organ transplantation in al amyloidosis...median overall survival on dialysis gertz et al. arch...
TRANSCRIPT
Organ transplantation in AL Amyloidosis
Andrea Havasi, MDBoston University
Renal Section

Disclosure of Conflict of Interest
I do not have a relationship with a for-profit and/or a not-for-profit organization to disclose


Renal Involvement in AL amyloidosis
• Over 70-78% of patients present with renal involvement
• Up to 40% require renal replacement therapy (RRT)
Gertz MA et al. Kidney Int. 2002. Gertz MA et al. Nephrol Dial Transplant. 2009. Havasi A et al. Am J Hematol. 2016.Palladini G et al. Blood. 2014.Sidiqi MH et al. Bone Marrow Transplant. 2019

Overall survival from diagnosis
Kyle RA et al. N Engl J Med 1997.
Gertz MA et al. Nephrol Dial Transplant. 2009.
Havasi A et al. Am J Hematol. 2016.
Palladini G et al. Blood. 2014.
Sidiqi MH et al. Bone Marrow Transplant. 2019
1990’s
• 12-18 months
Today
• HDM/SCT BU cohort with renal involvement: 8.2 years
• HDM/SCT Mayo cohort with or without renal involvement: 11.2 years
• All patients Pavia cohort: 3.9 years
• All patients Heidelberg cohort: 4.5 years

More patients with ESRD

Median overall survival on dialysis
Gertz et al. Arch Intern Med. 1992.
Havasi A et al. Am J Hematol. 2016.
Palladini G et al. Blood. 2014.
Sidiqi MH et al. Bone Marrow Transplant. 2019.
Batalini F at al. Biol Blood Marrow Transplant. 2018.
1990’s
• 8.2 months
Today
• 24-39 months; regardless of treatment modality
After starting dialysis mortality is mainly driven by
ESRD!!
(but OS 5.8 years if ESRD was reached before
HDM/SCT; 6% became dialysis-independent after
achieving CR and 33% had kidney transplantation)

Renal transplantation in AL amyloidosis??
• Concerns about recurrence in the graft
• Lack of data regarding overall survival and renal transplant outcomes
• No clear guidelines regarding renal transplant eligibility
Limited referral or acceptance
for renal transplantation
49 AL amyloidosis pts
Boston University
Amyloidosis Center
1987-2017
Median follow up
7.2 years
(0-19)
Angel-Korman A et al. KI. 2019.

Clinical features at diagnosis
Feature Median (range)
Age (years) 53.7 (26.4-73.8)
Gender Male: 82%
Race White 98%
Light chain clonalityLambda 61%
Kappa 37%
Creatinine 2 mg/dL (0.4-12)
eGFR 36 mL/min/1.73m2 (2-117)
Proteinuria 7.2 g/24 hr (0.1-42)
Organ involvementRenal only 20%, Cardiac 33%,
≥3 organs 43%
OS from diagnosis 15.4 years (1-20.7)
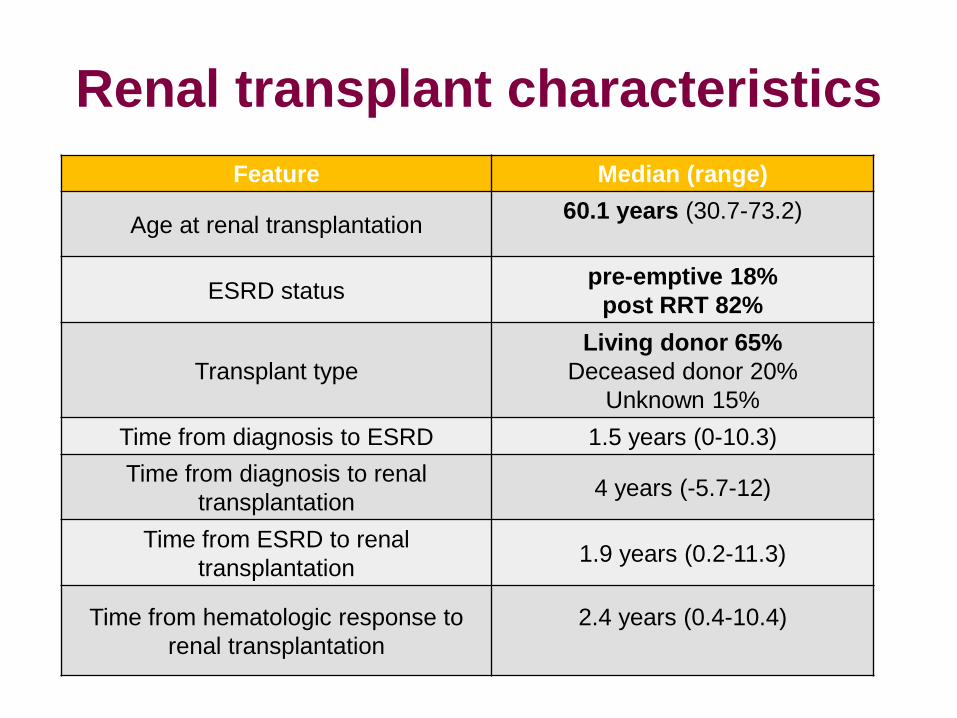
Renal transplant characteristics
Feature Median (range)
Age at renal transplantation60.1 years (30.7-73.2)
ESRD statuspre-emptive 18%
post RRT 82%
Transplant type
Living donor 65%
Deceased donor 20%
Unknown 15%
Time from diagnosis to ESRD 1.5 years (0-10.3)
Time from diagnosis to renal
transplantation4 years (-5.7-12)
Time from ESRD to renal
transplantation1.9 years (0.2-11.3)
Time from hematologic response to
renal transplantation
2.4 years (0.4-10.4)

