pediatric dentistry(2010全英班)
TRANSCRIPT
Pediatric dentistry
Zhao Wei

• Synonymous with dentistry for children pedodontics• Exists because children have dental and
orofacial problems
Definition
• An age-defined specialty that provides both primary and comprehensive preventive and therapeutic oral health care for infants and children through adolescence, including those with special health care needs (1995, by ADA’S)

Historical perspective• Up until the middle 1950s,dental office gave the sign
said: no children under age 13 treated in this office• Over the past several decades, specific educational
guideline for pediatric dentistry have been adopted and are imposed on all dental school
• Graduates of all accredited dental schools have not only a didactic education in dentistry for children but also a clinical education

• The ignorant notion that the “baby teeth don’t deserve care because you lose them anyway” has largely disappeared save for the most uninformed persons
• Advocate a routine dental appointment on or before the first birthday.
• The customary age of the first dental appointment was on or after the third birthday,which is far too old for the initiation of appropriate preventive services
• Addressing the needs of this age group remains a relevant challenge to the dental profession

Milestones in dentistry for children in the united states
• 1900 few children are treatment in dental office. • 1924 first comprehensive textbook on dentistry for children is published• 1927 American Society for the Promotion of Dentistry for children is established at the meeting of (ADA) • 1940 the American society for the promotion of dentistry of children changes its name the American society of dentistry for children (ASDC)

• 1942 the council on dental education recommends that all dental schools have pedodontics as part of their curriculum• 1948 The American academy of Pedodontics is formed • 1949 the first full week of February is designated national children’s dental week
• 1981 February is designated National children’s dental health month• 1984 the American Academy of Pedodontics changes its name to the American Academy of Pediatric Dentistry• 1995 a new definition is adopted for the specialty of pediatric dentistry by the ADA’S House of Delegates

• An age-defined specialty that provides both primary and comprehensive preventive and therapeutic oral health care for infants and children through adolescence, including those with special health care needs (1995, by ADA’S)

In china• 1998 The Chinese Academy of pediatric dentistry
is formed• 2000 The first edition of the textbook on pediatric
dentistry in Chinese is published

Challenges for pediatric dentistry in 21st century
• Preventive dentistry • Infant oral health

Acid-etch techniques, sealants, and composite resins
44thth

Dentistry of the disabled patient and other children with special needs

Early orthodontic diagnosis and treatment More sophisticated modalities of pain and
anxiety control such as sedation techniques
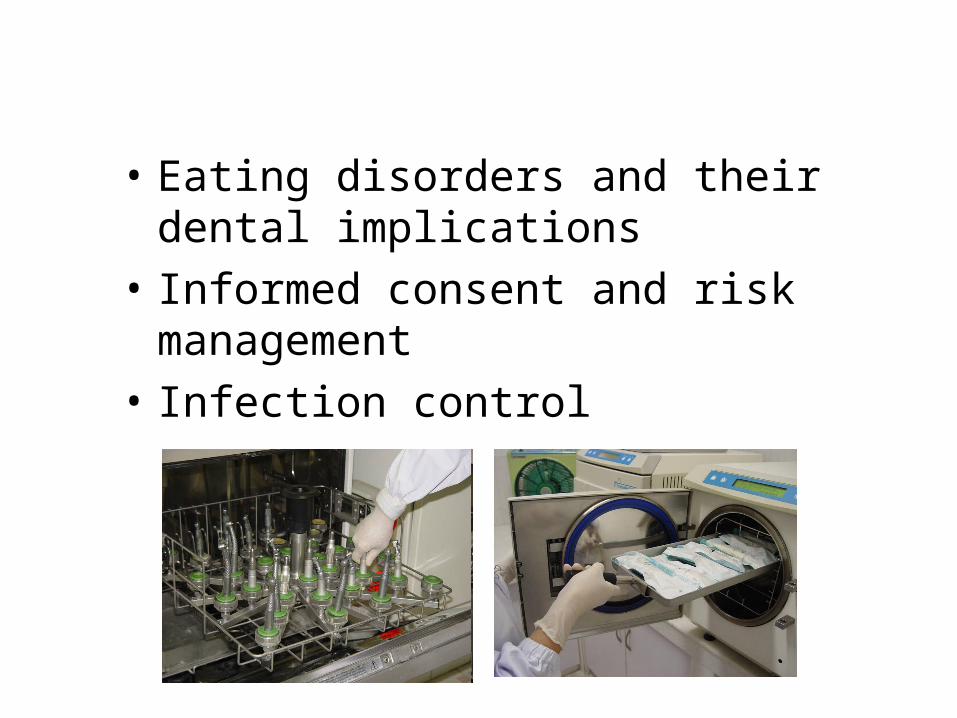
• Eating disorders and their dental implications
• Informed consent and risk management• Infection control

