ovarian cancer patients: influence of protein dose · c1'mol (hctmo1) to investigate its...
TRANSCRIPT

ICANCER RESEARCH56. 5179-5185. November 5, 19961
ABSTRACT
Thirty-one patients suspected of having ovarian cancer received asingle i.v. injection of radiolabeled (100 MBq ‘DIn)engineered humanC1'MOl (hCTMO1) to investigate its potential as an internalizing drugcarrier. hCTMO1 is a complementary-determining region-grafted humanIgG4 monoclonal antibody recognizing an ovarian carcinoma-associatedantigen, the MUC-1-gene product. The amount of radioactivity was determined in tumor tissue, various normal tissues, including liver biopsies,and blood samples obtained at laparotomy, 6 days after injection of either0.1 or 1.0 mg hCTMOlIkg of body weight.
Circulating antigen-15-3 was measurable in all patients before injection, and immune complex formation was already present at the end ofinfusion. In the 0.1 mglkg group, most of the radioactivity was bound toimmune complexes, whereas in the 1.0 mg/kg group, most was bound toIgG monomers. Increasing the hCTMO1 dose 10-fold did not influence theoverall disappearance of “Infrom the blood, but the elimination half-lifeof @‘indiumbound to immune complexes was increased 2-fold.
Uptake in tumor tissue 6 days postinjection at the 0.1 mg/kg dose was
7.6 times higher (P = 0.0009) than in normal tissue and 2.5 times higher
(P = 0.03) than in blood. At the 1.0 mg/kg dose, the uptake in tumor tissuewas 14.0 times higher (P 0.0003) than in normal tissue and 8.1 timeshigher (P = 0.0007) than in blood. Liver activity was substantial(23.7 ± 10.5 and 18.3 ±6.7% of the injected dose/kg for the 0.1 and 1.0
mgfkg dose group, respectively).
These results are superior to those found with other clinically testedanti-MUC-1 gene product antibodies. hCTMO1 seems to be a suitableearner for cytotoxic agents in ovarian carcinoma patients; the betteruptake results and tumor-to-blood ratios are obtained at the higher doseof 1.0 mg hCTMOlIkg body weight.
INTRODUCTION
Ovarian carcinoma is the leading cause of death from gynecologicalmalignancies and is the fourth most common malignancy in women.Despite a 70% response rate of platinum-based chemotherapy aftercytoreductive surgery, the 5-year survival rate is only 30% and the10-year survival rate is 20% (1, 2). Most patients have advanceddisease (stage III or IV) at the time of diagnosis. For these stages, the
5-year survival rate is only 5—20%.Most patients require second-linechemotherapy treatment for a relapse of the disease. In many instances, the tumor will become platinum-resistant, for which taxanes,a class of new chemotherapeutic agents, will probably be only apartial solution (3). Because current treatment regimens for ovariancancer are highly toxic and ultimately ineffective, many investigationshave been conducted to develop equally effective or more effectivetherapy of ovarian carcinoma with reduced side effects. One line ofinvestigation is the application of MAbs to more selectively directchemotherapeutic agents to tumor cells, thus limiting systemic expo
Received 6/I 8/96; accepted 9/16/96.The costs of publication of this article were defrayed in part by the payment of page
charges. This article must therefore be hereby marked advertisement in accordance with18 U.S.C. Section 1734 solely to indicate this fact.
I To whom requests for reprints should be addressed.
sure (4—6). We have investigated the biodistribution of engineered
hCTMO12 in ovarian carcinoma patients after i.v. administration.More than 90% of ovarian carcinomas express the MUC- 1 gene
product, recognized by hCTMO1, and therefore this antigen may be asuitable target for antibody-guided therapy in ovarian cancer patients(7—9).Previously, CTMO1-like antibodies have been successfullyused in treating ovarian cancer both in experimental and clinicalsettings (10, 1 1). The MUC-1 gene product is known under various
names [e.g., EMA, HMFG, MAM-6, CA 15—3,PEM, and episialin(12)]. In this article, we will use the term “PEM.―The antigen ispresent on the apical surface of most Secretory epithelia and overex
pressed on malignancies derived from these epithelia (8). PEM isinternalized continuously and recycled (13) and is shed into thecirculation, where it can be measured using one of the double
determinant commercially available CA15-3 assays. In breast cancerpatients, the CAI5-3 assay is used to monitor the disease (14).
In 1988, Aboud-Pirak et al. (15) developed and characterized amurine MAb CTMO1 reactive with the MUC-] gene product. ThisMAb was used to construct an immunoconjugate with a potentiallyhighly toxic antibiotic, calicheamicin ( 16). Significant growth inhibition in vitro and complete tumor remissions in animals bearing human
breast cancer xenografts have been demonstrated (16). To overcomethe problem of the induction of human antimouse antibodies and to beable to repetitively use the MAb in patients, CTMO1 has beenhumanized using complementary-determining region graft technology(17).
In the present study, patients with intra-abdominal tumor and suspected of having primary or recurrent ovarian carcinoma received i.v.
injections of hCTMO1 before cytoreductive surgery. The MAb waslabeled with a tracer dose of ‘@ ‘In,allowing the evaluation of two doselevels of the antibody on kinetics and tissue biodistribution as a
prelude to future therapy studies in ovarian carcinoma patients with ahCTMO1-antitumor antibiotic conjugate.
MATERIALS AND METHODS
Patient Population and Study Design. Thirty-onepatients (mean age,59.7 years; range, 30—80 years) strongly suspected of having primary or
recurrent ovarian cancer, as suggested by ultrasound, computed tomography,magnetic resonance imaging, or CAl 25 serum profile, and who were sched
uled to undergo surgery were entered in the study after giving informedconsent (Table I). The protocol was approved by the Dutch and English Health
Authorities and by the institutional review boards of the Free UniversityHospital, Amsterdam, the Netherlands, and Queen's Medical Center, Nottingham, United Kingdom. Patients had a life expectancy of at least 3 months anda WHO performance status of 0—3.
Fifteen patients received 0.1 mg/kg hCTMOI, and an additional 16 patientsreceived 1.0 mg/kg. Patients were operated on at day 6 p.i. Operations on
patients 5, 21, 27, and 28, as shown in Table 1, were performed on day 5 or
2 The abbreviations used are: hCTMOI, human CTMO1 ; CA, circulating antigen;
CEA,carcinoembryonicantigen;MAb,monoclonalantibody;PEM,polymorphicepithehal mucin; p.i., postinjection; %ID, percentage of injected dose.
