pac 03 dermatology vesicular, bullae, acneiform disease by stacey singer-leshinsky r-pac
TRANSCRIPT

PAC 03 DERMATOLOGYVesicular, Bullae, Acneiform Disease
ByStacey Singer-Leshinsky R-
PAC

Terms Vesicle: Bullae: Fluid filled blister
greater than 100cm in diameter
Acneiform:

Vesicular BullaeBullous Pemphigoid Humoral and cellular response
against self-antigens BP 180, 230. These are needed for dermo-epidermal cohesion.
Sub epidermal blister formation from cascade of events

Vesicular BullaeBullous Pemphigoid Lesions usually appear on
extremities first then trunk. Flexor surfaces of extremities.
Exacerbations/remissions.

Bullous PemphigoidHistory and Physical Exam
Non Bullous phase: mild to severe pruritus with excoriated, eczematous, papular, urticarial lesions
Bullous phase: Vesicles and bullae on erythematous skin. Filled with clear or blood tinged fluid. Erode and crust.

Bullous PemphigoidDrug Induced Diuretics, analgetics, antibiotics Drug acts as a trigger in patients
with genetic susceptibility by modifying immune response

Bullous PhemphigoidDiagnosis Clinical confirmed by
histopathology/immunopathology Immunofluorescence studies reveal
IgG and/or C3 at dermal-epidermal junction
IgE in serum Light microscopy of lesions reveals
eosinophils, neutrophils, lymphocytes

Bullous PhemphigoidDifferentials/Complications Differentials include erythema
multiforme, drug eruptions, dermatitis herpetiformis
Complications

Bullous PemphigoidTreatment Systemic or Topical corticosteroids.
Immunosuppressive medications Patients often go into a permanent
remission

Pemphigus Vulgaris IgG auto antibodies against cell
surface of keratinocytes. Results in acantholysis and blister formation.
Found in middle age-elderly Can be due to reaction to
medications 50-70% of patients have mucosal
lesions

Pemphigus VulgarisClinical manifestations
Pain Flaccid blister filled with clear
serous fluid Blisters fragile. Blisters rupture Mucosal lesions can precede
cutaneous lesions.

Pemphigus VulgarisDiagnosis Nikolsky’s sign positive. Asboe-Hansen sign: gentle
pressure on intact bulla forces fluid to spread under the skin away from site of pressure.
Immunofluorescence Tzanck smear: acantholytic cells

Pemphigus VulgarisDifferentials/complications Differentials: Acute herpetic stomatitis,
aphthous stomatitis, erythema multiforme, bullous lichen planus, bullous pemphigoid,
Complications Secondary infection Dehydration Often fatal unless treated with
immunosuppressive agents Recurrent and relapsing

Pemphigus VulgarisTreatment Treat dehydration Glucocorticoids- Immunosuppressive therapy-
Azathioprine, Methotrexate, cyclophosphamide

Pilosebaceous Unit Sebaceous gland
empties into hair follicle.
Pilosebaceous unit opens to surface.
Sebaceous gland produces sebum.

Pilosebaceous Unit Amount of sebum produced
depends on size of gland, rate of sebaceous cell proliferation
Large sebaceous glands Sebum production related
to androgens Sebaceous glands are rich
in staphyloccus epidermidis and Propionibacterium.

Acne Vulgaris Primarily disorder of adolescence.
Affecting 40-50 million in USA. Psychosocial and economic impact Clinically characterized by
comedones and inflammatory lesions
Etiology: unknown.

Acne Vulgaris Androgens cause sebaceous glands to
overproduce sebum. Bacteria secrete lipase which converts
lipids to fatty acids. Hyperkeratinization in lining of follicle
and follicle plugging. Papules, pustules, scarring result from
follicular rupture and inflammatory response

Acne VulgarisClinical manifestations
Non-inflammatory acne: open and closed comedones. , open comedones
Inflammatory acne: above expands to form papules, pustules, nodules and cysts of varying severity. 1-5mm filled with sterile pus.
Found on face, neck, shoulders and upper trunk

Acne VulgarisDiagnosis/Differentials
Hormone studies will rule out other etiologies
Differential diagnosis to include folliculitis, steroid folliculitis
Complications to include abscess formation and severe infection
Scarring

Acne VulgarisManagement Comedolytics- Sebum suppressive medications-
antiandrogens include spironolactone, oral contraceptives
Topical/Systemic antibiotics- emycin, clindamycin
Benzoyl peroxide- Severe Acne- Isotretinion(Accutane)-
inhibits sebaceous gland function and keratinization.

