ordinary grace and the high cost of caring in a challenging environment sponsored by: awhonn –...
TRANSCRIPT

Ordinary Grace and the High Cost of Caring
in a Challenging Environment
Sponsored by: AWHONN – Oklahoma Section
April 21-22, 2005 Tulsa, OK
Kathleen Brehony, Ph.D.

1. The high cost of caring.
2. Burnout/Stress and what you can do about it.
3. Remembering Grace and how to reinvigorate it in your personal and professional life.

Nurses number 2.7 million and rank as the nation’s largest health care profession
High quality nursing care reduces the rate of complications and lengths of stay in hospitals
A growing disparity between the supply and demand of nurses that is leading to a potentially overwhelming nursing shortage and health care crisis

Changing demographics
Ever-decreasing resources and increased demands on the health care system
Declining social value of nursing as a career
Changes in career opportunities
In spite of the critical value of the profession, nursing’s role in decision-making around health care issues remains limited
Changing economics of health care reimbusrement along with other pressures including mounting documentation requirements and stressful working conditions have contributed to nurse’s diminishing sense of career satisfaction

Hospital Nurse Staffing and Patient Mortality, Nurse Burnout, and Job
Dissatisfaction
Linda H. Aiken, PhD, RNSean P. Clarke, PhD, RNDouglas M. Sloane, PhDJulie Sochalski, PhD, RN
Jeffrey H. Silber, MD, PhD
October 23/30, 2002. Journal of the American Medical Association, 288, 1987-1993.Funding Source : National Institute of Nursing Research, National Institutes of Health
Cross-sectional analysis of linked data from 10,184 staff nurses surveyed 232,342 general, orthopedic and vascular surgery patients (between the ages of 20 and 85) discharged from the hospital between April 1, 1998 and November 30, 1999, and administrative data from 168 nonfederal adult general hospitals in Pennsylvania.

Sites for International Study of Hospital Outcomes
United States University of
Pennsylvania Ontario
University of Toronto
Mt. Sinai WHOCollaborating Centre
British Columbia University of British
Columbia Alberta
University of Alberta
Germany Hannover Medical
School England
London School of Hygiene and Tropical Medicine
Scotland Glasgow
University Nursing Initiative
of Scotland Scottish NHS

Outcomes in 232,342 Surgical Patients
4,535 (2.0%) died within 30 days of admission
53,813 (23.2 %) were observed to experience a major complication
the death rate among complicated patients (failure to rescue rate) was 8.4%
Source: Aiken et al 2002
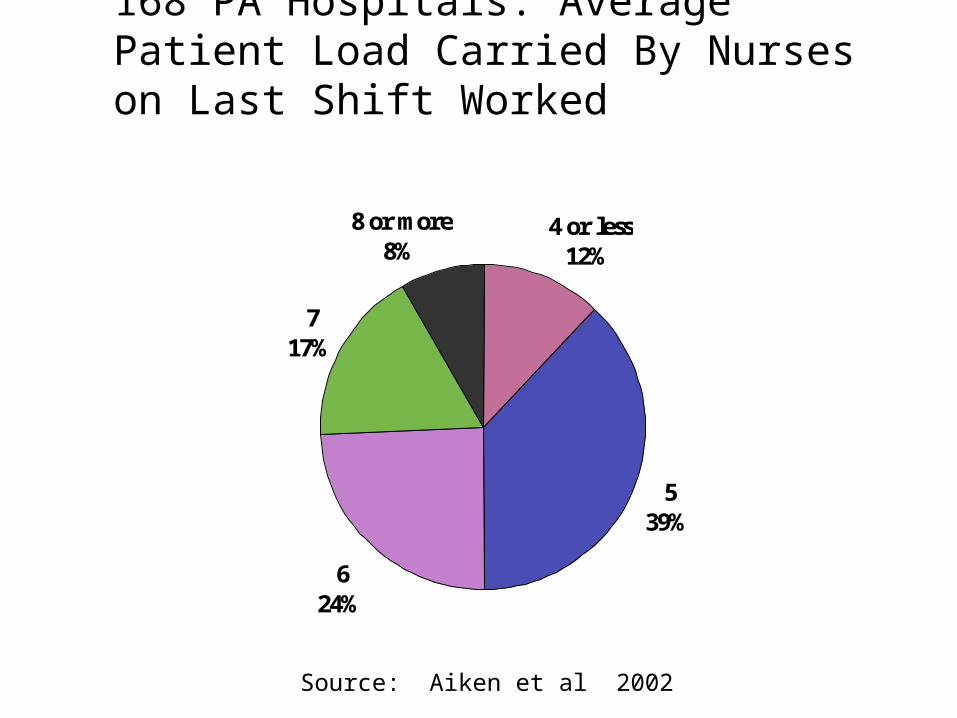
168 PA Hospitals: Average Patient Load Carried By Nurses on Last Shift Worked
4 or less12%
539%
624%
717%
8 or more8%
Source: Aiken et al 2002

Effect of Nurse Staffing on Mortality
For every one patient-per-nurse increase in nursing workloads in PA hospitals: 14% increase in risk of death within 30 days for an individual patient
After controlling for all the hospital and patient variables we have: 7% increase in risk of death
Source: Aiken et al 2002
Translating the Results
5 per 1000 fewer surgical patients of the types studied expected to die in hospitals with 4:1 versus 8:1 average ratios
~ 4 M similar procedures/year in U.S. hospitals: if all patients treated in hospitals at 4:1 vs. 8:1 ratios … up to 20,000 fewer deaths
Source: Aiken at al 2002

Conclusions (Aiken et al 2002):In hospitals with high patient-to-nurse-ratios, surgical patients experience higher risk-adjusted 30-day mortality and failure-to-rescue rates, and nurses are more likely to experience burnout and job dissatisfaction.

Inpatient Mortality Rates in 118,803 English Surgical Patients From 30 Trusts in Relation to Nurse Staffing Levels
2
2.2
2.4
2.7
1
1.21.4
1.6
1.82
2.2
2.42.6
2.8
Lowest Pt:NurseRatios
Highest Pt:NurseRatios
Cru
de
mo r
talit
y ra
t e %

Education Levels of Hospital Nurses and Patient Mortality
Aiken, Clarke, Cheung, Sloane, & Silber (September 24, 2003, Journal of the American Medical Association)
The proportion of hospital staff RNs holding baccalaureate or higher degrees as their highest (not initial) credential ranged from 0 to 77% across the hospitals.

Patient deaths after surgery are lowest in hospitals where nurses care for fewer patients on average and have higher
levels of education
0
5
10
15
20
25
20 40 60
High
Medium
Low
Dea
ths
per
1000
pat
ient
s
Patient-to-nurse ratios
% Bachelor’s-preparednurses
Source: Aiken et al 2003

Relationship Between Nurse Staffing and Selected Adverse Events Following
Surgery (Kovner & Gergen, 1998)
Significant inverse relationship between RN staffing levels and the following postoperative complications:
urinary tract infections pneumonia thrombosis pulmonary compromise
Estimated that one additional RN hour per patient day was associated with a 9% decrease in UTI and 8% decrease in pneumonia
Kovner et al. (2002)—only pneumonia associated with staffing

Blegen et al. (1998)
Increasing a unit’s total hours of care (RN, LPN, NA) is not associated with lower rates of adverse outcomes
Increasing the proportion of RN hours of care is associated with lower rates of adverse outcomes: medication errors pressure ulcers patient complaints patient falls

American Nurses Association Sponsored Studies (1997,
2000) Two major studies on the relationship between nurse
staffing and patient outcomes “that [could] reasonably be theorized to be preventable in some patients by the amount and skill mix of nursing provided.” (ANA, 2000, p. vii)
Associations between higher staffing and higher proportions of RNs and better outcomes across 9 states:
shorter lengths of stay lower risk of pressure ulcers lower risk of pneumonia lower risk of postoperative infections lower risk of urinary tract infections

Nurse Staffing and Patient Outcomes in Hospitals Needleman, Buerhaus, et al. (2001) (Report available at www.hrsa.gov)
Main analyses involved 1997 discharges from 799 hospitals across 11 states (AZ, CA, MA, MD, MI, NV, NY, SC, VA, WI, WV)
The study found statistically significant relationships between nurse staffing variables and the following patient outcomes in acute care :
Medical Patients: urinary tract infection, pneumonia, shock, upper gastrointestinal bleeding, length of stay
Patients Undergoing Major Surgery: urinary tract infection, pneumonia, failure to rescue (defined as the death rate among patients with sepsis, pneumonia, shock, upper gastrointestinal bleeding, or deep vein thrombosis)
Nurse Staffing and Patient Outcomes in Hospitals
Needleman, Buerhaus, et al. (2001). (Report available at www.hrsa.gov)
High RN staffing associated with 3-12% decrease in likelihood of events, high total nursing staffing associated with 2-25% decrease
No effects of staffing on mortality in either medical or surgical patients
Study conducted at Harvard and reported to HHS.
Published in New England Journal of Medicine in May 2002

