opioid utilization and health-care costs among patients with diabetic peripheral neuropathic pain...
TRANSCRIPT

papr_392 48..56
ORIGINAL ARTICLE
Opioid Utilization andHealth-Care Costs among Patients
with Diabetic PeripheralNeuropathic Pain Treated withDuloxetine vs. Other Therapies
Ning Wu, PhD*; Shih-Yin Chen, PhD*; Lindsay A. Hallett, MPH*;Luke Boulanger, MA, MBA*; Kimberly A. Fraser, BA*;
Chintan K. Patel, PharmD†; Yang Zhao, PhD†
*Health Economic Research and Quality of Life Evaluation, Abt Bio-Pharma Solutions, Inc.,Lexington, Massachusetts; †Global Health Outcomes, Eli Lilly and Company, Indianapolis,
Indiana, U.S.A.
� Abstract
Objective: This retrospective cohort study assessed subse-quent opioid utilization and health-care costs amongpatients with diabetic peripheral neuropathic pain (DPNP)who initiated duloxetine vs. other standard of care (SOC)treatments.Methods: Medical and pharmacy claims were analyzed forcommercially-insured individuals aged 18–64. Two studycohorts were constructed from DPNP patients who initiatedduloxetine or SOC medications (tricyclic antidepressants, ven-lafaxine, gabapentin, pregabalin) between March 1, 2005and December 31, 2005. Initiation was defined as a prior90-day period without access of the medication. The dispense
date of the first initiation was denoted as the index date.Patients with opioids dispensed in the prior 90 days wereexcluded. Opioid utilization including total days, number ofprescriptions filled, and morphine equivalent dosage wasassessed for overall, long-acting, and short-acting opioids.Health-care costs and opioid use in the 12-month post-indexperiod were examined via multivariate regression analyses.Results: Four hundred and ninety-nine DPNP patients (272duloxetine, 227 SOC) were identified. SOC patients hadhigher prevalence of comorbidities and pre-index health-care costs than duloxetine patients. Controlling for cross-cohort differences, duloxetine patients were significantly lesslikely to use any opioids than SOC patients. Also, duloxetinepatients had 20 fewer adjusted opioid supply days (largelydue to the use of short-acting opioids, P < 0.05) and signifi-cantly lower adjusted total costs ($8,088, P < 0.05) anddiabetes-related costs ($3,092, P < 0.05) in the 12-monthpost-index period, with most of the cost differences fromlower outpatient costs.Conclusions: DPNP patients who initiated duloxetinetherapy were less likely to have subsequent opioid use andhad lower health-care costs than SOC patients. �
Key Words: opioids, diabetic neuropathy, painful,health-care costs
Address correspondence and reprint requests to: Yang Zhao, PhD,USOR, Global Health Outcomes, Eli Lilly and Company, 1400 WestRaymond Street, Indianapolis, IN 46221, DC 4123, U.S.A. E-mail:[email protected].
Disclosure: The study was funded by Eli Lilly and Company. Yang Zhaoand Chintan Patel are employees of Eli Lilly and hold company stock.
Submitted: January 28, 2010; Accepted: March 25, 2010DOI. 10.1111/j.1533-2500.2010.00392.x
© 2010 The AuthorsPain Practice © 2010 World Institute of Pain, 1530-7085/11/$15.00Pain Practice, Volume 11, Issue 1, 2011 48–56

INTRODUCTION
Over 23 million individuals in the U.S.A. had diabetesmellitus in 2007, and as many as 50% of all diabeticpatients suffer from diabetic peripheral neuropathy(DPN),1 one of the most common complications associ-ated with diabetes. Approximately 11% of DPNpatients have DPN pain (DPNP) that often manifestsitself as a spontaneous painful, electric, burning, orshooting sensation,1,2 with 10–20% of DPNP patientsexperiencing moderate to severe pain.1,3,4 Many patientswith DPNP experience pain on a daily basis,2 which cansignificantly impair their health-related quality of lifeand reduce normal daily functioning.2,5
DPNP poses substantial economic burden to thesociety. DPNP leads to significant indirect costs due towork loss (absenteeism) and reduced productivity in thework place.6–9 Patients suffering from DPNP also incursignificant direct costs resulting from increased health-care resource utilization including physician officesvisits, hospital stays, and medication treatment.6,10
The recommended classes of pharmacologic agentsfor the management of DPNP include antidepressants(duloxetine, venlafaxine, tricyclic antidepressants[TCAs]), anticonvulsants (gabapentin, pregabalin), andopioids.11,12 The first-tier DPNP therapies consist ofduloxetine, oxycodone control release (CR), pregabalin,and TCAs,12 while gabapentin, tramadol (an opioid),and venlafaxine extended release are included on thesecond tier. Duloxetine, a serotonin-norepinephrinereuptake inhibitor, was the first agent approved by theU.S. Food and Drug Administration for the manage-ment of DPNP in late 2004, and has been shown to becost-effective compared with routine pain managementtherapies (ie, other antidepressants, analgesics, anticon-vulsants, and nonpharmacologic treatments).13 In 2005,pregabalin also received the indication for DPNP.
