pad rehabilitation toolkit a guide for healthcare professionals healthy steps for peripheral artery...
TRANSCRIPT
PAD Rehabilitation ToolkitA Guide for Healthcare
ProfessionalsHealthy Steps for
Peripheral Artery Disease (PAD)Developed by AACVPR and the Vascular Disease Foundation

What is PAD?
Peripheral artery disease (PAD) results fromsystemic atherosclerosis and involves blood
vesselsthroughout the body however, PAD is most
commonly used in reference to lower extremity disease.

About PAD• PAD symptoms result from limited arterial blood
flow, which causes debilitating, activity-induced, ischemic pain (intermittent claudication)
• PAD is associated with major limitations in mobility and physical functioning, and decreased quality of life
• Not all persons with PAD have symptoms
• Subsequent risk for other manifestations of CVD (heart attack and stroke) is high

Belch, J. J. F. et al. Arch Intern Med 2003;163:884-892.
Common PAD Risk Factors

Clinical Presentation of PAD
Hirsch AT et al. J Am Coll Cardiol. 2006;47:1239-1312.
Initial clinical presentation
Asymptomatic PAD
20%–50%
Atypical leg pain40%–50%
Claudication10%–35%
Critical Limb Ischemia (CLI)
1%–2%
PAD Population (50 years)
Two Major Goals in Treating Participants with PAD
Limb Outcomes Cardiovascular Morbidity and Mortality Outcomes
• Relieve Symptoms• Increase in peak
walking distance• Improvement in
quality-of-life indicators
• Prevention of progression to CLI and amputation
• Decrease mortality/morbidity from MI, stroke, and cardiovascular death

Essentials of Management for PAD:
Reduce Symptoms and Lower Risk for Coronary Artery Disease and Stroke
Risk Factor Normalization• Tobacco use
– Goal complete cessation
• Lipid management– Goal LDL <100 mg/dL
• Blood pressure control– Goal <140/90 mm Hg– Goal <130/80 mm Hg
(hypertension + diabetes or renal disease)
• Blood sugar control (patients with diabetes)– Goal A1C <7%
Ant platelet Therapies• Clopidogrel, ASA
Symptom-Directed Therapies• Supervised exercise rehabilitation
• Cilostazol
• Selective use of revascularization
Intermittent Claudication (IC)• “Claudicatio” (Latin: “to
limp”) Claudius was known to limp
• A symptom of PAD characterized by pain, aching, or fatigue in exercising leg muscles
• It can be thought of as ANGINA of the legs
Differential Diagnosis of Leg Pain(Other Potential Causes)
• Spinal canal stenosis• Peripheral neuropathy• Peripheral nerve pain– Herniated disc
impinging on sciatic nerve
• Osteoarthritis of the hip or knee
• Venous claudication• Symptomatic Baker’s
cyst• Chronic compartment
syndrome• Muscle spasms or
cramps• Restless leg syndrome
Also see Table 3 of Hirsch AT, et al. J Am Coll Cardiol. 2006;47:e1-e192.

