patients' needs, medicines innovation and the global public's interests
DESCRIPTION
New pharmaceutical and other treatments combined with the world-wide development of universally accessible health care systems could effectively eliminate infectious and noncommunicable disease-related deaths in people aged under 70 by the middle of this century, according to a new report from the London School of Economics and Political Science and the UCL School of Pharmacy, published today. Patients’ Needs, Medicines Innovation and the Global Public’s Interests shows that global life expectancy at birth increased by 30 years over the course of the last century, from 40 years to 70 years. Half of this progress has been due to health care technologies such as innovative vaccines and medicines.TRANSCRIPT
Patients’ Needs, Medicines Innovation and the Global Public’s InterestsAchieving affordable universal care, enhanced public health
and sustained investment in better treatments
Summary
• In1900world-wideaveragelifeexpectancyatbirthwasnomorethan40years.Todayitisabout70yearsformenandwomencombined.Advancesinmedicine,surgeryandmedicines(rangingfromantibioticsandanti-viralsthroughtovaccinesagainstdiseaseslikepneumonia,hepatitisandHPVanddrugsthatreducestrokeandheartdiseaserisks)haveaccountedforabouthalftheimprovementsinhealthachievedsince1950.
• Aslifeexpectancyrisesandbirthratesfallpeople’svaluesalter,andsocietiesgothroughprofoundchanges. Providing universal access to health care typically becomes an increased priority, whilerelationshipsbetweenhealthcareprofessionalsandhealthserviceusersbecomelessdirectiveandmorequestioning.Theinfluenceofpatientsandpatientorganisationsonhealthpoliciesandpracticestendstoincrease.Theydevelopenhancedrolesinareassuchasresearchandclinicaltrialgovernanceandhealthtechnologyassessment.
• Thereare importantopportunitiesforpharmaceuticalandother innovationstocontributefurthertoimprovingtheglobalpublic’shealthinareasrangingfromthediagnosis,preventionandtreatmentoftropicalinfectionsthroughtothemanagementofthecommonnon-communicableconditions.Therealsoareover6,000rarediseasesthatcollectivelyaffect100millionpeopleinthe‘developed’OECDnationsandupto500millionworld-wide.Manyarecurrentlydifficulttodiagnoseandlackdefinitivetreatments.
• By2050furtherprogresstowardsuniversalhealthcarecoverageanddelivery,combinedwithongoinghealth technology innovation, could virtually eliminatedisease relatedchild andworkingageadultdeaths. Itshouldalsosupportactiveageinginwaysthatcannotbeachievedbylifestylechangesalone. Realising such gainswill depend on the political will needed to provide better health carecombinedwith continuing public andprivate investment in high risk research in spheres such asmedicinesdevelopment.
• Patientsandpatientorganisationshaveimportantinterestsinbothfundinginnovationandassuringaccesstoeffectivetreatmentsaftertheyhavebeendeveloped.FollowingconcernsaboutthecostofandaccesstonewHIVmedicinesinthe1990s,somecommentatorsquestionthevalueofintellectualproperty rights (IPRs) suchaspharmaceuticalpatentsbecause they increase thepricesof recenttherapeutic developments. But without intellectual property rights private investment in high riskbiomedicalresearchwouldbeveryunlikelytotakeplace.Thiswouldalmostcertainlyhavenegative‘knockon’effectsonpublicfundingforfundamentalresearch.
An issue guide for medicine users and patient representatives
c
2 Patients’Needs,MedicinesInnovationandtheGlobalPublic’sInterests
• ThereislittlerealisticpossibilitythatalternativessuchasofferingStateorprivatedonorbackedprizesfordevelopingtherapeutic innovationscouldeverfullysubstituteforpatentsandregulatorydataexclusivitybasedapproachestomaintainingprivate investment inbiopharmaceutical innovation.ButinitiativesliketherecentlyproposedHealthImpactFund,AdvancedMarketCommitmentsandtheexamplessetbyorganisationssuchastheGatesFoundationmayusefullyaugmentIPRbasedprovisions.
• Ifaccesstonew‘essential’medicinesistobeenhancedinwaysthatdonotundermineinnovativecapacity,welldesignednationalandinternationalpurchasingarrangementsbackedbydifferentialpricingstrategiesarelikelytoplaykeyroles.Thereisacasefortheglobalextensionoftheperiodsofintellectualpropertyprotectionavailabletohealthtechnologyinnovators,balancedbyincreasedminimalcostsupplyobligationsinpoorcommunities.
• Differential pricing between and withinmarkets should allow innovators to enhance access toIP protected products without losing income and so reducing investment capacity. However,inappropriatemovementsofmedicinesbetweenmarketsandresentments inhigherpriceareascanmakesuchschemesdifficulttoimplement.Internationalagreementsabouttheprinciplesandcriteria onwhich differential pricing and allied approaches (including voluntary IPR and licencesharing)mightinfutureenhancetheirviability.
• Patientorganisationsshouldseektoclarifythedefinitionsofessentialmedicinesandpublichealthemergencies.Thiscouldhelpprotectworld-widepublicinterestsandpreventtheinappropriateuseofpowerslikecompulsorymedicineslicensing.
• Thereareuncertaintiesastohowrobustintellectualpropertyrightsshouldbeinordertosustainongoinginvestmentsinhighriskresearch.Individualsandorganisationsseekingtodefendpatientandpublicinterestsinmaintainingtheconditionsneededforcontinuinginnovationmaybeexposedtochargesthattheyaredefendingcommercialratherthanhealthinterests.Yetunder-investinginresearchforthefuturewouldharmtheinterestsofbothpatientsandtheglobalpublic.Liveslostandyearsofdisabilitycausedbecauseinnovationshavebeendelayedcanneverberegained.
• Measuresdevelopedbyhealtheconomiststoguideshorttermhealthresourceallocationdecisionsunder-estimate the long term society-wide value derived frommedicinal and allied innovations.Becauseoftheeconomicsoftheirdevelopmentandsupplynewmedicinestypicallybecome–aftertheexpiryofIPrights–lowcostresourcesforlongperiodsoftime.Thisisapowerfulreasonforcontinuingtoinvestininnovativeresearchinordertoimproveestablishedtreatmentsandcreatefundamentally new opportunities for the relief of suffering, the elimination of diseases and theenhancementoflife.
This report was researched and written by Mari Lundeby-Grepstad, David Tordrup of LSE and Tina Craig and David Taylor of UCL School of Pharmacy
The LSE research undertaken was funded by the International Alliance of Patients’ Organizations
Professor Taylor is accountable for the content of this document and for any errors it contains

Patients’Needs,MedicinesInnovationandtheGlobalPublic’sInterests 3
Innovations can encompass entirely new inventions
or involve new ways of using an existing technology
in a more productive and/or more cost effective man-
ner than was previously possible. In health care valu-
able innovations can relate to anything from fresh ap-
proaches to the use of professional time through to the
introduction of new surgical techniques or original com-
munication methods. Advances in social care and psy-
chological support can also enhance health outcomes.
However, this report is primarily concerned with un-
derstanding patient interests in medicines and relat-
ed forms of biomedical innovation, and the extent to
which intellectual property rights such as those con-
ferred by patents or via regulatory data protection
serve to improve public health now and in the future.

4 Patients’Needs,MedicinesInnovationandtheGlobalPublic’sInterests
Introduction
Because of scientific, industrial and agriculturalinnovation,thetwentiethcenturysawmajorworld-wideimprovementsinhumanhealthandlifeexpectancy.Forinstance,in1900inWesternEurope–thethenrichestpartoftheworld–lifeexpectancyatbirthwasnotyet50years.Butbytheendofthe1940s,beforetheantibioticrevolution had made its full impact and despite theimpactsofWorldWarII,ithadrisento60years.Thiswasdueinlargeparttodeclinesinchildandinfantmortalityassociatedwithenhancednutritionandimprovedlivingconditions.
Today average life expectancy is between 70 and 80years in countries ranging from the US and China toGermany,Turkey,ThailandandBrazil.Sincethe1980smuch the additional health gain achieved in moreaffluent societies has occurred amongst older people.As infectious diseases have become better controlledthecentralhealthchallenges facingmatureeconomieshaveshiftedawayfromreducinginfant,childandyoungadult mortality towards preventing and treating laterlife conditions. However, it is important to record thatas communities become richer and theirmembers onaverageoldertheratesofmortalityandseveredisabilitycausedby non-communicable conditions like vasculardiseasesoften fall in age specific terms (WHO,2012).Interventionswhichprotectpeoplefrominfectionsearlyin their lives and from events like heart attacks andstrokes inmid-lifealsopromotebetterhealthamongstpeopleintheir60s,70sand80s.
Fundamental advances have also been made in thepoorer parts of Asia andAfrica. In India, for example,average life expectancy at birth was in 1950 still lessthan 40 years. It is now over 65 years for men andwomen combined. Throughout the modern worldfactors such as tobacco smoking, hypertension andproblems associated with excessive food intake havelargelyreplacedalackofcleanwaterandunder-nutritionas themaincausesofavoidable illhealth.AsFigure1illustrates,eveninthosesub-SaharanAfricancountriesthat–likeSouthAfricaandNigeria–havebeenseverelyaffected by HIV and are still challenged by problemslike TB, malaria and childhood diarrhoea, average lifeexpectancyatbirthisnowaboutadecadelongerthanitwasinWesternEuropein1900.
Such successes deserve celebration by patients andthepublicworld-wide.Sustainablehealth improvementisnowcriticallydependentonmaintaining thematerialandsocialenvironmentsneededtoprotectphysicalandmental health andwellbeing.Reducingpollution levelsand avoiding catastrophic climate change, while alsofurtherincreasingenergyandfoodproduction,aretodayamongst the most critical global public health tasks.Butawarenessof thisshouldnotdrawattentionawayfromthat fact thatnewmedicinesandvaccines,alongwith developments in areas ranging from surgery tonursing,havebeenresponsibleforabouthalftheglobalhealth progress achieved since the end ofWorldWarII. If therapeutic innovation continues, pharmaceutical
products will contribute even more to health andwellbeingasthetwentyfirstcenturyunfolds.
AgainstthisbackgroundthisUCLSchoolofPharmacyreport, which was originally commissioned by theInternational Alliance of Patients’ Organizations(IAPO),1 explores questions relating to the benefits forindividuals and communities that further investmentin biopharmaceutical and related forms of innovationby research based companies, Universities and otherpublic and private institutions will generate in comingdecades.Itexaminesfactorsrelatingtopublicinterestsin the financingof ongoing innovation2 and the roleofintellectualpropertyrights(IPRs–seeBox1)infacilitatingthe the funding of research on better treatments forconditionsthatasyetcannotbesatisfactorilyprevented,alleviatedorcured.Theseinclude,forexample,infectionslike Dengue fever and Chagas Disease (Americantrypanosomiasis) and NCDs such as cancers, themusculoskeletal disorders and neurological conditionslikeAlzheimer’sdiseaseandmultiplesclerosis.
The advocates of intellectual property provisions suchaspatents and the temporarymonopolies they awardsee themas an essential element in the infrastructurethat underpins the global financing of medical andpharmaceutical research. By contrast, critics say thattheyinhibitcompetitionandfreetradeanddenypoorerpeople lowcostaccesstomedicinesandothergoodsthattheyneed.Itwas,forexample,recentlysuggestedby
1 TheIAPObriefwastodevelopapapertoequippatientadvocateswithanunderstandingoftheinformation,issues,challengesandopportunitiesappertainingtoinnovation.
2 Overthenextfewdecadesgeneticandotherbiomedicalresearchundertakeninareassuchascancerwillopenthewaytoarangeofinnovativetechnologiesrelevanttoareasrangingfromfoodandenergyproductionthroughtopollutioncontrol.Thiswillamplifythefuturepublichealthandwelfarebenefitsderivedfrompharmaceuticalresearch.
Figure 1: Life expectancy (LE) and healthy life expectancy (HLE), men, selected countries, 2010.
Source:Salomanetal,2012.
Years 0 10 20 30 40 50 60 70 80
Brazil
China
Germany
India
Japan
Russia
Sth.Africa
Sweden
Zimbabwe
USA
70.5
72.9
77.5
63.2
79.3
63.1
57.4
79.2
51.1
75.9
61.1
65.5
68.1
54.9
70.6
55.4
49.1
68.0
43.3
66.2
LEHLE

Patients’Needs,MedicinesInnovationandtheGlobalPublic’sInterests 5
agroupofUSbasedeconomiststhatthepatentsystem‘arose as a way to limit the power of [medieval] royalty to award [unlimited and arbitrary] monopolies to favoured individuals; but now its primary effect is to encourage large but stagnant incumbent firms to block innovation’ (BoldrinandLevine,2013).Atworst,itcouldbeargued,intellectual property laws have served to protect theabilityofAmericansandEuropeanstocontinueenjoyingwealthierandhealthierlifestylesthantheircounterpartsintheex-coloniesoftheworld.
Thereisno‘scientific’wayofjudgingwhich(ifeither)ofthesetwopolarisedsetsofviewsisobjectivelycorrect,ineithereconomicorethicalterms.Thereareveryprobablyelementsoftruthinboth.Thejudgementofferedhereisthatwithoutbothphysicalandintellectualpropertyrightswelfare promoting co-operation between people withconflictinginterestsisfrequentlyifnotalwaysimpossible.But any right can be abused if it is not tempered byhumanitarian values and counter-balancing duties andrequirements.
In the case of pharmaceuticals these range from theobligations placed on thosemarketing newmedicinesto publish information about their innovations and to
complywithsafetytestingrequirements,throughtotheirresponsibilitiestocontributeviataxationtothesupportofhealthcaresystems.Universalhealthcoverage(UHC)systemsinvolvingbothpublicandprivateproviderscan,when appropriately funded, organised and regulated,share risks and costs and assure access to healthservicesandproductsviaefficientpurchasingsystemsandcaredeliverystructures.
The existence inmany countries of drug price and/orprofit controls limits the valueof IP rights. It is arguedherethatpatentsandalliedprovisionssuchas‘regulatorydata exclusivity’ (see again Box 1) will throughout theforeseeablefuturecontinuetohaveanimportantroletoplayinthefinancingofpharmaceuticalandotherformsof innovation. Yet this conclusion should not obscurethe need to recognise and strengthen national andinternationalcommitmentstosecuringindividuals’rightstolifeandtomedicinesasandwhentheyareneededforsurvivalorforthereliefofmajorsuffering.
Cancercareisanexampleofanareawhereinfuturetherecould bemedicines affordability problems comparablewiththosethatinthepastaffectedHIVmedicinessupply(IMS,2013).Atpresentmanysophisticatedanticancer
Box 1. Types of innovation and intellectual property protection
An innovationmay be an entirely new invention or anewway of using an existing technology. It can alsoinvolve improving existing technologies or combiningtwoormoredifferenttechnologiesinfreshlyproductiveways. Health technologies include drug treatments,medicaldevices,diagnostictests,clinicalinterventions(ranging from psychotherapeuticmethods to surgicaloperations) and preventive techniques. Innovationsencompass anything from the introduction of newwaysofcounteringancientproblemsliketuberculosisorcancertooffsettinganticipatedchallenges, liketheemergenceofnewtypesofdrugresistantbacteriaandviruses.Theycanalsoallowestablishedproductsandservicestobemadeordeliveredinlesscostlyways.
The forms of intellectual property protection (IPP) orright (IPR) available range from trademarks such asbrandnamesandlogos(thatclassicallyservetomarkoutproductscomingfromtrustedmakers)throughtoregistered or unregistered designs, copyrightsandpatentsofvarious types.Forexample,apatentcanbe for amanufacturingprocess or for a finishedproduct. In some countries, including the US, trade secretscanalsobelegallyprotected.
Copyrightsandalliedprovisionsprotecttheexpressionofideasandconcepts,whereaspatentspermitlimitedperiods of exclusive exploitation of innovative ideasand concepts themselves. In highly regulated areassuch as the pharmaceutical sector regulatory data protection (RDP – also known as regulatory dataexclusivity) may play an additional role in sustaininginvestment. This for limited periods stops applicantswhowant tomarket ‘followon’ versions of products
thatarealreadybeingsuppliedbytheoriginalinnovatorfromusingtheresearchfindingssubmittedbythelattertoobtainanewmarketingauthorisation.RDPdoesnot,however,preventanyonefromprovidingoriginalclinicaltrialdatainsupportofamarketingapplication.
Intellectual property right durations vary betweenjurisdictionsandbythetypeofIPinvolved.Trademarks,for instance, normally endure indefinitely, and anauthor,artistormusiciancancurrentlyenjoycopyrightprotectionthroughouthisorherlifetimeplus(insettingssuch as the US and the EU) another 75 years. Bycontrast,designrightsarenormallygranted for justafewyears,whilepatentprotectiontermsformedicinesinmuchoftheworldnowrunfor20years.Abouthalfofthistimehastypicallyexpiredbeforepharmaceuticalproductsareclearedformarketentry.
Thereisno‘objective’wayofdeterminingfromapublicinterest perspective precisely how long a patent oranyotherIPtermshouldlast,orhowmuchasocietyought to invest in innovative research. It is importanttostress that IPRsexistalongsideother factorssuchas medicines price control schemes, health servicepurchasing policies and taxation systems that canalso encourage or discourage research investment.Inpracticepolicymakersmustpragmaticallybalancethese variables in the pursuit of their immediate andlongtermhealthandothersocio-economicgoals.Itissuggestedherethatcommunitiesoftendevotetoolittleoftheirresourcestoimprovingthefuture,asopposedtoconsuminginthepresent.Butthisvaluejudgementcannotbe‘proved’or‘disproved’byeconomicoranyotherformof‘scientific’analysis.
6 Patients’Needs,MedicinesInnovationandtheGlobalPublic’sInterests
medicines are palliative rather than curative, and aredifficult to use to optimum effect in the absence ofadvanced diagnostic and treatment facilities. There isthereforeacaseforarguingthatintheimmediatefutureresourcesshouldbemosturgentlyfocusedonpreventiveprogrammes such as HPV vaccination and tobaccousecessationcoupledwith the improvedalleviationofcancerrelatedpaininlessaffluentpopulations.
Butascurativetreatmentscontinuetoimproveitwouldbe for many people unacceptable if poor patientswere routinelydenied life saving treatmentscommonlyavailable in affluent communities. To avoid undesirableinterventions like the use of compulsory licensing inways that would undermine investment in continuinginnovationitwillbeintheglobalpublic’sinteresttofindequitablewaysofensuringuniversalaffordableaccessto essential anti-cancer medicines without sacrificinginnovators’ intellectual property rights. Viable waysforward are likely to involve combining systematicapproaches to differential pricing with the furtherdevelopmentofnationalhealthcaresystemsandwhererequired international treatment purchasing supportmechanisms.
Patient led care and innovation
Thisanalysisreviewssomeofthekeystepsinmedicinesinnovationachievedtodate,andhighlightspatientandpublic needs for further therapeutic improvements. Italsoconsidersmedicinesashigh technologyproductswhicharecostlyandriskytodevelop,butoncemarketedareoftenrelatively inexpensivetocopy.Thisunderlyingrealityexplainsmanyof thecontroversiesandconflictspresently linked to pharmaceutical pricing, supply andaccess.
Thisreportthengoesontooutlinetheoriginsofintellectualpropertyprovisionssuchaspatents,andtoexplorewhyresearchbasedpharmaceuticalproducersareunusuallyreliantonthetemporaryshieldingfromunregulatedfreemarketforcesthatintellectualpropertyrightsprovide.Itbriefly examines the reasons why patient involvementand leadership has become increasing important inhealth sector decisionmaking andaddresses a seriesofquestions relating to innovationand IPprovisionsofpotential interest to patients and their representatives.TheyincludethedegreetowhichthecurrentIPRsystemadequatelyincentivisesresearchintoorphanconditions(see, for instance, WHO, 2006; IFPMA, 2012) andwhether or not theWorld Trade Organisation’s TRIPS(Trade-Related Aspects of Intellectual Property Rights)agreement threatens, as some fear, to deprive peoplelivinginlessdevelopedcountriesofsuppliesoflowcostgenericmedicines.
This study concludes by offering suggestions for thefuture. It signposts theneed rationally tobalance,andwherepossiblepositively combine, thebenefitsof lowcostaccesstonewtherapeuticinnovationsagainstthelongtermvaluetohumanityofinvestinginresearchanddevelopment. In the short term there is little purposein producing newmedicines if thosemost in need ofthem cannot access either them or the professional
support required to use them to good effect. Yet tomaintain investment levels providing innovations mustbe profitable. There is also reason to argue that bothindividualsandnationsoftenunder-invest inthefuture,whileonoccasions(aswithestablishedantibiotics)over-consuminginthepresent.
Allsupply limitingorcost increasingpolicies riskbeingunpopularwithelectorates,howevergreattheirultimatebenefits. In the final analysis intellectual property lawsrepresent a logically coherent, market led rather thancentrally directed, mechanism for ‘taxing’ the use ofrecent innovations in order to defend public interestsin incentivising continuing investment in areas likemedicinesdiscovery.Thisservestheinterestsofpeoplewith presently untreatable conditions, and underpinsthefundingofincrementaland‘stepchange’innovationalike.InsocietiesthatlackrobustwelfaresystemsIPRsareoftenblamedforrestrictingimmediateminimalcostaccesstonewlyavailabletreatments.Yetthisshouldnotobscuretheiroverallvaluetotheglobalcommunity.
