pan london major trauma networks mass casualty … · pan london major trauma networks: ... hurst,...
TRANSCRIPT
PanLondonMajorTraumaNetworks:ResponsetoMassCasualtyIncidentVersion1.4March2016
2
Contents.DistributionList page3Glossary/Definitions page4AmendmentsList page5ForewordandAcknowledgements page6Background page7 OverviewofNetworks PlanningAssumptions OtherUsefulDocumentsCommandandControl page10 ActivationofthisPlan Co-ordinationofResources MutualAidRequestsandManagementIncidentRolesandResponsibilities page12 MajorTraumaCentres TraumaUnits AmbulanceServices HelicopterEmergencyMedicalServices CriticalCareNetworks NHSEngland(London) NHSProviderOrganisations ClinicalCommissioningGroupsProgression&Recovery page19 DuringTheFirst24hours Recovery&ResiliencePreparednessRolesandResponsibilities page26 MajorTraumaCentres TraumaUnits AmbulanceServices CriticalCareServicesAppendices
1. TheLondonMajorTraumaSystem page302. DamageControlResuscitation/Surgery page323. SpecialCircumstances–Burns,CBRN page334. Triage page34
3
DistributionListNHSEnglandNationalClinicalDirectorofEPRRNationalClinicalDirectorofMajorTraumaClinicalReferenceGroup MajorTrauma EPRR AdultCriticalCareLondonODNLeads–Trauma,Burns,CriticalCare,CommissioningLondonEPRRMajorTraumaNetworkClinicalDirectorsMajorTraumaNetworkManagersMajorTraumaCentreClinicalLeadsTraumaUnitClinicalLeadsChiefExecutiveofAcuteNHSTrustsRoyalCollegeofEmergencyMedicineRoyalCollegeofSurgeonsofEnglandRoyalCollegeofAnaesthesiaRoyalCollegeofPaediatricsandChildHealthIntensiveCareSociety/PaediatricIntensiveCareSocietyFacultyofPre-hospitalCareLondonAmbulanceServiceSouthEastCoastAmbulanceServiceSouthCoastAmbulanceServiceEastofEnglandAmbulanceServicePoliceBritishTransportPoliceFireandRescueLondonTransportLondonUndergroundLondonMilitaryLiaisonLondonHEMSKent,SurreyandSussexHEMSThamesValleyAirAmbulanceHampshire&IsleofWightAirAmbulanceEssexandHertsAirAmbulance
4
Glossary/DefinitionsBiological–pertainingtoinfectiousagentsusedinweapons.ExamplesbeingAnthrax,Plague,Typhus.CBRN=Chemical,Biological,RadiologicalandNuclearChemical–pertainingtochemicalweapons.Thesemaybelethalornonlethalagentsincluding–nerve,choking,blister,andincapacitatingagents.ChildrenandYoungPeople–thisgrouprefersfrombirthto16thbirthday.CodeRed–theidentificationofapatientrequiringbloodtransfusionHEMS–HelicopterEmergencyMedicalServicesakaAirAmbulanceIED–ImprovisedExplosiveDevice.Anexplosivedevicemadefrombasiccomponentsusedtodelivereithershrapnelorotheragents.The‘home-made’bomb.LocalEmergencyHospital–anacutecentrethatdoesnotmeetTraumaUnitcriteria.MajorIncident–anyoccurrencethatpresentsseriousthreattothehealthofthecommunityorcausessuchnumbersortypesofcasualties,astorequirespecialarrangementstobeimplemented.MajorTraumaNetwork(MTN)–agroupofhospitalsinahubandspokemodelwithaMajorTraumaCentresupportingseveralTraumaUnitsorlocalemergencyhospitalsMajorTraumaCentre(MTC)–ahospitalwithalltheacute/surgical/rehabilitativeservicesonsiteformajortraumaMassCasualtyIncident-aneventwithcasualtiesinthe100swherethenormalmajorincidentresponsemustbeaugmentedwithextraordinarymeasuresMERIT–MobileEmergencyResponseIncidentTeam.DoctorsandNurseswithpre-hospitalexpertisemobilisedtothescene.Nuclear–radiationagentsmadefromhighqualityfissionablematerials.ODN–OperationalDeliveryNetwork.Acommissioning/clinicalledco-operativegroupdrawingtogetherservices,oftenina‘hubandspoke’model.Radiological-pertainingtoweapons.Madefromradioactivematerialthatmaynotbeofhighorweaponsgrade.Thiswouldbethe‘dirtybomb’.TARN–TraumaAuditandResearchNetwork.Adatabasefortraumacareandresearch,producingregularqualityaudits.TraumaUnit(TU)–typicallyaDistrictGeneralHospitalwithanEmergencyDept(A&E)thathasmetasetofnationalcriteriaandsubmitsdatatoTARNforaudit.
5
AmendmentsDate Amender Version SectionAmendedwithdetails18Jan2016
WRIGHT 1.0 ConsultationVersion
25Jan2016
WRIGHT 1.1/1.2 Generalwordingpostworkinggroupclosedconsultation.Re-orderofkeytopics
March WRIGHT 1.3 Finalforrelease29March2016
WRIGHT 1.4 IndexingandPaginationUpdate

6
ForewordandAcknowledgementsFollowingthe introductionofTraumaNetworkstoLondonin2010theopportunityfor cross network collaboration and mutual support has never been greater. Thethreat of amass casualty incident in the capital remains high and this plan drawstogetherprinciplesofhowthenetworkswouldsupporteachother.Theinteractionswithotherkeyorganisations,themutualuseofairambulancesupportandtheuseofoutofLondonambulanceservicesisdescribed.Itisnotdesignedtoreplacetrustmajorincidentplansbuttosupplementthemintheeventofamasscasualtyevent.Itshouldbereadinconjunctionwith:LondonResiliencePartnership–MassCasualtyFrameworkV3.2August2015KelvinWright2016ThefollowingparagraphtakenfromtheLondonMassCasualtyFramework2009providesaconcisesummaryofthekeyelementsofplanning.Dealing with a mass casualties incident requires the planning, cooperation andresponseofnumerouspartneragencies.Thesetypesof incidenthavethepotentialtorapidlyoverwhelmservicesandcarefulpre-planningandacoordinatedresponsehasbeenshowntoprovidethebestoutcomeforcasualties.“Localcommunitiesmusttaketheleadindevelopingincidentcommandsystemsforinitialmanagement of such events. Hospital and pre-hospital providers play a keyrole in such planning. Ultimate management and disposition of large numbers ofcasualties[…]cannotfollowstandardpatientmanagementprotocols;newprotocolsareneeded.”(Severance,2002)“aproperlyandpracticallydesignedMCI(MassCasualtyIncident)plan,goodcomplianceof responders,andastrongsupportsystemof respondingagenciesarethemostimportantfactorsforsuccessfulemergencyresponsetoanyMCI.”(Wen-Hueietal.,2008)PrincipleworkingGroup2016SouthWestLondon&SurreyTraumaNetwork:KelvinWright,JoelStanding,AndyRhodes,JonathanBall,PeterMartin(ED)NorthEastLondonTraumaNetwork:SteveJupp,GarethDavies,MalikRamadan,NorthWestLondonTraumaNetwork:NiinaBell,JosephDaviesSouthEastLondonKentandMedwayTraumaNetwork:VickieOsborneSmith,TomHurst,LynneWatkins,PeterMartin(EPLO),DarrenDarbyLondonAmbulanceService:TracyPorterLondonOperationalDeliveryNetworks:LornaDoneganAdditionalcontributors2016ThechairwouldliketothanksallthosefromthefourLondonTraumaNetworks,LondonHEMS,LondonAmbulanceService,OperationalDeliveryNetworks,Kent,Surrey&SussexAirAmbulancewhocontributedtothiswork.