Examples of Other Recent Staffing Research
Cho, S.-H., et al.: The effects of nurse staffing on adverse events, morbidity, mortality and medical costs. Nursing Research. 2003; 52(2): 71-79.
McGillis Hall L et al. Nurse staffing models as predictors of patient outcomes. Med Care. 2003; 41(9):1096-1109.
Person SD et al. Nurse staffing and mortality for Medicare patients with acute myocardial infarction. Medical Care. 2004; 42(1):4-12.
Unruh L. Licensed nurse staffing and adverse events in hospitals. Med Care. 2003 Jan;41(1):142-52.
Issues for Clinicians and Managers (Clarke, Nursing Management, June 2003)
Financial imperatives v patient needs Burnout, job satisfaction issues in nursing
staff: potential for vicious cycles Perceptions of staff and managers are the
most important tool right now in evaluating the safety of staffing levels
Legal liability issues Communicating staffing decisions to staff
and patients/families

Minimum Staffing Ratios: The Goals
Proponents hope to alleviate some prominent concerns about patient safety
Minimum staffing requirements will lead to more manageable workloads, improve nurse job satisfaction and retention and ameliorate the hospital nurse shortage

Half of all Americans believe that the quality of health care is affected “a great deal” by a shortage of nurses (Harris Poll, 1999)
93% of Americans believe that the nursing shortage jeopardizes the quality of health care (Penn, Shoen,& Berland, 2001).
The size of the U.S. population older than 65 is projected to double over the next 30 years, growing to 70 million by 2030.
Those over age 85, who tend to require more health care services than the young, are the fastest growing segment of the population.
Source: U.S. Census Bureau, Decennial Census Data and Population Projections

The Bureau of Labor Statistics reports that jobs for RNs will grow 23 percent by 2008. That's faster than the average for all other occupations. About half of the RN workforce will reach retirement age in the next 15 years. The average age of new RN graduates is 31. They are entering the profession at an older age and will have fewer years to work than nurses traditionally have had. RN enrollments in schools of nursing are down. In fall 2000, entry-level BSN enrollment fell by 2.1 percent, dropping for the sixth year in a row, according to the American Association of Colleges of Nursing

Source: Vahey DC, Aiken LH, Sloane DM, Clarke SP and Vargas D., “Nurse Burnout and Patient Satisfaction,” Medical Care, 42(2): II-57-II-66, February
2004
3 Major Factors in Nurse Burnout
Surveys of 820 Nurses and Interviews with 621 AIDS patients in an urban hospital
environment
Inadequate numbers of nurses
Poor administrative support for nursing care
Poor doctor-nurse relationshipsThe same factors that lead to nurse burnout are
identical to the ones that lead to poor patient satisfaction with their care

The “Perfect Storm”
Demographic trends in the profession
Financial pressures within health care
Demand for health care and demand for nursing services within the health care system
Source: Sean Clarke, RN, PhD, CRNP, CSAssistant Professor, School of Nursing, University of Pennsylvania

SearchpopupresuFILEDATEdetnewsdesc


Work in which the demands imposed are threatening and not well-matched to the knowledge, skills, and ability tocope of the nurses involved
Work which does not meet the needs of the nurses involved
Situations in which nurses have little control over work
Situations in which nurses receive little support at or outside of work
Cox, T. and Griffiths, A. “Work-related stress in nursing: Controlling the risk to health.” Working paper, International Labor Office, Geneva,
Switzerland, 1996.
Work-Related Stress for Nurses

“Everyday the nurse confronts stark suffering, grief, and death as few other people do. Many nursing tasks are mundane and unrewarding. Many are, by normal standards, distasteful and disgusting. Others are often degrading; some are simply frightening.”
Hingley, P. “The humane face of nursing,” Nursing Mirror, No. 159, 1984, pg 19-22.
1. Dealing with death and dying.
2. Conflict with physicians.
3. Inadequate preparation to deal with the emotional needs of patients and their families.
4. Lack of staff support.
5. Conflict with other nurses and supervisors.
6. Workload.
7. Uncertainty concerning treatment.P. Gray-Toft and T.G. Anderson (1981a): “The nursing stress scale: Development of an instrument,” Journal of Behavioural Assessment, vol. 3, 1981, pp 11-23; P. Gray-Toft and T.G. Anderson (1981b): “Stress among hospital nursing staff: It’s causes and effects,” Social Science and Medicine, vol. 15A, 1981, pp 539-647.
7 Major Causes of Stress in Nursing

1. Leadership and planning
2. Delivery Systems
3. Legislation/regulation/policy
4. Professional Nursing Culture
5. Recruitment/retention
6. Economic value
7. Work environment
8. Public relations/communication
9. Education
10. Diversity
The 10 Domains: Areas of Concern Demanding Action

“Without good and careful nursing many must suffer greatly, and probably perish, that might have been restored to health and comfort, and become useful to themselves, their families, and the public, for many years after.” -- Benjamin Franklin (1751)

Stress is a reaction to a physical or psychological threat to the body. Some things will create stress in everyone (e.g., being attacked by a wild tiger).
Stress is also a personalized reaction because what may be a threat to one person may or may not be to another (e.g., speaking in front of groups).
Stress is also a struggle to adjust to a life change.
Stress is expressed physiologically, emotionally, cognitively, and behaviorally.
Stress
The term "stress" is short for distress, a word evolved from Latin that means "to draw or pull apart."

Innervated by the Sympathetic Nervous System
Increased respiration rate
Increased heart rate
Changes in blood flow (increasing flow to the skeletal muscles and decreasing to the periphery results in cold hands and feet)
Increased muscle tension
Increased metabolism
Increased perspiration/sweating
Decreased digestion
Changes in blood chemistry
Fight or Flight Response

The primary area of the brain that deals with stress is its limbic system. Because of its enormous influence on emotions and memory, the limbic system is often referred to as the emotional brain. It is also called the mammalian brain, because it emerged with the evolution with our warm-blooded relatives, and marked the beginning of social cooperation in the animal kingdom. Whenever you perceive a threat, imminent or imagined, your limbic system immediately responds via your autonomic nervous system – the complex network of endocrine glands that automatically regulates metabolism.

Your adrenal glands release adrenaline (also known as epinephrine) and other hormones that increase breathing, heart rate, and blood pressure. This moves more oxygen-rich blood faster to the brain and to the muscles needed for fighting or fleeing.
And, you have plenty of energy to do either, because adrenaline causes a rapid release of glucose and fatty acids into your bloodstream. Also, your senses become keener, your memory sharper, and you are less sensitive to pain.
Other hormones shut down functions unnecessary during the emergency. Growth, reproduction, and the immune system all go on hold. Blood flow to the skin is reduced. That's why chronic stress leads to sexual dysfunction, increases your chances of getting sick, and often manifests as skin ailments.
With your mind and body in this temporary state of metabolic overdrive, you are now prepared to respond to a life-threatening situation.

Selye’s General Adaptation Syndrome (GAS)
Stage Effect
Alarm “Fight or Flight” Response Intense ANS Arousal (e.g., heart rate, respiration rate, BP increase, etc.)
Resistance
Prolonged state of moderately high arousal Resistance saps energy and weakens immune system
Exhaustion
Vulnerability to illness increases Physical illnesses become more common

Chronic Stressors
(Long lasting threats)
Acute Stressors(Immediate threats)
Physical Stressors (threats to health and safety)
DiseaseStarvationPoverty
PredatorsCombatCrime
Psychosocial Stressors(life role demands)
UnemploymentDivorceChildcare
Work DeadlinesArgumentsFinal Exams
Point: We are less well-evolved to cope with psychosocial stressors.
Forms of Stress

Using brain imaging, combat veterans were found to have an 8% reduction in right hippocampal volume (i.e., the size of the hippocampus), measured with magnetic resonance imaging (MRI), while no differences were found in other areas of the brain.
This study also showed that diminished right hippocampal volume in the PTSD patients was associated with short-term memory loss. Similar results were found when researchers looked at PTSD sufferers who were victims of childhood physical or sexual abuse.
Bremner, J. D. “The Invisible Epidemic: PTSD, Memory Loss and the Brain” Yale University, School of Medicine. Grant by NIH, VA, and the National Center for PTSD Grant.

Note increased right basal ganglia:28 year old woman with chronic anxiety, conflict avoidance
Note increased right basal ganglia:44 year old man with chronic mild anxiety, conflict avoidance
Note increased right and left basal ganglia:48 year old man with panic disorder
Source: Daniel G. Amen, M.D. SPECT Imagingwww.amenclinic.com

Stress as Demands & Resources
Unpredictable/Uncontrollable events create demands
Demands require an adaptive response
Increased resources to:Attention narrows (focus on stressor)Physical & emotional arousal (devoted to coping)Immune system (increases in functioning)
Decreased resources to:
Sexual driveDigestive systemPain response
Stress = demands overwhelm resources

Primary Appraisal: “How threatening is the event?”
Secondary Appraisal: “Do I have the resources to cope with the
event?”

