pediatric disaster life support core content lecture 2 practical issues in pediatric disaster...
Post on 22-Dec-2015
218 views
TRANSCRIPT
Pediatric Disaster Life Support
Pediatric Disaster Life Support
Core Content Lecture 2
Practical Issues in Pediatric Disaster Medicine and Preparedness
Andrew L. Garrett, MD
Core Content Lecture 2
Practical Issues in Pediatric Disaster Medicine and Preparedness
Andrew L. Garrett, MD
Goals of this SectionGoals of this Section
Apply the concepts learned in the first section with a focus on the vulnerabilities of children in disaster
To teach specific information which will enhance the practical application of this information
Apply the concepts learned in the first section with a focus on the vulnerabilities of children in disaster
To teach specific information which will enhance the practical application of this information
Goals of this SectionGoals of this Section
To further develop the bio-psycho-social model’s applicability to pediatric disaster medicine and preparedness
To further develop the bio-psycho-social model’s applicability to pediatric disaster medicine and preparedness
Care of theChild During
Disaster
Biological
PsychologicalSoc
ial
Social

Pediatric TriagePediatric Triage
Pediatric TriagePediatric Triage
Triage is the sorting of patients During a disaster, the number of patients
may exceed the amount of medical resources
It is important to allocate the limited resources to those who will most benefit from them
Triage is the sorting of patients During a disaster, the number of patients
may exceed the amount of medical resources
It is important to allocate the limited resources to those who will most benefit from them
