strategies for success under the new medicare … for success under the new medicare waiver – part...
TRANSCRIPT

Strategies for Success Under the New Medicare Waiver – Part 2
Amy E. Boutwell, MD, MPP Collaborative Healthcare Strategies
May 21, 2014

Agenda
• Expanding your portfolio of strategies
1. ED based strategies
2. Enhanced services for high risk
3. Portfolio strategy in action
• Discussion

Expanding your portfolio of efforts The 2014 “Playbook”

2014 Playbook
• Section 1: Overview • Section 2: The Transitions: Handle with Care Driver Diagram • Section 3: Critically Review Your Readmission Efforts to Date • Section 4: Designing for Success: The Portfolio Strategy • Section 5: Essential Action
– Model Impact of Your Strategy – Improve Standard Care for All – Improve Transitions Across the Continuum
• Section 6: High Leverage Impact – Hospital to SNF – Hospital to HH – Hospital to Home with Services – Emergency Department Based Interventions
• Section 7: Special Topics – Medicaid Readmissions – Behavioral Health – Palliative Care and End of Life
• Glossary and Links to Resources • Online Resources • Transitions: Handle with Care Initiative Presentations and Webinars • Template Press Release • Readmission Data Analysis • Readmission Interview Protocol • Cross-continuum Team Sample Letter and Agenda • Hospital to SNF Action Planning Worksheet • Hospital to Home Health Action Planning Worksheet • Hospital to Home Action Planning Worksheet • Excel Tool: Readmission Strategy Impact Estimator
2014 Playbook - Appendices

The best way to avoid a readmission is to not admit in the first place
ED-based Interventions

MGH High Cost Beneficiary Demonstration Project (CMS) • Target population: most expensive Medicare FFS pts at MGH • Opportunity: Identify in ED, intervene to avoid hospitalization • Intervention: Flag in record to identify patient by registration in ED
– Patients’ full care team (SW, PCP, specialists) paged – Expectation clinicians will go to ED and avert admission
• Impact: only program in the demo that saved $$ • Lessons learned:
– May not stop patients from behavior of going to ED – These patients always “look bad” (physically, or labs) – Clinicians who know the patient know what baseline is – Partner with ED doc to reassure no substantial change is presents and
to assure that close follow up will occur
ED-based Interventions

ED to SNF Transitions • Hallmark Health System, metro Boston
– 2 hospital system, 70% admits via ED, hospitalists – 20 ED docs, 17 PAs
• ED Chief and Champion of this work explored myths of SNFs/EDs – Patients only seen once a month; can’t do IVs, etc – “ED admits everyone”
• Actions: – Discussion “why” – Education: our capacity/their capacity – Simplicity : establish contacts, standard transfer information – Feedback
• Results: increase in number of patients transferred from ED to SNF
ED-based Interventions
Adapted from presentation by Dr Steven Sbardella, System Director of Quality, Hallmark Health System, April 29 2014

Frequent ED visits for Behavioral Health patients • Non-teaching regional hospital in central/rural MA • Difficulty transferring patients to psych beds = lengthy boarding • Concept: reduce ED boarding by preventing ED visits • Opportunity: identify frequent ED BH patients in ED • Staff: PM and ED BH nurse navigator, 2 FTEs • Team: ED director, ED BH team, CNO, CIO, ED CM, cross-continuum
partners • Intervention: collaboration between community mental health provider, crisis
team, community health center, ED, documented identification, referral workflows between all 3 entities, standing orders for frequent BH ED users to facilitate med clearance; establishment of individualized care plans
• Impact: successful linkage; social work / harm reduction orientation • Time to implement: 10 weeks.
ED-based Interventions
1. Train ED staff on how to use INTERACT NH Capabilities List
2. Train ED staff on how to use INTERACT SNF-ED information
3. Meet with SNFs to discuss SNF-ED transfers & opportunities to treat and return from ED
4. Staff a dedicated admission avoidance clinician in ED to coordinate with community providers/services to facilitate d/c
5. Create a flag in ED record to identify recently d/c pts <30days
6. Create individual care plans for frequent ED users with recurrent but otherwise stable complaints
ED-based Interventions - Actions

Provide enhanced services The best “transition out” and “reception in” will not suffice for high risk

“High Risk Care Teams”
• Sometimes a “coach;” increasingly multi-disciplinary team
– Navigator – Behavioral health – Social Work – Pharmacist
• Address full complement of medical, social, logistical needs
– Affordable medications; waiving office visit copayments – Transportation – Stable housing – Navigating the healthcare system, asking questions, making appointments
• Identify using combination of clinical and non-clinical criteria
– History of high utilization, no PCP, numerous prescribers, numerous meds, behavioral health comorbidities, homeless….not “just” chronic disease