5179
Biodistribution of 111lndium-.labeled Engineered Human Antibody CTMO1 in
Ovarian Cancer Patients: Influence of Protein Dose
Arjan C. van Hof, Carla F. M. Moithoff, Quentin Davies, Alan C. Perkins, RenéH. M. Verheijen, Peter Kenemans,'Wim den Hollander, Abraham J. Wilhelm, Terry S. Baker, Mark Sopwith, Malcolm Frier, E. Malcolm Symonds,and Jan C. Roos
Departments of Obstetrics and Gynecology IA. C. s'. H., C. F. M. M., R. H. M. V., P. K.J, Nuclear Medicine [W. d. H., J. C. RI, and Pharmacy [A. J. Wi. University Hospital VrijeUniversiteit, 1007 MB Amsterdam, the Netherlands; Departments of Obstetrics and Gynecology [Q. D., E. M. S.J and Nuclear Medicine fM. F., A. C. P.]. Queen ‘sMedical Center,Nottingham, NG7 2UH, United Kingdom; and Celltech Therapeutics, Slough SLJ 4EN. United Kingdom fT. S. B., M. S.]
on April 29, 2020. © 1996 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
TableIPatient characteristicsBaselineTime
ofPatientAgeHistologyandCA15-3operationno.(yr)DiagnosisgradeFIGO―(units/mi)(days
p.i.)0.1
mg/kg155ResidualSerous,GillIlib4562
3b57 71PrimaryPrimary(+ borderline)Serous,
GIllMucinous,01IHc Ia500 1066455BorderlineSerousIa236566BorderlineMucinousIa215672BorderlineMucinousIllc246752RecurrenceSerous,
GillilIb206870BenignSeromucinous18569
10―4863PrimaryNEDSerous,Gill
Hemangioma11Th18 25661146PrimaryClear cell,GilIc13761272ResidualSerous,
Gillhe28561345ResidualSerous,GIlltIle4461454RecurrenceSerous,GIllhe4661561RecurrenceSerous,
GilHe2761.0
mg/kg1666BorderlineMucinousIa2461759RecurrenceSerous,
GIl!Ic861827PrimarySerous,Gilllie7361948PrimarySerous,0111th3162062PrimarySerous,
Gil11th11962172BenignMucinous
cystadenoma3052250RecurrenceSerous,Gillific3862384PrimarySerous,Gifiific13162469PrimarySerous,GillIc5962559PrimarySerous,Gillific15862642BenignEndometriosis962767BorderlineMucinousIa1782843OtherUterine
sarcoma10852964PrimaryMMTifi2163048BenignEndometriosis1363172PrimaryClear
cell ca Gill3006
ENGINEERED hCTMOI IN OVARIAN CANCER PATIENTS
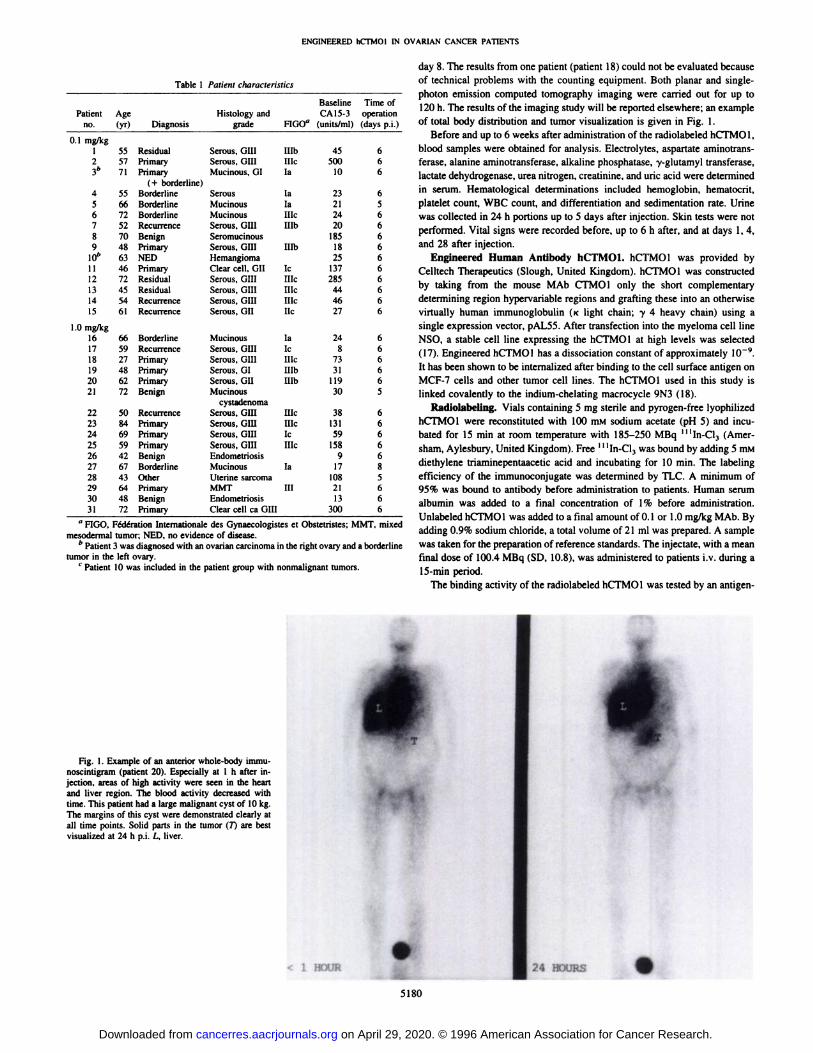
day 8. The results from one patient (patient 18)could not be evaluated becauseof technical problems with the counting equipment. Both planar and singlephoton emission computed tomography imaging were carried out for up to120h. The results of the imaging study will be reported elsewhere; an exampleof total body distribution and tumor visualization is given in Fig. 1.
Before and up to 6 weeks after administration of the radiolabeled hCTMO1,blood samples were obtained for analysis. Electrolytes, aspartate aminotransferase, alanine aminotransferase, alkaline phosphatase, y-glutamyl transferase,lactate dehydrogenase, urea nitrogen, creatinine, and uric acid were determinedin serum. Hematological determinations included hemoglobin, hematocrit,platelet count, WBC count, and differentiation and sedimentation rate. Urinewas collected in 24 h portions up to 5 days after injection. Skin tests were notperformed. Vital signs were recorded before, up to 6 h after, and at days 1, 4,and 28 after injection.
Engineered Human Antibody hCTMO1. hCTMO1 was provided byCelltech Therapeutics (Slough, United Kingdom). hCTMO1 was constructedby taking from the mouse MAb CTMOI only the short complementarydetermining region hypervariable regions and grafting these into an otherwisevirtually human immunoglobulin (ic light chain; y 4 heavy chain) using asingle expression vector, pAL5S. After transfection into the myeloma cell lineNSO, a stable cell line expressing the hCTMO1 at high levels was selected(17). Engineered hCTMO1 has a dissociation constant of approximately l0@.
It has been shown to be internalized after binding to the cell surface antigen onMCF-7 cells and other tumor cell lines. The hCTMO1 used in this study islinked covalently to the indium-chelating macrocycle 9N3 (18).
Radiolabeling. Vials containing 5 mg sterile and pyrogen-free lyophilizedhCTMO1 were reconstituted with 100 mM sodium acetate (pH 5) and incubated for 15 mm at room temperature with 185—250MBq ‘‘‘In-Cl3(Amersham, Aylesbury, United Kingdom). Free ‘‘‘In-Cl3was bound by adding 5 mMdiethylene triaminepentaacetic acid and incubating for 10 mm. The labelingefficiency of the immunoconjugate was determined by TLC. A minimum of95% was bound to antibody before administration to patients. Human serumalbumin was added to a final concentration of 1% before administration.Unlabeled hCTMO1 was added to a final amount of 0.1 or 1.0 mg/kg MAb. Byadding 0.9% sodium chloride, a total volume of 21 ml was prepared. A samplewas taken for the preparation of reference standards. The injectate, with a meanfinal dose of 100.4 MBq (SD, 10.8), was administered to patients iv. during a15-mm period.
The binding activity of the radiolabeled hCTMO1 was tested by an antigen
apj@ F6dérationInternationaledesGynaecologistesetObstetristes;MMT,mixedmesodermal tumor; NED, no evidence of disease.
b Patient 3 was diagnosed with an ovarian carcinoma in the right ovary and a borderline
tumor in the left ovary.C Patient 10 was included in the patient group with nonmalignant tumors,
Fig. 1. Example of an anterior whole-body immunoscmntigram(patient 20). Especially at 1 h after injection, areas of high activity were seen in the heartand liver region.The bloodactivitydecreasedwithtime.Thispatienthada largemalignantcystof 10kg.Themarginsof thiscystweredemonstratedclearlyatall time points. Solid parts in the tumor (7) are bestvisualized at 24 h p.i. L, liver.
