original: english healthy aging
TRANSCRIPT

W E L T G E S U N D H E IT S O R G A N IS A T IO N REGIONALBURO FOR EUROPA
W O R L D HEALTH ORGANIZATIONREGI ONAL O F F I C E F O R E U R O P E
B C E M H P H A f l 0 P T A H H 3 A U H ^ 3 H P A B 0 0 X P A H E H 11 a EBPOflEHCKOE PErHOHAJIbHOE BIOPO
ORGANISATION MONDIALE DE LA SANTEB U R E A U R E G I O N A L DE L ’ E U R O P E
REGIO NAL C O M M I T T E E F O R E U R O P E
R E G I O N A L K O M I T E E F U R E U R O P A
C O M I T E R E G I O N A L DE L ’E U R O P E
E B P O F I E H C K H H P E r H O H A J I b H b l H K O M H T E T
Fortieth SessionCopenhagen, 10-15 September 1990
Technical Discussions
EUR/RC40/Tech.Disc./l0621B11 June 1990 ORIGINAL: ENGLISH
HEALTHY AGING
Health for all by the year 2000 - at global, regional and national levels, is the most challenging health policy ever set by the Member States of WHO. Any approach towards attaining this far-reaching goal must examine the ways in which factors in society and the environment affect people's health - including the health of elderly people.
A policy for health for all will need to have positive health built up in new ways and in new settings, by new combinations of people, in addition to the methods and means used in the past. Healthy aging should not, and indeed cannot, develop as a separate entity: it must be fully integrated into this overall approach.

TARGET 2
Adding life to years
By the year 2000, people should have the basic opportunity to develop and use their health potential to live socially and economically fulfilling lives.
This target could be achieved if health policies in Member States gave a framework for developing, implementing and monitoring programmes that provide the environmental conditions, social support and services required to develop and use each person's health potential.*
a Targets for health for a l l . Copenhagen, WHO Regional Office for Europe, 1985 (European Health for All Series, No. 1).

CONTENTS
1. Introduction ................................................................. 1
2. The process of a g i n g ........................................................ 3
2.1 A challenging process ................................................. 32.2 Development and decline of the organism ........................... 32.3 Intervention in gerontology ......................................... 52.4 The multidimensional nature of the aging process................. 62.5 WHO's global research programme on aging ........................ 6
3. Environmental conditions, social support and services related tohealth status in the aging process ....................................... 7
3.1 Life after sixty: a new b e g i n n i n g ................................ 73.2 Health and health maintenance ....................................... 83.3 Illness or i m p a i r m e n t ................................................. 103.4 Change of function (physical or mental) ........................... 113.5 Change of a u t o n o m y ................................................... 133.6 M o r t a l i t y ............................................................... 143.7 Aging: a challenge to a l l ......................................... 15
4. C o n c l u s i o n s ................................................................. 15
4.1 The present status of elderly people in Europe ................. 154.2 Major problems to be a d d r e s s e d .................................... 164.3 Prospects and policy for the f u t u r e ............................... 16
R e f e r e n c e s ........................................................................ 17
Annex 1 Fact-sheet on a g i n g ................................................... 19Annex 2 Healthy aging - d e m o g r a p h y ......................................... 23
g a g e

EUR/RC40/Tech.Disc. /I0621Bpage 1
According to the WHO concept of health as a state of physical, mental and social wellbeing, and not merely the absence of disease and disability, health is a positive condition which involves the whole person throughout his or her life span. The implication of this positive and relative concept of health is that all people, whatever their circumstances or age, can achieve wellbeing by making full use of their existing capabilities. However, most health programmes have focused on disease as a biological deviation from the norm, rather than on the full range of health and relative health as a positive value.
Health for all thus requires the creation of mechanisms that promote the health capabilities of all people and the removal of barriers that may prevent use of the available potential. It also requires the enhancement of people's awareness of health as an important resource for leading a satisfying life and the development of attitudes and skills to enable them to make full use of their health capabilities, whether whole or residual, to enjoy life.
Certain population groups may sometimes be denied viable opportunities to use their capabilities, so that handicaps or functional limitations may actually result from the lack of such opportunities. This is a situation often faced by old people.
Although reduced functional capacity is correlated with advancing age, it is not clear what percentage of the reduced function is due to preventable loss of fitness and/or of social contacts. Most aging people do not show symptoms of mental or physical decline; on the contrary, they tend to enjoy a level of health which permits them to continue to lead socially and economically active lives. But a sometimes serious problem arises from the fact that an increasing proportion of old people live alone and in isolation. In many cases these elderly people need to have their somewhat reduced abilities stimulated, as well as to be given opportunities of using them. In other words, society should help the elderly to face aging as a new challenge for their later years, so as to make their aging process as healthy as possible (1).
Most people are aware that aging brings many and sometimes frequent changes, but not all recognize these changes as challenges. At all times, the science and art of living are a masterwork of wisdom acquired, but for many it is these last chapters of life which can be the most demanding and which call upon mental and spiritual resources as well as physical reserves.
Great and famous names are cited as examples of those who have made their last decades some of their best: from Confucius to Churchill and from Michelangelo to Picasso. But the other side of the coin shows thousands of elderly people with increasing physical infirmity, reduced mobility and little useful engagement in active enjoyable living. How much of this can be prevented? And must the former lead inevitably to the latter? Is it possible for the process of aging to be a process of growth, of developing new potential in all those with chronic illness or pain as well as in persons in good health? What of the aged who experience episodes of acute illness? Can they be restored to as good a state of wellbeing as before, if not better?For generations and in the majority of cultures, women have been the main carers of the old as well as of the young. But what if they themselves are
1. Introduction

EUR/RC40/Tech.Disc./I0621Bpage 2
elderly? Who cares for them? How can they be helped, not only to cope but also to pursue their own interests and maintain their own health?
WHO's interest in these and other relevant issues goes back to 1955. But it was only in 1974 that an expert committee's report on the planning and organization of geriatric services was published. In the next few years, it became clear that immediate action in favour of the elderly was called for.In 1980, a conference held in Mexico City examined the present and future status of the elderly. The report of that conference served as the basis for a policy paper prepared by WHO for the 1982 World Assembly on Aging, convened by the United Nations. And, in turn, the International Plan of Action on Aging endorsed by that Assembly became the framework for WHO activities between 1982 and 1987 (2).
At the thirtieth session of the WHO Regional Committee for Europe in Fez, in 1980, representatives of Member States of the European Region of WHO approved their first common health policy, the European strategy for attaining health for all. The strategy called for the formulation of specific regional targets to support its implementation. Although no target cites the elderly per s e , reference to this important and increasingly large group of each country's population is implicit throughout the 38 regional targets adopted in 1984. It was realized that if health for all was to be reached in Europe by the year 2000, two basic issues had to be tackled. In the "target book" (3) the first issue is described as being "to reduce health inequalities among countries and among groups within countries". This statement is then amplified:
All the people of the Region should be assured an equal opportunity to develop, maintain and use their health. Particular efforts should therefore be made to provide such an opportunity for those countries, groups and individuals who lack it most. The second issue is to strengthen health as much as to reduce disease and its consequences.Thus, health for all in Europe has four dimensions as regards health outcomes, involving action to:
- ensure equity in health, by reducing the present gap in health status between countries and groups within countries;
- add life to years, by ensuring the full development and use of people's integral or residual physical and mental capacity to derive full benefit from and to cope with life in a healthy way;
- add health to life, by reducing disease and disability;
- add years to life, by reducing premature deaths, and thereby increasing life expectancy."
Obviously each of these dimensions is pertinent to the subject of healthy aging.
The technical discussions at the fortieth session of the Regional Committee represent the first stage of an in-depth debate with Member States on an action plan to achieve the goal of "healthy aging"; this plan will be submitted to the Regional Committee in 1991 and - it is hoped - accepted at a major conference the following year. The latter is intended both to mark
EUR/RC40/Tech.Disc./I0621Bpage 3
WHO's contribution to the tenth anniversary of the adoption of the International Plan of Action on Aging and, more importantly, to provide Member States with a framework for drawing up comprehensive national policies that will result in innovative action for healthy aging throughout the Region.
2. The process of aging
2.1 A challenging process
What is healthy aging? What is "normal" aging?
The process of aging is one which many generations and most cultures have fought against, making use of a variety of substances ranging from ginseng to Guinness, from oysters to royal jelly and employing a multitude of practitioners from beauticians to cosmetic surgeons. Since the time of Hippocrates (460-377 BC) hundreds of theories have been put forward to explain the process, and an even larger number of ways of combating it have been described. To date there is no known evidence that any substance or technique can slow down the process.
Aging is a complex process of natural biological evolution of the whole body; for most human beings, it also raises emotional and psychological issues. Scientifically, because of its highly complex nature, it is one of the most challenging unresolved problems in biology. Emotionally, aging has a strong impact on most people because of the many deteriorations in physical appearance and body functions. The social and political implications of an aging planet have caused concern among many policy-makers, and in recent years this has resulted in better funding for research into the process (in the United States through the National Institute of Aging and in Europe through the EEC-supported European Federation for the Welfare of the Elderly).However, biotechnology has not yet met the prevailing scientific, social and clinical needs for products to halt or reverse the aging process.
From the scientific point of view, the possibility of experimentally modulating the aging process could be a useful approach to understanding its molecular mechanisms; socially, products to combat the signs of old age will continue to be in demand until pressures against "looking old" disappear; while in clinical terms aging is manifested in a large number of age-related diseases and syndromes, which, if healthy aging is to be achieved, need to be cured or prevented.
2.2 Development and decline of the organism
The human body maintains itself from inception through'maturation and reproduction, but then progressive deterioration occurs with an ever-increasing probability of death. The last phase in this process is called "aging".
Critical discussion of the biology of aging appears to have its origins in the writings of August Weismann over a century ago. Since then, significant progress has been made in the study of age-related changes at all levels of organization - biochemical at cellular level, and in physiological tissues and organs. One major principle which has emerged is that, functionally, almost all biological systems fail progressively with advancing age. Taken in isolation, not every single component may exhaust itself