Application of the other disciplines• To be a complete clinician capable of handling the
majority of needs of the children, a dentist need to know– Preventive dentistry techniques– Pulpal therapy– Instrumentation and restoration of teeth– Dental materials – Oral surgery– Preventive and interceptive orthodontics – The principle of prosthodontics

On the other hand• Certain basics in pediatric medicine• General and oral pathology • Growth and development • Knowledge of nutrition• The modes of management • A person would be happy dedicating a
significant amount of practice time to children

Patient management

Patient behavioral ratings
• Rating No.1: definitely negative(--)– Refuse treatment– Cries forcefully, uncontrallable behavior– Is extremely negative, associated with fear
• Rating No.2: negative(-)– Is reluctant to accept treatment– Displays evidence of slight negativism

• Rating No.3: positive (+)– Accepts treatment– Timid behavior: follows the dentist’s directions
in a shy, quiet manner• Rating No.4: definitely positive(++)
– Unique behavior: look forward to and understands the importance of good prevent care
The importance of conviction, experience,and good intentions
• The self-confidence of the dentist is essential
Patient management by domain
• Physical domain• Pharmacologic domain• Aversive domain• Reward-oriented domain• linguistic domain

Physical domain• From the use of hand restraint by a dental assistant to
the use of tools – Papoose board– Tape – Sheet with tape– Cloth wraps – Belt

Pharmacological techniquesPharmacological techniques
• Local anaesthesia
• Nitrous oxide/oxygen analgesia
• General anesthesia
This domain requires parental understanding about the techniques,risks and alternatives

Nitrous oxide/oxygen analgesia
Aversive domain• A technique can be describe as aversive if the use of
the technique on a child is objectionable enough that the child will cooperate in order to avoid the technique
• Parental spanking is an example of aversive management
• Some physical techniques can be regards as aversive if they are used or seem to be used as a punishment
• Hand over the mouth (HOM) is regarded by many to be an aversive technique

Reward-oriented domain
• Reward can be used to secure the cooperation of a child
• Be arranged by Dentist or Parent

Linguistic domain• Be those communication techniques that involve the c
onversation of the dentist with the child and the child with the dentist
• No child is competent in language before second birthday
• All normal children are competent in language after fourth birthday
• Dentist will be Communicator, teacher coach, rewarder, psychologist

Today’s offices are not frightening





Basics in managing children in pediatric dentistry

The child is not a little man !

Most dentists agree that the preschool child clearly requires the most energy and talent for effective management

• Entails bringing the child to the dental office for a tour and orientation
• With nothing being done• The child meets the receptionist, dental
assistant, and dentist
Preappointment experience

• Certain dental equipment can be shown and explained
• In “childese” language

• Should be kept as pleasant and simple as possible• An examination and fluoride treatment
The First dental visit

Tell-show-do• Backbone of the educational phase• Simple and usually works• Dictates that before anything is done the child is told what will be done shown by some sort of simulation.• Choice of words is important

Voice control• To interject more authority into his or her
communication with the child• The tone of voice is important• Can be used with deaf children• An essential technique for preschool
children

Hand-over-mouth• Calls for the dentist to place his or her hand over
the mouth of a hysterically crying child • Has to be paired with voice control• Not intended to scare the child• To get the child’s attention and quiet him

• As a tap on the lips to remind the child crying is not appreciated
• There is no airway restraint!• Remains somewhat controversial • A legitimate technique

Physical restraint• The use of hand restraint

• The use of tools
– Mouth props– Cloth wraps – Sheet with tape


• To treat the emergencies on hysterical children and children who can not be reached in language because of their age
• Developmentally disabled children • children who for whatever reason cannot
cooperate with the dentist
Indications

,
NoteNote
• The use of physical techniques necessitates explanations to parents
guardians caretakers • A written consent to treatment
Reward and Praise • Reward be arranged by dentist or parent• Reward by parent may have a negative effect • Request that parents not promise things like ice cream or to
ys as a reward for going to the dentist before the dental appointment
• The child may misreading the intentions of the parents as their offering a reward because they think the dental appointment will be difficult, frightening,or scary for the child

• Child react favorably to praise• Reward, Praise and effective communication
combined with tell-show-do can form an effective management technique

•Tell-show-do was rated as the most acceptable
technique, followed by•nitrous oxide sedation•general anesthesia
Eaton JJ, McTigue DJ Attitudes of contemporary parents toward behavior management techniques used in pediatric dentistry. Pediatr Dent. 2005 Mar-Apr;27(2):107-13
Parents attendance in the dental operatory

• Less than 8% of dentist want parents in
attendance during the treatment • The parent is seen as a contributor to
management or behavior problems
Should parents stay with the child during the Should parents stay with the child during the procedure or remain in the waiting room?procedure or remain in the waiting room?