24 IEXJRS •@iwxm
5180
on April 29, 2020. © 1996 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
ENGINEERED hCTMOI IN OVARIAN CANCER PATIENTS
coated bead assay. Briefly, PEM-coated polystyrene beads were incubated forI h at room temperature with 300 pA 1:30,000 diluted ‘‘‘In-hCTMOlinPBS/0.l% Tween 20. After washing the beads with PBS/0.l% Tween 20, theradioactivity bound to the beads was counted in a gamma-well counter (Cornpugamma, Wallace, Turku, Finland). Taking into account the labeling effi
ciency as obtained by TLC, the binding activity of the injectate was calculated.
Pharmacokinetics. Serial blood samples were drawn at completion of theinfusion and 1, 3, 6, 24, 96, and 144 h p.i. Urine was collected in portions of24 h up to 120 h p.i. to determine renal excretion of ‘‘‘In.The amount of
radioactivity in blood, plasma, and urine was measured in a gamma-wellcounter and expressed as %ID/ml. Corrections were performed for backgroundand decay. Size exclusion chromatography (silica-based gel filtration highperformance liquid chromatography) was used to determine the amount ofradiolabeled free hCTMOI and immune-complexed hCTMO1 in patientplasma samples. The plasma clearance of the hCTMOI and its immunecomplexes was analyzed using a model-dependent two-compartment nonlinearestimation program (MW Pharm, MediWare, Groningen, the Netherlands).
Within 4 h before injection and 1, 4, and 7 days after injection, blood samples
were taken to determine the amount of CA using the CA15-3assay (CentocorCA15-3 RIA; observed CAI5-3 concentration in normal serum and plasmasamples is 13.0 ±7.9 units/ml).
Tissue Distribution. At laparotomy, tumor lesions as well as various
normal tissues were removed or biopsied. When feasible, a liver biopsy wastaken. Tissues and blood were weighed, and the amount of radioactivity was
determined in a gamma-well counter and expressed as %lDfkg of tissue. Theuptake in normal tissues was calculated as the mean uptake in peritoneurn,muscle, fat, and skin. Corrections for decay, background, self adsorption, andradiation scatter (by measuring different volumes of the reference standards)
were applied.All samples were processed for routine histopathology and immunohisto
chemistry. For immunohistochemistry, freshly frozen tissue sections werefixed with acetone for 10 mm, air dried, washed with PBS, and incubated withbiotinylated hCTMOI or biotinylated negative control antibody for 60 mm atroom temperature. After washing, the sections were incubated for 5 mm withstreptavidin and for 15 mm with amino-ethylcarbazole (Zymed, Uden, theNetherlands). After washing with distilled water, tissue sections were counterstained with hematoxylin and mounted in aquamount (Zymed).
Statistical Analysis. The Wilcoxon rank test was used to analyze the
statistical differences between tissue uptakes for hCTMOI at both dose levels.
RESULTS
Radiolabeling. The mean labeling efficiency as determined byTLC was 98.0% (SD, 1.2; range, 95.0—99.9). The mean bindingactivity as determined by the antigen-coated bead assay was 75.1%bound hCTMO1 (SD, 6.0; range, 64.9—86.1).
Patients. No significant changes were noted in vital signs andhematological or biochemical serum and urine profiles at any timeafter administration. Administration of ‘@ ‘In-hCTMOI was uneventful in 30 of 31 patients. One h after injection, fever developed in onepatient; the fever persisted for 3 h and did not require medicalintervention. Of the 31 patients injected, 19 proved to have an ovarianmalignancy (Table 1). Eighteen patients had ovarian carcinoma; onepatient with a mixed MUllerian tumor of the ovary was included in theovarian carcinoma group. Five patients had borderline ovarian tumors,four patients had benign cystic ovaries, and one patient with highsuspicion of residual tumor after chemotherapy had no tumor atoperation, but a large hemangioma in the liver was found. One patienthad a leiomyosarcoma of the uterus. The patient whose data could notbe evaluated (patient 18) had ovarian carcinoma.
Pharmacokinetics. CAl 5-3 levels were measurable in all patientsbefore injection with a mean of 82.9 and 71 .0 units/mI in the 0.1mg/kg and 1.0 mg/kg dose group, respectively, which were notsignificantly different. High-performance liquid chromatography
analysis of plasma samples was performed to investigate the amountof monomeric IgG, aggregates, and breakdown products. All patients
50 1
Time after administration (h)150
A@1
CC0@0
VCUCC
C
0
B@!3°
C -C0V
.@ 20
UCC
C 10.C
0
* 0@0
B
A—@
50 100
Time after administration (h)
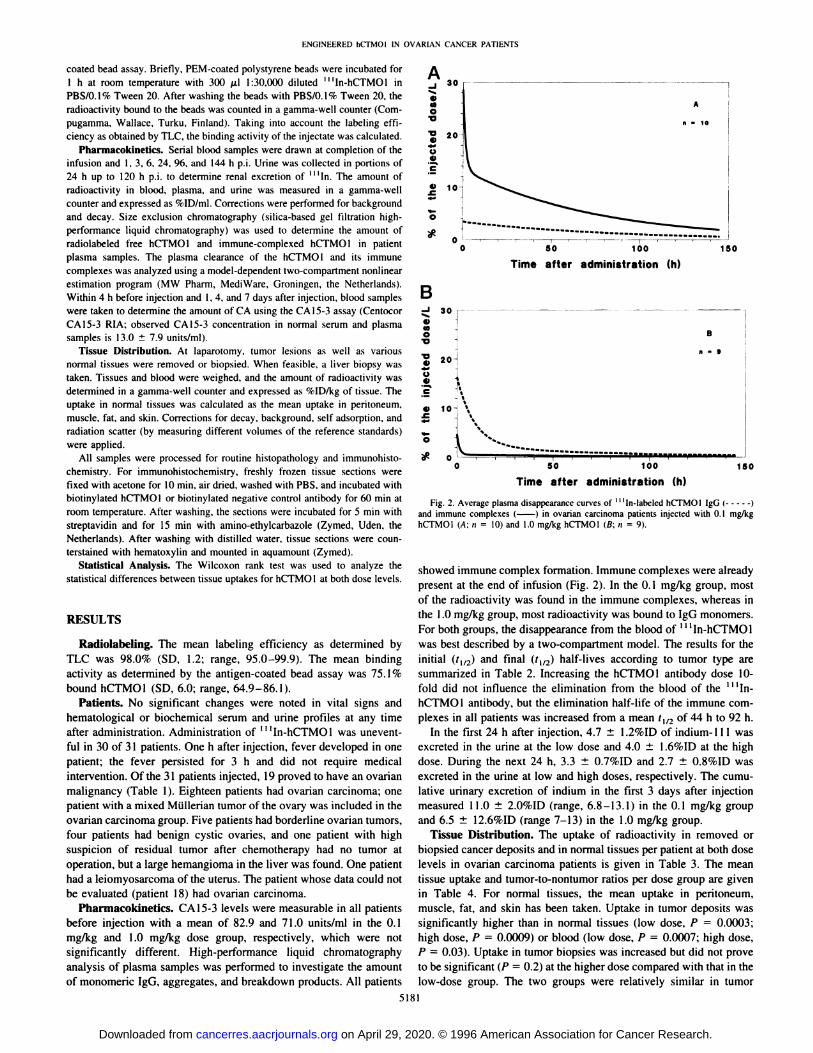
Fig. 2. Average plasma disappearance curves of ‘@ ‘In-labeledhCTMOI lgG (and immune complexes (—) in ovarian carcinoma patients injected with 0. 1 mg/kghCTMO1 (A; n = 10) and 1.0 mg/kg hCTMOI (B; n = 9).