EUR/RC40/Tech.Disc./I0621Bpage 4
functionally, but it is the mutual interactions of individual components to maintain the body that determine its survival.
In recent years numerous attempts have been made to intervene in the aging process of human beings, but where any effect has been achieved it has been local and short-lived. There has been no demonstrable effect on the process per se (4). However, it is hoped that recent developments in the understanding of molecular mechanisms of repair, maintenance and fidelity of information transfer may open up new approaches to modulation of the process. All aspects are closely linked to the crucial step of protein synthesis, the rate of which decreases with aging. It is believed that if methods can be found to maintain or to restore this rate, they could, in turn, lead to maintenance of the efficiency of the various repair mechanisms. The search for such methods would involve a wide range of techniques already in use in biotechnology - such as cloning and altering genes for the various gene products which are involved in repair and maintenance systems. These include enzymes for DNA repair and free radical scavenging systems; various components of protein synthetic machinery which are known to become inefficient or defective in old cells; and cell surface receptors which, with aging, lose their capacity to respond. Gerontologists hope to find means either of maintaining physical, biochemical or molecular youthfulness for a longer period or of delaying its decline or bringing about some reversal if it has already taken place.
In practical terms, this means avoiding, curing and alleviating the various age-related diseases which at present are costly in human, social and financial terms (Fig. 1)(4).
Fig. 1. Some age-related health problems
Atherosclerosis Autoimmune diseasesCerebrovascular and cardiovascular diseasesCataractCancersChronic renal failureDelayed wound and fracture healingDisruption of sleep/wakefulness and other biorhythms Increased susceptibility to infections HypothermiaIncreased adverse drug reactionsOsteoarthritisOsteoporosisParkinson's diseaseReduced absorption of nutrientsSenile dementia of Alzheimer's typeSenile diabetesSlower protein synthesis and turnover Slower metabolic clearance of drugsStructural and physiological impairments of the skin Urinary incontinence

EUR/RC40/Tech.Disc./l0621Bpage 5
Correcting the prevailing negative picture of age is necessary since fundamental psychological research has demonstrated that under certain conditions (such as the development of skills and abilities, and a stimulating environment) aging need not necessarily signify decline, and degenerative processes can be slowed down. It has also been shown that many degenerative phenomena should not be regarded as biologically conditioned and thus irreversible. The mere knowledge that there is flexibility in the aging process itself makes intervention measures meaningful.
Differential gerontology, based on evidence that the aging process can take different forms in different individuals in different phases of life, implies that standard intervention measures (or rehabilitation measures understood as "general remedial therapy") are no longer applicable. Rather it stresses the need for specific analysis of the individual personality and situation, prior to establishing an intervention programme.
It is vitally necessary to identify and take note of the patterns of aging as they vary from individual to individual. Such patterns are determined by the combined effect of a multitude of factors in what should be seen as part of a process of mutual interplay. Data from longitudinal surveys have shown that the type and development of the aging processes are determined by previous experiences. In other words, they are biographically conditioned. Situational factors, such as current life circumstances (e.g. accommodation, health status, economic and family conditions) are also crucial. The goals and values pursued by the individual also influence the process.
Aging has been described as a fate determined in various ways - although "fate" in this context does not signify something to be accepted passively: it is an evolution to be mastered and coped with at various levels. While aging is first and foremost a biological fate, it is also a social fate. The image of age in society and the role expectations of the social environment are as influential as biological factors in determining an individual's aging process. Biographical aspects, for example, are evident in relation to social isolation. Those who from an early age have a gregarious personality are more rarely termed "lonely" in later age. Naturally, specific conditions (e.g. widowhood, immobility) have a modifying effect on this phenomenon.
Aging is also a financial and economic fate, as is often demonstrated in the case of single or widowed women. It is in old age particularly that the financial situation hows its effect on the opportunity (or lack of opportunity) for cultivating social contacts, enjoying a wide range of stimulating leisure and intellectual activities and taking care of appearance, thus providing a positive self-image. Obviously, aging is also a historically determined fate, and since the early 1970s it has been shown to be an ecological fate too. It is now regarded as an established fact that the environment - at both micro and macro levels (i.e. from the layout and furnishings of a single room to nearby traffic or the surrounding countryside) - also has an influence on the aging process. For certain population groups (notably the lower socioeconomic groups and women) it is the environment which is responsible for worsening their situation. It can reduce the scope of activity, both geographically and socially, and hence cause a decline in the psychological strengths of the individual. In such circumstances intervention measures are urgently needed.
2.3 Intervention in gerontology

EUR/RC40/Tech.Disc./I0621Bpage 6
In view of the multiplicity of influences, it is clear that any intervention must be based on all the relevant information; it is therefore essential for a detailed analysis to be made of each individual situation and its cognitive representation. Only when this has been done can the scope and nature of a possible intervention programme be discussed (5).
2.4 The multidimensional nature of the aging process
Aging is seen as a process, taking place simultaneously in several dimensions, whereby an individual changes from one state to another. These dimensions may be labelled "health", "social", "economic", etc. Each may be divided into several components such as employment, income security, housing, education, social welfare, the family and so on.
The three main dimensions are neither independent nor mutually exclusive, of course, and movement between states in one dimension may precipitate, prevent, delay or even reverse transitions in the same or other dimensions. Thus, a transition from one particular economic state to another (e.g. loss or reduction of income due to retirement) or from one social situation to another (e.g. providing 24-hour care to an aged spouse just discharged from hospital) can and unfortunately often does lead to a changed health status. Similarly, a change in the latter can affect the social and/or economic dimensions of the aging process.
An elderly individual may pass through a series of states which deviate from health: from a dysfunctional state, possibly due to a degenerative or chronic condition, through physical or mental disability (resulting in restricted ability for self-care and increased dependence on others) to, finally, death. Obviously, transition through all possible states does not always occur and, with the exception of the ultimate state, changes can also take place in both directions. It is for this reason that regular assessments of the individual's social circumstances and environment are essential, if services are to be appropriate to each state experienced.
Thus the goals of policies and programmes for healthy aging are to prevent or delay transition from health to morbidity, or to promote improved function. For an elderly person already suffering from an illness or impairment, or compensating for a lifelong disablement from which a return to a healthy or unimpaired state is not feasible, the goal may be to prevent or delay that loss of function which would decrease his or her autonomy. For people with physical or mental dependency, the goal would be to return to an independent state or to prevent progression to a state of increased dependency. Thus services are geared to assisting and encouraging people to develop to the utmost their own potential for successful coping, by summoning latent resources and reserves.
2.5 W H O’s global research programme on aging
The Organization has realized that more knowledge is needed in order to understand the determinants of healthy aging, and that appropriate technologies are required to apply such knowledge to the best effect with a view to formulating, implementing and evaluating relevant policies and programmes. In May 1987, therefore, the World Health Assembly, acting on the recommendations of the Advisory Committee on Health Research, adopted resolution WHA40.29 requesting the Director-General to establish an

EUR/RC40/Tech.Disc./I0621Bpage 7
international research programme on aging, as an integral part of the Organization's programme on Health of the Elderly. This move also represents a positive response to the objectives and recommendations of the International Plan of Action on Aging. Subsequently, the Advisory Committee on Health Research identified the following objectives for the research programme:
to better understand the basic process of aging;
to find ways to prevent and control the clinical manifestations of age-related disorders; and
to ensure interaction between older persons and society and increase the opportunity, motivation, and support of older people to contribute productively to society.
The Committee also recommended the following initial priority areas for the programme:
- determinants of healthy aging;
- age-associated dementias;
- age-related changes in immune function; and
- nutritional changes associated with aging, with special emphasis on osteoporosis.
It is believed that the information generated by these proposed studies will add a new and vital dimension to world knowledge which is of direct relevance to the formulation of national plans of action for healthy aging (6).
3. Environmental conditions, social support and services related to health status in the aging process
3.1 Life after sixty: a new beginning
Retirement is a phenomenon of our times. In pre-industrial society there was always work for old people to do. The elderly had functions to perform, were considered useful right up to their demise, were taken notice of and were respected. That situation has changed. When there was no age-determined limit on working, there was no social devaluation of the elderly. Welfare services such as pension plans, originally well intentioned, have contributed to the loss of prestige of the older generation as a whole and have cultivated the false assumption that age signifies decline, helplessness and need.
Faculties which are not used atrophy. And the feeling of "no longer being used" leads to dissatisfaction and complicates the aging process. The feeling of "being useful", on the other hand, is a guarantee of wellbeing in old age, as many studies have shown.
The end of a working life can be a blessing to one person and a curse to another, depending on the importance given to the job, the person's state of health, and his or her family situation, leisure interests and financial situation. But it is also clear that the quality of life in old age depends upon adjusting attitudes to our own age, to our life in old age and to old

EUR/RC40/Tech.Disc./I0621Bpage 8
people in our society. Entry into retirement does not mean exit from society. Scientists of all disciplines, people working with aged people, politicians of all persuasions, trade unions and representatives of the older generation itself, need to work together to improve the quality of life in old age by developing, maintaining and promoting activity (7).
Unfortunately, however, today’s society regards the older person as one who gives a declining performance, losing competence, skills and abilities as years are gained. It sees the elderly as a homogenous group, almost exclusively passive, needy and dependent. Old people are thought of as takers and recipients (of pensions and welfare services), rarely as givers and helpers, and this in spite of research findings which show that nine out of ten people from 60 to 70 years old require no assistance whatsoever, and that seven out of ten people in the age group 70 to 80 years and even four out of ten people over 80 years succeed in coping with everyday life without the slightest assistance. A high level of competence in the elderly is therefore not merely a desirable aim, it is a reality (8).
It is the responsibility of society, as well as of each individual, to determine whether the extra years gained through increasing longevity are genuinely experienced as "years gained", or as "years lost". Should not the experience, knowledge and skills of the elderly be harnessed to help with policy-making? Should they not be involved in local and national policies helping to decide our future? (8).
Of course new activities should not be imposed. Each elderly person must seek out new areas of activity for himself or herself. Society is responsible for supporting such efforts, providing appropriate opportunities and facilities and using the expertise they have developed.
Some elderly people may take university courses, undertake educational travel to other countries, acquire a new language or refresh or develop new skills in the arts. Sporting activities and meetings with like-minded neighbours contribute to wellbeing and integration and make it possible to experience aging as an opportunity to gain skills. Looking back over "a life lived to the full", on duties and responsibilities successfully discharged and on crises successfully surmounted, also contributes to the positive experience of age. In surveys conducted in the Federal Republic of Germany, people have frequently observed that a sorrow which 50 or more years previously had "almost broken" them, had, in fact, enriched their lives (8).
Hans Thomae has remarked, on the subject of competent aging, that aging in the positive sense of maturing is successful when the many disappointments and privations which life metes out to the individual in old age do not lead to an accumulation of resentment, aggression and resignation, but when the realization of the many limitations on one's abilities enables one to develop the art of turning any situation and all its inherent potential to advantage(9). That must surely be the prime aim of all individuals in their attempts to achieve "healthy aging".
3.2 Health and health maintenance
One of the indicators used in programmes on the health care of the elderly is the measurement of self-perception of health status. In addition to clinically observable and definable diseases, a further measure of people's