The core challenge for patients andothers seeking todefend the public’s best interests in both affordablemedicines access and ongoing innovation is tounderstandthepresentsituationinthecontextof localand world-wide health needs, and help societies tomoveforwardwithabalancedapproachtocurrentcaredelivery and ongoing medicines discovery. As alreadysuggested,therearenoabsolutely‘correct’answerstomanyofthequestionsthischallengeraises,justastherecan be no certainty about the outcomes of high riskresearchprojects.Butpatientsandthewiderpubliccanexpectdecisionmakerstoconsidersuchcomplexissueswith an open mind, and to debate ways of resolvinglegitimateconflictsofinterestwithtransparency,honestyandwellbalancedjudgement.
Why Innovate?
For all but a small fraction of the 200-250 thousandyearsthatHomosapiens(‘wise[wo]man’)hasexisted,peoplelivedinsmallandisolatednomadicfamilygroups.There is reason to believe that they often possessedconsiderable‘handeddown’ localknowledgeofplantsandmineralsusedaspoisonsandmedicines.Buttherewas no reliable way beyond word of mouth for suchexpertisetoaccumulateandbesharedonalargescale.Uniqueunderstandingsmustoftenhavebeenlostwiththe passing of key individuals and/or particular tribalcultures.
However,withtheadventinthelast10,000orsoyearsofsettledagriculturalcommunitiesandinnovationsinfieldssuchaswritingandmathematics,peoples’capacitiestochangetheir livesandtheirenvironmentsbeganslowlybut exponentially to increase. The establishment oflargerandmore inter-connectedsocialgroupsopenedthewaytotheevolutionofuniquelyhumaninfectionslikesmallpox,polioandmeasles.Yetitintimealsoledtothedemographicandepidemiologicaltransitionsofthepasttwocenturies.
7
6
5
4
3
2
1
0
Hum
an p
opul
atio
n (b
illio
ns)
Patients’Needs,MedicinesInnovationandtheGlobalPublic’sInterests 7
Withtheemergenceoftownsandwidersocialsystemsthat extended beyond family and clan structures,opportunitiesalsoarosetodevelopmoresophisticatedapproachestomedicineandmedicines.Inparallelwiththeearlydevelopmentofmonotheisticreligionsthatservedto unify and promote co-operative behaviours acrossmostworldregions,severalseminalpharmacopeiasandmedicaltextsdatebackabout2,500years.IntheIndiancontext these include theCharakaSamhitaand in thecaseofChinatheHuangdiNejing,or‘YellowEmperor’sInnerCanon’. InEuropetheGreekHippocraticCorpusdatesfromthesametime.
ThislastwasfollowedshortlyafterthestartoftheChristianera by Galen’s innovative contributions tomedicine inthe Roman Empire. The subsequent establishment ofIslamicmedicineandpharmacyplayedanimportantrolein,for instance,furtherdisseminatingknowledgeaboutthe role of opiates in pain control across Europe andAsia, albeit that opium poppies were being cultivatedoverfivemillenniaagobySumerianslivinginpartofwhatisnowmodernIraq.3
Itwouldbebeyondthescopeofthisanalysistoattemptto describe the history of medicines development indepth.Butitisimportanttonotethat:
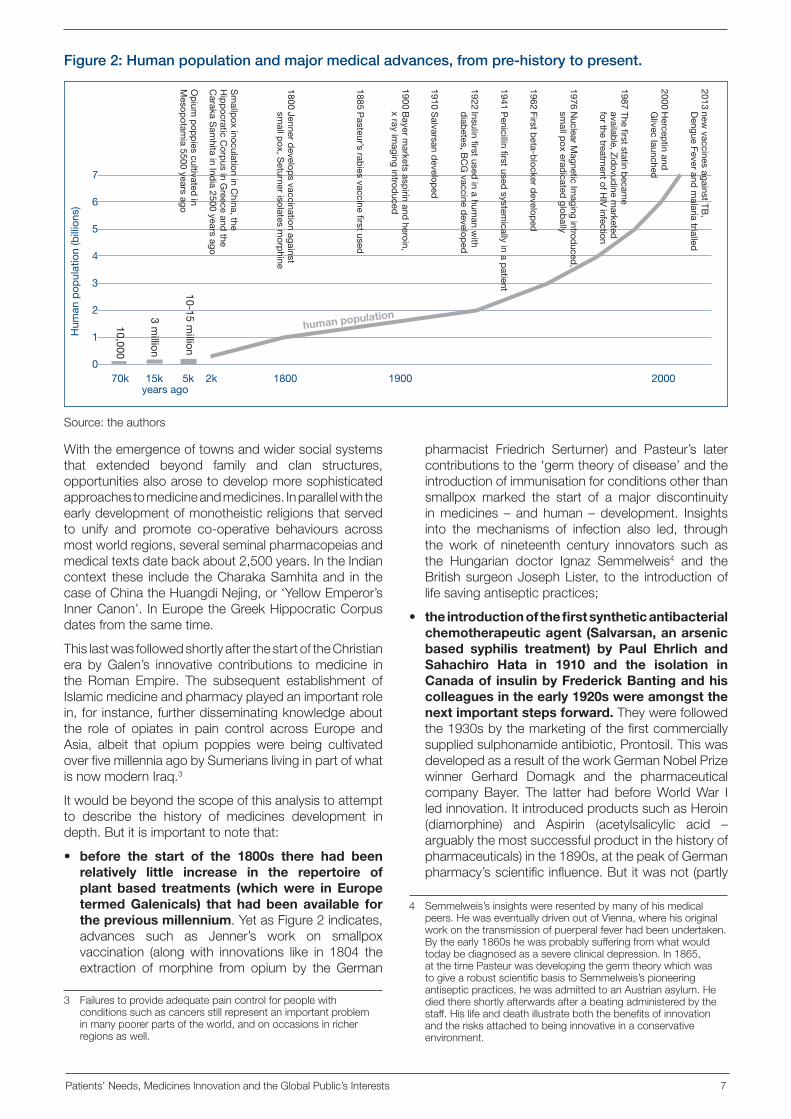
• before the start of the 1800s there had been relatively little increase in the repertoire of plant based treatments (which were in Europe termed Galenicals) that had been available for the previous millennium.YetasFigure2indicates,advances such as Jenner’s work on smallpoxvaccination (alongwith innovations like in 1804 theextraction of morphine from opium by the German
pharmacist Friedrich Serturner) and Pasteur’s latercontributionstothe‘germtheoryofdisease’andtheintroductionofimmunisationforconditionsotherthansmallpox marked the start of a major discontinuityinmedicines – and human – development. Insightsinto the mechanisms of infection also led, throughthe work of nineteenth century innovators such asthe Hungarian doctor Ignaz Semmelweis4 and theBritishsurgeonJosephLister, to the introductionoflifesavingantisepticpractices;
• the introduction of the first synthetic antibacterial chemotherapeutic agent (Salvarsan, an arsenic based syphilis treatment) by Paul Ehrlich and Sahachiro Hata in 1910 and the isolation in Canada of insulin by Frederick Banting and his colleagues in the early 1920s were amongst the next important steps forward.Theywerefollowedthe1930sbythemarketingofthefirstcommerciallysuppliedsulphonamideantibiotic,Prontosil.ThiswasdevelopedasaresultoftheworkGermanNobelPrizewinner Gerhard Domagk and the pharmaceuticalcompany Bayer. The latter had beforeWorldWar Iledinnovation.ItintroducedproductssuchasHeroin(diamorphine) and Aspirin (acetylsalicylic acid –arguablythemostsuccessfulproductinthehistoryofpharmaceuticals)inthe1890s,atthepeakofGermanpharmacy’sscientificinfluence.Butitwasnot(partly
3 Failurestoprovideadequatepaincontrolforpeoplewithconditionssuchascancersstillrepresentanimportantprobleminmanypoorerpartsoftheworld,andonoccasionsinricherregionsaswell.
Figure 2: Human population and major medical advances, from pre-history to present.
Source:theauthors
70k 15k 5k 2k 1800 1900 2000
10,000
3 million
10-15 million
2013 new vaccines against TB
, D
engue Fever and m
alaria trialled
2000 Hercep
tin and
Glivec launched
1987 The first statin became
available, Zidovudine m
arketed
for the treatment of H
IV infection
1976 Nuclear M
agnetic Imaging introduced,
small p
ox eradicated
globally
1962 First beta-b
locker develop
ed
1941 Penicillin first used
systemically in a p
atient
1922 Insulin first used in a hum
an with
diab
etes, BC
G vaccine d
eveloped
1910 Salvarsan d
eveloped
Op
ium p
opp
ies cultivated in
Mesop
otamia 5500 years ago
Sm
allpox inoculation in C
hina, the H
ipp
ocratic Corp
us in Greece and
the C
araka Sam
hita in India 2500 years ago
1800 Jenner develop
s vaccination against sm
all pox, S
eturner isolates morp
hine
1885 Pasteur’s rab
ies vaccine first used
1900 Bayer m
arkets aspirin and
heroin, x ray im
aging introduced
years ago
human population
4 Semmelweis’sinsightswereresentedbymanyofhismedicalpeers.HewaseventuallydrivenoutofVienna,wherehisoriginalworkonthetransmissionofpuerperalfeverhadbeenundertaken.Bytheearly1860shewasprobablysufferingfromwhatwouldtodaybediagnosedasasevereclinicaldepression.In1865,atthetimePasteurwasdevelopingthegermtheorywhichwastogivearobustscientificbasistoSemmelweis’spioneeringantisepticpractices,hewasadmittedtoanAustrianasylum.Hediedthereshortlyafterwardsafterabeatingadministeredbythestaff.Hislifeanddeathillustrateboththebenefitsofinnovationandtherisksattachedtobeinginnovativeinaconservativeenvironment.
8 Patients’Needs,MedicinesInnovationandtheGlobalPublic’sInterests
becauseof responses to theneed toprotectAlliedtroops) until during and afterWorldWar II that theantibiotic and wider pharmaceutical revolutionsgained rapid momentum. In the following decadesa tide of new small molecule based medicines forcommon conditions ranging from hypertension toasthma, diabetes andpeptic ulcer disease reachedglobalmarkets;and
• at the end of the twentieth century innovations such as Herceptin (trastuzumab, which until resistance develops is effective in about a fifth of breast cancers) and Glivec (imatinib mesylate, used initially in the treatment of chronic myeloid leukaemia) supplied by the Swiss companies Roche and Novartis marked the beginning of another phase of (bio)pharmaceutical development.Thisislikelytoinvolvetheintroductionof an increasing number of what may appear inclinical terms to be relatively modest advances forrare, low volume, indications.But the accumulationof knowledge accompanying such gains oughteventuallytopermitstepchangesintheeffectivenessofawiderangeoftreatments.
The basic answer to the question ‘why continue to innovate?’ is that if the health of people across theworld is to go on improving then new technologieswill be required to continue the fight against the untilrecently neglected tropical diseases (NTDs, of whichtherearearound20)andother infections,andcontaintheemergenceofresistanceinareasthatarepresentlywellcontrolled.Theyarealsoneededtopreventorlimittheprogressionofnon-communicable(althoughsociallymediated)diseases(NCDs)andpromotehealthy/active
ageinginwaysthatarenotcurrentlypossible.Lifestylechangesalonewillnotbeabletodelivergoalssuchasincreasing average healthy life expectancy at birth toover70years,howeverprotectivephysicalenvironmentsandlifestylesbecome.
AsdiscussedfurtherinBox2,manycommonconditionscannot as yet be prevented, cured or satisfactorilyameliorated. Even in areas such as pain control andthe treatmentof raisedbloodpressure–which recentstudiesontheglobalburdenofdiseaseindicateremainsthelargestsinglecauseofdisabilityandprematuredeathworld-wide–bettermedicinesare required toaddressthefundamentalmechanismsof ill-health(Murrayetal,2012:Coffman,2011).
Inadditiontoothercommonlyoccurringconditionsliketype2diabetes,thesolidcancersandthemajormentalillnesses, therearesome6-7 thousand ‘rare’diseasesthat in aggregate directly affect 100 million people inthe economically developed nations alone. Much ofthepoorerworldasyet lacksthediagnosticresourcesneeded to reveal the true global prevalence of suchdisorders.
Mostrare(alongwithmanycommon)conditionscannotas yet be prevented, and lack definitive treatments.Further,evenwhencommunicableornon-communicabledisease are in theory preventable ormanageablewithpresent medicines and vaccines, existing methods ofsupplyingandusing themoften fail toachieveoptimalhealthoutcomes.Innovativeclinicalpracticesandfreshapproaches to ‘public health oriented pharmaceuticalcare’ are required in fields such as the primary andsecondarypreventionofvasculardisease(WHO,2013;Wald, 2013). More pro-active approaches to relieving
Box 2. Priority needs and priority medicines
In2004theNetherlandsMinistryofHealthcommissionedtheWHOtoproduceareportentitledPriority Medicines for Europe and the World. At the request of theEuropeanCommission thiswasupdated in2013, foruseasaresearchprogrammeplanningresource.Theresulting analysis highlighted the high global burdensimposedby ischaemicheartdisease/CHDandstoke,andalsobydepressiveillness.Italsoemphasisedtheneedfor innovativetreatmentsfor indicationssuchasosteoarthritis, Alzheimer’s disease, hearing loss, lowback pain, chronic obstructive pulmonary disease(COPD), alcoholic liver disease,malaria, tuberculosis,diarrhoeal disease, pneumonia, neonatal conditionsand maternal mortality reduction in settings such asruralNigeriaandIndia.
Suchsourcesalsostressthecollectiveimpactsofrarediseases. Robust epidemiological data are in manyplaceslacking.Yetinaggregateraregeneticandotherconditions at any one time affect approaching half abillionpeopleacrosstheworldasawhole.Mostcannotas yet be prevented, and lack definitive treatment.Illustrative examples range from Addison’s DiseaseandCysticFibrosisthroughto,forinstance,Wegener’s
Granulomatosis(whichinvolvesorgandamagecausedbyrecurrentepisodesofbloodvesselinflammation)andZollinger-EllisonSyndrome.The latter ischaracterisedbyextensivegastro-intestinalulceration.
The latest edition of Priority Medicines for Europe and the World also underlines the importance oftropical conditions like Buruli ulcer (a necrotisinginfection), leposy, African sleeping sickness (Africantrypansomiasis),GuineaWormandYaws.Eventodaythese infections still severely affect around a billionpeople.
However, there is evidence that during the pastdecadesubstantiveprogresshasbeenmadetowardsestablishing public private partnerships capable ofovercomingthemarketandgovernancefailureswhichinthepast ledtounder-investment inresearchaimedat generating innovative solutions to health problemscommonly affecting the world’s poorest populations.Further improvements in diagnostic products,medicinesandvaccinesarestillurgentlyneeded.Butatthesametimeitistruetosaythattheterm‘neglectedtropicaldiseases’isnowwellonthewaytobecomingredundant.

Patients’Needs,MedicinesInnovationandtheGlobalPublic’sInterests 9
the burdens of parasitic disease via better applicationofexistingtreatmentscouldalsogenerateconsiderableadditional benefit many parts of Asia and Africa(Anderson,2013).
There are other unexploited opportunities for, forinstance, further reducing the incidenceof the variousformsofHepatitistogetherwithHPVandHIV infectionrates,aswellasachievingmoreprogressagainstancientscourgessuchasmalariaandTB.Theselastaregoodexamples of fields where both better use of existingtreatmentsandnewwaysof immunisingpeopleatriskofsuchillnessesorcuringthosewhofallvictimtothemareurgentlyneeded.
Necessary conditions for innovation
Itisoftensaidthatnecessityisthemotherofinvention.It is certainly the case that patient, professional andpublic demand for any new technology, product orservicecanbeavaluablepre-conditionforitssuccessfulintroduction.Buteven‘lifeordeath’needscannotalwaysbemet–simplywantinginnovationstooccurbringsnoguaranteeofdeliveringthem.Moreover,thefullutilityofnewtechnologiesonoccasionsonlybecomesapparent–inhealthcareaswellasinotherareas–decadesaftertheirinitialintroduction.
Forinstance,whenanti-depressantmedicineswerefirstmarketed in the1950s therewasonlya limitedpublicand professional awareness depressive illness, albeittherewasat that timeanextensiveand longstandinguse of drugs such as barbiturate sedatives for lesswell defined mental distress. (Barbiturate containingmedicineswerealsofirstmarketedbyBayerintheearly1900s, under trade names like Veronal and Luminal.)Such observations underline the fact that centralisedinterventions to support the funding of innovativeresearch can be counterproductive if they are undulydirective. IPRs such as those conferred by patentscounterthishazard,inthattheycanbeusedtorewardunplannedandpre-plannedinnovationsalike.
Overandabovetheavailabilityof fundingforresearch,the existence or otherwise of the human and culturalresources required to innovate successfully is anotherimportant factor. Inquiring and free thinking mindsare often vital for the successful identification andinterpretationofunexpectedphenomena.However,thekeypointtostressisthatalthoughpoliticalexpressionsof medicines and other development priorities canhighlight the desirability of, for instance, preventing orbeingable to treatconditions likeAlzheimer’sdisease,such progressmay – failing serendipitous luck – onlybecome possible when a complaint’s fundamentalmechanisms are sufficiently well understood to permiteffectivetargeting.
Research advancesmade since the 1970smean thatimprovements in therapy are becoming increasinglyavailable in thecaseofcancers.But this isnotyetsowithmuchoftheneurologicaldiseaseburden.Individualsandorganisationsseekingtoprotectpatientinterestsincontinuinginnovationneedsympatheticinsightintowhat
islikelytobescientificallypossibleasanextstepforwardatanyonetime,aswellasarobustunderstandingoftheprogressultimatelyneeded.
Medicines as economic entities
One of the reasons for misunderstandings anddisagreements about issues such as the pricing ofinnovativemedicinesandtheneedforintellectualpropertyrightsisthatalthoughpharmaceuticalproductsareoftenseenasobjectsofhighfinancial,clinicalandsocialvalue,themarginalcostoftheirproductionis–especiallywhentheyarebeingsuppliedinhighvolumes–typicallylowascomparedwiththeamountofmoneyneededtodevelopthem.This isparticularly true in thecaseof the ‘smallmolecule, cell surface receptor targeted’medicines atthe heart of the first great pharmaceutical revolutionwhichtookplacefromthestartofmasspenicillinuseinthelate1940sthroughto(followingpioneeringacademicdiscoveriesoriginalJapanesepharmaceuticalresearch)theglobalmarketingofstatinsforloweringlipidlevelsbyUScompaniessuchasMSDandPfizerinthe1990s.
An importantpointtoemphasise inthiscontext isthatthe‘value’ofmedicinesliesnotsomuchinthematerialstheycontainbutinthescientificchallengesandmaterialcosts of their development, togetherwith their clinicaleffectiveness in use.5 Research expenditures mayreasonably be taken to include investments made inthe pre-clinical development and clinical trials of notonly successful products, but also innovations thatfail to reach themarket.Even in thecaseof the largemolecule‘biologicals’thattodayaccountforaboutahalfofallpharmaceuticalspendingin‘developed’countries,pharmaceuticalproductsareinunitcosttermsnormallyrelatively inexpensive to supply once a marketingauthorisationhasbeenobtainedandanadequatesalesbaseestablished.
Hence when pharmaceutical products lose marketingexclusivityitisnormallypossibleforgenericmanufacturerstoofferthematafraction(oftenunder10percentinthecaseofmedicineswithsmallmoleculechemicalsastheiractivepharmaceuticalingredients)oftheinnovators’price,albeitthatwhenreturnsfalltocommoditylevelssupplycontinuitycanbecomeuncertain.Forobserverswhodonotdifferentiatebetweenthecostofthephysicalmaterialamedicine ismadeupofand thatof itsdevelopmentandendpointvaluetoitsusers,theexistenceof largedifferences between a generic manufacturers’ priceandthatoftheoriginalIPprotectedproductcanseemto provide evidence of exploitation. Yet this is, baringexceptional cases, an incorrect interpretation from aninformedpublicandpatientinterestviewpoint.
5 Substancessuchasgoldanddiamondshavebeenvaluedthroughouthistorybecauseoftheirscarcityaswellasthevarietyofdecorativeandpracticalusestowhichtheycanbeput.Butmodernmedicinescannormallybeproducedrelativelycheaplyinlargevolumes.Thevalueofsuchinnovationsrelatesmuchmoretotheirintellectualsubstancethantheirmaterialscarcity,afactwhichtraditionallymindedobserverscanfinddifficulttofullyaccept.

10 Patients’Needs,MedicinesInnovationandtheGlobalPublic’sInterests
Relatedpointsinclude:
• modern medicines are high technology products, but unlike items such as aircraft engines they do not have multiple parts. This adds further toinnovators’needsforpatentsand/oralternativessuchasregulatorydataprotection.Therelativesimplicityofpharmaceuticalsoftenmakesthemeasytocopy.Atthesametimetheirmanufacturersarenot,becauseof the need for regulatory approvals, easily able tomodify medicines once they are on the market. Inmanyothersectorsinnovativemanufacturersareableto‘keepaheadofthecompetition’throughserialre-designs;
• the effective removal of brand name and trade mark protection for innovative medicines in most OECD markets has since the 1980s further increased reliance on patents or regulatory process linked exclusivity for the revenues needed to support ongoing R&D. In advancedpharmaceutical markets medicine producers canno longer employbrandnameprotection to secure‘extra-normal’earnings.6Thisisdesirableinasmuchasmarketsthataremainlyreliantonbrandnamestodifferentiatebetweenmedicineswiththesameactiveingredientscanbecomedistorted.Butitonceagainleaves investors in pharmaceutical research anddevelopmentinavulnerableposition.Takentogetherwith other factors such phenomena help to explainwhy pharmaceutical research outlays may now bestabilisingorfallinginEuropeandtheUS–seeFigure3;and
• the introduction of more low volume ‘orphan’ treatments and the expanding role of complex biological molecules in modern therapeutics has fundamentally changed the world pharmaceutical market. Medicinesforraredisorders
havebydefinitionsmallermarketsthanthoseofthe‘blockbusters’ofthe20thcentury.Butthisdoesnotreducetheirdevelopmentcoststoacommensuratedegree. It may, for instance, sometimes be moreexpensivetorunclinicaltrialsfor‘orphan’conditionsthanitisformoreprevalentones(Daviesetal,2012).At the same time the growing number of biologicalas opposed to ‘chemical’ medicines has alteredthe economics and techniques of pharmaceuticalmanufacturing. When it cannot be assumed thatit is safe to substitute one biological product withanother‘biosimilar’agentthismight–foraperiod,atleast–reducetherelianceofpharmaceuticalsectorinnovatorsonIPRs.However,patientinterestscouldbenegativelyimpactedifthiswereinfuturetoresultinanunduerelianceonsecretproduction‘knowhow’asopposedtopublishedscience.