In the short-term, stress can be either a positive or negative experience (distress v eustress). It can keep us alert and ready to avoid danger.
Stress can increase our motivation to complete a task, improve our performance, and add excitement to our lives. Many recreational activities are stress producing and enjoyable because of it.
Stress releases norepinephrine which helps create new memories, improves mood, and encourages creative thinking.
But stress in the short term can be a negative experience when we feel it too strongly. It can interrupt or interfere with our desired performance. Too much stress in the short term can cause us discomfort and create in us a desire to avoid or leave certain situations.
Short-Term Effects of Stress

Distress v Eustress

Simply stated, moderate levels of arousal produce the best performances in most cases.

Long-Term Effects of StressWhen the stress reaction is repeatedly elicited or occurs on a chronic basis, the long-term effects can be serious, even deadly. Chronic stress can result in both physical and emotional disorders including: Fatigue Insomnia Headaches Backaches Muscle Pain Skin Disorders GI Dysfunctions Ulcers Increased Susceptibility to Infectious Disease
Sexual Dysfunction
Increased probability of Accidents
Psychiatric Disorders
Hypertension Cardiovascular Disease Stroke Heart Attacks More Rapid Aging Cancer

Cognitive dysfunction Impaired concentration, memory Poor judgment/decision making
Negative emotions Hostility (Anger, Irritability, Frustration, etc.)
Anxiety Depression
Fear
Physical dysfunction Immune system dysfunction Insomnia Cardiovascular system dysfunction Pain (Neck Pain, Back Pain, Headaches) Gastrointestinal problems (Ulcers, Irritable bowel)
Behavioral consequences Substance abuse
Role withdrawal Role performance
Consequences of Chronic Stress

Forty-three percent of all adults suffer adverse health effects from stress.
Seventy-five to 90% of all doctor's office visits are for stress-related ailments and complaints.
Stress is linked to six of the leading causes of death: heart disease, cancer, lung ailments, accidents, cirrhosis of the liver, and suicide.
The Occupational Safety and Health Administration (OSHA) declared stress a hazard of the workplace. In terms of lost hours due to absenteeism, reduced productivity and workers' compensation benefits, stress costs American industry more than $300 billion annually.
The lifetime prevalence of an emotional disorder is more than 50%, often due to chronic, untreated stress reactions.
STRESS and the High Cost of Caring

Psychneuroimmunology (PNI) Study of psychological influences on immune system functioning
Immune system Body’s system of defenses against viral & bacterial agents
Lymphocytes = White blood cells B Cells – neutralize “foreign agents” T Cells – attack infections
Immunosuppression Hypothalamic-pituitary-adrenal (HPA) axis produces cortisol in response to stress Cortisol energizes body for stress response (e.g., fight or flight)
Increased stress response = decreased immune system response
Stress and the Immune System

OrganismStimulus Response
S-O-R Model of StressStress = Demand Exceeds
Capacity
= Stressors

“When the cards are dealt and you pick up your hand, that is determinism; there’s nothing you can do except to play it out for whatever it may be worth. And the way you play your hand is free will.” -- Jawaharlal Nehru

Stress!! What Can You Do?Einstein on “Insanity”:
“Doing the same thing over and over again and expecting different results.”
What do you choose to see? Do you believe that there is nothing you can do or do you believe that there are lots of things you can do to ameliorate the high
cost of caring?

A Short Film
You will see six people playing basketball – three are wearing black shirts and three are wearing white shirts. Each player can do one of three things:
1. Dribble 2. Pass the ball 3. Bounce-Pass the ball
CAREFULLY COUNT THE NUMBER OF TIMES THAT PLAYERS IN WHITE SHIRTS BOUNCE-PASS THE BALL.

Four-Stage Stress Management Model Identify
(Physical, Cognitive, Behavioral)
Analyze
Develop Plan
Implement
Plan

Identify the Symptoms of Stress
Physiological
Cognitive
Behavioral

Physiological Signs of Stress Headache
Vomiting
Sleep disturbances
Fatigue
Shallow breathing
Dryness of the mouth or throat
Susceptibility to minor illness
Cold hands
Itching
Being easily startled
Chronic pain
Dysponesis
Increased heart rate
Pounding heart
Elevated blood pressure
Sweaty palms
Tightness of the chest, neck, jaw, and back muscles
Nausea
Diarrhea
Constipation
Urinary hesitancy
Trembling
Twitching
Stuttering and other speech difficulties

Cognitive Signs of Stress Forgetfulness Preoccupation Blocking Blurred vision Errors in judging distance Diminished or exaggerated fantasy life Reduced creativity Lack of concentration Lack of attention to detail Orientation to the past Decreased psychomotor reactivity and coordination Attention deficit Disorganization of thought Negative self-esteem and Pessimism Diminished sense of meaning in life Lack of control/need for too much control Negative self-statements and negative evaluation of experiences

Behavioral Signs of Stress Increased smoking Aggressive behaviors (e.g., road rage) Increased alcohol or drug use Carelessness Crying Under-eating or Over-eating Sleeplessness or want to sleep all the time Withdrawal Listlessness Hostility Accident-proneness Nervous laughter Compulsive behavior Impatience Diminished productivity Self-injurious behaviors/suicide

Keep a stress diary for one week. Use a small 3x5 notebook to record stressful situations and how your respond to them. By recording over time, you will come to better understand your own personal stressors. Your individual stress pattern is unique.
Note the physiological, behavioral, and cognitive signs of stress and assign a “Stress Rating” by ranking them on a 10-point scale (where 10 is “extremely stressful” and 1 is “not stressed at all). If you feel like you are “stressed all the time,” then record 4 times a day: 1) before work, 2) mid-day (before lunch), 3) after work, and 4) at bedtime.
Date
Time
Where you were
What you were doing
Signs of Stress (physiological, behavioral, cognitive)
Stress Rating (using 10-point scale)

Analyze the Sources of Stress
Environmental/Social/Professional Sources
Cognitive Sources
Physical Sources

Different life crises have different impacts. In many cases, however, it may be possible to anticipate crises and prepare for them. It may also be useful to recognize the impact of crises that have occurred so that you can take account of them appropriately. Some very interesting work in this area has been done by Drs T H Holmes and R H Rahe, with the Social Readjustment Scale. This allocates a number of 'Life Crisis Units' (LCUs) to different events, so that you can evaluate them and take action accordingly.
The idea behind this approach is to run down the LCU table, totaling the LCUs for life crises that have occurred in the previous 2 years. As a rule of thumb, you may anticipate some form of serious mental or physical effects of the crises according to the following table:
Life Crisis Units (LCUs) and the Probability of Stress-Related Illness:
300 80%+ 200-299 50% 150-199 33%

Holmes, T. H., & Rahe, R. H. (1967). The social readjustment rating scale. Journal of Psychosomatic Research, 11, 213-218.
Death of spouse 100
Divorce 73
Separation 65
Jail term 63
Death of close family member 63
Personal illness or injury 53
Marriage 50
Fired at work 47
Marital reconciliation 45
Retirement 45
Change in health of family member 44
Pregnancy 40
Sex difficulties 39
Gain of new family member 39
Business readjustment 38
Change in financial state 38
Death of close friend 37
Change to a different line of work 36
Change in number of arguments with spouse 35
A large mortgage or loan 30
Foreclosure of mortgage or loan 30
Change in responsibilities at work 29
Son or daughter leaving home 29
Trouble with in-laws 29
Outstanding personal achievement 28
Spouse begins or stops work 26
Begin or end of school or college 26
Change in living conditions 25
Change in personal habits 24
Trouble with boss 23
Change in work hours or conditions 20
Change in residence 20
Change in school or college 20
Change in recreation 19
Change in church activities 19
Change in social activities 18
A moderate loan or mortgage 17
Change in sleeping habits 16 C
Change in number of family get-togethers 15
Change in eating habits 15
Holiday 13 Christmas 12
Minor violations of law 11

Environmental/Social/Professional Sources of Stress
War
Terrorism
Possibility of natural disasters
Environmental toxins
Crowding
Noise
Disorganized environments
Large-Scale Environmental Sources of Stress

Environmental/Social/Professional Sources of StressCommon Family Stressors
Marital problems/Divorce
Financial problems
Health problems in family member
“Sandwich Generation”
Problems with behavior of a child
Blended families
Death of a family member
Member of the family leaving home and other significant life adjustments
Difficulty with achieving family/work balance (Dual role women)
Change in family residence
Isolation/loneliness
Beginning a new job
Retirement
Work overload
Time pressures
Role ambiguity or uncertainty
Lack of job security
Poor relationships with supervisors or colleagues
Responsible for things you cannot control
Common Work Stressors
Environmental/Social/Professional Sources of Stress

Dealing with death and dying
Conflict with physicians
Inadequate preparation to deal with the emotional needs of patients and their families
Lack of staff support
Conflict with other nurses and supervisors Workload
Uncertainty concerning treatment
Inadequate financial and other rewards
Physical stresses and strains
Special Work Stressors for Nurses

Cognitive Sources of Stress
Negative Self-Statements are converted into beliefs (generally, irrational beliefs such as Perfectionism)
Unrealistic expectations
Pessimistic world view
Imagining the worst outcomes
Ruminative worry
Illusions about change
Significant life events and our reactions
Victims of our autobiography
Unrealistic expectations
Black/White (“Either/Or”) v (“Both/And”) thinking
Failure to stay in the Present

One should be liked, or approved of, by almost everyone.
To be worthwhile, one must be competent in all things.
Things should always be the way we want them to be, and it’s terrible when they aren’t.
A person’s present and future behavior is irreversibly dependent upon significant past events. People can never change.
Every problem must have an ideal solution, and it’s really bad when this solution is not found.
Everything I do must automatically lead to an immediate payoff.
Individuals have little internal control over their personal happiness or misery.
If there is some possibility that something can go wrong, one should worry about it.
It is easier to avoid than to face difficulties and responsibilities inherent in living.
People can’t be trusted to make their own decisions.
Common Irrational and Self-Defeating Beliefs

Our History MAY Become Our Future
Habits are formed through repetition
Psychological and neurological “ruts” (Synaptic pathways)
Negative self-image, internal self-talk, self-defeating beliefs
The Good News! People can change through insight and action!