7
Background
OverviewofTraumaNetworksSince2010,Londonhasbeenservedby4MajorTraumaNetworks–TheNorthWestLondonTraumaNetworkTheNorthEastLondonTraumaNetworkTheSouthWestLondonandSurreyTraumaNetwork.TheSouthEastLondonandKentandMedwayTraumaNetworkThedistributionofthesenetworksisshowninappendix1.Following on from national work and a drive to improve the care of the severelyinjuredpatient,therehasbeenakeendrivetoensuretherightpatientreachestheright hospital in the right time. This hasmeant amove away from patients beingtakentotheirnearestA&Edepartmentand insteadtakentothemostappropriatehospital.ThismaybeaMajorTraumaCentreoraTraumaUnit.Thisisamoveawayfrom traditional thinking but ensures that the most severely injured patientsincluding children and young people are taken to a centre that is used to dealingwiththeirinjuries.EachofthesenetworkscomprisesaMajorTraumaCentre(RoyalLondonHospital,StMary’sHospital,King’sCollegeHospital,StGeorge’sHospital)supportedbyTraumaUnits. These have governance through the Operational Delivery Networks withregularpeerreviewsandanetworkClinicalDirector.TraumapatientswithanInjurySeverityScoreofgreaterthan15areideallytakentoa Major Trauma Centre using the pan-London Triage tool by either the LondonAmbulanceServiceoranairambulance(HEMS)service.Traumanetworkshaveanintegratedsystemforensuringthatthosepatientsunder-triagedtoaTraumaUnithaverapidaccess/transfertoaMajorTraumaCentre.WithintheMajorTraumaCentreexistalloftheacuteservicesrequiredtocarefortheseverelyinjuredpatient.Themultidisciplinaryteamsconsistofthoserequiredinrehabilitationaswellasacute/criticalcare.Air ambulances deliver enhanced medical care teams and other resources to thescene and allow for stabilisation and rapid transfer from scene to the appropriatefacility.TraumaunitsplayamajorroleinthemanagementofthosecasesnotrequiringtheservicesofaMajorTraumaCentreaswellasintakingtheirlocalpatientsbackwhentheynolongerneedtheMajorTraumaCentre.Thishubandspokemodelallowsfor
8
forward flow to continue by the flow of patients back to their own geographicalareas.
PlanningAssumptionsThe reader is familiar with the London Resilience Partnership Mass CasualtyFrameworkAug2015The reader has access to http://london.gov.uk/about-us/organisations-we-work/london-prepared/planning-emergencies-capitalAllMTNshaveamajorincidentplanbasedonthecurrentlevelofthreatassessmentwhichislinkedtootheremergencyplansegCBRN.EachoftheLondonTraumaODNsisadoptingaconsistentapproachforserviceandnetwork surge and escalation. This approach will be reflected in individual NHSHospitalandTraumaServicesplans.AllhospitalswillhaveabackgroundlevelofactivityatinitiationoftheplanAmasscasualtyeventislikelytobeeitherone‘bigbang’orseverallocalisedevents.The need for national direction i.e. COBR exists in amass casualty event from anearlystage.Thisshouldbenolaterthan1hour.London Ambulance Service will have an oversight of general demand includingtraumaactivityacrossthecapital.The receipt of 8 major trauma patients per hour signifies a large impact on anindividual Major Trauma Centre infrastructure. In a TU this is likely to beconsiderablylower.With4MajorTraumaCentresinLondonpatientsshouldbedistributedfromanearlystage i.e.potentially,4major traumapatients inanhourwill trigger theuseofanadjacentfacility.(akaSurgerecognition)In a multisite incident or one where terrorist activity is involved, access to someMTCsorTUsmayberestricted.The ambulance service will be extremely busy and inter-hospital transfer will notoccurwithinnormaltimeframes.Plansneed tobe inplace toensurepatients canbe safelymanaged in their initialhospitalforseveralhoursaftertheincidentisdeclared.‘StabiliseandAdmit’versus‘Stabilise and Transfer’. For those patients who require transfer for specialistintervention,thePTSprovidershouldbeutilised.
9
Thereis likelytobeaprolongedrecoveryperiodfortheNHSduringwhichallnon-urgentelectiveworkwillneedtobemanagedasperlocalareaplans.PrimaryCareandUrgentCareshouldexpecttoseehigheracuitypatientsintherecoveryperiodinordertoalleviatepressureontheacutetrustsandtheAmbulanceService.MilitarypersonnelwillNOTbeavailableinlargenumbersinthefirst72hoursduetotaskingelsewhere,althoughhigh-leveladvicewillbeavailableviaformalchannels.All healthcare providers (public, private, independent and voluntary) will have asupportingroleinmasscasualtysituations.Theyshouldreviewlocaloperatingpolicyandinfrastructure.TraumaUnitswillberequiredtotakeP1,P2andP3casualties.Masscasualtyincidentscaninvolvechildrenandtheirneedsmustbeconsideredinplanning.IntheeventofamasscasualtyincidentinvolvingchildrenitisanticipatedthattherewillbeasignificantproportionofP1injuries.Thisisrelatedtouseofnonagespecifictriagetoolsandthedesiretoremovechildrenfromthescene.WherethenumberofchildrenoverwhelmstheMTCcapacitychildrenmaypresentathospitalswhoarenotused todealingwith seriously injured children, thereforehospitalsmustcaterforchildrenandyoungpeopleintheirMajorIncidentPlan.
OtherUsefulDocuments
AustraumaPlanNovember2011,Version1NAustralianHealthProtectionPrincipalCommittee
LondonMassCasualtyFramework
August2015
NHSEnglandEPRRFrameworkMarch2013,Version2.0
TheMedicalResponsetoMultisiteTerroristAttacksinParis
LancetViewpointNov24,2015
How Does Casualty Load Affect Trauma Care in Urban Bombing Incidents ? AQuantitativeAnalysis.
AsherHirshberg,BradfordGScottetalJournalofTrauma,April2005,p686-695
ClinicalGuidelinesforUseinMajorIncidents EastofEngland
10
CommandandControl
ActivationofthisPlanBased on their assessment at the scene, London Ambulance Service (LAS) willdeclareaMassCasualtyIncidentandwillnotifyNHSEnglandLondonRegion.ActivationoftheMassCasualtyFrameworkwilloccurwhenthenumberofcasualtiesexceeds local response capabilities beyond theMajor Incident Plan. (this may befromtwohundredtoseveralthousand)NHS England(London) will activate the Mass Casualty Framework based on theirassessment of the situation. A dynamic approach to the situation, wheredevelopmentsareanticipated,ratherthanmerelyrespondedto,willbeneeded.It is necessary to take into account the dynamics of the incident, the nature andseverityofthetraumasuffered,theratioofambulance/medicalresourcesavailable,and the accessibility and appropriateness of clinical expertise/resource available,withinthecriticaltimeframe,inordertoreducemortalityfrominjury.Therefore,itisdifficult tomapoptionsagainst fixedcasualty thresholds,and theoptions thatareimplementedwillvaryfromonescenariotothenext.Onceamasscasualtyincidenthasbeendeclared,allrelevantresponseorganisationswillactivatetheirownMajor Incidentplans (if theyhavenotalreadydoneso)andtheMetropolitanPolice Service (MPS)will conveneameetingof the Strategic Co-ordinatingGroup(SCG).
Co-ordinationofresourcesIntheeventofaMassCasualtyIncidentinLondon,triedandtestedcommandandcontrol arrangements will be implemented within every responding agency, inaccordance with the LESLP and the London Resilience Command and ControlProtocol.In line with the Command and Control Protocol, a meeting of the StrategicCoordinatingGroupwillbeconvenedandchairedby thepolice.ThisgroupwillberesponsibleforsettingthestrategyforLondonandenactingstrategicleveldecisionsregardingtheresponse.TheLondonmultiagencyCommandandControlstructure,withcorrespondinglinesof communicationwill operate in amass casualty event, aswith any othermajorincidentwithasuddenonset.TraumanetworksmustdevelopclearlinesofcommunicationwithintheirnetworksbetweentheMTCandTUs.
11
Anearlydecisionastotheuseofhospitalsforprimaryincidentorbusinessasusuali.e.STEMI/HASUneedstobetaken.CabinetOfficeBriefingRoom(COBR)willprovidenationaloversightStrategic(Gold)willprovideregionaloversightTactical(Silver)willprovidelocaloversightOperational(Bronze)willalsoprovidelocaloversightunderSilver.
MutualAidRequestsandManagementAMassCasualty Incidentwillquicklyswampresources requiringaid fromadjacentambulanceservicesaswellasadjacenttraumanetworks.Dependingonthescaleoftheincidentitmaybenecessarytoutilisenationalresourcesinsupport.Thiswouldbeparticularlytrueinamajorburnincident.TheactivationofmutualaidwillbeviaNHSEcommandandNationalAmbulanceCo-ordinationCentre.
