ota · nonextensile approach to the posterior acetabular ... deep dissection ... ascending branch...
TRANSCRIPT

9/28/2015
1
Do We Need Specialty Plating for
Acetabular Fractures - Yes
Michael T. Archdeacon, M.D., M.S.E.
Peter J. Stern Professor & Chairman Department of Orthopaedic Surgery
University of Cincinnati Medical Center
September 28, 2015
Disclosure
Paid Consultant for Stryker
Royalties
Stryker; SLACK, Inc
Disclosure
Research Support:
OTA

9/28/2015
2
Disclosure
Deputy Editor:
JAAOS
Editorial Board:
JOT; JBJS; JOR; CORR
Anterior Approaches
AIP
AIP &
Lateral Window
Modified IL
Full IL
Least Exposure
Most Exposure
Posterior Column Stabilization
Posterior Column Lag Screw Often Placed Through
Secondary Lateral Window

9/28/2015
3
Plate Stabilization –
Posterior Column
Senior / Elderly Acetabulum Fx’s
Stabilization – Quad SurfaceMay Be Difficult Secondary To
Comminution / Osteoporosis
Multiple Plates May Be Required
Post Op
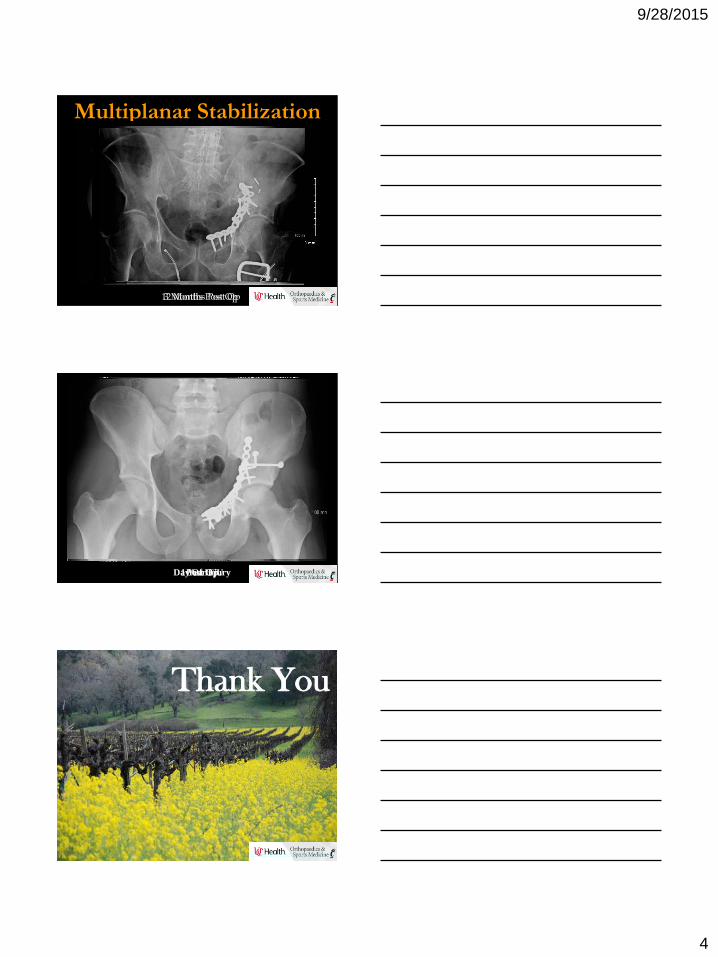
Multiplanar Stabilization –
Quad Surface Plating
9/28/2015
4
Multiplanar Stabilization
3 Months Post Op12 Months Post Op
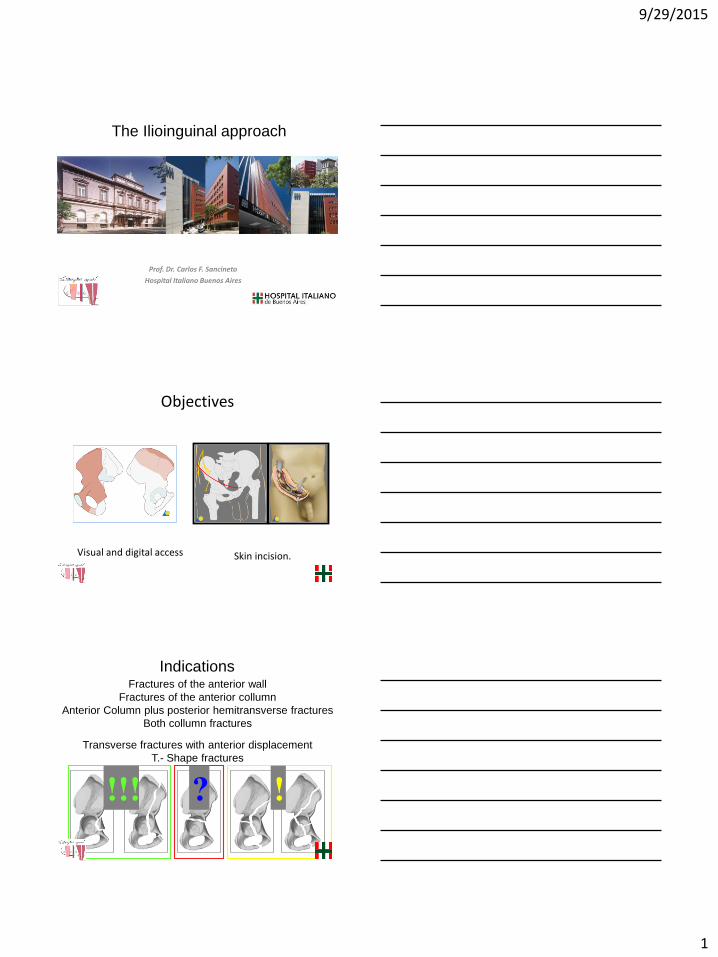
ACPHT AIP (Stoppa) Only
Day Of InjuryPost Op1 Year F/U
Thank You
9/29/2015
1
Prof. Dr. Carlos F. Sancineto
Hospital Italiano Buenos Aires
The Ilioinguinal approach
Visual and digital access Skin incision.
