open heart surgery clinical pathway - saswh instructor semi secure area/rqhr... · open heart...
TRANSCRIPT

1PG.
RQHR 746 (04/11)
Open Heart Surgery Clinical Pathway Inclusion Criteria: Any patient having open heart surgery whereby the attending surgeon has indicated the initiation of this
pathway.
Exclusion Criteria: Complicated medical condition(s), the development of post-op complications where the components of care listed on the pathway no longer suit the needs of care for the patient.
Patient History: LVEF% (circle): <20, 30, 40, 50, 60, 70+ Unknown
HTN Dyslipidemia PVD Cerebrovascular disease Obesity COPD Family History CAD Diabetes (circle one) Type I Type II Chronic Renal Failure CHF AF/Arrhythmia Previous MI Permanent Pacemaker Rheumatic Fever Previous CABG Previous Valve Surgery Internal Cardiac Defibrillator Stent Percutaneous Coronary Intervention (PCI) Other __________________________________ Smoker: Previous Current
Pneumococcal Vaccine previously given: Yes No Unknown
Target discharge date: (5 days after surgery) ________________ LPN/RN Initial_________
Clinical Pathways use the current best evidence gained from systemic reviews, as well as input from multidisciplinary teams, to outline the optimal course of care for all patients who have a specific condition or who are undergoing a specific procedure.
How to use the Clinical Pathway:
Place the Pathway on the front of the chart.
Document on the flow sheets, vital signs sheet and fluid balance sheet as per hospital protocol.
Document variances, comments for components of care not met, and abnormal assessment findings on the Health Care Team Progress Notes/Variance Tracking Record sheet.
Key outcomes/indicators for Pathway evaluation are in bold text.
Each discipline is responsible for initiating components of care that they are responsible for.
When a patient is transferred to local hospital or community service, send required documentation and indicate on the interagencyreferral where the patient is on the Pathway.
Reason Off Pathway - The pathway may be discontinued when the patient’s condition changes to the extent that the pathway can no longer be followed. Attending physician must be notified. Reason off pathway and action taken must be documented.
Open Heart Surgery Discharge Outcomes
▪ Weight at or progressing to pre-op weight.▪ Hemodynamic stability▪ All wounds are clean and dry▪ Respirations easy at rest and O₂ saturation on room air are normal for patient ▪ Patient initiates deep breathing/coughing exercises▪ Patient's activity is returning to normal▪ Patient verbalizes confidence with medications▪ Patient/family verbalize understanding of discharge education, follow-up care & appointments▪ Community supports in place to allow patient/family to manage safely at home

2PG.
3PG.
RQHR 746 (04/11)
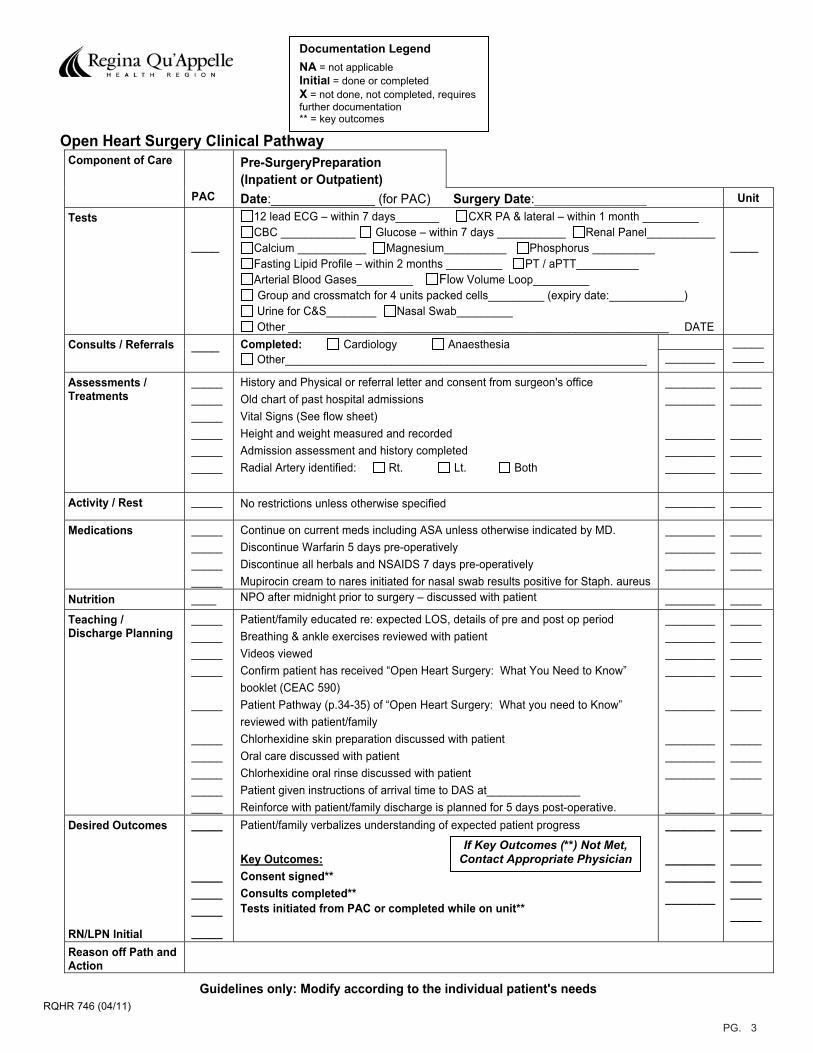
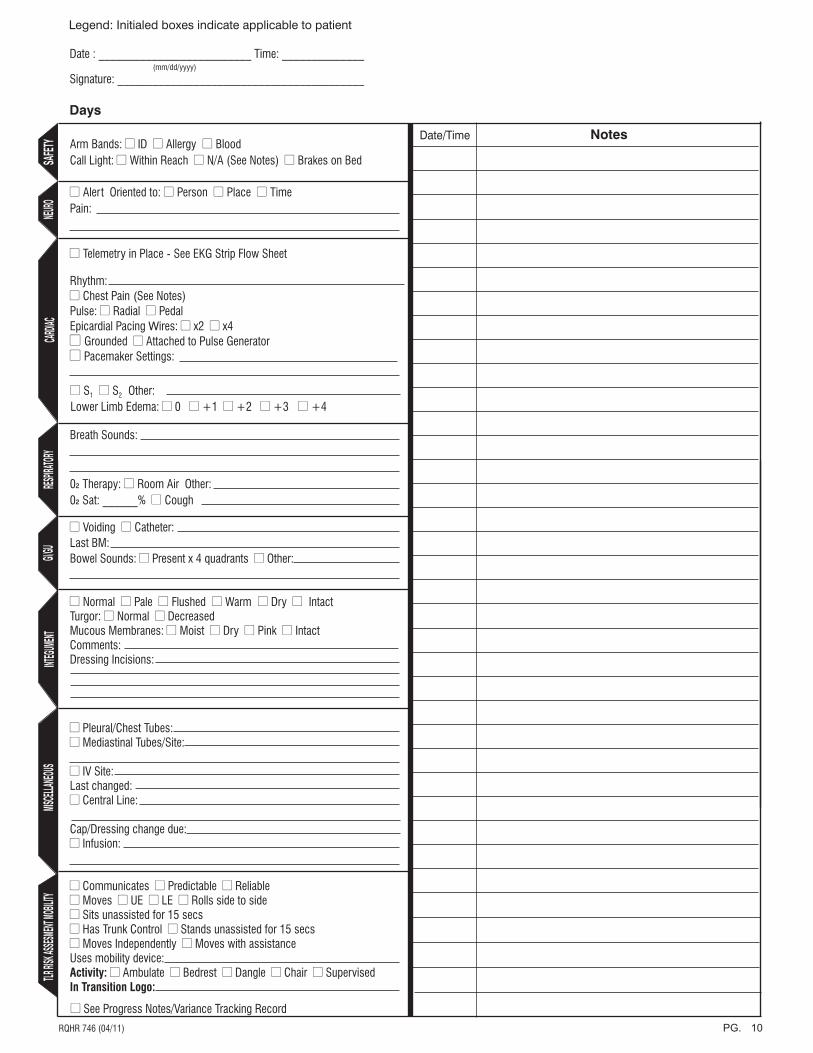
Documentation Legend
NA = not applicable Initial = done or completed X = not done, not completed, requires further documentation ** = key outcomes
Open Heart Surgery Clinical Pathway Pre-SurgeryPreparation (Inpatient or Outpatient)
Component of Care
PAC Date:_______________ (for PAC) Surgery Date:__________________ Unit Tests
____
12 lead ECG – within 7 days_______ CXR PA & lateral – within 1 month _________ CBC ____________ Glucose – within 7 days ___________ Renal Panel___________ Calcium ___________ Magnesium__________ Phosphorus __________ Fasting Lipid Profile – within 2 months _________ PT / aPTT__________ Arterial Blood Gases_________ Flow Volume Loop_________ Group and crossmatch for 4 units packed cells_________ (expiry date:____________)
Urine for C&S________ Nasal Swab_________ Other _____________________________________________________________ DATE
____
Consults / Referrals ____ Completed: Cardiology Anaesthesia Other__________________________________________________________ ________
__________
Assessments / Treatments
______________________________
History and Physical or referral letter and consent from surgeon's office Old chart of past hospital admissions Vital Signs (See flow sheet) Height and weight measured and recorded Admission assessment and history completed Radial Artery identified: Rt. Lt. Both
________________
________________________
__________
_______________
Activity / Rest _____ No restrictions unless otherwise specified ________ _____
Medications ____________________
Continue on current meds including ASA unless otherwise indicated by MD. Discontinue Warfarin 5 days pre-operatively Discontinue all herbals and NSAIDS 7 days pre-operatively Mupirocin cream to nares initiated for nasal swab results positive for Staph. aureus
________________________
_______________
Nutrition ____ NPO after midnight prior to surgery – discussed with patient ________ _____
Teaching / Discharge Planning
____________________
_____
__________ _______________
Patient/family educated re: expected LOS, details of pre and post op period Breathing & ankle exercises reviewed with patient Videos viewed Confirm patient has received “Open Heart Surgery: What You Need to Know” booklet (CEAC 590) Patient Pathway (p.34-35) of “Open Heart Surgery: What you need to Know” reviewed with patient/family Chlorhexidine skin preparation discussed with patient Oral care discussed with patient Chlorhexidine oral rinse discussed with patient Patient given instructions of arrival time to DAS at_______________ Reinforce with patient/family discharge is planned for 5 days post-operative.