Rosacea Peaks in 30-40’s. Associated with
Parkinson’s, might be associated with Helicobacter pylori or hair follicle mites (Dermodex folliculorum)
Related to vascular hyper-activity-Repeated episodes of dilation lead to release of inflammatory mediators into dermis.

Rosacea Involves nose, cheeks, forehead and
chin Complain of reddening of face with
heat, hot fluids, spicy foods and ETOH
Rhinophyma caused by sebaceous hyperplasia M>F
Blepharophyma Metrophyma

RosaceaTypes
Vascular Rosacea: Flushing and persistent central facial erythema with or without telangiectasia.
Papulopustular rosacea: central facial erythema with transient papules and pustules.

RosaceaTypes
Sebaceous hyperplasia: thickening skin, irregular surface nodularities and enlargement.
Ocular rosacea: Foreign body sensation in eyes. Photosensitivity, periorbital edema, telangiectasia of sclera.

RosaceaDiagnosis/Differentials Diagnosis: Clinical diagnosis,
histopathological features Differential diagnosis:
Acne vulgaris- Perioral dermatitis Seborrheic dermatitis Systemic Lupus Erythematosus

RosaceaManagement Avoid environmental and dietary triggers
such as heat/sun exposure, ETOH. Topical Metronidazole- Azelaic acid cream. Tetracycline- treats inflammation. Retinoids- Isotretinoin- Clonidine NO potent topical fluorinated steroids on
face

Hidradenitis Suppurativa Skin infection that affects apocrine
gland bearing skin sites especially the axillae and anogenital areas.
Characterized by recurrent boils and draining sinus tracts with scarring.

Hidradenitis Suppurativa Risk factors include obesity,
apocrine duct obstruction, family history
Inflammatory condition originating in the hair follicle. Follicle ruptures spilling contents into surrounding dermis.
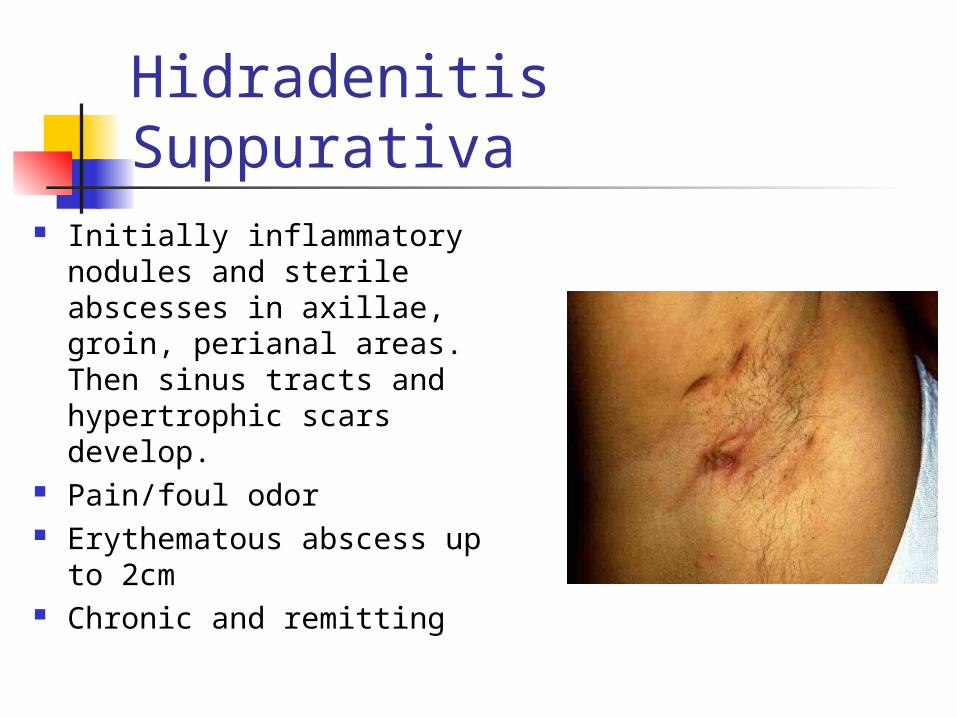
Hidradenitis Suppurativa Initially inflammatory
nodules and sterile abscesses in axillae, groin, perianal areas. Then sinus tracts and hypertrophic scars develop.
Pain/foul odor Erythematous abscess up to
2cm Chronic and remitting

Hidradenitis SuppurativaDiagnosis/Differentials Diagnosis:
Bacterial cultures for antibiotic therapy
Differentials: Cellulitis, pilonidal cysts, bacterial folliculitis
Complications: Squamous cell carcinoma

Hidradenitis SuppurativaManagement Might need incision and drainage if
large and painful. Antibiotics such as tetracycline,
cephalosporin, clindamycin, ciprofloxacin
Isotretinoin Corticosteroids Reduce friction and moisture.