Objectives
IndicationsFractures of the anterior wall
Fractures of the anterior collumn
Anterior Column plus posterior hemitransverse fractures
Both collumn fractures
Transverse fractures with anterior displacement
T.- Shape fractures
!!! !?
9/29/2015
2
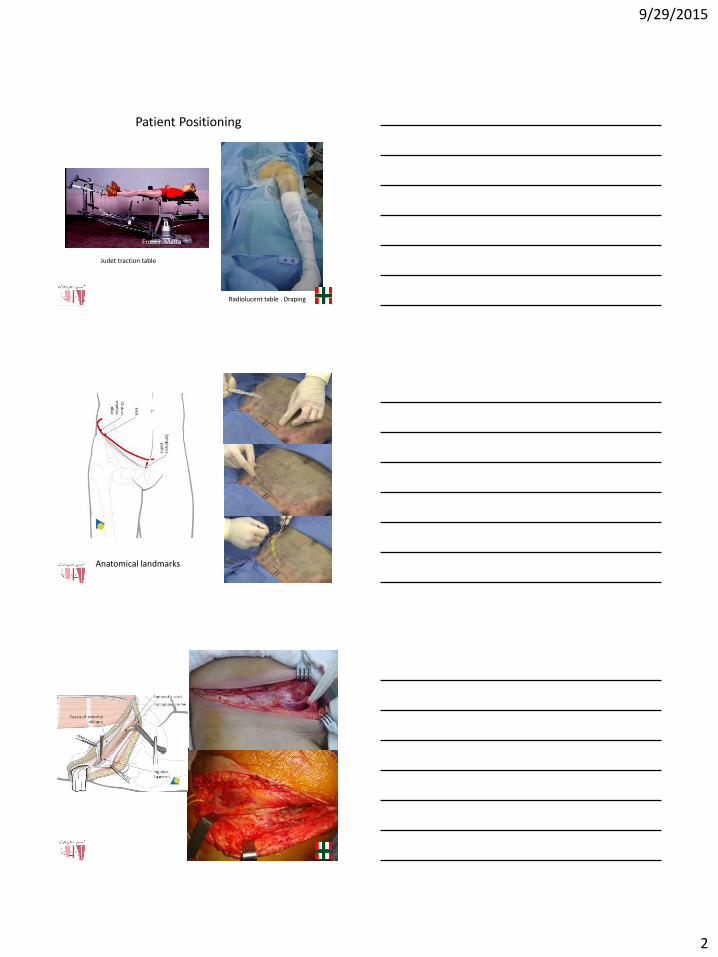
Patient Positioning
From J. Matta
Radiolucent table . Draping
Judet traction table
Anatomical landmarks

9/29/2015
3
Inguinal
Ligament

9/29/2015
4
Anteriorwall fracture.

9/29/2015
5
Associated Both Column
Fracture

9/29/2015
6
Associated Both Column
Fracture

9/29/2015
7
9/29/2015
8
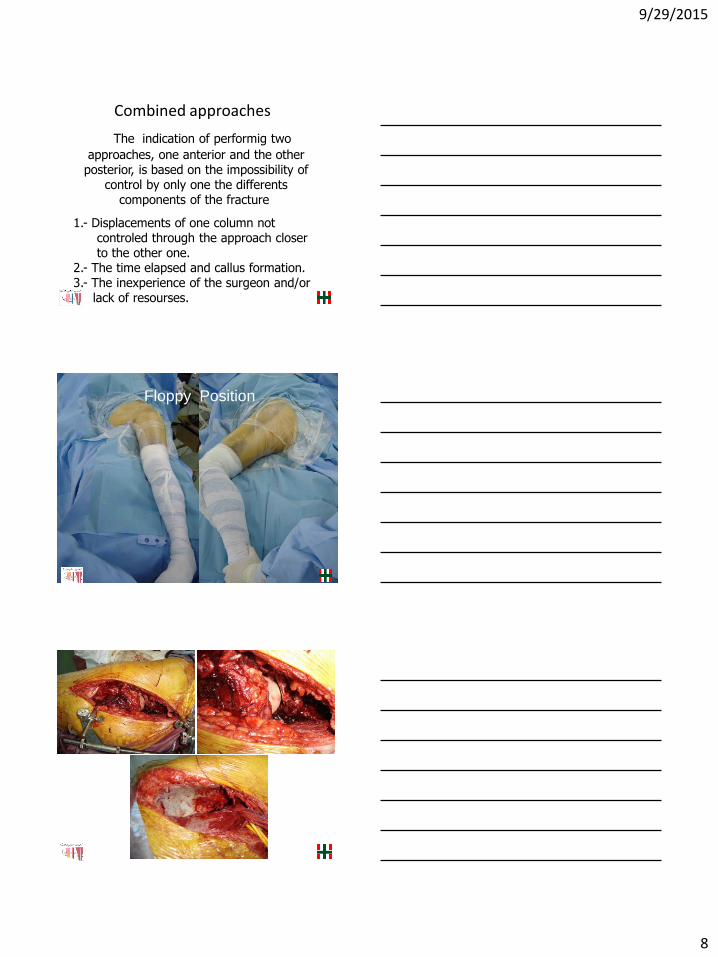
The indication of performig two
approaches, one anterior and the otherposterior, is based on the impossibility of
control by only one the differentscomponents of the fracture.
