relaxation
used in dentistry.
o Biofeedback: assist patient in regulating bodily functions normally controlled
subconsciously, e.g. BP, blood flow and muscle relaxation, done by electrodes on
muscles patient attempts to lower reading when muscles are stressed through relaxation
techniques.
o Negative biofeedback used with electrodes placed on masseter, with clenching or
bruxism a loud noise is made, causes patient to discontinue habits, little long-term effect
because parafunctional habits return as soon once machine removed.
- definitive treatment considerations for trauma
• trauma can lead to TMD which can be caused by macro or microtrauma
o can’t do much definitive treatment for macrotrauma b/c the trauma is usually no longer
present., so help with supportive therapy
o microtrauma is small amounts of force that are repeated over a long period of time (ie:
clench, bruxism). You can do definitive treatment (ie: reduce or eliminate)
Supportive therapy: this is symptomatic, now a replacement for definitive treatment, 2 types of supportive
therapies: pharmacologic and physical
1. Pharmacologic therapy:
• Good way for managing symptoms of TMD
• Medication not a cure but with physical therapy and definitive treatment, it can help
• Many TMD’s have symptoms that are periodoic or cyclic, so dentists have tendency to prescribe
drugs on a take as needed (prn) basis – encourages drug abuse
• When drugs are used in TMD, prescribe at regular intervals for a specific period.
• Analgesics: great for deep pain input
o Non-opiates good for mild to moderate pain. (ie Tylenol)
o Opiods: act on specific receptor sites in CNS and PNS and have depression qualities –
consider for short term use for moderate to severe acute pain
• Nonsteroidal anti-inflammatory drugs(NSAID’s): mild to moderate inflammatory conditions and
acute postoperative pain
o Ibuprofen great for reducing musculoskeletal pains

20
o Most NSAID’s reduce inflammation but diminish gastric secretions that protect stomach
wall pain reduction with stomach irritation & ulcers
• Anti-inflammatory agents: Helpful with inflammatory joint disorders and chronic centrally
mediated myalgia, need 3 weeks to achieve proper levels in blood
o Corticosteroids: potent anti-inflammatories but undesirable side effects.
o Oral corticosteroids: significant dose early in treatment and gradual reduction in dosing
until medication is stopped
o Can inject hydrocortisone into joint for pain relief and restricted movements
• Antidepressants: Effect related to ability to increase availability of the amines, serotonin, and
norepinephrine in CNS
o Effect related to ability to increase availability of the amines, serotonin, and
norepinephrine in CNS
o Tricyclic antidepressants good with doses as low as 10mg in treating muscle contraction
headaches and musculoskeletal pain
• Local Anesthetics: can differentiate true source of pain from a site of pain
o When source of pain is present in muscle or joint, injection of LA into source will
eliminate pain, which confirms the diagnosis
o Most common is 2% lidocaine and 3% mepivacaine
2. Physical therapy: Used with definitive treatment
Physical therapy modalities:
• Thermotherapy: use of heat to increase circulation to area
o Creates vasodilation in compromised tissues to reduce symptoms
• Coolant therapy: use of cold
o It relaxes muscles that are in spasm
o Ice to affected area and moved in circular motion without pressure to tissues
o When numbness starts, remove ice-not be left on tissues for longer than 5-7 mins
• Ultrasound therapy: Increase in temperature at interface of tissues to affect deeper tissues
o increases blood flow in deep tissues and separates collagen fibers to improve flexibility
of connective tissues
• Phonophoresis: Administering drugs through skin via ultrasound
• Iontophoresis: Med’s introduced into tissues w/o affecting any other organs, meds in a pad, pad
put on desired tissue area, drives med into tissue
• Electrogalvanic stimulation therapy: Use of electrical stimulation of muscle to cause contraction,
Rhythmic electrical impuse to muscle creates involuntary contractions and relaxations
• Transcutaneous electrical nerve stimulation: Continuous stimulation of cutaneous nerve fibers at
a subpainful level
• Acupuncture: Uses body’s own anti-nociceptive system to reduce levels pf pain
• Cold laser: accelerates collagen synthesis, increases vascularity of healing tissues, decrease
number of microorganisms, and decrease pain
Manual techniques:
• Soft tissue mobilization: Useful for muscle pain by superficial and deep massage
o Gentle message of tissues overlying painful area can reduce pain perception
o Deep massage better than gentle for reestablishing normal muscle function
• Joint mobilization: decreases inter-articular pressure and increases range of joint movement
• Muscle conditioning: Pts with TMD usually decrease use of jaw b/c of pain, if prolonged, can
cause muscles to shorten and atrophy
• Passive muscle stretching: counteracts shortened muscle length that contributes to decreased
blood flow
o Patient should open mouth slowly and until pain is felt
• Assisted muscle stretching: After muscle has been stretched, warmed with hand and procedure
repeated 2-3 times
• Resistance exercises: Use concept of reflex relaxation to give increase in mandibular opening.
