osborn hepatitis b c - cecentral
TRANSCRIPT

HEPATITIS B AND C IN THE HIVPATIENT PRIMARY CARE PATIENT: PRIMARY CARE PEARLSMelissa Osborn, MDEmory University School of Medicine

Case 1: HBV Initial visit to clinic
26 yo BM 26 yo BM HIV dx 2006 while incarcerated; never in care
RF: heterosexual sexRF: heterosexual sex
No OIs or other PMH16 213138
4.0 291792.5
47.1
16.2
1.25102
13101
CD4 6 (0 7%)Tot Prot 8.1Albumin 4.5AST 35
CD4 6 (0.7%)HIV viral load 124,000 copies/mLHep A antibody negativeHBsAg positive
ALT 16Tot bili 0.6Alk phos 54
Anti-HBs negativeAnti-HBc positiveHCV antibody negative
Workup of the Newly Diagnosed H titi B P ti tHepatitis B Patient
Establish whether acute hepatitis B is presentEstablish whether acute hepatitis B is presentDetermine phase of chronic hepatitis BChronic active hepatitis BChronic active hepatitis B
e-antigen positivee-antigen negativeg gHepatitis B carrier
Evaluate for signs/symptoms of portal hypertension g / y p p ypand end-stage liver diseasePreventive health measures

Acute Hepatitis B Virus Infection with RecoveryTypical Serologic Course
Symptoms
HBeAg ti HB
Typical Serologic Course
HBeAg anti-HBe
Total anti-HBc
IgM anti-HBc
anti-HBsHBsAg
Tite
r
Window Period anti-HBsHBsAg Window PeriodOnly core antibody
0 4 8 12 16 20 24 28 32 36 52 100
Weeks after Exposure
0 4 8 12 16 20 24 28 32 36 52 100
CDC

Chronic Hepatitis B (sAg+) HBeAg
Anti-HBe
HBV DNA
ALTI Cl
Inactive Carrier
Immune Tolerant
Immune Clearance(eAg+ chronic hepatitis)
Reactivation (eAg- chronic hepatitis)
Adapted from Yim, Hepatology 2006; 43:S173-181

Determining Hepatitis B StatusStep 1.
Screening serologies(HBsAg, anti-HBs, anti-HBc)
HBsAg- HBsAg+ HBsAg-ganti-HBc+anti-HBs+
Chronic Hepatitis Bg
anti-HBc-anti-HBs+
Vaccinated ImmuneStep 2Resolved HBV Immune
Vaccinated ImmuneStep 2. Determine stage:
HBeAg, anti-HBe, HBV DNA
HBeAg+anti-HBe-
HBV DNA 20000 IU/ L
HBeAg-Anti-HBe+
HBV DNA 2000 IU/ L
HBeAg-anti-HBe+/-
HBV DNA 2000 IU/ LHBV DNA>20000 IU/mL HBV DNA <2000 IU/mLHBV DNA>2000 IU/mL
Chronic Hepatitis B, eAg+ Chronic Hepatitis B, eAg- Chronic Hepatitis B carrier

Physical Findings in Advanced Liver Disease
Caput Medusae
→→
←Ascitessc es
Spider angioma (telangiectasia) Palmar erythema

Physical Findings in Advanced Liver DiseasePitting Edema
Splenomegaly
Scleral Icterus

Preventive Health Measures
Serologies for Hepatitis A and CVaccination for hepatitis A if non-immuneCounseling on alcohol abstinencegAvoidance of other liver toxinsCaution against raw oysters (Vibrio vulnificus risk)Caution against raw oysters (Vibrio vulnificus risk)Counseling on sexual transmission of hepatitis B
HBV Vaccination for sexual partnersHBV Vaccination for sexual partners
Screening for liver cancer (HCC) indicated in only a MINORITY of hepatitis B patientsMINORITY of hepatitis B patients
Most do not need surveillance

Case 1: Additional Lab Results
HIV genotype wild-typeHIV genotype wild typeHBe-antigen positiveAnti HBe negativeAnti-HBe negativeHBV DNA 159,000,000 IU/mL

Hepatitis B: Initiation of Treatmentp
When to startWhen to startWhat to startMonitoring on therapyMonitoring on therapy