1.- Displacements of one column notcontroled through the approach closerto the other one.
2.- The time elapsed and callus formation.3.- The inexperience of the surgeon and/or
lack of resourses.
Combined approaches
Floppy Position
9/29/2015
9
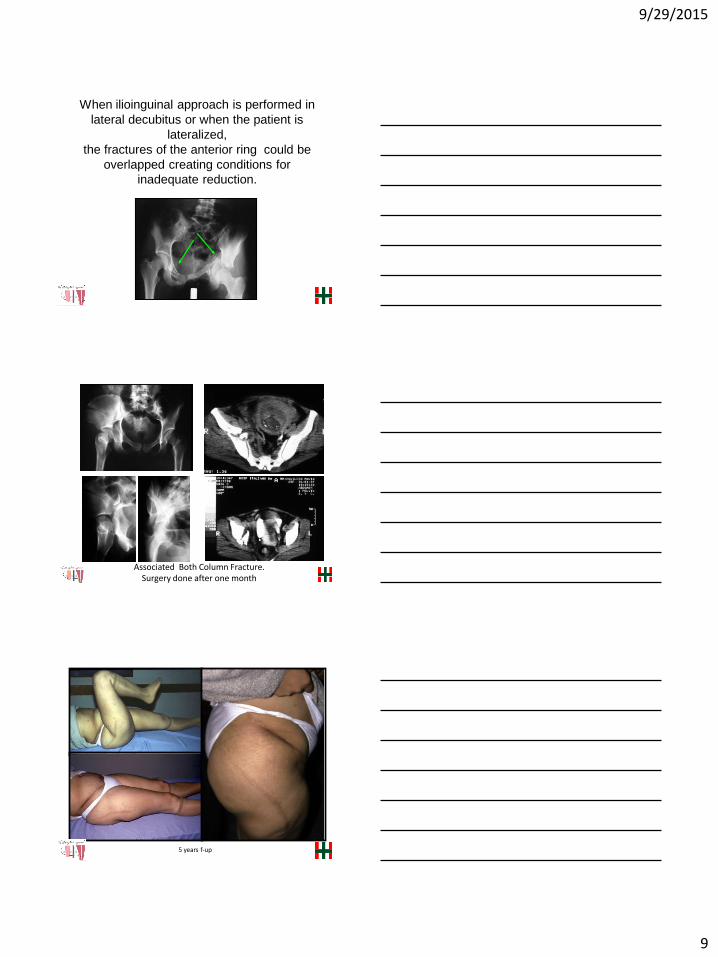
When ilioinguinal approach is performed in
lateral decubitus or when the patient is
lateralized,
the fractures of the anterior ring could be
overlapped creating conditions for
inadequate reduction.
Associated Both Column Fracture. Surgery done after one month
5 years f-up
9/29/2015
10
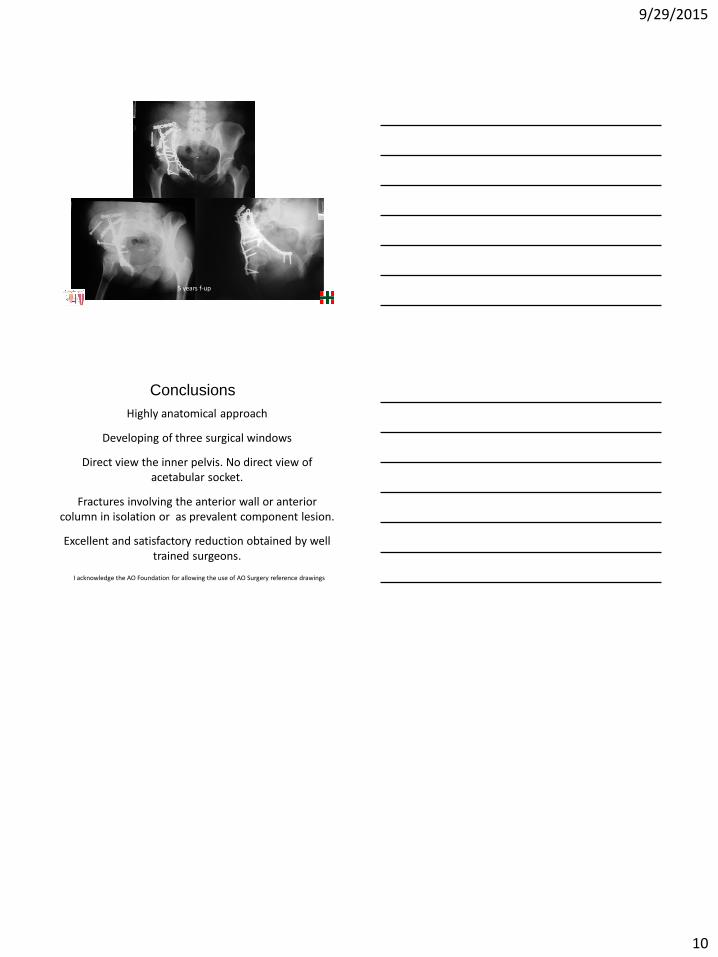
5 years f-up
Highly anatomical approach
Developing of three surgical windows
Direct view the inner pelvis. No direct view ofacetabular socket.