showed immune complex formation. Immune complexes were alreadypresent at the end of infusion (Fig. 2). In the 0. 1 mg/kg group, mostof the radioactivity was found in the immune complexes, whereas inthe I .0 mg/kg group, most radioactivity was bound to IgG monomers.For both groups, the disappearance from the blood of@@ ‘In-hCTMOIwas best described by a two-compartment model. The results for theinitial (t112) and final (t112) half-lives according to tumor type aresummarized in Table 2. Increasing the hCTMOI antibody dose 10-fold did not influence the elimination from the blood of the@@ tIn
hCTMO1 antibody, but the elimination half-life of the immune complexes in all patients was increased from a mean ‘1/2of 44 h to 92 h.
In the first 24 h after injection, 4.7 ±l.2%ID of indium-l 11 wasexcreted in the urine at the low dose and 4.0 ±1.6%ID at the highdose. During the next 24 h, 3.3 ±0.7%ID and 2.7 ±0.8%ID wasexcreted in the urine at low and high doses, respectively. The cumulative urinary excretion of indium in the first 3 days after injectionmeasured 11.0 ±2.0%ID (range, 6.8—13.1)in the 0.1 mg/kg groupand 6.5 ±12.6%ID (range 7—13)in the 1.0 mg/kg group.
Tissue Distribution. The uptake of radioactivity in removed orbiopsied cancer deposits and in normal tissues per patient at both doselevels in ovarian carcinoma patients is given in Table 3. The meantissue uptake and tumor-to-nontumor ratios per dose group are given
in Table 4. For normal tissues, the mean uptake in peritoneum,muscle, fat, and skin has been taken. Uptake in tumor deposits was
significantly higher than in normal tissues (low dose, P = 0.0003;
high dose, P = 0.0009) or blood (low dose, P 0.0007; high dose,P —0.03). Uptake in tumor biopsies was increased but did not proveto be significant (P = 0.2) at the higher dose compared with that in thelow-dose group. The two groups were relatively similar in tumor
150
5181
on April 29, 2020. © 1996 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
FragmentHalf-life0.1
mg hCTMO1/kg1.0 mghCfMOlIkgMalignant
(n = 10)Nonmalignant (n = 5)aMalignant (n 9)Nonmalignant (n =5)―lgGt½a
(h) ±SD(Range)t½fJ(h) ±SD(Range)4.2
±6.1(0.0—17.0)
64.7 ±20.2(36.2—95.0)7.6
±5.0(0.3—11.7)
54.4 ±16.6(33.0—76.7)4.1
±6.7(0.0—18.0)
47.9 ±27.0(27.2—114.7)5.4
±6.4(0.4—15.6)
48.6 ±16.6(31.5—71.4)Complext½a
(h) ±SD(Range)t½@(h) ±SD(Range)0.9
±0.6(0.3—2.1)
50.9 ±13.3(37. 1—74.2)0.7
±0.5(0.2—1.2)
37.5 ±6.7(30.0—44.5)0.8
±0.7(0.2—2.2)
94.0 ±58.8(49. 1—230.6)1
.5 ±I .8(0.2—4.6)
89.0 ±67.8(31.4—199.3)
ENGINEERED hCFMOl IN OVARIAN CANCER PATIENTS
Table 2 Plasma clearance of ‘111n-labeledhCTMOJ
a Patients 4, 5, 6, 8, and 10 (Table 1).
b Patients 16, 2 1, 26, 27, and 30 (Table 1).
burden. Liver activity was notably high in both dose groups (seeNo significant difference in tumor uptake was foundbetweenexamplein Fig. I). Liver activity was not decreased significantly byprimary ovarian tumors and metastases (0. 1 mg/kg, P = 0.2;1.0the
10-fold increase in MAb dose (P = 0.6), but only three livermg/kg, P = 0.4). Also, the stage of disease and differentiationgradebiopsiescould be taken in the high-dose group. A significant increaseof the tumors were of no significance to absolute uptake oruptakewas
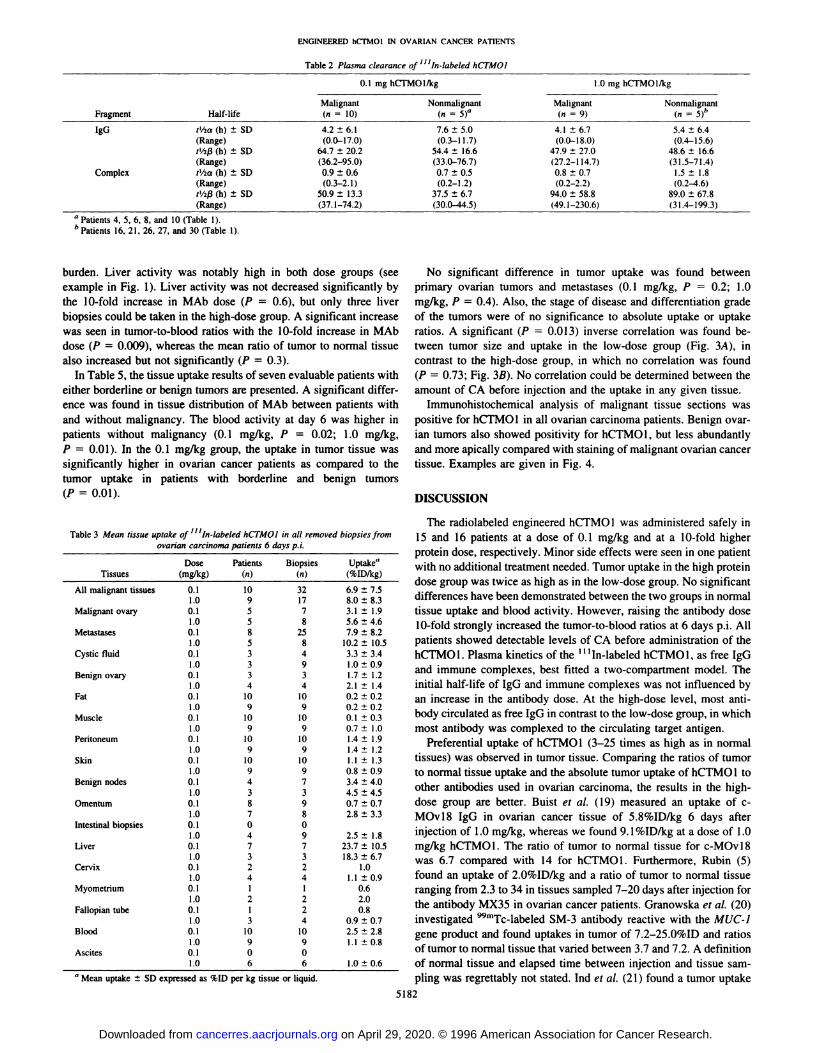
seen in tumor-to-blood ratios with the 10-fold increase in MAbratios. A significant (P = 0.013) inverse correlation was found bedose (P = 0.009), whereas the mean ratio of tumor to normal tissuetween tumor size and uptake in the low-dose group (Fig. 3A),inalso
increased but not significantly (P = 0.3).contrast to the high-dose group, in which no correlation wasfoundInTable 5, the tissue uptake results of seven evaluable patients with(P = 0.73; Fig. 3B). No correlation could be determined betweentheeither