Number of transplants per decade
Angel-Korman A et al. KI. 2019.

Overall survival after renal
transplant improved over the last
decade
OS from diagnosis OS from transplant
Angel-Korman A et al. KI. 2019.

Graft survival and recurrence rate
after renal transplant improved over
the last decade
Graft survival Recurrence in the graft
Angel-Korman A et al. KI. 2019.

Renal transplant outcomes –Overall survival
Angel-Korman A et al. KI. 2019.
USRDS
(cadaveric/
living)
(All
etiologies)
Our
cohort
(AL
only)
UK
National
amyloidosi
s center
2010
(AL only)
Mayo
clinic 2011
(AL only)
All types of
amyloid
patients
USRDS
2017
>65 yrs
(cadaveric/
living)
(All
etiologies)
DM
(cadaveric
/living)
(All
etiologies)
Number
of
patients
49 22 19 576
Overall
Survival
(years
from
renal Tx)
Media
nN/A
10.5
(1-20.3)
6.5
(0.2-13.3)
Not
reached5.8 N/A N/A
1 yr 97%/98.7% 96% 95% N/A 91% 94.2%/96% 96%/97%
3 yrs N/A 91% N/A N/A N/A 86%/89.5% 89%/93%
5 yrs 86%/93% 86% 67% N/A 70% 74%/82% 83%/87%

Renal transplant outcomes –Overall survival
Adapted from Angel-Korman A et al. KI. 2019.
USRDS
(cadaveric/
living)
(All
etiologies)
Our
cohort
(AL
only)
UK
National
amyloidosi
s center
2010
(AL only)
Mayo
clinic 2011
(AL only)
All types of
amyloid
patients
USRDS
2017
>65 yrs
(cadaveric/
living)
(All
etiologies)
DM
(cadaveric
/living)
(All
etiologies)
Number
of
patients
49 22 19 576
Overall
Survival
(years
from
renal Tx)
Media
nN/A
10.5
(1-20.3)
6.5
(0.2-13.3)
Not
reached5.8 N/A N/A
1 yr 97%/98.7% 96% 95% N/A 91% 94.2%/96% 96%/97%
3 yrs N/A 91% N/A N/A N/A 86%/89.5% 89%/93%
5 yrs 86%/93% 86% 67% N/A 70% 74%/82% 83%/87%

Renal transplant outcomes –Graft survival
USRDS
(cadaveric/
living)
(All etiologies)
Our
cohort
(AL
only)
UK National
amyloidosis
center 2010
(AL only)
Mayo clinic
2011
(AL only)
All types of
amyloid
patients
USRDS
2017
>65 yrs
(cadaveric
/living)
(All
etiologies)
DM
(cadaveric
/living)
(All
etiologies)
Number
of
patients
49 22 19 576
Median
Graft
Survival
(years)
9.1
6.9
(0.5-
18.8)
5.8Not
reached4.8
1 yrs 93.4%/97.2% 94% N/A (74%) N/A N/A/94% 92%/96%
3 yrs N/A 89% N/A N/A N/A N/A/87% 83%/88.5%
5 yrs 72.4%/84.6% 81% N/A (53%) N/A N/A/78% 73%/81.5%
Angel-Korman A et al. KI. 2019.