Fractures involving the anterior wall or anteriorcolumn in isolation or as prevalent component lesion.
Excellent and satisfactory reduction obtained by welltrained surgeons.
Conclusions
I acknowledge the AO Foundation for allowing the use of AO Surgery reference drawings
9/29/2015
1
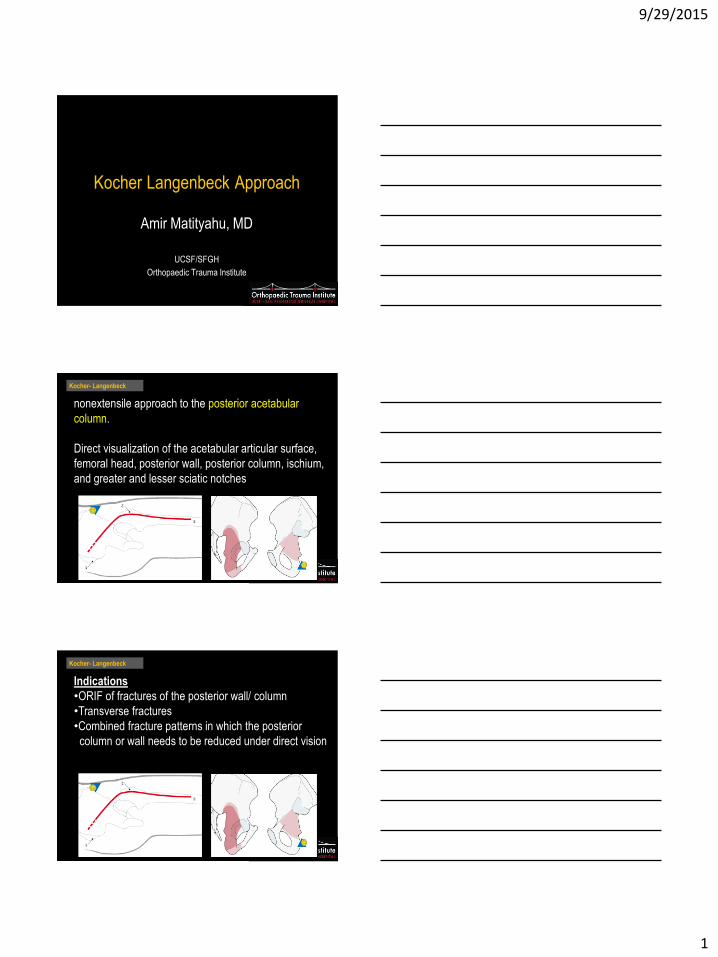
Kocher Langenbeck Approach
Amir Matityahu, MD
UCSF/SFGH
Orthopaedic Trauma Institute
nonextensile approach to the posterior acetabular
column.
Direct visualization of the acetabular articular surface,
femoral head, posterior wall, posterior column, ischium,
and greater and lesser sciatic notches
Kocher- Langenbeck
Indications
•ORIF of fractures of the posterior wall/ column
•Transverse fractures
•Combined fracture patterns in which the posterior
column or wall needs to be reduced under direct vision
Kocher- Langenbeck

9/29/2015
2
How to increase visualization
l Trochanteric osteotomy– Flip
– Slide
Login
ExecutiveEditor: PeterTraftonAuthors: KeithMayo, MichelOransky, PolRommens, CarlosSancineto
Acetabulum
Searchsearch...
