pandemic influenza: a zoonotic...
TRANSCRIPT
Pandemic Influenza: A Zoonotic InfectionKathleen M. Neuzil, MD, MPH
PATHUniversity of Washington
School of MedicineApril 28, 2008
Questions
•
What is the epidemiology of human influenza?
•
What is the role of animals in influenza epidemiology?
•
When do we worry about a pandemic?
Excess mortality: Hallmark of epidemic influenza
•
1837: Robert Graves, Dublin.
•
1847: William Farr, London.
•
1887-1956: Selwyn Collins, USA.
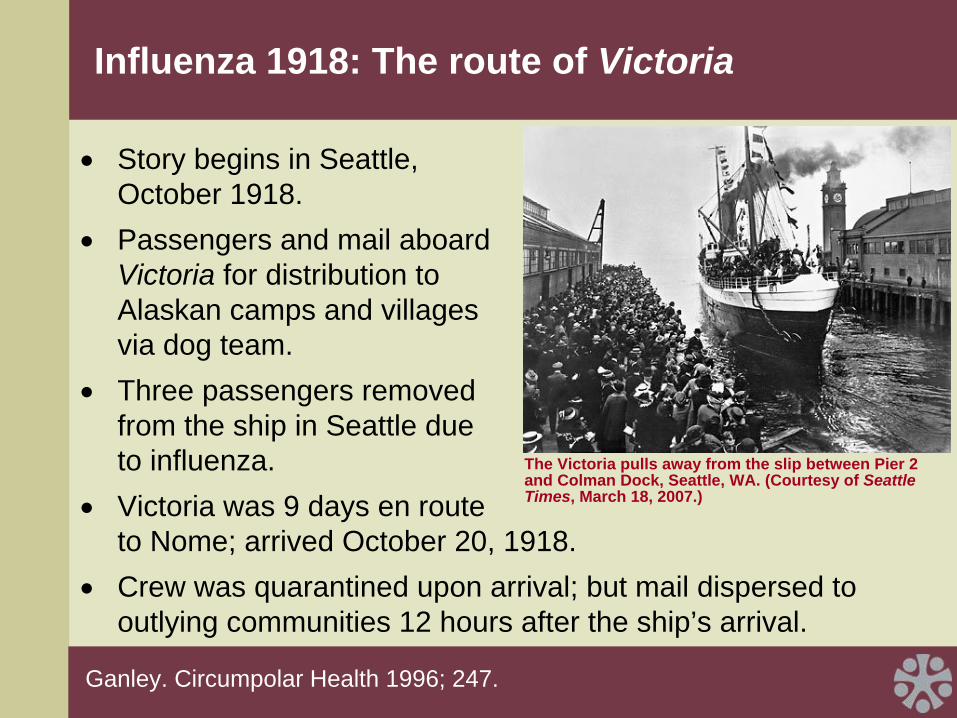
Influenza 1918: The route of Victoria
•
Story begins in Seattle, October 1918.
•
Passengers and mail aboard Victoria for distribution to Alaskan camps and villages via dog team.
•
Three passengers removed from the ship in Seattle due to influenza.
•
Victoria was 9 days en route to Nome; arrived October 20, 1918.
•
Crew was quarantined upon arrival; but mail dispersed to outlying communities 12 hours after the ship’s arrival.
Ganley. Circumpolar Health 1996; 247.
The Victoria pulls away from the slip between Pier 2 and Colman Dock, Seattle, WA. (Courtesy of Seattle Times, March 18, 2007.)