The LAS will coordinate the movement of all pre-hospital mutual aid resourceswithinLondon.TheTraumaNetworkssupportingLondonwillincludebutarenotrestrictedto–TheSussex Trauma Network, The Wessex Trauma Network, East of England TraumaNetwork.
12
IncidentRolesandResponsibilitiesGenericrolesandresponsibilities forrespondingtomajor incidentsarecoveredbytheLESLPmanual.Thedocumentcanbefoundhere:http://www.leslp.gov.uk/.Additionalagencieshavespecificguidelinesandprocedurestorespondtoincidentswhichwouldapplyinmasscasualtysituations.
MajorTraumaCentresThe Major Trauma centres will receive P1, P2 and P3 patients as triaged andtransportedbytheon-sceneservices.The aim will be to deliver the P1 and P2 patients to theMTCs in order to avoidsecondarytransfers.TheMTCwillprovideanincidentcontrolteamwithanetwork-wideremittoadviseclinical staff in TUs. This should comprise a senior surgeon and intensivist andpaediatrictraumasurgeon.Theremustbeamechanisminplaceforpan-networkcommunicationstoaidinlocalcommandandcontrol.Effective reporting back to LAS to advise on capacity and need for support mustoccur.ThereshouldbethefacilityforadditionalCriticalCare,HoldingandTreatmentareastoallowforlocalincreaseincapacity.The‘MajorIncidentPlan’mustallowfor‘MassCasualtySupplementation’Post the initial incident, the MTC will co-ordinate patient movement across thenetwork in conjunctionwithTU teams toensurepatients aremoved in to receivetreatmentandouttoreceiveon-goingcarewhenapplicable.
TraumaUnitsPrimaryroleistodealwithallpresentationsacrossalltriagecategoriesandensuringappropriatetriage,treatmentandtransfer.NoTraumaUnitorLocalEmergencyHospitalcanrefuseanypatientsresultingfromtheincidentorotherpatients.
13
Accept P1, P2 and P3 patients who arrive via pre-hospital care providers and byothermeans.Liaisewith theirNetworkMTCMajorTraumaConsultantswith regards to thebestcareforpatients,acceptingthatpatientswhowouldnormallybetransferredtotheMTCmayneedtostaywithintheTUforpartoralloftheircare.Liaise with the designated MTC Clinical Lead/Major Trauma Centre Command toensure a prompt and efficient flow ofmajor trauma patients across the NetworkwhichcouldincludetransferringsuitablepatientsoutoftheMTC,withpatientsafetyremainingparamount.WheredirectedbyNHSE, theNetworkor theMTCto liaisewithaspecifiedoutofareaMTCwith regards to the best care for patients, whichmay include agreeingtransferarrangementstothatoranotherMTC.
TransitionbacktonormalbusinessWorkwiththeMTCandotherTUstoprovide,wherenecessary,stafftoaccompanypatientsbeingrepatriatedtothemforon-goingcare.Work with the MTC and Network to assist in repatriating patients back to theirnearesthospitalwithinanacceptabletimeframe.
AmbulanceServicesThemanagementofmasscasualtyshouldensureallpatients,eitherdirectlyaffectedbytheincidentorthosewithnon-incidentrelatedurgentandemergencycareneedscontinuetoreceivesafeandhighqualitystandardsofcare.TheambulanceservicewillprioritisecasualtiesfromtheeventthenRed1or2cases.CategoryC1-4willnotreceiveafront-lineresponse.In the event of a London based mass casualty incident the London AmbulanceService NHS Trust (LAS) has responsibility for coordinating all movements andtransportationofcasualties.
TheLASwillhaveadedicated teamofTelecommunicationsDispatcherswithin theIncident Coordination Centre (known as the SOC - Special Operations Centre) toensure telecommunications with receiving hospitals, advising them of thedeclaration and keeping them updated with the current situation and patientmovements.
Nominatedhospitalswillbeadvisedoftheincidentinthestandardformat.
Where resources allow the LAS will provide a Hospital Ambulance Liaison Officer(HALO)atnominatedhospitals.
14
Alertingmessagesfromscene/ambulancetohospitalforindividualpatientsarelikelytobevagueornotoccur.
TheLASwillcontinuetomonitorcapacityatallnominatedhospitalsandacrossthetraumanetworks.
SecondaryTransfersPatienttransferrequestsreceivedduringand immediatelyafterthe incidentphasearelikelytoincursignificantwaitingtimes.Itisexpectedthateachtraumanetworkhas a nominated trauma coordinator to oversee patients within their network.Should the need arise to move a patient from a Trauma Unit to the MTC thecoordinator will contact the Trauma Network’s Patient Transfer Service providersusing the routine telephone process and agree an appropriate time framewith aseniorclinician.
Movementofnon-traumapatientstoalternativesitesshouldonlybeconsideredasalastresortwhenallsurgecapacityisexceeded.
Networks shouldconsider theuseofhospital-basedpatient transport services.Forchildren this should include CATS and STRS (paediatric retrieval services). Theseserviceswillnotbeabletooffertheirusual levelofresponseandalternativeplansshouldbeformulatedi.e.localescort/transfer.
BusinessAsUsualWherepossibletheLASwillutilisealternativehospitalsotherthanthosedesignatedtoreceiveincidentcasualtiesfornormalbusiness.
Consideration will be given to the transportation of STEMI/ACS/HASU patients tostandalone speciality units as well asmaximising the use of all other appropriatecarepathways
Allhospitalsshouldbepreparedtocontinuetoreceivenonincidentrelatedpatientsthroughoutthedurationoftheincidentphaseandduringtherecoveryperiod
The recovery period for hospitalswill be agreedwithNHSE and the flow to themmanagedaccordingly
Nationaldirection(COBR)maydictatethesuspensionofbusinessasusualservices.
HelicopterEmergencyMedicalservices(HEMS)Duringamajorormasscasualty incidentairambulanceaircraftandpersonnelcanfulfilmultipleroles.DeploymentandtaskingwillbeviaLAScontrol.1. Tacticalsceneassessmentfromtheair-Oninitialapproachtothescenethe
aircraft is ideallyplaced toperformadetailed reconnaissanceof theentirescene.Fromatacticalpointofview(silvercommand),thisearlyinformationcan be useful for establishing effective command structures. As soon as
15
reasonably practicable an air ambulance aircraft can be used to carry theAmbulanceForwardIncidentOfficer(bronzecommand)overthesceneforanassessment regarding deployment of ground and air resources, rendezvouspoints,triageareas,HEMShelicopterlandingareasetc.;
2. Deploymentofhelicoptercrewtoscene(difficultorremoteaccess)-Initial
command from the Ambulance Service (Forward Incident Officer / BronzeCommand) can be established in any remote location and effectivecommunication links can also be set up directly from the scene. Rapidsituation reports can allow Ambulance Control to send appropriateresources, including external agency resources such as Fire Service, Police,UrbanSearchandRescueandMountainRescuepersonnel.
3. Deployment of medical/surgical/trauma/MERIT teams to scene -Medical
teamsfromthedesignatedreceivinghospitalscanbeflowntothescene.Thespeed of transfer by air means that teams can be flown directly fromhospitalsorareasoutsidethe initialcatchmentareaofthe incident, leavingthecloserhospitalsfullystaffedforthereceptionofcasualties.
4. Delivery of medical equipment/supplies to scene - The aircraft can be
effectivelyusedtotransportmedicalequipmentandsuppliestothesceneifrequired.
5. Rapidtransportationoftime-criticalpatientstodesignatedhospitals-Due
to the speed of the aircraft, patients can be transferred to appropriatereceivinghospitalscapableofdeliveringspecialistdefinitivecare.Inaddition,theflexibilityoftheaircraftalsomeansthatpatientsdonotnecessarilyhavetobetransferredtothenearestreceivinghospital,butcanbeflownfurtherafieldtoeasethepressureonthesehospitals.
ResponseCo-ordinationDue to the nature of mass casualty incidents and recent experience; it is highlyprobablethatmultipleairassetsfrommultipleagencieswillberequiredtorespond.Co-ordinationofthisresponsewillbedeterminedbythelevelofincident:6. Level 1 Incidents – Involve 2 air assets from two different agencies. Co-
ordination will be conducted between the respective tasking authoritiesusingnormalprocesses.