ShortcutsAll PreparationsAll ApproachesAll Reductions &Fixations
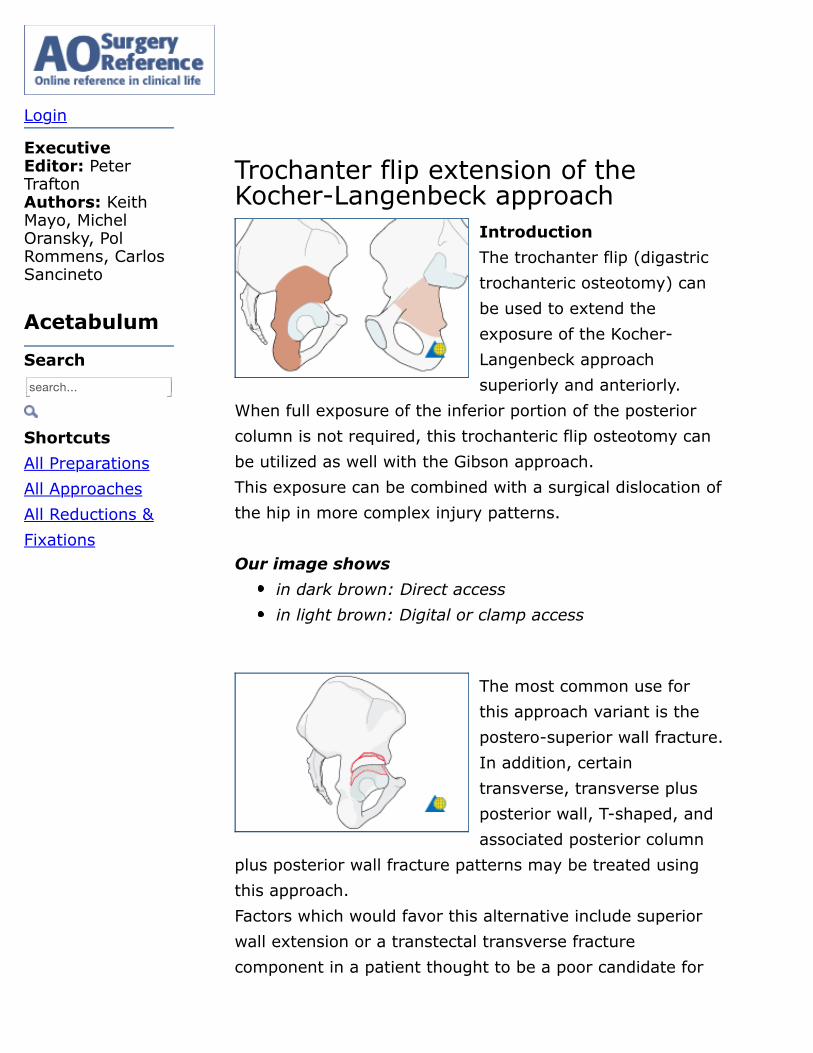
Trochanter flip extension of theKocher-Langenbeck approach
IntroductionThe trochanter flip (digastrictrochanteric osteotomy) canbe used to extend theexposure of the Kocher-Langenbeck approachsuperiorly and anteriorly.
When full exposure of the inferior portion of the posteriorcolumn is not required, this trochanteric flip osteotomy canbe utilized as well with the Gibson approach.This exposure can be combined with a surgical dislocation ofthe hip in more complex injury patterns. Our image shows
The most common use forthis approach variant is thepostero-superior wall fracture.In addition, certaintransverse, transverse plusposterior wall, T-shaped, andassociated posterior column
plus posterior wall fracture patterns may be treated usingthis approach.Factors which would favor this alternative include superiorwall extension or a transtectal transverse fracturecomponent in a patient thought to be a poor candidate for
in dark brown: Direct accessin light brown: Digital or clamp access
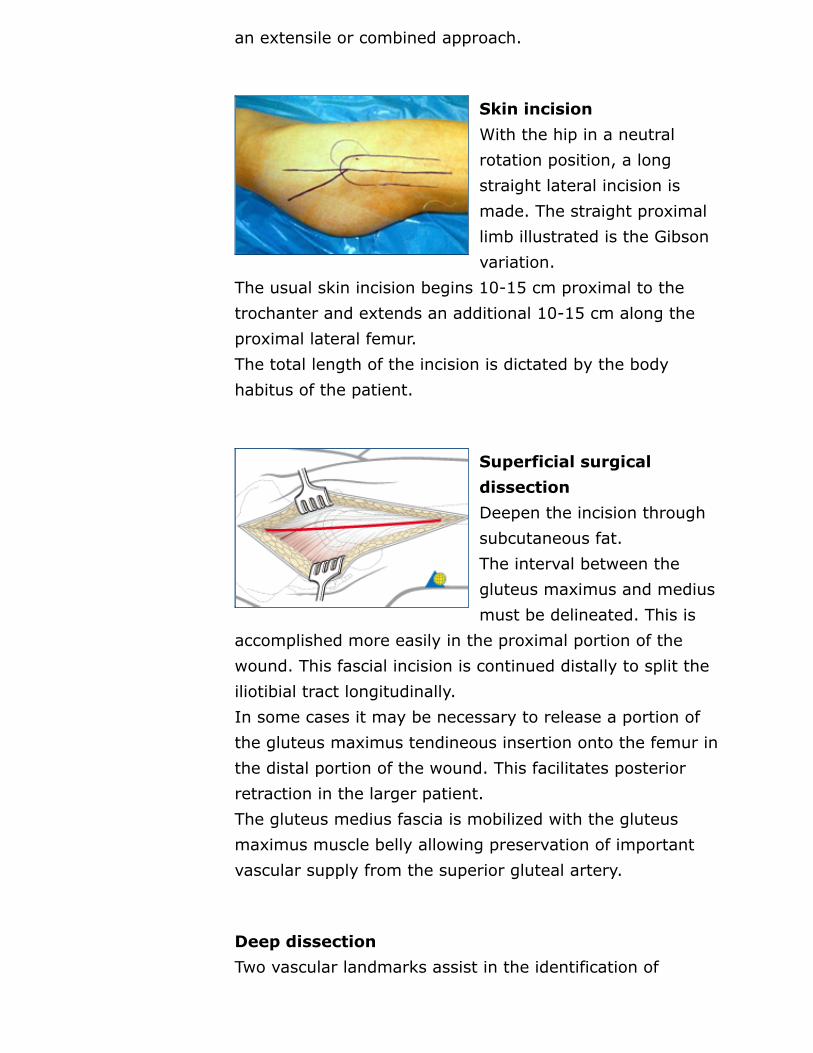
an extensile or combined approach.