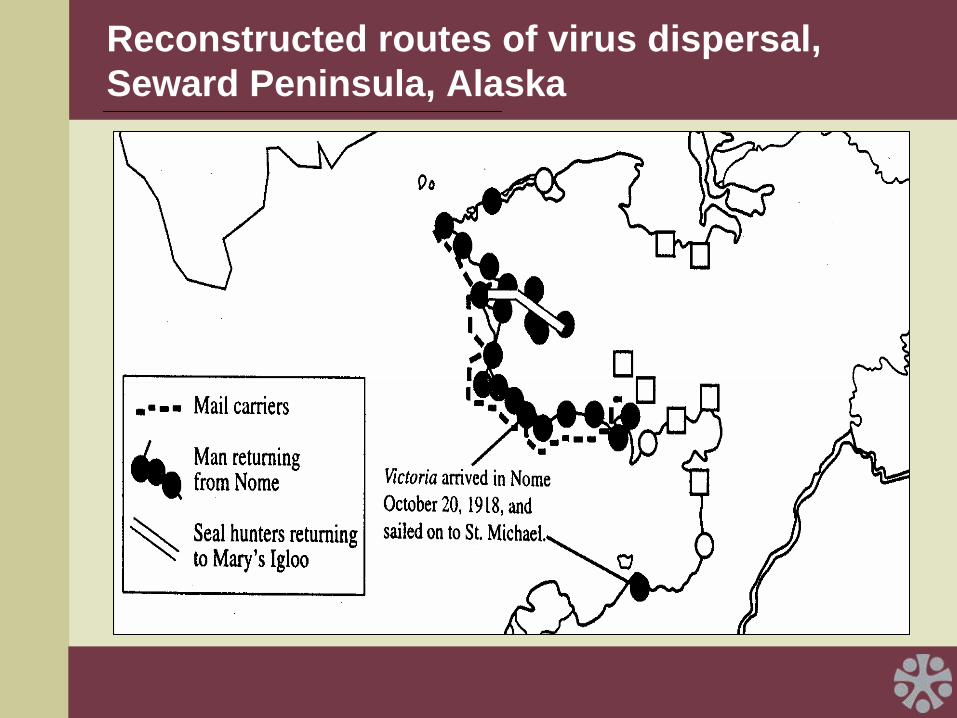
Reconstructed routes of virus dispersal, Seward Peninsula, Alaska
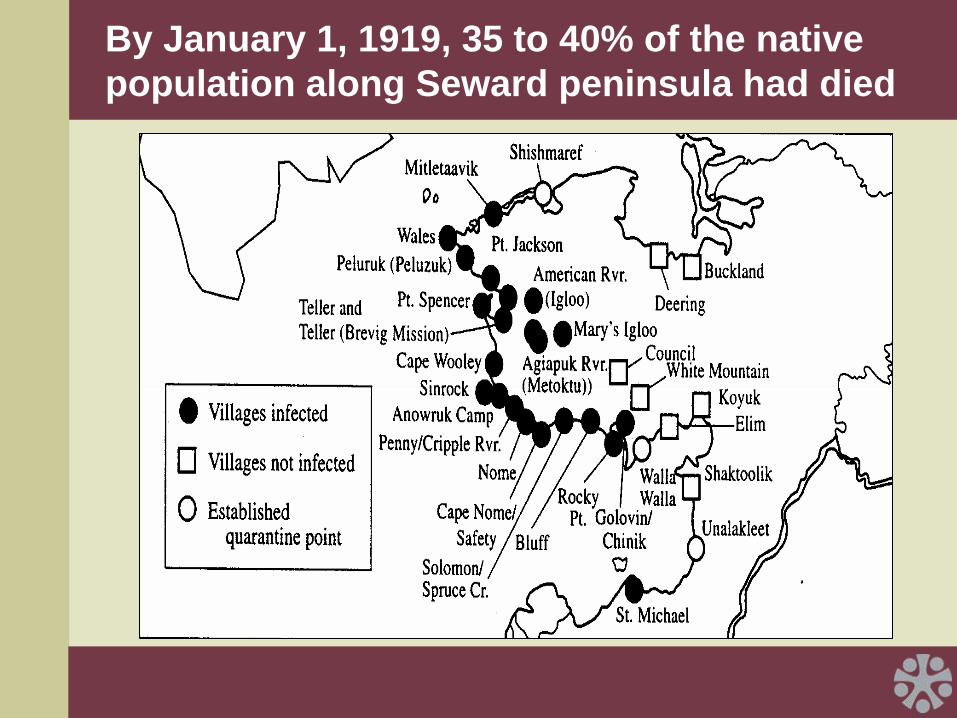
By January 1, 1919, 35 to 40% of the native population along Seward peninsula had died
Teller Mission, Alaska: 1918
•
Influenza spread through the village in 5 days.
•
Killed 72 people (85% of the adult population).
•
Victims buried in mass grave in permafrost.

Teller Mission, Alaska: 1997
•
Four victims exhumed; in situ lung biopsy.
•
Tissue: massive pulmonary hemorrhage (bleeding into lung) and edema (swelling of lung).
•
Influenza RNA isolated and sequenced (A/Brevig Mission/1/18/H1N1).
Reid et al. Proc Natal Acad Sci 1999; 96: 1651.Taubenberger JK et al. Science 1997; 275: 1793.
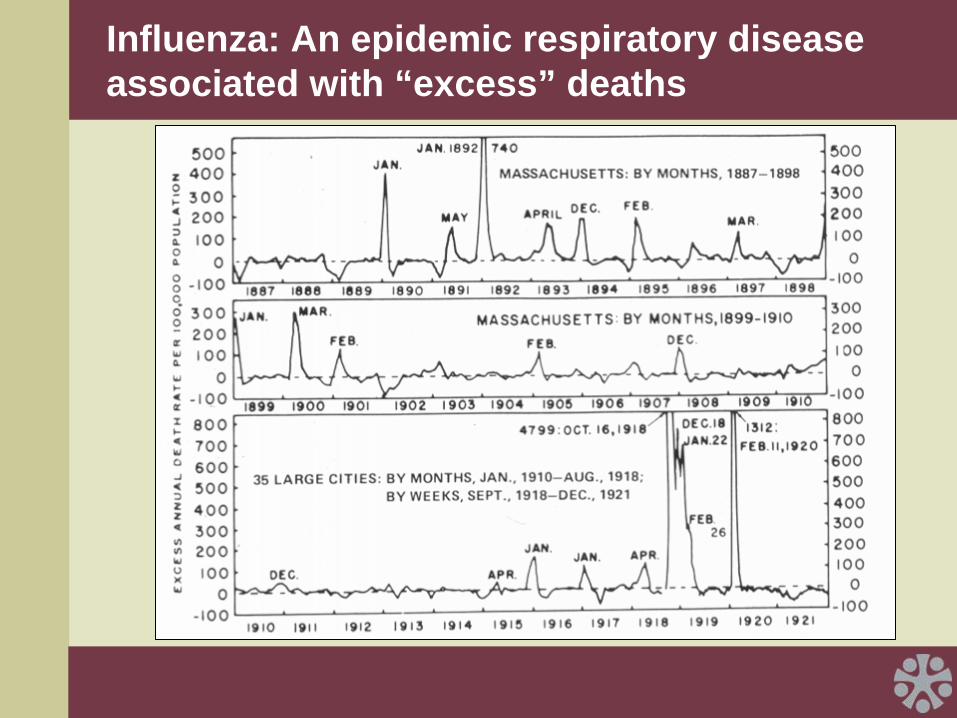
Influenza: An epidemic respiratory disease associated with “excess” deaths
“Hunt up your wood-workers and cabinet-makers and set them to making coffins. Then take your street laborers and set them to digging graves. If you do this you will not have your dead accumulating faster than you can dispose of them.”
Amer J Public Health 1918; 8: 787.