Opioids have been widely used in DPNP,14 as theyoften serve as adjunctive treatment for diabetic patientswith chronic pain.15 However, there is no evidence fromclinical trials to support opioid use in DPNP,15 andseveral issues potentially limit the clinical utility of thistreatment for managing DPNP. Opioid users must beclosely monitored to evaluate dosing and duration ofaction, and to prevent substance abuse. Abuse ofopioids can lead to expensive hospitalization anddetoxification programs, which may contribute to highlevels of health-care resource utilization and costs.16
Treatment termination or adjustments to dosing areimportant to ensure proper administration of opioids,
especially given the high risk of abuse and misuse,17
which may result in more frequent physician office visitsand urgent and/or emergency care.
Although new pharmacologic agents have beenapproved for the management of DPNP, few studies haveexamined how these therapies are used in the real worldpractice.14,18 No known study has examined how the useof different DPNP medications may have an impact onsubsequent opioid utilization and health-care costs.
In this study, a large U.S. administrative claims data-base was used to assess opioid utilization following theinitiation of duloxetine vs. other treatment among com-mercially insured DPNP patients and to examine thedifferences in health-care costs. We compared the preva-lence of common comorbidities associated with DPNPand prior select medication use between patients onduloxetine vs. other treatment. Controlling for differ-ences in patients demographics, comorbidities, andprior medication use, we further applied multivariateregressions to examine the differences in opioid utiliza-tion and health-care costs associated with the use ofduloxetine vs. other treatment.
METHODS
Data Source
The data used for this study were from the ThomsonMedstat’s MarketScan® Commercial Claims databasebetween 2004 and 2006 (Thomson Reuters HealthcareInc., Ann Arbor, MI, USA). Comprehensive informationon enrolment records, medical, and pharmacy claims arecaptured in the database. Medical claims record detailedinformation on both inpatient and outpatient medicalencounters including service date, place of service, Inter-national Classification of Diseases, 9th Revision, ClinicalModification (ICD-9-CM) diagnosis and procedurecodes. Pharmacy claims include National Drug Code(NDC), dispense date, quantity, and days of supply. Allclaims also contain billing information such as planpayment amount and patient out-of-pocket payment.Demographic and health insurance plan characteristicssuch as age, gender, U.S. geographic regions, and healthplan types are also available in the enrolment file.
Study Sample Selection
The study sample consisted of individuals who initiatedduloxetine or other DPNP standard of care (SOC)including TCAs, venlafaxine, gabapentin, and pregaba-lin11,12 between March 1, 2005 and December 31, 2005.Medication initiation was defined as a 90-day medica-
Opioid Utilization and Health-Care Costs among DPNP Patients • 49

tion gap for the selected agent, with the dispense date ofthe first initiation as the index date. All patients aged18–64 (as of the index date) were included if they: (1)had one or more medical service claims with diagnosisfor “diabetes with neurological manifestations” (ICD-9-CM 250.6x) or “polyneuropathy in diabetes” (ICD-9-CM 357.2x) in the 12-month pre-index period; (2)had one or more prescriptions for pain medications(eg, antidepressants, anticonvulsants, narcotics, non-narcotics, and nonsteroidal anti-inflammatory drugs[NSAIDs]) during the 12-month pre-index period; (3)had continuous enrolment during the 12 months beforeand after the index date; and (4) were opioid naïvepatients, defined as no pill coverage for any DPNP-related opioids (ie, codeine, hydrocodone, oxycodone,pentazocine, propoxyphene, tramadol, fentanyl, hydro-morphone, levorphanol, meperidine, methadone, mor-phine, buorphanol, and oxymorphine16) during the 90days prior to the index date. To ensure that duloxetine,venlafaxine, or TCAs studied here were mainly used forthe management of DPNP, patients initiated on thesemedications with any depression diagnosis (ICD-9-CM296.2x, 296.3x, 300.4, 309.1, 311) over the 12-monthpre-index period were excluded. Similarly, patients ini-tiated on gabapentin or pregabalin with prior epilepsy(ICD-9-CM 345.xx, 780.39) or neuralgia (ICD-9-CM053.12, 053.19) diagnosis during the 12-month pre-index period were also excluded.
Study Measures
Demographics, pre-index clinical characteristics, andprior health-care utilization were measured during the12-month pre-index period. Demographic informationassessed for each patient included age, gender, healthplan type, and geographic region (eg, northeast, northcentral, west, and south). Diabetes- and pain-relatedcomorbidities were assessed based on ICD-9-CM diag-nosis codes recorded in any diagnosis field in themedical claims (see Appendix). Utilization of diabetes-related medications (insulin and/or oral antidiabeticdrugs [OAD]) and pain-related medications (antidepres-sants, anticonvulsants, narcotics, non-narcotics, andNSAIDs) was examined. The number of total anddiabetes-related prescriptions filled was also reported.Proportion of patients with any inpatient hospitaliza-tion and total hospital days during the 12-month pre-index period were further assessed.