Renal transplant outcomes –Graft survival
USRDS
(cadaveric/
living)
(All etiologies)
Our
cohort
(AL
only)
UK National
amyloidosis
center 2010
(AL only)
Mayo clinic
2011
(AL only)
All types of
amyloid
patients
USRDS
2017
>65 yrs
(cadaveric
/living)
(All
etiologies)
DM
(cadaveric
/living)
(All
etiologies)
Number
of
patients
49 22 19 576
Median
Graft
Survival
(years)
9.1
6.9
(0.5-
18.8)
5.8Not
reached4.8
1 yrs 93.4%/97.2% 94% N/A (74%) N/A N/A/94% 92%/96%
3 yrs N/A 89% N/A N/A N/A N/A/87% 83%/88.5%
5 yrs 72.4%/84.6% 81% N/A (53%) N/A N/A/78% 73%/81.5%
Angel-Korman A et al. KI. 2019.

Eligibility criteria for renal
transplantation?

Overall survival from diagnosis:CR/VGPR vs PR/NR
Median OS:
17.9 y vs 9.7 y
Angel-Korman A et al. KI. 2019.

Overall survival from renal transplant:
CR/VGPR vs PR/NR
Median OS:
11.7 y vs 7 y
Angel-Korman A et al. KI. 2019.

Graft survival:CR/VGPR vs PR/NR
Median time to
graft loss:
10.4 y vs 5.5 y
Angel-Korman A et al. KI. 2019.

Recurrence of amyloid in the graft
• 14 pts (29%) had recurrent amyloidosis in the graft
• Median time from renal transplantation to
recurrence: 3.7 years (range 1.1-11.9)
• 20 pts received treatment for hematologic relapse:
graft survival was not different from the pts without
relapse (6.9 vs 8.3 years, p=0.35)
• 4 pts lost the graft due to amyloidosis
• 10 pts were successfully treated
• 6 pts HDM/SCT >>> VGPR or CR
Angel-Korman A et al. KI. 2019.

Lower recurrence in the graft in CR/VGPR
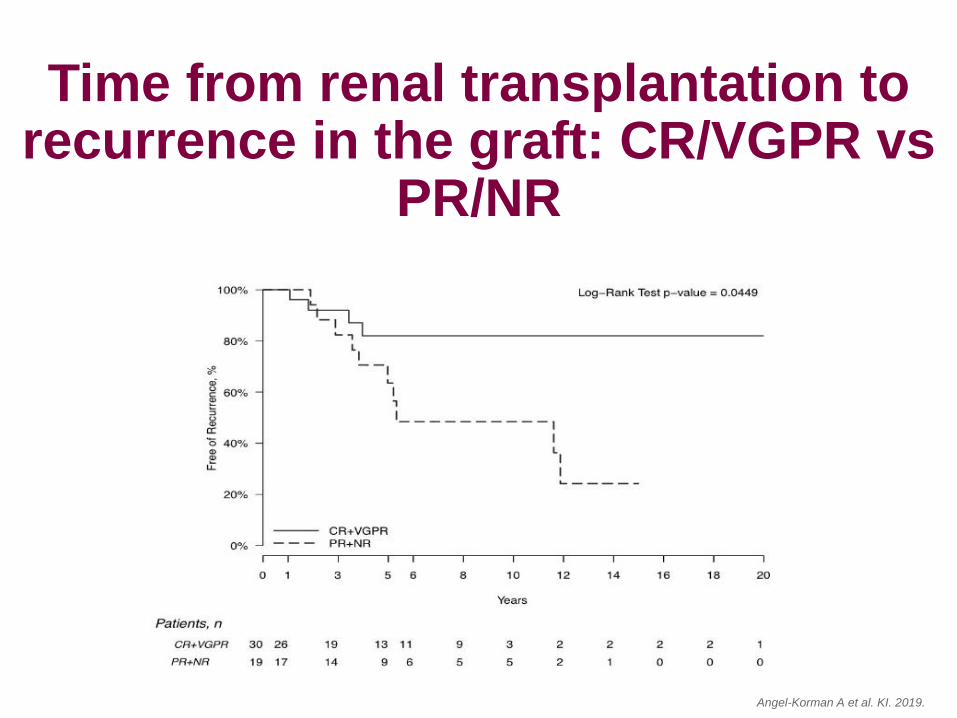
Time from renal transplantation to recurrence in the graft: CR/VGPR vs
PR/NR
Angel-Korman A et al. KI. 2019.