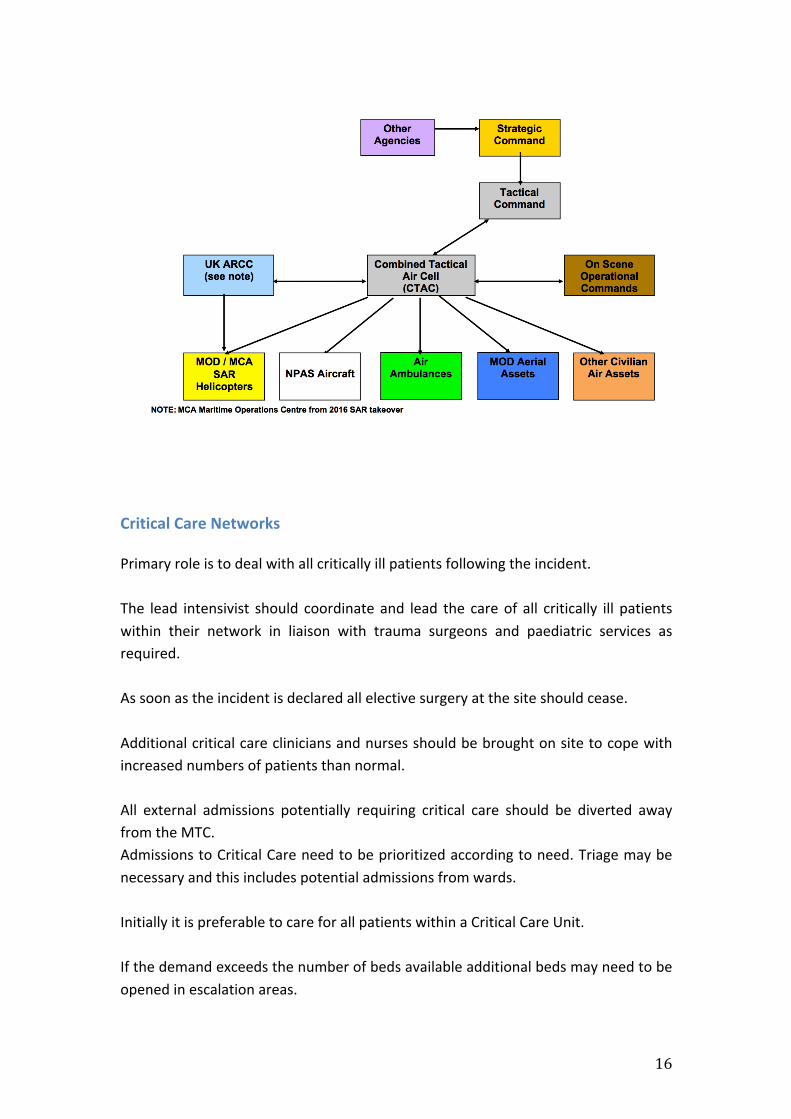
7. Level2 Incidents– Involve3ormoreairassetsfromtwoormoreagencies
attendingenduringincidentswheretacticalcommandhasbeenestablished.InsuchcircumstancesaCombinedTacticalAirCell (CTAC)willbeformed inaccordancewiththeIntegratedEmergencyAirResponseOperationsdoctrinetoprioritiseairtaskinginaccordancewiththeStrategicCommander’sintentandtheTacticalCommander’sobjectives(below).
16
CriticalCareNetworksPrimaryroleistodealwithallcriticallyillpatientsfollowingtheincident.The lead intensivist should coordinate and lead the careof all critically ill patientswithin their network in liaison with trauma surgeons and paediatric services asrequired.Assoonastheincidentisdeclaredallelectivesurgeryatthesiteshouldcease.Additionalcriticalcarecliniciansandnursesshouldbebroughtonsitetocopewithincreasednumbersofpatientsthannormal.All external admissions potentially requiring critical care should be diverted awayfromtheMTC.AdmissionstoCriticalCareneedtobeprioritizedaccordingtoneed.Triagemaybenecessaryandthisincludespotentialadmissionsfromwards.InitiallyitispreferabletocareforallpatientswithinaCriticalCareUnit.Ifthedemandexceedsthenumberofbedsavailableadditionalbedsmayneedtobeopenedinescalationareas.
17
If patients are discharged from critical care as a consequence of this incident andbefore they would normally be transitioned to ward care, then appropriatehandovertoreceivingteamsisrequired.TransitionbacktonormalbusinessManyofthecritically injuredmayrequire longstays incriticalcare.The impactonthenormalrunningofcriticalcareunitsmaythereforebeprolonged.Avoidable demand for critical care (including elective surgery) should be reduceduntilsuchatimewherebytherearenoescalationareasopenforthecareofpatientsfollowingtheincident.Secondary transfer of patients to TU and othermore localMTC (outside London)may be necessary to relieve pressures or to bring patients closer to family andcarers.
NHSEngland(London)Activate Regional Mass Casualty response plan, and alert health trustsaccordingly.
SupporttheEmergencyBedServiceinmanagingcriticalcarecapacity.EscalatetoNHSEngland(National)andbeginmutualaidprocess.NotifyLondonResilienceTeam(ifnotalreadyalertedthroughotheragency)Commission/supportthecommissioningbyCCGsofappropriatesupportservices(e.gmentalhealthassistance)formediumandlongtermpatientmanagementifrequired.SupportNHSorganisations in coordinationof rapiddischargeof acutepatientsinto community based organisations where it is safe to do so to create bedcapacityforpatientsfromtheincident.
NHSProviderOrganisationsActivatelocalmasscasualtyarrangements.Activate business continuity plans for patient capacity, patient transport asappropriatewherenormalservicesaredisruptedduetotheincident.
18
ClinicalCommissioningGroupsandCommissioningSupportUnitsActivatelocalmasscasualtyarrangements.Liaise with local organisations to support new ways of working, accelerateddischargeandsurgemanagement.Commissioningoflongtermsupport.
MetropolitanPoliceServiceCoordinatetheoverallemergencyresponse.To provide specialist staff to assist with aspects of the incident as andwhererequired, including investigators and hospital reception teams operating insupportofCasualtyBureauStaff.Assist in the designationof vehicles to act as emergency transportation at therequestoftheLondonAmbulanceServiceinsupportofpatienttransfer.
LondonFireBrigadeActivatearrangementstoallowforcasualtyrecoveryfromsceneasrequired.
LondonResilienceTeamActivatetheLondonStrategicCoordinationProtocol.
TransportProvidersPrepare to support patient movement outside of emergency vehicles at therequestofrespondingemergencyservices.
PublicHealthEnglandCommissionappropriatemonitoringofpatientsandsurvivorshealthoutcomes.
LocalAuthoritiesAssisthealthorganisationsintherapiddischargeofpatients.Manage and develop a Humanitarian Assistance Response as per thearrangementsoftheHumanitarianAssistancePlansforLondon.SupportNHSorganisationswherespecificsupportisdirectlyrequired.
19
Progression&Recovery DuringtheFirst24hoursThe first 24hrs as defined here for planning purposes begins approximately 4hrsafterdeclarationofMassCasualtyIncident(MCI),followingcompletionofamajoritytriageofallP1stoP3stotheirappropriatedesignatedTraumaNetworkMTCs&TUsbyLAS,HEMSandequivalent.UnitsthathavebeenalertedbyLASdirectlyshouldhaveactivatedtheirlocalMajorIncident Plans. In addition, if anMTC within a network is activated, then all TUswithin its Major Trauma Network will be put on standby levels accordingly. Thefollowingshouldformpartofindividualtrustresponse.
1. Additional Transport provider – It is recommended that each MTC haspotentialprovisionforadditionaltransportneedsasandwhenanMIorMCIisdeclared,toassistwithimmediateurgenttransfersofrepatriationsouttoTUswithintheirnetworktofreeupNTCcapacity.ThisTransportprovisionisnotforattendingthesceneoftheincident,butisalsotoworkinconjunctionwithLASAmbulanceLiaisonofficers.