________________________________
________
________________________
________
____________________
_____
_______________
_____Desired Outcomes RN/LPN Initial
_____
_______________
_____
Patient/family verbalizes understanding of expected patient progress
Key Outcomes:Consent signed** Consults completed** Tests initiated from PAC or completed while on unit**
________
________________
________
_____
_______________
_____
Reason off Path and Action
If Key Outcomes (**) Not Met, Contact Appropriate Physician
Guidelines only: Modify according to the individual patient's needs
4PG.
5PG.
RQHR 746 (04/11)
Documentation Legend
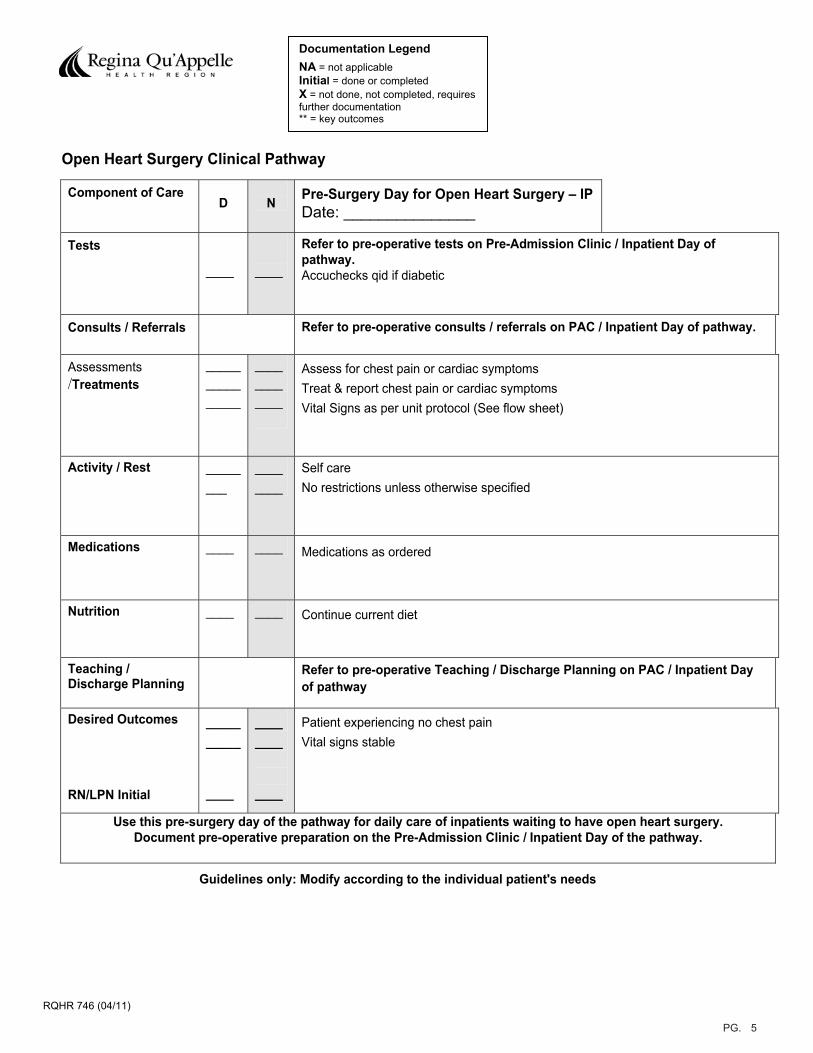
NA = not applicable Initial = done or completed X = not done, not completed, requires further documentation ** = key outcomes
Open Heart Surgery Clinical Pathway
Component of Care D N Pre-Surgery Day for Open Heart Surgery – IP
Date: _______________
Tests
____ ____
Refer to pre-operative tests on Pre-Admission Clinic / Inpatient Day of pathway.Accuchecks qid if diabetic
Consults / Referrals Refer to pre-operative consults / referrals on PAC / Inpatient Day of pathway.
Assessments /Treatments
_______________
____________
Assess for chest pain or cardiac symptoms Treat & report chest pain or cardiac symptoms Vital Signs as per unit protocol (See flow sheet)
Activity / Rest ________
________
Self care No restrictions unless otherwise specified
Medications ____ ____ Medications as ordered
Nutrition ____ ____ Continue current diet
Teaching / Discharge Planning
Refer to pre-operative Teaching / Discharge Planning on PAC / Inpatient Day f pathway o
Desired Outcomes RN/LPN Initial
__________
____
________
____
Patient experiencing no chest pain Vital signs stable
Use this pre-surgery day of the pathway for daily care of inpatients waiting to have open heart surgery. Document pre-operative preparation on the Pre-Admission Clinic / Inpatient Day of the pathway.
Guidelines only: Modify according to the individual patient's needs
6PG.
7PG.
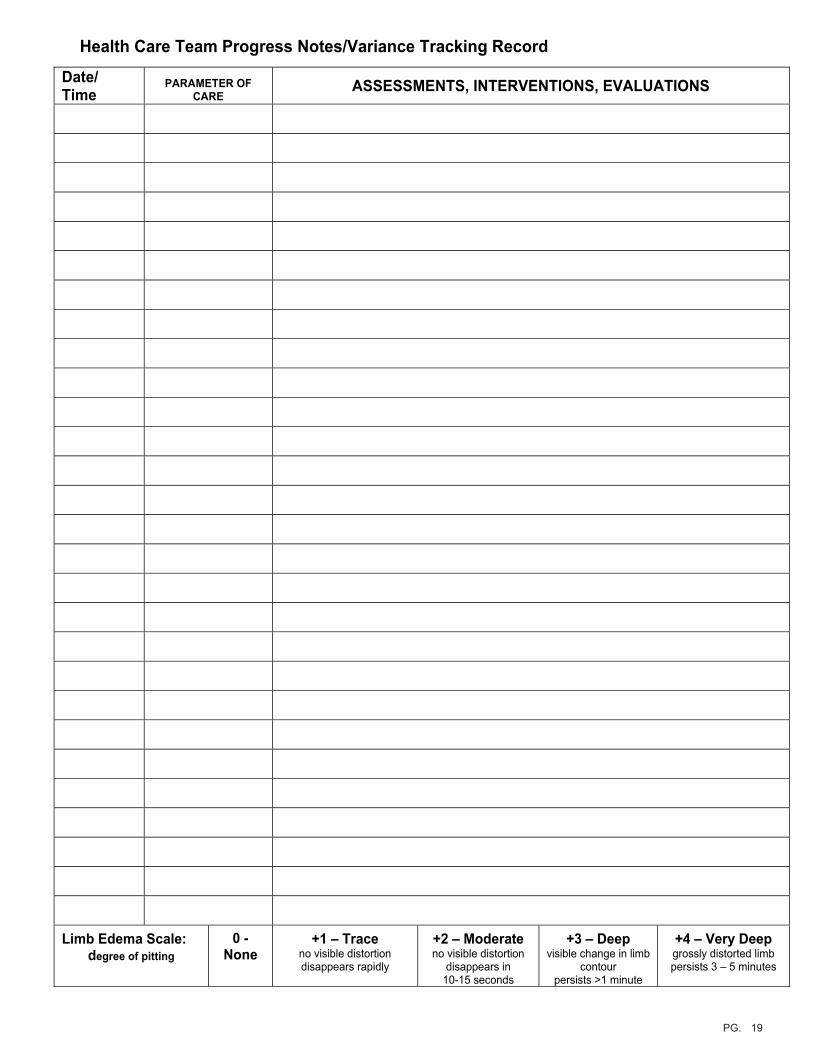
Health Care Team Progress Notes/Variance Tracking Record
Date/ Time
PARAMETER OF CARE
ASSESSMENTS, INTERVENTIONS, EVALUATIONS
Limb Edema Scale: degree of pitting
0 - None
+1 – Trace no visible distortion disappears rapidly
+2 – Moderate no visible distortion
disappears in 10-15 seconds
+3 – Deep visible change in limb
contour persists >1 minute
+4 – Very Deep grossly distorted limb persists 3 – 5 minutes
8PG.