Given these and other considerations itmight be thatin coming decades (during which biopharmaceuticalresearch and development could prove still moredifficult and time consuming to conduct, and healthcareresourcesmaybecomemorelimited)policymakersseeking affordable and more effective medicines willconsider extending the periods of exclusive supplyavailabletoinnovators.Inreturnforpermittingthelatterlonger periods of time to accrue returns from theirinvestments,legislatorscouldrequireextendedresearchbased industry commitments in areas such as tieredglobalpricingandthesupplyofessentialtreatmentsfreeoratminimal/marginalcostinverypoorcommunities.
Such reformsmight be able to serve patient interestsbetter than existing arrangements. However, beforequestions relating to such options are considered inmoredetailthisanalysisbrieflyconsidersthenatureandpurposesofintellectualpropertyprotection.
Intellectual Property Law and Access to Treatment
Theterms‘intellectualproperty’and‘intellectualpropertyrights’ have been in use for about a century. Yet theywerenotwidelyemployeduntil relativelyrecently.Theirgrowingutilisationunderlinesthefactthatinthemodernworldpatentsarenottheonlywayofprovidingpotentialinnovatorswithanincentivetoriskinvestingsubstantialresources in research and development projects thatmay well fail, however competent the people runningthem.7
Concepts relating to the rightful ownership of objectsthatindividualshavemade(oranimalstheyhavebred,orlandsthatthey‘discovered’)gobackfarinhumanhistory.ThemodernEnglish term ‘branding’can, for instance,
Figure 3: Pharmaceutical R&D Expenditure in Europe, USA and Japan
Source:EFPIA,2012(datanotinflationadjusted)
6 Theterm‘thegenericsparadox’appliestothefactthatinthepastinnovativemanufacturerswereabletoretainearningsbyraising(oratleastnotdropping)thepricesoftheirproductsafterpatent/IPexpirybyvirtueoftheinelasticbehaviourofbrand-loyalprescribers(Kanavosetal,2008).Intoday’sconditionssuchstrategiesarenotnormallyviableinmarketssuchastheUSandmostEUmemberStates,albeitthatinlessdevelopedmarketsbrandloyaltyremainsanimportantfactor.
7 Researchanddevelopmentprojectsaimedatfindinglowercostwaysofmakinggivenmedicinesandotherproductsarealsoofvaluetosociety,aswellastoindividualsseekingcommercialadvantage.Productionandsupply‘frugality’canandshouldcontributetoenhancingaffordabilityandaccessoverthelifecycleofatechnology.Butthefailurerisksinvolvedininvestinginthissortofinnovationareverymuchlowerthanthoseassociatedwithdevelopingnewtherapies.Hencethe‘price’ofthecapitalrequiredislower.

Patients’Needs,MedicinesInnovationandtheGlobalPublic’sInterests 11
be linked to the oldNorseword for burning, ‘brandr’.There isevidence thatpeople inscribedanimals’hideswith marks denoting ownership during the early IronAge.Subsequentlyartisansworkingintheancientworldalsoput personalmarks on the items they fabricated.In the Roman Empire, for instance, both builders andswordsmithsusedearlyformsoftrademark.
The granting by Royal courts – and in Greek historysomeCityStates–ofmonopoliestopermitincome(andtax)generationalsohasalonghistory,ashastheuseof‘tradesecrets’topreventwhat inventorshaveseenasundesirablecompetitionfromcopyists.InfeudalChina,forexample, revealingthesecretsofsilkproductionorsmugglingsilkwormsbeyond thenation’sborderswassubject to thedeathpenalty.Foraround twomillenniathispreventedtheproductionofsilkoutsidethecountry,and ensured high prices. Similarly, diamond polishingtechniqueswerekeptsecretinIndia.InancientIndiatheShreni–aformofearlyguild–inpartservedtoprotectwhatmaytodaybetermedmanufacturingsecrets.
The more immediate origins of modern intellectualproperty law relating to on the one hand productswith practical applications such as newdrugs or, say,diagnostic imagingmachines and on the other artisticdesigns and creations like works of music date backsome500years,toVeniceinsouthernEuropeandBritaintothenorth.In1623,forinstance,James1ofEnglandrevokedallpreviouslygrantedpatentsbyintroducinganewStatuteofMonopolies.
Until then, Royal grants had often served to restrictcompetitionandrewardindividualswhoweresupportersof themonarchy,ratherthan innovatorsper se.Butasa result ofmodernising pressures associatedwith thegradualstrengtheningofmerchantandtradinginterestslocatedoutsidetheRoyalCourt, therevised legislationprovided for the issuing of ‘letters patent and grants of privilege for the term of fourteen years or under,…. of the sole working or making of any manner of new manufactures…. to the true and first inventor’.
Copyright provisions (that have now been extendedfarbeyond theperiodsofprotectionprovided forbypatents)werefirst introducedatthestartofthe18thcentury. As industrialisation and mass productiongained momentum, laws to protect designs werealso introduced. In the US, where individuals’rights to intellectual property were enshrined in the1787 Constitution,8 a pioneering Patent Office wasestablished in1836.Asthequotation fromAbrahamLincoln’s 1860 lecture ‘Discoveries, Inventions and Improvements’ on the rear cover of this reportillustrates, intellectual property ownership hasthroughout theUnitedStates’history (and from longbeforeitseconomywasabletocompetewiththoseofthemajorEuropeanpowers)beenregardedascentralto the support of innovation and democraticallyunderpinnedeconomicprogress.
One important aspect of patents and allied provisionsis that they demand publication.Hence although theyawardtemporarymonopoliestheyalsopromotechangeinawaythatsecrecybasedapproachesdonot.In1883the Paris Convention for the Protection of IntellectualProperty represented the first international attempt toco-ordinatetheprotectionofinnovator’sandtheglobalpublic’s interests. Theconclusionsagreedat that timewere in part revised via a meeting held in Stockholmin 1967. However, substantive progress towardsharmonised world-wide arrangements has been slow.This has been because of deep seated conflicts ofperceivedandactualinterest,coupledwithanapparentlackofpoliticalappetiteforleadingfundamentalreform.
Many commentators describe intellectual propertyprovisionsintermsoftheircapacitytoenablesuccessfulinnovatorstorecoverthe‘sunkcosts’ofpastactivities.There is some validity in this perspective. But from apublic interestviewpointtheprimarypurposeofgrantssuchaspatentsisnottoproviderewardsforinnovationsthatarealreadyavailable.Itisrathertoaddressconcernsrelatingto thewillingnessof investors togoonputtinglargeamountsofmoneyintoinnovatingforthefuture.
Thefirst‘neo-medicinal’patentwasgrantedforEpsomsaltsinEnglandin1698.9Buttheterm‘patentmedicines’hasuntilquiterecentlyhad‘snakeoil’connotationsthatstemmedfromthedevelopmentofpharmacyintheUnitedStates.DespitethefactthataschoolofpharmacywasestablishedinPhiladelphiainasearlyas1813,American‘drug sellers’ were throughout the nineteenth centurynormallyunqualifiedandnot infrequentlycharlatans. Inthis context ‘patent’ or ‘secret’ medicines were oftencorruptedderivativesoftraditionaltreatmentsthatwerebrandedbutdidnot in factenjoypatents.These‘curealls’wereinmanyinstancesbothclinicallyineffectiveandhazardous,notleastbecauseofcommonadditivessuchascocaineand/ormorphine.
WHOestimatessuggestthatattheendofthetwentiethcentury approaching half the world’s population wasstill primarilydependenton traditionalmedicines for theday-to-day treatment of common complaints (Zhang,1999).Despitechangingpublicdemandsandattemptstoimproveaccesstoallopathic(modernsciencebased)medicinesthisisstill likelytobebroadlythecasetoday,despite the fact that virtually all the pharmaceuticalsclassifiedasessentialbytheWHOarealreadyavailableasgeneric,oratleastasoff-patentbutbranded,products.
The word ‘essential’ carries with it connotations ofboth effectiveness and suitability for low cost massuse. Medicines which can marginally improve or to alimiteddegreeextend(butdonotsave)livesonlywhensuppliedasapartofahighlysophisticatedhealthcareprogrammeshouldnot, itcanbeargued,beclassifiedas essential, especiallywhen the service infrastructureneededtosupporttheirbeingtakenbeneficiallydoesnotexist.
8 Philosophically,suchthinkingcanbelinkedtotheworkofseventeenththeoristssuchasJohnLocke,aswellastotheanalysesofferedbymorerecentAmericanentitlementtheoristssuchasRobertNozick.
9 Aformofmagnesiumsulphate.Epsomsaltshavevariousexternalandinternalmedicinalapplications.Thecompoundishighlysolubleandanearlyusewasas‘bathsalt’.EpsomitewasinitiallyextractedfromasourceclosetotheSurrytownofEpsom.
12 Patients’Needs,MedicinesInnovationandtheGlobalPublic’sInterests
Inadequacies in essential medicines supply and thelackofbasicprofessionalhelpneededtofacilitatetheireffectiveuse,coupledwithproblemsofpovertyandthesocialcomplicationsassociatedwithchangingpatternsof healthbelief,make somemodernday communitiesasvulnerabletomedicinesrelatedharmaspeoplewerein nineteenth century America. The challenges theyface range from having little or no access to effectivetreatments through to being exposed to the risks offalsified(counterfeit)and/orsub-standardproducts.
Some observers (in line with the commentsmade byIndiraGhandiat thestartof the1980s,quotedontherearcoverof this report) attribute suchphenomena totheeffectsofintellectualpropertylaws.Butthispositionis very questionable. The former Prime Minister’sremarks may have fairly represented the situation inwhich India found itself in the1950sandearly1960s,after the departure of the British (who during theirperiodinpowerhadfailedadequatelytosupportIndianindustrial development and local medicines supply)andtheshockofthe1962Sino-Indianconflict.Yetthefact that widespread problems relating to inadequatemedicinesprovisionhavepersistedafter Indiabecametheworld’smostsuccessfulgenericmedicinesexporterindicates that their causes – like those of inadequatehealthcareprovisionmorewidely–aremorecomplexthanissometimesassumed.
There is a danger that if the undesirable impacts ofpharmaceutical sector IPRs are exaggerated and their
benefitsunder-stated,theendresultwillbeasignificantundermining of medicines research funding in boththe private and public sectors (Box 3). At the sametimechallengessurroundingthetreatmentofHIVhavedemonstrated that on occasions a lack of affordableaccess to innovativeasopposed tomaturemedicinescan on occasions seriously endanger public health inpoor communities that lack universal health coveragesystems.Asalreadynoted,similarconcernsarestartingtoemergeinotherfields,mostnotablycancercare.
The significance of policy questions linked to theabove is explored below with regard to the WorldTrade Organisation’s TRIPS (Trade Related Aspectsof Intellectual Property Rights) agreement, and therelevance to global patient and public interests of theflexibilitiesdeclared(in2001)inDoha.Butbeforethisafurtherbriefdiscussionofissuesrelatingtothetreatmentof HIV is offered. The past weaknesses of not onlypharmaceutical industry but also some governments’approaches to this area has in recent decades donemuch to increase patient and wider public concernsabout thenegativepublichealth impactsof IPRs.Thedevelopmentofeffectiveanti-HIVdrugswasatriumphforresearchbasedcompaniesandtheirUniversityandotherpublicsectorpartners.However, thereputationaldamage to the innovative pharmaceutical industryassociatedwithHIVpatientsnotbeingabletoaffordlifesavingtreatmenthasbeencomparabletothat inflictedbytheThalidomidetragedyoftheearly1960s.
Box 3. The shared determinants of private and public spending on innovation
In an ideal world the public funding of innovativeresearch would arguably focus on areas where theincentivesintendedtomotivateprivateinvestmentareleast likely to prove adequate. This should minimisethe riskofharmfulmarket failures.Thishasbeen thecase in that, for instance,publicmoney ismore likelytobedevotedto‘fundamental’scientificinvestigations,while private agencies are more oriented towardsthe commercialisation of new therapeutic conceptsonce the possibility of a viable application has beendemonstrated. But in terms of research topics bothpublic and private investors have in the past oftenconcentrated their attention on issues of primaryimportance to countries at the forefront of humandevelopment, rather than thepriorityneedsofpoorerandlessadvancedcommunities.
Itwasperhapsassumedthatthelattercoulduseexistingtechnologiestoovercometheproblemsothernationshadleftbehindthem.Butthisisnotnecessarilythecase.Incontextssuchasthedevelopmentofnewtreatmentsfor tropical conditions, new approaches to fundingandrisksharingarenowcorrectingsuchimbalances.Relevant drivers have ranged from the examples setby institutionssuchas theGatesFoundationandtheCarterCenterthroughtotheglobalisationoftheworldeconomyand the changing situation andpriorities oftheresearchbasedpharmaceuticalindustry.
However, were the support structures that encourageprivate spending on high risk medicines and alliedinnovative research initially intended to meet needs inOECD and other relatively affluentmarkets to in futureprove inadequate to sustain investment levels, itwouldbe unwise to assume that public expenditures willautomatically replace reduced private capital and alliedfinancial flows. Governments, like businesses, seekcompetitive advantage. In the context of innovationthey can create and sustain the educational and otherinfrastructuresandthesocialandregulatoryenvironmentsrequired forsuccess,using funds raised fromdomestictaxes. Further ‘downstream’, companies generateinternationalsalesthroughtheircommercialactivities.Thiscaninturnfurthersustainpublicsectorrevenues.
The danger for patients and the other beneficiaries ofpharmaceuticalinnovationisthatiftheprospectofprivateprofitfromthesupplyofnewmedicinesdeclines,sotoointimewillpublicinvestmentinthediscoveryprocessesthatopenthewaytotheirdevelopment.Thereisalsoapossibilitythat,despitetheimportanceofpublicsectorvalues,adeclineincommercialethosdriveninnovationwillweakentheefficiencyoftheoverallsystem.Thekeypointtoemphasiseisthatpubliclyandprivatelyfundedagencies have vital andmutually complementary rolesto play in pharmaceutical and other science basedinnovativeprocesses(Mazzucato,2013).
Patients’Needs,MedicinesInnovationandtheGlobalPublic’sInterests 13
Theavailabledatasuggestthatinsubstantialareasofsub-SaharanAfricaupto50percentofthepeoplewhocouldbenefitfromARVtherapyarenowinreceiptofit(see,forinstance, UNAIDS 2012). In settings such as India thisfigure could in fact be closer (allowing for undiagnosedinfections)to25percent,andtherearealsolikelytobereservoirsofpoorlytreatedinfectionincountriessuchasChina, theRussianFederationandsomeotherpartsoftheformerSovietUnion.Yettheoverallglobalresponseto thishistoricallynew threat tohumanhealthcannowbeseenassuccessful.AtnoothertimeinhistorycouldtheHIVpandemichavebeensoeffectivelyandequitablycontained.Therapiddevelopmentofnewtreatmentswasmade possible by the conditions for innovation alreadybeinginplace(Box4).
Nevertheless,thecostofpatentedHIVtreatmentshasbeenamatter of frequent concern. At first US based activistsfearedthatbecauseHIVwasregardedasa‘gay’diseaseitstreatmentwouldbeneglectedbybothgovernmentsandpharmaceuticalcompanies.Thisprovedunfounded.YetasinsettingsfromtheUSWhiteHousetothetownsandvillagesof southern IndiaandAfrica it becamebetter understoodthatthediseasehadalreadyspreadwithinmanylessaffluentcommunities,questionsaboutthepriceofpatentprotectedanti-HIVmedicinesbecameincreasinglypressing.
By themiddle to late 1990s the cost of patentedHIVtreatmentswasacentralfocusofattention.At$10,000ormorepercapitaperannumitwasacceptableinrichernationswithuniversalhealthcaresystems.Yeteven inAmerica uninsured people, especially minority groupmembers,wereworriedthattheywouldnotgetaccesstoeffectivecare.Formostindividualsandfamiliesinthedevelopingworldlifesavinganti-retroviraltreatmentwasclearlyunaffordable.
As a result companies that had playedmajor roles increatingthetechnologyneededtocombatAIDSbecameseen as the instigators of barriers to its humanitarian
Anti-retroviral (ARV) medicines affordability
TheoriginsofHumanImmuneVirus(HIV)infectionlieinsub-SaharanAfrica,andtransfersofmicrobesfoundinapestopeopleviahunting.Sucheventsalmostcertainlyoccurredmany timesduring thecourseofhistory.ButwiththeopeningupoftheAfricaninteriorinthetwentiethcentury the chance of infections spreading into thewider human population progressively increased. Thefirstclearly identifiedcasesofwhatcametobeknownas AIDS occurred in the United States in the early1980s. Itwas at that timeoften seen as adiseaseofrelativelyadvantagedgaymen.Forexample,theFrenchphilosopherMichel Foucault – an occasional visitor toAmericanWestCoastsaunahouses–diedofitin1984.
Initially little could be done for people with HIV, otherthan providing compassionate nursing care. Butfollowing the introduction of AZT (whichwas originallyinvestigatedasapossibleanti-cancertherapy) in1987andthedevelopmentofitsuseincombinationwithotherdrugs in 1992, academic andpharmaceutical industryresearchersdevelopedincrementallymoreeffectiveARVtreatments.Today few individualswhohaveaccess tomodernpharmaceuticalcareandareabletotaketheirmedicinesasrecommendedarelikelytodieprematurelyasaresultofHIVinfection.
There is also evidence that the use of HAART (highlyactive anti-retroviral treatment) regimens reduces HIVtransmissionrisks.ItmightbethatinasyetrareinstancesthetimelyuseofARVmedicineshasdeliveredeffectivecures. Even if the development of a vaccine remainselusive, drug based therapies employed alongsideotherpublichealthinterventionsmay–givencontinuinginnovationsufficienttooffsetthechallengesofacquiredviraldrugresistance–ultimatelybecapableofeliminatingHIVfromtheworld-widehumanpopulation.
Box 4. Innovative surroundings
Innovative environments are characterised bycombinations of scarce resources being available,includingcriticalmassesofeducated,skilled,creativeand motivated people through to suitable physicalenvironments for them to live and work in. Systemsfor funding research viamechanisms such as grantsfrompublicbodiesalongwithopportunitiestoprovideprivateservicesprofitabilityarealso important,asareopen cultures which encourage new thinking andoriginal knowledge applications. Innovative potentialiscloselyassociatedwithoverallhumandevelopmentand theestablishmentof settings inwhich ideasandinformationcanbeexchangedsafely,withaconfidentsense that individual and corporate contributions toknowledgewillbefairlyrecognised.
Non-innovative environments may in the health carecontextbecharacterisedbypoor leadershipthat failsto prioritise treatment and service improvements,coupledwithweakITandotherserviceinfrastructures,
low public expectations and limited personaldevelopmentopportunities.Povertyisamajordriverofsuch negative variables. But above and beyond this,differences between national approaches in contextssuchasregulationandIPandalliedlegalprovisionscanhave significant impacts. For example, the increasingmonetaryandtimecostofestablishingclinicaltrialsinEurope appears in recent years to have reduced thenumberof investigationsbeingundertaken in theEU,ifnottheircost.
TheexistenceorotherwiseofmajorresearchorientedUniversities is another potentially important influenceon national abilities to conduct the scientific inquiriesneeded to underpin innovation. Patient organisationswithan interest in thedevelopmentofbettermedicaland pharmaceutical treatments should arguably beaware of such factors, and able when necessary todefend public interests in the balanced support ofefficientinnovation.
14 Patients’Needs,MedicinesInnovationandtheGlobalPublic’sInterests
application, largelybecause– itwasalleged–of theiruncaringuseof the IPRsavailable to them.Theywerechargedwithbeingnarrowlyconcernedwithkeepingthepricebasefortheirproductsuniversallyhighinordertomaximise their ‘richworld’ incomes,even though theycouldhavesavedlargenumbersoflivesbysupplyingatproductioncostlevelsinregionslikesub-SaharanAfricaandSouthAsia.
There was some truth in such allegations, albeit thatthesituationwasmorecomplexthanisoftenassumed.In many very poor countries patents were not evenfiled, because of the lack of infrastructure needed toestablishmedicines production (Attaran and Gillespie-White, 2001). Supported by organisations such asMedicines Sans Frontiers (MSF), Oxfam and HealthActionInternational(HAI),countrieslikeBrazilandSouthAfricamovedtodefendthehealthoftheirpopulationsbygrantingcompulsorylicencesforARVmedicinesand/oragainstthethreatofsuchinterventionsnegotiatinglowerpriceswiththeiroriginators.