Pediatric TriagePediatric Triage
In other words:
To do the most good for the most patients
In other words:
To do the most good for the most patients
Pediatric TriagePediatric Triage
Triage may occur at several points during a disaster The scene of destruction
Mass casualty incident
At a casualty collection point or field hospital At a receiving hospital
Mass casualty receiving
Triage may occur at several points during a disaster The scene of destruction
Mass casualty incident
At a casualty collection point or field hospital At a receiving hospital
Mass casualty receiving
Pediatric TriagePediatric Triage
Triage of children and adults is typically done simultaneously during a disaster
It is important to remember that although the injury process may be the same, a child’s vulnerability to that injury may be very different Specifically, their response to airway
obstruction
Triage of children and adults is typically done simultaneously during a disaster
It is important to remember that although the injury process may be the same, a child’s vulnerability to that injury may be very different Specifically, their response to airway
obstruction
Pediatric TriagePediatric Triage
The standard adult triage tools do not take into account the specific vulnerability that children have to dying from airway obstruction
Children may have a reversible period of respiratory arrest from which they may recover if treated promptly
The standard adult triage tools do not take into account the specific vulnerability that children have to dying from airway obstruction
Children may have a reversible period of respiratory arrest from which they may recover if treated promptly
Pediatric TriagePediatric Triage