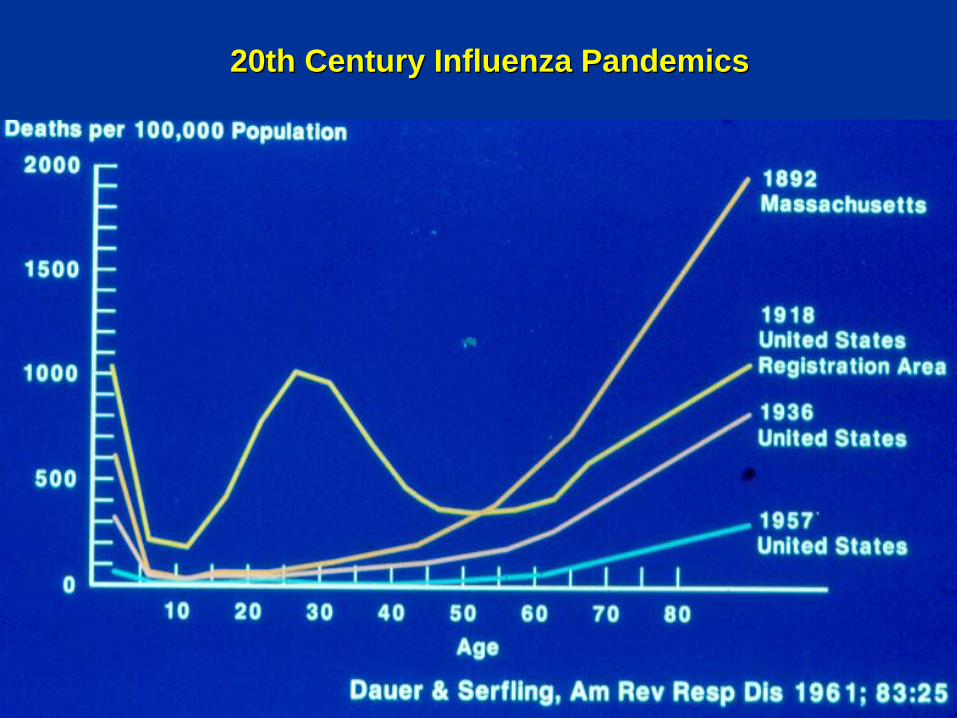
20th Century Influenza Pandemics20th Century Influenza Pandemics
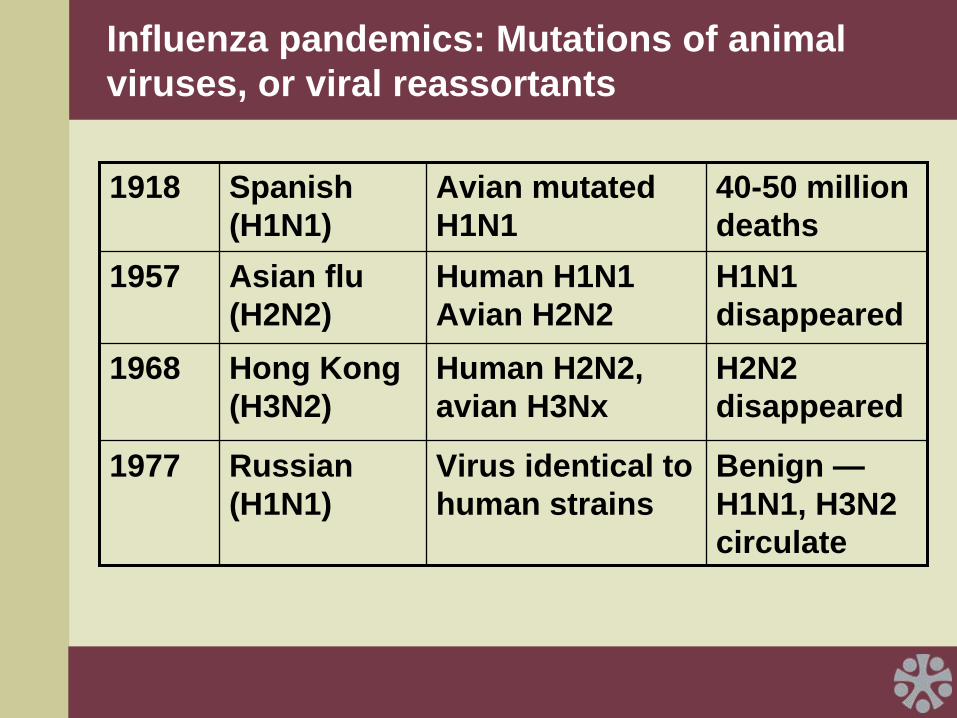
Influenza pandemics: Mutations of animal viruses, or viral reassortants
1918 Spanish (H1N1)
Avian mutated H1N1
40-50 million deaths
1957 Asian flu (H2N2)
Human H1N1 Avian H2N2
H1N1 disappeared
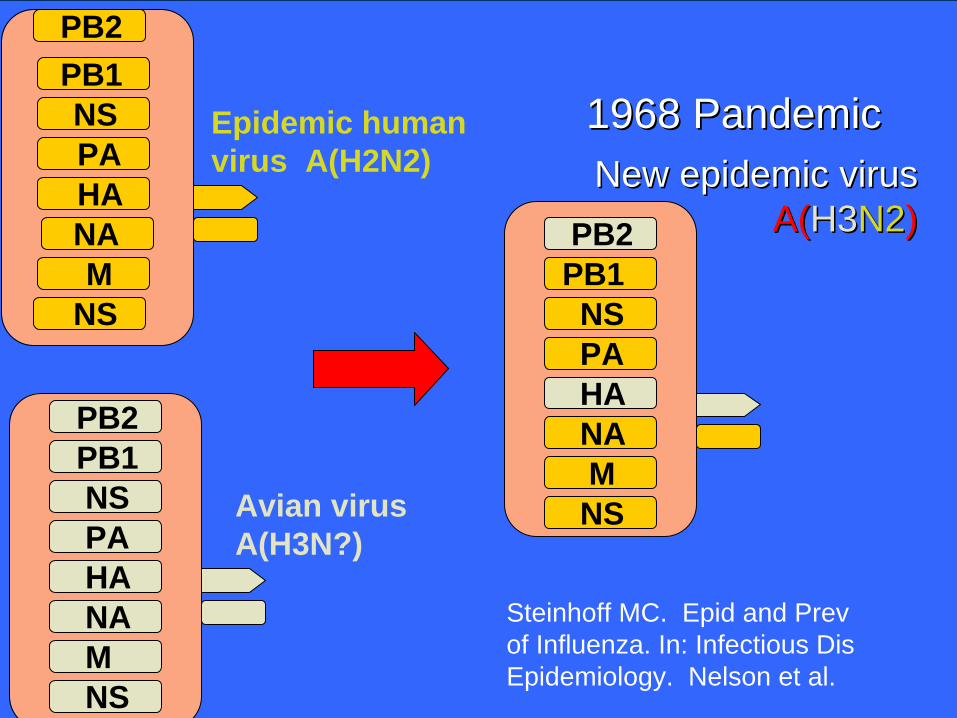
1968 Hong Kong (H3N2)
Human H2N2, avian H3Nx
H2N2 disappeared
1977 Russian (H1N1)
Virus identical to human strains
Benign — H1N1, H3N2 circulate