2. Additional front line staff– In linewithbusiness asusual, all non-residenton-call staff should be called upon immediately for on-site assistance andpreparedness.Theserolesarealreadypre-definedbyunitsinternalMIPlans.(AsperlocalMIplans-expectedonsitewithin30min-1hr)
3. FurtherSupportingfrontlinestaff–ItisrecommendedthatMTCs/TUshavethecapabilitytocalluponalloperationalstafftosupportcapacitypressuresaboveandbeyondbusinessasusualorMIplans.Thisgroupofstaffshouldbephased in after the initial management of the scenario to support theadditionaltasksinanMI&MCIscenario.Itwouldbeadvisedtheyattendsitewithin4-6hourstosupportthesecondphaseoftheinitial24hrsofresponse.
4. NHS Blood, Transplant & Antidote Supplies top up – MTCs should haveenoughonsitebloodtolast2-4hrsinaMCIevent,provisionsshouldbemadeforstockreplenishmentbeyondthatintheeventofMCI,aboveandbeyondthat of normal Major Incident plans. Also to be prepared for repeatneighbouringMIorMCIevents.
5. A&E/Theatres/Trauma Ward stock Supplies top up – MTCs should haveenoughonsiteequipmenttolast12hrsinaMCIevent,provisionsshouldbemade for stock replenishmentbeyond that in theeventofMCI, aboveandbeyondthatofnormalMajorIncidentplans.AlsotobepreparedforrepeatneighbouringMIorMCIevents.
20
6. PharmacystockSuppliestopup–MTCsshouldhaveenoughonsitedrugstolast18hrsinaMCIevent,provisionsshouldbemadeforstockreplenishmentbeyond that in the event ofMCI, above and beyond that of normalMajorIncident plans. Also to be prepared for repeat neighbouring MI or MCIevents.
7. Repatriation clearance – Trauma Units not on Major Incident red alertshouldbepreparedtoreceiveallrepatriationstotheirA&Edepartments’at2hrsnotice.ThiswillpotentiallyincludepatientsnotlocaltotheirareashouldaMajor Incident orMCI occur near the locationof a neighbouring TraumaUnit within the network, should they need to be protected to receive ahigher number of P2s & P3s. See diagram below for MI & MCI TraumaNetworkUnitStandbycontrols.
Summarypointsoffurtherconsideration;
• Datadashboardandmediamanagementguidance.• Stand-down does not mean stand down at all the hospitals, some may
continueMIresponselongerandsomemaybereadytostanddown• If a trauma unit is ready to stand down they should informmajor trauma
centres• MajorTraumacentresarelikelytoremainunderpressure,longer• Recoveryplanningmuststartimmediately,duringtheincident.• Casualtiesunder-triagedtotraumaunitsandshouldbeincludedinplanning• Repatriationstocontinueandbeexpediteduntillevelsstabilised• Continuedliaisonwithmulti-agencypartners• Transportarrangements• PreparationsforVIPvisits• Internalandexternaldatarequests• ContinuedpressureonBusinessContinuity.• Resourcedepletion(staff,suppliesincludingpharmacyandIHSSetc)
21
RecoveryandResilienceThissectiondetailsrecoveryprinciples.ItisappropriatetoactionatTrust,NetworkandRegional/Supra-regionallevel.Recoverygroupswillhappenatall levelsintheNHSafteramasscasualtytypeincidentwithcentralco-ordination.RecoveryStrategicObjectiveAsuggestedstrategicobjectivefortherecoveryphaseis:
• To re-establish the affected organisation/s to such a level where they cancontribute to theprovisionof critical servicesdemandedby thepublic andhealthcarecommunity.
Thisoverreachingobjectivewouldbesupportedbytwosubobjectives:
• Toreturntoanearnormaloperationalstatusasquicklyaspossible.• Toreturntoastateofreadinessforanyfurtherincidents.
Havingaseparaterecoveryteamwillenabletheorganisationtoconcentrateonboththeinitialresponseandtherecoveryprocesssimultaneously.It isessential thatthe issueofrecovery isgivenattentionatanearlystage,as it isvery easy to become embroiled in the response to an incident and thereby missopportunitiestoenableaswiftrecoverytonormaloperations.ThechairoftherecoverygroupwillbeassignedbyNHSEngland(London)andthenthe chair will request appropriate members of staff to join. This group will notbecomeinvolvedintheresponsetotheincidents,butwillfocusonrecovery.The chair of the recovery group will be the primary owner and recorder of therecoverydecisions in theirDecision Log. It is vital that the recoverygroup is givenoverviewofeachkeychangeenactedinresponsetoanincidentandthesequenceofthese changes. The recovery group will then reverse response changes whenappropriate and to return the site to business as usual, taking advantage of anyopportunitiesforlongtermimprovement.The recovery task group will consider these further points in relation to definingnormalityafteralargescaleincident:
• Normality after a large scale incident could be significantly different fromnormalitybeforetheincident.NHSEnglandwillneedtotakethisnewsetofcircumstancesintoaccountinitsstrategicplanningandprioritysettingaftertheincident.
22
• A large scale and/or prolonged incident could have significant long termadverse impacts on people. These effects could be both physical andpsychologicalandwillneedtobetakenintoaccountwhendealingwithstaff,donorsandothersinthemonthsfollowingtheincident.
• A formal process of reviewing lessons learned and applying these to the
relevantincidentplans,isimportanttoimprovefuturerecoveryoperations.RecoveryGroupCompositionThe group should contain experts from each impacted area and so each recoverygroupwillbedifferent,dependentonthesituation.Membersoftherecoverygroupcannotalsobemembersoftheresponsegroup,duetotheintenseworkloadofeach.Itshouldberecognisedthatstaffoncall,willinalllikelihoodbealreadyrespondingto the incident, soother staffwill have tobenominated tomakeup the recoverygroup.Asuggestedlistofdepartmentstoberepresentedintherecoverygroup(regional)is
1. CorporateCommunications2. Medical3. QualityAssurance4. IT5. HumanResources6. Finance7. Hospitals8. Facilities9. Transport
RecoveryDirectionandAdministrationThe primary action for the group is to establish a strategy, which sets out thedirectionthatalldecisionscanbemeasuredagainst.Accuraterecordkeepingregardingrecoveryisofparamountimportance.
• Thereneedstobeaclearaudittrailwithcomprehensiverecordsoftimings,notifications,decisions,actionsandexpenditure.Itwouldbebeneficialtousethe same recording systems that have been used in the response for therecoverygroupaswell.
• Review the viability of the organisation/s, to establish if they can berecovered.
• Establish time targets for key points of the recovery and a provisionaltimeframeforrecoveryofthesiteasawhole.
• Assess the impact on services and financial agreements and consider longtermfinancialimpactsandimplicationsfortheorganisation.
23
1) Theaimshouldbetorecovercriticalservices/activitiesfirst.2) Monitoravailabilityanddemandforproductsandservicestoidentifygapsto
ensure thatNHS England (London) is not anunnecessary constraint on thewiderNHS.
3) Re-establishnormalworkingpractice.StockUrgentpriorityshouldthereforebegiventorestoringstocksasquicklyaspossible.Consideration should be given to the impact of replenishing stock in the affectedregionattheexpenseofthewiderNHS.Closeliaisonwithhospitalsandinformationabouttheirstockswillbevital,including:criticalconsumables,fuel
Discussions with suppliers/contractors on the restoration actions should be heldconsidering:
The availability of suppliers/contractors that are required for criticalactivitiesTheresilienceofsuppliers/contractors- ifthis isunsatisfactory,considersourcingalternatives
EquipmentArrangeforinspection/service/replacement/recalibrationasrequired.Staff
• Providesupporttostaffthathavebeenpersonallyaffectedbyincident.• Reviewminimumstaffingrequirementsandidentifyanygapstoreplacestaff
whowillnotreturntowork.• Manageuseofanyvolunteers.• Monitor annual leave, dependent care leave, sick leave and other reasons
staffmaynotbeatwork.• Reviewanybacklogofstaffrelatedinformation(DBS,qualifications,etc.)and
arrangestafftrainingwhererequired.• UpdatekeyemergencycontactandOnCallrotainformation
Communication
• Ensurekeystakeholders(especiallyhospitals,usersofproductsandservices,and key suppliers) are kept fully informed regarding recovery changes andprogress.
• Acknowledgestaffcontributionsandthoseofexternalpartners,contractors,suppliers,volunteersetc.