Health Care Team Progress Notes/Variance Tracking Record
Date/ Time
PARAMETER OF CARE
ASSESSMENTS, INTERVENTIONS, EVALUATIONS
Limb Edema Scale: degree of pitting
0 - None
+1 – Trace no visible distortion disappears rapidly
+2 – Moderate no visible distortion
disappears in 10-15 seconds
+3 – Deep visible change in limb
contour persists >1 minute
+4 – Very Deep grossly distorted limb persists 3 – 5 minutes

9PG.
RQHR 746 (04/11)
Documentation Legend
NA = not applicable Initial = done or completed X = not done, not completed, requires further documentation ** = key outcomes
Open Heart Surgery Clinical Pathway Presurgery / Intraoperative Day of Surgery
Component of Care DAS /
Unit OR
Date:__________________ DAS Arrival Time:___________ Tests _____
__________
Pre-operative checklist complete Operating Room: Verify presence of angiogram CD Verify blood group and cross match present in OR
Assessments / Treatments
_____
______________________________ ____
_____
_____
_______________
Inform attending surgeon if patient has elevated temperature > 38º or new neurological symptoms preoperative. Vital Signs (See flow sheet) Clip hair the morning of surgery as per hair removal protocol (time:_______________) Pre-op chlorhexidine skin preparation completed a.m. of surgery, post hair clipping Chlorhexidine 0.12% oral rinse completed a.m. of surgery Start IV as ordered O₂ @ 3 L/min. per nasal prongs 2 hours pre-op
Operating Room: OR time < 5 hours Yes No Pump time < 100 minutes Yes No Body temperature on transfer to ICU________ Procedure: On pump CABG Off pump CABG Aneurysm Repair ASD Bentall Procedure Other_____________________ Assist Device (LV) Pacing Wires X _____ Donor Graft: Radial Artery L R Mammary Artery Saphenous Vein Valve Replaced: Aortic Mitral Tricuspid Valve Implant: Tissue Mechanical Valve repair only
Activity / Rest _____ Restricted after pre-operative medications given
Medications _______________
_____
_____
__________
_____
_____
Pre-op medications given with sips water only Verify warfarin discontinued for previous 5 days. Inform surgeon if not discontinued. Verify herbal products & NSAIDS discontinued for previous 7 days. Inform surgeon if not discontinued Verify Mupirocin ointment started for staph aureus positive nare swabs at least 24 hours prior to surgery. Inform surgeon if not. Pre-op antibiotics as ordered: Cefazolin 2g labeled with patient’s name and sent with
patient to OR holding Vancomycin 1g started on call to OR ( to be infused over 1
hour)
Nutrition / Elimination
_____
NPO since midnight before surgery
Teaching / Discharge Planning
_____ _____ Reinforce pre-op teaching
Desired Outcomes RN/LPN Initial
__________
__________
_____
__________
_____
Patient verbalizes understanding of pathway Patient transferred to Operating Room / Holding Area via stretcher @ ___________(time) Key Outcomes: Patient and family pre-op education complete** Patient's preparation complete for surgery**
Operating Room: Pre-op teaching reinforced Patient progresses through surgery and transferred to SICU**
Reason off Path and Action
If Key Outcomes (**) Not Met, Contact Appropriate Physician.
10PG.
11PG.
RQHR 746 (04/11)
Documentation Legend
NA = not applicable Initial = done or completed X = not done, not completed, requires further documentation ** = key outcomes
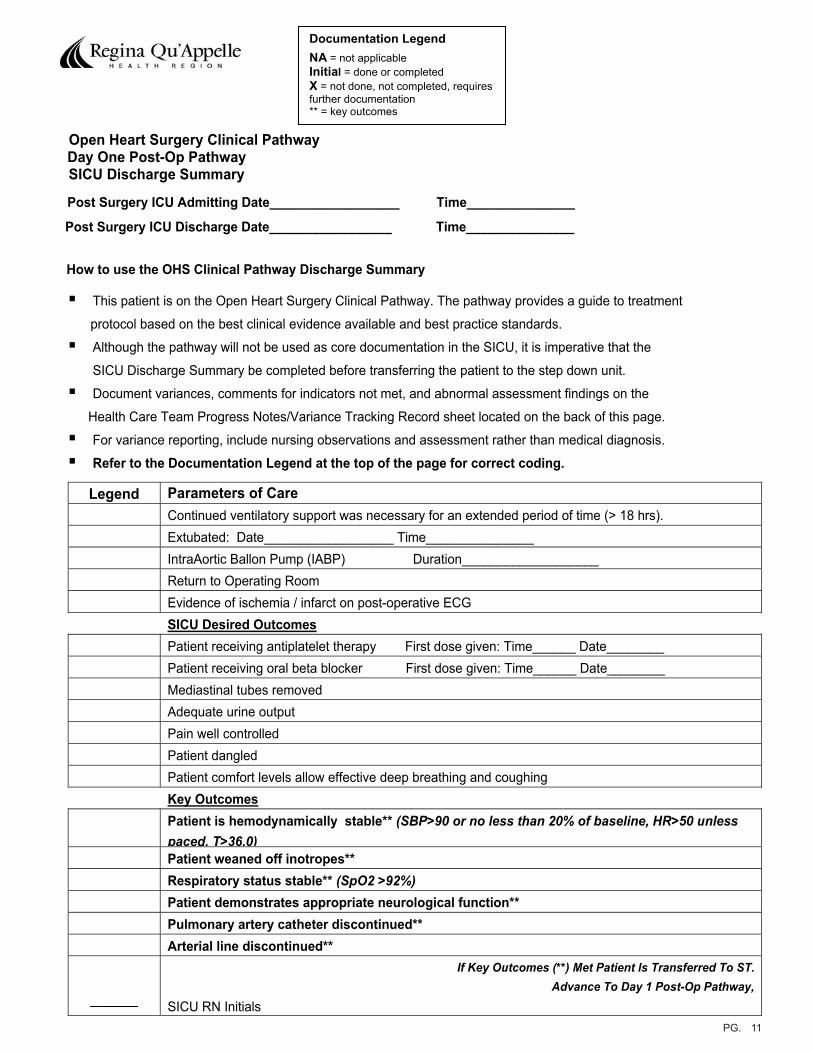
Open Heart Surgery Clinical Pathway Day One Post-Op Pathway
SICU Discharge Summary
Post Surgery ICU Admitting Date__________________ Time_______________
Post Surgery ICU Discharge Date_________________ Time_______________
How to use the OHS Clinical Pathway Discharge Summary
This patient is on the Open Heart Surgery Clinical Pathway. The pathway provides a guide to treatment
protocol based on the best clinical evidence available and best practice standards.
Although the pathway will not be used as core documentation in the SICU, it is imperative that the
SICU Discharge Summary be completed before transferring the patient to the step down unit.
Document variances, comments for indicators not met, and abnormal assessment findings on the
Health Care Team Progress Notes/Variance Tracking Record sheet located on the back of this page.
For variance reporting, include nursing observations and assessment rather than medical diagnosis.
Refer to the Documentation Legend at the top of the page for correct coding.