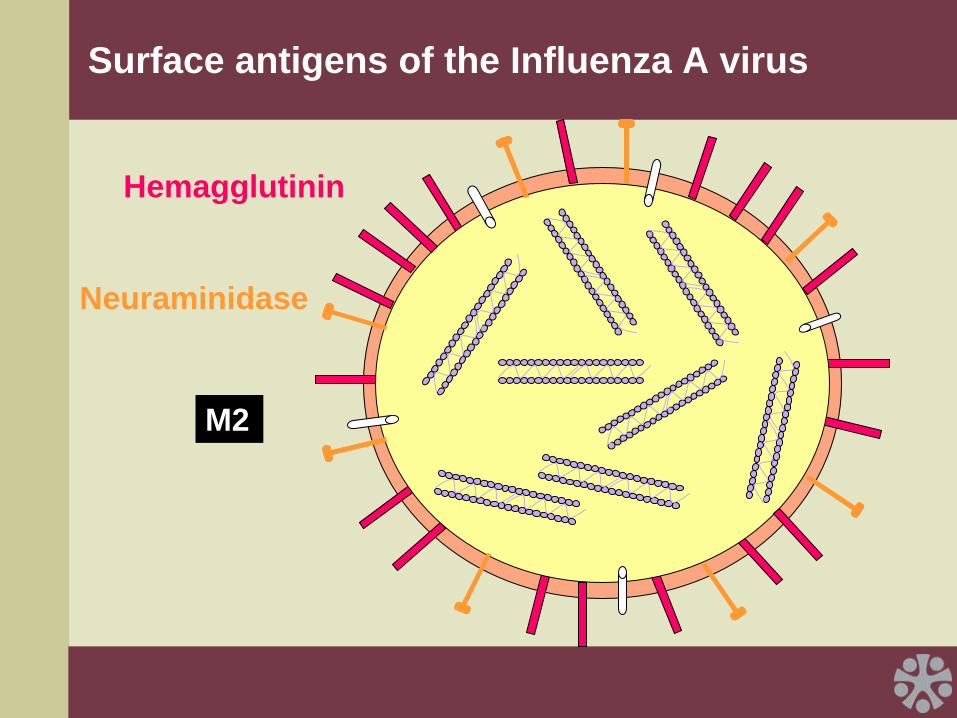
Surface antigens of the Influenza A virus
Hemagglutinin
Neuraminidase
M2
HANAM
NS
NSPAHANAMNS
PB2PB1
PB2
PB2
NSPA
PB1
HA
MNS
NA
PANS
PB1
Epidemic human virus A(H2N2)
Avian virus A(H3N?)
New epidemic virusNew epidemic virus A(A(H3H3N2N2))
1968 Pandemic1968 Pandemic
Steinhoff MC. Epid and Prev of Influenza. In: Infectious Dis Epidemiology. Nelson et al.
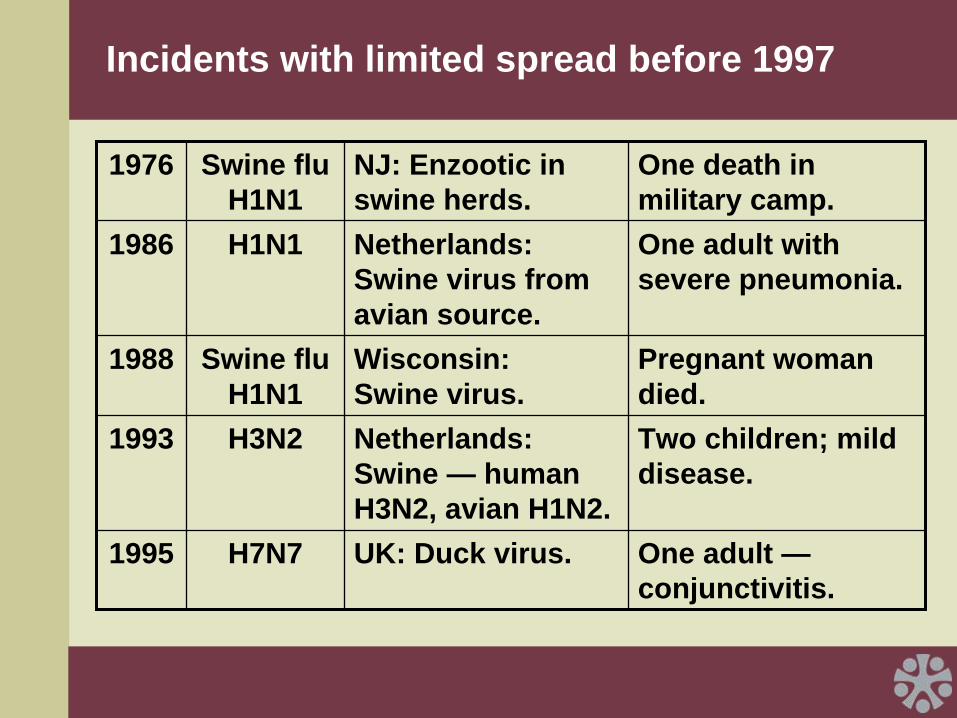
Incidents with limited spread before 1997
1976 Swine flu H1N1
NJ: Enzootic in swine herds.