Diagnosing PADUnderstanding the ABI
TASC Working Group. J Vasc Surg. 2000
ABI= Ankle Systolic Pressure/Brachial Artery Systolic PressureExample: 120mmHg/140mmHg = 0.86
Hirsch AT. Fam Pract Recert. 2000
ABI Interpretation
1.00-1.30
Normal
0.91-0.99
Borderline
0.41-0.90
Mild to Moderate
<0.40 Severe
>1.30 Non-Compressible Vessels
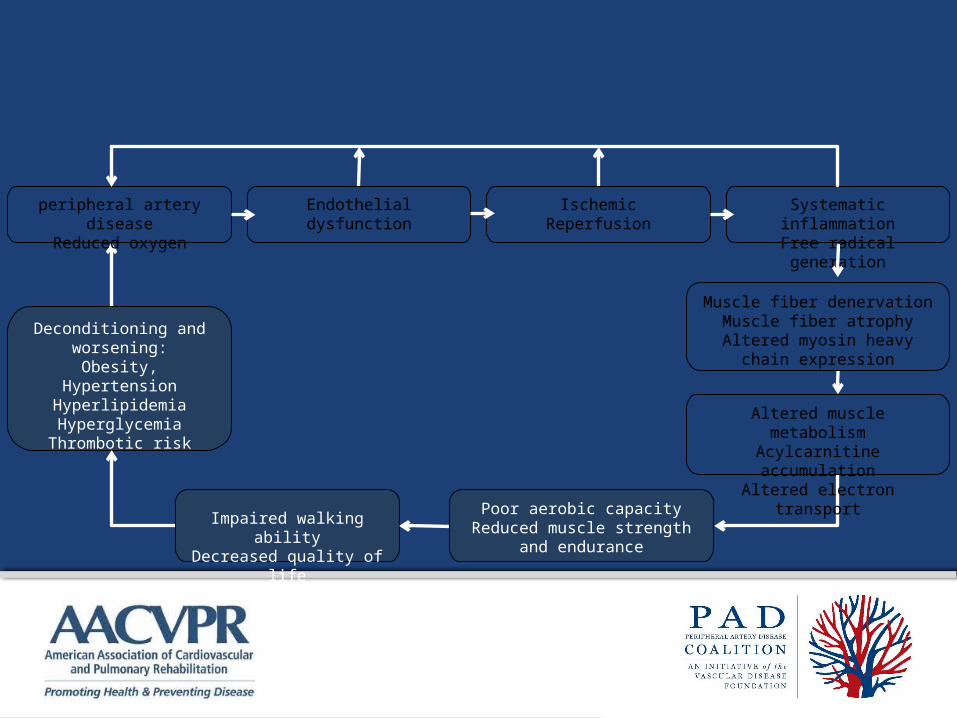
The Cycle of Disability in Intermittent Claudication
peripheral artery disease
Reduced oxygen
Endothelialdysfunction
IschemicReperfusion
Systematic inflammation
Free radical generation
Deconditioning andworsening:
Obesity, HypertensionHyperlipidemiaHyperglycemiaThrombotic risk
Altered muscle metabolismAcylcarnitine accumulationAltered electron transport
Impaired walking ability
Decreased quality of life
Muscle fiber denervationMuscle fiber atrophy
Altered myosin heavy chain expression
Poor aerobic capacityReduced muscle strength
and endurance
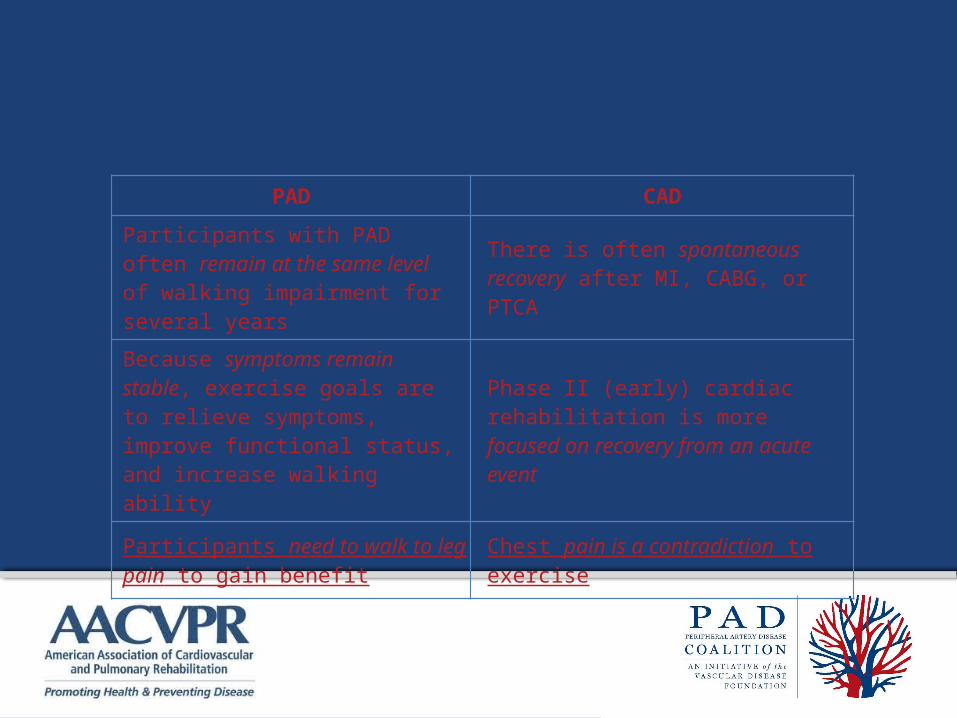
PAD versus CADExercise Rehabilitation
PAD CAD
Participants with PAD often remain at the same level of walking impairment for several years
There is often spontaneous recovery after MI, CABG, or PTCA
Because symptoms remain stable, exercise goals are to relieve symptoms, improve functional status, and increase walking ability
Phase II (early) cardiac rehabilitation is more focused on recovery from an acute event
Participants need to walk to leg pain to gain benefit
Chest pain is a contradiction to exercise