21
o promotes relaxation in elevator muscles, allows for increased mandibular opening
• Postural training: Cervical disorders are closely related to TMD symptoms
Chapter 12: Treatment of Masticatory Muscle Disorders
Myalgia is prominent complaint of patients with masticatory muscle (MM) disorders. Chronic masticatory
muscle disorders become more complicated, and treatment is generally oriented differently than for acute
problems.
Any restriction of mandibular movement is due to extracapsular muscular pain.
Masticatory Muscle Disorders
1. Protective Co-Contraction (common in dental offices)
• initial response of muscle to altered sensory input/injury - has been called protective muscle splinting
or co-activation - not a pathologic condition; a normal physiologic response of musculoskeletal
system
• pain felt in masticatory system can produce protective co-contraction
• clinically:
o increased activity of jaw-opening muscles during closure
o increase in closing muscle activity during mouth opening
Clinical Characteristics
• Structural dysfunction: Decreased range of movement, patient can normal range when
requested to do s
• Minimal pain at rest
• Increased pain to function
• Patient reports a feeling of muscle weakness
Definitive Treatment:
• Treating the muscle condition itself is not indicated.
• Treatment directed toward the reason for the co-contraction.
o E.G. co-contraction from poorly fitting restoration treatment consists of altering the
restoration to harmonize with existing occlusion
• Co-contraction is usually of short duration; if the causes are controlled, symptoms will resolve in
several days
2. Local Muscle Soreness (common in dental offices)
• noninflammatory, myogenous pain disorder.
• response of muscle to continued protective co-contraction, beginning several hours or days after
event associated with protective co-contraction.
• marked drop in range of movement, minimal pain at rest but pain with function, tender when
palpated
• with bruxing fabricate an occlusal appliance for nighttime use.
• Analgesics if pain continues, taken every 4 to 6 hours for a week
3. Myofascial pain or trigger point myalgia (common in dental offices)
• regional myogenous pain characterized by local areas of firm, hypersensitive bands of muscle known
as trigger points.
• often referred pain felt as a tension type of headache.
• caused by increased levels of emotional stress, presence of sleep disturbances, etc.
• chief complaint often pain and not the actual source (trigger point).
• Treatment is elimination of trigger points, done by stretching the muscle

22
4. Myospasm - involuntary CNS-induced tonic muscle contraction, associated with local metabolic
conditions within the muscle tissues.
• continued deep pain input or local metabolic factors associated with fatigue or overuse.
• patient reports a sudden onset of restricted jaw movement w/ muscle rigidity & acute malocclusion
common.
• pain at rest & pain is increased with function.
• Treatment - massage, vapocoolant spray, ice or LA injection into muscle, rest.
Nocturnal Bruxism - muscle hyperactivity that is difficult to control.
• Occlusion has no influence, stress influenced.