One death in military camp.
1986 H1N1 Netherlands: Swine virus from avian source.
One adult with severe pneumonia.
1988 Swine flu H1N1
Wisconsin: Swine virus.
Pregnant woman died.
1993 H3N2 Netherlands: Swine — human H3N2, avian H1N2.
Two children; mild disease.
1995 H7N7 UK: Duck virus. One adult — conjunctivitis.
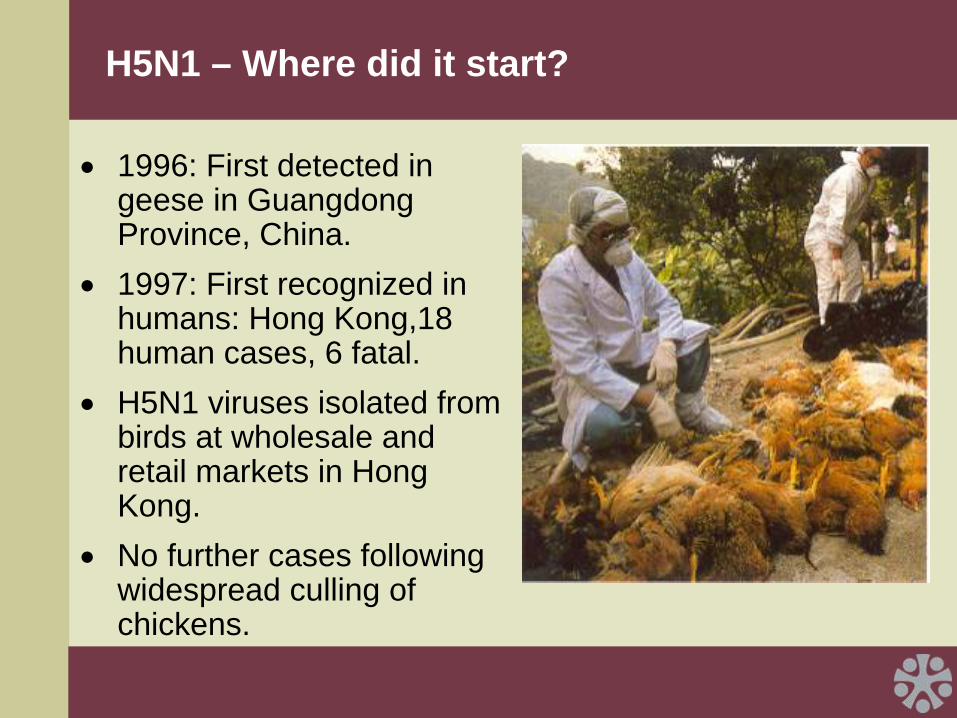
H5N1 – Where did it start?
•
1996: First detected in geese in Guangdong Province, China.
•
1997: First recognized in humans: Hong Kong,18 human cases, 6 fatal.
•
H5N1 viruses isolated from birds at wholesale and retail markets in Hong Kong.
•
No further cases following widespread culling of chickens.
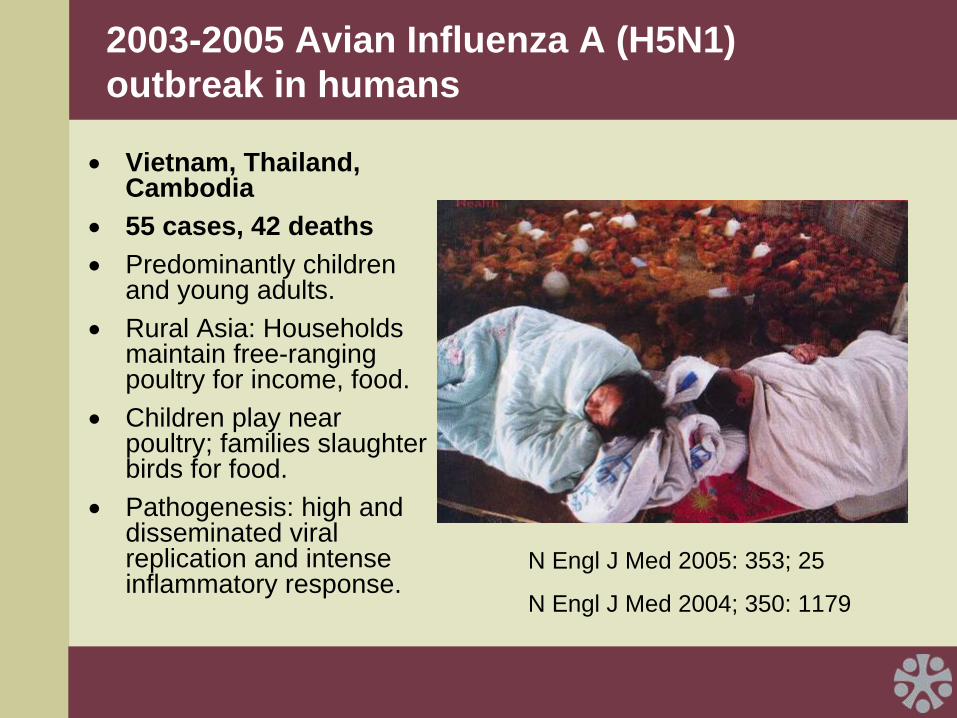
2003-2005 Avian Influenza A (H5N1) outbreak in humans
•
Vietnam, Thailand, Cambodia
•
55 cases, 42 deaths•
Predominantly children and young adults.