Health-care costs were estimated in both the12-month pre- and post-index periods. Health plan paidamount and patient out-of-pocket co-payment were
summed from both the medical and pharmacy claims.Diabetes-related costs were extracted based on themedical service claims coded with any diabetes diagno-sis (ICD-9-CM: 250.xx), and diabetes-related medica-tion costs were estimated based on pharmacy claims forinsulin and OADs. Costs were assessed overall and bymajor components (eg, inpatient, outpatient, and phar-macy), and were adjusted to 2007 U.S. dollars usingthe medical component of the U.S. consumer priceindex.19
Several opioid utilization measures were assessedduring the 12-month post-index period for total, short-,and long-acting opioids. Short-acting DPNP-relatedopioids included codeine, hydrocodone, oxycodone,pentazocine, propoxyphene, tramadol, fentanyl, hydro-morphone, meperidine, morphine, buorphanol, andoxymorphine.20 Long-acting DPNP-related opioids con-sisted of tramadol, fentanyl, hydromorphone, levorpha-nol, methadone, morphine, and oxycodone.20 Fivedifferent DPNP-related opioid utilization measures werereported: (1) percentage of patients with any opioiddispensed, (2) total number of opioid prescriptions dis-pensed, (3) total number of days on opioids (based onsupply days from the pharmacy claims), (4) days to firstopioid prescription, and (5) yearly cumulative morphineequivalent opioid dosage. Morphine equivalent dosageswere estimated by multiplying the quantity of each pre-scription per unit dispensed by a published morphineconversion factor per milligram of opioid.20,21
Analysis
Two study cohorts were created among selected DPNPpatients based on the index medication (duloxetine orSOC). For patients in each cohort, we examined demo-graphic characteristics, prior health-care utilization, theprevalence of comorbidities, and prior select medicationuse. Mean and standard deviation were reported forcontinuous variables, and student t-tests were used forcross-cohort differences. Percentages were reportedfor categorical variables, and between-cohort differ-ences were detected via chi-square tests. NonparametricWilcoxon tests were used for count variables.
Opioid utilization over the 12-month post-indexperiod was compared between the duloxetine and SOCcohorts. Several types of multivariate regression modelswere applied to estimate cross-cohort differences: (1)logistic regression models were used to estimate thelikelihood of any opioid use between cohorts, (2) Coxproportional hazards models were performed tocompare days before first opioid prescription, (3) linear
50 • wu et al.

regression models were applied to examine the adjustedtotal number of days on opioids and yearly cumulativemorphine equivalent dosage, and (4) Poisson regressionmodels were used to estimate the number of opioidprescriptions dispensed. Explanatory variables includedin all regression models included age, region, priordiabetes-related medication use, prior opioid use, anddiabetes- and pain-related comorbidities. For adjusteddifferences between duloxetine and SOC cohorts, oddsratios from logistic regression models, hazard ratiosfrom Cox proportional hazards models, and incidencerate ratios from Poisson regression models were furtherreported, where values less than 1 indicate a lower like-lihood of the outcome to occur among the duloxetinepatients vs. SOC patients. For example, an odds ratio of0.45 for any opioid use means that the probability ofhaving any opioid use among duloxetine patients is only0.45 times as likely as the SOC patients.
Finally, total and diabetes-related healthcare costs bytype of service (inpatient, outpatient, and pharmacy)were compared between cohorts. Since the distributionof health-care costs is skewed, the analyses were per-formed using generalized linear regression with a log-link and gamma distribution22,23 using the sameexplanatory variables as described above. Cost mea-sures (eg, inpatient costs) with a relatively large pro-portion of zero values (> 10%) were analyzed usingtwo-part models.22 First, the probability of nonzerovalues was fitted using logistic regression for the wholepopulation with age, region, prior diabetic medicationuse, diabetes- and pain-related comorbidities as theexplanatory variables. Second, the conditional meansfor nonzero values were estimated using multivariategeneralized linear regression among the subpopulationwith nonzero values using the same explanatory vari-ables. The estimated cost for each individual was calcu-lated as the probability from the logistic regressionmultiplied by the conditional mean from multivariategeneralized linear regression. Adjusted differencesbetween duloxetine and SOC cohorts were calculated asthe mean of differences among all individuals when theircohort variable was alternatively coded as “0” and“1”.22 Confidence intervals (CIs) for adjusted differ-ences were obtained by bootstrapping with 1,000 itera-tions, and the 95% CIs were estimated as the 2.5 and97.5 percentiles from the distribution of 1,000 marginaleffect estimates.24 All analyses were conducted usingSAS version 9.2 (SAS Institute, Inc., Cary, North Caro-lina), and findings of P values < 0.05 were consideredstatistically significant.
RESULTS
The study sample included 499 commercially-insuredDPNP patients: 272 duloxetine patients and 227 SOCpatients (Table 1). Baseline demographic characteristicswere similar between the two cohorts, as over 50% ofpatients in each cohort were female with a mean age ofapproximately 55 years. Most patients lived in the south-ern and north central regions, and the majority ofpatients were enrolled in a preferred provider organiza-tion. Patients in the SOC cohort had significantly moreinpatient stays (41% vs. 25%, P < 0.05) and longerhospital days (5.0 vs. 2.0, P < 0.05) than those in theduloxetine cohort. SOC patients also had significantlyhigher total health-care costs ($39 209 vs. $22,003,P < 0.05).