• Occlusal appliances decrease via noxious peripheral stimulus-excites negative feedback mechanism
and shuts down heavy muscle activity.
• No known treatment eliminates bruxism-always treat conservatively at first with reversible therapy.
Chapter 13: TMD and Treatments Temporomandibular joint (TMJ) disorders (Chapter 13)
Derangements of the condyle-disc complex (surgery always a last option)
• Disc displacements – definitive treatment = reestablish a normal condyle-disc relationship – anterior
positioning devices work 75% of time, joint sounds resistant to therapy
• Disc dislocations with reduction - The treatment goal of definitive therapy for disc displacements
and disc dislocations with reduction is to reduce intracapsular pain, not to recapture the disc. A
stabilization appliance should be used whenever possible because adverse long-term effects are
minimized. When this appliance is not effective, an anterior positioning appliance should be
fabricated.
• Disc dislocation without reduction – therapy should attempt to reduce or recapture the disc by
manual manipulation, which can be very successful with patients with initial locking episodes
(anterior positioning appliance makes this worse)
Structural incompatibility of the articular surfaces – caused by anything that disrupts normal functioning –
can be trauma, pathology, excessive mouth opening
• Deviation in form – change to smooth articular surface that makes alteration of normal condylar
movement, Treatment is to return structure to normal form – via surgery or having patient manage
symptoms (altered opening, chewing, etc)
Adherences and adhesions
• adherence = temporary sticking of joint
• adhesion more permanent fibrous attachment to articular surface, caused by prolonged joint loading.
• Treatment is to reduce loading (nocturnal or diurnal bruxing) – diurnal teach patient awareness,
nocturnal =stabilization appliance. Adhesions must have lesions broken by arthosccopic surgery
Subluxation – condyle moves past articular eminence,this is variation of norna;l, not pathology, only
definitve treatment is eminectomy (surgery reduces steepness of articular eminence)
Spontaneous dislocations – open lock, both condyle and disc dislocated. Treatment is to increase disc space
allowing disc to be retracted, when chronic eminectomy to correct the structures causing disorder
Inflammatory disorders of the TMJ – characterized by continous joint area pain made worse by function
• Synovitis and capsulitis – these can’t be differentiated clinically, if caused by macrotrauma treatment
is do nothing because inflammation is self-limiting, if trauma is recurrent try to protect joint from
further injury (athletic appliance)
• Retrodiscitis – inflammation of retrodiscal tissue
o extrinsic - no definitive treatment needed because cause of micotrauma generally gone,
supportive therapy usually to establish conditions for optimal healing

23
o intrinsic – intrinsic trauma often remains, treatment aims to remove source of trauma
• Arthritides – inflammation of articular surfaces of joint caused by joint overloading
o Osteoarthritis – one of most common affecting TMJ, treatment aims to decrease loading,
when muscle hyperactivity suspected make appliance to reduce loading force
o Osteoarthrosis – when bony changes are actively occurring, adaptive process so treatment
needed
o Polyarthritides – a group of arthritic conditions, rarely occurs in TMJ
• Traumatic arthritis – trauma can lead to loss of subarticular bone and change in occlusal function,
with gross trauma no definitive treatment indicated
• Infectious arthritis – bacteria into TMJ, usually from trauma (puncture wound), appropriate anti-
biotic therapy
• Rheumatoid arthritis – chronic, systemic disorder of unknown origin producing persistent
inflammation and destruction of articular surfaces, no treatment since cause is unknown
• Hyperuricemia – gout – increase in urate leading to urate crystals in joints, usually distal extremities,
treatment is to lower serum uric acid levels (modify diet)
• Psoriatic arthritis – inflammation with psoriasis, no treatment because cause unknown
• Ankylosing spondylitis – chronic inflammatory disease, mainly of spinal column, can affect TMJ
occasionally, unknown cause so no definitive treatment.