Available HBV Therapiesp
Active against HIV and Active against hepatitis B onlyhepatitis B
Lamivudine (LAM, 3TC)* Adefovir (ADV)*Lamivudine (LAM, 3TC)
Emtricitabine (FTC)
Tenofovir (TDF)*
Adefovir (ADV)
Telbivudine (LdT)*
Interferon-α2b*( )
Peg-interferon- α2a*
Entecavir (ETV)*
*FDA approved for hepatitis B
From the DHHS Guidelines…
Hepatitis B is an indication for the initiation of Hepatitis B is an indication for the initiation of antiretroviral therapy regardless of CD4 count

From the AASLD Guidelines on H titi BHepatitis B…
Lamivudine is not recommended as first-line therapy Lamivudine is not recommended as first line therapy for hepatitis B due to high resistance rates (which are even higher in coinfected patients)g p )Recommended first line agents are tenofovir and entecavirCombination therapy is not standard of care in monoinfected hepatitis B patients
Lok, Hepatology 2009; 507-39

Therapy of HIV/HBVpy /
Standard of care is to treat with a TruvadaStandard of care is to treat with a Truvada(tenofovir/emtricitabine)-based regimenHBV DNA should be monitored every three months HBV DNA should be monitored every three months until undetectable, then every six monthsIf initially HBeAg+, follow this annually for eAg loss If initially HBeAg+, follow this annually for eAg loss and conversion to e antibody

When to Refer
HBV virologic rebound while on Truvada or HBV virologic rebound while on Truvada or tenofovirEvidence of cirrhosis or end-stage liver diseaseEvidence of cirrhosis or end stage liver diseaseSuspected IRISPersistent or recurrent elevation of liver enzymes Persistent or recurrent elevation of liver enzymes despite HBV viral suppression
Suggestive of alternative causeSuggestive of alternative cause

Hepatitis B: Pitfalls and PearlspImmune reconsitution inflammatory syndrome
fEspecially if starting CD4<50HBV suppressed much slower than HIV
H l d ARTHeavy pre-exposure to lamivudine in ART-experienced patients
Lik l h b l i di i t t HBVLikely harbor lamivudine-resistant HBV
Changes in ART regimen: consider HBVM d i f i if l May need to continue tenofovir even if no longer effective for HIV
Entecavir and telbivudine cross resistant with Entecavir and telbivudine cross-resistant with lamivudine/emtricitabine

Case 2: Hepatitis C: To Treat or Not t T t?to Treat?
45 yo AAM with HIV diagnosed in 198945 yo AAM with HIV diagnosed in 1989Current ARVs: AZT/3TC/LPV/r
Hepatitis C genotype 1aHepatitis C, genotype 1a
140 110 1293
1975 915.4
Tot Prot 7 3CD4 543 (21%)
140
4.3 23
110
1.0
1293
1975.946.4
Tot Prot 7.3Albumin 3.9AST 51ALT 54
HIV viral load <40 copies/mLHCV viral load >10,000,000 IU/mLHep A antibody positiveHBsAg negative
Tot bili 0.5Alk phos 100
HBsAg negativeAnti-HBs positiveAnti-HBc positive
Hepatitis Cp
Selecting candidates for treatmentSelecting candidates for treatmentValue of liver biopsyWhen to referWhen to referScreening for HCC
WhWhoHow
A il bl t t t t t t i th i liAvailable treatments, treatments in the pipeline

Selecting Candidates for Treatment: F th AASLD G id liFrom the AASLD Guidelines…
“Hepatitis C should be treated in the HIV/HCV co-epa s C s ou d be ea ed e V/ CV coinfected patient in whom the likelihood of serious liver disease and a treatment response are judged to
h h k f b d f h d ffoutweigh the risk of morbidity from the adverse effects of therapy.”
Ghany, Hepatology; 2009; 49: 1335-74

Who are these patients?p
Higher risk for adverse events or
CD4>200 Cirrhosis
Most likely to benefitHigher risk for adverse events or treatment nonresponse
Fibrosis stage >F1Genotype 2 or 3
Genotype 1Low CD4 countyp
Non-cirrhotics Baseline anemiaBaseline Baseline thrombocytopeniaBaseline neutropeniaBaseline neutropeniah/o depression