The most common diabetes-related comorbidity forpatients in both cohorts was cardiovascular disease, fol-lowed by cerebrovascular/peripheral vascular diseaseand retinopathy (Table 2). Compared with duloxetinepatients, those in the SOC cohort had significantlyhigher rates of cardiovascular disease (76.2% vs.62.9%, P < 0.05), cerebrovascular/peripheral vasculardisease (30.4% vs. 19.5%, P < 0.05), and infectionsrelated to diabetes (2.6% vs. 0.4%, P < 0.05). The mostcommon pain-related condition was low back pain,
Table 1. Baseline Demographic and Prior HealthcareUtilization
Duloxetine SOC
Number of patients 272 227Age: mean (SD) 54.6 (7.2) 55.1 (6.2)Female (%) 56.6 53.7Region (%)
Northeast 4.4 6.2North central 32.4 29.1South 51.1 52.4West 11.0 12.3Unknown 1.1 0.0
Health plan type (%)Comprehensive 16.2 20.3HMO 13.6 16.3PPO 52.2 47.6POS 14.3 14.1Other 2.9 0.9Missing 0.7 0.9
Any inpatient stay (%) 24.6 40.5*Total hospital days: mean (SD) 2.0 (6.5) 5.0 (12.4)*Total healthcare costs: mean
(SD)$22,003 ($38,492) $39,209 ($63,110)*
Data source: Thomson Medstat’s MarketScan commercial claims database2004–2006.Note: Student t-test for continuous variables (age, total hospital days, totalhealthcare costs); Chi-square test for categorical variables (female, region, healthplan type, any inpatient stay).* Statistically significant at P < 0.05.HMO, health maintenance organization; POS, point of service (with or withoutcapitation); PPO, preferred provider organization; SD, standard deviation; SOC,standard of care; Other includes CDHP (consumer directed health plan) and EPO(exclusive provider organization).
Opioid Utilization and Health-Care Costs among DPNP Patients • 51

which was also more prevalent among SOC patientsthan duloxetine patients (29.5% vs. 19.9%, P < 0.05).
Approximately 70% of patients used OADs andbetween 48.0 and 52.9% used insulin prior to duloxet-ine or SOC initiation (Table 3). Close to 60% ofpatients in both cohorts used antidepressant medica-tions, with selective-serotonin reuptake inhibitors(SSRIs) being the most commonly prescribed. Com-pared with SOC patients, a significantly higher propor-tion of duloxetine patients had prior use ofanticonvulsants (64.3% vs. 44.9%, P < 0.05), particu-larly gabapentin (53.7% vs. 39.2%, P < 0.05). Prior useof narcotics was significantly more common amongSOC patients than duloxetine patients (79.3% vs.54.0%, P < 0.05), primarily due to greater utilization ofoxycodone (32.2% vs. 8.8%, P < 0.05) and tramadol(30.0% vs. 7.4%, P < 0.05). On average, patients in theSOC cohort had more unique medications dispensedcompared with those in the duloxetine cohort (17.5 vs.15.9, P < 0.05).
Table 4 presents the opioid utilization over the12-month post-index period for patients in the dulox-etine and SOC cohorts. Compared with SOC patients,those who initiated duloxetine were less likely to use anyDPNP-related opioids (54.0% vs. 76.7%, P < 0.05) andwere dispensed fewer opioid prescriptions (1.9 vs. 3.6,P < 0.05). Duloxetine patients also had fewer days onopioids (26.9 vs. 51.4, P < 0.05), had their first DPNP-related opioid prescription filled 82 days later (241 vs.159, P < 0.05), and had significantly lower yearly cumu-lative morphine equivalent dosages (1,404 mg vs.
2,496 mg, P < 0.05). Similar trends were found forshort-acting opioid utilization, although no significantdifferences were found for long-acting opioid use.Adjusting for differences in demographics, prior medi-cation use, and comorbidities, duloxetine patients hadsignificantly less opioid use than SOC patients on allutilization measures for both overall (except yearlycumulative opioid dose in morphine equivalents) andshort-acting opioids.
Patients in the duloxetine cohort had significantlylower total direct health-care costs compared with thosein the SOC cohort ($25 466 vs. $37,524, P < 0.05),primarily due to lower outpatient costs ($9,196 vs.$17,933, P < 0.05) (Table 5). Duloxetine patients alsohad lower diabetes-related outpatient costs than SOCpatients ($1,806 vs. $3,772, P < 0.05). Controlling fordemographics, prior diabetic medication use, anddiabetes- and pain-related comorbidities, duloxetinepatients had $8,088 significantly lower total directhealth-care costs and $3,092 lower diabetes-relatedcosts than SOC patients (both P < 0.05), with majority
Table 2. Diabetes- and Pain-related Comorbidities
Duloxetine SOC
Diabetes-related comorbidities (%)Cardiovascular disease 62.9 76.2*Cerebrovascular and peripheral vascular disease 19.5 30.4*Retinopathy 14.0 14.1Skin problems 11.4 12.8Hypoglycemic events 10.7 10.1Other metabolic diseases 7.7 12.8Nephropathy 5.9 6.6Obesity 3.3 6.2Anxiety 3.3 2.2Infections-related to diabetes 0.4 2.6*
Pain-related comorbidities (%)Low back pain 19.9 29.5*Osteoarthritis 15.1 20.3Fibromyalgia syndrome 6.6 5.3Migraine 2.9 3.5Psoriatic arthropathy 1.5 0.4Rheumatoid arthritis 1.1 0.9
* Statistically significant at P < 0.05 (chi square test).SOC, standard of care.