Inflammatory disorders of associated structures – tendons and ligaments become painful
• Temporal tendonitis – hyperactive temporalis muscle can cause soreness at insertion to coronoid
process. Treatment is rest, if clenching/bruxism then make stabilization appliance, analgesics can
also help
• Stylomandibular ligament inflammation - pain at angle of mandible radiating towards TMJ and ear,
treated with rest.
General considerations when treating acute trauma to the TMJ – initial exam must determine if trauma
caused soft or hard tissue damage – radiographs, once hard tissue identified and managed the soft tissues of
TMJ can be addressed.
Chapter 14: Tx of Chronic MN Hypomobility and Growth Disorders I. Chronic mandibular hypomobility - the inability of the pt to open the mouth to a mormal range; rarely
accompanied by painful symptoms of progressive destructive changes; If function is impaired, tx is
indicated; no impaired fx, no tx
• A. Ankylosis – abnormal immobility of a joint; cause – hemarthrosis secondary to trauma and
inflammation leads to more fibrous tissue; history – limited mouth opening w/out pain;
definitive tx may not be indicated
o 1. Capsular fibrosis – most common and can occur between the condyle and the disc
or the disc and the fossa
o 2. Bony – rare; occurs between the condyle and the fossa (disc would have to have
been lost)
• B. Muscle contracture – painless shortening of a muscle
o 1. Myostatis – muscle is kept from fully lengthening (stretching) for a prolonged time;
often secondary to another disorder
Two types of exercise to reestablish resting length of muscles:
a. Passive stretching – pt opens to full limit of movement and then
gently stretches beyond restriction
b. Resistant-opening exercises - A neurologic feedback can be used
to help achieve relaxation. This is accomplished by initiating mild
24
contraction of the antagonistic muscle groups. When the elevator
muscles will not properly relax, contraction of the depressors provided
by resistance to opening feeds neurologic input to the elevator muscles
to relax.
o 2. Myofibrotic – excessive tissue adhesions within the muscles or sheaths, so can’t
slide over themselves disallowing full lengthening; follows trauma or myositis
o C. Coronoid process impedance - During mandibular opening the coronoid process
passes anteroinferiorly between the zygomatic arch and the lateral surface of the maxilla.
If its pathway is impeded, it will not slide smoothly and the mouth will not open fully.
Causes: long coronoid process or encroachment of fibrous tissues
Tx: alteration of responsible tissues
II. Growth disorders
• A. Congenital and developmental bone disorders – trauma is contributing factor in many
cases
o 1. Agenesis – no growth
o 2. Hypoplasia – insufficient growth
o 3. Hyperplasia – too much growth
o 4. Neoplasia – uncontrolled, destructive growth
• B. Congenital and development muscle disorders – normal range of MN movement is likely
present with any of these conditions
o 1. Hypotrophy – lack of development
o 2. Hypertrophy – over development
o 3. Neoplasia – uncontrolled, destructive growth
Because most bone growth and muscle growth disorders are not associated with pain or dysfunction,
supportive therapy is not indicated. Definitive treatment for these disorders does not fall within the context
of the Okeson book.
Chapter 15: Occlusal Appliance Therapy Occlusal Appliance:
AKAs: splint, bite guard, night guard, interocclusal appliance, or orthopedic device (i.e., orthotic).
• 3 main Uses:
1. To temporarily provide a more orthopedically stable joint position.
2. To introduce an optimum occlusal condition that reorganizes the neuromuscular reflex
activity;
3. To protect the teeth and supportive structures from abnormal forces that may create
breakdown, tooth wear, or both.
Why splint therapy is favorable to management of TMD:
• Initial therapy should generally be reversible and noninvasive.
• Appliance becomes diagnostic
o It is extremely important that when it reduces symptoms, the precise cause-and-effect
relationship be identified before irreversible therapy is begun. These considerations are
necessary to ensure that more extensive treatment will produce long-term success.