Skin incisionWith the hip in a neutralrotation position, a longstraight lateral incision ismade. The straight proximallimb illustrated is the Gibsonvariation.
The usual skin incision begins 10-15 cm proximal to thetrochanter and extends an additional 10-15 cm along theproximal lateral femur.The total length of the incision is dictated by the bodyhabitus of the patient.
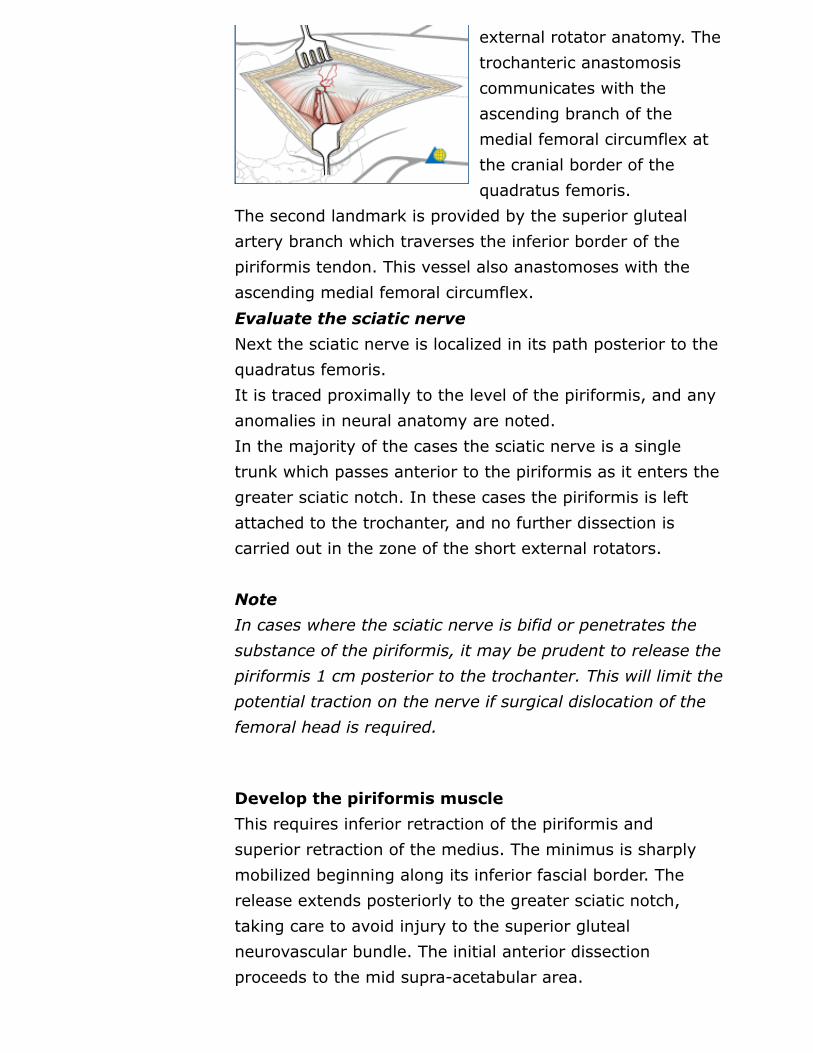
Superficial surgicaldissectionDeepen the incision throughsubcutaneous fat.The interval between thegluteus maximus and mediusmust be delineated. This is
accomplished more easily in the proximal portion of thewound. This fascial incision is continued distally to split theiliotibial tract longitudinally.In some cases it may be necessary to release a portion ofthe gluteus maximus tendineous insertion onto the femur inthe distal portion of the wound. This facilitates posteriorretraction in the larger patient.The gluteus medius fascia is mobilized with the gluteusmaximus muscle belly allowing preservation of importantvascular supply from the superior gluteal artery.
Deep dissectionTwo vascular landmarks assist in the identification of
external rotator anatomy. Thetrochanteric anastomosiscommunicates with theascending branch of themedial femoral circumflex atthe cranial border of thequadratus femoris.
The second landmark is provided by the superior glutealartery branch which traverses the inferior border of thepiriformis tendon. This vessel also anastomoses with theascending medial femoral circumflex.Evaluate the sciatic nerveNext the sciatic nerve is localized in its path posterior to thequadratus femoris.It is traced proximally to the level of the piriformis, and anyanomalies in neural anatomy are noted.In the majority of the cases the sciatic nerve is a singletrunk which passes anterior to the piriformis as it enters thegreater sciatic notch. In these cases the piriformis is leftattached to the trochanter, and no further dissection iscarried out in the zone of the short external rotators.
NoteIn cases where the sciatic nerve is bifid or penetrates thesubstance of the piriformis, it may be prudent to release thepiriformis 1 cm posterior to the trochanter. This will limit thepotential traction on the nerve if surgical dislocation of thefemoral head is required.
Develop the piriformis muscleThis requires inferior retraction of the piriformis andsuperior retraction of the medius. The minimus is sharplymobilized beginning along its inferior fascial border. Therelease extends posteriorly to the greater sciatic notch,taking care to avoid injury to the superior glutealneurovascular bundle. The initial anterior dissectionproceeds to the mid supra-acetabular area.

Develop the minimus-piriformis intervalNext the interval between thepiriformis and gluteusminimus is developed.This requires inferiorretraction of the piriformis.