However • 66% parents wished to be present• They can act as an advocate for their
child and verify his or her safety

There are several options:depending on the dentist’s office policy
• Routinely exclude parents• If the parent wishes, allow him to enter • With the exception of parents of
very young child patient with developmental disabilities


Four age groups
• Conception to age three• The primary dentition years: 3 to 6 years• The transitional years: 6 to 12 years• adolescence

• The child from conception to age 3 historically has not
been involved in professional dental provision• In fact ,until recently dentistry has never actively
encouraged children of this age to be involved in professional care
Conception to age threeConception to age three
Conception to age threeConception to age three•The child from conception to age 3 historically has not been The child from conception to age 3 historically has not been involved in professional dental provisioninvolved in professional dental provision
•In fact ,until recently dentistry has never actively encouraged In fact ,until recently dentistry has never actively encouraged children of this age to be involved in professional carechildren of this age to be involved in professional care
•Age 3 has for many years been the customary entry age of Age 3 has for many years been the customary entry age of children to the dental experiencechildren to the dental experience
•It is deeply believed that prevention programs must be started It is deeply believed that prevention programs must be started well before age 3 to ensure successwell before age 3 to ensure success
•Therefore, focus on the needs of an age group the has been Therefore, focus on the needs of an age group the has been virtually overlooked previouslyvirtually overlooked previously

The primary dentition years: 3 to 6 years
• Deal with children with a complete primary dentition
• To understand the morphology and anatomy of the primary dentition
• How to preserve dental arch integrity• How to intercept malocclusions in the primary
dentition • Restoration • Pulp therapy

The transitional years: 6 to 12 years
• The majority of children shed all of their primary teeth and gain all of their permanent teeth except the third molars
• Treatment needs of young permanent teeth• Orthodontic considerations• Esthetic considerations• Prevention needs of the preschool child• Children responsibility for their own oral
hygiene


Adolescence
• Prevention• Treatment• Dental and facial
esthetics • Periodontal disease

Early child caries (ECC)
Bottle caries Bottle caries in an old Child showing arrested Caries

Rampant caries

Remarkable advances in dental restorative materials in the 1980s and 1990s are irrevobably changing pediatric Restorative dentistry

