patrick willemot core im academic ½ day 2010 october 14
TRANSCRIPT

Antiretroviral therapyand immune reconstitution
inflammatory syndromesPatrick Willemot
Core IM Academic ½ day2010 October 14
Overview of presentationHAART
Briefly, when to startPrinciples of therapyMedication classes
Effects, side-effects, and pearls
IRISDefinitions, clinical presentationsHow to avoidHow to treat

When to start HAART?When the risks of deferring therapy outweigh
the risks of the therapy…
Early therapy Deferred therapy
Pros Increased viral suppressionImproved immune recoveryImproved survival
Reduced toxic exposureDelaying failure of first regimenDelaying “pill burden”
Cons Increased toxic exposureIncreasing drug resistanceIncreasing “pill burden”
Increased virologic failureIncomplete immune recoveryPremature death
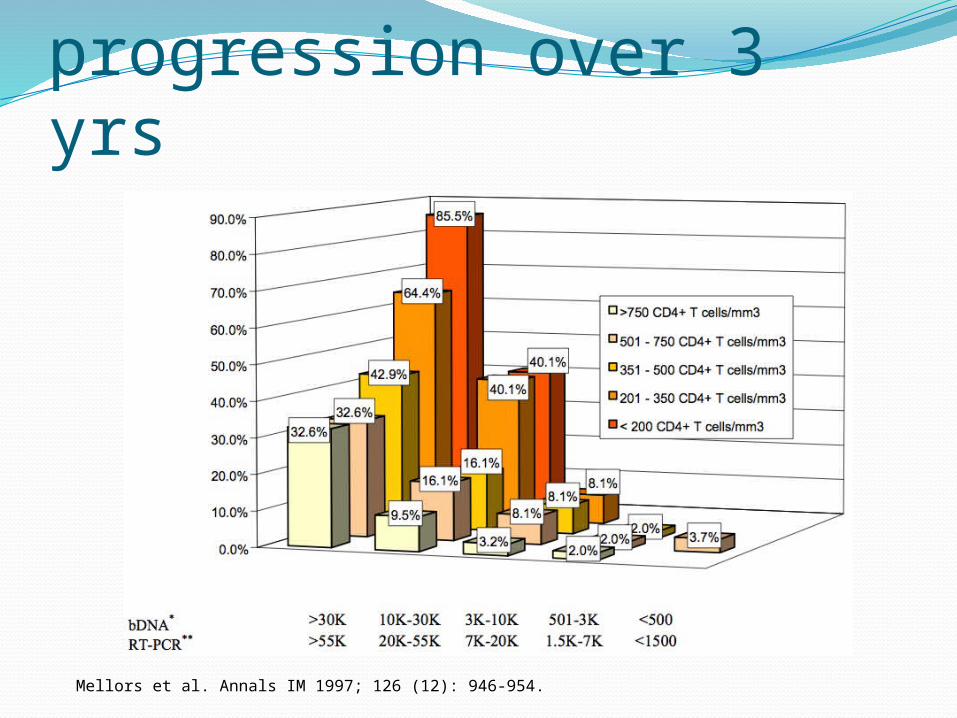
Risk of progression over 3 yrs
Mellors et al. Annals IM 1997; 126 (12): 946-954.

When to start HAART?Practically speaking:
If symptomatic (incl. OIs, HIVAN, HIVAD, neo)If pregnantIf HBV coinfected (possibly HCV too…)If immunologic or virologic progression:
Strong RCT evidence for HAART in pts with CD4 <350
Observational cohort data for pts with CD4 >350/>500 *
If ready & willing to engage in lifelong, uninterrupted tx
* NA-ACCORD. NEJM 2009 Apr 30; 360 (18): 1815-1826.
When not to defer starting?If unable to adhere to regimen
Psychosocial variablesComorbidities prohibitive to HAART
On meds with signif interactions Unable to ingest/absorb meds Acute non-tuberculous mycobacterial infection
Long-term non-progressor, elite controller