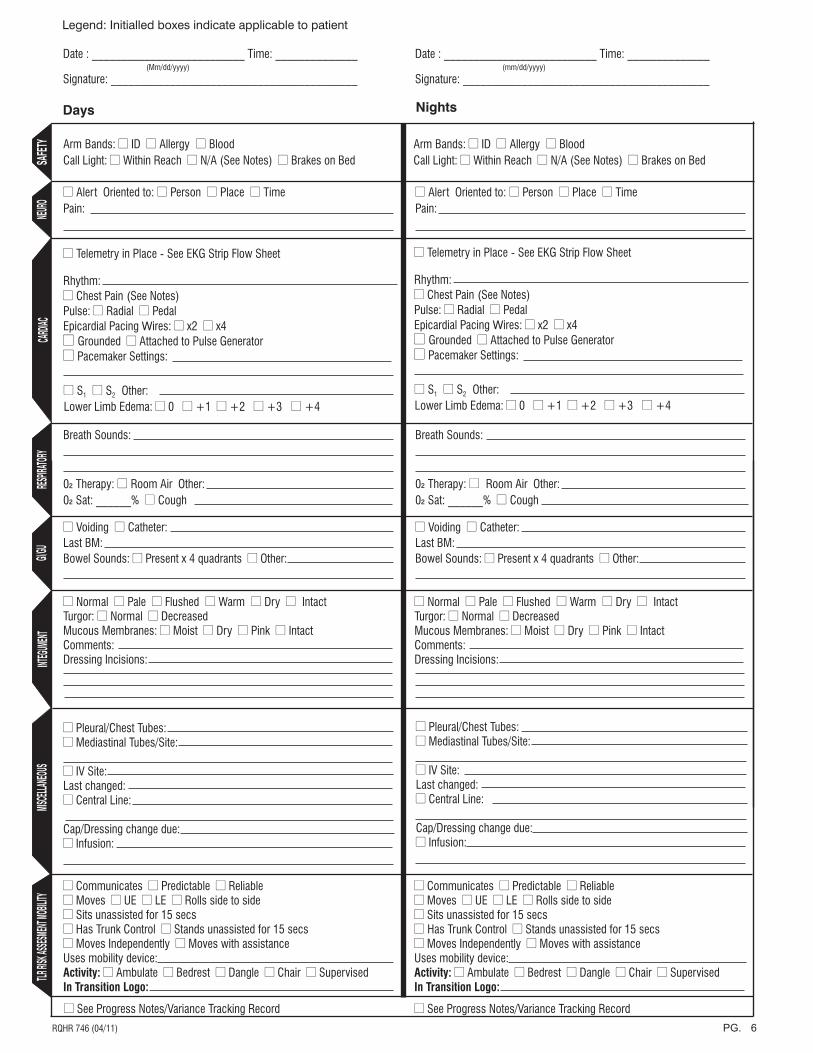
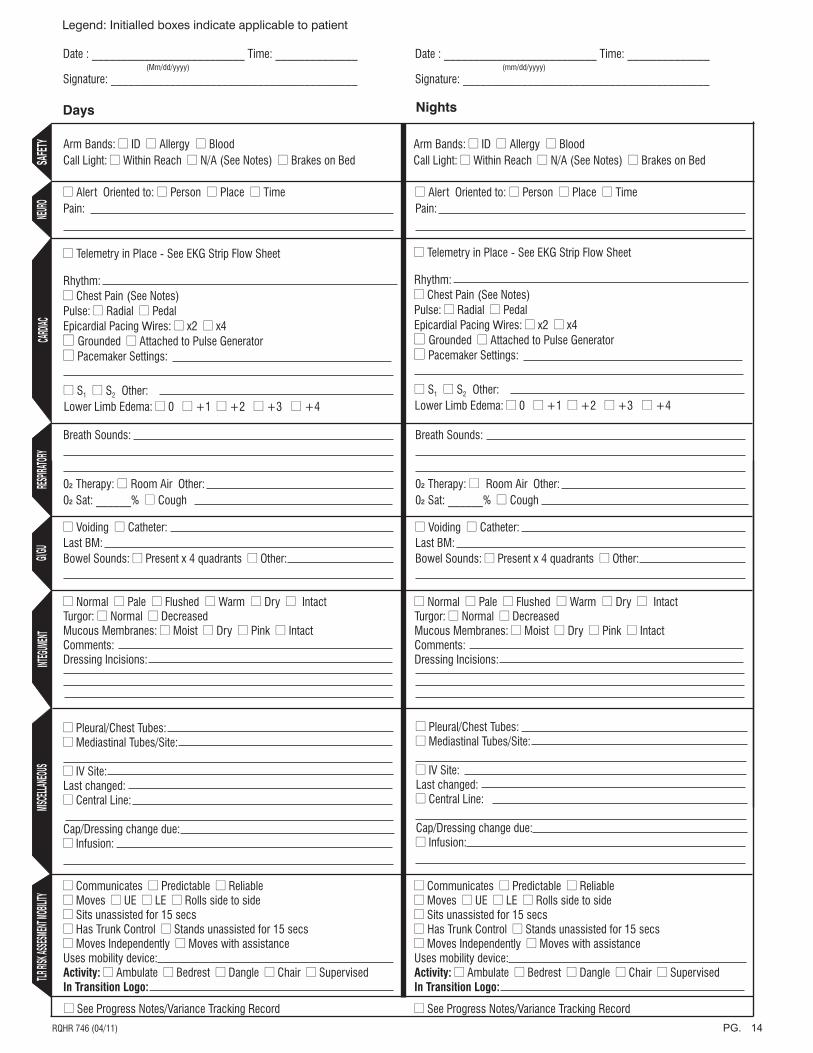
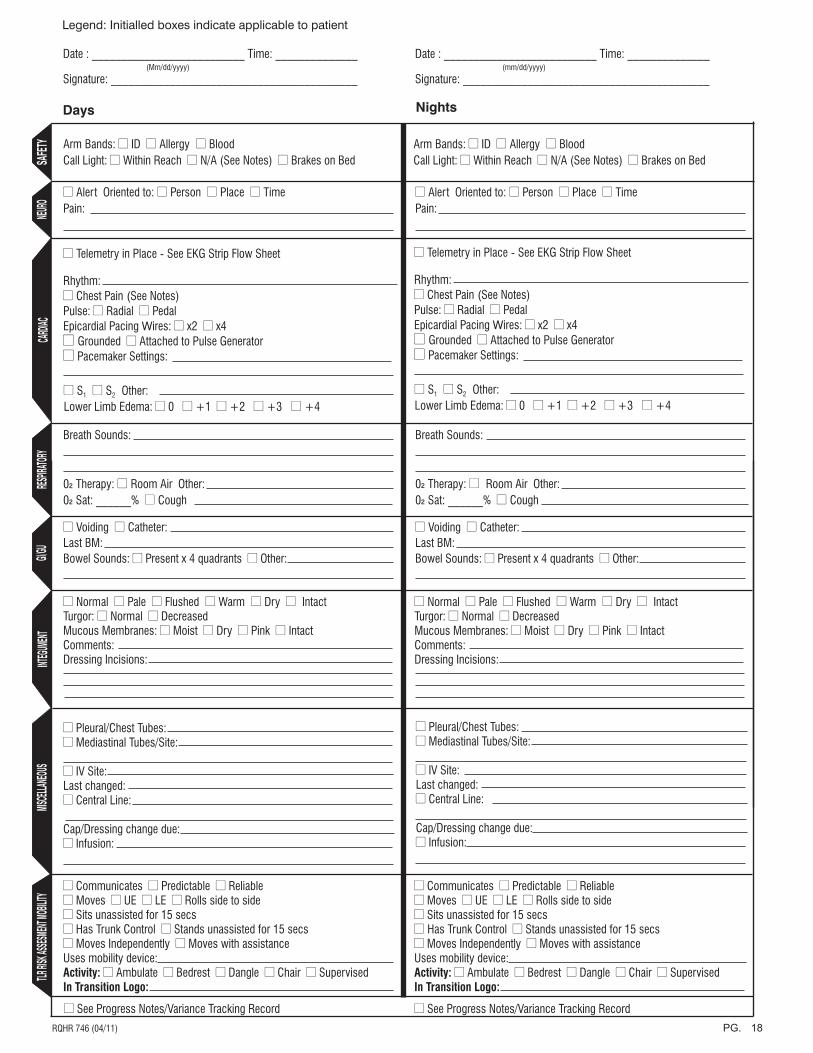
Legend Parameters of Care Continued ventilatory support was necessary for an extended period of time (> 18 hrs). Extubated: Date__________________ Time_______________ IntraAortic Ballon Pump (IABP) Duration___________________ Return to Operating Room Evidence of ischemia / infarct on post-operative ECG SICU Desired OutcomesPatient receiving antiplatelet therapy First dose given: Time______ Date________ Patient receiving oral beta blocker First dose given: Time______ Date________ Mediastinal tubes removed Adequate urine output Pain well controlled Patient dangled Patient comfort levels allow effective deep breathing and coughing Key OutcomesPatient is hemodynamically stable** (SBP>90 or no less than 20% of baseline, HR>50 unless paced, T>36.0)Patient weaned off inotropes** Respiratory status stable** (SpO2 >92%)Patient demonstrates appropriate neurological function** Pulmonary artery catheter discontinued** Arterial line discontinued**
______
If Key Outcomes (**) Met Patient Is Transferred To ST. Advance To Day 1 Post-Op Pathway,
SICU RN Initials

12PG.
13PG.