• BRIDGE – Social work-based transitional care model – Assess “person in context” – Make contact in hospital; reassess at 24-48h after going home,
as needs change/emerge; reassess periodically over 30d
– Observation: Don’t require / use additional “slush funds” for transitional care – they are adept at getting patient linked to existing services (medicaid waiver, AAA, ADRC, etc)
– Observation: Don’t medicalize social complexity – “work the case” and refer for services, follow up, advocate for the patient, but don’t “escalate” care medically when they encounter barriers
Enhanced Care: BRIDGE
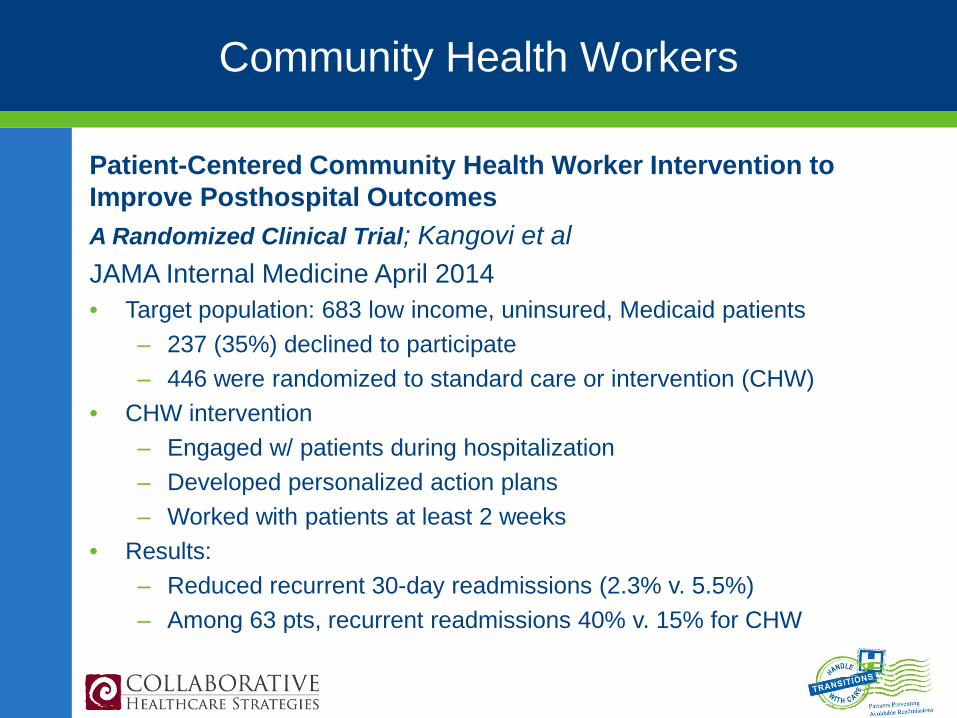
Patient-Centered Community Health Worker Intervention to Improve Posthospital Outcomes A Randomized Clinical Trial; Kangovi et al JAMA Internal Medicine April 2014 • Target population: 683 low income, uninsured, Medicaid patients
– 237 (35%) declined to participate – 446 were randomized to standard care or intervention (CHW)
• CHW intervention – Engaged w/ patients during hospitalization – Developed personalized action plans – Worked with patients at least 2 weeks
• Results: – Reduced recurrent 30-day readmissions (2.3% v. 5.5%) – Among 63 pts, recurrent readmissions 40% v. 15% for CHW
Community Health Workers

Preventing 30-Day Hospital Readmissions A Systematic Review and Meta-analysis of Randomized Trials Leppin et al; JAMA Internal Medicine (online first) May 12 2014 • Review of 42 published studies of discharge interventions
• Found that multi-faceted interventions were 1.4 times more effective
– Many components – More people – Support patient self-care
• Interventions published more recently had fewer components are were
found to be less effective
46-study Meta-Analysis: What Works?
http://archinte.jamanetwork.com/article.aspx?articleid=1868538

The Portfolio Strategy in Action

Costlier care is often worse care. Photograph by Phillip Toledano.
What a Texas town can teach us about health care.
McAllen, Texas, the most expensive town in the most expensive country for health care in the world, seemed a good place to look for some answers.
THE COST CONUNDRUM
The New Yorker June 1 2009
by Atul Gawande
Annals of Medicine
McAllen is in Hidalgo County, which has the lowest household income in the country, but it’s a border town, and a thriving foreign-trade zone has kept the unemployment rate below ten per cent.