• Helpful in ruling out certain causes
o When a malocclusion is suspected of contributing to a TMD, occlusal appliance therapy
can quickly and reversibly introduce a more desirable occlusal condition.
o If it does not affect the symptoms, the malocclusion is probably not a cause and certainly
the need for irreversible occlusal therapy should be questioned.
• It is useful in reducing symptoms
FABRICATION AND ADJUSTMENT OF THE APPLIANCE
• Care must be taken to construct an appliance that will be both
25
o compatible with the soft tissues and
o provide the exact alteration in function needed to eliminate the cause.
• An improperly adjusted appliance will
o diminish treatment effects
o may introduce doubt on the part of both patient and dentist in the diagnosis and future
treatment.
Types of Occlusal Appliances
• Two most frequently used:(1) the stabilization appliance (muscle relaxation appliance)-
primarily used to reduce muscle pain, generally fabricated for the maxillary arch; provides an
occlusal relationship considered optimal for the patient; When it is in place, the condyles are in
their most musculoskeletally stable (MS) position when the teeth are contacting evenly and
simultaneously; Canine disocclusion of the posterior teeth during eccentric movement is also
provided; goal is to eliminate any orthopedic instability between the occlusal position and the
joint position, thus removing this instability as a causative factor in the TMD
Indications:
used to treat muscle pain disorders.
can decrease the parafunctional activity that often accompanies periods
of stress.
TMD that relates to muscle hyperactivity (e.g., bruxism
the patient with local muscle soreness or chronic centrally mediated
myalgia
for patients experiencing retrodiscitis secondary to trauma.
• can help minimize forces to damaged tissues, thus permitting
more efficient healing.
• (2) the anterior positioning appliance (orthopedic-repositioning appliance)
o its goal is to change the position of the mandible in relationship to the cranium
• Other types of occlusal devices are:
o the anterior bite plane,
o the posterior bite plane,
o the pivoting appliance,
o the soft or resilient appliance
The anterior bite plane -is a hard acrylic appliance worn over the maxillary teeth that provides contact with
only the mandibular anterior teeth. It is primarily intended to disengage the posterior teeth and thus eliminate
their influence on the function of the masticatory system
Posterior Bite Plane =Usually fabricated for mandibular teeth. Consists of areas of hard acrylic located over
the posterior teeth and connected by a cast-metal lingual bar. Provide occlusal contact only on the posterior
teeth
Pivoting appliance- a hard acrylic device that covers one arch and provides a single posterior contact in each
quadrant. This contact is usually established as far posterior as possible. A superior force is applied under
the chin push the anterior teeth close together and pivot the condyles downward around the posterior
pivoting point. The device is inserted, and elastic bandages wrapped from the chin to the top of the head to
decrease forces on the joint.
Soft or Resilient appliance-a device fabricated of resilient material that is usually adapted to the maxillary
teeth to achieve even and simultaneous contact with the opposing teeth Protective athletic splints decrease
damage to oral structures when trauma is received and for patients who exhibit high levels of clenching.
Common treatment considerations of appliance therapy
-Research evidence indicates that occlusal appliance therapy is successful treatment in reducing symptoms in
70-90% of TMDs. However much controversy exists the exact mechanism.
Seven features must be considered before any permanent occlusal therapy is attempted:
• Alteration of the occlusal condition: all occlusal appliances temporarily alter the existing
occlusal condition. A change, especially toward a more stable and optimum condition, generally
decrease muscle activity may result in reduction of symptoms.