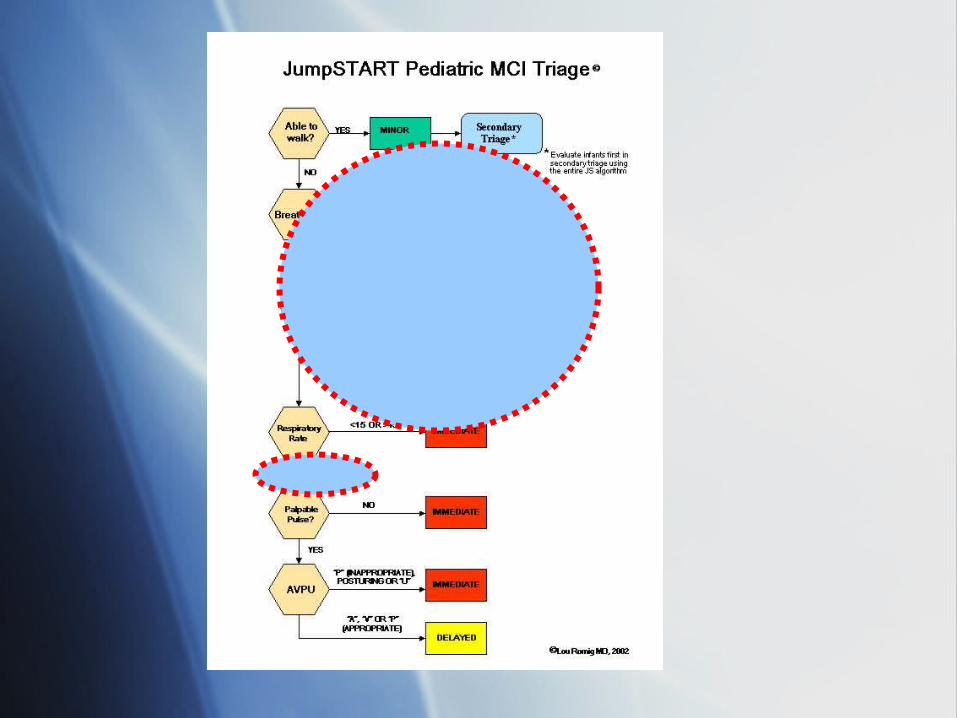
Due to this, a specific pediatric triage tool was developed and tested JumpSTART
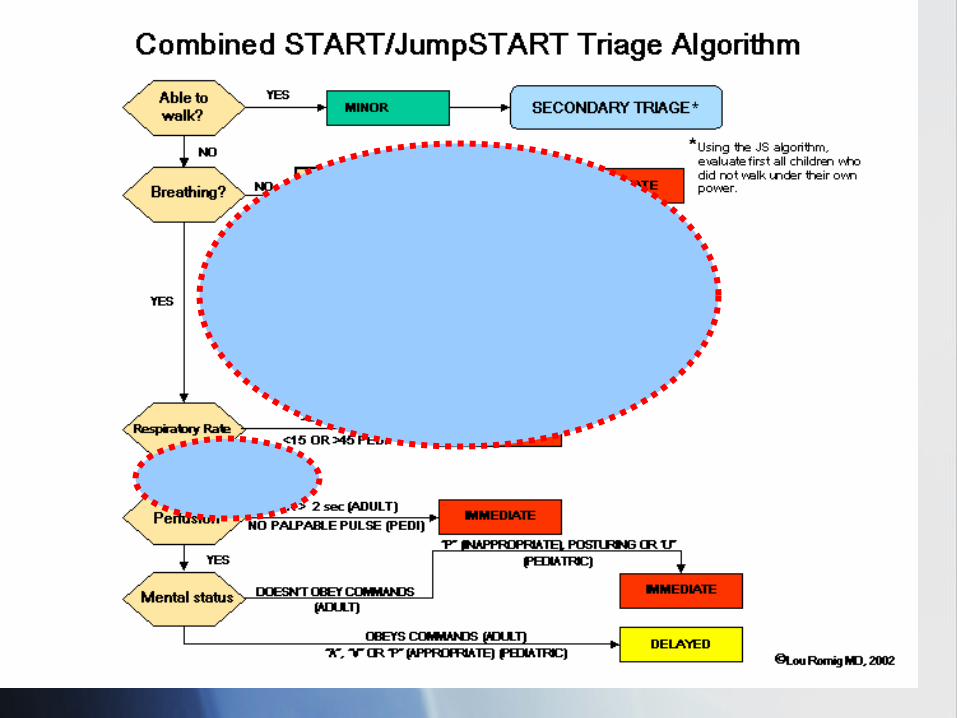
Builds from the concepts of triage taught in START triage, which is commonly utilized
Due to this, a specific pediatric triage tool was developed and tested JumpSTART
Builds from the concepts of triage taught in START triage, which is commonly utilized

START Triage (adults)
Confused?Confused?
If you remember the specific vulnerability children have to airway compromise, this makes sense
The “Jumpstart” term refers to the extra chance we give a child to breathe before we declare them a BLACK TAG
If you remember the specific vulnerability children have to airway compromise, this makes sense
The “Jumpstart” term refers to the extra chance we give a child to breathe before we declare them a BLACK TAG
ExamplesExamples
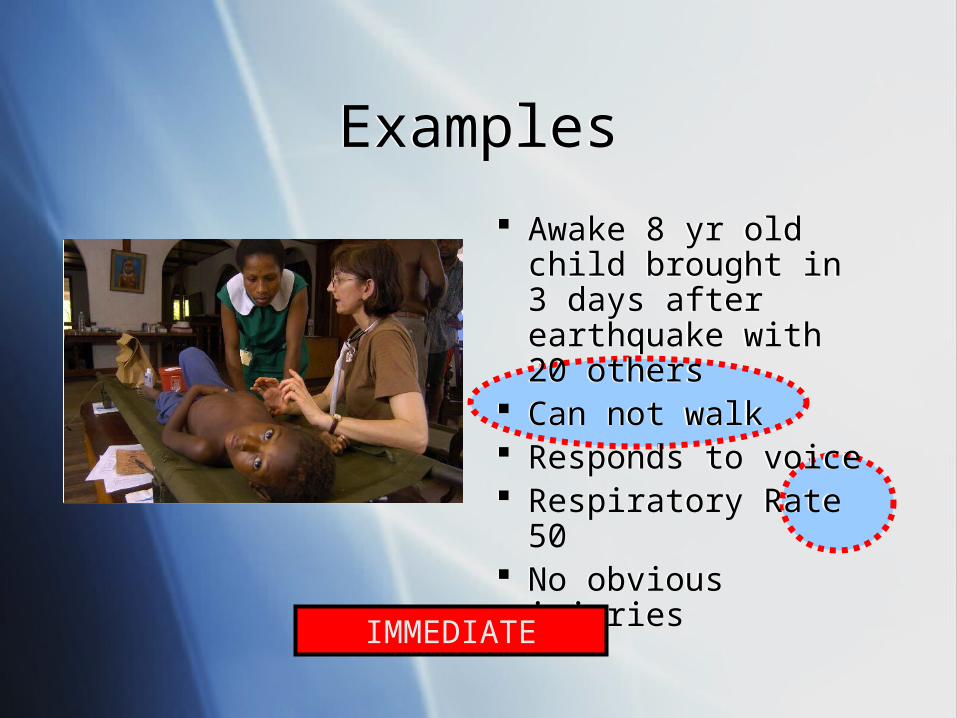
Awake 8 yr old child brought in 3 days after earthquake with 20 others
Can not walk Responds to voice Respiratory Rate 50 No obvious injuries
Awake 8 yr old child brought in 3 days after earthquake with 20 others
Can not walk Responds to voice Respiratory Rate 50 No obvious injuries
IMMEDIATE
ExamplesExamples
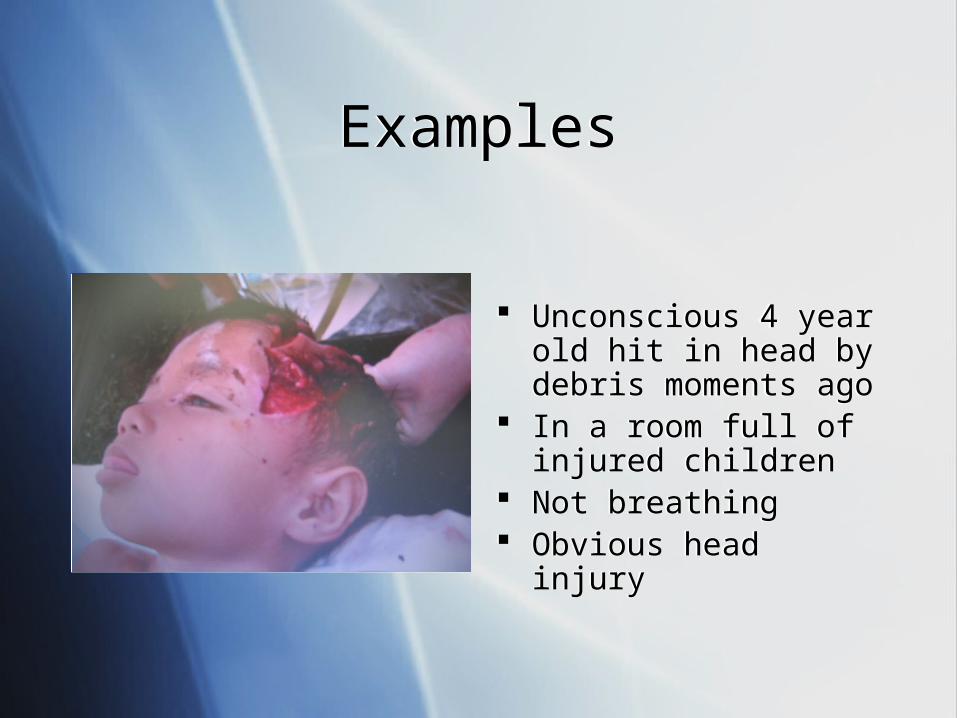
Unconscious 4 year old hit in head by debris moments ago
In a room full of injured children
Not breathing Obvious head injury
Unconscious 4 year old hit in head by debris moments ago
In a room full of injured children
Not breathing Obvious head injury
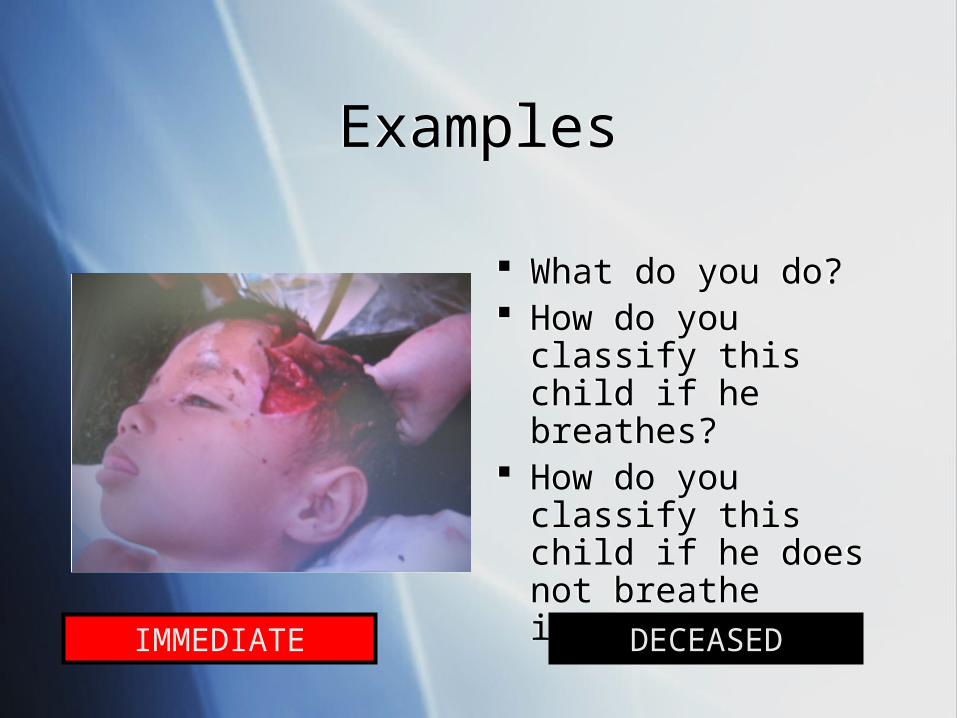
What do you do? How do you classify
this child if he breathes?
How do you classify this child if he does not breathe immediately?
What do you do? How do you classify