RQHR 746 (04/11)
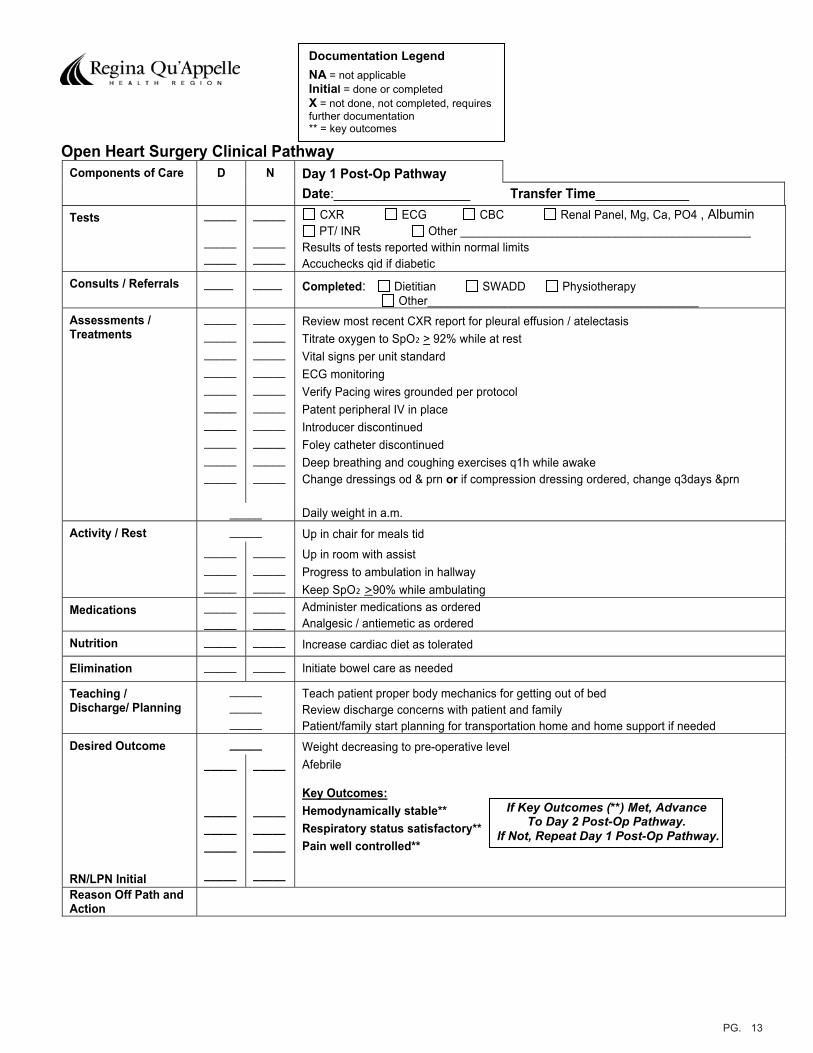
Documentation Legend
NA = not applicable Initial = done or completed X = not done, not completed, requires further documentation ** = key outcomes
Open Heart Surgery Clinical PathwayComponents of Care D N Day 1 Post-Op Pathway
Date:___________________ Transfer Time_____________ Tests _____
__________
_____
__________
CXR ECG CBC Renal Panel, Mg, Ca, PO4 , Albumin PT/ INR Other _____________________________________________
Results of tests reported within normal limits Accuchecks qid if diabetic
Consults / Referrals ____ ____ Completed: Dietitian SWADD Physiotherapy Other__________________________________________
Assessments / Treatments
__________________________________________________
__________________________________________________
Review most recent CXR report for pleural effusion / atelectasis Titrate oxygen to SpO₂ > 92% while at rest Vital signs per unit standard ECG monitoring Verify Pacing wires grounded per protocol Patent peripheral IV in place Introducer discontinued Foley catheter discontinuedDeep breathing and coughing exercises q1h while awake Change dressings od & prn or if compression dressing ordered, change q3days &prn
_____ Daily weight in a.m. Activity / Rest _____ Up in chair for meals tid
_______________
_______________
Up in room with assist Progress to ambulation in hallway Keep SpO₂ >90% while ambulating
Medications __________
__________
Administer medications as ordered Analgesic / antiemetic as ordered
Nutrition _____ _____ Increase cardiac diet as tolerated
Elimination _____ _____ Initiate bowel care as needed
Teaching / Discharge/ Planning
__________ _____
Teach patient proper body mechanics for getting out of bed Review discharge concerns with patient and family Patient/family start planning for transportation home and home support if needed
Desired Outcome _____ Weight decreasing to pre-operative level
RN/LPN Initial
_____
_______________
_____
_____
_______________
_____
Afebrile
Key Outcomes:Hemodynamically stable** Respiratory status satisfactory** Pain well controlled**
Reason Off Path and Action
If Key Outcomes (**) Met, Advance To Day 2 Post-Op Pathway.
If Not, Repeat Day 1 Post-Op Pathway.
14PG.
15PG.
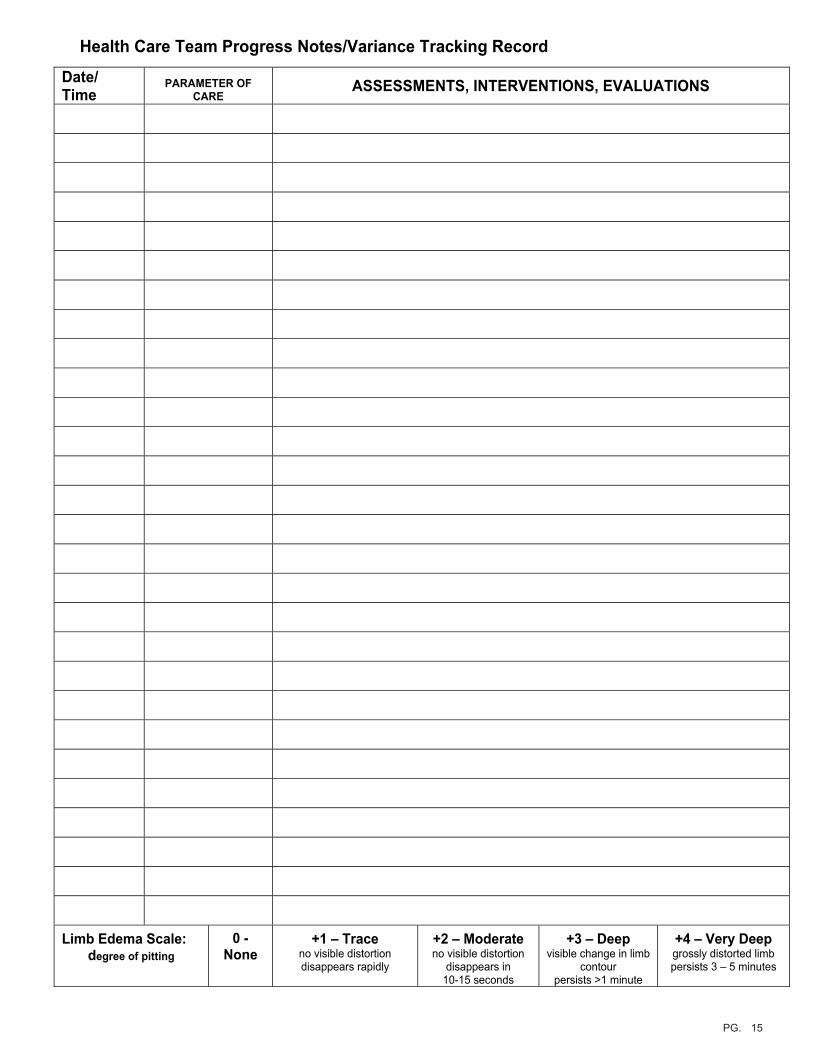
Health Care Team Progress Notes/Variance Tracking Record
Date/ Time
PARAMETER OF CARE
ASSESSMENTS, INTERVENTIONS, EVALUATIONS
Limb Edema Scale: degree of pitting
0 - None
+1 – Trace no visible distortion disappears rapidly
+2 – Moderate no visible distortion
disappears in 10-15 seconds
+3 – Deep visible change in limb
contour persists >1 minute
+4 – Very Deep grossly distorted limb persists 3 – 5 minutes

16PG.
Health Care Team Progress Notes/Variance Tracking Record
Date/ Time
PARAMETER OF CARE
ASSESSMENTS, INTERVENTIONS, EVALUATIONS
Limb Edema Scale: degree of pitting
0 - None
+1 – Trace no visible distortion disappears rapidly
+2 – Moderate no visible distortion
disappears in 10-15 seconds
+3 – Deep visible change in limb
contour persists >1 minute
+4 – Very Deep grossly distorted limb persists 3 – 5 minutes

17PG.
RQHR 746 (04/11)
Documentation Legend
NA = not applicable Initial = done or completed X = not done, not completed, requires further documentation ** = key outcomes
Open Heart Surgery Clinical Pathway Components of Care D N Day 2 Post-Op Pathway
Date:___________________ Transfer Time_____________ Tests ____
________
____
________
CXR ECG CBC Renal Panel, Mg, Ca, PO4, Albumin PT / INR Other___________________________________________
Results of tests reported within normal limits Accuchecks qid if diabetic
Consults / Referrals ____ _____ Completed: Dietitian SWADD Physiotherapy Other___________________________________________
Assessments / Treatments
_____________________________________________
_____________________________________________
Vital signs as per unit standard Titrate oxygen to SpO₂ > 92% while at rest Patent peripheral IV in place ECG monitoring Verify Pacing wires grounded Foley catheter discontinued Introducer discontinued Deep breathing and coughing exercises q1h while awake Incisions: Dressing change od & prn Open to air 48 hours post op if not draining
compression dressing – change q3days & prn (last done:______________) _____ Daily weight in a.m.
Activity / Rest _____ Up in chair for meals tid _______________
_______________
Up in room with assist Progress ambulation in hallway with assistance, as needed Keep SpO₂ >90% while ambulating
Medications __________
__________
Administer medications as ordered Administer analgesic / antiemetics as required
Nutrition __________
__________
Cardiac diet Other diet_______________________
Elimination _____ _____ Initiate bowel care as needed
Teaching / Discharge Planning
____________________
Reinforce proper body mechanics when getting out of bed Reinforce discharge date with patient and family Discuss discharge concerns with patient / family, assess need for community services. Assess need for dietitian, social work consult
Desired Outcome _____ Weight decreasing to pre-operative level
RN/LPN Initial
____________________
____________________
_____
____________________
____________________
_____
Afebrile Chest incision healing Leg / arm incisions healing Nausea and pain well controlled
Key Outcomes:Vital signs stable** Rhythm stable** Pain well controlled** Mobilizing**
Reason Off Path and Action
If Key Outcomes (**) Met, Advance To Day 3 Post-Op Pathway.