18
Rio Grande Valley - Map
H
B
M

Sept 2009
Jan 2010
July 2012
Sept 2012
Nov 2012
Feb 2013
Mar 2013
April 2013
July 2013 Current
Palliative Care / Hospice
Project Red – Appt. w/PCP or Clinic and FU Calls
CCTP – CTI Coach and PAC Program
Discharge Assessment within 24 hour of admission
Transitional CM
Walgreen’s Well Transition Program
Registration Identifying Possible Readmissions in the ED

20

21
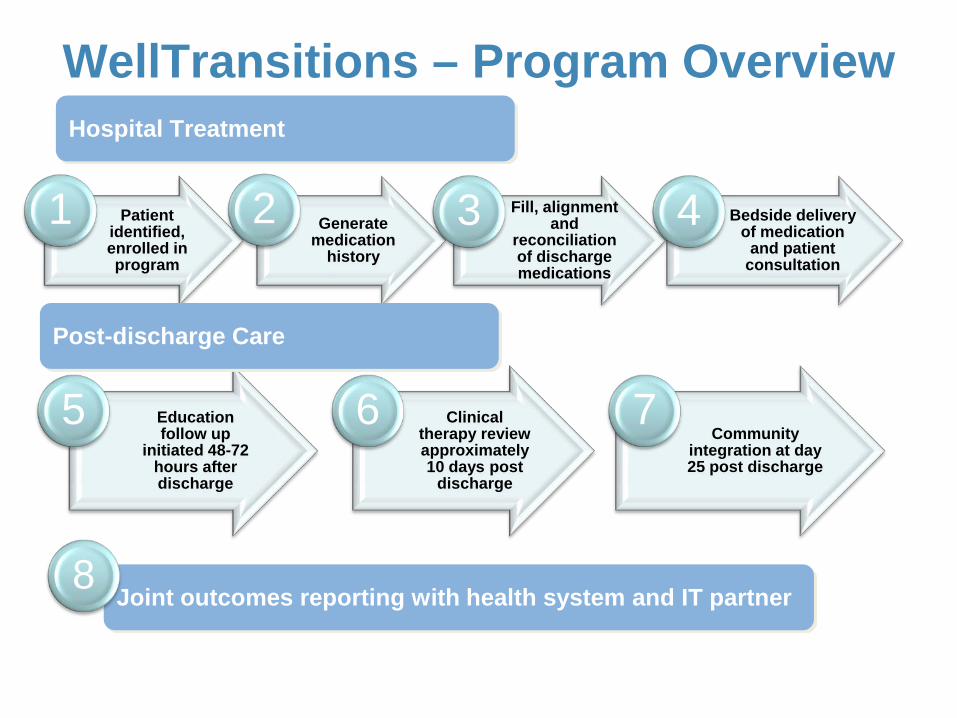
WellTransitions – Program Overview
Patient identified, enrolled in program
1 Generate medication
history
2 Fill, alignment and
reconciliation of discharge medications
3 Bedside delivery of medication
and patient consultation
4
Hospital Treatment
Education follow up
initiated 48-72 hours after discharge
5 Clinical therapy review approximately 10 days post
discharge
6 Community
integration at day 25 post discharge
7
Post-discharge Care
Joint outcomes reporting with health system and IT partner 8

23

24

Readmission Decline for VBHS
• Fiscal Year 2011 = 28% Readmission Rate
• Fiscal Year 2012 = 21.1% Readmission Rate • Fiscal Year 2013 = 13.7% Readmission Rate
50% readmission reduction!
Story courtesy of Angela Blackford, Valley Baptist Health System

Valley Baptist Health System Readmission Reduction Portfolio of Efforts
• Redesign Discharge Process
• RN/SW Case Managers Start DC Plan within 24 h of Admission
• Discharge Plans for 30 days
• Transitional CM Team - Identify, Monitor, Call, Home and Nursing Home Visits, Medication Reconciliation
• Create and Foster Community Collaboration
• Increase Patient Satisfaction
• Improve Patient Safety
• Decrease Readmissions
• Eliminate Any Readmission Penalty Over Time
• Collect Data and Trend Results

1. Know your readmission data
2. Ask your patients & their families why readmissions occur
3. Inventory your current readmission reduction efforts
4. Quantify your hospital’s 1 and 5 year readmission reduction goals
5. Develop a multifaceted strategy
6. Invest resources – in staff and tools - to get the job done
6 Recommendations

Thank you
Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies
Advisor, Maryland Hospital Association [email protected]