this child if he breathes?
How do you classify this child if he does not breathe immediately?
ExamplesExamples
IMMEDIATE DECEASED
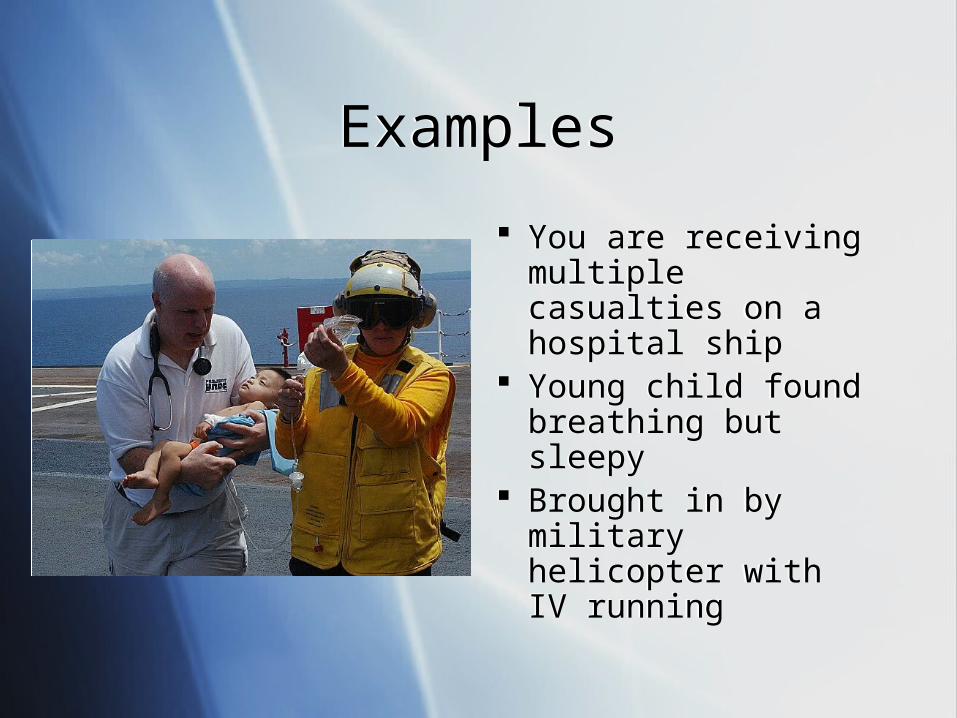
You are receiving multiple casualties on a hospital ship
Young child found breathing but sleepy
Brought in by military helicopter with IV running
You are receiving multiple casualties on a hospital ship
Young child found breathing but sleepy
Brought in by military helicopter with IV running
ExamplesExamples
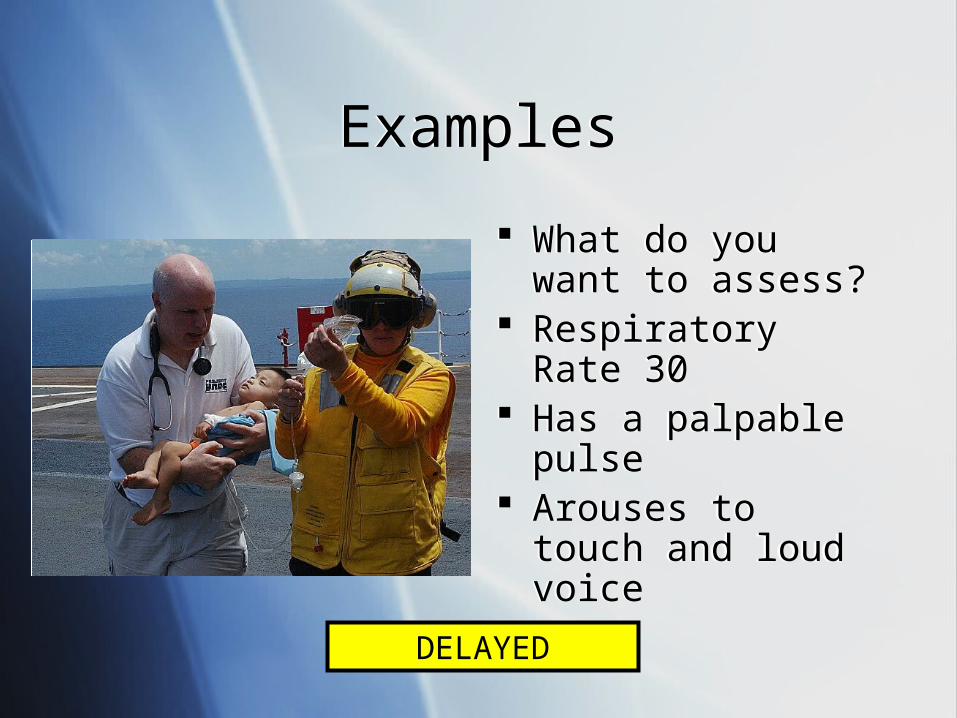
What do you want to assess?
Respiratory Rate 30 Has a palpable pulse Arouses to touch and
loud voice
What do you want to assess?
Respiratory Rate 30 Has a palpable pulse Arouses to touch and
loud voice
ExamplesExamples
DELAYED
Pediatric TriagePediatric Triage
Focus on integration of children in to the triage system
Once a child is classified as a color, quickly move them to a treatment area in order of severity RED first, then YELLOW, then GREEN
Focus on integration of children in to the triage system
Once a child is classified as a color, quickly move them to a treatment area in order of severity RED first, then YELLOW, then GREEN

Children with Special Health Care Needs
Children with Special Health Care Needs

Children with Special Health Care Needs (CSHCN)
Children with Special Health Care Needs (CSHCN)
Children with special medical or physical needs Wheelchair or crutches Learning disability Vision, hearing, or language impaired Technology dependent
Ventilator Dialysis
Children with special medical or physical needs Wheelchair or crutches Learning disability Vision, hearing, or language impaired Technology dependent
Ventilator Dialysis