If Not, Repeat Day 2 Post-Op Pathway.
18PG.
19PG.
Health Care Team Progress Notes/Variance Tracking Record
Date/ Time
PARAMETER OF CARE
ASSESSMENTS, INTERVENTIONS, EVALUATIONS
Limb Edema Scale: degree of pitting
0 - None
+1 – Trace no visible distortion disappears rapidly
+2 – Moderate no visible distortion
disappears in 10-15 seconds
+3 – Deep visible change in limb
contour persists >1 minute
+4 – Very Deep grossly distorted limb persists 3 – 5 minutes

20PG.
Health Care Team Progress Notes/Variance Tracking Record
Date/ Time
PARAMETER OF CARE
ASSESSMENTS, INTERVENTIONS, EVALUATIONS
Limb Edema Scale: degree of pitting
0 - None
+1 – Trace no visible distortion disappears rapidly
+2 – Moderate no visible distortion
disappears in 10-15 seconds
+3 – Deep visible change in limb
contour persists >1 minute
+4 – Very Deep grossly distorted limb persists 3 – 5 minutes
21PG.
RQHR 746 (06/10)
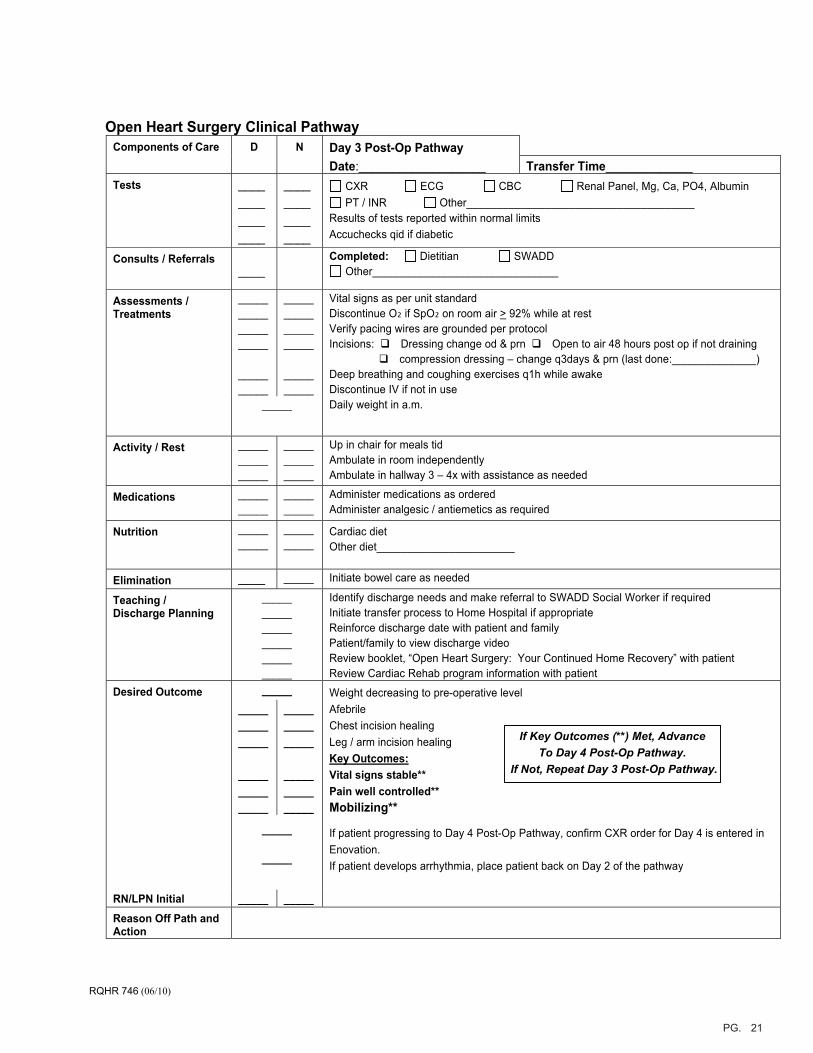
Open Heart Surgery Clinical Pathway Components of Care D N Day 3 Post-Op Pathway
Date:___________________ Transfer Time_____________ Tests ____
____________
________________
CXR ECG CBC Renal Panel, Mg, Ca, PO4, Albumin PT / INR Other______________________________________
Results of tests reported within normal limits Accuchecks qid if diabetic
Consults / Referrals ____
Completed: Dietitian SWADD Other_______________________________
Assessments / Treatments
____________________
__________
____________________
__________
Vital signs as per unit standard Discontinue O₂ if SpO₂ on room air > 92% while at rest Verify pacing wires are grounded per protocol Incisions: Dressing change od & prn Open to air 48 hours post op if not draining
compression dressing – change q3days & prn (last done:______________) Deep breathing and coughing exercises q1h while awake Discontinue IV if not in use
_____ Daily weight in a.m.
Activity / Rest _______________
_______________
Up in chair for meals tid Ambulate in room independently Ambulate in hallway 3 – 4x with assistance as needed
Medications __________
__________
Administer medications as ordered Administer analgesic / antiemetics as required
Nutrition __________
__________
Cardiac diet Other diet_______________________
Elimination ____ _____ Initiate bowel care as needed
Teaching / Discharge Planning
______________________________
Identify discharge needs and make referral to SWADD Social Worker if required Initiate transfer process to Home Hospital if appropriateReinforce discharge date with patient and familyPatient/family to view discharge video Review booklet, “Open Heart Surgery: Your Continued Home Recovery” with patient Review Cardiac Rehab program information with patient
Desired Outcome _____ Weight decreasing to pre-operative level _____
__________
_______________
_______________
_______________
Afebrile Chest incision healing Leg / arm incision healingKey Outcomes:Vital signs stable** Pain well controlled** Mobilizing**
_____
_____
If patient progressing to Day 4 Post-Op Pathway, confirm CXR order for Day 4 is entered in Enovation. If patient develops arrhythmia, place patient back on Day 2 of the pathway
RN/LPN Initial _____ _____Reason Off Path and Action
If Key Outcomes (**) Met, Advance To Day 4 Post-Op Pathway.
If Not, Repeat Day 3 Post-Op Pathway.
22PG.

23PG.
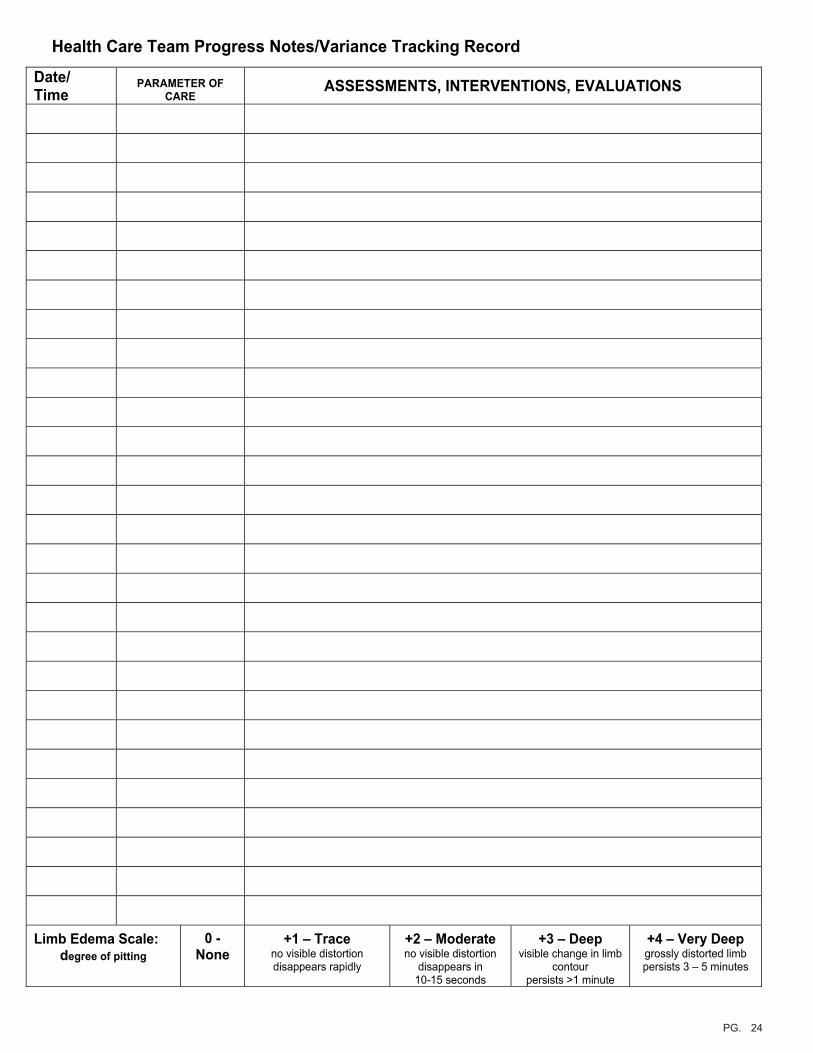
Health Care Team Progress Notes/Variance Tracking Record
Date/ Time
PARAMETER OF CARE
ASSESSMENTS, INTERVENTIONS, EVALUATIONS
Limb Edema Scale: degree of pitting
0 - None
+1 – Trace no visible distortion disappears rapidly
+2 – Moderate no visible distortion
disappears in 10-15 seconds
+3 – Deep visible change in limb
contour persists >1 minute
+4 – Very Deep grossly distorted limb persists 3 – 5 minutes
24PG.