26
• Alteration of the condylar position: to either a more structurally compatible and functional
position effect on joint stability can decrease in symptoms
• Increase in the vertical dimension: this effect is universal, regardless of treatment goals. Increase
in vertical dimension can temporarily decrease muscle activity and symptoms
• Cognitive awareness: As cognitive awareness is increased, factors that contribute to the disorder
are decreased decrease in the symptoms
• Placebo effect: Approximately 40% of the patients suffering from certain TMDs respond
favorably to such treatment. May be from the competent and reassuring manner or favorable
doctor-patient relationship…
• Increased peripheral input to the central nervous system: Noctural muscles hyperactivity appears
to have its source in the CNS. An occlusal appliance is placed between the teeth provides a
change in peripheral input and thus decrease CNS-induced bruxism bruxism return if use of
device is stopped.
• Regression to the mean: the common fluctuation of symptoms associated with chronic pain
condition. The intensity of the pain often varies on a daily basis. Patient most commonly report
when the pain intensity is great. When therapy is provided and the symptoms return to average
level, the clinician mist question if the reduction was a result of therapeutic effect or simply a
natural regression of the patient’s symptoms to the mean.
Chapter 16: Treatment Sequencing Treatment sequencing is also an important part of managing TMD problems. Knowing when to institute
specific treatment in the overall management of a disorder can be critical. Sometimes the success or failure
of a treatment can be determined by the relative sequence in which it is introduced. Occasionally, treatment
will fail to eliminate the symptoms. When this occurs, the diagnosis must be reexamined for accuracy. Some
instances may arise in which the diagnosis is accurate but the treatment is unable to alter the causative
factors.
This chapter shows 11 flow charts for the management of TMD.
• Please note that these are appropriate for most patients but not all.
• When more than one diagnosis is established, the therapist must follow more than one sequencing
diagram.
• An accurate medical/dental history and clinical exam are a must in order to establish the proper
diagnosis.
• In many patients, the primary disorder becomes the one that most closely relates to the chief
complaint.
• Reversible and noninvasive forms are used to manage the disorder initially. If these don’t work,
more aggressive or irreversible treatment may be indicated.
o The decision to undergo surgical correction of an intra-capsular disorder must be made by
the patient and not by the therapist.
o The patient must be well informed to make the proper decision.
The patient needs to understand the success vs failure
advantages vs disadvantages
risk of and expected results.
The patient also needs to know about the possibility of post-operative pain.
See text for actual flowcharts (if you actually give a damn!).

27
Chapter 17: General Considerations in Occlusal Therapy Occlusal Therapy – 2 types
• Reversible- temporarily alters the occlusal condition, the joint position or both- when removed
original conditions return (ex. Occlusal appliance)
• Irreversible- permanently alters the occlusal condition so that the original condition can not be
recovered (ex. fixed prosthetic, orthodontic therapy and selective grinding)
• Used only when determined to be beneficial to patient – 2 general indications:
o Treatment of TMDs
o Treatment in conjunction with other necessary measures that will significantly alter the
existing occlusal condition
• Permanent improvement of the occlusal condition is likely to eliminate functional disturbances
of masticatory system, thus only indicated when significant evidence exists to support that the
occlusal condition is the cause
o Occlusal condition can become a causative factor in TMD:
By way of an acute change in the occlusal condition (alter sensory input)
By way of orthopedic instability
• Indicated in the absence of any functional disturbance of masticatory system
• The patient's dental malocclusion may not pose a significant risk factor for TMD. The
malocclusion needs to be evaluated for its relationship to the joint positions. If the intercuspal
position (ICP) is in harmony with the musculoskeletally stable (MS) position of the condyles, it
does not pose a significant risk factor for TMD
• Treatment goals- resolve symptoms of TMD permanently that has been successfully eliminated
with the reversible occlusal therapy- Achieve a stable and reproducible position in MN. The
condyles should be in the MS position and orthopedic stability has been established:
o 1. The condyles are resting in their most superoanterior position against the posterior
slopes of the articular eminences.
o 2. The articular discs are properly interposed between the condyles and the fossae. In
those cases when a disc derangement disorder has been treated, the condyle may now be
articulating on adaptive fibrotic tissue, with the disc still displaced or even dislocated.