EUR/RC40/Tech.Disc./I0621Bpage 9
health status is to ask how they themselves rate, or perceive, their own health. This measurement of health is often called subjective assessment, whereas clinical examinations are considered to provide an objective evaluation.
Despite the high prevalence of clinically definable diseases, it has been found that a large proportion of the elderly rate their health as good. The criteria people use for rating their own health are not clear, but it has been suggested that there is a general tendency for health aspirations to decrease with aging, with the result that a person's expected level of health is achieved even as his or her clinically defined health status declines. Empirical studies on self-rated health have shown that the factors associated with health ratings vary somewhat among different age groups. Elderly people, it is reported, pay attention mainly to their physical fitness and the consequences of biological aging, while middle-aged people rate indicators of physical and mental capacity equally.
It is recognized that the concept of self-rated health is a complex one. For example, in a study carried out among the elderly in Tampere, Finland, health self-ratings correlated with the number of reported diseases, the number of various symptoms, the level of functional ability and general life satisfaction. In longitudinal studies, it has been shown that longevity in terms of survivorship is more closely related to subjective than to objective health. One survey undertaken in Bonn, Federal Republic of Germany, found that the elderly who felt "healthy" also showed a high level of interest in their environment, greater activity, less boredom, less loneliness and a less restricted perspective of future time than other elderly people in the sample(10). These findings give rise to a number of questions.
Of course, we know that many old people seek and develop their own individual ways of achieving a new and different quality of life after retirement. But what do they need from the environment and the social and health services in order to maximize their potential for health of mind, body and spirit? Is there identifiable preparation for healthy aging? Is "education for life" a subject on school curricula? How does one develop personal skills with which to learn how to prepare for life's various stages and stresses and also to cope successfully with any non-preventable chronic illness or disablement which may occur?
Countrywide plans of action should focus on efforts to generate living and working conditions which are safe, stimulating, satisfying and enjoyable,i.e. to create a supportive environment which is clean, pleasant and free from barriers to health. At the same time, local authorities need to make the necessary environmental changes, including easy access to public buildings and shops, available and affordable wholesome fresh food and the provision of social, educational, cultural and transport facilities and sports equipment. Sometimes new legislation may be needed. The mass media may also assist in changing the attitudes of the public and, where necessary, of health and social workers themselves. Possibilities for self-help and contributions from voluntary organizations and charities may in some instances need to be provided, developed, supported and more closely coordinated. Perhaps we should also question whether current support systems provide autonomy or encourage dependence.

EUR/RC40/Tech.Disc -/I0621Bpage 10
Life's critical events, e.g. retirement, bereavement, reduction in income and loss of social status, are probably more numerous during one's later years, and it is at such times that the response of health and social workers is of crucial importance. It has been said that many of life's social and economic problems are now "medicalized", and that medical therapy in the form of psychotropic drugs is a danger at such times. Yet stress management is not always given the priority it would appear to deserve. Would the development of relevant programmes help to lessen the incidence of drug, alcohol and nicotine abuse among the elderly?
Screening has been widely discussed as one means of ensuring the maintenance of health in older persons, and controversy surrounds the proposed practice. But there is a difference of opinion regarding whether it should cover a wide range of diseases and be carried out by a gerontological/geriatric expert, or whether it should be a regular medical examination performed by the elderly person's own physician in the home environment. Some experts query whether screening should be done at all and doubt its cost-effectiveness. At the present time, the general public often receive conflicting advice about self-care, e.g. how often they should present for measurement of their blood pressure. Should and could a medical consensus be arrived at? In a number of Member States, the fact that much chronic illness and disability is found among the (apparently) "healthy" aged has led to the development of a variety of screening and case-finding methods which aim to diagnose the disease or condition at an asymptomatic stage. There has, however, been no general agreement about the tests to be included. Instead, a large variety of procedures have been initiated (11). It is suggested that this has led to overenthusiastic use of tests, unnecesssary treatments and iatrogenic disease. Yet the needs of the elderly are subject to change: aging is a dynamic process and once-only assessments are considered by some to be inadequate, leading to misclassification of elderly people. Under such circumstances the health and social services are seen as providing not a safety net but an enwrapping mesh for all time.
The major concern is to provide a support system which helps the elderly person to maintain health, autonomy and activity. Perhaps we need to decide how (in what form and by which mechanisms) the health and social services can give that appropriate backing to the healthy elderly and, when needed, to their families and friends.
3.3 Illness or impairment
Impairment of mobility has been found to be one of the most important factors inhibiting independent living (11). Given the increases in the number of elderly people predicted by demographers, it is obviously a matter of great importance and urgency that each Member State keeps its old people active and mobile. Only then will they be a national social resource rather than a national economic burden. As previously stated, most aging people are indeed able and would prefer to remain in a productive occupation, but national retirement policies usually discard these experienced and skilled human resources which no society should leave untapped (3).
It is generally recognized that the life span is itself a continuum, and that steps to prevent illness, impairments, handicaps and disabilities should be taken in childhood, continued through adolescence and maintained in middle age. This is the concept of primary prevention which, by a variety of

EUR/RC40/Tech.Disc./l0621Bpage 11
approaches, is applied in the majority of Member States. For practical reasons, however, most countries concentrate on specific medical and social needs and divide problems by age groups and populations by chronological age. In no group could this be more inappropriate than in the elderly.
It is often in the acute care setting that an elderly person finds his or her life taken over by staff who have little or no knowledge of the aging process and the heterogeneous nature of the elderly as a group. It has been suggested that all postgraduate medical and nursing curricula should contain some theory and practice of gerontology and geriatrics. But in these days of numerous medical specialties and explosive progress in medical technology, is such a proposal feasible? Most such educational programmes are already extensive. It has also been suggested that the training syllabi of student social workers and therapists should cover certain aspects of aging and include information on relevant legislation, social services, pension schemes and local rehabilitation programmes. In particular, it is said, students should be familiar with the rights of the elderly (12).
One urgent need, discussed at a recent WHO seminar, is for appropriate and early activation of elderly patients (11). Hospital stays not only frequently develop or increase dependence, they also sometimes lead to a reduction in functional ability. Excellent opportunities exist before discharge for giving advice on healthy aging, but they are rarely taken. The patient's records sent back to the community care level are often inadequate and rarely include information on the individual's level of functioning or ability to cope. Often the environment to which the patient is returning is unknown and/or unassessed in terms of his or her daily living activities.
How often does rehabilitation of the elderly hospital patient begin at the earliest possible stage? How often is it continued immediately after discharge? Whose responsibility is it to see that this is done? Whose job is it to see that discharge information, giving details of physiotherapy and occupational therapy received and the regime to be followed, is sent to the right person in the community? And who is that "right person"?
Even when the pathology of a disease or condition is irreversible, the undesirable physical, emotional and social sequelae need not be. The control of chronic pain is one example of the many areas in which further research could improve the quality of life for many elderly people. Epidemiological studies have identified numerous pathological and physiological changes which give rise to locomotor problems and chronic pain. The dissemination of relevant information and advice about self-help through physical exercises, changed lifestyles and working conditions and the possible benefits of alternative approaches to drugs, such as balneotherapy, acupuncture, yoga techniques and so on, could bring relief to many. Elderly patients also probably constitute the largest single group able to benefit from an extension of home care services to provide rehabilitative procedures, thereby improving the quality of their lives. The value of preventing their dependence on the state is considerable in economic terms; in humanitarian terms it is beyond measure.
3.4 Change of function (physical or mental)
There is a growing trend in both the United States of America and Europe towards an expansion of community-based services for people with chronic loss

EUR/RC40/Tech.Disc./I0621Bpage 12
of function (physical and/or mental). The aim is to keep these people - of all ages - in their own homes rather than provide the services they need in an institutional setting. The rationale is basically humanitarian, but in some instances economic advantages also play a part.
From prospective studies, it is known that many countries will experience the need to provide and develop more such services over the next few decades. Their planning needs to be based on local answers to general questions. Analyses will have to be made of the types of care already available and of strategies and approaches that are cost-effective. It has been suggested that consideration needs to be given to drawing up programmes to train community nurse practitioners to oversee such services. Information from feasibility studies will be needed, as will data on emerging technologies and innovations in home care. Few planning models have yet been developed, and comprehensive assessment of those already in use will be valuable.
While care in the community is in itself a generally welcome policy objective, there is a growing recognition that it often imposes heavy demands on relatives, friends and neighbours. Moreover, in the development of community services and of organized voluntary contributions to care insufficient attention seems to have been paid to the needs of such informal carers, leaving many inadequately prepared, uninformed, isolated and manifesting signs and symptoms of chronic stress or "burn-out". The risks to carers' physical wellbeing tend to be acknowledged more readily than the dangers of mental ill health. The two aspects can of course be related. However, the mental stress associated with caring needs to be recognized and addressed in positive ways. Suppressed feelings over a long period can result in the carers breaking down, with adverse consequences for themselves, their dependants and society at large. Much of the frustration, anger and stress is generated in the context of practical caring tasks, and providing continuous care means that the carer and dependent person are consigned to each other's company without respite.
Carers are likely to want information about the specific disabling conditions affecting their relative or friend. Supplying this at the most appropriate level of comprehension is particularly problematic. Some conditions, such as multiple sclerosis and some forms of dementia, are unpredictable. In all instances, however, it is important for carers to be provided not only with adequate practical information but also with opportunities for receiving counselling, guidance and respite.
The emotional difficulties of carers are also caused by wider social factors, e.g. economic policies or the lack of social and legal recognition.As the majority of carers are women, many are trying to reconcile the caring role expected of them with paid employment and domestic duties. The nineteenth century assumption, that caring is naturally and solely women's work, needs to be challenged. It has been suggested that there is an urgent need for Member States to identify ways and means of enhancing the lives of those elderly women carers who are themselves experiencing changes brought about by the aging process and who need assistance with "aging healthily" under especially difficult circumstances (11).
Care in a nursing home will continue to be needed by some elderly people. As it is the aim of such institutions to be centres of living as well as of care, the staff members themselves often need help and encouragement.