The minimus muscle should be protected because it carriesthe circumflex vessels. It is sharply released from theretroacetabular surface.
Trochanteric osteotomyThe plane of the trochantericosteotomy is then preparedby cauterizing thetrochanteric anastomoticvessels.It may be useful to predrill
the trochanter for subsequent reattachment prior to theosteotomy.The osteotomy is then carried out from the tip of thetrochanter to the base of the vastus tubercle using a saline-cooled oscillating saw. A small portion of the medius tendonis left temporarily attached to the intact femur until thetrochanter can be mobilized. This provides an additional aidto prevent injury to the retinacular vessels caused by anexcessively thick osteotomy.
Anterior exposure andmobilization gluteusminimusThe vastus lateralis fascia isincised from the vastustubercle distally a distance of5-8 cm to allow extra
periosteal mobilization of the proximal lateralis muscle bellywith the trochanteric segment.The trochanter is progressively everted utilizing a Hohmannretractor placed over the anterior aspect of the greatertrochanter. Now, the small remaining gluteus mediusattachment to the intact trochanteric ridge is released. Attimes the piriformis insertion will be partially attached to themobile trochanteric fragment. This should be released as thetrochanter is everted.Flex and externally rotate the hip to improve anteriorexposure.This allows complete mobilization of the gluteus minimusfrom the retroacetabular surface along the superior capsuleto its femoral insertion along the anterior aspect of thetrochanter.The minimus insertion may also straddle the trochantericosteotomy. If so, it must be released from the intact femurto allow full trochanteric mobilization.
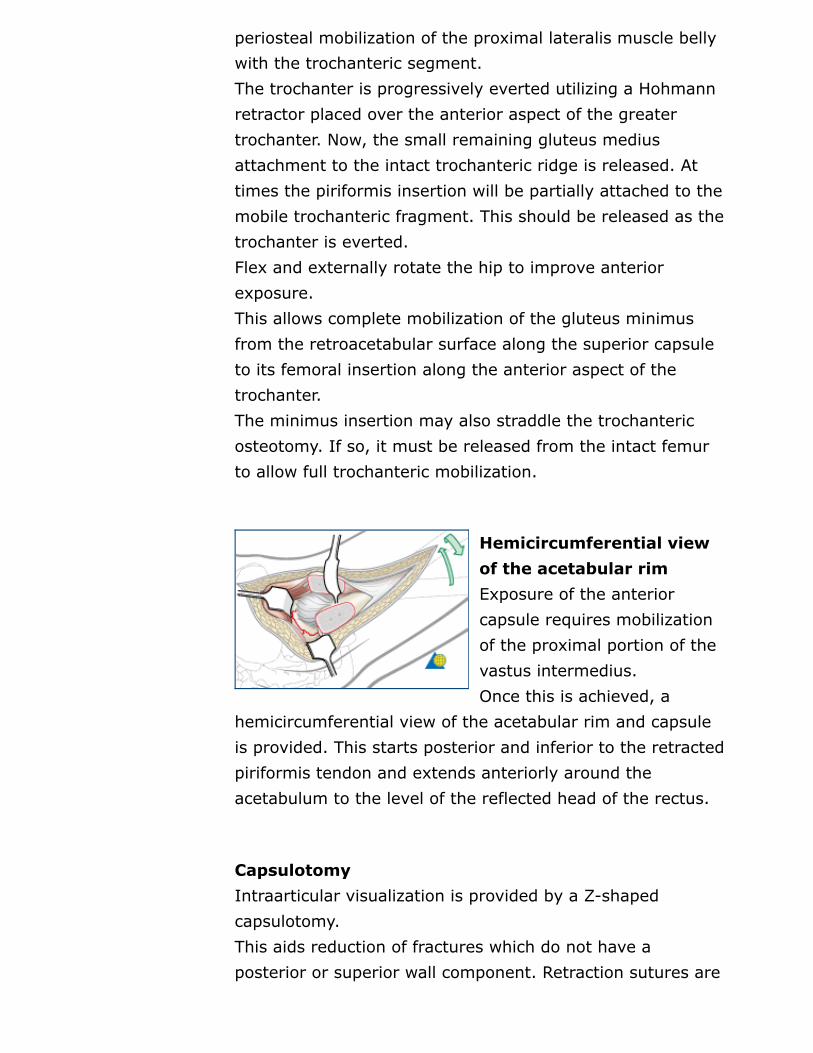
Hemicircumferential viewof the acetabular rimExposure of the anteriorcapsule requires mobilizationof the proximal portion of thevastus intermedius.Once this is achieved, a
hemicircumferential view of the acetabular rim and capsuleis provided. This starts posterior and inferior to the retractedpiriformis tendon and extends anteriorly around theacetabulum to the level of the reflected head of the rectus.
CapsulotomyIntraarticular visualization is provided by a Z-shapedcapsulotomy.This aids reduction of fractures which do not have aposterior or superior wall component. Retraction sutures are
useful.
Reflect the posterior wallfragmentWhen a posterior wall fractureis present, the capsularpedicle to the wall fragmentsmust be preserved. Thecapsulotomy is modified to
incorporate the posterior wall at its margin.The wall fragments are then reflected inferiorly to assist injoint visualization. The labrum is typically intact at theanterior aspect of the wall fragment, but is avulsed at thepostero-inferior margin.