At the same time activists such as James Love ofKnowledge Ecology International co-operated with DrYusuf Hamied of the Indian pharmaceutical companyCipla to develop a $1 a day combination therapy. This‘offer’madeworld-wideheadlinesandarguablycatalysedseveralformsofprogress.ItsimpacthasbeenlinkedwiththesubsequentdevelopmentoftheGlobalFundforHIV,TBandMalariaandadoptionoftheDohadeclarationonTRIPSandpublichealthattheendof2001.
Putting public health first
From a public and patient interest perspective, a keypoint to make in relation to the establishment of thestill improving essential drug supply system for theglobal management of HIV is that research basedpharmaceutical companies and many governmentswere(despitewarnings)inthe1990sslowtounderstandthe gravity of the HIV pandemic.Many public officialsand industry executives seemed initially blind to thehealth consequences of failing to provide universallyaffordable treatment, and the impacts thiswouldhaveonpatientandpublicopinion.Inretrospectthereseemslittle excuse for such inadequacies. However, modelsof development in which ‘new’ diseases typically onlybecame problematic as populations grew richer andagedmayhavecreatedmindsetsinwhichitwasdifficulttoseethatmeetingthechallengeofHIVwoulddemandmaking theworld’s newestmedicines rapidly availableintheworld’spoorestandleastsophisticatedsocieties.
In the leadership vacuum that for a time ensued,pharmaceutical companies on occasions becamescapegoats for the inability of the world communityto takeeffectiveaction.But regardlessof the faultsofothers, the governance and direction of the researchbasedpharmaceutical industry itself failed tomeet thestandardsthatmany21stcenturyconsumershadcometo expect (Wolff, 2012). Companies’ did not alwaysappeartohavethepursuitofbetterglobalpublichealth,via both medicines innovation and facilitating goodaccesstoessentialcare,asahighprioritygoal.Saying
inanunqualifiedmannerthattheprimaryresponsibilityof any health care related organisation is to itsshareholders is intoday’senvironmentwidelyregardedasunacceptable.
Patient Interests in Better Medicines and Better Health
Theexistenceofpatentsandsimilarformsofexclusivityforinnovatorssometimesappearstoberegardedastheroot cause of people being unable to obtain essentialmedicines in timely and affordable ways. (See, forexample,MSF, 2012.) But the view taken here is thatIPRs(asopposedtofactorssuchaspovertyandalackof the political andmanagerial will needed to improvehealthcaresystems)arenotthefundamentalcauseofsuch supply problems.Without IPRs thedevelopmentof effective anti-retroviral therapies and many otherinnovations would almost certainly have been slowerthanhas in factbeenthecase,andthere isno logicalreasontobelievethatIPprovisionssuchaspatentsareincompatiblewith thesystemsneededtoassuregoodglobalaccesstoessentialtreatments.
Giventhatnewmechanismsfordrugandalliedproductpurchasingandsupplyarenowevolvingtoprotecttheinterests of the world community in better access totreatment(asisso,forinstance,inthecaseoftheGAVIAlliancewithvaccines)itisimportantnottolosesightofparallelglobalpublicinterestsininvestingininnovation.It isagainst thisbackgroundthataseriesofquestionsthatpatientsandtheirrepresentativesmaywishtoaskare explored below.However, before this it is relevanttoconsiderwhyitmattersmorethaneverbeforewhatpatientsandtheirrepresentativesthinkaboutmedicineresearchandsupply.
Self care in health care
Throughout history individuals have sought to carefor their own health and that of their families. Yetas populations pass through demographic andepidemiologicaltransitionpeoplelivinginthembecomeincreasinglyinformedandintellectuallymoreable(Flynn,2009).Suchtrendsenhancepeoples’abilitiestopursuetheirgoalsandchangetheirrelationshipswithauthorityfiguressuchashealthcareprofessionals.Asindividualsin post transitional societies come to feel themselves,theirchildrenandothersinandbeyondtheirimmediatecommunitiestobeentitledtolongandhealthylivestheybecomemorequestioning,andaccesstogoodqualityhealthcaretendstobecomemoreofacollectivepriority(TaylorandBury,2007).
At the same time health service users also becomeincreasingly likely to reject paternalistic relationships infavourofmoreequalpartnerships(Charlesetal,1997).Hencethedemandsplacedonnotonlycliniciansbutalsoresearchers,patientsandpatientorganisationschange.For example, concepts such as obtaining informedconsent tomedical interventionsgaingreatercurrency
Patients’Needs,MedicinesInnovationandtheGlobalPublic’sInterests 15
(Staceyetal,2008).Demandsforthefullpublicationofclinicaltrialfindingssimilarlyincrease.
In addition to enhancing therapeutic dialogue at thepersonal level, strengthened patient participation inhealthandsocialcaredecisionmakingcanaddsystemicvalue. This is achieved via enabling individuals andgroups to bearwitness as to howpower is exercisedin therapeutic relationshipsand topromoteawarenessof good and bad practices. Such reforms reduce thedangers associated with institutionalised professionaland other provider side interests dominating practice,researchand/orpolicycultures.Inmuchthesamewaythatunlockingclosedhospitalwardscanrevealabuses,openingbothserviceandresearchplanningtochallengeanddebatefocusesattentionmoreclearlyonthepursuitofconsumerinterests.
Beyond this, patient participation in areas suchas research governance can contribute to theunderstandingofboth‘objective’and‘subjective’facts(Kayeet al, 2012;FDA,2013). For instance, theworkoforganisationssuchastheEURORDIS(RareDiseasesEurope)andothersimilarbodieshashelpedtoenhancescientific understanding of disorders that due to theirrarityareoftenpoorlydescribedintheavailableclinicalliterature (Mavris and Le Cam, 2012). Likewise in theUSNORD(theNationalOrganisationofRareDisorders)wasinlargepartresponsibleforgeneratingthepoliticalunderstanding and will that led to the original 1983OrphanDrugAct(Box5).IntheUKpatientinvolvementin the work of NICE (now the National Institute forHealthandCareExcellence)hasalsohelpedto informapproachestovaluingmedicines.
Patient led understanding of the impacts of rareconditions on individuals and minorities can counter-balancecrude‘greatestgoodforthegreatestnumber’thinking about social justice. Even the communicationof subjectiveexperiencesofparticular formsof illness,disability and exclusion can contribute usefully todevelopingappropriatetreatmentandcareapproaches.
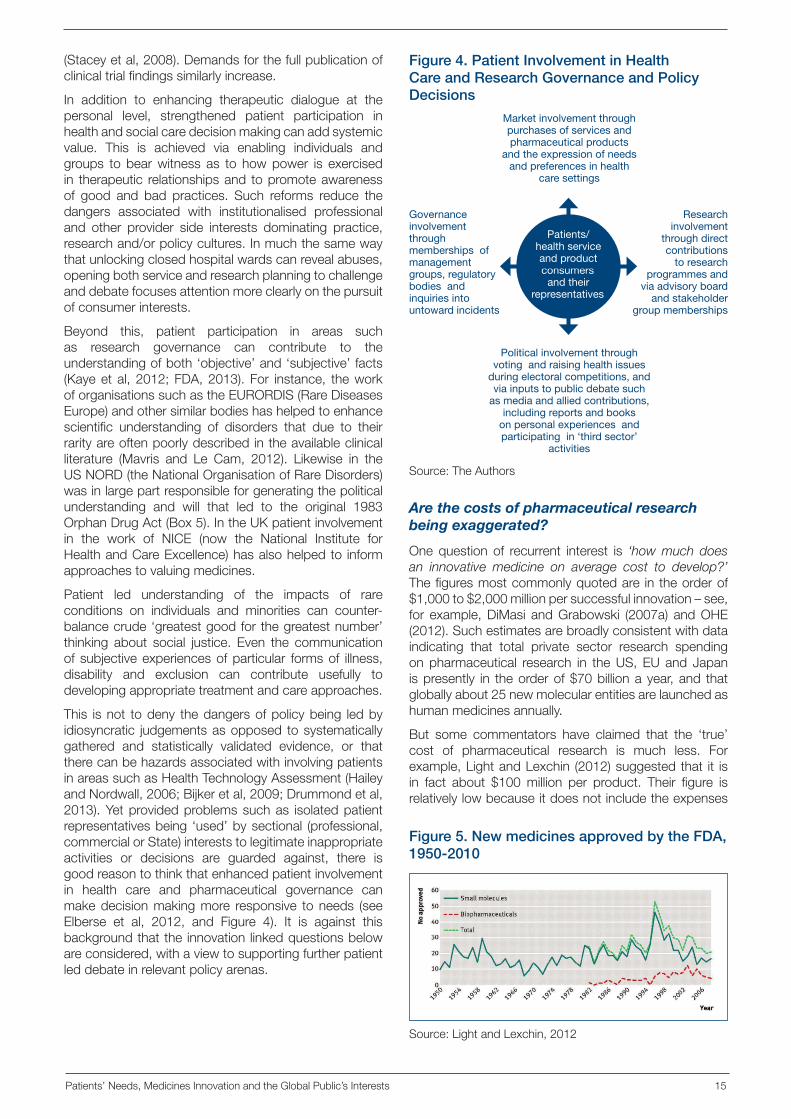
This isnot todeny thedangersofpolicybeing ledbyidiosyncratic judgementsasopposed tosystematicallygathered and statistically validated evidence, or thattherecanbehazardsassociatedwithinvolvingpatientsinareassuchasHealthTechnologyAssessment(HaileyandNordwall,2006;Bijkeretal,2009;Drummondetal,2013).Yetprovidedproblemssuchas isolatedpatientrepresentativesbeing ‘used’bysectional (professional,commercialorState)intereststolegitimateinappropriateactivities or decisions are guarded against, there isgoodreasontothinkthatenhancedpatientinvolvementin health care and pharmaceutical governance canmakedecisionmakingmore responsive toneeds (seeElberse et al, 2012, and Figure 4). It is against thisbackgroundthatthe innovation linkedquestionsbelowareconsidered,withaviewtosupportingfurtherpatientleddebateinrelevantpolicyarenas.
Are the costs of pharmaceutical research being exaggerated?
Onequestion of recurrent interest is ‘how much does an innovative medicine on average cost to develop?’Thefiguresmostcommonlyquotedare intheorderof$1,000to$2,000millionpersuccessfulinnovation–see,for example,DiMasi andGrabowski (2007a) andOHE(2012).Suchestimatesarebroadlyconsistentwithdataindicating that total private sector research spendingon pharmaceutical research in theUS, EU and Japanispresently in theorderof$70billionayear,and thatgloballyabout25newmolecularentitiesarelaunchedashumanmedicinesannually.
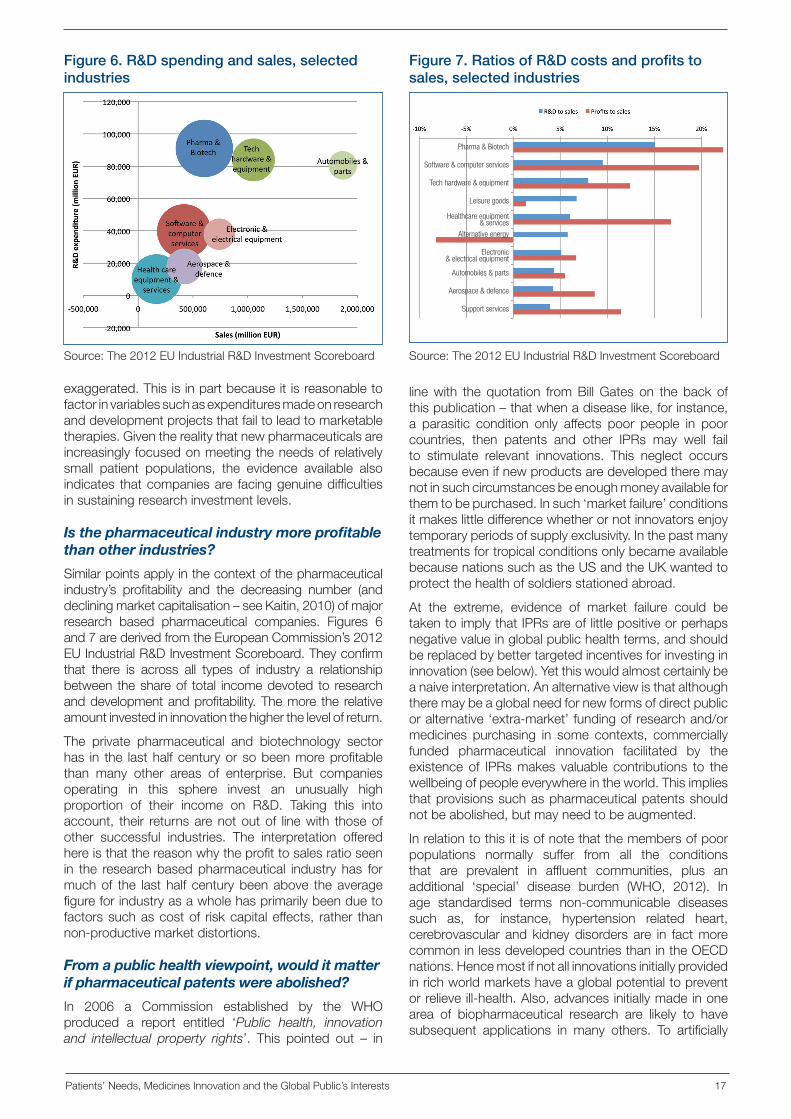
But some commentators have claimed that the ‘true’cost of pharmaceutical research is much less. Forexample,LightandLexchin (2012)suggestedthat it isin fact about $100million per product. Their figure isrelativelylowbecauseitdoesnotincludetheexpenses
Figure 4. Patient Involvement in Health Care and Research Governance and Policy Decisions
Source:TheAuthors
Market involvement through purchases of services and pharmaceutical products
and the expression of needs and preferences in health
care settings
Political involvement through voting and raising health issues
during electoral competitions, and via inputs to public debate such
as media and allied contributions, including reports and books
on personal experiences and participating in ‘third sector’
activities
Governance involvement through memberships of management groups, regulatory bodies and inquiries into untoward incidents
Research involvement
through direct contributions
to research programmes and
via advisory board and stakeholder
group memberships
Patients/health service and product consumers
and their representatives
Figure 5. New medicines approved by the FDA, 1950-2010
Source:LightandLexchin,2012

16 Patients’Needs,MedicinesInnovationandtheGlobalPublic’sInterests
incurredasaresultoffailedresearchprojectsandmakesnoallowanceforthecostsof‘riskcapital’.Thelattertermreferstothepremiumneededtoencourageinvestorstoputmoneyintoprojectswithahighchanceoffailure.
Theseauthorshavealsopointedtodataindicatingthat,notwithstandingrisingresearchoutlaysstemminginlargepartfromextendedclinicaltrialrequirements,thenumberof fundamentally newmedicines enteringmarkets likethat of the US has stayed broadly constant since the1950s(Figure5).ThistheybelieverefutesclaimsthatthepharmaceuticalsectorisfacinganinnovationcrisisandmightrequireenhancedIPRssuchaslongerperiodsofregulatorydataexclusivitytoremainviable.
From a patient and public interest perspective suchobservationsareimportant.Theysuggestthattoomuchisbeingcharged for innovativemedicines, and/or that
industry–andalsopublicandvoluntarysector10–fundedresearchcouldbemanagedmoreefficiently. (Voluntarysectororganisationsandpublicbodies likeUniversitiesoftenpossessIPrightsthatpharmaceuticalcompaniesexploit on their behalf. Hence a share of the earningsfrompharmaceuticalinnovationsisreturnedtothem.)
Bothresearchandregulatoryprocessescouldprobablybemademoreefficient.YettheconclusiondrawnhereisthatestimatesthatthedevelopmentcostsofinnovativemedicinesarenowwelloverUS$1,000millionarenot
Box 5. Incentives for meeting special needs
Conventionalapproachestomaximisingwelfaretypicallyseek to provide ‘the greatest good for the greatestnumber’. They emphasise the importance of ‘costeffectiveness’infieldssuchashealthcareprovision.Butotherconceptsofsocialjusticefocusmoreonprovidingfortheneedsoftheleastadvantagedinsociety.Hencethe‘orphandrug’legislationpioneeredinAmericainthe1980s–andsubsequentlyintroducedinplacessuchasAustralia,Japanand theEU–seeks toconferspecialadvantages on innovators who develop treatmentsfor relatively small groups of patients. These rangefrom providing support aimed at accelerating and/orminimisingthecostsofdruglicensingthroughtotheuseofregulatorydataprotection(RDP)toprovidemedicinesthathavebeendevelopedfororphanindicationswithaperiodoffreedomfromminimalcostcompetition.
Providedpurchasers(andbodiessuchaspricesettingagencies)donotattempttonegatetheimpactofsuchlegislationby, for instance,encouraging the ‘off label’(unlicensed) use of cheaper alternatives when theseareavailable,suchpoliciesbalanceshorttermmarketforceswith a considered long term understanding ofmeetinghumanneed.
Awareness of the fact that many pharmaceuticalsdevelopedforuseinadultshavebeenemployedonan‘ad hoc’basisinthetreatmentofchildrenledtosimilarlegislation in the field of paediatric medicine. In theUnitedStates,whichalsoledglobalreforminthisarea,two formsof targeted legislationpromote investmentin paediatric drug development. They are the BestPharmaceuticals forChildrenAct (theBPCA)and thePaediatricResearchEquityAct(PREA).TheBPCAwaspassed in 2002. It built on reforms first implementedin the 1990s, and allows innovators to qualify for anadditional six months of marketing exclusivity forinnovativedrugs (added to theendof thepatent life)if studies related to their role in child treatment arevoluntarily completed and submitted to FDA. ThePREA,bycontrast,requiressuchstudies.
The equivalent legislation in Europe, which wasintroduced in 2007, also adds six months to theeffectivepatentlifeofmedicinesthatareappropriatelytested and presented for use in children. There areadditional RDP provisions for off-patent medicinesdevelopedforuseinchildren.Onceagain,forthelatterarrangements to incentivise ongoing investment it isvitalthatprescribersdonotbowtopressuresuselowercostpresentations‘offlabel’.
Suchregulatoryinnovationshavehelpedtoimprovetheworkingoftheoverallpharmaceuticalmarket.Butotherproblems remain, or are emerging. For example, inrelationtochallengessuchasdevelopingmoreeffectivetreatments for cancers and other complex NCDsthere is a strengthening case for adaptivemedicineslicensing.This involvesmovingawayfromasimplistic‘on/off’approachtodecidingwhetheraninnovative(bio)pharmaceuticalproductis‘safe’or‘unsafe’,towardsacarefully phased introduction process. But for this toworkinthepublic’sbestinterestsitwillprobablyrequirean equivalently stepped approach to IPP, with eachnewstepattractinga freshperiodof targetedmarketexclusivity.
Anotherpossibleexampleofmarketfailureisthatofantibiotic development. Innovation in this field hasbeen discouraged by the fact that well intentionedprescribing policies often minimise the early useof new medicines. This allows them to be held inreserveforusewhenresistancetoestablishedanti-bacterial product means that they are no longereffective.Despitethewidelyrecognisedneedfornewantibiotics(WHO,2013)thishasparadoxicallymeantthat commercial research funders (and indirectlypublic agencies) have had little reason to invest inthisarea.ThisisbecausenewproductsareunlikelytoachievesignificantsalesuntilafterIPRexhaustion.Suchproblemshighlightthecontinuingneedtotailorincentives for therapeutic innovation to fit specificpublichealthrequirements.
10 Insomeareaspublicandcharitablyfundedinvestmentsexceedthoseofindustry.Forinstance,Kanavosetal(2010)calculatedthatintheperiodleadingupto2010inEurope,theUSandJapan,researchbasedpharmaceuticalindustryexpenditureintheoncologyfieldwas,atalittleover$3billionperannum,onlyaboutathirdofthatmadebypublicbodiessuchastheUSNationalInstitutesforHealth(NIH).Voluntarysectorspendingwasabout$900millioninthatyear.
Patients’Needs,MedicinesInnovationandtheGlobalPublic’sInterests 17
exaggerated.Thisisinpartbecauseitisreasonabletofactorinvariablessuchasexpendituresmadeonresearchanddevelopmentprojectsthatfailtoleadtomarketabletherapies.Giventherealitythatnewpharmaceuticalsareincreasingly focusedonmeetingtheneedsofrelativelysmall patient populations, the evidence available alsoindicates thatcompaniesare facinggenuinedifficultiesinsustainingresearchinvestmentlevels.
Is the pharmaceutical industry more profitable than other industries?
Similarpointsapplyinthecontextofthepharmaceuticalindustry’s profitability and the decreasing number (anddecliningmarketcapitalisation–seeKaitin,2010)ofmajorresearch based pharmaceutical companies. Figures 6and7arederivedfromtheEuropeanCommission’s2012EUIndustrialR&DInvestmentScoreboard.Theyconfirmthat there is across all types of industry a relationshipbetween theshareof total incomedevoted to researchanddevelopmentandprofitability.Themore the relativeamountinvestedininnovationthehigherthelevelofreturn.
The private pharmaceutical and biotechnology sectorhas in the lasthalfcenturyorsobeenmoreprofitablethan many other areas of enterprise. But companiesoperating in this sphere invest an unusually highproportion of their income on R&D. Taking this intoaccount, their returnsarenotoutof linewith thoseofother successful industries. The interpretation offeredhereisthatthereasonwhytheprofittosalesratioseenin the researchbasedpharmaceutical industry has formuchof the last half centurybeenabove theaveragefigureforindustryasawholehasprimarilybeenduetofactorssuchascostof riskcapitaleffects, rather thannon-productivemarketdistortions.