Children with Special Health Care Needs (CSHCN)
Children with Special Health Care Needs (CSHCN)
Children with Special Health Care Needs (CSHCN)
Children with Special Health Care Needs (CSHCN)
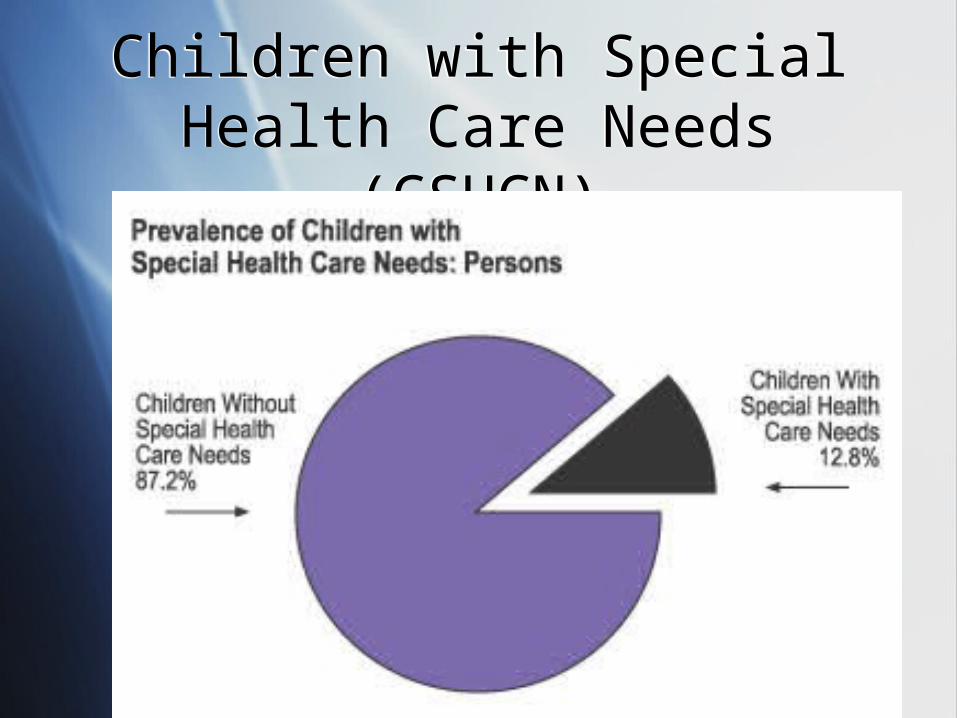
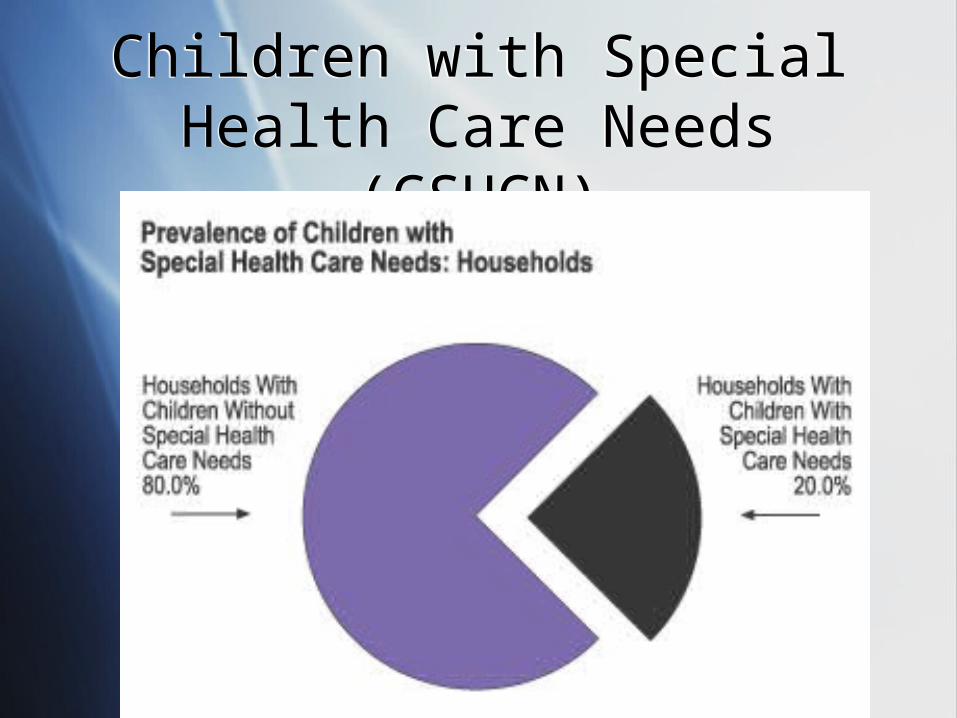
Prevalence of CSHCNPrevalence of CSHCN
Based on a national survey 1 in 5 households self identify as having a
CSHCN Approximately 1 in 8 children are identified by
parents as being CSHCN
Care of these children must be integrated in to the care of all children during a disaster
Based on a national survey 1 in 5 households self identify as having a
CSHCN Approximately 1 in 8 children are identified by
parents as being CSHCN
Care of these children must be integrated in to the care of all children during a disaster
Special Challenges for CSHCNSpecial Challenges for CSHCN
Sheltering Controversy: Together or separately? Controversy: Should CSHCN be considered medical
patients if they are not injured or ill?
Decontamination What is the best way to decontaminate medical
hardware such as a wheelchair? How do we decontaminate technology, such as a
ventilator?
Sheltering Controversy: Together or separately? Controversy: Should CSHCN be considered medical
patients if they are not injured or ill?
Decontamination What is the best way to decontaminate medical
hardware such as a wheelchair? How do we decontaminate technology, such as a
ventilator?
Special Challenges for CSHCNSpecial Challenges for CSHCN
Transportation Take equipment with or leave behind during
evacuation?
For all of these topics, special advance planning is required to be successful in taking care of all children
Transportation Take equipment with or leave behind during
evacuation?