EUR/RC40/Tech.Disc./l0621Bpage 13
Their responsibilities are overwhelmingly great: they have to provide an atmosphere that helps the elderly to maintain the maximum freedom of choice, independence and mobility; they give treatments as prescribed and, in accordance with ethical guidelines produced by professional bodies, they are expected to provide a safe environment in which elderly people may meet their daily needs in spite of disabilities or handicaps. They also cope with the residents' problems of loneliness (even in a crowd), apathy, incontinence, mental confusion, bereavement and failing faculties, and indeed with the overall management of their charges' changed and changing lives.
For those patients who are unable to feed, wash or dress themselves or who are in some other way dependent, and for whom rehabilitation procedures offer no prospects, nursing care is inevitable. The standard of this care depends not only on the high personal qualities of each carer but also on their professional training and teamwork.
Just as each country must develop its own services according to the needs of its population, so it must develop its own educational programmes for professionals and other personnel, such as community or village health workers, who will provide those services. Nevertheless, certain general principles apply to all. Firstly, maintaining standards of care is the tripartite responsibility of those in clinical practice, management and education. Secondly, all countries need to foster, in their health and social workers, attitudes, empathy and aptitudes which will ensure an elderly person's right to privacy, choice and control of his or her own destiny.
In terms of educational programmes, this issue raises many questions, for few Member States have full programmes or even courses in gerontology and geriatrics for all health professionals. Should theoretical and practical instruction in this field be included in basic training? If so, what should be the focus? What clinical experience should be made available? How can students learn to make comprehensive assessments without violating an elderly person's privacy? How can teachers develop in their students an appreciation of the importance of protecting the liberty of the individual, so that each old person is able to retain all possible control over his or her own living and - eventually - dying?
3.5 Change of autonomy
Liberty is an elusive concept. No human being has complete freedom of action. Most people are constrained by work, income, housing and a host of other factors which limit the range of courses open to them. For those elderly people who are frail or disabled and living on a small pension, what they may like to do and what is physically or financially possible diverge even further. It would be unrealistic not to acknowledge that this is inevitable. It has been said, however, that there are ways in which society further restricts this narrowing range of choice; one is to impose on elderly people forms of care and treatment which are the outcome of social perceptions, social anxiety, convenience or custom rather than inescapable necessity. Old people are taken from their homes when assisted domiciliary physical treatment might enable them to stay there; they are subjected, in long-stay hospitals and homes, to regimes which deprive them of many basic human dignities; and they are often not properly consulted about the care or treatment which they receive (13). What is needed is not necessarily a massive increase in resources but a more skilled, varied and sensitive use of

EUR/RC40/Tech.Disc./l0621Bpage 15
On the other hand, some deaths can be the end of distressing protracted illnesses. Problems associated with dying in acute pain from malignant lesions and conditions have been widely discussed in recent decades, and much better understanding, approaches and treatments have been developed. Hospices have proliferated in a number of countries and act as teaching and resource centres as well as offering care for patients and their families or friends. The art of giving terminal care demands the highest standards of nursing, and this covers the relief of distressing symptoms, including pain. It should also comprise care of the bereaved elderly spouse or friend, as he or she faces a very major life change.
3.7 Aging: a challenge to all
Healthy aging has been, and is likely to continue to be, defined in a variety of ways according to cultural, sociological and anthropological perceptions, attitudes and values. But it would appear obvious that with advancing years, one priority of younger generations - to increase life expectancy - gives way to another: to ensure the quality of life. And while that quality of life is certainly dependent upon the individual's own personal development, responses to the changes and challenges of aging and utilization of inner resources, as at any age, the full attainment of an individual's potential depends upon many factors. It requires the right environment, reliable support and encouragement, and appropriate assistance readily available. In the context of healthy aging, this means developing national and local plans of action which provide conditions and services for today's elderly people and preparatory programmes for the old people of future decades- the year 2000 and beyond.
Aging is therefore a challenge not only to each individual but also to families, communities and governments. And it is to the latter that the former are looking for action. The challenge is great, and so must be the response.
4. Conclusions
4.1 The present status of elderly people in Europe
Aging affects every man, woman and child - even unborn. Aging also affects the economy, the social structure and the health care system of every nation. It is, therefore, everyone's concern.
Over the next few decades there will be more old people throughout the Region. In 1960, 14.4% of Europe's total population was over the age of 60 years. By 1980, this had increased to 16.9%. It is now projected that by the turn of the century this figure will have risen to 20.2%, while twenty years later it will be 25.1%. The group which is increasing in size most rapidly is the "old old" - people aged 80 years or more.
At present, Sweden has the highest proportion of old people. By the year 2000, the largest numbers will be found in the Federal Republic of Germany and in Greece. In 2025, it is projected the largest numbers of elderly people will be living in Switzerland, the Netherlands, Luxembourg and the Federal Republic of Germany.

EUR/RC40/Tech.Disc./10621Bpage 16
4.2 Major problems to be addressed
Aging is not a disease but a physiological process that affects everybody. It cannot be prevented or postponed, and changes due to aging affect everyone. These changes affect senses such as vision and hearing.
Other changes due to pathology may result in illness and/or disability. Some, but not all, are preventable. Little was known previously about the oldest age groups (people over 85 years). Studies carried out among long-living people have now elucidated differences between age groups and have contributed to a better understanding of some of the real possibilities for the prevention and treatment of diseases in old age. There is evidence that many of the changes that are at present common in old age are preventable: they are not inevitable concomitants of biological aging but are rather the results of earlier and/or current exposure to various risks.
The assessment of people's functional abilities has become increasingly important, for several reasons. Chronic diseases that develop gradually over several years or decades play a predominant role in the disease spectrum. In the majority of instances they could be completely cured, and the question that must then be asked is how much do they limit a person's functional ability. Predictions about the development of the health and wellbeing of elderly populations therefore appear to be more closely associated with the level of functional abilities than with the prevalence of chronic diseases.This means that particular attention has to be paid to a person's behaviour and to his or her ability to cope with daily activities, duties and situations.
4.3 Prospects and policy for the future
Efforts need to be focused on maintaining fitness for as long as possible. This presupposes educating people in healthy lifestyles, the management of stress, the need for adequate exercise and nutrition and the prevention of loss of autonomy, as well as on the prevention of disease.Because the impairment of sensory, psychomotor and motor functions is typical of the elderly, it is assumed that the future rapid growth in the numbers of people aged 85 years and above will lead to a significant increase in overall disability among the aged, and that consequently there will be a greater demand for both specialized health services and various forms of social support. Provided that findings in respect of age cohort differences in health and functional ability can be applied in general, certain trends within the elderly population can be anticipated. On the one hand, the health and functional ability of those aged under 75 years will improve and they will look for better opportunities to remain in society and be actively involved in various spheres of it; on the other hand, the large increase by the year 2000 in the proportion of those aged 85 years and over will inevitably lead to increased numbers of frail and disabled people, who will have difficulty in coping with the tasks of everyday life and will therefore be in need of health and social services of a personal care nature.
One major concern is the net result of these two trends in terms of the prevalence of disability and the corresponding need for services. At present, disease and disability are sometimes just postponed; it is likely that in future the later years of a very long life will bring a compressed period of multiple pathology.

EUR/RC40/Tech.Disc./I0621Bpage 17
Whereas in the past the majority of countries developed services for the elderly as part of their general systems of care for all members of society, it is now apparent that the processes of aging, particularly when considered in conjunction with the rapid changes in environmental and living conditions, call for special arrangements, services and priorities within those care systems.
Informal carers are less available than they were even a few years ago. Often these were wives and mothers who now seek paid employment. Neighbourliness is reported as being on the decline in some countries, while nongovernmental organizations are finding it increasingly difficult to recruit volunteers for such work. An important question to be asked is therefore who will replace these traditional carers?
For a certain percentage of elderly people (e.g. those who are severely disabled and/or living alone) there may be no option other than a form of institutional care. The future task is to ensure a balance between the provision of community services for home care and the provision of institutional care. The latter demands not only higher quality but also greater variety. The value of rehabilitative facilities for the elderly, for example, has been greatly underestimated in the past, but such services often increase the functional ability of elderly people, thus enabling them to enjoy more independent living again.
These new strategies require new tactics to bring about the necessary changes in attitudes towards aging and the aged, both among health and allied professionals and among the general public. If they are to be successful, they will also need new "ammunition" in the form of redistributions of human and financial resources.
REFERENCES
1. Kruse, A. & Lehr, U. Longitudinal analysis of the development process in chronically ill and healthy persons - Empirical findings from the Bonn longitudinal study of aging (BOLSA). International psychogeriatrics,1(1): (1989).
2. An aging planet. Geneva, World Health Organization, 1989.
3. Targets for health for all. Copenhagen, WHO Regional Office for Europe, 1985 (European Health for All Series, No. 1).
4. Rattan, S. & Clark, B. Ageing: a challenge for biotechnology. Trends in biotechnology, 6: 58-62 (1988).
5. Lehr, U . , ed. Interventionsgerontologie. Darmstadt, Dr Dietrich Steinkopff Verlag, 1979 (Praxis der sozialpsychologie, No. 11).
6. WHO programme for research on aging: meeting of interested parties.Geneva, World Health Organization, 1989 (unpublished document IRP/HEE 120).