•
Rural Asia: Households maintain free-ranging poultry for income, food.
•
Children play near poultry; families slaughter birds for food.
•
Pathogenesis: high and disseminated viral replication and intense inflammatory response.
N Engl J Med 2005: 353; 25
N Engl J Med 2004; 350: 1179

H5N1: How did it spread?
•
1997-May 2005: largely confined to SE Asia.
•
Infected wild birds in Qinghai Lake, China; rapidly spread westward.
•
Death of swans and geese marked spread into Europe, India and Africa.
•
Ducks may be “stealth carriers.”•
Wild mallard ducks do not always show signs of disease when infected with highly pathogenic H5N1 viruses.
N Engl J Med 2006; 355: 2174
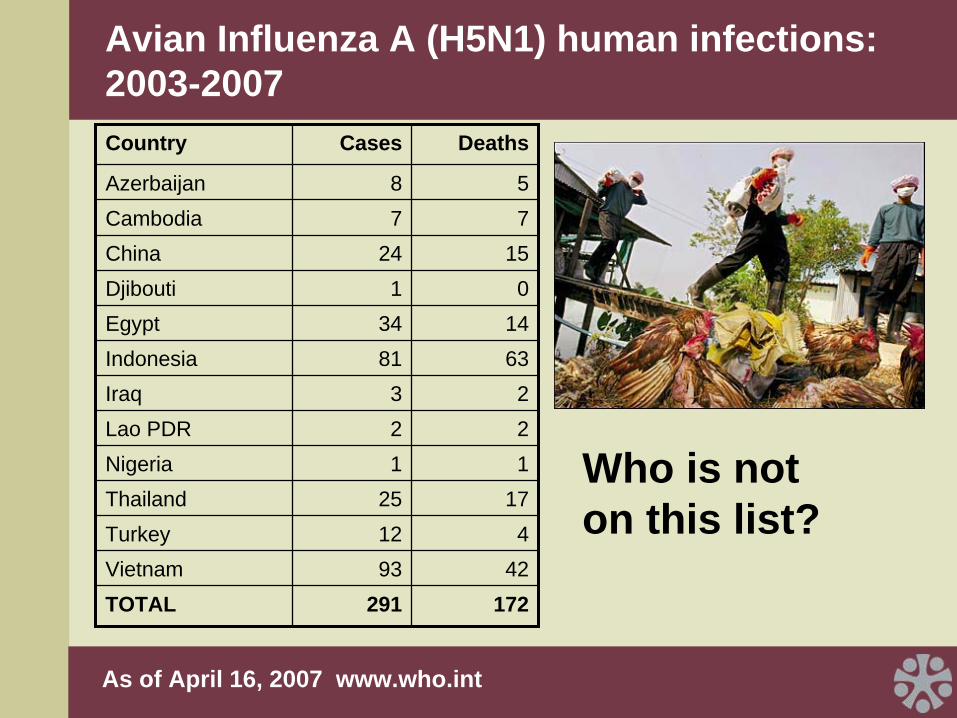
Avian Influenza A (H5N1) human infections: 2003-2007
Who is not on this list?
Country Cases Deaths
Azerbaijan 8 5Cambodia 7 7China 24 15Djibouti 1 0Egypt 34 14Indonesia 81 63Iraq 3 2Lao PDR 2 2Nigeria 1 1Thailand 25 17Turkey 12 4Vietnam 93 42TOTAL 291 172
As of April 16, 2007 www.who.int
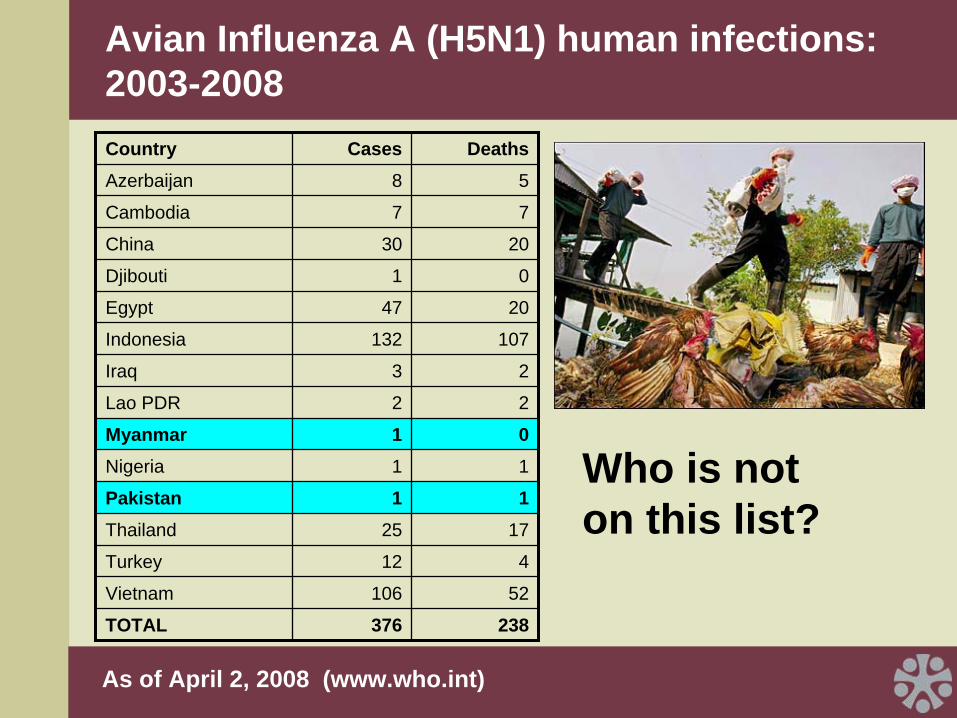
Avian Influenza A (H5N1) human infections: 2003-2008
Who is not on this list?