Benefits of Exercise Training in Participants with PAD and
IC• Supervised exercise training increases
– functional capacity • greater walking distance before experiencing
symptoms
– quality of life• Functional benefits are greatest when
– exercise sessions last longer than 30 minutes – sessions take place at least 3 times per week– walking into leg pain– the program lasts 6 months or longer
Role Of Direct Supervision• Supervision increases the likelihood that the exercise
session will be carried out according to guidelines• As participants improve their walking ability, the
exercise workload should be increased by increasing treadmill grade or speed (or both), to assure that there is always the stimulus of claudication pain during the workout
• As participants increase their walking ability, there is the possibility that cardiac signs and symptoms may appear as they achieve higher heart rates and blood pressures
• Additional monitoring is determined by clinical responses
Stewart, Hiatt, Regensteiner, Hirsch. NEJM 347:1941-1957 December 12, 2002.

Potential Mechanisms for Exercise-Induced
Improvements• Improved oxygen extraction and utilization by
exercising muscle
• Improved endothelial function
• Improved blood rheology
• Improved gait and walking economy
• Increased tolerance to pain
• Possibly increased blood supply

Mechanisms by Which Exercise May Improve Function & Symptoms in
Claudication
Stewart, Hiatt, Regensteiner, Hirsch. NEJM 347:1941-1957 December 12, 2002.
peripheral artery disease
Reduced oxygen
Endothelialdysfunction
IschemicReperfusion
Systematic inflammation
Free radical generation
Deconditioning andworsening:
Obesity, HypertensionHyperlipidemiaHyperglycemiaThrombotic risk
Altered muscle metabolismAcylcarnitine accumulationAltered electron transport
Impaired walking ability
Decreased quality of life
Muscle fiber denervationMuscle fiber atrophy
Altered myosin heavy chain expression
Poor aerobic capacityReduced muscle strength
and endurance
Effects of exercise training on pathophysiological correlates of claudication
Good evidence for improvement
Potential improvement
Short-term: may worsenLong-term: may improve

Goals of Medical Evaluation Before Exercise Rehabilitation• To confirm diagnosis of PAD and IC• To confirm absence of
– Critical limb ischemia– Unstable angina– Decompensated heart failure– Uncontrolled cardiac arrhythmias– Severe or symptomatic valvular disease– Other conditions that could be aggravated by exercise including,
but not limited to, severe joint disease, uncontrolled diabetes, or uncontrolled hypertension
• To screen for exercise-induced myocardial ischemia & arrhythmias– Exercise stress testing is preferred– Careful questioning for symptoms is an alternative
Pre-Exercise Functional Evaluation
• May be either
– Formal treadmill testing protocols
– Observation during initial treadmill exercise session
• Goal is to determine
– Claudication threshold
– Cardiovascular response to exercise
– Establish parameters for the exercise prescription

Use of a Pain Scale in PAD Exercise Rehabilitation
1 No Pain
2 Onset of Pain
3 Mild Pain
4 Moderate
5 Severe

PAD Exercise Guidelines• Warm-up and cool-down: 5 minutes each
• Mode: Treadmill walking
• Intensity: Walk to claudication pain (3-4 of 5 on the scale), maintain for 8-10 min. Increase speed or grade when pain becomes less than moderate.
• Duration: Initially, accumulate 35 min of walking in bouts of 8-10 min each. Rest between bouts until pain subsides. Progress to 50 min, including 5 minutes warm up and cool down.
• Frequency: 3-5 times/week
• Total Time: At least 3 monthsSource; Regensteiner and Hiatt: ACSM Resource Manual 2001.

Specifics About Exercise Prescription
• The initial training intensity is defined as the % inclination that brings on the onset of claudication pain (level 2 of 5 on the claudication scale), with the initial speed set at 2.0 mph
• During the initial exercise session– Participants walk to a mild to moderate pain level (3-4
of 5 on the claudication scale) at the initial training intensity above, then
– Stop and rest until the claudication pain has completely abated and then
– Resume walking at the initial training intensity again

Goals of the Initial Training Sessions
• For the participant to understand the claudication scale, foot care, and purpose of exercise training
• To teach warm up and cool down principles
• To accumulate 15 minutes or more of total exercise treadmill time, excluding warm up and cool down
Goal of Subsequent Exercise Sessions
• Cumulative exercise session of 50 minutes (including rest periods)
• Advance speed and inclination over time to maintain a claudication stimulus to exercise training
• Warm-up and cool-down periods of 5 minutes each
• Total of 60 minutes per session