EUR/RC40/Tech.Disc./I0621Bpage 18
7. Kruse, A. et a l ., ed. Gerontologie: wissenschaftliche Erkenntnisse und Folgerungen flir die Praxis. Beitrage zur II Gerontologischen Woche, Heidelberg, 18-23 June 1987. Munich, Bayerischer Monatspiegel Verlagsgesellschaft mbH, 1988.
8. Rott, C. & Oswald, F . , ed. Kompetenz im Alter. Beitrage zur III Gerontologischen Woche, Heidelberg, 2-6 May 1988. Vaduz, Liechtenstein Verlag AG, 1989.
9. Thomae, H. [The individual and his world - a theory of personality.] Gottingen, Verlag flir Psychologie, 1968.
10. Continuity of care of the elderly: report on a WHO working group. Copenhagen, WHO Regional Office for Europe, 1987 (unpublished document EUR/ICP/HEE 127).
11. Preventable disablements in old a g e : report on a travelling seminar. Copenhagen, WHO Regional Office for Europe, 1989 (unpublished document EUR/ICP/HEE 222).
12. Medicosocial work and nursing: the changing needs: report on two WHO meetings. Copenhagen, WHO Regional Office for Europe, 1983 (EURO Reports and Studies, No. 79).
13. Norman, A. Rights and risks. London, Centre for Policy on Aging, 1982.
14. Wolf, R. & Bergman, S. Stress, conflict and abuse of the elderly. Jerusalem, Brookdale Institute of Gerontology and Adult Human Development, 1989.
15. Baker, A. Slow euthanasia or S h e’ll be better off in a hospital. British medical journal, 2, 1986.
EUR/RC40/Tech.Disc./I0621Bpage 19
Annex 1
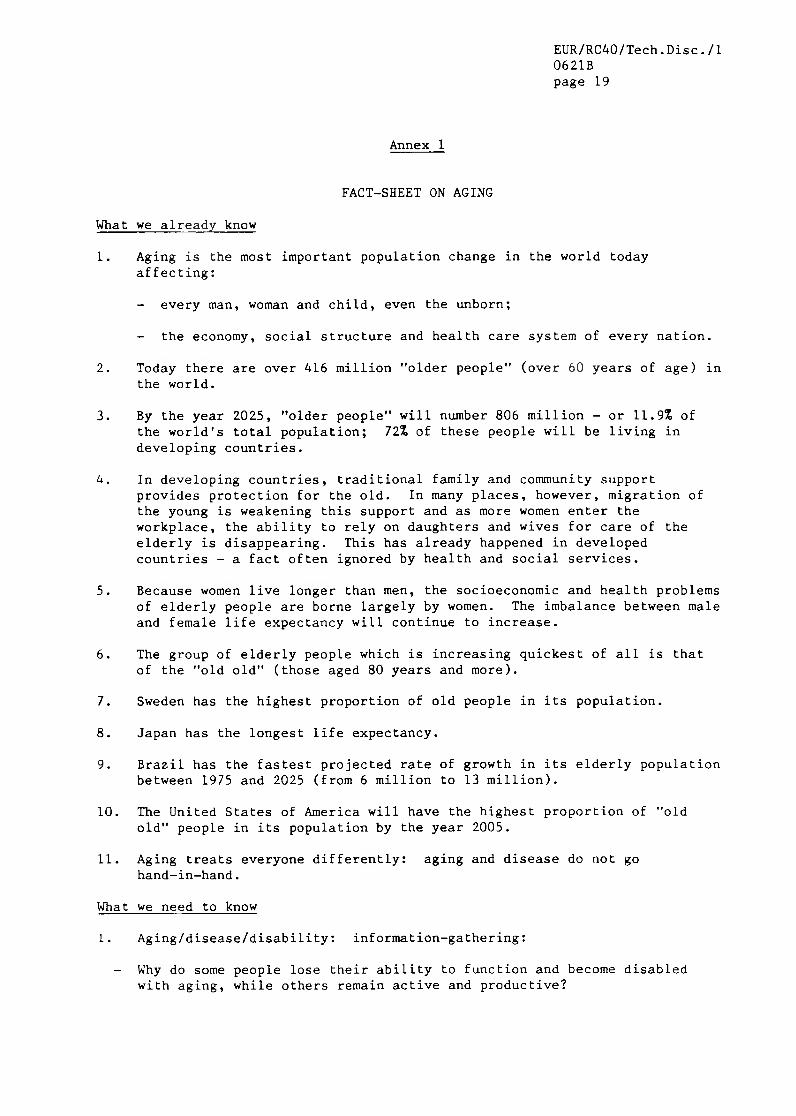
FACT-SHEET ON AGING
What we already know
1. Aging is the most important population change in the world today affecting:
- every man, woman and child, even the unborn;
- the economy, social structure and health care system of every nation.
2. Today there are over 416 million "older people" (over 60 years of age) in the world.
3. By the year 2025, "older people" will number 806 million - or 11.9% of the world's total population; 72% of these people will be living in developing countries.
k. In developing countries, traditional family and community supportprovides protection for the old. In many places, however, migration of the young is weakening this support and as more women enter the workplace, the ability to rely on daughters and wives for care of the elderly is disappearing. This has already happened in developed countries - a fact often ignored by health and social services.
5. Because women live longer than men, the socioeconomic and health problems of elderly people are borne largely by women. The imbalance between male and female life expectancy will continue to increase.
6. The group of elderly people which is increasing quickest of all is that of the "old old" (those aged 80 years and more).
7. Sweden has the highest proportion of old people in its population.
8. Japan has the longest life expectancy.
9. Brazil has the fastest projected rate of growth in its elderly population between 1975 and 2025 (from 6 million to 13 million).
10. The United States of America will have the highest proportion of "old old" people in its population by the year 2005.
11. Aging treats everyone differently: aging and disease do not go hand-in-hand.
What we need to know
1. Aging/disease/disability: information-gathering:
- Why do some people lose their ability to function and become disabled with aging, while others remain active and productive?

EUR/RC40/Tech.Disc./I0621Bpage 20
- Why is male life expectancy less than that of women? What implications does this fact have for "healthy aging"?
- How healthy and/or functioning are the "old old"? What are the implications for health and social services?
- What should be changed in lifestyles/behaviour (e.g. physical exercise, nutrition, stress) in order to maintain health and productivity into later years of life?
- How can disability be predicted, prevented or postponed?
- How can multisectoral collaboration affect lifestyles?
- What are the channels for achieving desirable changes in lifestyles (e.g. publications, the mass media, decision-makers)?
2. Aging/disease/disability: fact-finding intervention
How can the health needs of middle-aged people (i.e. 45-49 years) be identified?
- What action should be taken to promote health in these people?
How can the health needs of the "young old" (60-75 years) be identified?
- What action should be taken to promote health in these people?
- How do the disabilities (sensory, locomotor, mental, multiple) of aging and aged people affect them and their families?
What should be done to lighten the burden of care-givers (in developed countries 80% are women and many are also in gainful employment)?
3. Aging/disease/disability: research
- What is the relationship of age to infection and immunity?
- How does the environment affect immunity?
What risk factors contribute to diseases commonly found in old people such as osteoporosis and Alzheimer's disease?
- What causes symptoms frequently experienced in aging such as sleep disturbance, back pain, profuse sweating, feelings of lightheadedness and fainting, muscle/neck stiffness, anxiety and feelings of insecurity, confusion, nervousness or overexcitement?
- What should be done to diminish or eliminate these symptoms?
- What other issues should we be exploring, and which indicators should we use to monitor the aging process?
Will future generations be healthier in old age than present ones?

EUR/RC40/Tech.Disc./I0621Bpage 21
- How can they be compared (e.g. life expectancy, cohort differences, prediction of longevity)?
4. Identification of simple indicators for "healthy aging"
Such indicators have not yet been defined. In order to do so, might it be helpful to focus attention on the quality of life; on improving databases, particularly on morbidity in primary health care and morbidity followed by disability; on interventions in long-term care; and on supportive environments?