Country Cases DeathsAzerbaijan 8 5
Cambodia 7 7
China 30 20
Djibouti 1 0
Egypt 47 20
Indonesia 132 107
Iraq 3 2
Lao PDR 2 2
Myanmar 1 0Nigeria 1 1
Pakistan 1 1Thailand 25 17
Turkey 12 4
Vietnam 106 52
TOTAL 376 238
As of April 2, 2008 (www.who.int)
Why is H5N1 of particular concern?
•
Mutates rapidly, acquires genes from viruses infecting other species.
•
H5N1 clades and subclades differ in antigenic structure.
•
Direct transmission from birds to humans.
•
Causes severe disease in humans.
•
Acquisition of drug resistance on therapy.
•
Increasing numbers of human clusters.
•
Environmental resistance.
Risk ractors for Avian Influenza
•
Exposure to live poultry.•
Exposure to ill poultry and butchering of birds (NOT culling).
•
Direct contact with poultry (plucking, preparing diseased birds; handling fighting cocks; playing with poultry; consumption of duck’s blood; possibly undercooked poultry).
WHO. NEJM 2005; 353;13.

H5N1: Human-to-human transmission?
•
Infection after close contact with infected child leading to illness and death.
•
Evidence of antibodies to H5 in health care workers who cared for patients in Hong Kong in 1997.
•
Intensified surveillance (PCR) with contacts has led to detection of mild cases, more infections in older adults, and increased numbers of family clusters in Vietnam.
•
Family clusters in Indonesia.
NEJM 2005; 353;13.
NEJM 2006; 355: 2186.
Environment-to-human transmission?
•
Theoretical given survival of H5N1 in environment.
•
Oral ingestion of contaminated water during swimming?
•
Contamination of hands from infected fomites and subsequent self-inoculation?
•
Poultry feces used as fertilizer?
WHO. NEJM 2005; 353;13.
WHO: Pandemic alert
•
Influenza A virus with a novel HA or novel HA and NA — substantial proportion of the population has little or no antibody to the novel virus.
•
Novel virus demonstrates ability to cause disease in humans.
•
Novel virus demonstrates ability to spread easily among humans.
So…
•
H5N1 is a novel virus with ability to infect and cause disease in humans
•
Limited human to human transmission at present
•
Total number of cases small; case fatality rate high
•
Exposure and risk of future cases increasing with increasing spread of virus among birds
•
Is avian influenza worth the investment of resources, and if so, what can/should be done?

How do we determine the burden of illness during How do we determine the burden of illness during annual influenza epidemics?annual influenza epidemics?
“…probably the most under-rated major pathogen in the developed world…one of the major infectious causes of death from a single microorganism.”
John Bartlett Update in Infectious Diseases
Annals of Internal Medicine August 1999
Impact of Influenza, U.S.Impact of Influenza, U.S.
•
More than 20,000 excess deaths per typical epidemic
•
>90% of deaths in persons >65 years
•
110,000 or more excess hospitalizations ($600 million direct costs)
•
Severe epidemic costs $12 billion
So what should be done, pre-pandemic (now!)?
•
Improve surveillance worldwide.
– All types of influenza.– All types of respiratory
disease.– Easier, more reliable, less
expensive diagnostics.– Year-round surveillance.– Clinical research on human
cases/ populations.
Reduce opportunities for human infection
•
Education about human behaviors.
•
Control spread in birds/animals (collaboration between animal and public health sectors).
•
Improve approaches to environmental detection of virus.

General emergency preparedness
•
Clearly-defined plans, leadership structure.
•
Responsibility/accountability.
•
Communications.
•
Surge capacity — Mass delivery mechanisms for drugs/vaccines/health services.
•
Stockpiles of essential medical supplies.
•
Table-top exercises.

February 8, 2007

Preventing/minimizing morbidity and mortality
•
Pandemic vaccines – Supplies, equitable access, developing country manufacturers, novel ways to use less antigen (make limited supply go further).
•
Antivirals – International stockpiles, supplies, equitable access, developing country manufacturers, international clinical trials networks.
•
Community mitigation strategies – Quarantines/border or school closures.

Flu vaccine supply: Inadequate, inequitable
>95% of world flu vaccine comes from 9 countries4 European companies produce 65% of world supply
Fedson DS. Vaccine Development for an Imminent Pandemic. Human Vaccines 2006: 2(1)38-42.Dennis C. Flu-vaccine makers toil to boost supply. Nature 440:1099. Apr 2006.
Influenza vaccines landscape analysis: Key findings
•
The global need for a pandemic vaccine is an estimated 7 billion courses.
•
Planning for the availability of a pandemic vaccine should envision at most a six-month time horizon, and likely shorter.
•
Should an outbreak of pandemic influenza occur today, the “best case” scenario within this timeframe is that 1.2 billion courses of pandemic vaccine could be produced from current capacity within six months.
•
In the short term, new adjuvants could facilitate “dose sparing” but in the long term, new innovative technologies that could increase global supply are needed.
•
Proposal approved to advance promising new pandemic flu vaccines into development.