Contraindications to Interferon/Ribavirin
AbsoluteD d li diDecompensated liver disease
Uncontrolled depression or psychiatric disease
Untreated thyroid disease
Pregnancy
Severe concurrent medical disease: CHF, sig CAD, poorly controlled DM, COPDCOPD
RelativeInadequate hematologic indices (Hb<13, ANC<1500, plts<75)
Cr>1.5
Active substance use
Inability to adhere to a complex medical regimenInability to adhere to a complex medical regimen
Other considerations
Patient motivationPatient motivationSocial supportFinances/payor sourceFinances/payor sourceJob status, ability to take leave if necessary

Do you really need a liver biopsy before treatment?before treatment?
PROSOnly reliable way to stage diseaseEstablish urgency of treatmentMy answer: NOIf therapy is difficult, helps to know how hard to push onwardEvaluate for other diseases
My answer: NOIndividualizedPatient inputCONS
Invasive procedure with risksM b l bl
Patient inputRisk vs Benefit
May not be availableDoesn’t change outcomeMay not change decision about whether to treatMay not change decision about whether to treat

Serum Markers of Fibrosis
AST-Platelet Ratio Index (APRI)AST Platelet Ratio Index (APRI)FIB-4 IndexForns IndexForns IndexSHASTA IndexFib Fib Fib HFibrotest, Fibrosure, Fibrometer, Hepascore
Can discriminate no fibrosis from advanced fibrosis but NOT good at discriminating F2-3Overlap in score between stages leads to misclassification
fibrosis but NOT good at discriminating F2-3
May have a role in stratifying who needs a biopsy

Current Standard Therapy: Pegylated Interferon + RibavirinPegylated Interferon + Ribavirin
Peg interferon α2b Peg interferon α2aPeg-interferon-α2b(PEG-INTRON)
Linear configuration, 12 kil d lt
Peg-interferon-α2a (PEGASYS)
Branched chain configuration, 40 kil d lt
OR
12 kilodaltonsWeight-based: 1.5 μg/kg/wk IM for geno 2,3
or 3 μg/kg/wk IM for other genos
40 kilodaltonsFixed dose of 180 μg IM per week
Both used in combination with ribavirin 800-1200Both used in combination with ribavirin 800 1200 mg divided bid depending on genotype and weight
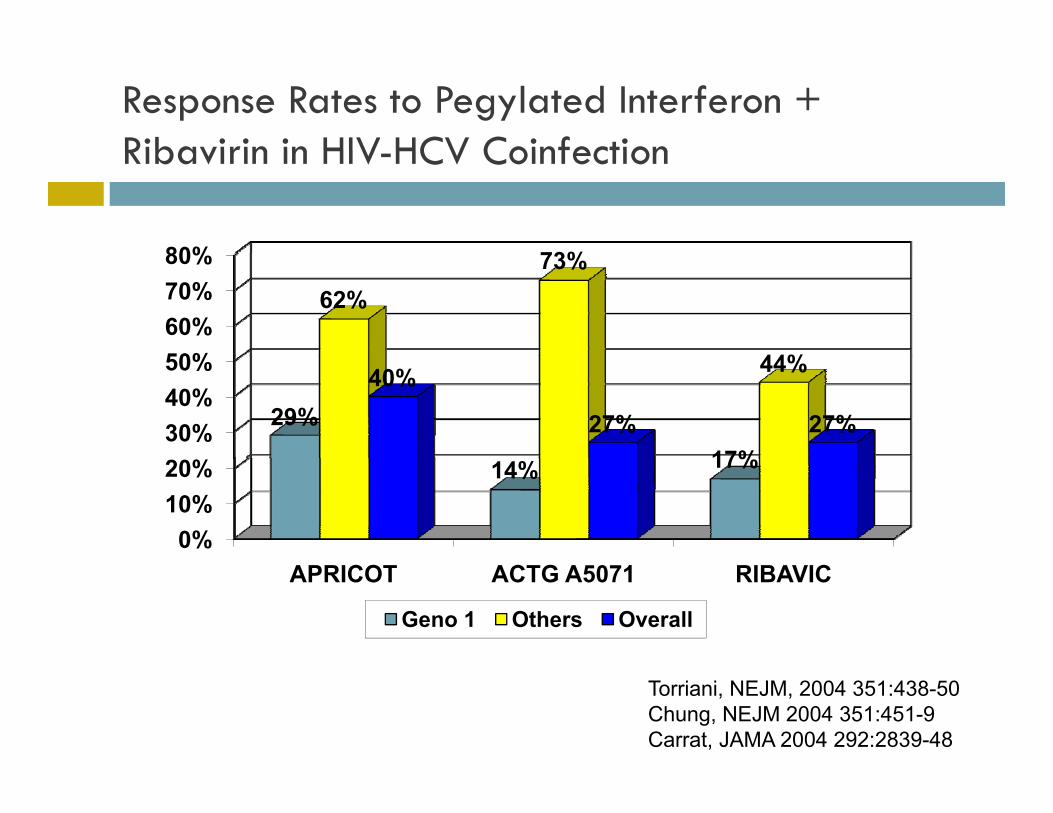
Response Rates to Pegylated Interferon + Ribavirin in HIV HCV CoinfectionRibavirin in HIV-HCV Coinfection
80% 73%
50%60%70%80%
62%73%
44%
30%40%50%
29%
17%
44%40%
27% 27%
0%10%20% 14% 17%
APRICOT ACTG A5071 RIBAVIC
Geno 1 Others Overall
Torriani, NEJM, 2004 351:438-50 Chung, NEJM 2004 351:451-9 Carrat, JAMA 2004 292:2839-48