For all of these topics, special advance planning is required to be successful in taking care of all children
Sheltering for ChildrenSheltering for Children
Hurricane Katrina taught us many harsh lessons about how important shelter planning is
Hurricane Katrina taught us many harsh lessons about how important shelter planning is
Sheltering IssuesSheltering Issues
Hygiene Children pose a special risk to maintaining
hygiene in a shelter operation Basic supplies such as wipes and diapers
frequently overlooked Children are at a special risk of acquiring
gastrointestinal and respiratory diseases Children are exceptionally good at spreading
these diseases Must plan for handwashing/sanitizing
Hygiene Children pose a special risk to maintaining
hygiene in a shelter operation Basic supplies such as wipes and diapers
frequently overlooked Children are at a special risk of acquiring
gastrointestinal and respiratory diseases Children are exceptionally good at spreading
these diseases Must plan for handwashing/sanitizing
Sheltering IssuesSheltering Issues
Safety and Supervision Shelters are dangerous environments Rarely childproofed Children move quickly throughout environment Easy to get lost Possible criminal element
Safety and Supervision Shelters are dangerous environments Rarely childproofed Children move quickly throughout environment Easy to get lost Possible criminal element
Sheltering IssuesSheltering Issues
Health Maintenance Clean water and healthy food a challenge Children require something to do
Consider a recreational therapy group Children require more sleep
Shelters are frequently loud Pediatric Health Screening important
Prevention of disease Maintaining primary care for extended stays
Health Maintenance Clean water and healthy food a challenge Children require something to do
Consider a recreational therapy group Children require more sleep
Shelters are frequently loud Pediatric Health Screening important
Prevention of disease Maintaining primary care for extended stays

DecontaminationDecontamination
Decontamination of ChildrenDecontamination of Children
Special issues must be accounted for before undertaking decontamination of children
Advance planning will make the difference Goal is to integrate care of children with
that of the general population
Special issues must be accounted for before undertaking decontamination of children
Advance planning will make the difference Goal is to integrate care of children with
that of the general population
Decontamination of ChildrenDecontamination of Children
Parents After a disaster or major emergency, most
parents will not separate from their children Decontamination patient flow must account for
this Takes longer than expected to decontaminate
parent and child
Parents After a disaster or major emergency, most
parents will not separate from their children Decontamination patient flow must account for
this Takes longer than expected to decontaminate
parent and child
Decontamination of ChildrenDecontamination of Children
Temperature Extremes Decontamination water must not be ice cold for
young children Risk of hypothermia, especially in winter Children must be covered immediately
Risk of injury if too hot or chemicals used Do not use bleach in decon water Do not use rough scrubbing devices
Temperature Extremes Decontamination water must not be ice cold for
young children Risk of hypothermia, especially in winter Children must be covered immediately
Risk of injury if too hot or chemicals used Do not use bleach in decon water Do not use rough scrubbing devices
Decontamination of ChildrenDecontamination of Children
Special Equipment Have a plan for special equipment on children
or adults Wheelchairs Electronic equipment Firearms
Special Equipment Have a plan for special equipment on children
or adults Wheelchairs Electronic equipment Firearms
Decontamination of ChildrenDecontamination of Children
Special Issues How long does it take a child to take a shower
or bath normally? Children may not be cooperative Children will likely be frightened with
protective suits How do you track a non-verbal, naked child
after decontamination?
Special Issues How long does it take a child to take a shower
or bath normally? Children may not be cooperative Children will likely be frightened with
protective suits How do you track a non-verbal, naked child
after decontamination?
Chemical and Biologic AgentsChemical and Biologic Agents
Chem/Bio ResponseChem/Bio Response
Frequently lumped together
Each will present to a different group and on a different timeline
Frequently lumped together
Each will present to a different group and on a different timeline
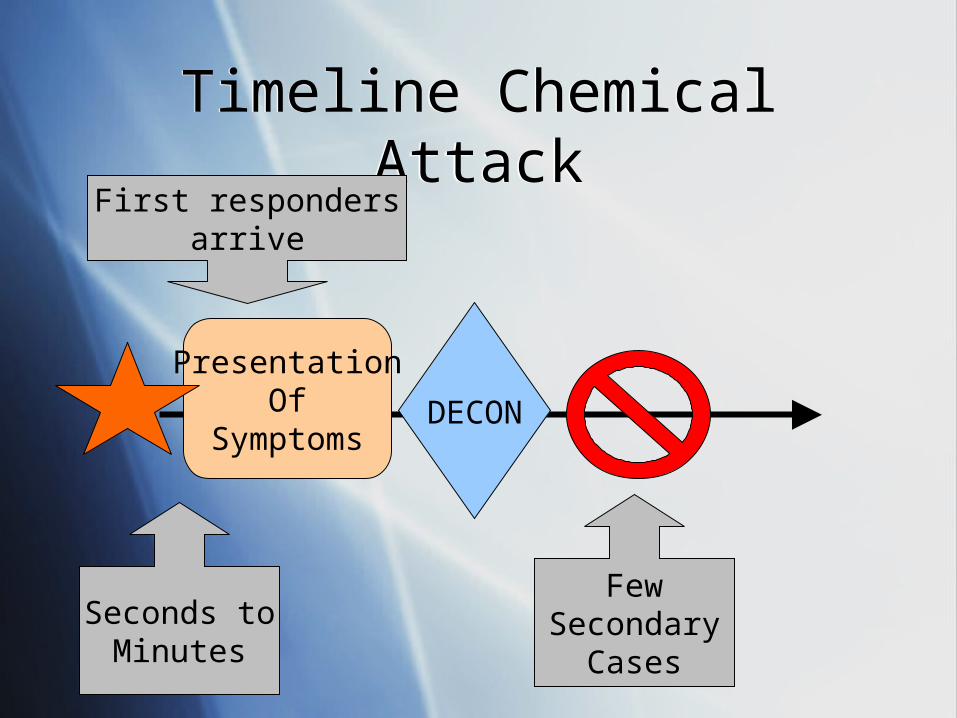
Timeline Chemical AttackTimeline Chemical Attack
PresentationOf
Symptoms
Seconds toMinutes
First respondersarrive
DECON
FewSecondary
Cases
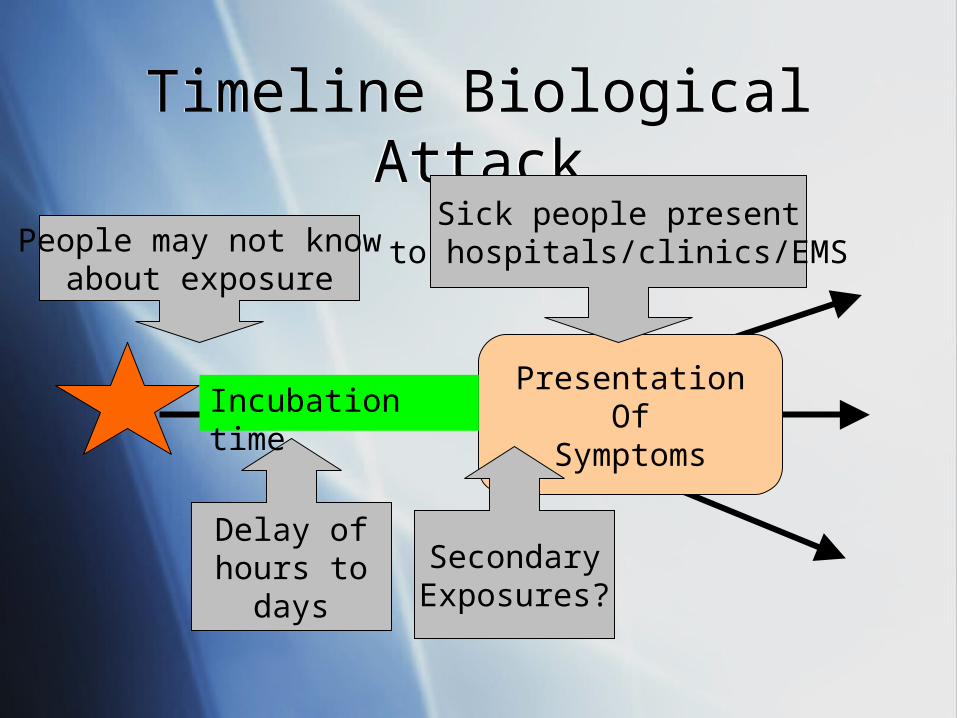
Timeline Biological AttackTimeline Biological Attack
PresentationOf
Symptoms
Delay ofhours to
days
People may not knowabout exposure
SecondaryExposures?