Table 3. Select Medication Use in 12-Month Pre-indexPeriod
Duloxetine SOC
Diabetes-related medications (%) 91.2 88.6Oral antidiabetic drugs 69.5 69.6Insulin 52.9 48.0
Pain-related medications (%)Any antidepressant 59.6 60.8
SSRI 30.5 30.0Tricyclic 21.3 22.9Venlafaxine 6.3 4.9Duloxetine 4.4 11.5*Bupropion 8.1 8.8Other antidepressants 4.8 5.7
Any anticonvulsant 64.3 44.9*Gabapentin 53.7 39.2*Pregabalin 2.2 0.0*Other anticonvulsants 18.8 12.3
Non-narcotics 4.4 2.6Narcotics 54.0 79.3*
Oxycodone and combinations 8.8 32.2*Tramadol 7.4 30.0*Codeine and combinations 5.9 9.3Hydrocodone and combinations 32.4 39.7Propoxyphene and combinations 17.3 18.5Other narcotics 5.2 7.1
NSAIDs 41.5 45.4Cox-2 17.7 22.0Other NSAIDs 30.9 34.8
Number of medications dispensed: mean (SD) 15.9 (6.9) 17.5 (7.3)*Diabetes-related medications 1.8 (1.1) 1.7 (1.1)
Note: Chi-square test for categorical variables (medication utilization); Wilcoxon testfor number of medications dispensed.* Statistically significant at P < 0.05.NSAIDs, non-steroidal anti-inflammatory drugs; SD, standard deviation; SOC,standard of care.
52 • wu et al.
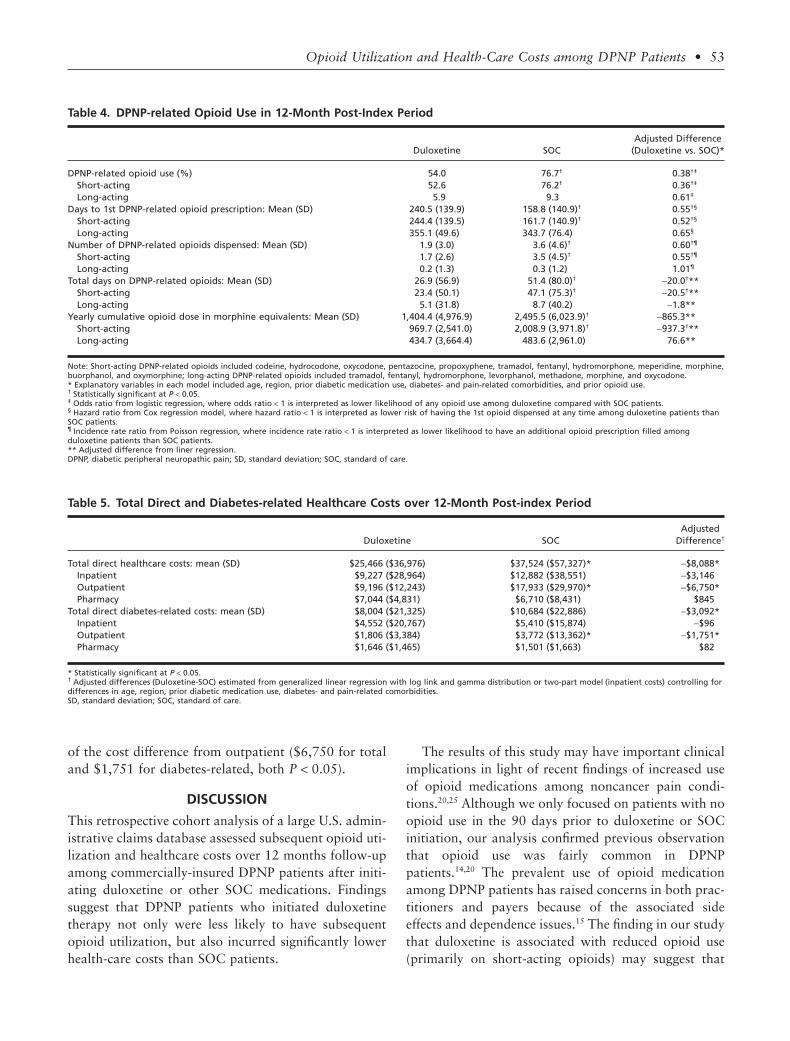
of the cost difference from outpatient ($6,750 for totaland $1,751 for diabetes-related, both P < 0.05).