Health Care Team Progress Notes/Variance Tracking Record
Date/ Time
PARAMETER OF CARE
ASSESSMENTS, INTERVENTIONS, EVALUATIONS
Limb Edema Scale: degree of pitting
0 - None
+1 – Trace no visible distortion disappears rapidly
+2 – Moderate no visible distortion
disappears in 10-15 seconds
+3 – Deep visible change in limb
contour persists >1 minute
+4 – Very Deep grossly distorted limb persists 3 – 5 minutes
25PG.
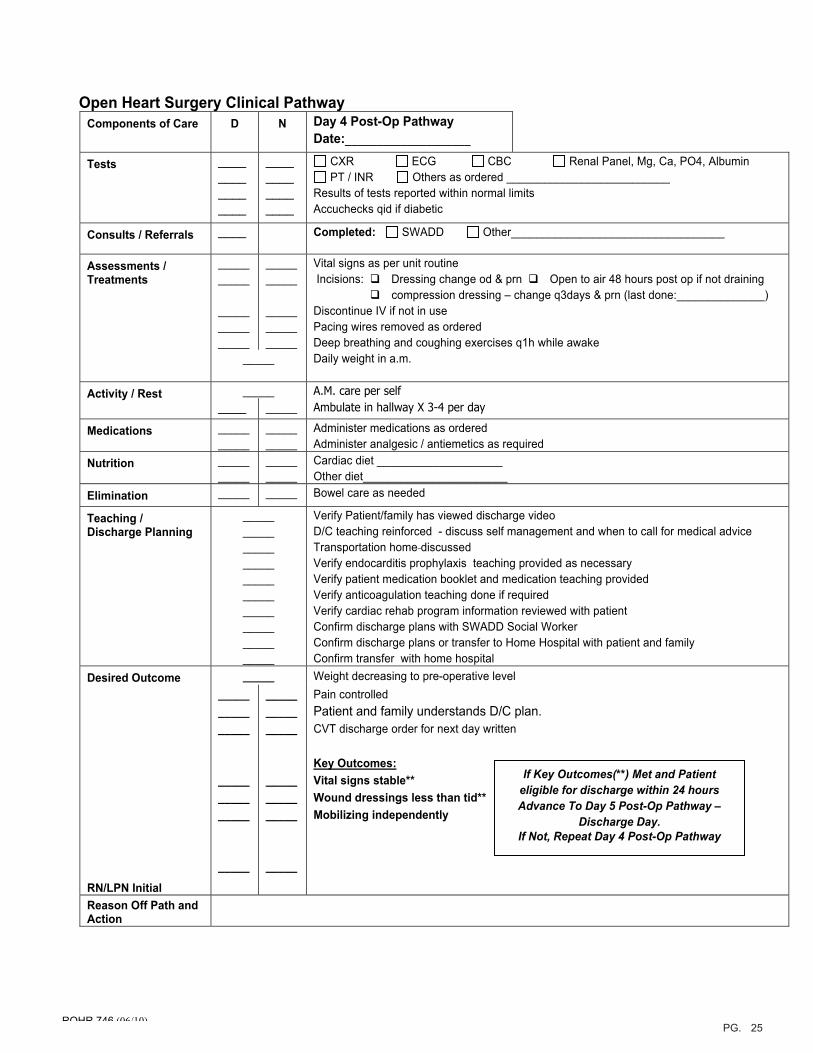
Open Heart Surgery Clinical Pathway Components of Care D N Day 4 Post-Op Pathway
Date:____________________
Tests ____________ ____
____________ ____
CXR ECG CBC Renal Panel, Mg, Ca, PO4, Albumin PT / INR Others as ordered __________________________
Results of tests reported within normal limits Accuchecks qid if diabetic
Consults / Referrals ____ Completed: SWADD Other__________________________________
Assessments / Treatments
__________
_______________
__________
_______________
Vital signs as per unit routine Incisions: Dressing change od & prn Open to air 48 hours post op if not draining compression dressing – change q3days & prn (last done:______________) Discontinue IV if not in use Pacing wires removed as ordered Deep breathing and coughing exercises q1h while awake
_____ Daily weight in a.m.
_____ A.M. care per self Activity / Rest ____ _____ Ambulate in hallway X 3-4 per day
Medications __________
__________
Administer medications as ordered Administer analgesic / antiemetics as required
Nutrition __________
__________
Cardiac diet ____________________ Other diet_______________________
Elimination _____ _____ Bowel care as needed
Teaching / Discharge Planning
__________________________________________________
Verify Patient/family has viewed discharge video D/C teaching reinforced - discuss self management and when to call for medical advice Transportation home discussed Verify endocarditis prophylaxis teaching provided as necessary Verify patient medication booklet and medication teaching provided Verify anticoagulation teaching done if required Verify cardiac rehab program information reviewed with patient Confirm discharge plans with SWADD Social Worker Confirm discharge plans or transfer to Home Hospital with patient and family Confirm transfer with home hospital
Desired Outcome _____ Weight decreasing to pre-operative level
RN/LPN Initial
_______________
_______________
_____
_______________
_______________
_____
Pain controlled Patient and family understands D/C plan. CVT discharge order for next day written
Key Outcomes:Vital signs stable** Wound dressings less than tid** Mobilizing independently
Reason Off Path and Action
If Key Outcomes(**) Met and Patient eligible for discharge within 24 hours Advance To Day 5 Post-Op Pathway –
Discharge Day. If Not, Repeat Day 4 Post-Op Pathway
RQHR 746 (06/10)
26PG.
27PG.
Health Care Team Progress Notes/Variance Tracking Record
Date/ Time
PARAMETER OF CARE
ASSESSMENTS, INTERVENTIONS, EVALUATIONS
Limb Edema Scale: degree of pitting
0 - None
+1 – Trace no visible distortion disappears rapidly
+2 – Moderate no visible distortion
disappears in 10-15 seconds
+3 – Deep visible change in limb
contour persists >1 minute
+4 – Very Deep grossly distorted limb persists 3 – 5 minutes
28PG.
Health Care Team Progress Notes/Variance Tracking Record
Date/ Time
PARAMETER OF CARE
ASSESSMENTS, INTERVENTIONS, EVALUATIONS
Limb Edema Scale: degree of pitting
0 - None
+1 – Trace no visible distortion disappears rapidly
+2 – Moderate no visible distortion
disappears in 10-15 seconds
+3 – Deep visible change in limb
contour persists >1 minute
+4 – Very Deep grossly distorted limb persists 3 – 5 minutes
29PG.
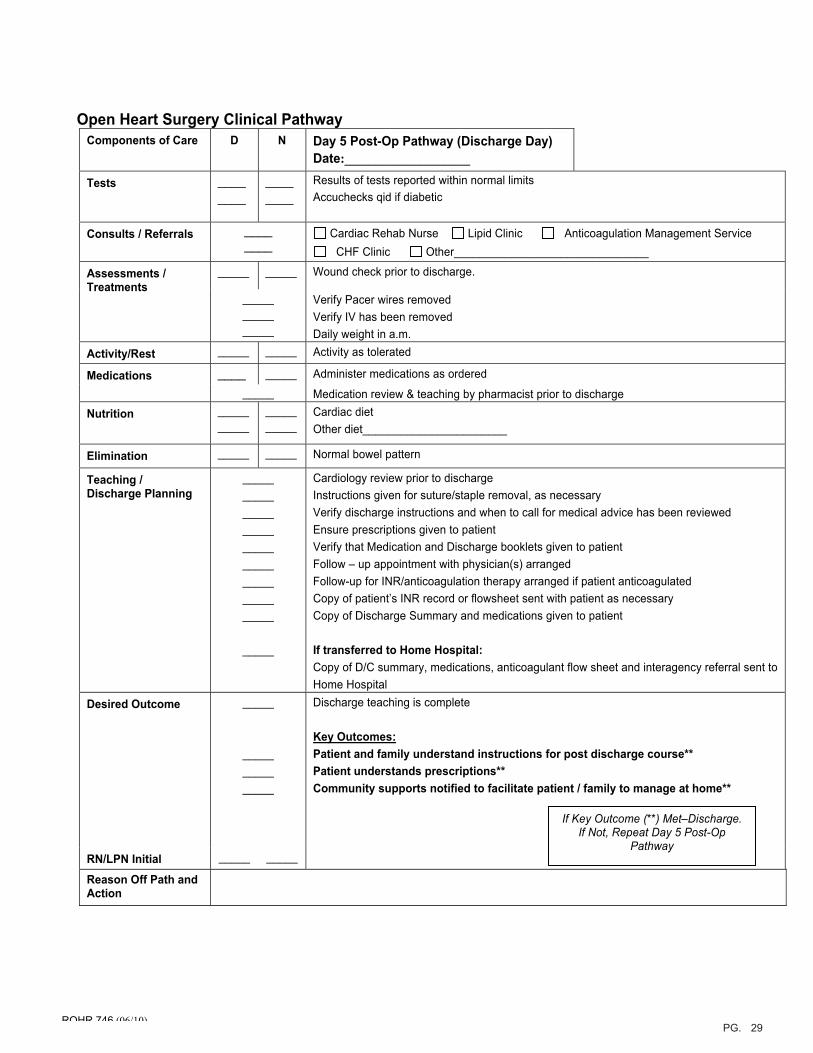
Open Heart Surgery Clinical Pathway Components of Care D N Day 5 Post-Op Pathway (Discharge Day)
Date:____________________
Tests ________
________
Results of tests reported within normal limits Accuchecks qid if diabetic
Consults / Referrals ________
Cardiac Rehab Nurse Lipid Clinic Anticoagulation Management Service CHF Clinic Other_______________________________
_____ _____ Wound check prior to discharge. Assessments / Treatments
__________ _____
Verify Pacer wires removed Verify IV has been removed Daily weight in a.m.