The Structure of Emotional Responses
Albert Ellis: A-B-C Model
Activating Event(e.g., Boss’s reprimand)
A
C Feelings and Behavior
(e.g., upset, nervous, defensive)
This is the model that most people believe.

Between A (Activating Event) and C (Feelings and Behavior) is B -- your thinking and your self-talk.
A
B
C
Activating Event(e.g., Boss’s reprimand)
Feelings and Behavior(e.g., upset, nervous, defensive OR
disappointment, but kept in perspective)
Your Thinking(e.g., “I can’t do anything right” OR“I made a mistake, but I’ll be more
careful next time.”)

Locus of Control
(A Continuum)
Internal
Locus of Control
External
Locus of Control
Free Will
DestinyVs.
Learned Helplessness – the failure to avoid or escape from an unpleasant or aversive
stimulus that occurs as a result of previous exposure to unavoidable painful stimuli.”

Learned Helplessness has been observed in dogs, rats,
mice, cats, monkeys, and even Walleyed Pike!

On Elephants and Fleas

Physical Sources of Stress
Poor or unbalanced diet
Lack of exercise
Smoking
Alcohol & Drug use (including the inappropriate use of prescribed medication)
Caffeine
Poor sleep habits
No time for relaxation
Hormonal exacerbation of emotional states

Develop a Stress Management Plan:
Techniques Discover a Larger Perspective
Change Your Point of View - Optimism
Cognitive Restructuring
Relaxation/Meditation/Prayer/Silence
Change in Physical Health Habits
Changing the Situation
Self-Expression
Humor
Time Management
Social Support and Connections

Discover a Larger Perspective
The Eagle Nebula – 7 Million Light Years Away

Become involved in a regular practice of prayer and participate in a worship community
Experience your faith
Read about your own tradition
Explore other religious & spiritual traditions
Take classes in philosophy, metaphysics or other disciplines that focus on meaning
Investigate your family genealogy
Look to nature
Write down or sketch your thoughts and reflections
Some Ways of Discovering a Larger Perspective

Optimistic versus Pessimistic Cognitions During Hard Times
Optimistic Pessimistic
Temporary Permanent
Specific Pervasive
External Personal
Source: Martin Seligman, Learned Optimism
Optimism to Reduce Stress

In a 23-year study done in a small town in Ohio by researchers from Yale and Miami Universities, people over 50 who viewed aging as a positive experience lived an average of 7.5 years longer than those who did not -- a big gap. (The researchers controlled for such possible confounding factors as race, gender, state of health, morale, and loneliness.) People got more mileage out of optimism, in fact, than from lowering blood cholesterol levels. And other things being equal, they got more mileage out of their will to live than other psychological factors.
Mayo Clinic researchers followed 447 people whose personal traits had been evaluated 30 years earlier. Those classified as optimists had half the risk of early death compared to those classified as pessimistic or "mixed." The optimists had fewer problems as they aged--fewer limitations, less pain, and more energy.
In a study called "Is the Glass Half Empty or Half Full?" Harvard researcher Dr. Laura Kubzansky found that optimism, as evaluated in the way people explain events in their lives to themselves and others, was protective against heart disease. Other studies have found that optimists tend to recover faster after coronary bypass surgery than pessimists. Dr. Kubzansky and other researchers believe that negative emotions and chronic pessimism should be regarded as risk factors for heart disease.
1/17/05

BBC Interview with the Dalai Lama:
“Why would I give them my mind?”

“If the only prayer you said in your whole life was ‘Thank you,’ it would be sufficient.”
-- Meister Eckhart

1. RECOGNIZE: Become more aware of your thoughts and feelings that occur in response to stressful situations. These Negative Automatic Thoughts (NATs) often go under the radar – unconscious and knee-jerk. Eavesdrop on this internal monologue by asking yourself: “What were my thoughts and what was I saying to myself about the situation that contributed to my feelings of stress?”
Cognitive Restructuring to Reduce Stress
1. Recognize
2. Challenge
3. Change

2. CHALLENGE: Reframe with questions
Is this thought really true?
What is the worst thing that could happen?
What is the likelihood of the worst happening?
Am I overemphasizing a negative aspect of this situation?
Is there anything that might be positive about this situation?
Am I “catastrophizing” or “awfulizing,” jumping to conclusions, or assuming a negative outcome?
How do I know this situation will turn out this way?
Is there another way to look at this situation?
What difference will this make next week, month, year? Will I even remember this a year from now?
If I had one month to live, how important would this be?
Have I done everything I can to change the situation for the better?
Am I using words like “never,” “always,” “worst,” “terrible,” or “horrible,” to describe the situation?

Good Luck? Bad Luck? Who Knows?
“Do you have the patience to wait till
your mud settles and the water is clear? Can you remain unmoving
till the right action arises by itself?”
-- Tao te Ching

Use the “double-standard technique”: Ask yourself: “Would I say this to a close friend with a similar problem? If not, what would I say to him/her?” Give yourself the same encouraging, empathic messages you would giveto a good friend.
Reflect on past experience: “Has anything like this happened to me in the past and, if so, how did it turn out?”
2. CHALLENGE: Cont’d.

Replace “awfulizing” with healthy, realistic alternative cognitions. With practice, you can learn to use Cognitive Restructuring to turn off the negative stress filter, catch and reframe NATs and develop a greater sense of control over your mental responses to stress.
3. CHANGE: Replace Old Cognitions with New Ones

1. Identify the Self-Defeating Belief
2. Develop a realistic alternative
3. Systematically substitute the realistic alternative for the Self-Defeating Belief

Self-Defeating Belief Realistic AlternativeOne should be liked, or approved of, by almost everyone.
No one is liked by everyone. It’s unrealistic to expect to be.
To be worthwhile, one must be competent in all things.
One should not expect to be perfect in all respects.
Things should always be the way we want them to be, and it’s terrible when they aren’t.
Things are not always the way we want them to be, but that’s not the end of the world.
A person’s present and future behavior is irreversibly dependent upon significant past events. People can never change.
People can and do change.
Every problem must have an ideal solution, and it’s really bad when this solution is not found.
Many problems don’t have ideal solutions. It’s unrealistic to expect them to.
Everything I do must automatically lead to an immediate payoff.
Only a small proportion of what I do leads to an immediate payoff.
Individuals have little internal control over their personal happiness or misery.
We can exercise a great deal of control over our own happiness or make our misery worse.
If there is some possibility that something can go wrong, one should worry about it.
We should make reasonable preparations for adversity, but excessive worrying won’t help.
It is easier to avoid than to face difficulties and responsibilities inherent in living.
In the long run, it’s better to face difficulties and accept responsibility.
People can’t be trusted to make their own decisions.
I can facilitate other people’s decision making, but I can’t decide for them.