EUR/RC40/TechoDisc0621Bpage 23
Annex 2
HEALTHY AGING - DEMOGRAPHY

Table 1. Estimated and projected percentage of total population In major age groups (0-14, 15-59, 60 and over), Europe, Northern America and the USSR
~ I960, 1980, 2000, 2020, 2025 (X)
Region or country
1960 1980 2000 2020 2025
0-14 15-59 60+ 0-14 15-59 60+ 0-14 15-59 60+ 0-14 15-59 60+ 0-14 15-59 60+
NORTHERN AMERICA 31.3 55.8 13.0 22.5 61.9 15.5 20.2 63.0 16.8 18.2 57.4 24.3 17.9 55.6 26.4
Canada 33.5 55.8 10.7 22.5 63.8 13.7 18.9 64.2 17.0 17.0 57.2 25.7 16.6 55.3 28. 1
United States of America 31.0 55.8 13.2 22.5 61.7 15.7 20.3 62.9 16.8 18.3 57.5 24.2 18.1 55.7 26.3
EUROPE 25.8 59.8 14.4 22.4 60.7 16.9 18.5 61.3 20.2 16.8 58.1 25.1 16.6 56.4 27.0
EASTERN EUROPE 28.0 59.3 12.7 23.6 61.3 15.1 20.1 61.9 18.0 18.7 58.9 22.4 18.2 58.6 23.2
Bulgaria 26.1 62.5 11.4 22.1 62.2 15.7 18.2 60.5 21.2 17.4 58.1 24.6 17.1 57.7 25.2
Czechoslovakia 27.4 59.1 13.4 24.3 60.0 15.7 20.3 63.3 16.4 18.4 59.6 22.0 18.0 59.4 22.7
German Democratic Republic 21.1 58.8 20.2 19.7 61.1 19.2 17.4 61.5 21.1 16.4 58.0 25.5 15.8 56.1 28.1
Hungary 25.3 60.7 14.0 21.9 60.9 17.2 17.8 62.3 19.9 16.6 58.3 25.1 16.3 58.5 25.2
Poland 33.5 57.2 9.4 24.3 62.5 13.2 21.5 62.5 16.0 20.4 58.2 21.4 19.6 58.2 22.2
Romanla 28.2 61.2 10.6 26.7 60.1 13.3 21.3 60.8 18.0 18.7 60.5 20.8 18.4 60.7 20.9
NORTHERN EUROPE 24.1 59.5 16.4 21.2 59.0 19.8 19.0 60.8 20.2 17.0 57.6 25.4 17.0 55.6 27.4
Denmark 25.2 59.3 15.5 20.8 59.7 19.5 16.6 62.8 20.6 14.9 56.9 28.2 14.8 55.1 30.0
Finland 30.4 58.4 11.2 20.3 63.3 16.4 17.5 63.1 19.4 16.4 56.1 27.5 16.2 54.8 28.9
Iceland 34.7 54.0 11.4 27.5 59.0 13.5 21.7 63.3 15.0 18.4 59.9 21.8 17.7 57.8 24.5
Ireland 31.1 53.1 15.8 30.6 54.6 14.8 24.5 62.4 13.1 21.1 62.1 16.8 20.3 61.2 18.4
Norway 25.9 57.9 16.2 22.2 57.6 20.3 18.5 61.5 19.9 16.3 57.9 25.8 16.1 56.4 27.5
Sweden 22.0 60.7 17.3 19.6 58.5 21.9 16.9 60.3 22.8 15.5 55.5 29.0 15.6 54.3 30.0
United Kingdom 23.3 59.9 16.9 20.9 59.0 20.1 19.3 60.3 20.4 17.2 57.7 25.2 17.2 55.3 27.5
SOUTHERN EUROPE 27.1 60.6 12.3 24.4 60.4 15.2 18.2 61.4 20.4 16.4 59.0 24.6 16.1 57.1 26.8
Albania 41.1 51.3 7.6 35.9 56.5 7.7 28.2 62.1 9.7 23.1 62.4 14.5 22.3 61.0 16.7
Greece 26.5 61.4 12.1 22.8 59.7 17.5 17.1 59.8 23.1 16.4 57.5 26.1 16.1 56.4 27.5
Italy 24.8 61.6 13.6 22.3 60.7 17.0 16.5 61.0 22.4 14.5 58.3 27.2 14.4 56.0 29.6
Ma 11 a 36.8 52.6 10.6 23.1 63.3 13.7 19.6 64.9 15.5 18.3 58.2 23.5 17.7 57.5 24.8
Portugal 29.2 59.1 11.7 25.9 59.5 14.6 19.3 61.5 19.3 17.5 60.0 22.5 17.1 58.1 24.8
Spain 27.4 60.2 12.3 26.6 58.6 14.9 18.6 61.8 19.6 16.9 59.4 23.7 16.6 57.3 26. 1
Yugoslavia 30.5 59.7 9.8 24.8 63.7 11.5 19.9 62.2 17.9 18.0 59.3 22.6 17.5 58.2 24.3
WESTERN EUROPE 24.1 59.6 16.4 20.3 61.6 18.1 17.5 61.0 21.6 15.5 56.8 27.7 15.5 54.6 29.9
Austria 22.1 59.9 18.0 20.4 60.4 19.1 16.6 62.2 21.2 14.8 57.8 27.3 14.6 55.1 30.2
Belgium 23.5 58.9 17.6 20.2 61.5 18.3 17.4 61.0 21.6 16.1 57.4 26.5 15.9 55.5 28.6
France 26.4 56.8 16.8 22.3 60.5 17.2 19.5 60.5 19.9 17.4 57.2 25.4 17.2 55.8 27.0
Germany, Federal Republic of 21.3 62.3 16.4 18.2 62.5 19.3 15.8 60.4 23.8 13.8 56.5 29.7 14.1 53.3 32.6
Luxembourg 21.3 62.4 16.2 19.0 63.4 17.6 16.4 62.2 21.4 14.7 56.4 28.9 14.7 54.1 31.2
Nether lands 30.0 56.9 13.1 22.3 62.0 15.7 17.0 64.0 19.0 14.4 57.1 28.5 14.4 54.3 31.3
Switzerland 23.6 61.5 14.9 19.7 62.0 18.2 16.5 60.7 22.8 14.1 54.5 31.5 14.3 52.1 33.7
UNION OF SOVIET SOCIALIST REPUBLICS 30.7 59.3 10.1 24.8 62.1 13.2 23.6 59.5 16.9 21.4 59.5 19.1 20.8 58.6 20.6
Source: Derived from World population prospects 1988. New York, United Nations Department of International Economic and Social Affairs, 1989
(Populat ion Studies No. 106).
EUR/RC40/Tech.Disc./I
0621B
page 24
EUR/RC40/Tech.Disc./l0621Bpage 25
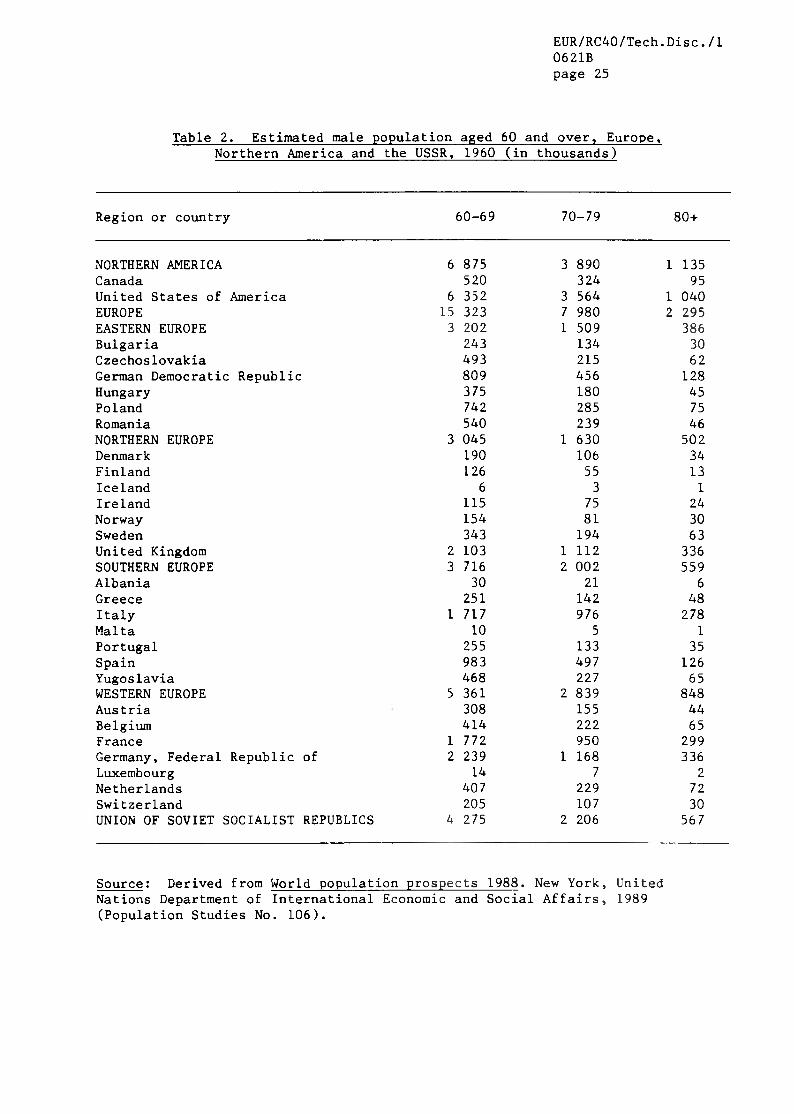
Table 2. Estimated male population aged 60 and over, Europe,Northern America and the USSR, 1960 (in thousands)
Region or country 60-69 70-79 80+
NORTHERN AMERICA CanadaUnited States of America EUROPEEASTERN EUROPEBulgariaCzechoslovakiaGerman Democratic RepublicHungaryPolandRomaniaNORTHERN EUROPEDenmarkFinlandIcelandIrelandNorwaySwedenUnited KingdomSOUTHERN EUROPEAlbaniaGreeceItalyMaltaPortugalSpainYugoslavia WESTERN EUROPE Austria Belgium FranceGermany, Federal Republic ofLuxembourgNetherlandsSwitzerlandUNION OF SOVIET SOCIALIST REPUBLICS
6 875 3 890 1 135520 324 95
6 352 3 564 1 04015 323 7 980 2 2953 202 1 509 386
243 134 30493 215 62809 456 128375 180 45742 285 75540 239 46
3 045 1 630 502190 106 34126 55 13
6 3 1115 75 24154 81 30343 194 63
2 103 1 112 3363 716 2 002 559
30 21 6251 142 48
1 717 976 27810 5 1
255 133 35983 497 126468 227 65
5 361 2 839 848308 155 44414 222 65
1 772 950 2992 239 1 168 336
14 7 2407 229 72205 107 30
4 275 2 206 567
Source: Derived from World population prospects 1988. New York, UnitedNations Department of International Economic and Social Affairs, 1989(Population Studies No. 106).

EUR/RC40/Tech.Disc./I0621Bpage 26
Table 3. Estimated female population aged 60 and over, Europe,Northern America and the USSR, 1960 (in thousands)
Region or country 60-69 70-79 80+
NORTHERN AMERICA CanadaUnited States of America EUROPEEASTERN EUROPEBulgariaCzechoslovakiaGerman Democratic RepublicHungaryPolandRomaniaNORTHERN EUROPEDenmarkFinlandIcelandIrelandNorwaySwedenUnited KingdomSOUTHERN EUROPEAlbaniaGreeceItalyMaltaPortugalSpainYugoslavia WESTERN EUROPE Austria Belgium FranceGermany, Federal Republic ofLuxembourgNetherlandsSwitzerlandUNION OF SOVIET SOCIALIST REPUBLICS
7 616 4 627 1 613527 339 111
7 086 4 286 1 50120 141 11 784 3 7884 322 2 278 626
277 168 45640 329 96
1 201 686 196475 255 65
1 032 493 141697 347 83
3 891 2 451 886214 125 40176 96 28
6 3 1120 83 31172 103 39378 233 80
2 815 1 801 6654 684 2 767 860
34 24 7307 194 63
2 173 1 302 38412 6 1
340 202 721 219 703 227
597 336 1057 244 4 288 1 416
433 250 78506 300 104
2 425 1 614 6153 150 1 704 480
16 9 3455 260 86257 150 50
8 174 4 844 1 498
Source: Derived from World population prospects 1988. New York, UnitedNations Department of International Economic and Social Affairs, 1989(Population Studies No. 106).

EUR/RC40/Tech.Disc./I0621Bpage 27
Table 4. Estimated male population aged 60 and over, Europe,Northern America and the USSR, 1980 (in thousands)
Region or country 60-69 70-79 80+
NORTHERN AMERICA CanadaUnited States of America EUROPEEASTERN EUROPEBulgariaCzechoslovakiaGerman Democratic RepublicHungaryPolandRomaniaNORTHERN EUROPEDenmarkFinlandIcelandIrelandNorwaySwedenUnited KingdomSOUTHERN EUROPEAlbaniaGreeceItalyMaltaPortugalSpainYugoslavia WESTERN EUROPE Austria Belgium FranceGermany, Federal Republic ofLuxembourgNetherlandsSwitzerlandUNION OF SOVIET SOCIALIST REPUBLICS
9 463 5 191 1 871840 454 156
8 619 4 734 1 71417 317 12 544 3 4653 368 2 647 636
350 233 58508 390 86478 508 144393 291 75985 721 161654 503 112
3 806 2 378 669236 148 52167 102 25
7 5 2133 75 24200 120 44435 286 96
2 616 1 635 4254 901 3 225 860
56 28 8388 276 91
2 165 1 476 41112 9 2
354 213 451 337 795 218
586 427 845 243 4 294 1 301
261 213 59388 271 85
1 729 1 519 4882 075 1 793 495
14 10 2520 313 115253 174 56
5 620 4 096 1 200
Source: Derived from World population prospects 1988. New York, UnitedNations Department of International Economic and Social Affairs, 1989(Population Studies No. 106).

EUR/RC40/Tech.Disc./I0621Bpage 28
Table 5. Estimated female population aged 60 and over, Europe,Northern America and the USSR, 1980 (in thousands)
Region or country 60-69 70-79 80+
NORTHERN AMERICA CanadaUnited States of America EUROPEEASTERN EUROPEBulgariaCzechoslovakiaGerman Democratic RepublicHungaryPolandRomaniaNORTHERN EUROPEDenmarkFinlandIcelandIrelandNorwaySwedenUnited KingdomSOUTHERN EUROPEAlbaniaGreeceItalyMaltaPortugalSpainYugoslavia WESTERN EUROPE Austria Belgium FranceGermany, Federal Republic ofLuxembourgNetherlandsSwitzerlandUNION OF SOVIET SOCIALIST REPUBLICS
11 299 7 531 3 799954 594 287
10 340 6 934 3 51022 077 18 871 7 5494 527 3 983 1 324
384 281 82630 593 198844 904 334501 429 150
1 323 1 125 380844 650 179
4 431 3 498 1 580263 203 96242 183 63
8 6 3140 93 39223 163 78470 367 169
3 072 2 473 1 1286 020 4 485 1 626
66 34 12455 337 135
2 623 2 086 82813 10 3
422 298 901 673 1 146 412
764 569 1457 099 6 905 3 018
396 371 14446 7 418 173
2 086 2 279 1 1743 225 3 107 1 193
18 15 5610 455 209296 258 118
10 888 9 683 3 515
Source: Derived from World population prospects 1988. New York, UnitedNations Department of International Economic and Social Affairs, 1989(Population Studies No. 106).