Restorative techniques



Pulpal therapy
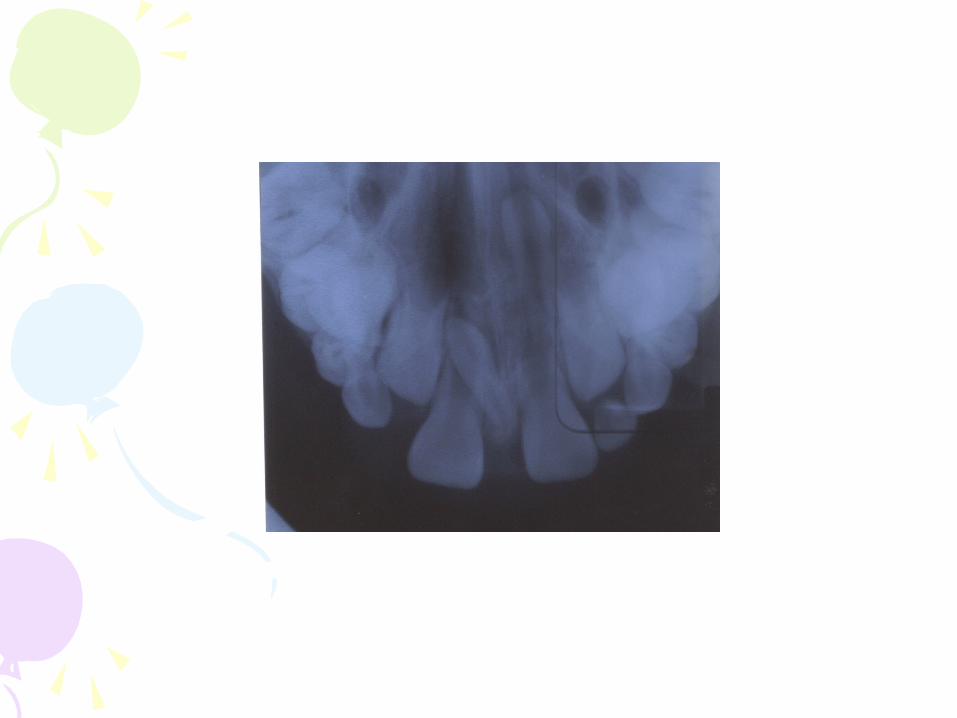
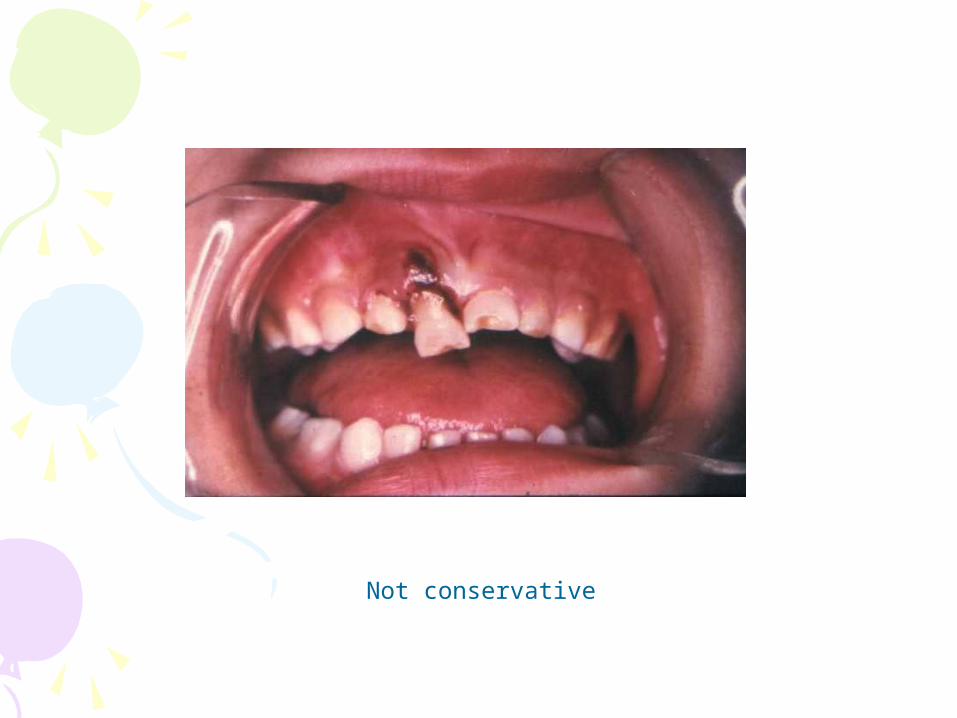
Not conservative
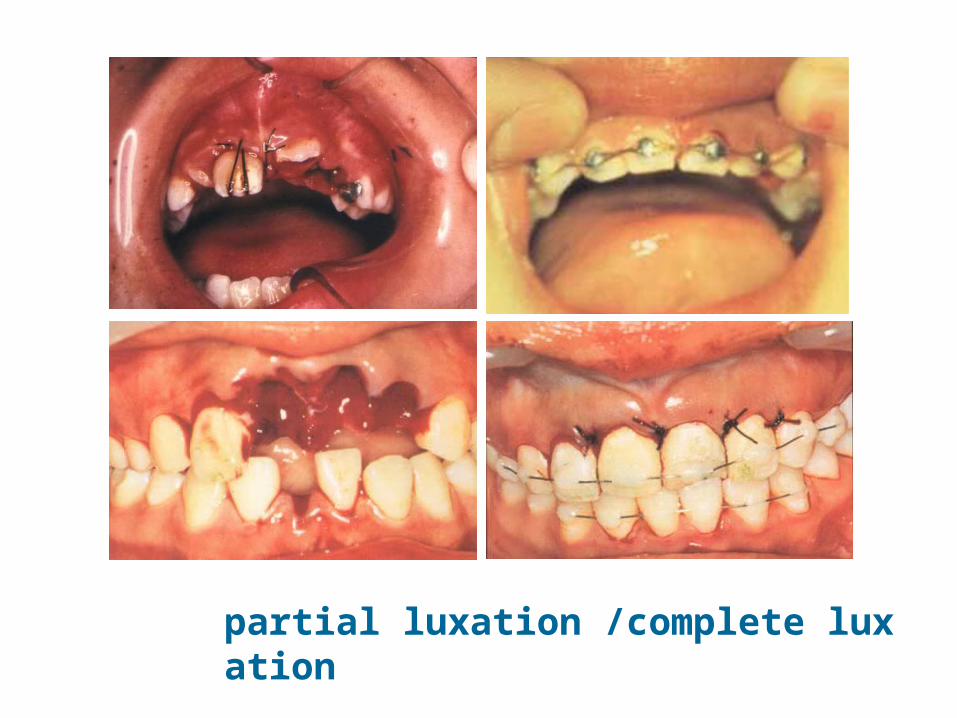
partial luxation /complete luxation

Space maintenanceSteelless crown


Interceptive orthodontics

Pits and fissure sealant