borderline or benign tumors are presented. A significant difference was found in tissue distribution of MAb between patients withand without malignancy. The blood activity at day 6 was higher inamount
of CA before injection and the uptake in any given tissue.Immunohistochemical analysis of malignant tissue sections was
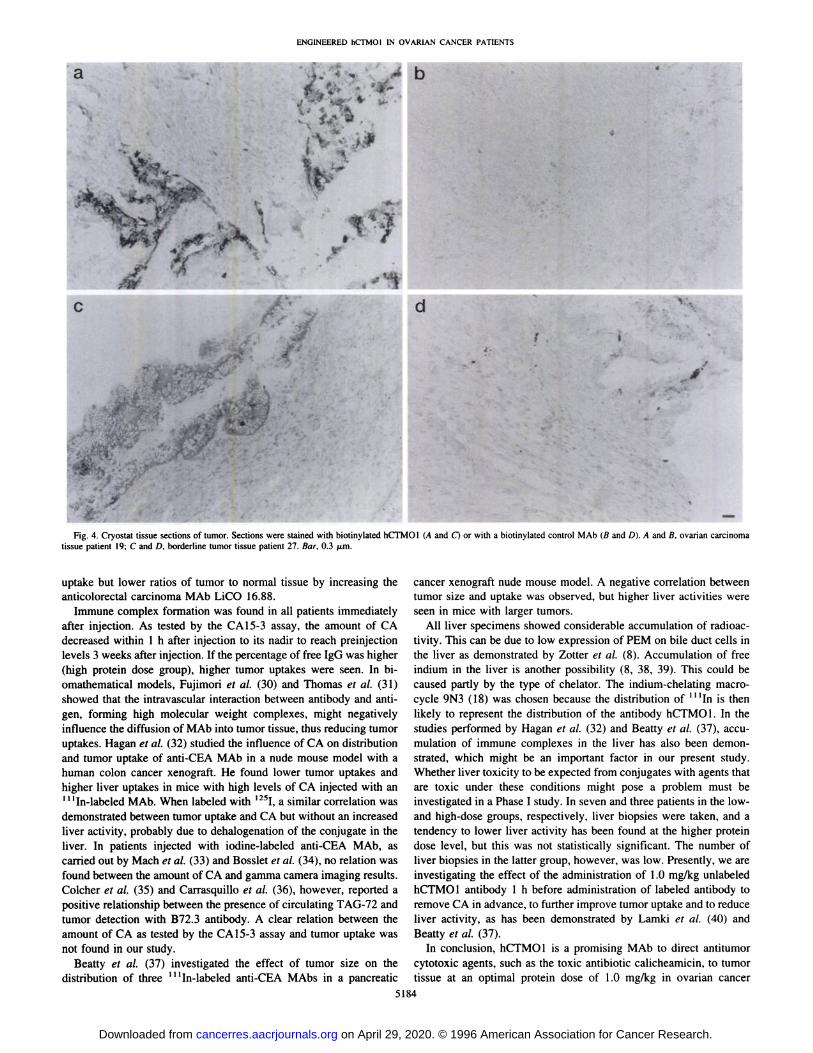
positive for hCTMO1 in all ovarian carcinoma patients. Benign ovarpatients without malignancy (0.1 mg/kg, P = 0.02; 1.0 mg/kg,ian tumors also showed positivity for hCTMOI, but lessabundantlyP
= 0.01). In the 0. 1 mg/kg group, the uptake in tumor tissue wasand more apically compared with staining of malignant ovariancancersignificantlyhigher in ovarian cancer patients as compared to thetissue. Examples are given in Fig.4.tumor
uptake in patients with borderline and benigntumors(P=0.01).Table
3 Mean tissue uptake of “In-labeled hCTMOJ in all removed biopsiesfromovarian carcinoma patients 6 days p.i.The
radiolabeled engineered hCTMO1 was administered safely in15 and 16 patients at a dose of 0.1 mg/kg and at a 10-fold higher
. . . . .
protein dose, respectively. Minor side effects were seen in one patientwith no additional treatment needed. Tumor uptake in the high protein
, . . .
dose group was twice as high as in the low-dose group. No sigmficant.
differences have been demonstrated between the two groups innormal.
Dose Patients Biopsies Uptake―
Tissues (mg/kg) (n) (n)(%ID/kg)All
malignant tissues 0.1 10 32 6.9 ±7.51.0 9 17 8.0 ±8.3Malignant
ovary 0.1 5 7 3.1 ±I.9tissue uptake and blood activity. However, raising the antibodydoseM
@?@ 25@@@
etastases@@ 8 10.2@ 10.510-foldstrongly increased the tumor-to-blood ratios at 6 days p.i. All
patients showed detectable levels of CA before administration oftheCysticfluid 0.1 3 4 3.3 ±3.4
. 1.0 3 9 1.0±0.9
Bemgn ovary 0.1 3 3 1.7 ±I .21.0 4 4 2.1 ±I.4hCTMO1.
Plasma kinetics of the ‘‘‘In-labeledhCTMO1, as free IgGand immune complexes best fitted a two-compartment model. The
, , .initial half-life of IgG and immune complexes was not influencedbyFat
0.1 10 10 0.2 ±0.2
Muscle @:? io 10 g:@@ g:@an
increase in the antibody dose. At the high-dose level, most antibody circulated as free IgG in contrast to the low-dose group, inwhichI
.0 9 9 0.7 ±1.0most antibody was complexed to the circulating targetantigen.Peritoneum?‘@@ @o i@@@@
Skin 0.1 10 10 1.1 ±1.3Preferential
uptake of hCTMO1 (3—25 times as high as in normal
tissues) was observed in tumor tissue. Comparing the ratios oftumor.1.0 9 9 0.8 ± 0.9
Bemgn nodes ?:@@@@@ @tonormal tissue uptake and the absolute tumor uptake of hCTMO1 to
other antibodies used in ovarian carcinoma, the results in the highOmentum 0.1 8 9 0.7 ±0.7dose group are better. Buist et a!. (19) measured an uptake of c
. . . 1.0 7 8 2.8 ±3.3
Intestinal biopsies 0.1 0 01.0 4 9 2.5 ±1.8MOvl8
IgG in ovarian cancer tissue of 5.8%IDIkg 6 days after. .
injection of 1.0 mg/kg, whereas we found 9. 1%IDIkg at a dose of1.0Liver0.1 7 7 23.7 ±10.5mg/kg hCTMO1 . The ratio of tumor to normal tissue for c-MOv18.1.0 3 3 18.3±6.7
Cervix 0.1 2 2 1.0
1.0 4 4 1.1 ±0.9was
6.7 compared with 14 for hCTMO1. Furthermore, Rubin (5)found an uptake of 2.0%ID/kg and a ratio of tumor to normaltissueMyometrium
0. 1 1 1 0.6
Fallopian tube @‘?@@@I .0 3 4 0.9 ±0.7ranging
from 2.3 to 34 in tissues sampled 7—20days after injection forthe antibody MX35 in ovarian cancer patients. Granowska et al. (20)investigated 99mTc@labeledSM-3 antibody reactive with theMUC-1Blood
0.1 10 10 2.5 ±2.8
Ascites @:? o 0 lI 0.8gene
product and found uptakes in tumor of 7.2—25.0%IDand ratios@ tumor to normal tissue that varied between 3.7 and 7.2. AdefinitionI
.0 6 6 1.0 ±0.6of normal tissue and elapsed time between injection and tissue sampling was regrettably not stated. Ind et a!. (21) found a tumor uptake
DISCUSSION
a M@ uptake ± SD expressed as %ID per kg tissue or liquid.