EUR/RC40/Tech.Disc. / I0621Bpage 29
Table 6. Projected male population aged 60 and over, Europe,Northern America and the USSR, 2000 (in thousands)
Region or country 60-69 70-79 80+
NORTHERN AMERICA CanadaUnited States of America EUROPEEASTERN EUROPEBulgariaCzechoslovakiaGerman Democratic RepublicHungaryPolandRomaniaNORTHERN EUROPEDenmarkFinlandIcelandIrelandNorwaySwedenUnited KingdomSOUTHERN EUROPEAlbaniaGreeceItalyMaltaPortugalSpainYugoslavia WESTERN EUROPE Austria Belgium FranceGermany, Federal Republic ofLuxembourgNetherlandsSwitzerlandUNION OF SOVIET SOCIALIST REPUBLICS
10 237 7 323 3 1831 095 731 2859 137 6 589 2 896
23 743 14 834 4 6825 083 2 929 706
464 316 80599 385 90914 401 109450 291 73
1 517 886 2121 139 650 1423 724 2 592 998
232 157 69220 135 42
9 7 3129 80 29169 139 62392 296 144
2 563 1 770 6457 110 4 502 1 426
106 52 15563 344 144
2 947 1 945 60614 8 3
447 301 981 803 1 287 4071 225 562 1527 826 4 812 1 554
344 222 69485 329 100
2 505 1 804 5633 464 1 814 570
19 11 3671 418 154335 213 95
12 134 5 742 1 066
Source: Derived from World population prospects 1988. New York, UnitedNations Department of International Economic and Social Affairs, 1989(Population Studies No. 106).

EUR/RC40/Tech.Disc./I0621Bpage 30
Table 7. Projected female population aged 60 and over, Europe,Northern America and the USSR, 2000 (in thousands)
Region or country 60-69 70-79 80+
NORTHERN AMERICA CanadaUnited States of America EUROPEEASTERN EUROPEBulgariaCzechoslovakiaGerman Democratic RepublicHungaryPolandRomaniaNORTHERN EUROPEDenmarkFinlandIcelandIrelandNorwaySwedenUnited KingdomSOUTHERN EUROPEAlbaniaGreeceItalyMaltaPortugalSpainYugoslavia WESTERN EUROPE Austria Belgium FranceGermany, Federal Republic ofLuxembourgNetherlandsSwitzerlandUNION OF SOVIET SOCIALIST REPUBLICS
11 899 10 295 6 5551 187 973 567
10 707 9 318 5 98526 985 21 909 10 3836 104 4 628 1 579
532 412 122744 625 216
1 031 726 321592 521 167
1 890 1 455 5131 315 889 2404 086 3 576 2 185
253 212 138253 218 11510 8 4
136 107 53183 186 125415 384 270
2 824 2 451 1 4728 199 6 338 2 741
108 64 22655 434 211
3 436 2 810 1 23917 11 5
559 441 1922 030 1 691 7921 388 883 2788 596 7 366 3 878
392 368 188549 471 229
2 828 2 579 1 3133 727 3 047 1 601
21 17 7709 588 350366 294 189
16 311 11 830 5 012
Source: Derived from World population prospects 1988. New York, UnitedNations Department of International Economic and Social Affairs, 1989(Population Studies No. 106).

EUR/RC40/Tech.Disc./l0621Bpage 31
Table 8. Projected male population aged 60 and over, Europe,Northern America and the USSR, 2020 (in thousands)
Region or country 60-69 70-79 80+
NORTHERN AMERICA CanadaUnited States of America EUROPEEASTERN EUROPEBulgariaCzechoslovakiaGerman Democratic RepublicHungaryPolandRomaniaNORTHERN EUROPEDenmarkFinlandIcelandIrelandNorwaySwedenUnited KingdomSOUTHERN EUROPEAlbaniaGreeceItalyMaltaPortugalSpainYugoslavia WESTERN EUROPE Austria Belgium FranceGermany, Federal Republic ofLuxembourgNetherlandsSwitzerlandUNION OF SOVIET SOCIALIST REPUBLICS
19 916 10 785 4 1121 994 1 177 435
17 913 9 603 3 67530 425 18 691 7 3497 044 3 598 1 259
510 336 129949 516 132
1 066 544 227627 343 105
2 515 1 144 3771 376 714 2894 961 3 415 1 200
312 236 81330 221 6618 10 4
214 117 35273 181 65495 419 153
3 304 2 221 7918 617 5 329 2 338
205 98 33572 393 216
3 309 2 238 98724 14 4
573 331 1382 374 1 482 6161 553 770 3429 803 6 350 2 552
447 294 108640 373 147
3 487 2 244 8743 751 2 423 1 050
25 15 51 034 680 231
414 319 13617 014 6 781 2 761
Source; Derived from World population prospects 1988. New York, UnitedNations Department of International Economic and Social Affairs, 1989(Population Studies No. 106).

EUR/RC40/Tech.Disc. / I0621Bpage 32
Table 9. Projected female population aged 60 and over, Europe,Northern America and the USSR, 2020 (in thousands)
Region or country 60-69 70-79 80+
NORTHERN AMERICA CanadaUnited States of America EUROPEEASTERN EUROPEBulgariaCzechoslovakiaGerman Democratic RepublicHungaryPolandRomaniaNORTHERN EUROPEDenmarkFinlandIcelandIrelandNorwaySwedenUnited KingdomSOUTHERN EUROPEAlbaniaGreeceItalyMaltaPortugalSpainYugoslavia WESTERN EUROPE Austria Belgium FranceGermany, Federal Republic ofLuxembourgNetherlandsSwitzerlandUNION OF SOVIET SOCIALIST REPUBLICS
21 877 14 345 8 6072 158 1 491 870
19 709 12 847 7 73333 170 24 547 14 9857 988 5 076 2 533
572 445 2141 092 755 3091 148 733 460
728 533 2492 920 1 671 8401 528 939 4615 313 4 388 2 542
333 294 164357 292 15318 11 7
228 147 67282 219 137513 501 297
3 565 2 910 1 7099 334 6 957 4 485
204 108 47623 495 342
3 625 2 989 2 02225 17 8
655 474 2842 532 1 858 1 1821 663 1 010 597
10 536 8 126 5 425488 389 236681 485 318
3 889 2 896 1 9193 931 3 113 2 191
28 19 111 069 828 490
447 392 25820 329 10 487 8 088
Source: Derived from World population prospects 1988. New York, UnitedNations Department of International Economic and Social Affairs, 1989(Population Studies No. 106).

EUR/RC40/Tech.Disc. / I0621Bpage 33
Table 10. Projected male population aged 60 and over, Europe,Northern America and the USSR, 2025 (in thousands)
Region or country 60-69 70-79 80+
NORTHERN AMERICA CanadaUnited States of America EUROPEEASTERN EUROPEBulgariaCzechoslovakiaGerman Democratic RepublicHungaryPolandRomaniaNORTHERN EUROPEDenmarkFinlandIcelandIrelandNorwaySwedenUnited KingdomSOUTHERN EUROPEAlbaniaGreeceItalyMaltaPortugalSpainYugoslavia WESTERN EUROPE Austria Belgium FranceGermany, Federal Republic ofLuxembourgNetherlandsSwitzerlandUNION OF SOVIET SOCIALIST REPUBLICS
20 807 13 106 4 7012 129 1 371 513
18 669 11 729 4 18632 176 20 699 7 8816 694 4 429 1 298
503 362 133896 611 153
1 146 631 242548 406 117
2 342 1 543 3731 260 876 2805 436 3 582 1 349
325 238 97321 245 7519 12 4
238 136 40281 204 74504 406 187
3 731 2 330 8679 572 5 836 2 460
249 119 38617 433 212
3 713 2 346 1 02924 15 4
651 373 1412 723 1 610 6751 587 935 359
10 474 6 851 2 773510 296 124671 429 149
3 527 2 607 9014 201 2 427 1 164
25 17 51 101 754 270
436 320 15918 173 9 214 2 551
Source: Derived from World population prospects 1988. New York, UnitedNations Department of International Economic and Social Affairs, 1989(Population Studies No. 106).

EUR/RC40/Tech.Disc./l0621Bpage 34
Table 11. Projected female population aged 60 and over, Europe,Northern America and the USSR, 2025 (in thousands)
Region or country 60-69 70--79 80+
NORTHERN AMERICA 22 597 17 151 9 661Canada 2 249 1 741 998United States of America 20 338 15 402 8 659EUROPE 34 534 26 973 15 909EASTERN EUROPE 7 452 6 127 2 626Bulgaria 550 481 225Czechoslovakia 1 011 878 348German Democrati c Republic 1 221 812 490Hungary 620 608 268Poland 2 667 2 216 842Romania 1 382 1 134 453NORTHERN EUROPE 5 768 4 607 2 781Denmark 347 297 189Finland 346 326 168Iceland 20 13 7Ireland 250 173 77Norway 289 245 147Sweden 517 488 340United Kingdom 3 980 3 050 1 843SOUTHERN EUROPE 10 183 7 449 4 724Albania 245 133 55Greece 641 525 344Italy 3 976 3 091 2 120Malta 24 19 9Portugal 731 515 297Spain 2 864 1 979 1 268Yugoslavia 1 694 1 181 628WESTERN EUROPE 11 132 8 789 5 778Austria 549 388 263Belgium 712 553 324France 3 908 3 424 1 965Germany, Federal Republic of 4 339 3 079 2 383Luxembourg 28 22 11Netherlands 1 130 923 542Switzerland 461 396 289UNION OF SOVIET SOCIALIST REPUBLICS 20 923 13 818 7 544
Source: Derived from World populat ion prospects 1988. New York, 1 Affairs,
United1989Nations Department of International
(Population Studies No. 106).Economic and Socia