Principles of therapySuppress viral replicationAllow T-cell repopulation
Chances of immunoreconstitution are somewhat predicated upon T-cell nadirVery low nadirs will not repopulate to fully
normal levelsA decimated T-cell library may not have a
immune repertoire upon reconstitution
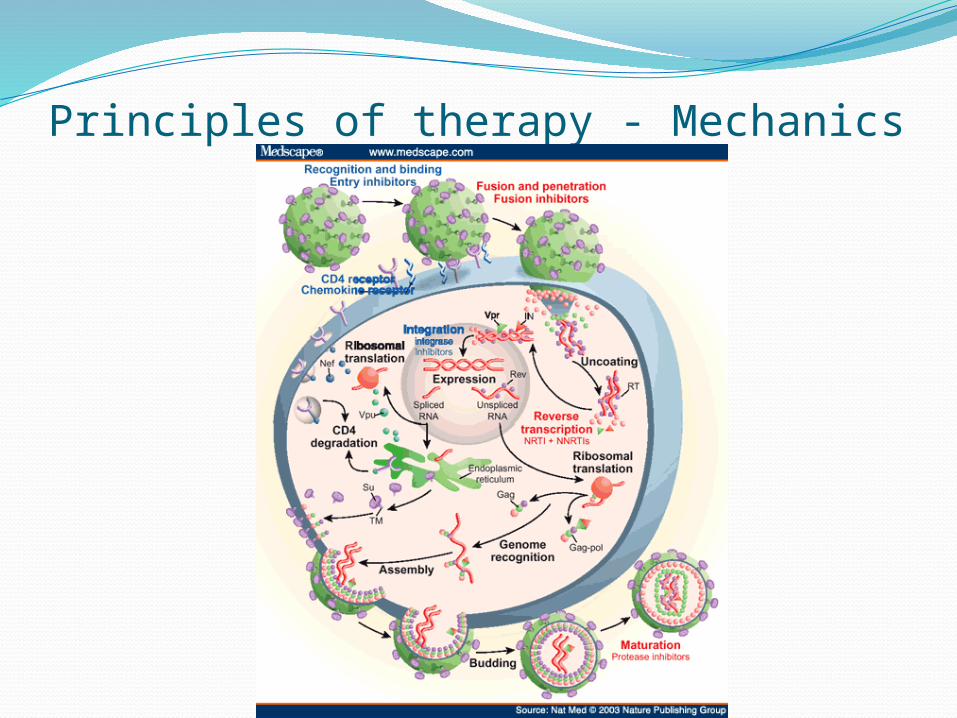
Principles of therapy - Mechanics
Principles of therapy – in practiceUse NRTI backbone –> 2 NRTIs+ a third active drug from another class
NNRTIritonavir-boosted PIintegrase inhibitor
When failure occurs, use viral genotyping (+/- phenotyping) to guide salvage therapy
Brace yourselves…
Medication ClassesNucleos(t)ide reverse transcriptase inhibitorsLamivudine (3TC)Emtricitabine (FTC, Emtriva)
Zidovudine (AZT, ZDV)
Stavudine (d4T, Zerit)
Didanosine (ddI, Videx)
Abacavir (ABC, Ziagen)
Tenofovir (TDF, Viread)
- 3TC, FTC select for M184V: less suscept ABC, ddI; more suscept AZT, d4T, TDF- Don’t combine ddI and d4T: high incid neuropathy, pancreatitis, lactic acidosis

NRTI coformulations:AZT/3TC (Combivir): bid, more cellular complixTDF/FTC (Truvada): once-daily, potent against
HBV3TC/ABC (Kivexa): once-dailyAZT/3TC/ABC (Trizivir): daily, but virol. inferior

NRTI toxicitiesNRTIs also inhibit γ-polymerase in
mitochondria –> mitochondrial death -> cellular toxicitymyelosuppression, peripheral neuropathy,
lipoatrophy, myopathy, lactic acidosis, steatohepatitis, pancreatitis, (reports of non-cirrhotic portal HTN with ddI)
Abacavir hypersensitivity (5-8%)FLI, progressive ->->-> SIRS deathHLA-B*5701 testing
Tenofovir: A/CKI incl. Fanconi-like

Medication ClassesNon-nucleoside RTIs
Efavirenz (EFV, Sustiva)Nevirapine (NVP, Viramune)Delavirdine (DLV, Rescriptor)
Etravirine (ETR, Intelence)

NNRTI toxicities & issuesToxicities
Rash (including SJS, TEN)Hepatotoxicity (including fulminant hepatic
failure)
Other issues:Efavirenz –> teratogenic, neuropsychiatricNevirapine –> more toxic in women, CD4>250K103N, K181C mutations negate EFV, NVP,
DLV
Coformulation: FTC+TDF+EFV (Atripla): daily dosing

Medication ClassesProtease inhibitorsOld-school: Indinavir, Saquinavir, Nelfinavir,
Ritonavir, Tipranavir (more tox, more pills, diff sched)
New school: rtv-boosting (P450 3A4 inh)Lopinavir/rtv (LPV/rtv, Kaletra)Fosamprenavir (FPV, Lexiva)Atazanavir (ATV, Reyataz)Darunavir (DRV, Prezista)
PI toxicities & issuesGI side effects: NV, DDyslipidemia, LipodystrophyHepatitis
Indinavir -> crystal nephrolithiasisRitonavir -> NVD++, dysgeusiaAtazanavir -> indir hyperbili, nephrolith, needs
H+ for absorption; less dyslip; I50L mutationLPV/rtv –> long QT, TdPDarunavir -> not susceptible to other PI
mutations
Medication ClassesIntegrase strand transfer inhibitorRaltegravir (RAL, Isentress)
ADRs: headache, nausea, diarrhea, fever, CPK elev
lower genetic barrier to resistance than boosted PIs
bid dosing
Medication Classes - OthersCCR5 Antagonist (prevents CCR5-gp120
interaction)Maraviroc (MVC, Celsentri) –> SAP
Coreceptor tropism assay (i.e. look for CXCR4 tropism) Has durable responses at 96 wks, up and coming MSK, cough, fever, orthostasis, rash, hepatotox, abdo
pain
Fusion inhibitor (binds gp41, prevents memb approx)Enfuvirtide (T20, Fuzeon)
sc injection bid; site rxn 100%; HSR <1%; pneumonia