on April 29, 2020. © 1996 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

Patientno.UptakeRatiosTumorNormal―LiverBloodTumor/normal2Tumor/blood0.1
mg/kg12.40.529.41.35.01.926.40.81.87.93.532.30.535.60.84.93.171.30.222.30.58.32.593.70.40.49.85.2113.23.23.21.00.41217.41.05.45.718.03.0132.20.817.91.92.71.1142.60.334.21.510.31.7153.40.420.81.37.92.6Mean4.5
±4.70.8 ±0.923.7 ±10.5'2.5 ±2.87.6 ±4.72.5 ±1.3(Range)(1.3—17.4)(0.2—3.2)(5.4—35.6)(0.5—9.1)(1.0-18.0)(0.5—5.4)1.0
mg/kg1727.41.510.62.818.19.7194.90.322.00.617.98.2201.80.122.30.216.68.22221.61.51.414.815.7233.71.21.53.12.42412.80.30.839.716.6254.10.90.74.56.1293.90.70.85.44.6311.90.31.06.21.9Mean9.1
±9.40.8—0.518.3 ±6.7―11 ±0.814.0 ±11.48.1 ±5.2(Range)(1.8—27.4)(0.1—1.5)(10.6—22.3)(0.2—2.8)(3.0—39.7)(1.9—16.6)
Table 5 Meantissue uptake―1111n-labeled hCTMOJ in biopsies from borderline andbenign ovarian tumor patients 6 daysp.i.Tissue0.1
mg/kg hCTMOI 1.0 mg/kg hCTMO1(@4)b(,,3)CMean
±SD Range Mean ±SDRangeTumor
Normaf'1.0±0.4 0.5—1.4 5.9 ±2.0 3.9—8.6
0.3 ±0.1 0.2—0.3 1.7 ±0.51.4—2.3Blood0.5±0.2 0.3—0.8 2.8 ±0.7 2.0—3.5
ENGINEERED hCTMOI IN OVARIAN CANCER PATIENTS
Table 4 Mean tissue uptakea and tumor to nontumor ratios of― ‘In-labeledhCTMOI in biopsies from ovarian carcinoma patients 6 days p.i.
a Uptake is expressed as %ID per kg tissue or blood.
b Mean uptake in fat, muscle, peritoneum, and skin.
â€n 7.d@
100
1O
AS
SS
S
SC
S SS
S
.
a Uptake is expressed as %ID per kg tissue or blood.
b Patients 4, 6, 8, and 10 (Table I).
C Patients 16, 26, and 30 (Table 1).
d Normal tissues is the mean uptake in fat, muscle, skin, and peritoneum.
of 7.6%ID and a ratio of tumor to normal tissue of 3.8 for 99mTc@labeled SM-3 24—30h after injection. Perkins et a!. (22) performedstudies in 19 patients suspected of having ovarian cancer using@@ ‘InNCRC48 (IgG3) anti-PEM antibody and measured 8.0 ±2.0%IDIkgin five malignant tumors and 4.0 ±3.0%IDIkg in 13 benign tumorsbiopsied at varying operating days (between 4 and 14 days p.i.). Wardet a!. (23) studied the MUC-1 gene recognizing MAb HMFG2, whichwas iodinated, and measured a tumor uptake of 4.9%IDfkg and a ratioof tumor to normal tissue of 2 at 4 h after injection. Epenetos et a!.(24)areexperiencedin theuseof PEMantibodiesfor theimagingandtreatment of ovarian carcinoma; however, their data on uptakes arevery heterogeneous and cannot be used for a comparison here.
A tendency toward a dose-dependent increase in tumor uptake ofhCTMO1 was observed; however, this was not statistically significant. Strong dose dependency was found for the tumor-to-blood ratiosin favor of the higher dose. Worlock (25) also found a dose dependency of tumor uptake with MAb DU-PAN 1 in a pancreatic cancerxenograft model. In patients, Taylor et a!. (26) demonstrated the samephenomenon with indium-labeled antimelanoma antibody mZMEO18.In contrast, Boerman et a!. (27) demonstrated a negative effect ontumor uptake and tissue ratios by increasing the protein dose for threedifferent antibodies in a colon cancer xenograft model. Patt et a!. (28)showed a positive effect of the dose on tumor localization for fourdifferent antibodies. In contrast, Rosenblum et a!. (29) found a higher
A
a)Cl)0
V
0a)C
a)
0
B03
a)0)0
Va)
0a)C
a)
0
I
o.1@@0.1 1 10 100 1000 10000 100000
Tumor Size (cm3)
100
BS
S
10. .
S S@S
S
S
I
[email protected] 1 10 100 1000 10000 100000
Tumor Size (cm3)
Fig. 3. Relation between uptake (expressed as %ID/kg) in ovarian cancer tissue ofI I ‘In-labeled hCTMO1 and tumor size (in cm') in ovarian carcinoma patients injected
with 0.1 mg/kg hCTMO1 (A) and 1.0 mg/kg hCTMO1 (B).
5183
on April 29, 2020. © 1996 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
ENGINEERED hCFMOI tN OVARIAN CANCER PATIENTS
4a
4
d
A.. -4
-S@
C
S -‘
Fig. 4. Cryostat tissue sections of tumor. Sections were stained with biotinylated hCTMO1 (A and C) or with a biotinylated control MAb (B and D). A and B, ovarian carcinomatissue patient 19; C and D, borderline tumor tissue patient 27. Bar, 0.3 @zm.
uptake but lower ratios of tumor to normal tissue by increasing theanticolorectal carcinoma MAb LiCO 16.88.
Immune complex formation was found in all patients immediatelyafter injection. As tested by the CA15-3 assay, the amount of CAdecreased within 1 h after injection to its nadir to reach preinjectionlevels 3 weeks after injection. If the percentage of free IgG was higher(high protein dose group), higher tumor uptakes were seen. In biomathematical models, Fujimori et a!. (30) and Thomas et a!. (31)showed that the intravascular interaction between antibody and antigen, forming high molecular weight complexes, might negativelyinfluence the diffusion of MAb into tumor tissue, thus reducing tumoruptakes. Hagan et a!. (32) studied the influence of CA on distributionand tumor uptake of anti-CEA MAb in a nude mouse model with ahuman colon cancer xenograft. He found lower tumor uptakes andhigher liver uptakes in mice with high levels of CA injected with an11‘In-labeled MAb. When labeled with 1251 a similar correlation was
demonstrated between tumor uptake and CA but without an increasedliver activity, probably due to dehalogenation of the conjugate in theliver. In patients injected with iodine-labeled anti-CEA MAb, ascarried out by Mach et a!. (33) and Bosslet et a!. (34), no relation wasfound between the amount of CA and gamma camera imaging results.Colcher et a!. (35) and Carrasquillo et a!. (36), however, reported apositive relationship between the presence of circulating TAG-72 andtumor detection with B72.3 antibody. A clear relation between theamount of CA as tested by the CA15-3 assay and tumor uptake wasnot found in our study.
Beatty et a!. (37) investigated the effect of tumor size on thedistribution of three ‘‘‘In-labeledanti-CEA MAbs in a pancreatic
cancer xenograft nude mouse model. A negative correlation betweentumor size and uptake was observed, but higher liver activities wereseen in mice with larger tumors.