Activity/Rest _____ _____ Activity as tolerated
Medications ____ _____ Administer medications as ordered_____ Medication review & teaching by pharmacist prior to discharge
Nutrition __________
__________
Cardiac diet Other diet_______________________
Elimination _____ _____ Normal bowel pattern
Teaching / Discharge Planning
___________________________________ __________
_____
Cardiology review prior to discharge Instructions given for suture/staple removal, as necessaryVerify discharge instructions and when to call for medical advice has been reviewed Ensure prescriptions given to patient Verify that Medication and Discharge booklets given to patient Follow – up appointment with physician(s) arranged Follow-up for INR/anticoagulation therapy arranged if patient anticoagulated Copy of patient’s INR record or flowsheet sent with patient as necessaryCopy of Discharge Summary and medications given to patient
If transferred to Home Hospital: Copy of D/C summary, medications, anticoagulant flow sheet and interagency referral sent to Home Hospital
Desired Outcome
_____
_______________
Discharge teaching is complete
Key Outcomes:Patient and family understand instructions for post discharge course** Patient understands prescriptions** Community supports notified to facilitate patient / family to manage at home**
RN/LPN Initial _____ _____
Reason Off Path and Action
If Key Outcome (**) Met–Discharge. If Not, Repeat Day 5 Post-Op
Pathway
RQHR 746 (06/10)
30PG.
31PG.
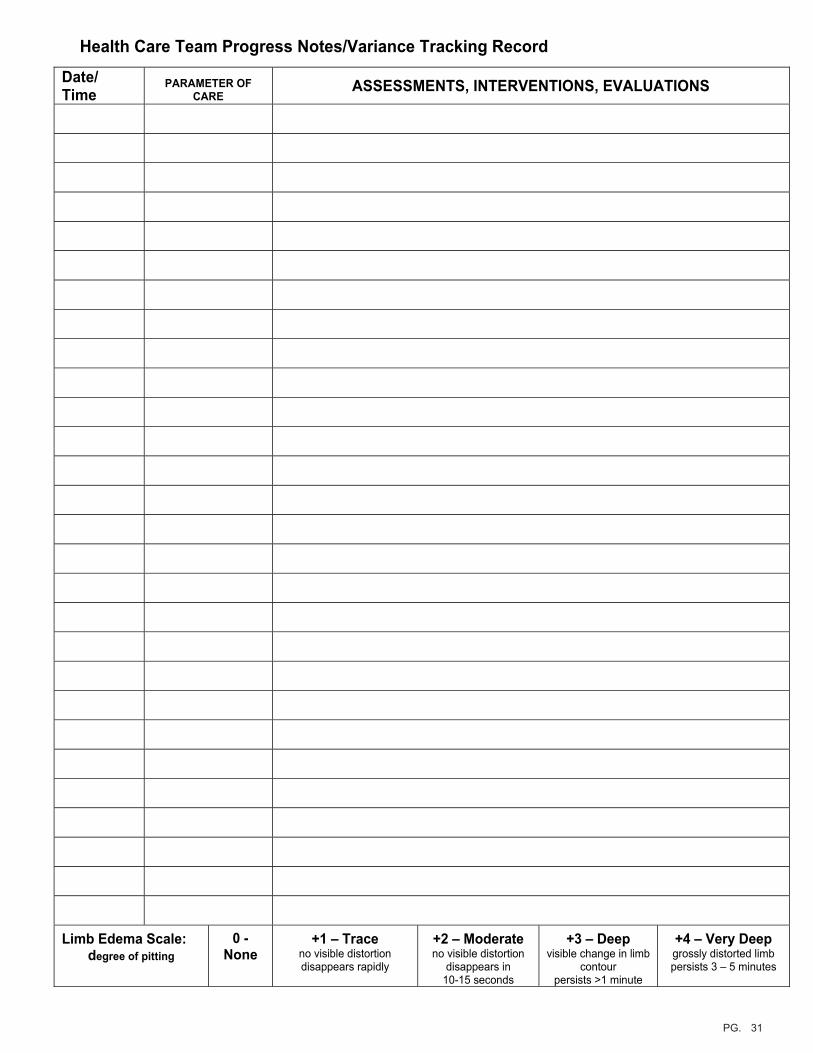
Health Care Team Progress Notes/Variance Tracking Record
Date/ Time
PARAMETER OF CARE
ASSESSMENTS, INTERVENTIONS, EVALUATIONS
Limb Edema Scale: degree of pitting
0 - None
+1 – Trace no visible distortion disappears rapidly
+2 – Moderate no visible distortion
disappears in 10-15 seconds
+3 – Deep visible change in limb
contour persists >1 minute
+4 – Very Deep grossly distorted limb persists 3 – 5 minutes
32PG.
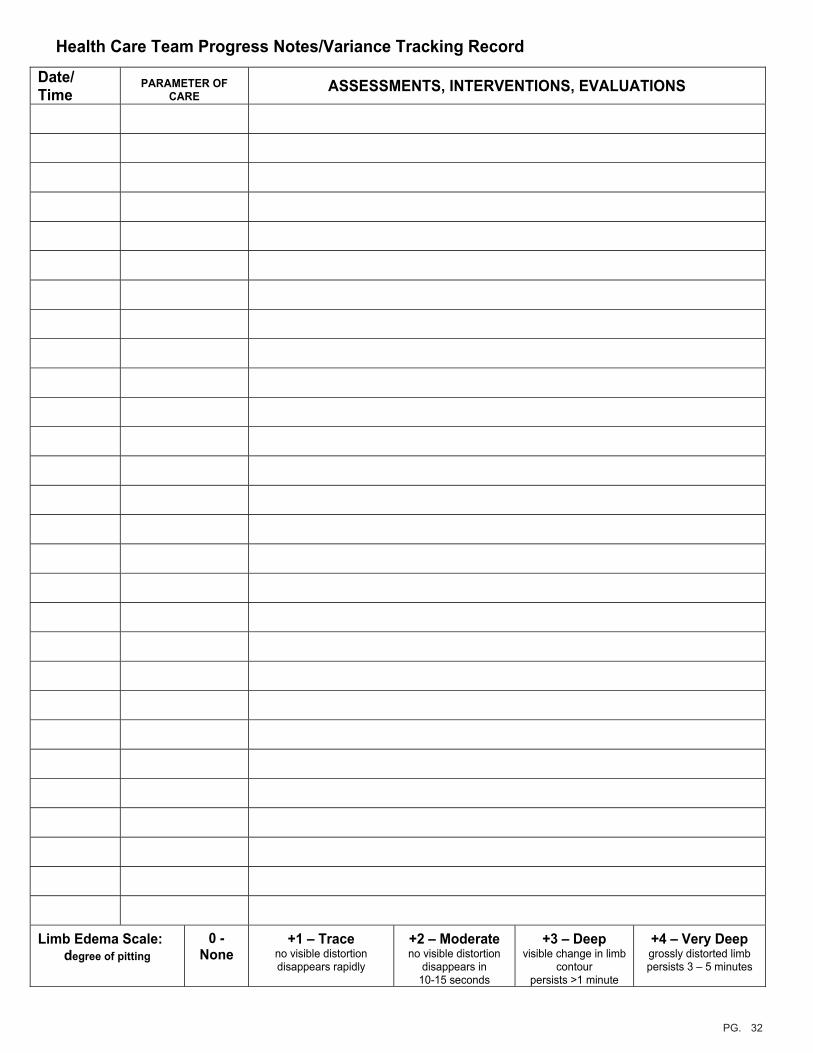
Health Care Team Progress Notes/Variance Tracking Record
Date/ Time
PARAMETER OF CARE
ASSESSMENTS, INTERVENTIONS, EVALUATIONS
Limb Edema Scale: degree of pitting
0 - None
+1 – Trace no visible distortion disappears rapidly
+2 – Moderate no visible distortion
disappears in 10-15 seconds
+3 – Deep visible change in limb
contour persists >1 minute
+4 – Very Deep grossly distorted limb persists 3 – 5 minutes