Progression of the Exercise Training Intensity
• Should occur during the session after the participant can exercise for
– at least 8 minutes without stopping for 3-4/5 claudication pain
– cumulative exercise duration of 50 minutes including rest periods
• Increase inclination by 1-2% maintain the same speed (2.0 mph)

General Guidelines for Progression of Exercise Training Intensity During
Rehabilitation• Continue to increase inclination as tolerated in
subsequent sessions until reach 10% at 2.0 mph
• Then increase speed by 0.1 to 0.2 mph at 10% with goal to achieve more than 8 minutes before rest is needed for claudication pain (3-4/5)
• When reach 3.0 mph/10% inclination, then increase inclination by 1-2%, up to 15%
• Final step is to increase speed by 0.1 to 0.2 mph increments as tolerated
Case Study:History & Clinical Profile
• 70 year old white female • Wt: 180 lbs. • Ht: 62” • BMI = 32.9• Current smoker: 1/2 pack per day• Hyperlipidemia, hypertension• Cardiac History: CABG January, 2004, and
NSTEMI June, 2006

• Pertinent medical hx: Bilateral PAD
• Current meds: cilostazol, lisinopril, furosemide, simvastatin, clopidogrel, aspirin
• Resting BP: 128/46; RHR: 64
• Resting ECG: Non-specific ST-T wave ‘s
Case Study:History & Clinical Profile

Exercise Test Results• Onset of leg pain @ 2.0 mph / 7% grade
• Maximal pain @ 2.0 mph / 10.5% grade
• Normal BP & HR response
• No complaints of angina
• Stress ECG: No changes
Case Study:History & Clinical Profile

• What is the beginning exercise prescription?
Case Study:Exercise Training Scenarios
• What is the beginning exercise prescription?
• Treadmill walking at 2 mph / 7% grade
• Walk to moderate pain (3 or 4 on scale)
Case Study:Exercise Training Scenarios
During the first 12 exercise sessions Participant progresses
from 2.0 mph/7% grade to a workload of 2.0 mph / 10%
grade. During sessions 13 – 24, the maximum walking
time at 2.0 mph/10% grade was 7 min. What is theprescribed workload for session #25?
A.2.0 mph / 10% gradeB.2.2 mph / 10% gradeC.2.0 mph / 12% gradeD.2.5 mph / 10% grade
Case Study:Exercise Training Scenarios
Case Study:Exercise Training Scenarios
During the first 12 exercise sessions Participant progresses
from 2.0 mph/7% grade to a workload of 2.0 mph / 10%
grade. During sessions 13 – 24, the maximum walking
time at 2.0 mph/10% grade was 7 min. What is theprescribed workload for session #25?
A.2.0 mph / 10% gradeB.2.2 mph / 10% gradeC.2.0 mph / 12% gradeD.2.5 mph / 10% grade

Other Program Considerations• Treadmill or other walking exercise is the
cornerstone.
– If possible it should be used during each exercise session
• Other forms of exercise can also be added for cardiovascular health but have not been shown to improve claudication symptoms
• Invite participants to join your facility’s CV risk factor education sessions
Interventional Treatment• Surgical or percutaneous intervention is
recommended to treat:
– ischemic rest pain
– tissue loss
– vocational limiting claudication
• Further information is available at– http://www.padcoalition.org/resources/slides.php– http://www.acc.org/qualityandscience/clinical/pdfs/
05%20Treatment%20-20Revascularization%20for%20Individual%20with%20PAD%20-%20the%20Symptomatic%20Leg.PPT

Post Interventional Considerations
• Avoid compression garments if ABI<0.8
• If stents, avoid extended squatting or exercises that may compress the stent
• Avoid walking if plantar foot wound
• Observe for recurrent symptoms and notify health care provider if these occur
• Stress importance of excellent foot care
Assessing Participant Outcomes and
Program Effectiveness• Treadmill Testing• Six Minute Walk Test• Shuttle Walk Test• Four Meter Walking Velocity• Repeated Chair Rise• Standing Balance• Quality of Life Questionnaire• Program Demographics • Attendance

Marketing Considerations• Surgeons are generally aware of the benefits of
exercise training for IC but do not think about or know how to refer participants to programs
• Medical physicians are not always aware of benefits of exercise for these patients
• Clinical practice guidelines stress discussion of supervised exercise training with patients with IC
• Capture this marketing opportunity!
Keys to Successful Programs• Efficient use of staff and equipment
• Build on successful existing programs
• Feasible business plan with enthusiastic support by administration
• Effective communication with referring physicians
• Awareness that successful marketing depends on every team member

PAD Coalitionwww.vasculardisease.org/PADcoalition/
AACVPRwww.aacvpr.org/