All liver specimens showed considerable accumulation of radioactivity. This can be due to low expression of PEM on bile duct cells inthe liver as demonstrated by Zotter et a!. (8). Accumulation of freeindium in the liver is another possibility (8, 38, 39). This could becaused partly by the type of chelator. The indium-chelating macrocycle 9N3 (18) was chosen because the distribution of ‘@ ‘Inis thenlikely to represent the distribution of the antibody hCTMO1. In thestudies performed by Hagan et a!. (32) and Beatty et a!. (37), accumulation of immune complexes in the liver has also been demonstrated, which might be an important factor in our present study.Whether liver toxicity to be expected from conjugates with agents thatare toxic under these conditions might pose a problem must beinvestigated in a Phase I study. In seven and three patients in the lowand high-dose groups, respectively, liver biopsies were taken, and atendency to lower liver activity has been found at the higher proteindose level, but this was not statistically significant. The number of
liver biopsies in the latter group, however, was low. Presently, we areinvestigating the effect of the administration of 1.0 mg/kg unlabeledhCTMO1 antibody 1 h before administration of labeled antibody toremove CA in advance, to further improve tumor uptake and to reduceliver activity, as has been demonstrated by Lamki et a!. (40) andBeatty et a!. (37).
In conclusion, hCTMO1 is a promising MAb to direct antitumorcytotoxic agents, such as the toxic antibiotic calicheamicin, to tumortissue at an optimal protein dose of 1.0 mg/kg in ovarian cancer
5184
. ) -,-
g@:@.@J@@i4rd4@@%..s a@-\@i4@_,
@. :@*
on April 29, 2020. © 1996 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

ENGINEERED hCTMOI IN OVARIAN CANCER PATIENTS
patients. Whether or not predosing with cold antibody can prevent theformation of radiolabeled immune complexes, thus reducing liverradioactivity and increasing tumor uptake, is an intriguing question,which is the subject of further study.
ACKNOWLEDGMENTS
We thank P. Baker, H. Greuter, J. Klein Gebbinck, and R. von Meier fortheir expert technical assistance, Dr. R. Verstraeten for the statistical analysis,
and Drs. J. B. Vermorken, C. W. Burger, and T. J. M. Helmerhorst for assisting
in the clinical part of the study. We also thank Dr. D. Shochat for informative
discussions.
REFERENCES
1. Venesmaa, P. Epithelial ovarian cancer: impact of surgery and chemotherapy onsurvival during 1977—1990.Obstet. Gynecol., 84: 8—11, 1994.
2. Krommer, C. F., and Szalai, J. P. A. Review of 28 years of treating advanced ovariancancer. Anticancer Res., 13: 817—826, 1993.
3. Trimble, E. L., Adams, J. D., Vena, D., Hawkins, M. J., Friedman, M. A., Fisherman,J. S.,Christian,M.C.,Canetta,R.,Onetto,N.,Hayn,R.,andArbuck,S.G.Paclitaxelfor platinum-refractory ovarian cancer: results from the first I 000 patients registeredto National Cancer Institute treatment referral center 9103. J. Clin. Oncol., ii:2405—2410,1993.
4. Massuger, L. F. A. G., Kenemans, P., Claessens, R. A. M. J., Verheijen, R. H. M., andCorstens, F. H. M. Detection and localization of ovarian cancer with radiolabeledmonoclonal antibodies. Eur. J. Obstet. Gynecol. Reprod. Biol., 41: 47—63,1991.
5. Rubin, S. C. Monoclonal antibodies in the management of ovarian cancer. Cancer(Phila.), 71: 1602—1612,1993.
6. Riethmuller,G., Schneidergadicke,E., andJohnson,J. P. Monoclonalantibodiesincancer therapy. Cuff. Opin. Immunol., 5: 732—739,1993.
7. Tashiro, Y., Yonezawa, S., Kim, Y. S., and Sato, E. Immunohistochemical study ofmucin carbohydrates and core proteins in human ovarian tumors. Hum. Pathol., 25:364—372, 1994.
8. Zotter, S., Hageman, P. C., Lossnitzer, A., Mooi, W. J., and Hilgers, J. Tissue andtumor distribution of human polymorphic epitheial mucin. Cancer Rev., 11—12:55—101,i988.
9. Buist,M.,andKenemans,P. Imagingandradioimmunotargetingof ovariancancer.TumorTargeting,1: 149—162,1995.
10. Molthoff,C. F. M.,Pinedo,H. M.,Schluper,H. M.M.,Rutgers,D. H.,andBoven,E. Comparison of 1-131 labeled anti-episialin l39H2 with cisplatin, cyclophosphamide or external-beam radiation for anti-tumor efficacy in human ovarian cancerxenografts. mt. J. Cancer, 5!: 108—115, 1992.
11. Maraveyas, A., and Epenetos, A. A. Targeted immunotherapy: an update with specialemphasis on ovarian cancer. Acts Oncol., 32: 741—746,1993.
12. Hilkens, J., Ligtenberg, M. J. L., Vos, H. L., and Litvinov, S. V. Cell membraneassociated mucins and their adhesion-modulation properties. Trends Biochem. Sci.,17: 359—363,1992.
13. Litvinov, S. V., and Hilkens, J. The epithelial sialomucin, episialin, is sialylatedduring recycling. J. Biol. Chem., 268: 21364—21371, 1993.
14. Bon,G. G., Kenemans,P., vanKamp,G.J., Yedema,C. A.,andHilgers,J. Reviewon the clinical value of polymorphic epithelial mucin tumor markers for the management of carcinoma patients. J. NucI. Med. Allied. Sci., 34: 151—162,1990.
15. Aboud-Pirak,E., Sergent,T., Otte-Slachmuylder,C., Abarca,J., Trouet,A., andSchneider, Y. J. Binding and endocytosis of a monoclonal antibody to a highmolecular weight human milk fat globule membrane-associated antigen by culturedMCF-7breastcarcinomacells.CancerRes.,48: 3188—3196,1988.
16. Hinman,L. M., Hamana,P. R., Wallace,R., Menendez,A. T., Durr,F. E., andUpeslacis, J. Preparation and characterization of monoclonal antibody conjugates ofthe calicheamicins: a novel and potent family of antitumor antibiotics. Cancer Res.,53:3336—3342,1993.
17. Baker, T. S., Bose, C. C., Caskey-Finney, H. M., King, D. J., Lawson, A. D. G.,Lyons, A., Mountain, A., Owens, R. J., Rolfe, M. R., Sehdev, M., Yarranton, G. T.,and Adair,J. R. Humanizationof an anti-mucinantibodyfor breastand ovariancancer therapy. In: R. L. Ceriani (ed), Antigen and Antibody Molecular Engineeringin Breast Cancer Diagnosis and Treatment, pp. 61—82.New York: Plenum Press,1994.
18. Turner, A., King, D. J., Farnsworth, A. P. H., Rhind, S. K., Pedley, R. B., Boden, J.,Boden, R., Millican, T. A., Millar, K., Boyce, B., Beeley, N. R. A., Eaton, M. A. W.,and Parker, D. Comparative biodistributions of indium-I 11-labeled macrocycle chimeric B72.3 antibody conjugates in tumor-bearing mice. Br. J. Cancer, 70: 35—41,1994.
19. Buist, M. R., Kenemans, P., den Hollander, W., Vermorken, J. B., Molthoff, C. F. M.,Burger, C. W., Helmerhorst, T. J. M., Bask, J. P. A., and Roos, J. C. Kinetics and
tissue distribution of the radiolabeled chimeric monoclonal antibody MOvI8 andF(ab')2 fragments in ovarian carcinoma patients. Cancer Res., 53: 5413—5418,1993.