Although this condition may not be ideal, it is adaptive and should be considered
functional in the absence of pain.
o 3. When the mandible is brought into closure in the MS position, the posterior teeth
contact evenly and simultaneously. All contacts occur between centric cusp tips and flat
surfaces, directing occlusal forces through the long axes of the teeth.
o 4. When the mandible moves eccentrically, the anterior teeth contact and disocclude
the posterior teeth.
o 5. In the upright-head position (i.e., alert-feeding position), the posterior tooth contacts
are more prominent than the anterior tooth contacts.
• There are two general considerations: (1) The simplest treatment that will accomplish the
treatment goals is generally the best, and (2) treatment should never begin until the clinician can
visualize the end results.
Rule of thirds
• Often the critical factor determining the appropriate treatment is the buccolingual arch
discrepancy of the maxillary and mandibular posterior teeth. The extent of this discrepancy
establishes which treatment will be appropriate.
• This relationship is best examined by first placing the condyles in the MS position (i.e., CR) with
a bilateral manual manipulation technique. In this position, the jaws are gently closed in a hinge
axis movement until the first tooth touches lightly. At this point the buccolingual relationships of
the maxillary and mandibular teeth are examined. If the centric cusps are located near the

28
opposing central fossae, only slight alterations in the occlusal condition will be needed to
achieve the treatment goals. The greater the distance that the centric cusps are positioned from
the opposing fossae, the more extensive will be the treatment needed to achieve the treatment
goals.
• Each inner incline of the posterior centric cusps is divided into three equal parts. If (when the
mandibular condyles are in their desired position) the centric cusp tip of one arch contacts the
opposing centric cusp inner incline in the third closest to the central fossa, selective grinding can
usually be performed without damage to the teeth
• If the opposing centric cusp tip makes contact in the middle third of the opposing inner incline,
crown and fixed prosthodontic procedures will usually be most appropriate for achieving the
treatment goals. In these cases selective grinding is likely to perforate the enamel, creating the
need for a restorative procedure.
• If the cusp tip contacts the opposing inner incline on the third closest to the cusp tip or even on
the cusp tip, the appropriate treatment is orthodontic procedures. Crown and fixed prosthodontics
in these instances will often create restorations that cannot adequately direct occlusal forces
through the long axes of the roots, thus producing a potentially unstable occlusal relationship.
• It is equally important to visualize the buccolingual relationship of the entire arch in determining
appropriate treatment. On occasion the tooth contact will not be typical of the entire arch and
therefore not be the best determinant of treatment.
• Five factors can influence the selection of treatment: (1) symptoms, (2) condition of the
dentition, (3) systemic health, (4) aesthetics, and (5) finances.
Chapter 18: Articulators in Occlusal Therapy Mounted casts allow lingual examination of the patient’s occlusion
Mounted casts good for patient education
Occlusal contacts can be examined without the influence of the neuromuscular system
Diagnostic prewax – good to see what can and can’t do, show patient what to expect
Non-adjustable articulator
• inexpensive, little time spent mounting casts
Semi-adjustable
• 3 adjustments that can lead to close duplication of condylar movements
o Condylar inclination
Angle condyle descends along articular eminence
o Lateral translational movement (bennet angle)
Angle at which orbiting condyle moves inward
o Intercondylar distance
Distance between rotational centers of the condyles
• Semi adjustable requires face-bow, CR, eccentric interocclusal records
fully adjustable articulators
• has 3 adjustments in semi-adjustable plus rotating condylar movement
• also has complete range of intercondylar distances (semi only has small med large)
• requires: exact hinge axis location, pantographic recording, CR
o pantograph duplicates mandibular movement exactly
• A lot more time and expense, saves time clinically to a point

29
Chapter 19: Selective Grinding
Selective grinding: a procedure by which the occlusal surfaces of the teeth are precisely altered to improve
the overall contact pattern. Because this procedure is irreversible and involves the removal of tooth structure,
it is of limited usefulness. Therefore proper indications must exist before it is considered.