From a public health viewpoint, would it matter if pharmaceutical patents were abolished?
In 2006 a Commission established by the WHOproduced a report entitled ‘Public health, innovation and intellectual property rights’. This pointed out – in
linewith the quotation fromBill Gates on the back ofthispublication–thatwhenadiseaselike,forinstance,a parasitic condition only affects poor people in poorcountries, then patents and other IPRs may well failto stimulate relevant innovations. This neglect occursbecauseevenifnewproductsaredevelopedtheremaynotinsuchcircumstancesbeenoughmoneyavailableforthemtobepurchased.Insuch‘marketfailure’conditionsitmakeslittledifferencewhetherornotinnovatorsenjoytemporaryperiodsofsupplyexclusivity.InthepastmanytreatmentsfortropicalconditionsonlybecameavailablebecausenationssuchastheUSandtheUKwantedtoprotectthehealthofsoldiersstationedabroad.
At the extreme, evidence of market failure could betakentoimplythatIPRsareoflittlepositiveorperhapsnegativevalueinglobalpublichealthterms,andshouldbereplacedbybettertargetedincentivesforinvestingininnovation(seebelow).Yetthiswouldalmostcertainlybeanaiveinterpretation.Analternativeviewisthatalthoughtheremaybeaglobalneedfornewformsofdirectpublicoralternative‘extra-market’fundingofresearchand/ormedicines purchasing in some contexts, commerciallyfunded pharmaceutical innovation facilitated by theexistence of IPRsmakes valuable contributions to thewellbeingofpeopleeverywhereintheworld.Thisimpliesthatprovisionssuchaspharmaceuticalpatentsshouldnotbeabolished,butmayneedtobeaugmented.
Inrelationtothisitisofnotethatthemembersofpoorpopulations normally suffer from all the conditionsthat are prevalent in affluent communities, plus anadditional ‘special’ disease burden (WHO, 2012). Inage standardised terms non-communicable diseasessuch as, for instance, hypertension related heart,cerebrovascular and kidneydisorders are in factmorecommoninlessdevelopedcountriesthanintheOECDnations.Hencemostifnotallinnovationsinitiallyprovidedinrichworldmarketshaveaglobalpotentialtopreventorrelieveill-health.Also,advancesinitiallymadeinonearea of biopharmaceutical research are likely to havesubsequent applications in many others. To artificially
Figure 6. R&D spending and sales, selected industries
Source:The2012EUIndustrialR&DInvestmentScoreboard
Figure 7. Ratios of R&D costs and profits to sales, selected industries
Source:The2012EUIndustrialR&DInvestmentScoreboard
Pharma & Biotech
Software & computer services
Tech hardware & equipment
Leisure goods
Healthcare equipment & services
Alternative energy
Electronic & electrical equipment
Automobiles & parts
Aerospace & defence
Support services
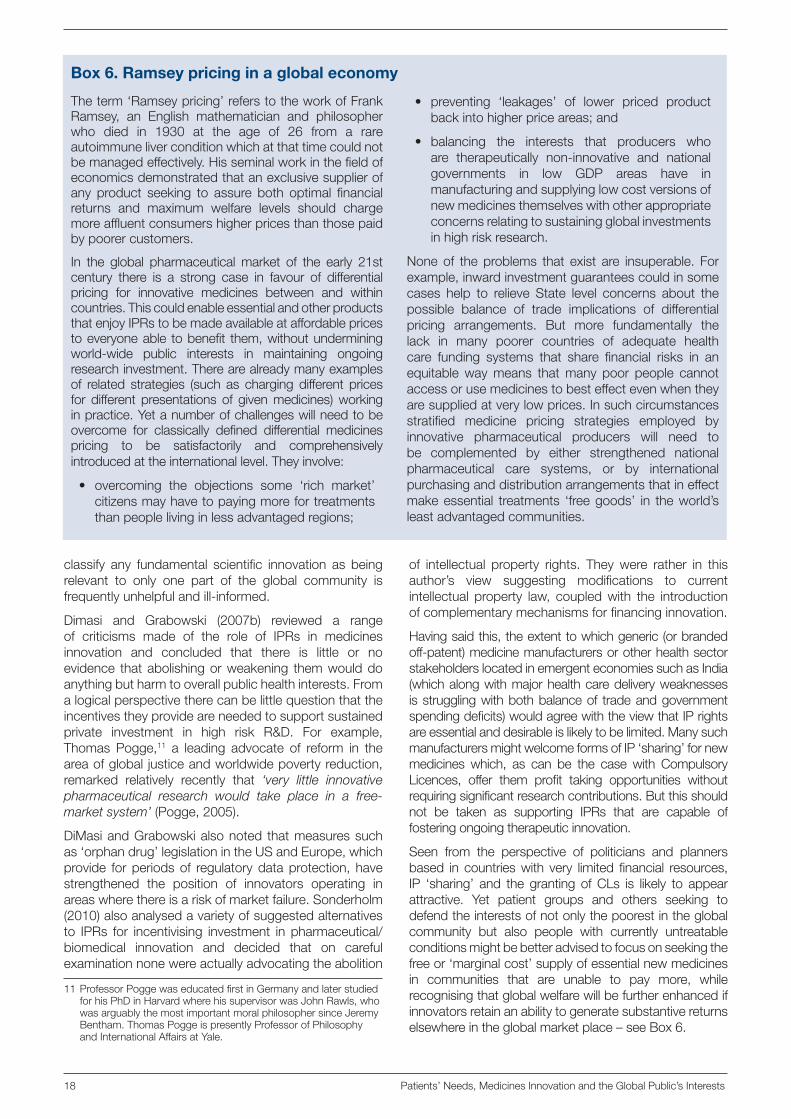
18 Patients’Needs,MedicinesInnovationandtheGlobalPublic’sInterests
classify any fundamental scientific innovation as beingrelevant to only one part of the global community isfrequentlyunhelpfulandill-informed.
Dimasi and Grabowski (2007b) reviewed a rangeof criticisms made of the role of IPRs in medicinesinnovation and concluded that there is little or noevidence thatabolishingorweakening themwoulddoanythingbutharmtooverallpublichealthinterests.Fromalogicalperspectivetherecanbelittlequestionthattheincentivestheyprovideareneededtosupportsustainedprivate investment in high risk R&D. For example,Thomas Pogge,11 a leading advocate of reform in theareaofglobal justiceandworldwidepovertyreduction,remarked relatively recently that ‘very little innovative pharmaceutical research would take place in a free-market system’ (Pogge,2005).
DiMasiandGrabowskialsonoted thatmeasuressuchas‘orphandrug’legislationintheUSandEurope,whichprovide forperiodsof regulatorydataprotection,havestrengthened the position of innovators operating inareaswherethereisariskofmarketfailure.Sonderholm(2010)alsoanalysedavarietyofsuggestedalternativesto IPRs for incentivising investment in pharmaceutical/biomedical innovation and decided that on carefulexaminationnonewereactuallyadvocatingtheabolition
of intellectual property rights. Theywere rather in thisauthor’s view suggesting modifications to currentintellectual property law, coupledwith the introductionofcomplementarymechanismsforfinancinginnovation.
Havingsaidthis,theextenttowhichgeneric(orbrandedoff-patent)medicinemanufacturersorotherhealthsectorstakeholderslocatedinemergenteconomiessuchasIndia(whichalongwithmajorhealthcaredeliveryweaknessesisstrugglingwithbothbalanceof tradeandgovernmentspendingdeficits)wouldagreewiththeviewthatIPrightsareessentialanddesirableislikelytobelimited.ManysuchmanufacturersmightwelcomeformsofIP‘sharing’fornewmedicines which, as can be the case with CompulsoryLicences, offer them profit taking opportunities withoutrequiringsignificantresearchcontributions.Butthisshouldnot be taken as supporting IPRs that are capable offosteringongoingtherapeuticinnovation.
Seen from the perspective of politicians and plannersbased in countrieswith very limited financial resources,IP ‘sharing’ and the granting ofCLs is likely to appearattractive. Yet patient groups and others seeking todefendtheinterestsofnotonlythepoorestintheglobalcommunity but also people with currently untreatableconditionsmightbebetteradvisedtofocusonseekingthefreeor‘marginalcost’supplyofessentialnewmedicinesin communities that are unable to pay more, whilerecognisingthatglobalwelfarewillbefurtherenhancedifinnovatorsretainanabilitytogeneratesubstantivereturnselsewhereintheglobalmarketplace–seeBox6.
11ProfessorPoggewaseducatedfirstinGermanyandlaterstudiedforhisPhDinHarvardwherehissupervisorwasJohnRawls,whowasarguablythemostimportantmoralphilosophersinceJeremyBentham.ThomasPoggeispresentlyProfessorofPhilosophyandInternationalAffairsatYale.
Box 6. Ramsey pricing in a global economy
Theterm‘Ramseypricing’referstotheworkofFrankRamsey, an English mathematician and philosopherwho died in 1930 at the age of 26 from a rareautoimmuneliverconditionwhichatthattimecouldnotbemanagedeffectively.Hisseminalworkinthefieldofeconomicsdemonstratedthatanexclusivesupplierofany product seeking to assure both optimal financialreturns and maximum welfare levels should chargemoreaffluentconsumershigherpricesthanthosepaidbypoorercustomers.
In the global pharmaceutical market of the early 21stcentury there is a strong case in favour of differentialpricing for innovative medicines between and withincountries.ThiscouldenableessentialandotherproductsthatenjoyIPRstobemadeavailableataffordablepricestoeveryoneable tobenefit them,withoutunderminingworld-wide public interests in maintaining ongoingresearchinvestment.Therearealreadymanyexamplesof related strategies (such as charging different pricesfor different presentations of givenmedicines)workinginpractice.Yetanumberofchallengeswillneedtobeovercome for classically defined differential medicinespricing to be satisfactorily and comprehensivelyintroducedattheinternationallevel.Theyinvolve:
• overcoming the objections some ‘rich market’citizensmayhavetopayingmorefortreatmentsthanpeoplelivinginlessadvantagedregions;
• preventing ‘leakages’ of lower priced productbackintohigherpriceareas;and
• balancing the interests that producers whoare therapeutically non-innovative and nationalgovernments in low GDP areas have inmanufacturingandsupplyinglowcostversionsofnewmedicinesthemselveswithotherappropriateconcernsrelatingtosustainingglobalinvestmentsinhighriskresearch.
None of the problems that exist are insuperable. Forexample,inwardinvestmentguaranteescouldinsomecases help to relieve State level concerns about thepossible balance of trade implications of differentialpricing arrangements. But more fundamentally thelack in many poorer countries of adequate healthcare funding systems that share financial risks in anequitablewaymeans thatmany poor people cannotaccessorusemedicinestobesteffectevenwhentheyaresuppliedatverylowprices.Insuchcircumstancesstratified medicine pricing strategies employed byinnovative pharmaceutical producers will need tobe complemented by either strengthened nationalpharmaceutical care systems, or by internationalpurchasinganddistributionarrangementsthatineffectmakeessential treatments ‘freegoods’ in theworld’sleastadvantagedcommunities.

Patients’Needs,MedicinesInnovationandtheGlobalPublic’sInterests 19
Did the TRIPS agreement stop poor communities getting access to low cost essential medicines?
TheTRIPSagreementisatopicofcontinuingcontroversy,albeit that its terms are in some instances now beingsuperseded by those of separately negotiated bilateraltrade agreements. The origins of TRIPS, which in thecontextofpatentsonpharmaceuticalsisnotduetocomeinto fulleffect in the leastdevelopednationsuntil2016,datebacktothe1980sandaGeneralAgreementonTariffsandTrade (GATT– the forerunnerof theWTO)meetingheld in Uruguay. It was during the so-called ‘Uruguayround’thatitwasagreedthatallmembernationsshouldmove towardsgrantingpatentswith thesame termsofprotectionasthoseexistingin‘thedevelopedworld’.
This ledon to in1994 theWTOAgreementonTrade-Related Aspects of Intellectual Property Rights. India,for example, signed the TRIPS agreement when itelectedto jointheWTOin1995.Thiswaswithaviewto it coming into full effect in 2005, the year inwhichanewPatentActwas introduced in that country. TheglobalpharmaceuticalindustryandthegovernmentsofcountriesliketheUSandtheUKsupportedtheTRIPSapproach (Abbott, 2009). It extended ‘the western concept of intellectual property (IP) to developing countries. Members of the WTO…. have had to adopt a patent system…. that would allow product and process patents for pharmaceuticals and vaccines’ (MilstienandKaddar,2006).
Many observers saw this as a desirable raising of IPprotection standards to a global ‘best practice’ level.The proponents of the TRIPS agreement believedthat itwouldopen theway to increased investment inemergenteconomiesandmoretradingbetweenpoorerandrichercountries,whileatthesametimeprotectingglobalpatientinterestsincontinuinginnovation.ThereisresearchevidencethattheintroductionofstrengthenedIP protection correlates positively with inward capitalinvestment levels (Pugatch et al, 2012). But for thecritics of TRIPS it threatened an inappropriately earlyintroductionofadvancedstandardIPRsintoeconomiesthatdonotasyethavetheresearchandalliedcapacitiestocompetewithmoredevelopednations.
Somehavetermedsuchdevelopments‘kicking away the ladder’ (Chang,2002).TheprominentAmericanwelfareeconomistJeffreySachshascommentedthat:‘We were proposing, in a sense, that the rest of the world be made safe for American ideas, as they adopted intellectual property rights that gave patent protection to our very innovative economy.’
Thereareobviouswelfarehazardsthatcouldarisefrommoves that reinforce the power and position of richernationsasagainst theirpoorerpartners.Nevertheless,increased international tradingsincethestartof1990sappears to have been associated with a closing ofaveragenationallivingstandardsacrosstheglobe.Therehavealsobeenmorerapidincreasesinlifeexpectancyin less affluent communities as compared to matureindustrial economies, even though cutting infant and
childmortalityisadifferenttaskfromthatofpromotinghealthyageingand improvingagespecificsurvivalandfreedomfromdisabilityinlaterlife.
However, TRIPS was agreed before concerns aboutaccesstoeffectiveHIVtreatmentshadfullymaterialised.In the face of the at that time growing concerns thataccess tonewHIV treatmentswouldbe further limited,aMinisterialConferenceheldinDohain2001‘reaffirmed the principle that TRIPS does not and should not preventcountries from taking measures to safeguard public health’ (MilstienandKaddar,2006).Awaiverwasagreedto the effect that ‘the scheme ultimately negotiated…..envisioned a process of back-to-back compulsory licences that would enable any country needing medicines at lower prices than those charged by local patentees to seek assistance from others able and willing to produce the drugs for export purposes, without interference from the patentee in either country’ (Reichman,2009).
This view of the resultant Doha declaration suggeststhatcountriesthatjudgethattheirpopulationsareatriskbecauseaninnovativemedicineistoocostly12canissuea Compulsory License (CL) for its local manufacture,and also export the CL version of the medicine inquestion to other nations in a similar position. Yetcommentatorsconcernedwiththefinancialsustainabilityof pharmaceutical innovation argue that there is adanger of ‘public health emergencies’ being definedsobroadlyas to justifyCLsbeinggrantedagainstanymedicine of any type, regardless of whether or notthis would in practice mean better outcomes for lessadvantagedconsumers.Coupledwithfactorssuchthelowlevelofroyaltiestypicallygrantedtoinnovatorsandfears–justifiedornot–thatlowcostcopiesofpatentedmedicinesmightbesuppliedinaffluentmarketsorusedtotreat‘medicaltourists’,thishasraisedconcernsthattheworld-wideintellectualpropertysystemisindangerofbeingseriouslyunderminedbytheinappropriateuseofCLgrantingpowers.
Thereisariskofoverstatingsuchhazards,giventhattwothirdsoftheglobalpharmaceuticalmarketbyvaluestilllieswithintheNorthAmerica,theEUandJapan.Thereisalsoariskofexaggeratingtheirimportance,giventhecontinuing reality that 1-2 billion of theworld’s peoplestill lack consistently adequate access to essentialmedicines.Butinseekingtoreconcileconflictingpublicand patient interests in optimising present accessto medicines while sustaining investment in futuretherapeutic improvements the view suggested here isthatitwouldbedesirableiftheWTO,wherepossibleinconsultationwith patient representatives and agenciessuchastheWHO,couldestablishagenerallyacceptedsupra-national mechanism for defining ‘public healthemergencies’ and determining when IPP treatmentsfornon-communicabledisorderssuchas,for instance,cancersshouldbemadeuniversallyaccessible.
12Rememberingthatwellover90percentofallmedicinesontheWHO’sessentialdruglistareoffpatent,andthatinthepoorestpartsoftheworldasignificantproportionofnewmedicineshavetodatebeenneitherregisterednorcoveredbyactivelyenforcedIPRs.Thisleavesthefieldopenfornon-originalsupplierstoofferalternativeproductsasandwhentheyareavailable.
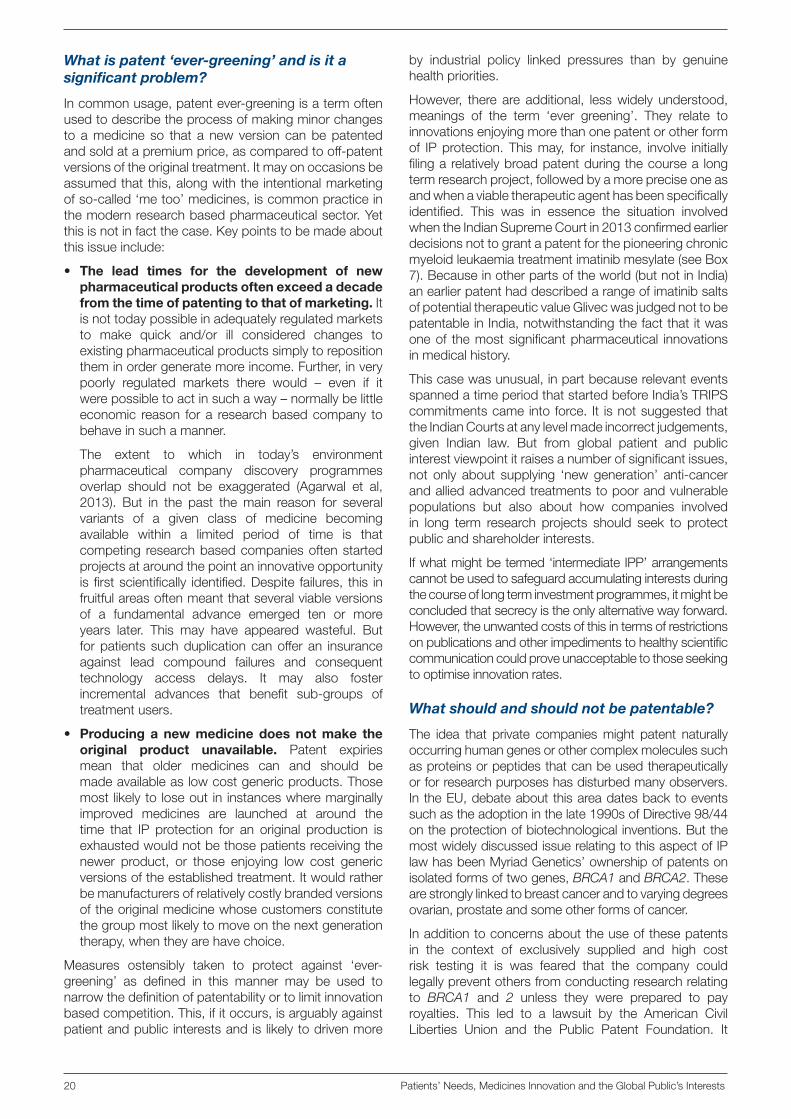
20 Patients’Needs,MedicinesInnovationandtheGlobalPublic’sInterests
What is patent ‘ever-greening’ and is it a significant problem?
Incommonusage,patentever-greeningisatermoftenusedtodescribetheprocessofmakingminorchangesto amedicine so that a new version canbepatentedandsoldatapremiumprice,ascomparedtooff-patentversionsoftheoriginaltreatment.Itmayonoccasionsbeassumedthatthis,alongwiththeintentionalmarketingofso-called‘metoo’medicines,iscommonpracticeinthemodernresearchbasedpharmaceuticalsector.Yetthisisnotinfactthecase.Keypointstobemadeaboutthisissueinclude:
• The lead times for the development of new pharmaceutical products often exceed a decade from the time of patenting to that of marketing.Itisnottodaypossibleinadequatelyregulatedmarketsto make quick and/or ill considered changes toexistingpharmaceuticalproductssimplytorepositiontheminordergeneratemoreincome.Further,inverypoorly regulated markets there would – even if itwerepossibletoactinsuchaway–normallybelittleeconomic reason fora researchbasedcompany tobehaveinsuchamanner.
The extent to which in today’s environmentpharmaceutical company discovery programmesoverlap should not be exaggerated (Agarwal et al,2013). But in the past themain reason for severalvariants of a given class of medicine becomingavailable within a limited period of time is thatcompeting researchbasedcompaniesoftenstartedprojectsataroundthepointaninnovativeopportunityisfirstscientifically identified.Despite failures, this infruitfulareasoftenmeantthatseveralviableversionsof a fundamental advance emerged ten or moreyears later. This may have appeared wasteful. Butforpatientssuchduplicationcanofferan insuranceagainst lead compound failures and consequenttechnology access delays. It may also fosterincremental advances that benefit sub-groups oftreatmentusers.