20. Granowska, M., Britton, K. E., Mather, S. J., Lowe, D. G., Ellison, D., Bomanji, J.,Burchell, J., Taylor-Papadimitriou, J., Hudson, C. R., and Shepherd, J. H. Radioimmunoscintigraphy with technetium-99m-labeled monoclonal antibody. SM3, ingynaecological cancer. Eur. J. NucI. Med., 20: 483—489, 1993.
21. md, T. E. J., Granowska, M., Britton, K. E., Morris, G., Lowe, D. G., Hudson, C. N.,and Shepherd, J. H. Perioperative radioimmunodetection of ovarian carcinoma usinga hand held gamma detection probe. Br. J. Cancer, 70: 1263—1266,1994.
22. Perkins, A. C., Symonds, I. M., Pimm, M. V., Price, M. R., Wastie, M. L., andSymonds, E. M. Immunoscintigraphy of ovarian carcinoma using a monoclonalantibody ( ‘‘‘In-NCRC48) defining a polymorphic epithelial mucin (PEM) epitope.NucI. Med. Commun., 14: 578—586, 1993.
23. Ward, B. G., Mather, S. J., Hawkins, L. R., Crowther, M. E., Shepherd, J. H.,Granowska, M., Britton, K. E., and Slevin, M. L. Localization of radioiodine conjugated to the monoclonal antibody HMFG2 in human ovarian carcinoma: assessmentof intravenous and intraperitoneal routes of administration. Cancer Res., 47: 47 19—4723, 1987.
24. Epenetos, A. A., Snook, D., Durbin, H., Johnson, P. M., and Taylor-Papadimitriou, J.Limitations of radiolabeled monoclonal antibodies for localizations of human neoplasms. Cancer Res., 46: 3183—3191, 1986.
25. Worlock, A. J., Zalutsky, M. R., and Metzgar, R. S. Radiolocalization of humanpancreatic tumors in athymic mice by monoclonal antibody DU-PAN I. Cancer Res.,50: 7246—7251, 1990.
26. Taylor, A., Milton, W., Eyre, H., Christian, P., Wu, F., Hagan, P., Alazraki, N., Datz,L., and Unger,M. Radioimmunodetectionof humanmelanomawith indium-II1-labeled monoclonal antibody. J. NucI. Med., 29: 329—337,1988.
27. Boerman, 0. C., Sharkey, R. M., Wong, G. Y., Blumenthal, R. D., Aninipot, R. L.,and Goldenberg, D. M. Influence of antibody protein dose on therapeutic efficacy ofradioiodinated antibodies in nude mice bearing GW-39 human tumor. Cancer Immunol. Immunother., 35: 127—134,1992.
28. Patt, Y. Z., Lamki, L. M., Haynie, T. P., Unger, M. W., Rosenblum, M. G., Shirkhoda,A., and Murray, J. L. Improved tumor localization with increasing dose of indium11I-labeled anti-carcinoembryonic antigen monoclonal antibody ZCE-025 in metastatic colorectal cancer. J. Clin. Oncol., 6: 1220—1230, 1988.
29. Rosenblum, M. G., Levin, B., Roh, M., Hohn, D., McCabe, R., Thompson, L.,Cheung, L., and Murray, J. L. Clinical pharmacology and tissue disposition studies of1-131-labeled anticolorectal carcinoma human monoclonal antibody LICO 16.88.Cancer Immunol. Immunother., 39: 397—400, 1994.
30. Fujimori, K., Covell, D. G., Fletcher, J. E., and Weinstein, J. N. Modeling analysis ofthe global and microscopic distribution of immunoglobulin G, F(ab')2, and Fab intumors. Cancer Res., 49: 5656—5663, 1989.
31. Thomas, G. D., Chappell, M. J., Dykes, P. W., Ramsden, D. B., Godfrey, K. R., Ellis,J. R. M., and Bradwell, A. R. Effect of dose, molecular size, affinity, and proteinbinding on tumor uptake of antibody or ligand: a biomathematical model. CancerRes., 49: 3290—3296,1989.
32. Hagan, P. L., Halpern, S. E., Chen, A., Krishnan, L., Frinke, J., Bartholomew, R. M..David, G. S., and Carlo, D. In vito kinetics of radiolabeled monoclonal anti-CEAantibodies in animal models. J. Nucl. Med., 26: 1418—1423, 1985.
33. Mach, J. P., Buchegger, F., Forni, M., Ritschard, J., Berche, C., Lumbroso, J. D.,Schreyer, M., Girardet, C., Accolla, R. S., and Carrel, S. Use of radiolabeledmonoclonal anti-CEA antibodies for the detection of human carcinomas by externalphotoscanning and tomoscintigraphy. Immunol. Today, 239—249, 1981.
34. Bosslet, K., Steinstrasser, A., Schwarz, A., Harthus, H. P., Luben, G., Kuhlmann, L.,and Sedlacek, H. H. Quantitative considerations supporting the irrelevance of circulating serum CEA for the immunoscintigraphic visualization of CEA expressingcarcinomas. Eur. J. NucI. Med., /4: 523—528,1988.
35. Colcher, D., Milenic, D. E., Ferroni, P., Carrasquillo, J. A., Reynolds, J. C., Roselli,M., Larson, S. M., and Schlom, J. in vito fate of monoclonal antibody B72.3 inpatients with colorectal cancer. J. Nucl. Med., 31: 1133—1142, 1990.
36. Carrasquillo, J. A., Abrams, P. G., Schroff, R. W., Reynolds, J. C., Woodhouse, C. S.,Morgan, A. C., Keenan, A. M., Foon, K. A., Perentesis, P., Marshall, S., Horowitz,M.,Szymendera.J., Englert,J., Oldham,R. K.,andLarson,S. M.Effectof antibodydose on the imaging and biodistribution of indium-I I 1 9.2.27 anti-melanoma monoclonal antibody. J. NucI. Med., 29: 39—47, 1988.
37. Beatty, B. G., Beatty, J. D., Williams, L. E., Paxton, R. J., Shively, J. E., and
O'Connor-Tressel, M. Effect of specific antibody pretreatment on liver uptake ofI I ‘In-labeled anticarcinoembryonic antigen monoclonal antibody in nude mice bear
ing human colon cancer xenografts. Cancer Res., 49: 1587—1594,1989.38. Himmelsbach, M., and wahl, R. L. Studies on the metabolic fate of I I I-indium
labeled antibodies. NucI. Med. Biol., 16: 839—845, 1989.39. Buijs, W. C. A. M., Massuger, L. F. A. G., Claessens, R. A. M. J., Kenemans, P., and
Corstens, F. H. M. Dosimetric evaluation of immunoscintigraphy using indium- 111-labeled monoclonal antibody fragments in patients with ovarian cancer. J. NucI. Med.,33: 1113—1120,1992.
40. Lamki, L. M., Murray, J. L., and Rosenblum, M. G. Effect of unlabeled moab onbiodistribution of indium-I 11 labeled moab. NucI. Med. Commun., 9: 553—564,1988.
5185
on April 29, 2020. © 1996 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
1996;56:5179-5185. Cancer Res Arjan C. van Hof, Carla F. M. Molthoff, Quentin Davies, et al. Protein DoseAntibody CTMO1 in Ovarian Cancer Patients: Influence of
Indium-labeled Engineered Human111Biodistribution of
Updated version
http://cancerres.aacrjournals.org/content/56/22/5179
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/56/22/5179To request permission to re-use all or part of this article, use this link
on April 29, 2020. © 1996 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from