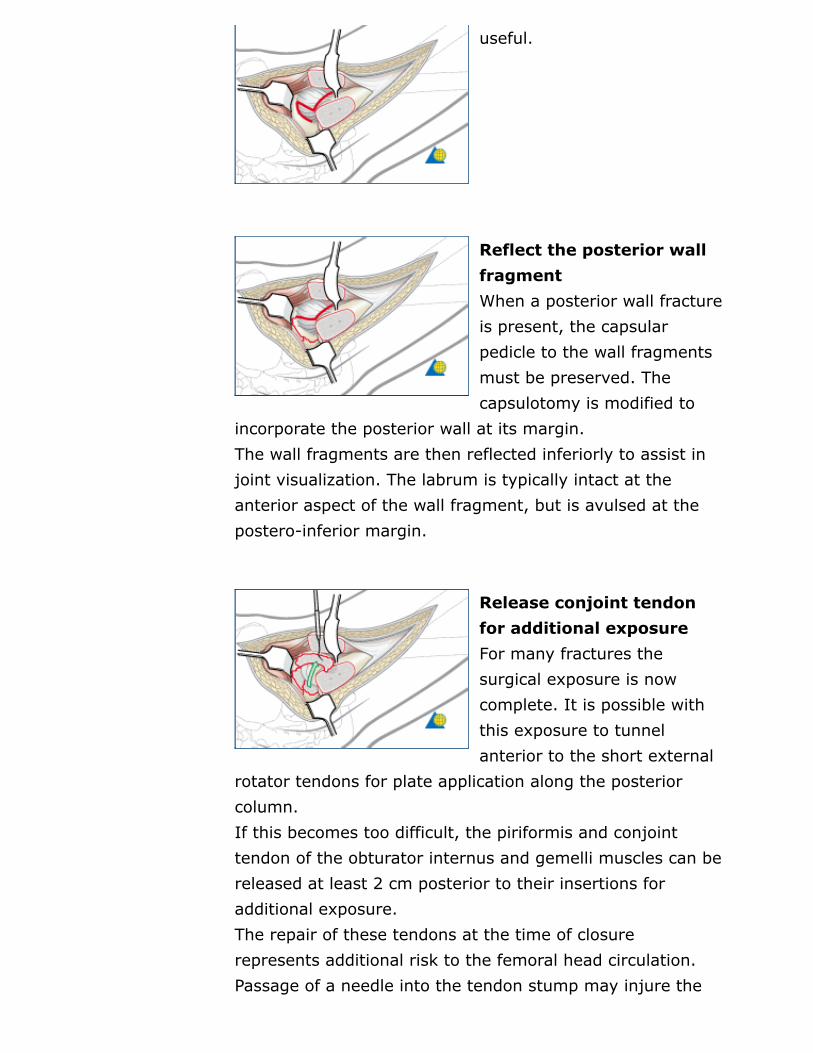
Release conjoint tendonfor additional exposureFor many fractures thesurgical exposure is nowcomplete. It is possible withthis exposure to tunnelanterior to the short external
rotator tendons for plate application along the posteriorcolumn.If this becomes too difficult, the piriformis and conjointtendon of the obturator internus and gemelli muscles can bereleased at least 2 cm posterior to their insertions foradditional exposure.The repair of these tendons at the time of closurerepresents additional risk to the femoral head circulation.Passage of a needle into the tendon stump may injure the

ascending branch of the medial femoral circumflex artery.
Dislocation of the hip joint“Figure of four” extensionof the approachMore complex fracturepatterns may requireextension of this approach toinclude anterior surgical
dislocation.This is accomplished by careful placement of the involvedlimb in a “figure-four” position (flexion to 90 degreescombined with adduction and external rotation).A sterile pouch is required for this maneuver. Divide theligamentum teres with a pair of curved scissors to reducethe force required for dislocation.
Dislocation of the femoralheadWith the femoral headdislocated, appropriateanterior and posteriorretraction provides apanoramic view of the joint.
Visualization of anterior column and limbDislocation is best used for visualization and reduction of the

anterior column or anterior limb of the ischiopubic segment.However, because of soft-tissue limitations it is usuallynecessary to relocate the hip to provide access for implantinsertion.The sequence of dislocation and reduction may have to berepeated multiple times during the reconstruction.
ClosureFor many fractures the surgical exposure is now complete.It is possible with this exposure to tunnel anterior to theshort external rotator tendons for plate application along theposterior column.If this becomes too difficult, the piriformis and conjointtendon of the obturator internus and gemelli muscles can bereleased at least 2 cm posterior to their insertions foradditional exposure.The repair of these tendons at the time of closurerepresents additional risk to the femoral head circulation.Passage of a needle into the tendon stump may injure theascending branch of the medial femoral circumflex artery. When the reconstruction is completed, the capsule is closedloosely to allow drainage of any secondary hemarthrosis. The trochanter is then reattached with lag screws. Thenumber (2-3) and diameter (3.5-4.0) of screws utilized isdependent on bone density.The vastus lateralis fascia is repaired and the short rotatortendons are reapproximated.Deep drains are placed as needed. The gluteus maximustendon is repaired, and lastly, the iliotibial tract and glutealfascia are closed.Subcutaneous drains follow, and subcutaneous and skinclosure are completed.
TweetTweet 0
0
v1.0 2007-07-220LikeLike