Myths of the Perfect Nurse
Cares deeply for all patients
Has no life aside from serving mankind
Considers herself the physician’s handmaiden
Never makes an error*
Is compulsively neat and perfect
Is always calmStrive for “perfection” in limited (and critical)
areas

What's my goal?
I need to calm down.
This situation isn't worth it.
I'll take a few seconds here to relax.
My body is telling me it isn't happy.
What can I do to calm down? Ok, time for a warm bath! Ok, time for a walk around the block. What's the best way out of here?
I'm just human. So, I'll do the best I can, and let the rest go.
During Stress: Refocus Your Thoughts, Reset Your
Bearings

God grant me the serenity to accept the things I cannot
change; courage to change the things I
can;and wisdom to know the
difference.
--Reinhold Niebuhr
The Serenity Prayer

Relaxation, Meditation, Prayer, Silence to Reduce Stress
Relaxation Response Innervated by the Parasympathetic Nervous System
Relaxation is not the same state as sleep, recreation, or hypnosis
Relaxation is a specific, integrated, innate, physiological state of the body that includes: Decreased respiration rate
Decreased heart rate
Changes in blood flow (away from the skeletal muscles – resulting in warm hands and feet)
Decreased muscle tension
Decreased metabolism
Increased digestion
Changes in blood chemistry

Stress v Relaxation: What is the Message?
Short-Term Effects of Relaxation Response
Alleviation of immediate stress
Feelings of refreshment
New outlook and improved creativity
Long-Term Effects of Relaxation Response
Reduction of headaches, muscle aches, anxiety
Reduction of the effects of long-term problems associated with the chronic occurrence of the stress reaction
Vibrant health
Patients with hypertension experienced significant decreases in blood pressure and needed fewer or no medications over a three-year measurement period (Eileen M. Stewart).
Patients with chronic pain experienced less severity of pain, more activity, less anxiety, less depression, less anger, and they visited the managed care facility where they received care 36 percent less of- ten in the two years after completing the program than they did prior to treatment (Margaret A. Caudill).
Seventy-five percent of patients with sleep-onset insomnia were cured and became normal sleepers. Sleeping also improved for the other 25 percent, and most patients took significantly fewer sleep medications (Gregg D. Jacobs). Patients with complaints described by the admitting personnel as psychosomatic and who were frequent users of a health maintenance organization reduced their number of visits by 50 percent (Carolinej.C. Hellman).
Effects of Relaxation Response: Research Results from MindBody Institute in
Boston
Source: Herbert Benson, Timeless Healing, Scribner

Patients who suffered from anxiety or mild or moderate depression were less anxious, depressed, angry, and hostile (Herbert Benson).
Women suffering from symptoms of premenstrual syndrome (PMS) experienced a 57 percent decrease in severity. The more severe the PMS, the more effective the relief with the relaxation response (Irene L. Goodale).
Patients undergoing painful X-ray procedures experienced less anxiety and pain and needed one- third the amount of pain and anxiety medications usually required (Carol L. Mandle).
Patients who had open-heart surgery had fewer postoperative arrhythmias and less anxiety following surgery (Jane Lesserman).
Migraine and cluster headache sufferers found they had fewer and less severe headaches (Herbert Benson).
High school sophomores increased their self-esteem (Herbert Benson).
Working people experienced reduced symptoms of depression, anxiety, and hostility (Patricia Carrington).
Working people had fewer medical symptoms, fewer illness days, improved performance, and lower blood pressure (Ruanne K Peters).
Research on the Relaxation Response

Meditating nuns have increased activity (red) in regions used for concentration
Source: Andrew Newberg, M.D. Director of Clinical Nuclear Medicine, Director of NeuroPET Research, and Assistant Professor in the Department of Radiology at the Hospital of the University of Pennsylvania
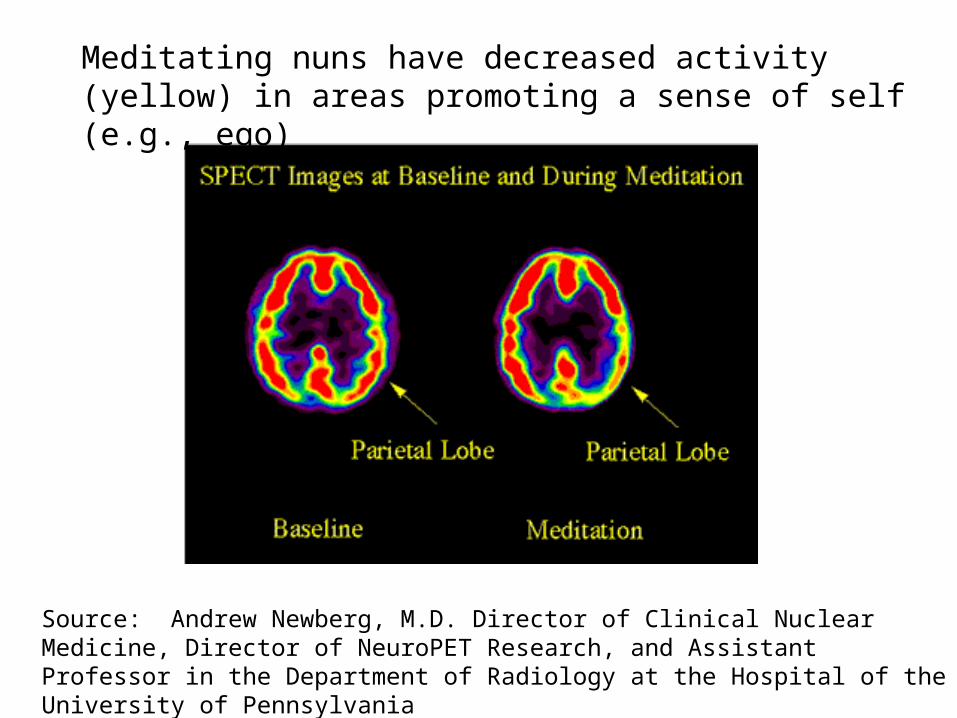
Source: Andrew Newberg, M.D. Director of Clinical Nuclear Medicine, Director of NeuroPET Research, and Assistant Professor in the Department of Radiology at the Hospital of the University of Pennsylvania
Meditating nuns have decreased activity (yellow) in areas promoting a sense of self (e.g., ego)

Progress in psychoneuroimmunology Stress and the immune system Health behaviors and immune function Stress and wound healing Social support as a buffering factor Cancer incidence and metastasis Progress in cardiovascular physiology Stress and cardiovascular function Health behaviors and cardiovascular function
Mind/Body Connection Well Documented:

Do’s and Don’ts of Relaxation Techniques
Do Don’tWear comfortable, loose clothing and have proper back support
Put yourself in an awkward position or one that will make it easy to fall asleep
Allow your mind to quiet down. Let tense thoughts pass through like clouds going across the sky
Think your way into tension – let stressful thoughts pass through
Stay alert and conscious – focus on your breathing and the feelings in your body
Allow yourself to become groggy or sleepy – If you start to fall asleep, open your eyes, sit up and return to relaxation
Go at your own pace and let go of your muscles as your body decides to give up tension
Expect yourself to relax all at once – You must practice step by step
Give your body messages of appreciation for relaxing
Get down on yourself or be impatient
Stay aware of your breathing Smoke before, during or after relaxation – let your body breathe
Two Popular Relaxation Techniques:
Muscle-Tension Release Guided Imagery
1. Find a quiet place where you will not be interrupted.
2. Get comfortable – loose clothes, take off glasses, comfortable chair with your head supported.
3. Stretch and take a deep breath
4. Close your eyes.
5. Repeat the word “calm” (or one of your choosing) each time you exhale.
6. Breathe in through your nose, hold your breath to a slow count of 5, exhale through your mouth. Follow your breath with your mind.
7. Practice for about 15 minutes each day.
8. Begin to notice the difference in your body when it you are in a relaxed state vs. stressed state.

Change Physical Health Habits to Reduce Stress
Take 15-20 minutes each day to relax Get regular physical activity, such as walking or other exercise (exercise is a very powerful stress buster) Eat healthy, well-balanced meals Pray or meditate to strengthen your religious or spiritual side Get enough sleep Bring pleasure into your life with things you enjoy, such as visiting with friends, starting a hobby, reading, or listening to music
Smoke – If you do, quit, even if it takes several attempts to succeed Drink too much alcohol -- Alcohol does not reduce the effects of stress and may keep you from facing issues you should handle in better ways Drink too much coffee (or caffeine)—Coffee in small amounts seems harmless, but too much can make you feel nervous and tense Overeat, especially between meals—Try to replace "nervous eating" with a healthy habit such as relaxation, physical exercise, or pleasurable activities

1. Record the current frequency and typical circumstances of the behavior you want to change.
2. Set a realistic behavioral goal for yourself.
3. Initiate a planned strategy for change.
4. Reward yourself for succeeding.
5. Don’t give up if you fail to meet your goal.
Steps to Changing Health-Related Behaviors

Change the Situation to Reduce Stress
Get Involved! Individually and Collectively work toward
the implementation of the recommendations of Nursing’s Agenda for
the Future!
1. Collective Efforts
2. Personal Efforts
"Never doubt that a small group of thoughtful, committed people can change the world. Indeed, it is the only thing that
ever has." -- Margaret Mead