Hypersensitivity Vasculitis Immune complex mediated
inflammation of small vessels such as arterioles, capillaries, venules.
Occur as an exaggerated immune response to a drug, infection or autoantibodies
This leads to injury to vessel walls, and so decreased function and blood flow.

Hypersensitivity Vasculitis
Patients might report use of a new drug, history of streptococcal infection or collagen/vascular disease such as lupus, Rheumatoid Arthritis
If not isolated then can have systemic vascular involvement of kidneys, muscles, joints, GI tract, peripheral nerves

Hypersensitivity Vasculitis Palpable purpura 1-
3mm in diameter Usually localized to
lower third of legs/ankles
Lesions are scattered, discrete, confluent
Lesions can form papules and ulcers due to lack of blood supply

Diagnosis: confirmed by skin
biopsy (vascular and perivascular infiltration of broken up leukocytes)
Look for evidence of systemic disease
Hypersensitivity VasculitisDiagnosis

Hypersensitivity VasculitisComplications/Differentials
Complications Systemic vascular involvement Necrosis Irreversible damage to kidneys
Differential diagnosis Thrombocytopenia purpura Disseminated intravascular coagulation Rocky Mountain Spotted Fever Steven Johnson Syndrome

Hypersensitivity VasculitisManagement
Antibiotics If skin involvement use colchicine
or Dapsone If visceral involvement then use
steroids such as Prednisone combined with Cytotoxic immunosuppressives

Folliculitis Common disorder with perifollicular
pustules. Etiology: staphylococcus aureus,
pseudomonas aeruginosa chemical irritation, friction, perspiration, shaving, skin injury.
Follicle infiltrate of lymphocytes, neutrophils, macrophages. Can lead to formation of abscess.

Folliculitis Papule or pustule on
erythematous base Asymptomatic, mild
discomfort or pruritic Favors areas with terminal hair
Eye involvement: Healing can lead to
keloids

FolliculitisDiagnosis/Differentials Diagnosis
History and physical exam Cultures, gram stains, KOH
Differentials Insect bites Scabies Rosacea Tinea

FolliculitisManagement Wash area with antibacterial soaps Topical and/or oral antibiotics
(s.aureus-often resistant to pcn so use dicloxacillin or cephalosporin or emycin or clindamycin)
Pseudomonas Antifungals/Antivirals

Xerosis Dry skin Can be a natural occurrence
sometimes associated with aging , second to contact dermatitis. Also exogenous causes such as dry climate, excessive exposure to water
Etiology:

XerosisClinical Manifestations Pruritus Involves back, abdomen,
extremities Dry rough, scaly skin Cracking, fissuring

XerosisDiagnosis Diagnosis: histological findings Differential Diagnosis: Eczema,
contact dermatitis, scabies

XerosisManagement Moisturizing agents humectants
(alpha hydroxy acids- dry water from deeper layers to skin surface), occlusives which reduce water loss by epidermis

Example 1 Prodrome of
erythematous skin prior to bullae eruption
Pruritus weeks to months prior to blister eruption
Extremities first then trunk
What is this? What do immunofluorescence studies reveal?
Treatment

Example 2 Mucosal lesions Flaccid blister on
normal or erythematous skin.
Blisters rupture leading to erosions
What sign is positive?
What happens if not treated?
Treatment options:

Example 3 Follicular
comedones with or without inflammatory papules, pustules and nodules
What is the cause of this condition?
What is the management?

Example 4 Blood vessels dilate
easily and leakage of inflammatory mediators into dermis
Aggravated by what medication
Describe the appearance of the lesion
Describe the management

Example 5 Chronic infection
of apocrine sweat glands
Inflammatory red hard raised nodules in axilla, groin, perineum
What is this? What is the
management?

Example 6 What is this? What bacteria are
involved with this?
What is the treatment of this?