• Producing a new medicine does not make the original product unavailable. Patent expiriesmean that older medicines can and should bemadeavailableaslowcostgenericproducts.Thosemost likelyto loseout in instanceswheremarginallyimproved medicines are launched at around thetime that IP protection for an original production isexhaustedwouldnotbethosepatientsreceivingthenewer product, or those enjoying low cost genericversionsoftheestablishedtreatment.Itwouldratherbemanufacturersofrelativelycostlybrandedversionsoftheoriginalmedicinewhosecustomersconstitutethegroupmostlikelytomoveonthenextgenerationtherapy,whentheyarehavechoice.
Measures ostensibly taken to protect against ‘ever-greening’ as defined in this manner may be used tonarrowthedefinitionofpatentabilityortolimitinnovationbasedcompetition.This,ifitoccurs,isarguablyagainstpatientandpublic interestsandis likelytodrivenmore
by industrial policy linked pressures than by genuinehealthpriorities.
However, there are additional, lesswidely understood,meanings of the term ‘ever greening’. They relate toinnovationsenjoyingmorethanonepatentorotherformof IPprotection.Thismay, for instance, involve initiallyfilingarelativelybroadpatentduringthecoursea longtermresearchproject,followedbyamorepreciseoneasandwhenaviabletherapeuticagenthasbeenspecificallyidentified. This was in essence the situation involvedwhentheIndianSupremeCourtin2013confirmedearlierdecisionsnottograntapatentforthepioneeringchronicmyeloidleukaemiatreatmentimatinibmesylate(seeBox7).Becauseinotherpartsoftheworld(butnotinIndia)anearlierpatenthaddescribedarangeofimatinibsaltsofpotentialtherapeuticvalueGlivecwasjudgednottobepatentableinIndia,notwithstandingthefactthatitwasoneof themostsignificantpharmaceutical innovationsinmedicalhistory.
Thiscasewasunusual,inpartbecauserelevanteventsspannedatimeperiodthatstartedbeforeIndia’sTRIPScommitmentscameintoforce. It isnotsuggestedthattheIndianCourtsatanylevelmadeincorrectjudgements,given Indian law. But from global patient and publicinterestviewpointitraisesanumberofsignificantissues,not only about supplying ‘newgeneration’ anti-cancerandalliedadvancedtreatmentstopoorandvulnerablepopulations but also about how companies involvedin long term research projects should seek to protectpublicandshareholderinterests.
Ifwhatmightbetermed‘intermediateIPP’arrangementscannotbeusedtosafeguardaccumulatinginterestsduringthecourseoflongterminvestmentprogrammes,itmightbeconcludedthatsecrecyistheonlyalternativewayforward.However,theunwantedcostsofthisintermsofrestrictionsonpublicationsandotherimpedimentstohealthyscientificcommunicationcouldproveunacceptabletothoseseekingtooptimiseinnovationrates.
What should and should not be patentable?
The idea that private companiesmight patent naturallyoccurringhumangenesorothercomplexmoleculessuchasproteinsorpeptidesthatcanbeusedtherapeuticallyorforresearchpurposeshasdisturbedmanyobservers.IntheEU,debateaboutthisareadatesbacktoeventssuchastheadoptioninthelate1990sofDirective98/44ontheprotectionofbiotechnologicalinventions.ButthemostwidelydiscussedissuerelatingtothisaspectofIPlawhasbeenMyriadGenetics’ownershipofpatentsonisolatedformsoftwogenes,BRCA1andBRCA2.Thesearestronglylinkedtobreastcancerandtovaryingdegreesovarian,prostateandsomeotherformsofcancer.
Inadditiontoconcernsabouttheuseofthesepatentsin the context of exclusively supplied and high costrisk testing it is was feared that the company couldlegallypreventothersfromconductingresearchrelatingto BRCA1 and 2 unless they were prepared to payroyalties. This led to a lawsuit by the American CivilLiberties Union and the Public Patent Foundation. It
Patients’Needs,MedicinesInnovationandtheGlobalPublic’sInterests 21
claimed thatMyriad’spatentswere invalid in that theycould hinder biomedical research and impair patients’access todiagnostic testing,andso topotentially life-savingmedicalinterventions(Chuang&Lau,2010).
Early in 2013 an Australian Federal Court judgementfavoured Myriad Genetics’s case. However in June2013 the US Supreme Court ruled against Myriad’spatentsontheisolatednaturalgenes,whilstconfirmingthe patentability of artificially synthesised ‘cDNA’ andother ‘manmade’biologicalsubstances.Althoughthisdoes not remove all concerns surrounding intellectualproperty rights for products such as monoclonalantibodiesproducedbyrecombinantDNAtechniques,itprovidessignificantassurancethatIPRscannotbeusedto inhibit fundamental research.An increasing numberofnewtherapiesarebiopharmaceuticals.It isthereforeimportant from a consumer perspective important toinsurethatlegalmechanismsoperateappropriately,andallow for legitimate income generation by innovatorswithout blocking ongoing discovery processes orimposingunduecostsonpatientsorservicefunders.
Kent (2006) has underlined the fact that the BRCA1and 2 debate has in a number of important respectsbeenaspecialcase,andthatevenbeforetheSupremeCourtrulingresearchhasnotinthemainbeenimpededby patent holders seeking to prosecute investigatorsfor (non-commercial) infringements of IP rights. He,alongwithmany other commentators concernedwithenhancing patient welfare, concluded that – despitea potential for abuse – when properly used IP rightsare a necessary component of innovative health careenvironments.13
Whenknowledgecanbeappliedvianovelinterventionstoachievedefinedpracticalendsthere isgoodreason
Box 7. Meeting the needs of people with Chronic Myeloid Leukaemia (CML)
Chronic myeloid (or myelogenous) leukaemia is aform of ‘white cell blood cancer’ that is normally –but not always – associated with the ‘Philadephiachromosome’.The latterwasdiscovered justover50yearsagoinlaboratoriesintheUScityofPhiladelphia.It occurs as the result of an abnormal translocation(misplacement)ofgeneticmaterialduringcelldivision,which inappropriately ‘switches on’ a further cellreplication signal. Understanding the mechanismsinvolved in thisprocesswasan importantstep in thebuildupofknowledgeaboutthecausesandnatureofcancers thathasaccompaniedwhatonoccasions ismisleadingly seen as the fragmenteddevelopment ofanti-cancerdrugssincethe1950s.
Theintroductionofimatinibmesylate(GleevecorGlivec–seemaintext)asatreatmentforCMLfourdecadesaftertheidentificationofthePhiladelphiachromosomewas a milestone in the history of medicines. Usedconsistently inthemanner intendedby itsoriginators,this medicine can extend the lives of many peoplewithCMLforadecadeormore.However,asignificantnumberofpatientsmissormiss-timetheirmedicationdoses(inpartbecauseofadesiretocontrolsideeffects,theoccurrenceofwhichmaybethoughttobeevidenceoftreatmentbeing‘toopowerful’)andareconsequentlyexposedtoagreatlyincreasedriskofdrugresistance.Alternative medicines are now available which arestartingto‘blockoff’resistancepathways.Buttheydonotasyetofferdefinitivesolutionstothisproblem.
One way of further helping to meet CML and otherpatients’ needs is therefore to establish ‘adherencesupport’programmesasanintegralpartoflaterstagedrugresearchdevelopment.Itisalsovitallyimportanttofacilitatetheearlyandaccuratediagnosisofconditionslike cancers, alongside timely access to correctlyprescribed treatments. In countries like the US and
UKtheincidenceofCMLisalittleover10permillionpopulation and the mean age of diagnosed onsetis approaching 65 years. In India the best availableresearchsuggestsasimilarpicture(Dikshitetal,2011).Yet some sources claim that there is amean age ofCMLonsetofonly40years,andanoverall incidencerateofaround40permillioninIndia’srelativelyyoungpopulation.
Discrepancies like these underline the fact that thereareoftenuncertaintiesabout the levelofunmetneedfor innovative medicines in developing communities.In India executives working in Novartis, the researchbased pharmaceutical company responsible forGlivec’s original development, believe that its freesupplyscheme(whichiscurrentlyservingover15,000people–Shahani,2013)ismeetingtherequirementsofthegreatmajorityofIndianswithaconfirmeddiagnosisofCMLwhoareunabletoaccesstreatmentviaotherroutes.Theyemphasisetheneedtoincreaseaccurateandearlydiagnosisrates.Yetotherobserversappearto believe that there are large numbers of peoplewho are not being well cared for, primarily becauseof inadequatemedicines supply.This they suggest isdespite the Novartis scheme and the long standingavailabilityoflowcostversionsofimatinibmesylateontheIndianmarket.
Withoutpopulationwide-accesstoadequatediagnosticservicesandchecksas towhetherornotsuggestedtreatmentsareinfactneeded,assessingtheextenttowhichpatientsarebeingunder (orover)medicated ishighlyproblematic.Achievingbetteraccesstoeffectivemedicines is important.Yetpatientorganisationsandother agencies concerned with meeting health careneedsshouldbeawarethatsimplysupplyingmedicinesdoes not guarantee their appropriate use in complexcontextslikeCMLtherapy.
13 ItcouldbearguedthatCubaoffersanexceptiontothisrule,inthatinthecontextofmedicinesandvaccinesithasachievedarelativelyrobustinnovativerecordintheabsenceofconventionallydefinedIPrights.However,inmarketeconomiesIPrightsservetolimittemporarilytheimpactsofunfetteredcompetition.IncommunistCuba,whichhashistoricallyenjoyedamedicallywellinformedleadershipandacommandapproachtoeconomicdevelopment,suchprotectionhasnottodatebeenrequired.Thisisbecauseitscommandbasedeconomyhaslargelyoperatedoutsidethemorecompetitivelybasedglobalsystem.

22 Patients’Needs,MedicinesInnovationandtheGlobalPublic’sInterests
to conclude that it is in the public’s interest that theresultant technologies should be granted IPRs. Butundefinedrestrictionsontheuseofnaturalphenomenaby scientists in attempts to understand the worldaround them and develop new products with usefulapplications should not be accepted. (See also, forinstance, theNuffieldCouncil onBioethics,2002.) ForthepurposesofthisanalysisakeyfindingtohighlightisthatalthoughIPRsmayonoccasionshavebeenputtocounter-productiveuses, thisdoesnotmeanthat theyare inherently undesirable. What ultimately matters istheendbeingpursuedand,asinotherareas,arobustpolicyunderpinningforlegalprovisions:‘a patent is not a goal in itself, rather it is a right created…. as a means to achieve a larger social goal’ (Trotter,2012).
Are new forms of intellectual property protection needed?
As already noted, the measures contained in the USOrphanDrugsActpassedatthestartofthe1980sandthe subsequent provisions introduced in Europe andelsewherehaveservedtoreinforcetraditionalIPRswithadditional regulatory data based forms of protection.Similar approaches havebeen adopted in the contextof paediatric (child) medicine development. There aredifferences between the strategies employed in theUS, theEUandJapan.But typically thearrangementsintroduced have permitted medicines developedfor orphan indications 10 years of ‘data exclusivity’,independentlyofanyotherentitlements.
This means that regulators cannot approve newmarketingapplicationsforinnovative‘orphan’productsduringtheregulatorydataexclusivityperiodgrantedtoencourageinnovationonthebasisofpre-existingsafety
andefficacyinformation.Similarly,inboththeUSandtheEUconductingpaediatrictrialsonamedicineformulatedtobefitforpurposecanextendtheperiodofexclusivityavailableonall protectedpresentationsof the relevantactive ingredient(s) for aperiodof sixmonths. Fromapatient and public interest perspective concerns andissuesofspecialnoteinthiscontextinclude:
• the introduction of such measures reflects anacceptancewithintheworld’sstrongereconomiesthatformsofexclusivityoverandabovethoseassociatedwith conventional patenting are necessary for themaintenanceofpharmaceuticalinnovation;and
• incentives like thoseoutlinedaboveareof no valueto innovators and ultimately to meeting patients’long term requirements if purchasers fail to buyappropriately licensed products once they areavailable,on thegrounds– forexample– that theyaremoreexpensivethanalternativeversionsthatcanbe used ‘off licence’. This underlines the need forcoherentpoliciesandpracticeswhichrespectthefullrange of public interests involved in pharmaceuticalsector regulation, and do not just focus on costminimisation.
Similarpointsapplytotheprotectionofpatients’interestsindevelopingnewclinical uses formature (established,off-patent) medicines. Innovative pharmaceuticals oftenhave more than one potential therapeutic application,but at the time of initial marketing have normally onlybeen developed forwhatwas at the time regarded asthe clinically most important (and/or most financiallyviable)use.Onebarriertodevelopingtwoormoreinitialindicationsearly inadrug’s lifecycle is that ifmarkedlydifferentdosesarerequiredtogenerategivenmeasureofhealthgainpricingcomplicationsmaywellensue(Box8).
Box 8. Different prices for different uses of the same medicine?
There is evidence that chargingdifferent amounts forthe samemedicine in richer andpoorer communitiescan,althoughsometimescontroversial,beintheglobalpublic’s interest. In some circumstances chargingdiffering sums for a given medicine when it is usedin different clinical contexts may also be beneficial.However, the justification for this is often difficult forobservers such as politicians andmedical and otherprescriberstoaccept.Itrelatestothefactthatthemainvalueofinnovativemedicinesdoesnotlieinproducingthesubstancesofwhichtheyaremade,butrather inthecostsandchallengesoftheirdevelopmentandthebenefitsconferredonusers.
As described in the main text, newly identifiedpharmaceutical treatments frequentlyhavemore thanonepotential application.But the resources availableoftenallowonlyresearchontheclinicallymostimportantand/or commerciallymost promising indication to betaken forward. Alliedwith this, innovators sometimesfear that if the drug volumes needed to generate agivenunitbenefitaresignificantlydifferentincontrastingtherapeuticsettings(orifthenumbersofpatientswithoneconditionaremuchmoreor lessthanthosewith
another) this will lead to pricing problems. In today’sregulatory environment the clinical research costs ofdevelopingeachseparateindicationforamedicinearelikelytobebroadlysimilar.Yetvariationsinthevolumesof active ingredient neededmaymean that the pricepergramofdrug suppliedwould (at leastduring theperiod before IPR expiry) have from an economicperspective to vary by several orders of magnitudebetweencontexts.
It is not inpatients’ or thepublic’s long term interestthat factors like these should impede innovation.Progress inorphanandpaediatricdrug licensinghasstarted to resolve such difficulties. Yet in other areasinvolving possible second and subsequent usesof established medicines problems remain. Whenconfrontedwithdifferentpricesforthesamemedicineprescribersandothersmaywellfeelthatanattemptisbeingmadetodefraudhealthcarefunders.Giventhissituation,patients’organisationscouldinfutureseektounderstandandexplainthisfieldtodoctors,managersand others responsible for making and influencingprescribingandallieddecisions.

Patients’Needs,MedicinesInnovationandtheGlobalPublic’sInterests 23
Likewise,oncemedicineshavebecomeavailableaslowcostgenericsthiscanbeamajorbarriertodevelopingnew clinical trial validated indications for them, eventhough ‘second use’ patents or other forms of IPRare in theory already available. As suggested above,some purchasers see paying significantly above thecommodity level for an ‘old’ drug as being at bestunnecessary and at worst wasteful. A message tostressfromthestandpointofpatientswhowouldbenefitfrom the development of new indications for ‘mature’medicinesisthat,overandaboveIPRbasedincentivesbeingnominallyinplace,researchinvestorsarelikelytorequirerobustreassurancesthattheywillinpracticebeabletoestablishincomestreamsadequatetojustifytheinvestmentdecisionsneeded.
Thepublic’s interest inprovidingthe latterrestsonthedesirabilityofstimulatingfuturespendingonproductiveinnovations.There isacase for the future introductionofstrengthened formsof IPprotection forsecondandsubsequent uses of off-patent drugs, designed tobuild on and extend incentives alreadyprovided for inthecurrentorphanandpaediatricmedicineslegislation(Jacob,2013).TheextenttowhichfurtheradjustmentsinthescopeanddurationIPRsformedicinesandalliedproductsmightbebothjustifiedandpoliticallypossibleistouchedonagainlaterinthisreport.Buttheconclusiontostresshereisthatalthoughgovernmentsmayimposepricecontrolsonpharmaceuticalswiththeobjectiveofcurbingcosts,14thereisfromapatientandglobalpublicinterest standpoint a counterbalancingneed to ensurethatspendingondeveloping innovativetechnologies isnotundulyrestricted.
Could and should the financing of biopharmaceutical research be completely separated from the commercial sale of medicines?
There are many other patient and public interestquestions to be asked about the interfaces betweeninnovation, IP law and medicines pricing, quality,safetyandaccessin,forinstance,areaslikemedicinescounterfeiting.Yetasfarasthisreportisconcernedthemostimportantissuesrelatetotheoptionsavailablefordelinkingresearchfundingfromthecommercialmarketplace.While forreasonsalready indicatedtheabolitionof patents and other IPRs is unlikely to offer a viablewayforward,reducinginnovator’sfinancialdependenceon IPR exploitation may be desirable in somecircumstances.Opening specific new funding streamscan – as the Gates Foundation has demonstrated infields such as malaria medicines development – offervaluableadditions toglobal investment inmedicalandpharmaceuticalinnovation.
The performance of the regulated, mixed public andprivate market for pharmaceuticals that in its currentformdevelopedintheUSandEuropeintheaftermathofthe1939-46war,has–asindividualssuchasBillGateshaveemphasised–beenrobustasfarastheimmediateinterests ofmost people in the developedworld havebeen concerned. But for others in poorer developingregions there is still a need for further improvement.Thetaskaheadisnottodismantlearrangementswhichhave delivered to good effect in more advantagedenvironments.Itisrathertocreateanextendedsystemthatismorecapableofmeetingtheneedsofrichworldminorities together with the particular requirements ofpopulationsinlessdevelopedeconomies.
WithrespecttothisdebatetheWellcomeTrusthasrecentlyproducedstatementsthathighlightthepositiveroleplayedbyIPRs,andwarnagainstremovingthebenefitsofmarketcompetitioninthemedicinesresearchanddevelopmentfundingprocess.(See,forexample,WellcomeTrust,2012,2013). Inpractical termscommerciallydrivenprocessesare often of value in pushing forward innovations, andencouragingtheiruptakeviamarketingandproductandservicesupportactivities.
However,JamesLoveandotherreformadvocateshavesuggested the introductionof prizes to encourage thedevelopment of new medicines in high priority fields(Love and Hubbard, 2007; Stiglitz 2006a, 2006b;Vastag2012.)ThisconceptcanbedatedbacktoandbeyondinitiativessuchastheBritishAdmiralty’seffortsintheearly1700stoincentivisethecreationofareliablenautical clock to aid navigation. This was a notablesuccess,albeitthatonthatoccasionthepromisedprizewasnotpaiduntil itswinnerJamesHarrisonwasveryclosetobankruptcy.
There is a logical case supporting the view that anextendeduseofprizesfortheintroductionofsuccessfultreatmentscouldinsomeareasusefullyaugmentresearchfundingarrangements.Butincomplexandfastevolvingfieldsthereisadangertheymaylacktheflexibilityneededtomaintaintheirrelevancetochangingpublicandpatientneeds.Theextenttowhichsuchanapproachcouldbescaledupbeyondtheoccasional ‘once-off’ level isalsouncertain,andthereisnoevidencetosuggestthataprizebasedapproachcouldeverfullyreplaceexistingIPRs.
Examplesofrelatedconceptsinclude:
• Pogge and Hollis’s Health Impact Fund (HIF).Thiswould,ifintroduced,offerpharmaceuticalinnovatorsanopportunitytoregistertheirproductswithacentralFundandtoreceiveafinancialrewardcommensuratewith the projected world-wide benefits generated,in return for supplying at the cost of productionwhereverthetreatmentinquestionisneeded(Hollis,2008). Thismay be seen as a variant of Love andHubbard’sproposals, coupledwitha formof ‘valuebasedpricing’.Fromatheoreticalperspective ithasanumberofattractiveaspects,albeitthatinpracticaltermsthelevelofrewardrequirementsandthemostappropriate timingofpaymentsduemaybedifficulttodetermine.
14Pricecontrolscanhaveundesiredconsequencesasaresultofmarketdistortions.Forexample,genericmanufacturersseekingincreasedreturnsmaystopmakingessentialmedicinesifthepricelimitsimposedareundulylow,andfocustheiractivitiesinotherlessimportantareas.Abetterapproachistowhereverpossiblefostercompetitionviainformedmedicinespurchasingandgoodprescribing.
24 Patients’Needs,MedicinesInnovationandtheGlobalPublic’sInterests
• Advanced Market Commitments.AMCs typicallyinvolve public agencies agreeing to purchase givenvolumesofproductssuchasnewdrugsorvaccinesataguaranteedpricefromcompaniespreparedtofundthe research programmes needed to develop them(Glennersteretal,2006,Sonderholme2010c.)AMCsalsohaveasimilarbutmorespecificallytargetedroletothatofdrugdevelopmentprizeoffers.