DISCUSSION
This retrospective cohort analysis of a large U.S. admin-istrative claims database assessed subsequent opioid uti-lization and healthcare costs over 12 months follow-upamong commercially-insured DPNP patients after initi-ating duloxetine or other SOC medications. Findingssuggest that DPNP patients who initiated duloxetinetherapy not only were less likely to have subsequentopioid utilization, but also incurred significantly lowerhealth-care costs than SOC patients.
The results of this study may have important clinicalimplications in light of recent findings of increased useof opioid medications among noncancer pain condi-tions.20,25 Although we only focused on patients with noopioid use in the 90 days prior to duloxetine or SOCinitiation, our analysis confirmed previous observationthat opioid use was fairly common in DPNPpatients.14,20 The prevalent use of opioid medicationamong DPNP patients has raised concerns in both prac-titioners and payers because of the associated sideeffects and dependence issues.15 The finding in our studythat duloxetine is associated with reduced opioid use(primarily on short-acting opioids) may suggest that
Table 4. DPNP-related Opioid Use in 12-Month Post-Index Period
Duloxetine SOCAdjusted Difference
(Duloxetine vs. SOC)*
DPNP-related opioid use (%) 54.0 76.7† 0.38†‡
Short-acting 52.6 76.2† 0.36†‡
Long-acting 5.9 9.3 0.61‡
Days to 1st DPNP-related opioid prescription: Mean (SD) 240.5 (139.9) 158.8 (140.9)† 0.55†§
Short-acting 244.4 (139.5) 161.7 (140.9)† 0.52†§
Long-acting 355.1 (49.6) 343.7 (76.4) 0.65§
Number of DPNP-related opioids dispensed: Mean (SD) 1.9 (3.0) 3.6 (4.6)† 0.60†¶
Short-acting 1.7 (2.6) 3.5 (4.5)† 0.55†¶
Long-acting 0.2 (1.3) 0.3 (1.2) 1.01¶
Total days on DPNP-related opioids: Mean (SD) 26.9 (56.9) 51.4 (80.0)† -20.0†**Short-acting 23.4 (50.1) 47.1 (75.3)† -20.5†**Long-acting 5.1 (31.8) 8.7 (40.2) -1.8**
Yearly cumulative opioid dose in morphine equivalents: Mean (SD) 1,404.4 (4,976.9) 2,495.5 (6,023.9)† -865.3**Short-acting 969.7 (2,541.0) 2,008.9 (3,971.8)† -937.3†**Long-acting 434.7 (3,664.4) 483.6 (2,961.0) 76.6**
Note: Short-acting DPNP-related opioids included codeine, hydrocodone, oxycodone, pentazocine, propoxyphene, tramadol, fentanyl, hydromorphone, meperidine, morphine,buorphanol, and oxymorphine; long-acting DPNP-related opioids included tramadol, fentanyl, hydromorphone, levorphanol, methadone, morphine, and oxycodone.* Explanatory variables in each model included age, region, prior diabetic medication use, diabetes- and pain-related comorbidities, and prior opioid use.† Statistically significant at P < 0.05.‡ Odds ratio from logistic regression, where odds ratio < 1 is interpreted as lower likelihood of any opioid use among duloxetine compared with SOC patients.§ Hazard ratio from Cox regression model, where hazard ratio < 1 is interpreted as lower risk of having the 1st opioid dispensed at any time among duloxetine patients thanSOC patients.¶ Incidence rate ratio from Poisson regression, where incidence rate ratio < 1 is interpreted as lower likelihood to have an additional opioid prescription filled amongduloxetine patients than SOC patients.** Adjusted difference from liner regression.DPNP, diabetic peripheral neuropathic pain; SD, standard deviation; SOC, standard of care.
Table 5. Total Direct and Diabetes-related Healthcare Costs over 12-Month Post-index Period
Duloxetine SOCAdjusted
Difference†
Total direct healthcare costs: mean (SD) $25,466 ($36,976) $37,524 ($57,327)* -$8,088*Inpatient $9,227 ($28,964) $12,882 ($38,551) -$3,146Outpatient $9,196 ($12,243) $17,933 ($29,970)* -$6,750*Pharmacy $7,044 ($4,831) $6,710 ($8,431) $845
Total direct diabetes-related costs: mean (SD) $8,004 ($21,325) $10,684 ($22,886) -$3,092*Inpatient $4,552 ($20,767) $5,410 ($15,874) -$96Outpatient $1,806 ($3,384) $3,772 ($13,362)* -$1,751*Pharmacy $1,646 ($1,465) $1,501 ($1,663) $82
* Statistically significant at P < 0.05.† Adjusted differences (Duloxetine-SOC) estimated from generalized linear regression with log link and gamma distribution or two-part model (inpatient costs) controlling fordifferences in age, region, prior diabetic medication use, diabetes- and pain-related comorbidities.SD, standard deviation; SOC, standard of care.