• ProvideregularupdatesviaCommandandControl,intranet,externalwebsiteandConnect.
• Offer reassurance, advice, guidance and access to Occupational Health asappropriate.
• Reviewcommunicationsplans.
24
• Keepthepublic,patientsandstaffappraisedonrestorationplans.• Reassurethepublicandstaffofacontinuingservice.
InformationRestoreinformationBack-up/restorecoreinformationasrequired:- Staffrecords.- Accounting/payrollrecords.- Donorrecords.- ITsystems.- Paperbasedsystems.- Anyotherkeysystem/data.Premises
• Security-Reviewarrangements• Contamination-Identifyareasthatrequiredeepclean/decontaminationand
initiatecleaningincludingremovalofanywasteproducts• Maintenance-Identifyandarrangeformaintenanceworktobecarriedout,
ensurethatalternativefacilitiesareavailableifnecessaryRestoration
IfanyfacilitieshavebeenusedformultioralternativepurposesconsiderimplicationsofrevertingtooriginalpurposeIn cases of partial/total relocation of services consider implications tofullyrestoreservices
MutualAidArrangements
• Review agreements with other organisations regarding staffing, use offacilitiesandsupplies.
• Establishnewagreementswithorganisationsifpreviousarrangementsarenolongerviable.
LessonsIdentified
• Reviewandupdateprocessesandactivities.• Sharebestpracticeandlearningwithotherhealthpartners.
RecordKeeping,IncidentLogsandPostIncidentReports
At all levels of command, it is necessary to clearly document the appointment ofIncidentManagers,andthismustbedoneatthetimeofappointmentorchangeaspartoftheIncidentLog.Themanagementofanincidentwillultimatelyresultinsomeformofrecordoftheeventsthatunfoldedinbringingaboutasuccessfulconclusiontotheincident.Theserecordsmaytakeoneoranyofthefollowingforms:
- Minutes- ChronologicalLogs
25
- PersonalLogs- DecisionLogs- Emails- Maps- FlipCharts- ComputerEntries- Photographs- PressReleasesandReports- AudioRecords
Itisimportanttorememberthatanyrecordsofeventsaresubmissableaspotentialevidence in the event of a Public Inquiry or Legal proceeding. All entriesmust beclear,intelligible,andaccurate.IncidentLogBookAcrossalllevelsofincidenttype,whereanincidenthasbeennotifiedordeclareditwill be the responsibility of all involved in the management and recovery of theincident, to create and maintain an Incident log. This log will capture allcontemporaneous notes (notes made at the time or shortly after an event orincident).All decisions and risk assessments will be recorded in this log. The log will behandwritten and each decision or risk assessment outcome will be recorded,together with the rationale for making it, why other options were not deemedsuitable,thetimeanddateitwasmade,andthesignatureofthepersonmakingit.Thelogshouldbecompletedatthetimeandwillcaptureallkeyeventsduringtheincident.SuggestedAgendaforFirstRecoveryGroupMeetingThe following is a list of points that could be put on the initial agenda for anyRecoveryCo-ordinatingGroupmeeting.
1. Introductions2. Termsofreferenceforthegroup3. Membership
a. Responsibilitiesandauthorityb. Otheragenciesthatmayberequired
4. Briefing / progress report, including the latest impact assessment and theresponsestrategy(briefoverview,keepconcise)
5. Agree recovery strategy (including detailed objectives and targets asnecessary)
6. Immediateactions/orurgentissuesrelatedtotheincident7. Recoveryactionplanformulationanddelegationoftasks(includingdeciding
whatSub-Groupsarerequired)8. Prioritiesforaction9. Anyotherissues10. Scheduleofmeetings
26
PreparednessRolesandResponsibilitiesItistheresponsibilityofallagenciestoprepareandpracticefortheuseofthisplan.
MajorTraumaCentresShouldregularlycheckandupdatetheirmajorincidentpolicy.MustconsiderthethreatofterroristattackeitherinLondonorelsewherewithintheNetwork.An expectation that up to 100 walking wounded patients could be received plusmoreseverelyinjuredpatients.That usual lines of communications within the Trauma Unit, the Network MTCand/orspecialistcentresmaybedownorinundated.ActioncardsforeachinhousespecialtyincludingEmergencyDepartment,Theatres,SurgicalTeams,Radiologistetc.Develop the role of a senior surgical floor walker to liaise with internal specialityleads and theMTC specialists. Thiswill also be available to provide advice to theTraumaUnits.Workwith the Critical CareNetwork to ensure a visible real time bed status is inplaceforintensivecareandhighdependencypatients.Workwithin their TraumaNetwork to develop a robust Network Planwhichmayinclude:
1) a system for tracking patients across the Network during the MCI andduring/aftertransitiontonormalbusiness2) communicationswith press agencies, patients, relatives and theworriedwell3) agreeing with relevant Clinical Commissioning Groups and NHS England(NHSE) their supporting role with repatriating patients/displaced patientsaftertheevent.4)agreeingwithroleoflocalemergencyhospitals/minorinjuryunitsduringaMI/MCI
Ensure all appropriate surgeons have completed a recognised Damage ControlSurgerycourse.DamageControlPrinciplesareinappendix2.Ensureanuptodatecontactlistisavailable,settingoutwhotoliaisewithduringtheincident itself on a clinical, EPPR, and executive/management level during theincident itself, transitionback tobusinessasnormal, for repatriations,non traumatransfersoutandpostincident.
27
Ensure that adequate supplies of compressive dressings, tourniquets and novelhaemostaticsareavailable.Major Trauma Centres must ensure that within their networks the key areas ofconsideration:
Resuscitation and Paediatric Intensive Care Capacity, including in time ofoverwhelming demand creating intensive care capacity for children withintheadultsetting.Triage–anunderstandingofagespecificphysiologicalvariables.TheuseofSMARTtapesmayassist.Clear pathways and guidance for those hospitals not used looking afterchildren who are seriously injured. Telephone advice will need to be bothpaediatricspecificandtrauma.Confidenceofnonpaediatricspecialties:OutreachtoTraumaUnits, trainingand guidelines need to be provided to assist with the confidence of non‘trained’specialties.Equipment:TobeabletoprovideDamageControlResuscitationtomultiplechildren,includingPaediatriccoderedguidelines.
TraumaUnitsEachUnittoreviewtheirTrustMajorIncidentPlaninthebodyoractioncards:Consider the threat of terrorist attack either in London or elsewhere within theNetwork.An expectation that up to 100 walking wounded patients could be received plusmoreseverelyinjuredpatientsnotnormallywiththeTU’scohortofinjuredpatients.That expertise may need to be sought via telephone consultation for specialistadvicewithrespecttomultiplepatientsinjuredwithburns,chemicalattack,gunshotwounds,limbamputationand/orpatientsrequiringplasticsurgeryintervention.Liaison with the primaryMajor Trauma Centre and co-located Trauma Units and,wherenecessary,otherMajorTraumaCentres(MTC).That usual lines of communications within the Trauma Unit, the Network MTCand/orspecialistcentresmaybedownorinundated.ActioncardsforeachinhousespecialtyincludingEmergencyDepartment,Theatres,SurgicalTeams,Radiologistetc.Develop the role of a senior surgical floor-walker to liaise with internal specialityleadsandtheMTCspecialists.
28
TUsandEmergencyHospitalswithintheregionwhoarerelativelyunaffectedbythecasualtysurgeare likely toberequired toreceiveredistributedpatients fromnontrauma specialties, such as stroke/cardiac etc. This could be directly in from pre-hospitalcareprovidersorfromaffectedMTCsorotherTUs.Workwith the Critical CareNetwork to ensure a visible real time bed status is inplaceforintensivecareandhighdependencypatients.Workwithin their TraumaNetwork to develop a robust Network Planwhichmayinclude:
1) a system for tracking patients across the Network during the MCI andduring/aftertransitiontonormalbusiness2) communicationswith press agencies, patients, relatives and theworriedwell3) agreeing with relevant Clinical Commissioning Groups and NHS England(NHSE) their supporting role with repatriating patients/displaced patientsaftertheevent.4)agreeingwithroleofLocalEmergencyHospitals/MinorInjuryUnitsduringaMCI.