Improve workplace design and environmental conditions
Clearly define nurses’ roles and responsibilities
Ensure that the workload meets workers' capabilities and resources (e.g., adequate staffing) Design jobs to provide meaning, stimulation, and opportunities for workers to use their skills
Give staff opportunities to participate in decisions affecting their jobs
Make sure there are good communications between all sectors of the workplace Put clear career development plans into place and address any uncertainties about future employment prospects
Implement flexi-hours and other strategies that will help nurses balance work and home life
Get Involved!
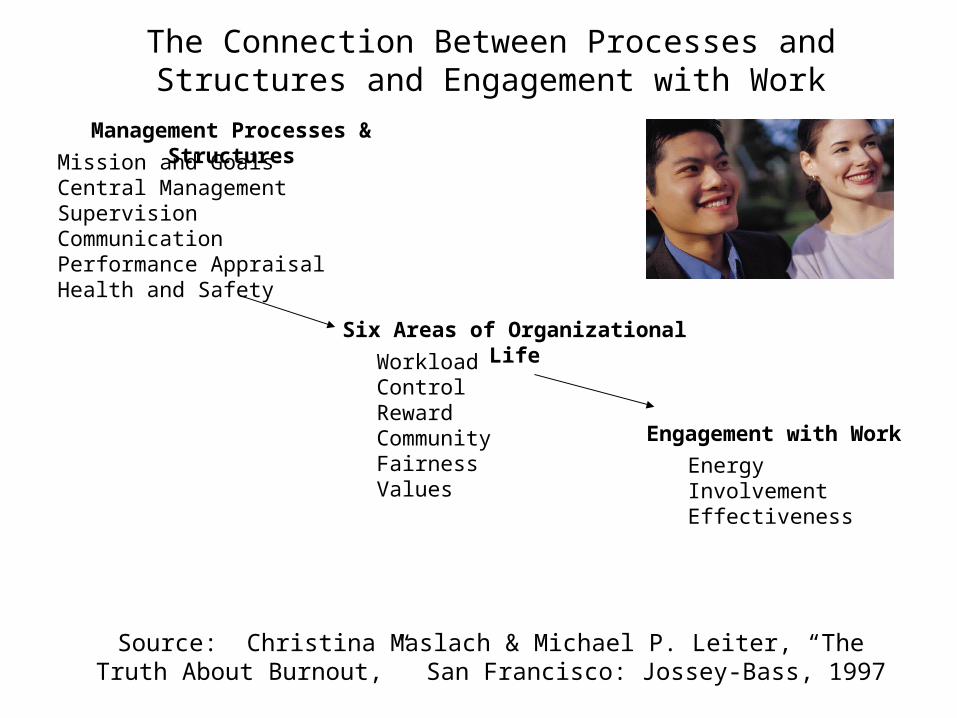
The Connection Between Processes and Structures and Engagement with Work
Source: Christina Maslach & Michael P. Leiter, “The Truth About Burnout,” San Francisco: Jossey-Bass, 1997
Management Processes & StructuresMission and Goals
Central ManagementSupervisionCommunicationPerformance AppraisalHealth and Safety
Six Areas of Organizational LifeWorkload
ControlRewardCommunityFairnessValues
Engagement with Work
EnergyInvolvementEffectiveness

Personal Approaches to Changing the Stressful Situation
Get clarification of your job responsibilities
Delegate when possible
Learn to say “no”
Transfer to another department or another supervisor
Suggest alternative solutions to your supervisor
Find another job
Find another profession
BRAINSTORM!

Personal Approaches to Changing the Stressful Situation
A powerful source of stress for many people – especially women – is the failure to express one’s feelings and, instead hold things in until they’re ready to pop.
This the “Volcano Syndrome.”

Assertiveness is the honest and clear expression of thoughts, feelings, and opinions that is respectful and does not violate the rights or dignity of another. In other words, Assertiveness is about standing up for yourself, believing in your opinions and your right to be heard and getting your needs met. But it is also about respecting the opinions and needs of others.
Assertiveness is a SKILL that can be learned and it reduces stress by allowing you to have greater control in interpersonal situations and set limits.
A Continuum

Passive Assertive Aggressive
Characteristics Allow others to choose for you. Emotionally dishonest. Indirect. Inhibited.
Choose for self. Appropriately honest. Direct. Self-Respecting.
Choose for others. Inappropriately honest (tactless). Direct.
Your Feelings Anxious. Ignored. Helpless. Manipulated.
Confident. Self-Respecting. Valued.
Righteous. Superior. Controlling.
Others’ Feelings
Guilty or superior. Frustrated with you.
Valued. Respected. Humiliated. Hurt. Defensive. Resentful.
Others’ View of You
Lack of respect. Distrust. Do not know where you stand.
Respect. Trust. Know where you stand.
Vengeful. Angry. Distrustful. Fearful.
Outcome Others achieve their goals at your expense. Your rights are violated.
Outcome determined by above-board negotiation. Your and others’ rights respected.
You achieve your goal at others’ expense. Your rights upheld; others violated.
Underlying Belief System
I should never make anyone uncomfortable or displeased…expect myself.
I have a responsibility to protect my own rights: I respect others but not necessarily their behavior.
I have to put others down to protect myself.
Comparison of Alternative Behavior Styles

Areas of Assertive Behavior
1. Setting limits (e.g., saying “no,” refusing requests)
2. Expressing negative feelings (e.g., delivery criticism, expressing angry feelings)
3. Expressing positive feelings (e.g., expressing compliments, expressing feelings of warmth or appreciation)
4. Initiating activities or conversations
Very few people are either always assertive or always non-assertive. There is a great deal of situational specificity – most people find it easy to be assertive in certain situations but not in other or all situations.

Components of Assertive Behavior
1. Verbal (what you are saying)
2. Non-Verbal (what your body is saying)
3. Affective (how you are feeling)
4. Cognitive (what you are thinking)
5. Listening (what are you hearing)
Assertiveness is not a series of short, unconnected responses, but rather an interpersonal style that allows the opportunity to express one’s own thoughts, feelings, and needs openly and clearly to other people in a way that is respectful. It results in clear, authentic communication as well as increasing self-confidence and self-esteem.
Verbal Component of Assertive Behavior
Empathy or Positive Statement (lets the other person know you experience empathy or note what they are doing right – NOT a self-deprecating statement)
Conflict Statement (what the problem is)
Action Statement (what you would like the other person to do)

Non-Verbal Component of Assertive Behavior
Eye contact
Posture
Facial expression
Voice characteristics (e.g., volume, tone, pitch)
Touching
Personal space
Hand gestures
Latency to respond (shorter = more assertive)
Duration of response (longer = more assertive)

Research shows that about 98% of what we communicate is non-verbal.
Very strong cultural differences in non-verbal communication.
We send confusing messages when there is a disconnect between verbal and non-verbal components of our communications.
The Duchenne smile, named after the researcher Guillaume Duchenne, who first described it. It is a genuine smile. The corners of the mouth curl up and the skin around the eyes crinkles in crow's feet like shape. The facial muscles involved in this expression are difficult to control voluntarily. Therefore, it's difficult to fake a Duchenne smile unless your smile from within.
The Pan American smile, named after the airline, is a perfunctory smile. It is nothing but a courtesy smile as in the case of a flight attendant responding to a patron. It's an expression of courtesy and politeness rather than inner joy. Alas, the Pan Am airline is dead but the smile will live forever.

Affective Component of Assertive Behavior
How are you feeling?
When people hesitate to make an assertive response, it is because of one of two reasons: 1) They don’t know what to do (skills deficit) 2) They feel uncomfortable doing so (anxiety inhibition)
The majority of people resist behaving assertively because they feel anxious or uncomfortable doing so, not because they don’t know what they “should” do.
Cognitive Component of Assertive Behavior
What are you thinking?
People high in assertiveness expect more positive outcomes.
People low in assertiveness across a variety of situations, often tell themselves all the negative things that will result if they behave assertively (e.g., my boss will fire me, my friend will dislike me).
“The Myth of the Good Friend.”
“The Myth of Modesty.”
Listening Component of Assertive Behavior
The active listener is reflective and empathic, in order that the sender may feel accepted and understood. The active listener is objective and nonjudgemental, to avoid clouding the issue with feelings of guilt and inferiority. By identifying the feelings being transmitted, the active listener is essentially telling the sender he/she is free to express his/her emotions. By clarifying the direction of these feelings, the active listener is promoting the problem-solving process.

Talk about your stress with a friend or therapist
Listen to others when they need an ear
Express your suffering/stress through art or ritual
Process
and the
Story of the
Chinese Potter
Express Yourself to Reduce Stress

“Humor is a prelude to faith and laughter is the beginning of prayer.”
-- Reinhold Niebuhr
Keep a Sense of Humor to Reduce Stress

Laughter Really Is the Best Medicine
Through the “reverse exhalation” capacity of the lungs, the physical contractions of laughter cause extra oxygen to enter the body, moving stagnant air and increasing the body’s blood oxygen level – This is aerobic, like “inner jogging.”
The muscle movement of laughter increases peripheral circulation – associated with the innervation of the parasympathetic nervous system and the “relaxation response.”
In many ways the breathing patterns of laughter are similar to those that naturally occur during meditation.
Laughter lowers serum cholesterol, reduces stress-related hormones, and increases virus killer cells, B-cells, and activated T lymphocytes – all of which improve immune system functioning and offset the immunosuppressive effects of stress.
Laughing releases endorphins – the body’s own natural opiates – which diminish both physical and emotional pain.