Table 12. Estimated and projected populations of major world regions,
1960> 1980, 2000, 2020, 2025 (In thousands)
Total population Persons 60 and over Code Region or country ____________________________________________________________ _________________________________________
i960 1980 2000 2020 2025 i960 1980 2000 2020 2025
810 Union of Soviet Socialist Republics 214 335 265 546 307 737 343 212 351 450 21 564 35 002 52 095 65 460 72 224900 World total 3 019 376 4 450 210 6 251 055 8 062 274 8 466 516 243 577 381 842 612 333 1 033 125 1 201 337901 More developed regions 944 851 1 136 406 1 262 482 1 340 063 1 352 087 118 524 173 453 235 666 317 732 342 743902 Less developed regions 2 074 525 3 313 804 4 988 573 6 722 211 7 114 430 125 053 208 389 376 667 715 393 858 594903 Africa 281 076 481 034 872 234 1 441 285 1 580 984 13 820 23 395 42 002 83 296 100 531904 Latin America 217 649 361 756 539 697 719 032 760 378 12 249 23 453 42 280 81 085 96 854905 Northern America 198 663 251 808 294 830 327 153 332 998 25 756 39 153 49 492 79 641 88 02 )906 Eastern Asia 791 292 1 176 115 1 501 277 1 693 806 1 728 571 57 956 92 563 168 080 295 856 346 22/908 Europe 425 070 484 436 508 569 513 811 512 290 61 312 81 824 102 536 129 167 1 38 171909 Oceania 15 782 22 794 30 139 37 349 38 964 1 708 2 660 3 932 6 442 7 208910 Eastern Africa 82 310 144 040 269 185 471 764 523 025 3 790 6 404 11 709 23 077 27 789911 Middle Africa 32 668 52 269 93 498 161 769 179 645 1 692 2 579 4 587 8 716 10 382912 Northern Africa 65 115 107 811 181 481 257 629 275 020 3 425 6 208 10 586 21 729 26 4 30913 Southern Africa 19 895 32 458 51 172 73 235 78 023 1 189 1 979 3 381 6 707 8 030914 Western Africa 81 088 144 455 276 898 476 887 525 271 3 725 6 224 11 739 23 067 27 901915 Caribbean 20 353 29 260 38 566 47 021 48 759 1 369 2 441 3 709 6 324 7 66 7916 Central America 50 456 92 677 145 125 200 157 213 186 2 515 4 706 9 476 19 775 24 174920 South-eastern Asia 224 605 360 063 523 814 668 733 700 545 12 015 20 489 37 263 72 317 88 203921 Southern Asia 595 049 948 413 1 502 312 2 054 594 2 173 801 33 821 57 628 103 931 198 541 237 934922 Western Asia 55 856 98 244 170 447 263 300 286 535 3 376 5 681 10 746 21 377 26 029923 Eastern Europe 96 713 109 397 117 112 122 554 123 292 12 323 16 485 21 028 27 499 28 627924 Northern Europe 75 647 82 494 84 995 85 899 85 752 12 405 16 363 17 161 21 817 23 524925 Southern Europe 118 197 138 806 148 768 150 707 150 271 14 587 21 117 30 315 37 059 40 221926 Western Europe 134 513 153 740 157 694 154 650 152 976 21 996 27 860 34 033 42 791 45 797927 Australia - New Zealand 12 687 17 808 22 242 25 972 26 753 1 553 2 453 3 511 5 661 6 278928 Melanesia 2 583 4 196 6 832 10 109 10 914 127 166 342 64 5 772931 South America 146 840 239 820 356 007 471 854 498 434 8 365 16 306 29 095 54 985 65 013935 Asia 1 666 801 2 582 836 3 697 849 4 680 433 4 889 452 107 170 176 361 320 020 588 092 698 392940 Korea 35 529 56 149 76 176 91 488 94 233 1 886 3 282 6 755 13 685 16 224954 Micronesia 194 316 436 522 534 9 17 33 62 70957 Polynesia 317 473 630 746 764 18 24 46 74 87
Source: Derived from World population prospects 1988. Neu York, United Nations Department of International Economic and Social Affairs 1989 (Population Studies No. 106).
EUR/RC40/Tech.Disc./l
0621B
page 35
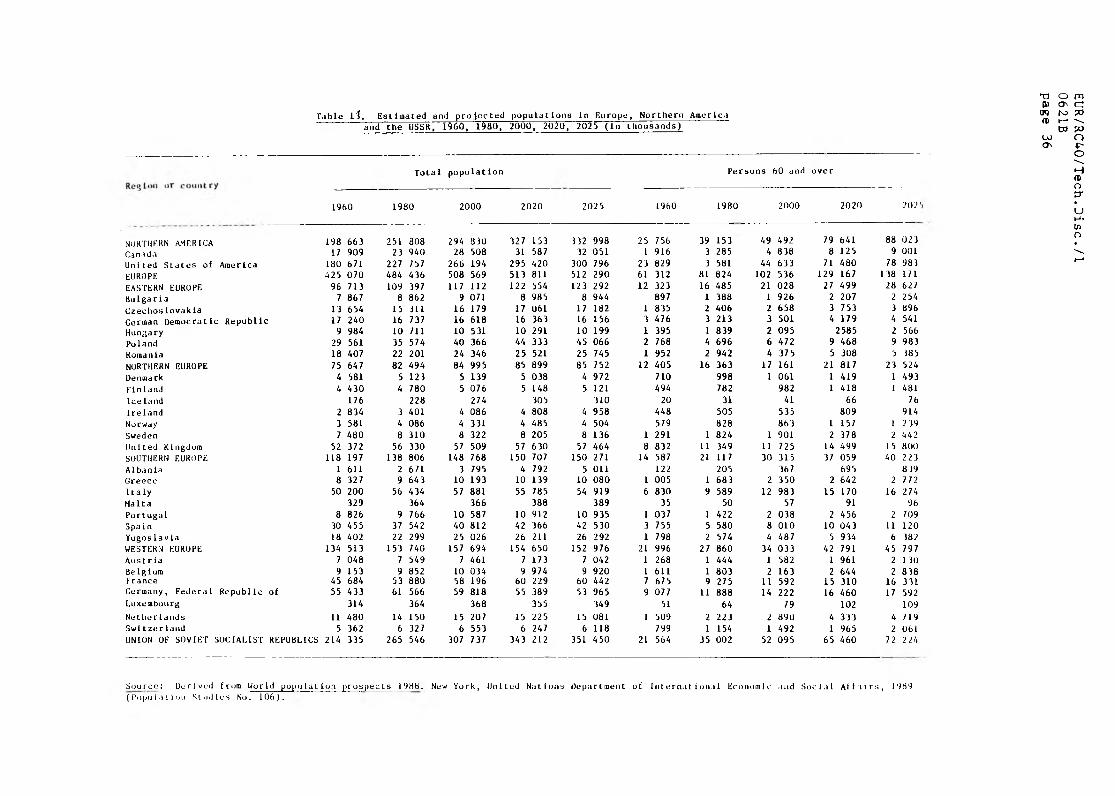
Table li. Estimated and projected populations in Europe, Northern America and the USSR, i960, 1980, 2000, 202q, 2025 (in thousands)
Total population Persons 60 and over
1960 1980 2000 2020 2025 I960 1980 2000 2020 202'
NORTHERN AMERICA 198 663 251 ao8 294 830 327 153 332 998 25 756 39 153 49 492 79 641 88 02 3
Canada 17 909 23 940 28 508 31 587 32 051 1 916 3 285 4 838 8 125 9 001
United States of America 180 671 227 757 266 194 295 420 300 796 23 829 3 581 44 633 71 480 78 983
EUROPE •125 070 484 436 508 569 513 811 512 290 61 312 81 824 102 536 129 167 138 171
EASTERN EUROPE 96 713 109 397 117 112 122 554 123 292 12 323 16 485 21 028 27 499 28 627
Bulgaria 7 867 8 862 9 071 8 985 8 944 897 1 388 1 926 2 207 2 254
Czechoslovakia 13 654 15 311 16 179 17 061 17 182 1 835 2 406 2 658 3 753 3 896
German Democratic Republic 17 240 16 737 16 618 16 363 16 156 3 476 3 213 3 501 4 179 4 541
Hungary 9 984 10 711 10 531 10 291 10 199 1 395 1 839 2 095 2585 2 566
Poland 29 561 35 574 40 366 44 333 45 066 2 768 4 696 6 472 9 468 9 983
Romania 18 407 22 201 24 346 25 521 25 745 1 952 2 942 4 375 5 308 5 385
NORTHERN EUROPE 75 647 82 494 84 995 85 899 85 752 12 405 16 363 17 161 21 817 23 524
Denmark 4 581 5 123 5 139 5 038 4 972 710 998 1 061 1 419 1 493
Finland 4 430 4 780 5 076 5 148 5 121 494 782 982 1 418 1 481
Ice land 176 228 274 305 310 20 31 41 66 76
I re 1 and 2 834 3 401 4 086 4 808 4 958 448 505 535 809 914
Norway 3 581 4 086 4 331 4 485 4 504 579 828 863 1 157 1 2 39
Sweden 7 480 8 310 8 322 8 205 8 136 1 291 1 824 1 901 2 378 2 442
United Kingdom 52 372 56 330 57 509 57 630 57 464 8 832 11 349 11 725 14 499 15 800
SOUTHERN EUROPE 118 197 138 806 148 768 150 707 150 271 14 587 21 117 30 315 37 059 40 223
Albania 1 611 2 671 3 795 4 792 5 011 122 205 367 695 819Greece 8 327 9 643 10 193 10 139 10 080 1 005 1 683 2 350 2 642 2 772
Italy 50 200 56 434 57 881 55 785 54 919 6 830 9 589 12 983 15 170 16 274
Malta 329 364 366 388 389 35 50 57 91 96
Portugal 8 826 9 766 10 587 10 912 10 935 1 037 1 422 2 038 2 456 2 709Spain 30 455 37 542 40 812 42 366 42 530 3 755 5 580 8 010 10 043 11 120
Yugoslavla 18 402 22 299 25 026 26 211 26 292 1 798 2 574 4 487 5 934 6 382
WESTERN EUROPE 134 513 153 740 157 694 154 650 152 976 21 996 27 860 34 033 42 791 45 797Austria 7 048 7 549 7 461 7 173 7 042 1 268 1 444 1 582 1 961 2 130Belglum 9 153 9 852 10 034 9 974 9 920 1 611 1 803 2 163 2 644 2 838France 45 684 53 880 58 196 60 229 60 442 7 675 9 275 11 592 15 310 16 331Germany, Federal Republic of 55 433 61 566 59 818 55 389 53 965 9 077 11 888 14 222 16 460 17 592Luxembourg 314 364 368 355 349 51 64 79 102 109
Ne t he r 1 ands 11 480 14 150 15 207 15 225 15 081 1 509 2 223 2 890 4 333 4 719Swltzerland 5 362 6 327 6 553 6 247 6 118 799 1 154 1 492 1 965 2 061UNION OF SOVIET SOCIALIST REPUBLICS 214 335 265 546 307 737 343 212 351 450 21 564 35 002 52 095 65 460 72 2 24
Source: Derived from World population prospects 198B. New York, United Nations Department of International Economic and Social Affairs, 1989 (Population Studies No. 106).
EUR/RC40/Tech.D
isc./I
0621B
page 36