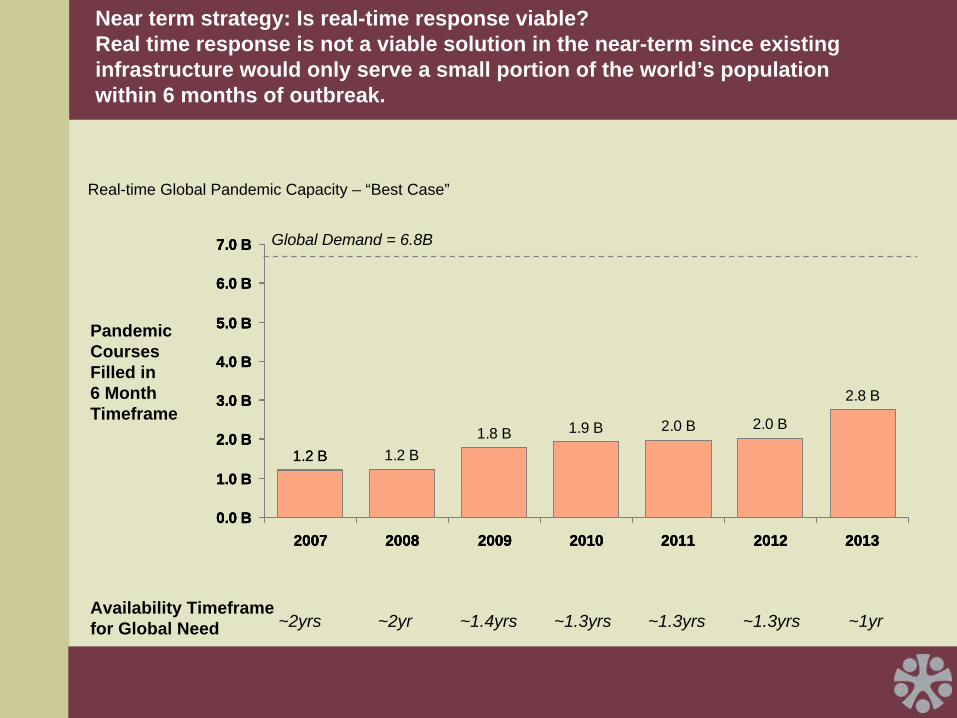
Near term strategy: Is real-time response viable? Real time response is not a viable solution in the near-term since existing infrastructure would only serve a small portion of the world’s population within 6 months of outbreak.
0.0 B
1.0 B
2.0 B
3.0 B
4.0 B
5.0 B
6.0 B
7.0 B
2007 2008 2009 2010 2011 2012 2013
Real-time Global Pandemic Capacity – “Best Case”
1.2 B
0.0 B
1.0 B
2.0 B
3.0 B
4.0 B
5.0 B
6.0 B
7.0 B
2007 2008 2009 2010 2011 2012 2013
1.2 B 1.2 B1.8 B 1.9 B 2.0 B 2.0 B
2.8 B
0.0 B
1.0 B
2.0 B
3.0 B
4.0 B
5.0 B
6.0 B
7.0 B
2007 2008 2009 2010 2011 2012 2013
Global Demand = 6.8B
Availability Timeframe for Global Need
Pandemic Courses Filled in 6 Month Timeframe
~2yrs ~1.4yrs ~1.3yrs ~1.3yrs ~1.3yrs ~1yr~2yr
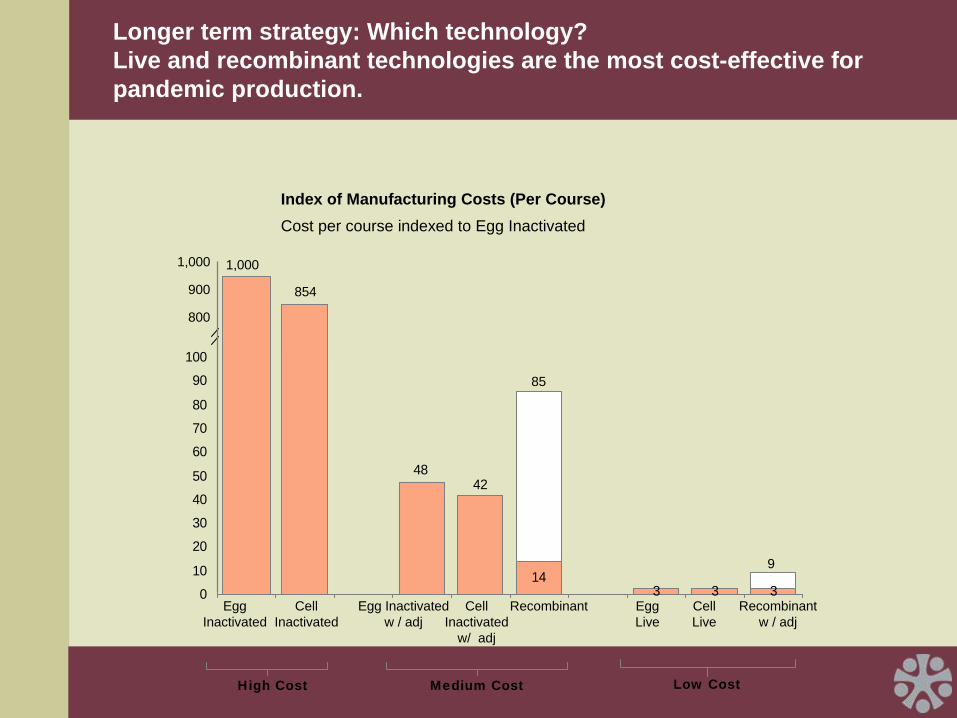
Longer term strategy: Which technology? Live and recombinant technologies are the most cost-effective for pandemic production.
Index of Manufacturing Costs (Per Course)Cost per course indexed to Egg Inactivated
143 3 3
4248
0
10
20
30
40
50
60
70
80
90
100
1,000
854
1,000
900
800
85
9
Egg Inactivated
Cell Inactivated
Egg Inactivated w / adj
Cell Inactivated
w/ adj
Recombinant Egg Live
Cell Live
High Cost Medium Cost Low Cost
Recombinant w / adj
Summary
•
H5N1 is highly pathogenic and has crossed the species barrier to cause many human fatalities and pose an increasing pandemic threat.
•
Yearly influenza epidemics are associated with substantial morbidity and mortality; impact in developing countries uncertain, but likely substantial.
•
Investment in pandemic preparedness can yield more immediate health gains.