Time Management to Reduce Stress
Time management refers to actively structuring your time so that you avoid stress and maximize the likelihood of engaging in those activities that you view as important.
Organization is crucial.
Designating time that honors and reflects your priorities and values is critical.
Drop low value jobs/tasks.
Avoid distractions.
Create more time.

Not Enough Time?
Time-use studies show that leisure time from 1965 to 1985 actually increased by 5 hours per week.
The average American schedule has more than 40 hours a week that could be used to make deposits into our social capital account and the important connections in our life.
Question of priorities & values, not of time.

Make Values Personal
1. Identify Five (5) CORE VALUES that are both personal and professional.
2. List at least two BEHAVIORS that exemplify those values.
3. Close your eyes – meditate on the past two weeks of your personal and professional life.
4. Honestly appraise how often you act on your values.
5. Write down typical examples of when you live your values and when you don’t.
6. Discuss.

Values – Food for Thought:
Assertiveness Balance Caring Courage Courtesy
Commitment Compassion Confidence Creativity Consideration
Detachment Determination Enthusiasm Excellence Equality
Flexibility Faithfulness Forgiveness Friendliness Fairness
Gentleness Generosity Honor Humility Helpfulness
Honesty Idealism Innovation Integrity Independence
Inter-Dependence
Genuineness Empathy Joyfulness Justice
Kindness Love Loyalty Mercy Moderation
Knowledge Obedience Orderliness Modesty Patience
Peacefulness Prayerfulness Purposefulness Respect Responsibility
Risk-Taking Objectivity Quality Happiness Security
Self-Discipline Service Steadfastness Trust Truthfulness
Tolerance Harmony Wisdom Unity Self-Knowledge
Self-Esteem Wealth Fame Success Intimacy
Beauty Pleasure Excitement Contentment Teamwork
EXAMPLE
Value = BALANCE
Behaviors = 1. Eat a healthy dinner with my family at least four nights a
week.
2. Play tennis twice a week.
Evaluate = The Past Two Weeks.

Television: Time Stealer
Americans spend more hours alone in front of their TV sets (3-4 hours per day) than in any other activity except work & sleep
TV watching accounts for more than ½ of all leisure time activity
Heavy television watchers are more likely to be pessimistic, overestimate crime rates, and spend less time engaged with others
The only leisure time activity that is associated with decreased (rather than increased) social capital and connections
“The data suggest that most Americans would rather watch Friends than have friends.” – Robert Putnam, Bowling Alon
Longer work hours are associated with more (not less) civic engagement and connections (e.g., report 30% less TV)

In his book Love and Survival: The Scientific Basis for the Healing Power of Intimacy, physician Dean Ornish summarizes the power of connections this way: “I am not aware of any other factor in medicine – not diet, not smoking, not exercise, not stress, not genetics, not drugs, not surgery – that has a greater impact on our quality of life, incidence of illness, and premature death from all causes.”
Stay Connected to Reduce Stress

The Dark Side of Connection: Faulty Boundaries
Armor
Jell-O
Semi-Permeable Membranes

Be Aware that “Compassion Fatigue” Affects BodyMindSpirit
Some Symptoms of this “Care-Giving Shutdown” Fatigue
Joylessness
Pessimism
Social Withdrawal
Uninterested in intimacy or sex
Concentration Difficulties
Irritability
Depression
Physical Symptoms and Illness
Feeling like you’re “just going through the motions” – lack of passion or meaning
Negative Coping Behaviors – Substance Abuse, “Soft Addictions”

“Illumined Selfishness” – Healthy Self-Care Nurture BodyMindSpirit
Physical Regimen to Deal with Stress
Quiet Time for Reflection, Prayer, Meditation, Solitude
Creative Activities
Social Support – Talk About It!
Spiritual Support
Optimism
Humor
Approach NOT Avoidance
Cognitive Reframing
Caregivers often think we are the “Energizer Bunny” and can keep going and going and going – This is a dangerous belief!

Balanced Wellness
Physical Health
Intellectual Health
Spiritual Health
Emotional/Social Health

Work environment factors leading to burnout include:
role conflict ambiguity autonomy no opportunity to participate in decisions lack of control of one's job giving too much and not taking self-care
Individual personality characteristics of people at risk of suffering from burnout include:
young idealistic professionals who have unrealistic expectations about the work situation empathic people who pour too much of themselves into their job an individual's reaction to stress coupled with their stress-coping
mechanisms

The MBI-Human Services Survey (Maslach Burnout Inventory) measures burnout as it manifests itself in staff members in human services institutions and health care occupations such as nursing, social work, psychology, and ministry.
Emotional Exhaustion
Depersonalization
Personal Accomplishment
Subscales of Burnout Maslach Burnout Inventory
“Burnout is the index of dislocation between what people are and what they have to do, It represents an erosion in values, dignity, spirit, and will – an erosion
of the human soul.”

MBI-HSS: Twenty-two items written as statements answered on a 7-point scale.
Emotional Exhaustion Subscale:
I feel emotionally drained from my work.
Working with people all day is really a strain for me.
Frequency Patterns:
High Burnout – several times a month or more
Low Burnout – several times a year or less

Depersonalization subscale:
I’ve become more callous toward people since I took this job.
I worry that this job is hardening me emotionally.
Frequency Patterns:
High Burnout – once a month or more
Low Burnout – once or twice a year or less

Personal Accomplishment Subscale (reverse scoring):
In my work, I deal with emotional problems very calmly.
I feel I’m positively influencing other people’s lives through my work.
Frequency Patterns:
High Burnout – less than once a week
Low Burnout – several times a week or daily

Integration of Dualities
As in all dualities, the wise strive to “hold the tension of the opposites” to integrate and balance opposing forces as we allow ourselves to experience compassion for others AND for ourselves.
Become a Lake
“We are here to awaken from the illusion of our separateness.”
-- Thich Nhat Hanh, Vietnamese Buddhist Monk
“By our very natures, humans are prepared to be social animals. We are biologically and psychologically prepared for attachment and bonding. Our need for connection is – from birth and beyond – a fundamental survival need.”
-- Living a Connected Life
A Social Animal


Maslow’s Hierarchy of Needs

The Roseto Effect – 1950s
A small town in Pennsylvania – A close-knit community of Italian immigrants who lived longer lives than people in neighboring towns and were virtually free of heart disease.
Had they found the alchemical Elixir Vitae?
No! They had high levels of social cohesion, trust, and mutual respect. They were connected.
From 1979 to 1994, eight large-scale community-based studies confirmed what those early researchers found in Roseto.
Scientific StudiesFive decades of medical and epidemiological research has shown the powerful and positive effects of connections on:
Heart and cardiovascular disease
Stroke
Respiratory Diseases
Cancer
Allergies, Colds, and other Infectious Diseases
AIDS/HIV
Depression, Stress and other Psychological Problems
Interesting Gender Difference
When women are stressed – they move toward greater connection with other (“Tend and Befriend” rather than “Fight or Flight”)
Men under stress tend to “hole up”
Women respond to stress with a surge of brain chemicals (such as oxytocin) that buffer the “fight or flight” response, pushes them toward social contact, which releases more oxytocin which calms them further. Estrogen (a female hormone) has an enhancing effect on oxytocin whereas testosterone (a male hormone) reduces it.
Klein, Laura & Taylor, Shelley (UCLA Stress Research Lab), 2002

A Thousand Words For Snow

Assumptions for the Model
1. Everyone needs a variety of people and relationships in their lives
2. Relationships are not static; they change, as do our lives and needs.
3. Think of the “rings” in the model as semi-permeable membranes
4. It is the inner circle of relationships – those with whom we are connected by the heart – that constitute our “tribe” or true safety net. These are the containers that serve as our containers for emotional and spiritual growth
5. With the possible exception of our biological family, most relationships do not begin within this inner circle
6. Don’t mistake the “map” for the “territory” – life is really more complex than any model can describe
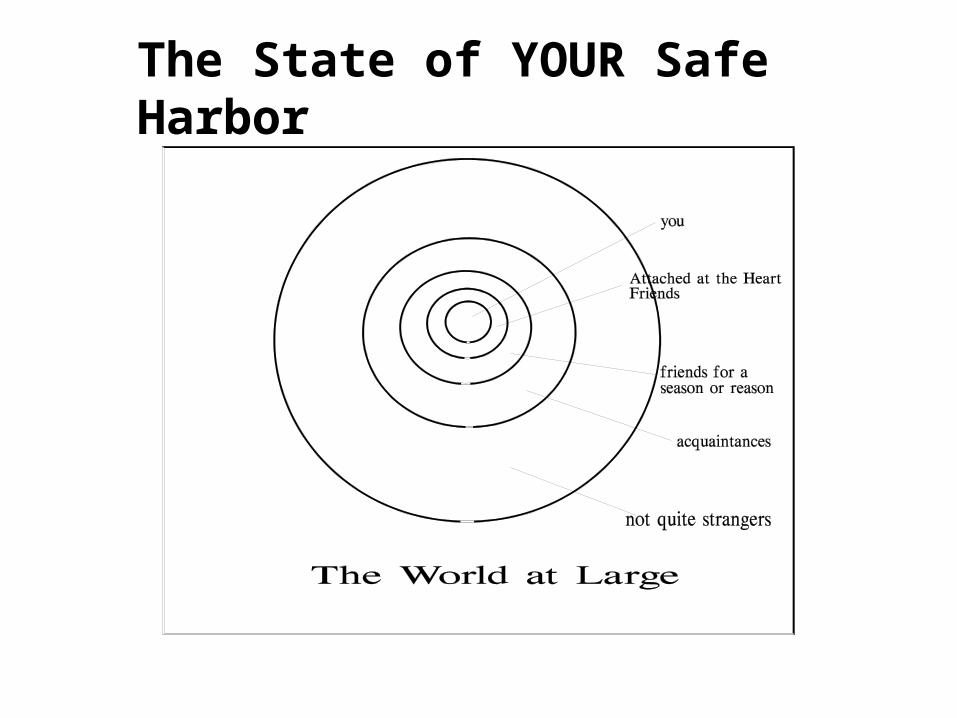
The State of YOUR Safe Harbor