A selective-grinding procedure can be used to (1) assist in managing certain temporomandibular disorders
(TMDs) and (2) complementary treatment associated with major occlusal changes (ie. Ortho).
Selective grinding is appropriate only when alterations of the tooth surfaces are minimal so that all
corrections can be made within the enamel structure. The outcome of selective grinding needs to be
accurately predicted because it is irreversible.
Using the rule of thirds (chapter 17) is helpful in predicting the outcome of selective grinding.
An antero-superior shift of the mandible from CR to ICP will be noted. The shorter the slide, the more likely
it is that selective grinding can be accomplished within the confines of the enamel. Normally an anterior slide
of less than 2 mm can be successfully eliminated by a selective-grinding procedure.
Generally, when the slide has a great horizontal component,
it is more difficult to eliminate within the confines of the
enamel. If it is almost parallel with the arc of closure (i.e.,
large vertical component), eliminating it is usually easier.
Positive occlusal awareness is when you’re equilibration
procedure is poor and you introduce new interferences
An acceptable method for reshaping tooth surfaces is the use
of a small green stone in a high-speed handpiece.
Equilibration can be devided into three steps:
First step: removal of all tooth contacts that interfere with centric relation
Second step: the selective removal of tooth structure that interferes with lateral excursions
Remove all non-working interferences
At this step, the practitioner should decide if cuspid guided or a type of group function is necessary
Depends on existing mobility patterns and pre-existing occlusal scheme
Third step: elimination of all posterior contacts that occur during protrusive movement
Helps to develop a balanced protrusive movement so that anterior teeth are in contact during anterior
disclusion
The deeper a cusp tip is located in a fossa, the greater is the chance to develop a lateral interference
All posterior teeth must have at least one centric relation contact and have heavier contact than the anterior
teeth
You CANNOT eliminate bruxism with equilibration
A lot of the chapter deals with procedure, and how to develop and take away contacts

30
Chapter 20: Restorative Considerations in Occlusal Therapy
All restorative procedures are, in some way, occlusal therapy – restorative therapy and occlusal therapy
inseparable.
Treatment goals: stabilize tooth and provide optimum functional conditions
• Posterior contacts – stability with opposing & adjacent teeth, harmonious occlusion when closing
o Instability: undercarvingfracture, carve contacts onto flat areas
• Anterior contacts – normal form and functionprovide guidance for mandible during eccentric
movement
• Mandibular position – no functional problems get max ICP
o With functional problem resolve problem, then do operative procedure
Closely examine occlusal conditions before operative procedure diagnostic casts or articulating paper to
mark contacts helps reestablish post-procedure
Fixed prosthodontics: same goals as for operative
• Planning/sequencing fixed prosthodontic treatment develop anterior tooth contacts first, with
acceptable guidance for eccentric mandibular movement, posterior teeth developed in harmony with
that guidance.
Anterior guidance table – capture morphology and fuction of anterior teeth guidance pre-restoration
• Characteristics of original guidance duplicated, provide identical guidance
• Ensure posterior teeth don’t start disoccluding during eccentric movement
Tripodization – stable intercuspal relationship – each centric cups with 3 equal contacts around cusp tip
stable position for cusp
Cusp tip to flat surface contact – good enough, easier for amalgam restorations, forces get directed through
long axis
Additive waxing technique
1. Centric cusps with ivory wax, 1/3 into occlusal surface
2. Marginal ridges – blue wax
3. Central fossa contact areas – blue wax
4. Centric cusp ridges – red wax
5. Mesial & distal centric cusp ridges – green wax
6. Centric cusp triangular ridges – red wax?
7. Non-centric cusp tips – ivory wax
8. Non-centric cusp ridges – red wax
9. Mesial & distal non-centric cusp ridges – green wax
10. Non-centric cusps triangular ridges – red wax