Adverse Effects of Therapypy
Interferon Ribavirin
Flu-like symptomsMyalgias, arthralgias
Hemolytic anemiaN / i iFevers
Depression, irritability
Nausea/vomitingRash
Cognitive impairmentLeukopenia, thrombocytopenia
GoutMetallic taste in mouth
thrombocytopeniaFatigueThyroid dysfunction
Teratogenic
y yRetinopathy

When to Refer: Hepatitis Cp
Patients who meet criteria for treatment and are Patients who meet criteria for treatment and are interested in hearing pursuing treatmentEnd-stage liver diseaseEnd stage liver diseaseThose who have failed hepatitis C therapy previouslypreviously
?why did they fail
Detection of hepatocellular carcinomaDetection of hepatocellular carcinoma

Screening for HCCg
Indicated in hepatitis C with CIRRHOSISIndicated in hepatitis C with CIRRHOSISAASLD guidelines recommend surveillance using ultrasound every 6 monthsultrasound every 6 monthsAFP no longer recommended as a screening testAbnormal ultrasounds (nodule >1 cm) should be Abnormal ultrasounds (nodule >1 cm) should be followed up with contrast-enhanced MRI or 4-phase multidetector CT scanmultidetector CT scan
Bruix, Hepatology 2010; 52: 1-35

Who Has Cirrhosis?Histologically by biopsyRadiographicallyClinically: End-stage liver disease/portal h ihypertension
Ascites, esophageal varices, encephalopathy
C id i h i ( d h i ) i ti t Consider cirrhosis (and hence, screening) in patients with:
Thrombocytopenia (with no other explanation)Thrombocytopenia (with no other explanation)Splenomegaly (with no other explanation)Skin stigmata of liver diseasegStage III fibrosis on a liver biopsy >3-5 years ago with no intercurrent treatment

Hepatitis C: Pitfalls and Pearls
Consider acute hepatitis C with elevated LFTs and h/o d ( MSM)recent unprotected sex (esp among MSM)
Screen with HCV antibody and HCV viral loadC id l HCV tib d i t i k MSMConsider annual HCV antibody screen in at-risk MSM
Didanosine (absolute) and zidovudine (relative) are contraindicated with ribavirincontraindicated with ribavirin
Change regimen prior to HCV therapy
Do not be reassured by normal transaminases: Do not be reassured by normal transaminases: significant fibrosis can still be presentHCV RNA has normal variation – an increase or HCV RNA has normal variation an increase or decrease in viral load does not correlate with change in disease severity

Q i ?Questions?