Trauma Units (TUs) will ensure they fully meet the Pan London/Local Networkcriteria.TraumaUnitswillensuretheyhavetheinfrastructureandstaffskillset/mix24/7todealwith:
TheimmediatecareofveryseriouslyinjuredpatientswhomayarrivebutwhowouldnormallygodirectlytoaMajorTraumaCentre(MTC).Lessseverelyinjuredtraumapatients,includingthewalkingwounded.
Ensure all appropriate surgeons have completed a recognised Damage ControlSurgerycourseandallothertrainingsetoutintheTUcriteriaismet.Thiswillenablethe TUs to deliver DCS to a larger cohort of patients so removing the need fortransfer.DamageControlPrinciplesareinappendix2.Ensureanuptodatecontactlistisavailable,settingoutwhotoliaisewithduringtheincident itself on a clinical, EPRR, and executive/management level during theincident itself, transitionback tobusinessasnormal, for repatriations,non traumatransfersoutandpostincident.Ensure that adequate supplies of compressive dressings, tourniquets and novelhaemostaticsareavailable.

29
AmbulanceServicesDevelopandexerciseaMassCasualtyPlaninaccordancewithstatutoryobligationsdefinedinTheLondonResiliencePartnershipMassCasualtyFrameworkVersion3.2August2015p22.
CriticalCareServicesEachTraumaNetworkshouldreviewwheretheircriticalcarecapacityisandhowitcanbeaccessed.ThisshouldincludehospitalsdesignatedasMTC,TUandalsootherhospitalsthatmaynothaveanEDormaybe inthe independentsectorthatcouldprovidesupportincaseofoverwhelmingneed.EachcriticalcareunittoreviewtheirTrustMajorIncidentPlan.ThereshouldbeanexpectationthateachMTCshouldbeabletofreeup10level3bedswithin2hoursoftheincident.Each MTC should have plans to provide a further sustained increase in level 3capacityforanother10patientswithin12hoursoftheincident.ThereshouldbeanexpectationthateachTUshouldbeabletofreeup5level3bedswithin2hoursoftheincident.Localplanswoulddictatehowadditionallevel3capacitycanbefreedup.Local plans should be in place to open up escalation areas for level 2 patients inordertofreeuptherequiredlevel3capacities.Eachcriticalcareunitshouldregularlyreviewtheresourcesrequiredtoopenuptherequiredcapacityintheeventofsuchanincident.Thisshouldincludetheprovisionoftrainedstaff,equipmentanddrugs.
30
Appendices
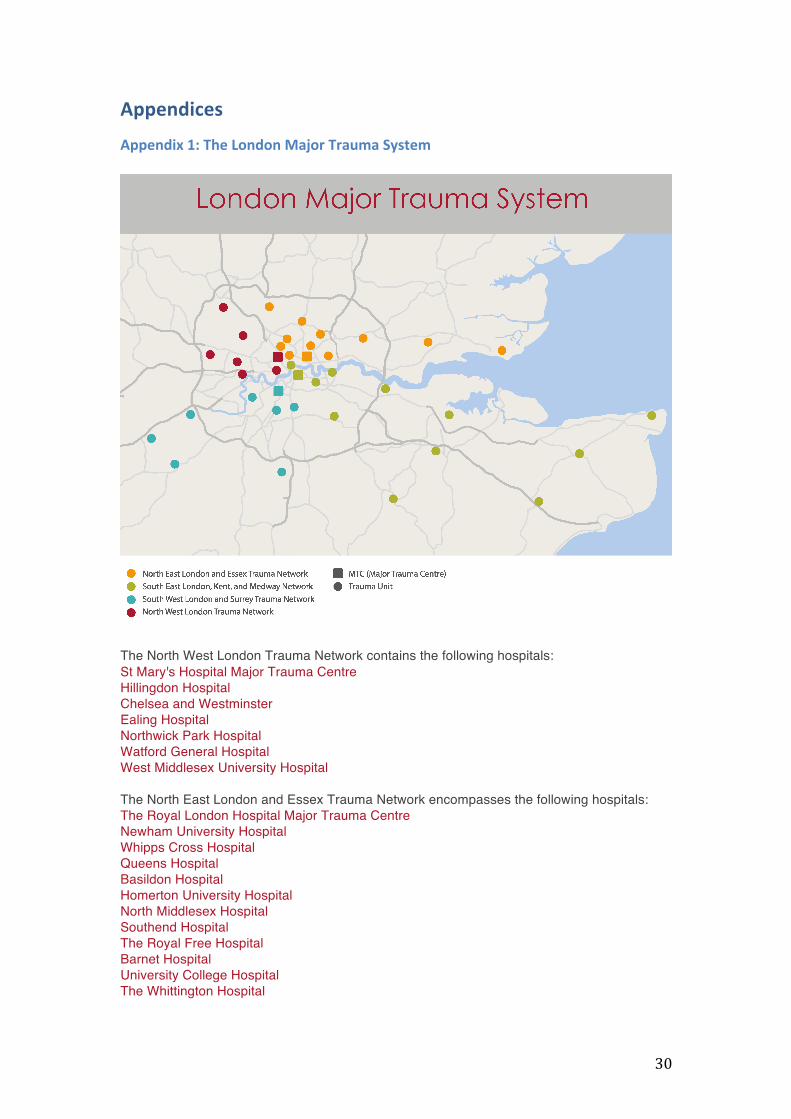
Appendix1:TheLondonMajorTraumaSystem
The North West London Trauma Network contains the following hospitals:St Mary's Hospital Major Trauma Centre Hillingdon Hospital Chelsea and Westminster Ealing Hospital Northwick Park Hospital Watford General Hospital West Middlesex University Hospital The North East London and Essex Trauma Network encompasses the following hospitals: The Royal London Hospital Major Trauma Centre Newham University Hospital Whipps Cross Hospital Queens Hospital Basildon Hospital Homerton University Hospital North Middlesex Hospital Southend Hospital The Royal Free Hospital Barnet Hospital University College Hospital The Whittington Hospital
31
The South West London and Surrey Trauma Network contains the following hospitals: St George's Hospital Major Trauma Centre St Peter's Hospital Chertsey Croydon University Hospital St Helier Hospital Kingston Hospital Royal Surrey County Hospital Frimley Park Hospital East Surrey Hospital The South East London, Kent and Medway Trauma Network contains the following hospitals: Kings College Hospital Major Trauma Centre St Thomas' Hospital Darent Valley Hospital William Harvey Hospital Queen Elizabeth Queen Mother Hospital Maidstone Hospital Kent and Canterbury Hospital Tunbridge Wells Hospital Medway Maritime Hospital Princess Royal University Hospital Orpington University Hospital Lewisham Queen Elizabeth Hospital London
32
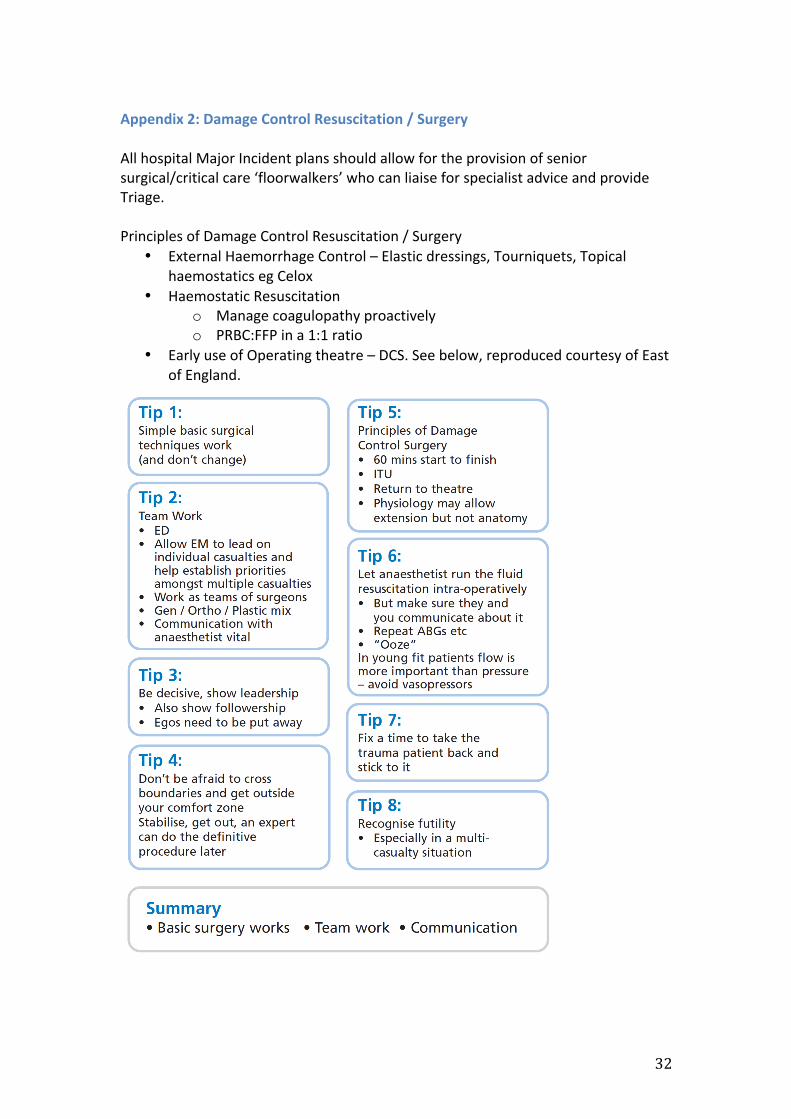
Appendix2:DamageControlResuscitation/SurgeryAllhospitalMajorIncidentplansshouldallowfortheprovisionofseniorsurgical/criticalcare‘floorwalkers’whocanliaiseforspecialistadviceandprovideTriage.PrinciplesofDamageControlResuscitation/Surgery
• ExternalHaemorrhageControl–Elasticdressings,Tourniquets,TopicalhaemostaticsegCelox
• HaemostaticResuscitationo Managecoagulopathyproactivelyo PRBC:FFPina1:1ratio
• EarlyuseofOperatingtheatre–DCS.Seebelow,reproducedcourtesyofEastofEngland.