Opioid Utilization and Health-Care Costs among DPNP Patients • 53

duloxetine can be used prior to other SOC, as the use ofduloxetine may potentially lead to reduced risk of sub-sequent dependence or substance abuse. Also, DPNPpatients initiated on duloxetine had significantly lowertotal and diabetes-related health-care costs than thoseinitiated on SOC. The reduced health-care costs amongduloxetine patients, particularly from the outpatientsetting, might be explained by the observation thatduloxetine patients had less opioid use that may requireless intense or frequent monitoring in outpatient settingthan SOC patients. Further studies are needed toexamine the impact of duloxetine vs. SOC on clinicaloutcomes among DPNP patients as these measures arenot captured in claims databases.
Despite similarities in baseline demographic charac-teristics, duloxetine and SOC patients had somewhatdifferent comorbidities, health-care utilization andcosts, and prior medication use in the 12-month pre-index period. The higher prevalence of cerebrovascular/peripheral vascular disease, cardiovascular disease, andlow back pain among SOC patients may indicate thatthese patients had different disease severity or healthstatus than duloxetine patients, which is also consistentwith the higher utilization and costs observed in theSOC cohort. Not surprisingly, DPNP patients in bothcohorts had many different medications prescribed withSOC patients having more prescriptions dispensed. Thecomorbid medical conditions and complex medicationregimens among DPNP patients may have negativeimpact on their medication adherence, especially onadditional new therapies. Our study suggests thatchoosing duloxetine for the management of DPNP maypotentially help ease the medication burden (especiallyon opioid utilization); however, clinicians need to con-sider all the factors including clinical and economicoutcomes as well as patient preference when selectingappropriate pharmacologic treatments.
Consistent with previous studies,14,18 antidepressantand anticonvulsant medication use was high amongDPNP patients prior to the initiation of duloxetine orSOC with SSRIs being the most frequently used anti-depressant. Similar to previous research,14,18 the use ofNSAIDs reported in this study was also high eventhough NSAIDs are not recommended for managingDPNP.11,26 Given the prevalence of common comorbidpain conditions, it is possible that NSAIDs were usedfor other circumstances other than DPNP. Neverthe-less, further investigation may be necessary as patientsmight be at risk of renal impairment for NSAIDsoveruse.27
Several study limitations need to be noted when inter-preting these results. First, the retrospective cohortdesign did not allow us to determine whether thereduced opioid utilization was directly resulted from theuse of duloxetine. Although we adjusted for observableimbalance between cohorts via multivariate regressionmodeling, unobservable confounders may bias theresults. The severity of DPNP was not captured in ourdata, which has been found to significantly impacthealthcare utilization and costs and is associated withdiminished quality of life.28 Although this study con-trolled for diabetes-related comorbidities as a proxy forDPNP severity, the direct impact of DPNP severity wasunknown. Direct treatment costs calculated in this studywere based on plan and patient out-of-pocket paymentfor each service, and did not capture indirect costsincurred by patients including lost productivity, travelexpenses, and opportunity costs associated with timelost seeking treatment. As over-the-counter medicationswere not captured in the administrative claims data, ourresults may underestimate the actual pharmacy utiliza-tion and associated costs.
CONCLUSIONS
Commercially-insured DPNP patients who initiatedduloxetine therapy had significantly less subsequentopioid use compared with those who initiated otherSOC medications. Furthermore, duloxetine patientsincurred lower total and diabetes-related healthcarecosts, largely due to lower outpatient costs in the12-month post-index period.
REFERENCES
1. Argoff CE, Cole BE, Fishbain DA, Irving GA. Dia-betic peripheral neuropathic pain: clinical and quality-of-lifeissues. Mayo Clin Proc. 2006;81:S3–S11.
2. Galer BS, Gianas A, Jensen MP. Painful diabeticpolyneuropathy: epidemiology, pain description, and qualityof life. Diabetes Res Clin Pract. 2000;47:123–128.
3. Boulton AJ. Management of diabetic peripheral neu-ropathy. Clin Diabetes. 2005;23:9–15.
4. Boulton AJ, Malik RA, Arezzo JC, Sosenko JM. Dia-betic somatic neuropathies. Diabetes Care. 2004;27:1458–1486.
5. Benbow SJ, Wallymahmed ME, MacFarlane IA. Dia-betic peripheral neuropathy and quality of life. Q J Med.1998;91:733–737.
6. Gore M, Brandenburg NA, Hoffman DL, et al.Burden of illness in painful diabetic peripheral neuropathy: thepatients’ perspectives. J Pain. 2006;7:892–900.
54 • wu et al.
7. Stewart WF, Ricci JA, Chee E, et al. Lost productivetime and costs due to diabetes and diabetic neuropathic pain inthe US workforce. J Occup Environ Med. 2007;49:672–679.
8. Gore M, Brandenburg NA, Dukes E, et al. Painseverity in diabetic peripheral neuropathy is associated withpatient functioning, symptom levels of anxiety and depression,and sleep. J Pain Symptom Manage. 2005;30:374–385.