Additionalideasrangefromtheestablishmentofpatentpoolstofacilitateresearchinneglecteddiseaseareasthrough to thepossibility thatgovernmentscould inselectedsituations‘buyout’patentsorotherIPRsandtheneitherencouragefree‘priceplusquality’basedgeneric competition, or commission local or globalproducerstosupplyinbulkatthelowestsustainablecost.A largebodyof literatureontheviability theseandotheropportunitiesexists.Butforthepurposesofthisstudykeyobservationsinclude:
• A fundamental question at the heart of the present IP debate relates to the extent to which poorer countries should have a ‘free ride’ with regard to funding pharmaceutical innovations.AuthorssuchasPoggehavearguedthatmoreaffluentnationsshouldbepreparedtopermitthemsuchanadvantage.Others,suchasSonderholme(2010b),havepointedoutthatthecurrentcostofprivatepharmaceuticalresearchinthedevelopedworldisabout$70billionperannumandthatthebalanceofworldeconomicpowerisshiftingawayfromEuropeandperhapstheUS.Insuchcircumstancesthepolitical/socialwillneededtomovesignificantlyfurtherinthedirectionoftheOECDeconomiesbeingtheexclusivefundersofhighrisk pharmaceutical research may prove lacking, otherthaninveryparticularinstancesofspecialneed.
• In the absence of strong intellectual property rights, governments and other agencies may markedly under-estimate the full value of biopharmaceutical and other medical innovations in the face of immediate political priorities like keeping taxes low.Thiscouldleadtomajorlongtermwelfarelosses.SomepublicconflictsoveraccesstoIPprotectedmedicinesmayreflectinstitutionalpurchasers’unwillingness to pay premium prices for innovations,even incircumstanceswherebothpublicopinionandlongtermeconomiclogicmayinfactfavouruse.
In a variety of countries ongoing political concernsaboutanti-cancerdrugaccessandefficacyillustratethisproblem.Ithasbeenestimatedthatthecapitalisedvalueofbeingabletoeffectivelytreatallcancerscouldbeintheorderof$50,000billionintheUSalone(MorphyandTopel,2006).That issome50 times thecurrentworldannualconsumptionofallpharmaceuticals.Aspectsofmethodology underpinning this and similar estimatesmay be questioned. Yet they underline the potentialimportance of further biomedical advances, not onlyin oncology but areas such as, say, the prevention ofneurologicalandmusculoskeletaldisorders.Theultimateworthofsustainedinvestmentinareasliketheseislikelytofarexceedthevalues impliedbyfragmented‘healtheconomic’calculationsmadetoinformshorttermhealthsectorresourceallocationdecisions.
Patient Centred Progress
A central message of this report is that successfullyfostering medicines and wider health care innovationwhile pursuing national and international patient andpublicinterestsintheimproveddeliveryofcareislikelytorequirecoordinatedeffortonawidevarietyoffronts.Both new medicines development and establishedtreatmentaccessissuesneedtobeunderstoodintheirbroad social and economic contexts, rather than asisolatedchallenges.
The extent to which provisions like IPRs protect ornegatelocaland/orglobalpublicinterestsisnotsimplya function of variables such as patent termdurations.It isdeterminedby interactionsbetween the latterandfactorssuchasthedegreetowhichhealthcarefundingarrangementspermitfinancialrisksharingandsoassureuniversalcaredelivery.Withoutrobust,welldesignedandregulated public or private health care systemswhichprotectagainstcatastrophichealthcarecostsfallingonindividualsand familiesnopopulation,affluentorpoor,can be assured consistent and equitable access tomodernhealthcaretechnologies(Wong-Reiger,2013).
Otherkeyvariablesrangefromtheexistence(orotherwise)of efficient pharmaceutical purchasing systems to thewaymedicinespricingschemesare implemented,andthequalityofgovernance inbothpubliclyandprivatelyfundedresearchinstitutions.Thenatureofinternationalagreements on aid and trade relating to productslike diagnostics, vaccines and medicines is anotherimportant consideration. Bodies representing patientand public interests in health and health care haveresponsibilitiesrelatingtoallthesefields,andmanymorebesides.However,thetopicsbrieflydiscussedbelowareparticularlyrelevanttomedicinesusersconcerns’abouttreatment costs and the degree to which innovatorscanforlimitedperiodsbeprotectedfromtheeffectsofuncheckedmarketcompetitionwithoutharmingpublicinterestsinaffordablecaredelivery.
Ensuring safety without impeding innovation
In the half century since the Thalidomide tragedy,whichat thestartof the1960scaused10,000babiesto be borne with physical impairments, sophisticatedsystems of medicines safety regulation have beenestablished to protect populations across the world.Few commentatorswould question the importance ofsuch advances. But for people facing serious illnessand/or premature death, taking even highly significanttherapeutic risks is not necessarily unacceptable. It isalsonotautomaticallythecasethatcurrentapproachesto regulating thepharmaceutical sector ingeneral andmedicinessafetyinparticularwillbeeithereconomicallyefficient(notleastasjudgedbytheHTAcriteriausedbybodiessuchasGermany’s IQWiGorBritain’sNICE)orcommensuratewiththeamountsofspenttoreducetherisksofharminotherareas.
Fromaglobalpublic interestperspective, for instance,it is relevant to observe that – as compared with theavoidableharmcausedbyThalidomideoutsidetheUS,
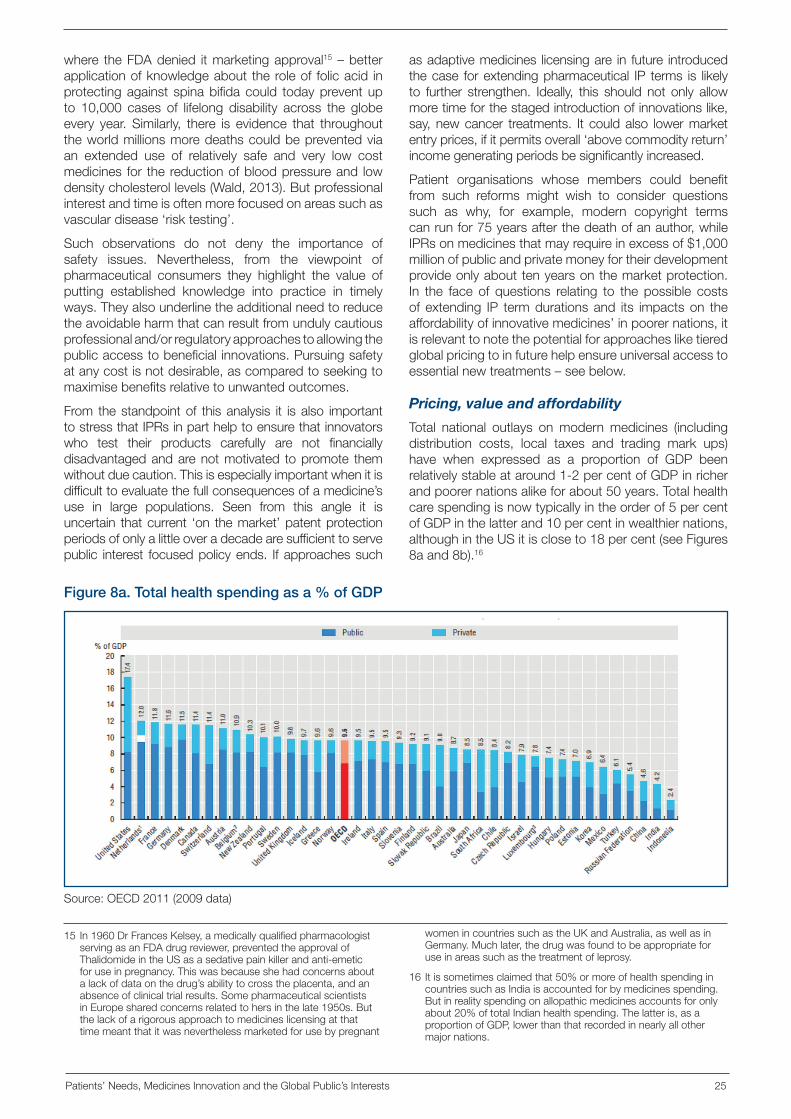
Patients’Needs,MedicinesInnovationandtheGlobalPublic’sInterests 25
where theFDAdenied itmarketingapproval15–betterapplicationofknowledgeabout theroleof folicacid inprotectingagainst spinabifidacould todaypreventupto 10,000 cases of lifelong disability across the globeevery year. Similarly, there is evidence that throughouttheworldmillionsmoredeathscouldbepreventedviaan extended use of relatively safe and very low costmedicines for thereductionofbloodpressureand lowdensitycholesterollevels(Wald,2013).Butprofessionalinterestandtimeisoftenmorefocusedonareassuchasvasculardisease‘risktesting’.
Such observations do not deny the importance ofsafety issues. Nevertheless, from the viewpoint ofpharmaceutical consumers they highlight the value ofputting established knowledge into practice in timelyways.Theyalsounderlinetheadditionalneedtoreducetheavoidableharmthatcanresultfromundulycautiousprofessionaland/orregulatoryapproachestoallowingthepublicaccesstobeneficialinnovations.Pursuingsafetyatanycostisnotdesirable,ascomparedtoseekingtomaximisebenefitsrelativetounwantedoutcomes.
From thestandpointof thisanalysis it isalso importanttostressthatIPRsinparthelptoensurethatinnovatorswho test their products carefully are not financiallydisadvantagedandarenotmotivated topromote themwithoutduecaution.Thisisespeciallyimportantwhenitisdifficulttoevaluatethefullconsequencesofamedicine’suse in large populations. Seen from this angle it isuncertain thatcurrent ‘on themarket’patentprotectionperiodsofonlyalittleoveradecadearesufficienttoservepublic interest focusedpolicyends. Ifapproachessuch
asadaptivemedicines licensingare in future introducedthecase forextendingpharmaceutical IP terms is likelyto further strengthen. Ideally, this should not only allowmoretimeforthestagedintroductionofinnovationslike,say,newcancer treatments. It couldalso lowermarketentryprices,ifitpermitsoverall‘abovecommodityreturn’incomegeneratingperiodsbesignificantlyincreased.
Patient organisations whose members could benefitfrom such reforms might wish to consider questionssuch as why, for example, modern copyright termscanrunfor75yearsafterthedeathofanauthor,whileIPRsonmedicinesthatmayrequireinexcessof$1,000millionofpublicandprivatemoneyfortheirdevelopmentprovideonlyabouttenyearsonthemarketprotection.In the face of questions relating to the possible costsof extending IP termdurationsand its impactson theaffordabilityofinnovativemedicines’inpoorernations,itisrelevanttonotethepotentialforapproachesliketieredglobalpricingtoinfuturehelpensureuniversalaccesstoessentialnewtreatments–seebelow.
Pricing, value and affordability
Total national outlays onmodernmedicines (includingdistribution costs, local taxes and trading mark ups)have when expressed as a proportion of GDP beenrelativelystableataround1-2percentofGDPinricherandpoorernationsalikeforabout50years.Totalhealthcarespendingisnowtypicallyintheorderof5percentofGDPinthelatterand10percentinwealthiernations,althoughintheUSitiscloseto18percent(seeFigures8aand8b).16
15 In1960DrFrancesKelsey,amedicallyqualifiedpharmacologistservingasanFDAdrugreviewer,preventedtheapprovalofThalidomideintheUSasasedativepainkillerandanti-emeticforuseinpregnancy.Thiswasbecauseshehadconcernsaboutalackofdataonthedrug’sabilitytocrosstheplacenta,andanabsenceofclinicaltrialresults.SomepharmaceuticalscientistsinEuropesharedconcernsrelatedtohersinthelate1950s.Butthelackofarigorousapproachtomedicineslicensingatthattimemeantthatitwasneverthelessmarketedforusebypregnant
Figure 8a. Total health spending as a % of GDP
Source:OECD2011(2009data)
womenincountriessuchastheUKandAustralia,aswellasinGermany.Muchlater,thedrugwasfoundtobeappropriateforuseinareassuchasthetreatmentofleprosy.
16 Itissometimesclaimedthat50%ormoreofhealthspendingincountriessuchasIndiaisaccountedforbymedicinesspending.Butinrealityspendingonallopathicmedicinesaccountsforonlyabout20%oftotalIndianhealthspending.Thelatteris,asaproportionofGDP,lowerthanthatrecordedinnearlyallothermajornations.
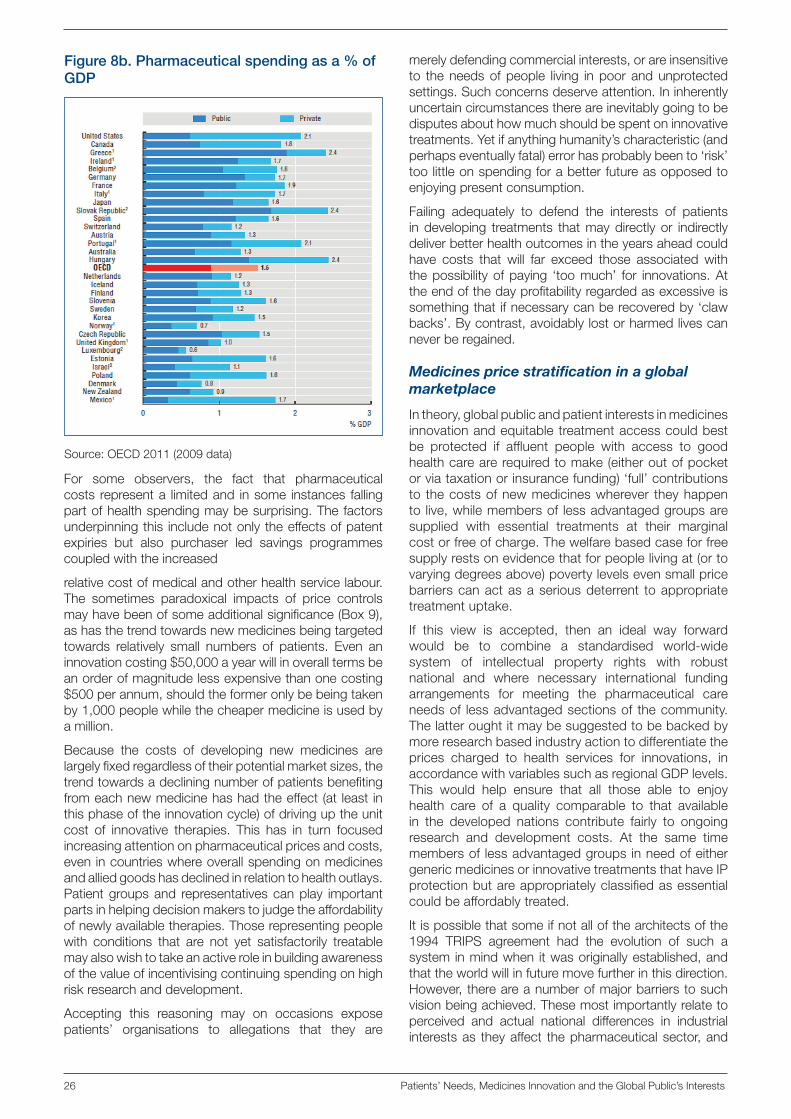
26 Patients’Needs,MedicinesInnovationandtheGlobalPublic’sInterests
For some observers, the fact that pharmaceuticalcosts representa limitedand insome instances fallingpartofhealthspendingmaybesurprising.Thefactorsunderpinningthis includenotonlytheeffectsofpatentexpiries but also purchaser led savings programmescoupledwiththeincreased
relativecostofmedicalandotherhealthservicelabour.The sometimes paradoxical impacts of price controlsmayhavebeenofsomeadditionalsignificance(Box9),ashasthetrendtowardsnewmedicinesbeingtargetedtowards relatively small numbers of patients. Even aninnovationcosting$50,000ayearwillinoveralltermsbeanorderofmagnitudelessexpensivethanonecosting$500perannum,shouldtheformeronlybebeingtakenby1,000peoplewhilethecheapermedicineisusedbyamillion.
Because the costs of developing new medicines arelargelyfixedregardlessoftheirpotentialmarketsizes,thetrendtowardsadecliningnumberofpatientsbenefitingfromeachnewmedicinehashadtheeffect(at least inthisphaseoftheinnovationcycle)ofdrivinguptheunitcost of innovative therapies. This has in turn focusedincreasingattentiononpharmaceuticalpricesandcosts,evenincountrieswhereoverallspendingonmedicinesandalliedgoodshasdeclinedinrelationtohealthoutlays.Patientgroupsand representativescanplay importantpartsinhelpingdecisionmakerstojudgetheaffordabilityofnewlyavailabletherapies.Thoserepresentingpeoplewith conditions that are not yet satisfactorily treatablemayalsowishtotakeanactiveroleinbuildingawarenessofthevalueofincentivisingcontinuingspendingonhighriskresearchanddevelopment.
Accepting this reasoning may on occasions exposepatients’ organisations to allegations that they are
merelydefendingcommercialinterests,orareinsensitiveto theneedsofpeople living inpoor andunprotectedsettings.Suchconcernsdeserveattention.Ininherentlyuncertaincircumstancesthereareinevitablygoingtobedisputesabouthowmuchshouldbespentoninnovativetreatments.Yetifanythinghumanity’scharacteristic(andperhapseventuallyfatal)errorhasprobablybeento‘risk’toolittleonspendingforabetterfutureasopposedtoenjoyingpresentconsumption.
Failing adequately to defend the interests of patientsindeveloping treatments thatmaydirectlyor indirectlydeliverbetterhealthoutcomesintheyearsaheadcouldhave costs that will far exceed those associated withthepossibilityofpaying ‘toomuch’ for innovations.Attheendofthedayprofitabilityregardedasexcessiveissomethingthatifnecessarycanberecoveredby‘clawbacks’.Bycontrast,avoidablylostorharmedlivescanneverberegained.
Medicines price stratification in a global marketplace
Intheory,globalpublicandpatientinterestsinmedicinesinnovationandequitabletreatmentaccesscouldbestbe protected if affluent people with access to goodhealthcarearerequiredtomake(eitheroutofpocketorviataxationorinsurancefunding)‘full’contributionsto thecostsofnewmedicineswherever theyhappento live,whilemembersof lessadvantagedgroupsaresupplied with essential treatments at their marginalcostorfreeofcharge.Thewelfarebasedcaseforfreesupplyrestsonevidencethatforpeoplelivingat(ortovaryingdegreesabove)povertylevelsevensmallpricebarrierscanactasaseriousdeterrent toappropriatetreatmentuptake.
If this view is accepted, then an ideal way forwardwould be to combine a standardised world-widesystem of intellectual property rights with robustnational and where necessary international fundingarrangements for meeting the pharmaceutical careneedsof lessadvantagedsectionsof thecommunity.Thelatteroughtitmaybesuggestedtobebackedbymoreresearchbasedindustryactiontodifferentiatetheprices charged to health services for innovations, inaccordancewithvariablessuchasregionalGDPlevels.This would help ensure that all those able to enjoyhealth care of a quality comparable to that availablein the developed nations contribute fairly to ongoingresearch and development costs. At the same timemembersof lessadvantagedgroupsinneedofeithergenericmedicinesorinnovativetreatmentsthathaveIPprotectionbutareappropriatelyclassifiedasessentialcouldbeaffordablytreated.
Itispossiblethatsomeifnotallofthearchitectsofthe1994 TRIPS agreement had the evolution of such asystem inmindwhen itwasoriginallyestablished,andthattheworldwillinfuturemovefurtherinthisdirection.However,thereareanumberofmajorbarrierstosuchvisionbeingachieved.Thesemostimportantlyrelatetoperceived and actual national differences in industrialinterestsas theyaffect thepharmaceuticalsector,and
Figure 8b. Pharmaceutical spending as a % of GDP
Source:OECD2011(2009data)

Patients’Needs,MedicinesInnovationandtheGlobalPublic’sInterests 27
Box 9. The limits of ‘value based pricing’ for medicines
Since the 1960s health economics has made muchprogress. This was initially related to pharmaceuticalindustry support, linked to companies’ efforts tocommunicatethevalueofinnovations.Morerecently,ithasbeenstronglyassociatedwithgovernmentbodies’effortstocontrolcostsandoptimisetheuseofthepublicresourcesspentonhealthcareingeneralandmedicinesinparticular.Onekeystepforwardwas,fromthe1980sonwards, the introduction into widespread use of theQualityAdjustedLifeYear(QALY)andtheparallelconceptof the Disability Adjusted Life Year (DALY). Althoughinpractice verydifficult toassesswithaccuracy, ‘costperQALY’measures are used to estimate the relativeutilityofinterventionsandsotopermit‘valueformoney’comparisonswithinthehealtharena.
Throughouttheworldpublicandprivatehealthspendingonhealthandalliedservices roseasapercentageofGDPduringthe lasthalfcentury,primarilybecauseofincreasedoutlaysonhealthsectorlabour.InassociationwiththistrendQALYbasedcalculationshavebecomeprogressively more widely employed as a means ofguiding the allocation of health sector funds inwayswhichwill increase serviceefficiency.However, in theUSinparticularobjectionshavebeenraisedtovaluingonelifemorethananotherbecauseofaperson’sageorhealthstatus.
While acknowledging the importance of efforts toensure that limited resources are used wisely inattempts to improvewelfare, it is inaddition true thattraditionalhealtheconomicstechniqueshavehadlittleto offer in areas such as understanding how socialrelationswithinthehealthsectorinfluenceproductivity
andoutcomes.Further,theycannotaddressquestionssuch as ‘how much of its income ought a nation to spend on health services?’ or ‘what is the long term value of investing in areas such as biopharmaceutical innovation as opposed to improving the provision of existing means of care?’
There are major uncertainties involved in trying toassess how new technologies will in future develop,and in predicting how in the long term advances inareas such as, say, genetics, the neurosciences andbio-engineering will impact on not only health andhealthcarebutotheraspectsofhumandevelopmentand survival. The scale of the unknowns involveddiscouragesmainstreamacademicsandotheranalystsfromspeculatingaboutbroadquestionssuchas‘what would developing technologies that enable health professionals to prevent or cure all cancers and/or complaints such as Alzheimer’s Disease be worth to humanity over the course of the twenty first century?’