Know Thyself You can’t have a better relationship with
anyone else than the one you have with yourself
What do you bring into your relationships?
How well do you know yourself?
The Persona and The Shadow
Emotional Intelligence (EQ)
“To know others is to be wise, to know oneself is to be enlightened” – Tao Te Ching

“If we really want to love, we must learn how to
forgive.” - Mother Theresa

Forgiveness: A Special Opportunity for Healing and Health Those who have studied it can tell you without qualification that
forgiveness is a sign of strength. Not only is it a very human quality, displays of forgiveness and reconciliation are common among monkeys, apes and other primates, and suggest this behavior has been around for over thirty million years. And research conducted at the University of Wisconsin in 1997 indicates forgiveness can be taught and with positive results.
On January 2, 1998, ABC News reported "studies show that letting go of anger and resentment can reduce the severity of heart disease and, in some cases, even prolong the lives of cancer patients."
Dr. Frederick DiBlasio of the University of Maryland is one of many family therapists successfully using forgiveness as a tool to reconcile couples when other techniques have proved ineffective.
Everett Worthington, Jr. who is a professor of Clinical Psychology at Virginia Commonwealth University and a pioneer in forgiveness research, has found that people who won't forgive the wrongs committed against them tend to have negative indicators of health and well-being: more stress-related disorders, lower immune-system function, and worse rates of cardiovascular disease than the population as a whole.
www.forgiving.org

Charlotte vanOyen Witvliet, PhD (assistant professor of psychology at Hope College in Holland, MI) is investigated the physiological effects of forgiveness and unforgiveness. Results demonstrated that unforgiving thoughts increase sympathetic nervous system arousal, heart rate, and blood pressure.
Porter Storey, MD, (medical director of the Hospice at the Texas Medical Center and a pain and symptom management consultant at the M.D. Anderson Cancer Center in Houston). “Forgiveness can dramatically improve a lot of parameters in patients much more effectively than expensive medications, and it has essentially no bad side effects." His focus is on forgiveness among terminally ill cancer patients. In the 20 years Dr. Storey has been caring for dying patients, he has noticed that those who are able to let go of past anger and hurt experience a dramatic reduction in anxiety and distress. This observation led him to begin investigating the ability of a counseling intervention to increase forgiveness as well as patients' sense of hope and overall quality of life.
Forgiveness has been shown to predict both physical and emotional health. This research confirms that association with self-reports of physical symptoms, number of medications used, quality of sleep, and several indices of psychological well-being (Kathleen Lawler, Ph.D.).

Forgiveness is something virtually all Americans aspire to -- 94% surveyed in a nationwide Gallup poll said it was important to forgive -- but it is not something we frequently offer. (In the same survey, only 48% said they usually tried to forgive others.)
"Everyone thinks forgiveness is a lovely idea, until they have something to forgive.” – C.S. Lewis

Self-forgiveness, which enables us to release our guilt and perfectionism.
Forgiveness we extend to others and receive from them, intimates and enemies alike.
Forgiveness of God that assures us of our worth and strengthens us for this practice.
Three kinds of forgiveness, all interrelated:

Awakening to the Ordinary Grace that Surrounds Us
It all depends upon how you start out!
Believing is Seeing.
What do you believe about the nature of humankind and grace itself?
What is your worldview?

Our Culture and Media Tend to Focus on What is Wrong with Humankind
“Good news is no news.”
“If it bleeds, it leads.”
Center for Media and Public Affairs – 2003 Year in Review of Top Television News Stories – Based on 11,834 stories broadcast on ABC,
NBC, CBS

Good-Natured
Binti-Jua and the Brookfield Zoo (IL)
August 16, 1996Binti-Jua is Swahili for “Daughter of
Sunshine”
Humans share 98.4% of our DNA with chimpanzees.
Bonobos and Compassion (Robert Yerkes, Frans de Waal,
etc.)

Is Empathy/Compassion Inborn in Human Beings?
Martin Hoffman’s (NYU) research shows that even day-old infants show remarkable empathy and will cry at the sound of
another infants’ crying.
Psychologist Carolyn Zahn-Waxler, Ph.D., et al (NIMH) observed children whose parents were hurt somehow - either physically (e.g., father had a bad headache) or emotionally (e.g., mother received bad news and was crying). They discovered that even very young children had a very well-developed sense of empathy. They reacted with concern, wanting to help or "fix" the problem, and they offered comfort and compassion to the parent who was hurt.

Rescuing Hug
Brielle and Kyrie Jackson – born 10/17/95 twelve weeks ahead of due date. Preemies were placed in separate incubators to reduce the risk of infection at The Medical Center of Central Massachusetts in Worcester.
Kyrie (born 2 pounds, 3 ounces) was doing well but Brielle(born 2 pounds) was failing. A compassionate and quick-thinking nurse, Gayle Kasparian. remembered that a common procedure in Europe was for double-bedding of multiple-birth babies. With the parents’ blessing, she placed Brielle in the incubator with Kyrie.
As soon as the door closed, Brielle snuggled up to Kyrie and calmed down. Within minutes Brielle’s blood-oxygen readings were the best they had been since her birth. As they dozed, Kyrie wrapped her tiny arm around her smaller sibling.
Sooner than expected, the twins went home from the hospital!

Empathy is a neurological phenomenon, says Thomas Lewis, M.D. (co-author A General Theory of Love). “Watching one in pain fires the same neurons fired when the one watching undergoes the same type of pain,” he said. This means that the brain empathizes with another by generating an internal model of that other. To put it simply, empathy at least partly relies upon neural modeling.
There are few professions that require expressions of love like the healthcare profession does. Medical caregivers possess immense potential for expressing love. Unfortunately, says Harvard University psychiatrist Gregory Fricchione, “physicians take very little time to express love through listening and spending time with patients.” Patients who face the challenges brought by separation from friends, family and familiarity need thelove of those in the medical fields, he said.
Fricchione pointed to research related to the role that the brain’s amygdala plays in patient stress and worry. “The amygdala continually sends signals related to fear and anxiety when the patient is told of their illness and its possible affects,” he said. However, he added, the nurture, compassion and social attachment provided by caregivers can significantly reduce the amygdala’s power to paralyze patients through fear.
Love and Medicine

Original Sin v Original Blessing (Matthew Fox)
“We are born originally pure.” (Dalai Lama)
“We have been loved since the beginning.” (Julian of Norwich – 15th Century Christian mystic)
“Among all the strange things that men have forgotten, the most universal and catastrophic lapse of memory is that by which they have forgotten that they are living on a star.” (G.K. Chesterton)
What We Believe Sets the Stage for Our Experience
We Determine What We Tune In To

Good and Evil
Are good and evil opposites or two sides of the same human coin?
The banality of evil (Hannah Arendt on Adolf Eichmann)
“There is a capacity of virtue in us, and there is a capacity of vice to make your blood creep.” (Ralph Waldo Emerson)
What does it mean to be human?

Amazing Grace Surrounds Us As Close as Our Next Breath
John Newton 1725-1807
John Newton was the captain of a slave ship. On May 10, 1748 on a homeward voyage, while he was attempting to steer his ship through a violent storm, he experienced what he was to refer to later as his “great deliverance.” He recorded in his journal that when all seemed lost and the ship would surely sink, he exclaimed, “Lord, have mercy upon us.” Later in his cabin he reflected on what he had said and began to believe that God had addressed him through the storm and that grace had begun to work for him. He returned to England, decided to become a minister, and applied to the Archbishop of York for ordination. He wrote hundreds of hymns, the best known of which is “Amazing Grace.”

All kinds of people demonstrated ordinary grace
Felt connections (never pity or sentimentality)
Faith in the goodness of others
To help others is a privilege, a blessing
Humor
Humbleness
Impulse to do good is immediate
Negatives into positives
What is it about some people who see ‘compassion’ as a verb?

Thank you for coming and Godspeed on your
journey.
Kathleen and co-author Dorothy
Kelly
www.fullpotentialliving.com
252-473-4004