9. Jude EB, Jacob K. Managing painful neuropathy indiabetes. Pol Arch Med Wewn. 2008;118:260–261.
10. Candrilli SD, Davis KL, Kan HJ, et al. Prevalenceand the associated burden of illness of symptoms of diabeticperipheral neuropathy and diabetic retinopathy. J DiabetesComplications. 2007;21:306–314.
11. Argoff CE, Backonja MM, Belgrade MJ, et al. Con-sensus guidelines: treatment planning and options. Diabeticperipheral neuropathic pain. Mayo Clin Proc. 2006;81:S12–S25.
12. Diabetic peripheral neuropathic pain: consensusguidelines for treatment. J Fam Pract. 2006;55(suppl):3–19.
13. Wu EQ, Birnbaum HG, Mareva MN, et al. Cost-effectiveness of duloxetine versus routine treatment for U.S.patients with diabetic peripheral neuropathic pain. J Pain.2006;7:399–407.
14. Wu N, Chen S, Boulanger L, et al. Duloxetine com-pliance and its association with healthcare costs amongpatients with diabetic peripheral neuropathic pain. J MedEcon. 2009;12:192–202.
15. Jensen TS, Backonja MM, Hernandez JS, et al. Newperspectives on the management of diabetic peripheral neuro-pathic pain. Diab Vasc Dis Res. 2006;3:108–119.
16. Benyamin R, Trescot AM, Datta S, et al. Opioidcomplications and side effects. Pain Physician. 2008;11:S105–S120.
17. Robinson-Papp J, Simpson DM. Safety profile oftreatment in diabetic peripheral neuropathic pain. Pain Med.2007;8:S43–S49.
18. Boulanger L, Zhao Y, Foster TS, et al. Impact ofcomorbid depression or anxiety on patterns of treatment andeconomic outcomes among patients with diabetic peripheralneuropathic pain. Curr Med Res Opin. 2009;25:1763–1773.
19. Bureau of Labor Statistics. Consumer price index.www.bls.gov/cpi/ (accessed 20 January 2008).
20. Sullivan MD, Edlund MJ, Fan MY, et al. Trends inuse of opioids for non-cancer pain conditions 2000–2005 incommercial and Medicaid insurance plans: the TROUP study.Pain. 2008;138:440–449.
21. Braden JB, Fan MY, Edlund MJ, et al. Trends in useof opioids by noncancer pain type 2000–2005 among Arkan-sas Medicaid and HealthCore enrollees: results from theTROUP study. J Pain. 2008;9:1026–1035.
22. Afifi AA, Kotlerman JB, Ettner SL, Cowan M.Methods for improving regression analysis for skewed con-tinuous or count responses. Ann Rev Public Health.2007;28:95–111.
23. McCullagh P, Nelder JA. Generalized LinearModels. 2nd ed. London: Chapman and Hall; 1989.
24. Efron B, Tibhirani R. An Introduction to the Boot-strap. New York: Chapman and Hall; 1993.
25. Gilson AM, Ryan KM, Joranson DE, Dahl JL. Areassessment of trends in the medical use and abuse of opioidanalgesics and implications for diversion control: 1997–2002.J Pain Symptom Manage. 2004;28:176–188.
26. Barrett AM, Lucero MA, Le T, et al. Epidemiology,public health burden, and treatment of diabetic peripheralneuropathic pain: a review. Pain Med. 2007;8:S50–S62.
27. Boulton AJ. Treatment of symptomatic diabetic neu-ropathy. Diabetes Metab Res Rev. 2003;19:516–521.
28. Currie CJ, Poole CD, Woehl A, et al. The financialcosts of healthcare treatment for people with Type 1 or Type 2diabetes in the UK with particular reference to differingseverity of peripheral neuropathy. Diabet Med. 2007;24:187–194.
Opioid Utilization and Health-Care Costs among DPNP Patients • 55

Appendix
Condition ICD-9-CM
Diabetes-relatedAnxiety 300.0x, 300.2x, 300.3x, 309.81Cardiovascular disease 390–398.xx, 401.x–403.xx, 404.1, 404.9, 405.xx, 410.xx–417.x, 420.xx–429.xxCerebrovascular and peripheral vascular disease 430.xx–437.xx, 440.xx–444.xx, 447.xx–454.xx, 457.xx–459.xx, 456.3x, 785.4xHypoglycemic events 250.8x, 251.0x–251.2xInfections-related to diabetes 038.xx, 790.7xNephropathy 580.9x, 581.81, 581.9x, 582.9x, 583.81, 588.8x, 593.9xObesity 278.xxOther metabolic diseases 251.3x, 270.3x, 276.xxRetinopathy 362.0x, 362.1x, 362.2x, 362.41, 363.31, 365.44, 366.41Skin problems 707.xx
Pain-relatedFibromyalgia syndrome 729.1xLow back pain 720.1x, 721.3x, 721.9x, 722.1x, 724.02, 724.2x, 724.5x, 724.8x, 733.82Migraine 346.0x, 346.1x, 346.2x, 346.8x, 346.9xOsteoarthritis 715.xxPsoriatic arthropathy 696.xxRheumatoid arthritis 714.xx
56 • wu et al.