33
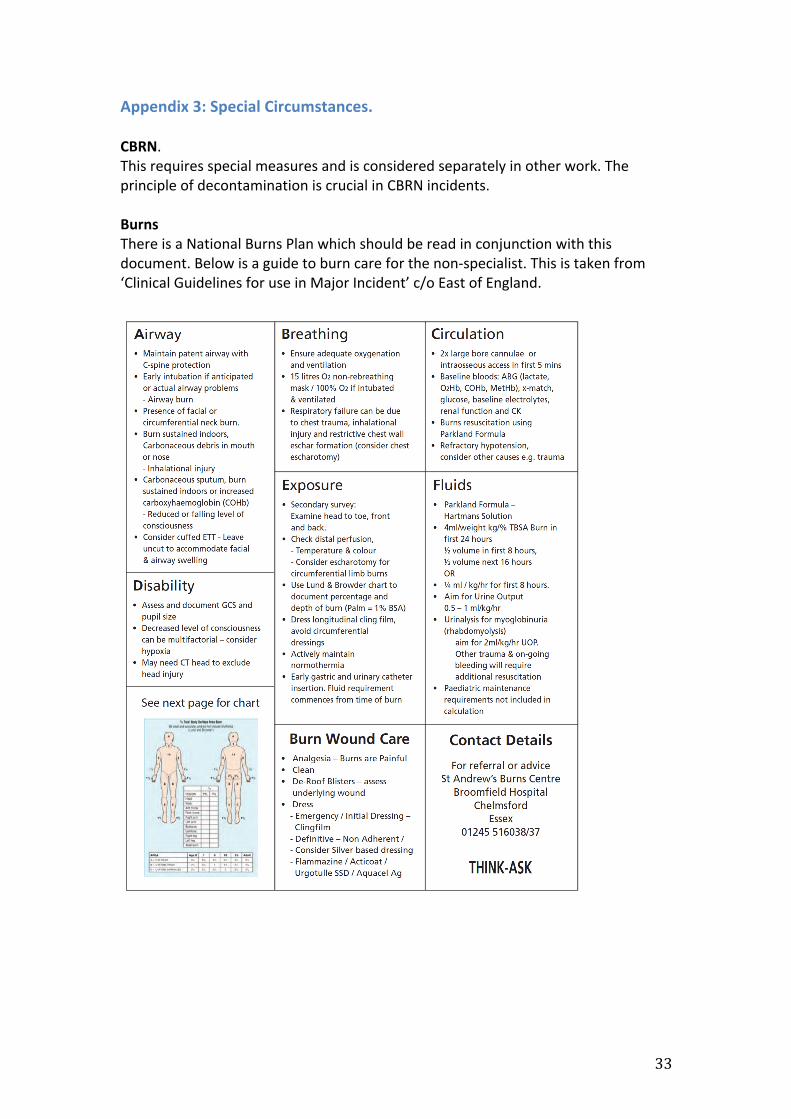
Appendix3:SpecialCircumstances.CBRN.Thisrequiresspecialmeasuresandisconsideredseparatelyinotherwork.TheprincipleofdecontaminationiscrucialinCBRNincidents.BurnsThereisaNationalBurnsPlanwhichshouldbereadinconjunctionwiththisdocument.Belowisaguidetoburncareforthenon-specialist.Thisistakenfrom‘ClinicalGuidelinesforuseinMajorIncident’c/oEastofEngland.
34
Appendix4:TriageInthecontextofamajorincidentthetermtriageisusedtodecideonthepriorityoftreatment/transport.Inanon-majorincidentcontextthetermisusedtodefinethebestdestinationhospitalforapatient.Bothovertriageandundertriageareassociatedwithincreasedmortality.DuringmajorincidentstheabilitytosupportsecondarytransferfromTUtoMTCwillbelimited–duringmasscasualtyscenariositmaybeimpossible.During a mass casualty incident there is a significant risk of overwhelming the 4majortraumacentresifthetraumatriagetoolisfollowed.Distinguishingbetweenamajorincidentandmasscasualtysituationmaybedifficultiftherearemultipleincidentsites.The trauma triage tool is too sensitive to use during amass casualty incident andshouldbedisregarded.Thetriagesorttoolrequiresadditionalanatomicaltriagebyaseniorclinicianinordertopreventpotentiallyavoidablemortality.Ambulanceresources(vehiclesandstaff)willbescarceintheearlyphaseofamasscasualtyevent.Patientsarelikelytoarriveathospitalbyothermeans.High velocity firearm incident and a significant explosion may produce a highnumberofpatientswithmajor limb injurieswith theriskofexsanguinationandorlimblossduetovascularinjury.Transfertohospitalassoonaspossibleisapriority.Duringanincident:Expertandtimelymedicaladviceshouldbeavailabletotheambulancecommandersand a major focus of this advice should be on triage strategy (priority anddestination).Initial triage at scene should continue to be performed using the sieve / sortmethodology. Creating P1, P2 and P3 categories. The category of P4 (Expectant)shouldbeconsideredinamasscasualtyscenariobutmustbesuitablyauthorisedbyCommand.Subsequent anatomical triage must be undertaken by the most experiencedcliniciansonscene.WherepossiblethisshouldbeamemberoftheLASMERIT,APPorLondon’sAirAmbulance(HEMS)emerituspools.This re-triage shoulddefinewhich typeof receivinghospital thepatient shouldbetakentoe.g.MTC,TUwithspecificspecialtyorTU.ChildrenandYoungpeoplemaybetriagedwithagespecifictoolsorusingthetoolshownbelow.Traumaunitshaveamajorroleintreatingpatientsinamasscasualtysituation.

35
Patients thatwouldnormallybetriagedtoaMTCwillbetriagedtoTUs;exampleswillvarydependingonthesurgicalcapabilitiesoftheunit.Co-locationoftheCasualtyClearingCentremedical leadwiththeLoadingOfficerispartoftheLondonAmbulanceServiceplan.Consideration shouldbegiven tousingambulances to theirmaximumeffect. Staffshouldusediscretionandusevehiclestotransportmultiplepatientsatatime.EachTUmusthavedefinedtelephonesupportfromitsMTCinthehandlingofcasesduringanevent.If information at scene is available to assist in assigning the type of destinationhospitals itshouldbeused.However intheabsenceofthis,destinationsshouldbedefinedbytheLondonAmbulanceServiceSpecialistOperationsCentremakingitasequitableaspossible.Allpatientsshouldundergore-triageattheMTC/TU.There should be early and clear reporting to command regarding numbers ofpatients.