What HAART to start?“Preferred” regimens
EFV/TDF/FTC (AtriplaTM)ATV/rtv (ReyatazTM) + TDF/FTC (TruvadaTM)DRV/rtv (PrezistaTM) + TDF/FTC (TruvadaTM)RAL (IsentressTM) + TDF/FTC (TruvadaTM)
“Alternative” regimenspreferred in pregnancy
LPV/rtv (KaletraTM) + AZT/3TC (CombivirTM)
NB: this is for ARV-naïve patients
Immune reconstitution inflammatory syndromes

IRIS… or, when HAART goes awryOIs regress once specific T-cell immunity is
regenerated
The same immunity may precipitate disease as inflammation develops around previously immunoneglected antigens (pathogens or autoantigens)
No formal official definition…
IRIS – when to suspect itWhen counts have been below OI thresholds
for a long time (months) without adequate prophylaxis
Development within first 4-6 months of initiation of therapy, sometimes within weeksdon’t necessarily need to have a CD4 rise on
bloodwork
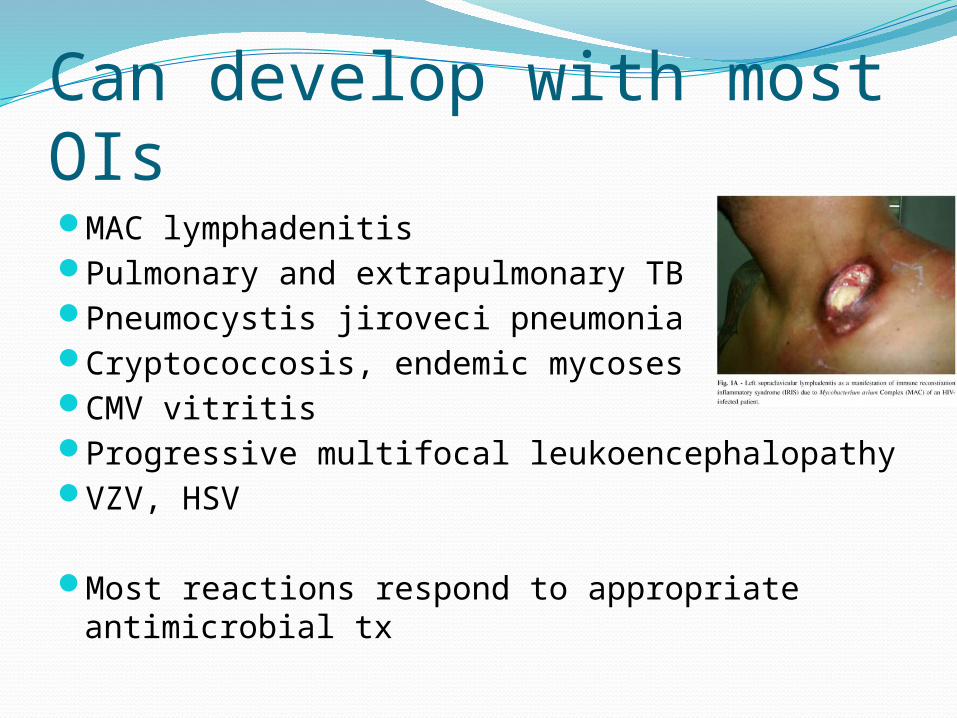
Can develop with most OIsMAC lymphadenitisPulmonary and extrapulmonary TBPneumocystis jiroveci pneumoniaCryptococcosis, endemic mycosesCMV vitritisProgressive multifocal leukoencephalopathyVZV, HSV
Most reactions respond to appropriate antimicrobial tx
IRIS with HBV/HCV is trickiermay evolve to fulminant hepatic failure
Alternatively, may get sAg clearance and sAb positivity
DDx: hepatotoxicity, removal of anti-HBV meds, …
Other immune diseasesSarcoidGraves’
How to avoidIf no tx other than HAART (e.g. JC virus ->
PML), or evidence for harm from deferring HAART (PCP), then start HAART
For OIs for which there is specific tx, consider OI tx prior to HAART (reduce antigen burden)e.g.: giving PCP proph x 1-2 months before
HAARTCryptococcal meningitis, NTB infectionneed to weigh risk of IRIS with risk of deferring
HAART
Recap of presentationHAART
When to start – when benefits outweigh risksPrinciples of therapy – NRTI backbone +
NNRTI/PI/ISTIMedication classes
Class side-effects, and individual medication issues
IRISConcept definitionHow to preventHow to treat
… un chausson avec ça?For lots more info:
www.aidsinfo.nih.gov
Questions?
Comments?
Concerns?