However,patientsandthepublichaveavitalinterestinrecognisingthe importanceof investingforthefuture.Patientorganisationsseekingtodefendtheirmembers’interestsinsustaininginnovationshouldbeawareofthepossibility that apparently objective approaches suchascostperQALY linked ‘valuepricing’ formedicinesandotherinnovationscouldsystematicallyunder-valuethe long term community returns to be derived fromspendingonhighriskresearchanddevelopment.Theyshouldalsobeabletocommunicatetodecisionmakerswhythis isso,andhowsuchriskscanbeminimisedthroughthebalancedpursuitofbetteraccesstocaretodayandbettertreatmentstomorrow.
to local capacities and willingness to develop healthcaresystemsthatrespondadequatelytovaryingpatientneedsandabilitiestopay.
It is thereforemore likely that (subject to the terms ofthe ‘freetrade’agreementsbeingnegotiatedbetween,for instance, the EU and America on the one handand India on the other) IPRs and the ceiling prices ofpharmaceuticalinnovationswillfortheforeseeablefutureremainstrongerandhigherintherichercountriesoftheworldthaninpoorernations.Acceptingthisuncriticallycould insomecircumstancesincreaseinequitieswithinemergenteconomies,particularlywhenbetteroffpeoplebenefitfromlowmedicinepricesbutfailtomake‘transferpayments’ sufficient to support the health servicesneeded by less fortunate citizens. Yet global patientandpublicinterestsinthecontinuedprivate(andpublic)sector funding of biomedical innovation need not beunderminedifpriceboundariesbetweenregionsdonotdeteriorate.Thismighthappenbecauseofillicittrading,orifpoliticalforcesunderminethewillingnessofpeopleincountries liketheUSandthoseoftheEUtoaccepthigherprices formedicines than thosepaid individualselsewhereintheworld.
People and organisations seeking better treatmentsfor themselves, for their contemporaries and/or futuregenerations would on the basis of the assessmentofferedherebewell advised to recognise the valueofand defend IPP based incentives for innovation,whileat the same time advocating well targeted medicinesaccesssupportforlessadvantagedpeople.Insummary,the approach suggested here is that in addition toconsidering the advantages of further extending theduration of IPRs for new pharmaceutical products inthe OECD nations, patient organisations and othersinterested in both continuing biomedical progressand assuring appropriate global access to effectivetreatmentsshould:
• press for the establishment of internationally agreed criteria for identifying ‘public health emergencies’ and situations in which there is an urgent need to enhance access to IP protected and/or generic medicines. The purpose of thiswould be to help prevent arbitrary governmentinterventions that in effect confiscate or transferintellectualpropertyrightsawayfrominnovators,whileat the same time improving theglobal community’s
28 Patients’Needs,MedicinesInnovationandtheGlobalPublic’sInterests
ability to identify and correct life endangering andavoidable pharmaceutical market and wider healthcaresystemfailures;and
• seek to ensure that mechanisms for, and the extent of, price stratification between markets are also systematically based on transparent principles.Patientsand thewiderpublicalsohavean interest in arrangements that prohibit ‘leakages’of low cost IP protected pharmaceutical productsfrom lower to higherGDP regions. Progress in thisarea could also serve to reinforce the integrity ofmedicineslicensingsystems,andtheglobalqualityofpharmaceuticalproducts.
Fromaglobalpublicintereststandpointarelatedissuetoclarifyistheextenttowhichinternationalcompaniesofferingpatentedorother IPprotectedmedicinesatalowcost inpoorsettingsremainable tochargehigherpricesinmoreaffluentcontexts.Thehistoryof‘paralleltrading’ (or inUS terms re-importing) in the EuropeanUnionsuggeststhatitmaybedifficultifnotimpossibletomaintainthecommitmenttosocialjusticeandhumanwelfare needed to make price differentiation basedstrategies deliver desired outcomes. Butwithout sucharrangementstheglobal introductionofpreventiveandclinical applications of the major advances currentlyoccurring in areas such as genetics and molecularbiologycouldbeneedlesslyslowed.
Conclusion
Supplyingpharmaceuticalsofanysort is rarely, ifever,enough by itself to solve complex public or personalhealthproblems.Yetalongwithotherhealthprotectingand promoting interventions, improved diagnostics,vaccines and medicines supply and use can makeimportantdifferencestothehealthofnotonlyindividualsbutentirepopulations.Seenfromthisviewpoint,assuringaccesstomodernpharmaceuticalsis‘one of the most pressing and morally compellingproblems we face as humanity’ (Williams,2012).
Similarconclusionscanbedrawninrelationtoongoingpharmaceuticalandotherformsofbiomedicalinnovationandworld health, even though ensuring that sufficientresourcesareallocated toactivities like research is aninherently more uncertain task than seeking to makeexistingcarearrangementsmoreefficient. Thereisinthefirsthalfofthetwentyfirstcenturyanhistoricopportunityfor humanity to complete the global processes ofdemographicandepidemiologicaltransitionthatbeganinEuropeataroundthestartofthe1800s.Givencontinuingbiomedicalandpharmaceuticalinnovationcoupledwithextendedhealth carecoverageanddelivery, child and‘workingage’adultmortalityduetoinfectiousandmanyformsof non-communicable disease couldbe virtuallyeliminatedby2050(Peto,2012).
It is also possible that by then average healthy lifeexpectancy at birthwill be extended to over 80 yearsin every world region, and that technologies linked tocurrent biopharmaceutical progress will be making
importantcontributions infieldsranging fromfoodandfuelproductiontothemanagementofatmosphericandoceanic pollution. But translating the promise of suchbenefits into realised health gainwill not only demandthenationalandinternationalpoliticalwillneededto,forexample,furtherextenduniversalhealthcoverage.Itwillin addition require themaintenance and strengtheningof the economic and social mechanisms required tochannel resources into costly high risk research andgenerateproductiveinnovations.
Acentralmessageofthisreportisthatintellectualpropertyrightshaveavitalroletoplayinthis lastcontext.EvenifinfutureadditionalincentivessuchasStateorprivatedonorbackedprizesforthedevelopmentoftherapeuticsolutions to priority problemswere to be funded, andproposals such as Pogge and Hollis’s Health ImpactFundgivenlargescaleinternationalsupport,itisunlikelythat such initiatives could replace provisions such aspatentsorregulatorydataprotectionsinawaythatwillbenefitratherthanharminternationalwelfarestandards.
Someobserversmaygenuinelybelieve that theglobalsystem for conferring IPRs is ‘broken’, and shouldbe dismantled. But the conclusion offered here isthat preserving and in some contexts strengtheningintellectualproperty rightshasanessential role toplayin facilitating continuing private and public investmentinpharmaceuticalandotherformsofinnovation.Thisissodespite the fact that it ineffect involves imposingatemporary‘tax’ontheuserecentdevelopmentsinordertoencouragedesiredspendingonongoingresearch.
This is not to say that agencies such as patientorganisationsthathavearemittofosterthedevelopmentofbettertreatmentsshouldignoretheneedsofpeopleliving in economically less advantaged communitiesfor better access to today’s life saving and enhancingmedicines.Itisinsteadtoarguethatadditionalprovisionsandreformsshouldbe introducedalongsidetraditionalapproaches to IP law to ensure that sometimesconflictingglobalpublicinterestsinpresentaccessandfutureinnovationaremetaseffectivelyaspossible.
Somecommentatorsmayarguethatprovidinguniversalglobalaccesstogoodqualityhealthcareandeffectivemodern pharmaceuticals is an unaffordable, utopian,goal.However,asecondkeyfindingof thisanalysis isthatalthoughskilledhealthprofessionalsareatanyonetimeafiniteandrelativelyexpensiveresource,productslike medicines are – once they have been developedforuse inclinicalorwidersettings–normally relativelyinexpensive to make. As manufacturing technologiesimprove this could increasingly be the casewith largemolecule biopharmaceuticals, as well as with smallmolecule ‘chemical medicines’. Although innovativetreatments are initially expensive because of the needto test them thoroughlyand tomaintain theeconomicconditions required for further investment, their supplycosts in time fall significantly. The fact that in someless advanced markets combinations of prescriberand consumer loyalty and sometimes questionablemarketingpracticesmightonoccasionsallowbrandedmaturemedicines tomakemargins that appear close

Patients’Needs,MedicinesInnovationandtheGlobalPublic’sInterests 29
tothoseearnedbypatentedinnovationsshouldnotbepermittedtoobscurethistruth.
Thefinalmessageofthisanalysisisthereforethatpatientsand thepublicshouldbeconfident thatafter theexpiryofIPrightspharmaceuticalinnovationsnormallybecomepermanentlyavailablelowcostresources.Thisisinmarkedcontrasttootherhealthcarefactorcosts,whichtypicallyincrease over time as societies increase theirwealth. Itrepresentsapowerful reason forcontinuing to invest innewpharmaceuticals. Innovativemedicinesdonotonlyincrementally improve upon established treatments.Theycanopenupfundamentallynewandcosteffectiveopportunities for thereliefofsuffering, theeliminationofdiseaseandtheenhancementoflife.Communicatingthisrealitytopolicymakersandelectoratesisfromapatientstandpointlikelytobecomeaprogressivelymorevitaltaskasthetwentyfirstcenturyunfolds.

30 Patients’Needs,MedicinesInnovationandtheGlobalPublic’sInterests
ReferencesAgarwalP.,SanseauP.andCardonL.R.(2013)Noveltyinthetarget landscape of the pharmaceutical industry. Nature Reviews Drug DiscoveryVolume: 12,Pages: 575–576
AndersonR.(2013)personalcommunicationYearpublished:
Attaran A and Gillespie-White L. (2001). Do Patents forAntiretroviralDrugsConstrainAccesstoAIDSTreatment
inAfrica?Journal of the American Medical Association (JAMA)286(15): 1886-1892
BanerjeeA.,Hollis,A.andPoggeT.(2010).Thehealthimpactfund: incentives for improving access to medicines. Lancet 375,166-169
Berndt E. R., Glennerster R., Kremer M. R. et al (2007).Advancemarketcommitmentsforvaccinesagainstneglecteddiseases: estimating costs and effectiveness. Healtheconomics,16,491-511.
Bijker W. E., Bal R. and Hendriks, R. (2009). Paradox ofScientific Authority: The Role of Scientific Advice inDemocracies.Boston:theMITPress
BoldrinM.andLevineD.K.(2013).TheCaseAgainstPatents.Journal of Economic Perspectives,27,3-22.
BoseleyS. (2012).Does eu/india free trade agreement spell the end of cheap drugs for poor countries?Availableatwww.guardian.co.uk/society/sarah-boseley-global-health/2012/feb/10/hiv-infection-pharmaceuticals-industry Last accessedSeptember2013
Chang,H.J.(2002).Kicking Away the Ladder – Development Strategy in Historical Perspective.AnthemPress,London
CharlesC.,GafniA.andWhelanT. (1997).Shareddecision-making in themedicalencounter:Whatdoes itmean? (Or ittakesatleasttwototango).Social Science & Medicine,44(5),681-692.
Coffman T.M. (2011). Under pressure: the search for theessential mechanisms of hypertension. Nature MedicineVolume:17,Pages:1402–1409
DaviesJ.E.,NeidleS.andTaylorD.G.(2012)Developingandpaying for medicines for orphan indications in oncology:utilitarianregulationversusequitablecare?Br J Cancer 106 (1):pp14–17
DikshitR.P.,NagraniR.,YeoleB.etal(2011)ChangingtrendsinChronicMyeloidLeukaemiainGreaterMumbai,India,overaperiodof30years. Indian J Med Paediatr Oncol32(2):96–100
DiMasi J.A. and Grabowski H.G. (2007a). The cost ofbiopharmaceutical R&D: is biotech different? Managerial & Decision Economics28:469-479.
DimasiJ.A.andGrabowskiH.G.(2007b).Shouldthepatentsystemfornewmedicinesbeabolished?Clinical pharmacology and therapeutics,82,488-490.
DrummondM.,TarriconeR.andTorbicaA.(2013).AssessingtheAddedValueofHealthTechnologies:ReconcilingDifferentPerspectives.Value in Health16(1),S7-S13.
ElberseJ.E.,PittensC.A.C.M.,BuningT.D.C.andBroerseJ. E. W. (2012). Patient involvement in a scientific advisoryprocess: Setting the research agenda formedical products.Health Policy,107(2-3),231-242.
EU(2012).The2012IndustrialR&DScoreboard.Luxembourg:PublicationsOfficeoftheEuropeanUnion
FDA (2013) Patient Network News. Available at: http://patientnetwork.fda.gov/LastaccessedSeptember2013
FlynnJ.R(2009)Whatisintelligence?BeyondtheFlynneffect.Cambridge:CambridgeUniversityPress
Gates B. (2005). http://www.gatesfoundation.org/speeches-commentary/pages/bill-gates-2005-world-health-assembly.aspx.LastaccessedSeptember2013
GagnonM.P.,DesmartisM.,Lepage-SavaryD.etal.(2011).Introducing patients’ and the public’s perspectives to healthtechnology assessment: A systematic reviewof internationalexperiences.Int J Technol Assess Health Care,27(1),31-42
Hailey,D.andNordwallM.(2006).Surveyontheinvolvementof consumers in health technology assessment programs.International Journal of Technology Assessment in Health Care,22(4),497-499
HollisA.(2008).Thehealthimpactfund:ausefulsupplementtothepatentsystem?Public Health Ethics1:124-133.
JacobR.(2013)Personalcommunication
IFPMA (2012) Ending Neglected Tropical Disease. Geneva:International Federation of Pharmaceutical ManufacturersAssociations
IMS Consulting Group (2013). Securing IP and Access toMedicine:IsOncologytheNextHIV?Availableathttp://www.imsconsultinggroup.com/deployedfiles/consulting/Global/Content/Our%20Latest%20Thinking/Static%20Files/IMSCG_Compulsory%20Licensing%20-%20Securing%20IP%20and%20Access%20to%20Medicine_March%2020.pdf LastaccessedOcober2013
Kaitin K. (2010). Deconstructing the Drug DevelopmentProcess: thenew faceof innovationClin Pharm Ther87 (3):356-361
KanavosP.,Costa-FontJ.andSeeleyE.(2008).Competitionin off-patent drugmarkets: Issues, regulation and evidence.EconomicPolicy23:499-544
KanavosP.,SullivanR.,LewisonG.etal (2010).TheRoleofFunding and Policies on Innovation in Cancer DrugDevelopment.London:TheLondonSchoolofEconomicsandPoliticalScience
Kaplan W., Virtz V.J., Teeuwisse A. et al (2013). PriorityMedicines forEuropeand theWorld,2013update.Geneva:WorldHealthOrganisation
KayeJ.,CurrenL.,Anderson,N.etal.(2012).Frompatientstopartners:participant-centric initiatives inbiomedicalresearch.Nature Reviews Genetics13(5),371-376.
KentA. (2006).Patientsand IP–shouldwecare?Script-ed3,4,260-264
KuhnR.andBeallR.F. (2012).The time forpharmaceuticalcompulsorylicensinghasexpired.Nature Medicine,18,1168-1168.
Love, J. and Hubbard, T. (2007). The big idea: prizes tostimulateR&Dfornewmedicines.Chicago-Kent Law Review, 82, 1519 – 1554.
LoveJ.(2011).Theproductionofgenericdrugsinindia.British Medical Journal342: d1694
LightD.W.andLexchinJ.R.(2012).Pharmaceuticalresearchanddevelopment:whatdowegetforallthatmoney?British Medical Journal,345:e4348
Patients’Needs,MedicinesInnovationandtheGlobalPublic’sInterests 31
Mestre-FerrandizJ.,SussexJ.andTowseA.(2012).TheR&DCosts of a New Medicine. London: The Office of HealthEconomics
MurrayC.J.L.,VosT.,LozanoR.etal(2012)Disability-adjustedlifeyears(DALYs)for291diseasesandinjuriesin21regions,1990—2010:a systematicanalysis for theGlobalBurdenofDiseaseStudy2010.Lancet380,2197-2223
MSF (2012) http://www.doctorswithoutborders.org/press/release.cfm?id=6338,lastaccessedSeptember2013
NuffieldCouncilonBioethics(1999).EthicalIssuesinResearchInDevelopingCountries.London:NuffieldCouncilonBioethics
PetoR. (2012)HarveianOration.Seehttp://www.rcplondon.ac.uk/webstreamed-events/harveian-oration-2012-halving-premature-death-sir-richard-petoLastaccessedJune2013
PoggeT.W.2005.Humanrightsandglobalhealth:aresearchprogram.Metaphilosophy,36,182-209.
PugatchM.P.,ChuR.andTorstenssonD.(2012).Assemblingthe pharmaceutical R&D puzzle for needs in the developingworld.ThePugatchConsilium.
Pugatch M.P., Torstensson D. and Chu R. (2012). TakingStock: How Global Biotechnology Benefits from IntellectualPropertyRights.ThePugatchConsilium.
Reichman J.H. (2009a).Comment: compulsory licensing ofpatented pharmaceutical inventions: evaluating the options.The journal of law, medicine & ethics,37,247-263.
ReichmanJ.H.(2009b).Intellectualpropertyinthetwenty-firstcentury:willthedevelopingcountriesleadorfollow?Houst law rev,46,1115-1185.
SalomonJ.A.,WangH.,FreemanM.K.etal(2012)Healthylifeexpectancy for 187 countries, 1990-2010: A systematicanalysisfortheGlobalBurdenDiseaseStudy2010.The Lancet380,2144-62.
SamantR.andBennettC.(2008).Decisionmakinginoncology:Areviewofpatientdecisionaidstosupportpatientparticipation.CA: A Cancer Journal for Clinicians58(5),293-304.
ShahaniR.(2013)Personalcommunication
SonderholmJ.(2010a).Intellectualpropertyrightsandthetripsagreement.Research working papers,1,1-48.
SonderholmJ.(2010b).Areformproposalinneedofreform:acritique of thomas pogge’s proposal for how to incentivizeresearch and development of essential drugs.Public health ethics,3,167-177.
Sonderholm J. (2010c). A theoretical flaw in the advancemarketcommitmentidea.Journal of medical ethics,36,339-343.
StiglitzJ.(2007).Prizes,notpatents.Post-autistic Economics Review,42,46-47
TaylorD.G.&BuryM. (2007)Chronic illness,expertpatientsandcare transition.Sociology of Health & Illness 29, 27-45.Trotter, a. 2012. Enforcement costs: some humanitarianalternativestostrongerpatentrights.Medico-legal journal,80,22-32.
UNAIDS (2012).Global report:UNAIDS report on the globalAIDS epidemic 2012. New York: Joint United NationsProgrammeonHIV/AIDS
VastagB.(2012).‘Radical’billseekstoreducethecostofaidsdrugsbyawardingprizesinsteadofpatents.Washington Post,May19thedition
Vogel l. (2010).Fundproposedtopay fordrugswithgreaterglobal impact. Canadian Medical Association Journal 182,e231-e232
Wellcome Trust (2013). Policy on Intellectual Property andPatenting. http://www.wellcome.ac.uk/About-us/Policy/Policy-and-position-statements/WTD002762.htm LastaccessedSeptember2013
WaldN.J.(2013)Personalcommunication
WaldN.J.andMisselbrookD.(2011)The Future of Prevention in Cardiovascular Disease. London: the Royal Society ofMedicinePress
WellcomeTrust(2013).TheapproachoftheWellcomeTrustinmanaging intellectual property to maximise public healthbenefit. http://www.wellcome.ac.uk/About-us/Policy/Policy-and-position-statements/WTX037150.htm Last accessedSeptember2013
WHO(2006)PublicHealth,InnovationandIntellectualPropertyRights.Geneva:WorldHealthOrganisation
WHO (2012)Goodhealth adds life to years:Globalbrief forWorldHealthDay2012.Geneva:WorldHealthOrganisation
WHO (2004) Priority Medicines for Europe and the World.Geneva:WorldHealthOrganisation
WilliamsO.D.(2012).Accesstomedicines,marketfailureandmarketintervention:ataleoftworegimes.Glob public health,1-17.
WolffJ.(2012).The Human Right to Health. NewYork:W.W.Norton&Co
Wong-ReigerD.(2013).Personalcommunication
ZhangX(1999)TraditionalMedicineWorldwide–TheRoleofWHO.Drug Information Journal33,321-6

In the world’s history certain inventions and discoveries occurred of peculiar value, on account of their great efficiency in facilitating all other inventions and discoveries. Of these were the art of writing and of printing, the discovery of America, and the introduction of patent laws
[the most important].
Abraham Lincoln, 1860
Medicines, which may be of the utmost value for poorer countries, can be bought by us only at exorbitant prices, since we are unable to have adequate independent bases of research and production. This apart, sometimes dangerous new drugs are tried out on populations of weaker countries although their use is prohibited within the countries of manufacture. It also happens publicity makes us victims of habits and practices which are economically wasteful or wholly contrary to good health… My idea of a better ordered world is one in which medical discoveries would be free of patents and there would be no profiting
from life or death.
Indira Gandhi, 1981
Political systems in rich countries work well to fuel research and fund health care delivery, but only for their own citizens. The market works well in driving the private sector to conduct research and deliver interventions, but only for people who can pay. Unfortunately, the political and market conditions that drive high quality health care in the developed world are almost entirely absent in the rest of the world. We have to make these forces work better for the world’s poorest people.
Bill Gates, 2005
CopyrighttheUCLSchoolofPharmacyJanuary2014. Price£7.50. ISBN978-0-902936-29-4