Cause of death # of pts
Progressive amyloidosis 10/23
Renal failure 2
Treatment related 2
Sepsis 2
Heart failure (non-AL) 1
Surgical complication (unrelated) 1
CVA 1
Unknown 4
Cause of death in kidney transplant recipients
Angel-Korman A et al. KI. 2019.
No difference in OS and graft survival
• HDM/SCT vs. chemotherapy (39 vs 10 pts)
• Hematologic relapse vs no relapse (20 vs 29 pts)
• HDM/SCT before vs after renal transplantation (33
vs 6 pts)
• Living vs. cadaveric
• Pre-emptive
• Number of organs involved
• Cardiac involvement at the time of diagnosis
• κ vs λ
What does not seem to change renal
transplant outcome?

• Standard therapies
• No change in regimen while getting treatment for
AL amyloidosis
• During SCT: mycophenolate on hold
• Only 4 acute rejections
Immunosuppressive regimens
• 4 y (range -5.7-12) from diagnosis
• 1.9 y (range 0.2-11.3) from ESRD
• 2.4 y (range 0.4-10.4) from hematological response
Why?
• The time it requires to go through the transplant
evaluation (both recipient and donor, if available)
• Wait time on the cadaveric transplant list
• Patients’ preference regarding the timing of
transplantation
Timing of renal transplantation

Wait 6-12 months post hematologic response
to document the durability of response and to
recover from therapy related toxicities
Timing of renal transplantation
Our recommendation

Limitations
• Small sample size
• Mostly white (98%) perhaps representing under-diagnosis of amyloidosis in other races or ethnicities
• Retrospective study
• The choice of treatment, the timing of treatment and renal transplantation were physician and patient dependent >>>>> selection bias

Heart transplantation in AL
amyloidosis

• Mayo Clinic; 1992-2011; 23 pts; median age 53
• OS: 3.5 years (95%CI: 1.2-8.2)
• OS in CR (=7 pts) in response to chemoth or
HDM/SCT: 10.8 years
• Survival is better in pts with limited extra-cardiac
involvement
• 5-year survival 43% vs 85% for non-amyloid
• Eight patients had rejection at a median of 1.8
months post OHT (range 0.4 to 4.9 mo)
What did we learn from heart transplants?
Grogan M at al. World J Transplant. 2016.
Gray Gilstrap L at al. J Heart Lung Transplant. 2014.

Grogan M at al. World J Transplant. 2016.
Cause of death # of pts
Progressive amyloidosis 12/20
Complications of HDM/SCT 3
Post-transplant lymphoproliferative disorder 2
Acute rejection 1
Cardiac vasculopathy 1
Metastatic melanoma 1
Myelodysplastic syndrome 1
Unknown 1
Cause of death in heart transplant recipients

• MGH/BU; 2000-2011
• 18 pts
• median age 56
• OHT followed by HDM/SCT
• OS similar to non-amyloid, restrictive (p = 0.34),
non-amyloid dilated (p = 0.34), or all non-amyloid
cardiomyopathy patients (p = 0.22) in the SRTR
database
What did we learn from heart transplants?
Dey BR at al. Transplantation. 2010.

Disease-free survival of heart
transplant recipients
0
0.2
0.4
0.6
0.8
1
0 20 40 60 80 100
■MGH/BU♦Hosenpud
Dis
ease
-fre
e S
urv
ival
P=0.04
Hosenpud JD at al. Circulation 1991.
Dey BR at al. Transplantation. 2010.
• Survival is better in pts with limited extra-cardiac
involvement, s/p HDM/SCT and CR
• More rejection episodes
What did we learn from heart transplants?

• Kidney transplantation can have a good outcome in carefully selected AL amyloidosis patients
• Recurrence of disease can still be managed without leading to graft loss
• Peri-transplant and post-transplant management require a multidisciplinary approach involving nephrologists, transplant surgeons and hematologists with experience in the treatment of this rare disease
Summary
Summary
We recommend consideration of renal
transplantation for those patients who
achieved CR or VGPR

• Should dialysis-dependent pts without extra-renal
amyloidosis receive chemotherapy while on dialysis
for the sole purpose of achieving a clonal response
to allow listing or undergo renal transplantation
followed by chemotherapy/SCT to prevent ongoing
amyloid deposition and disease recurrence in the
graft?
• Renal transplantation while being actively treated?
• Larger cohort?
Further questions

ACKNOLEDGMENTS
• The McCaleb Award from the Amyloidosis Center, Boston University School of Medicine, Alan and Sandra Gerry Amyloid Research Laboratory
• NIH/NIDDK/K08
• The Renal Section, Boston Medical Center