Sick people presentto hospitals/clinics/EMS
Incubation time
Biological AgentsBiological Agents
Category A Category B Category C
Smallpox Anthrax Plague Botulism Tularemia Ebola Marburg
Q Fever Brucellosis Glanders Melioidosis VEE Ricin SEB Cholera
Nipah Hantavirus Yellow Fever MDRTB TBE
Category A Category B Category C
Smallpox Anthrax Plague Botulism Tularemia Ebola Marburg
Q Fever Brucellosis Glanders Melioidosis VEE Ricin SEB Cholera
Nipah Hantavirus Yellow Fever MDRTB TBE
Biological AgentsBiological Agents
Category A
Smallpox Anthrax Plague Botulism Tularemia Ebola Marburg
Category A
Smallpox Anthrax Plague Botulism Tularemia Ebola Marburg
• Most Cat. A agents are detectable in their full-blown form
• Characteristic symptoms, X-rays, or progression
• Lab evaluation not typically rapid
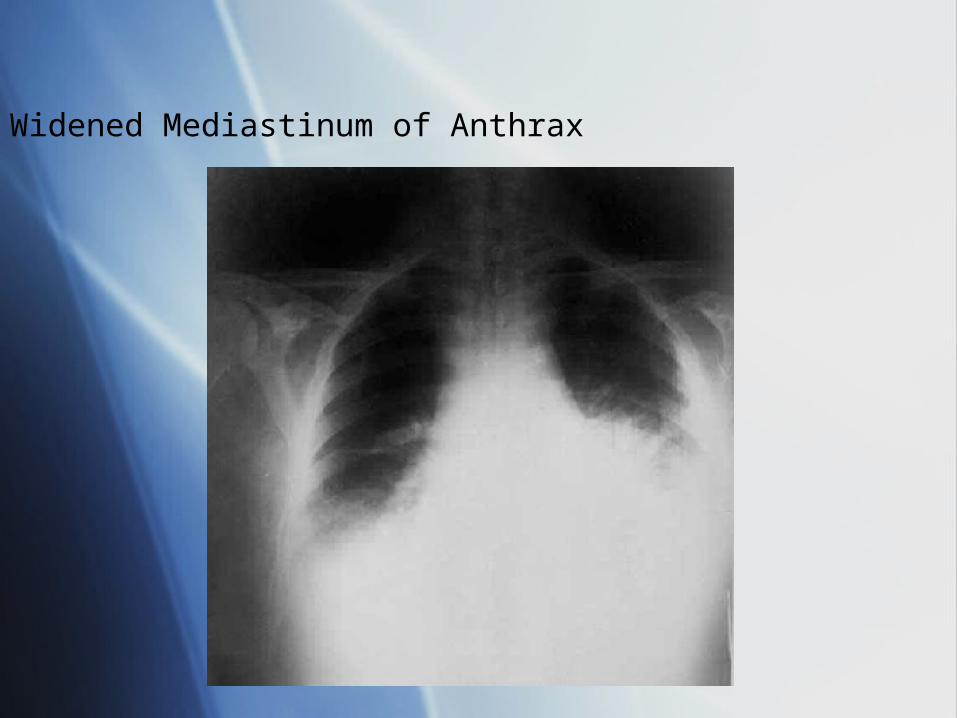
Widened Mediastinum of Anthrax
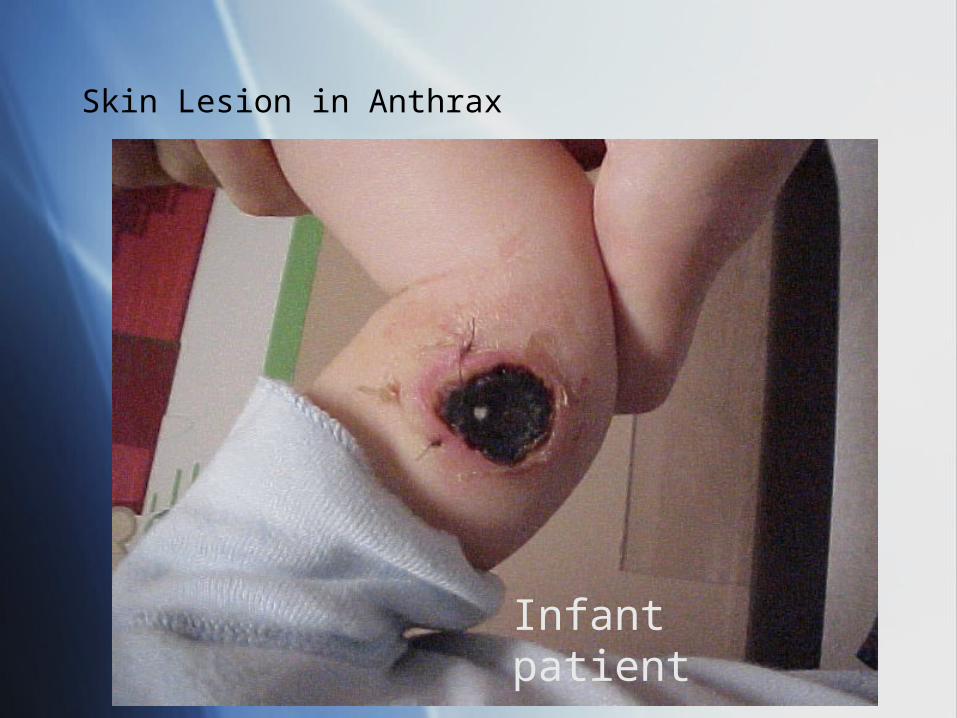
Skin Lesion in Anthrax
Infant patient
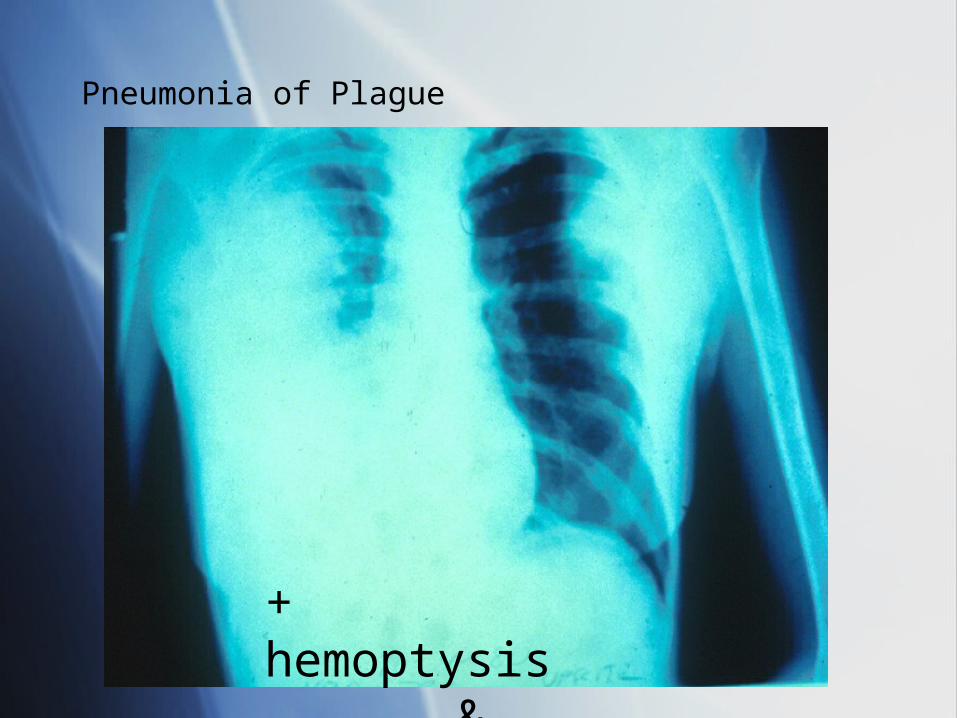
Pneumonia of Plague
+ hemoptysis & fever
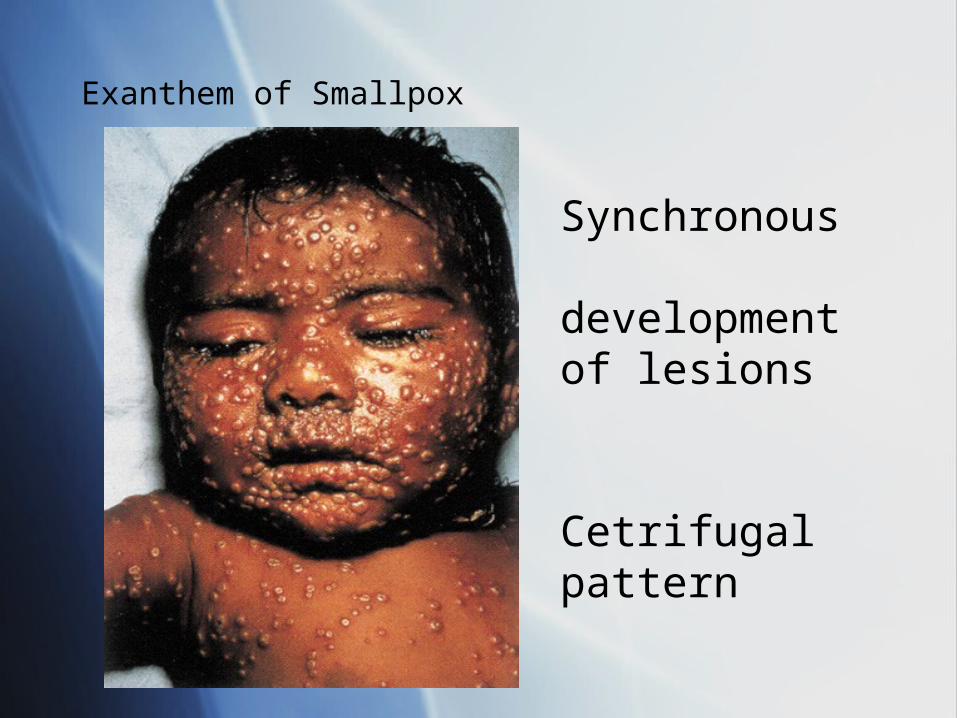
Exanthem of Smallpox
Synchronous development of lesions
Cetrifugal pattern
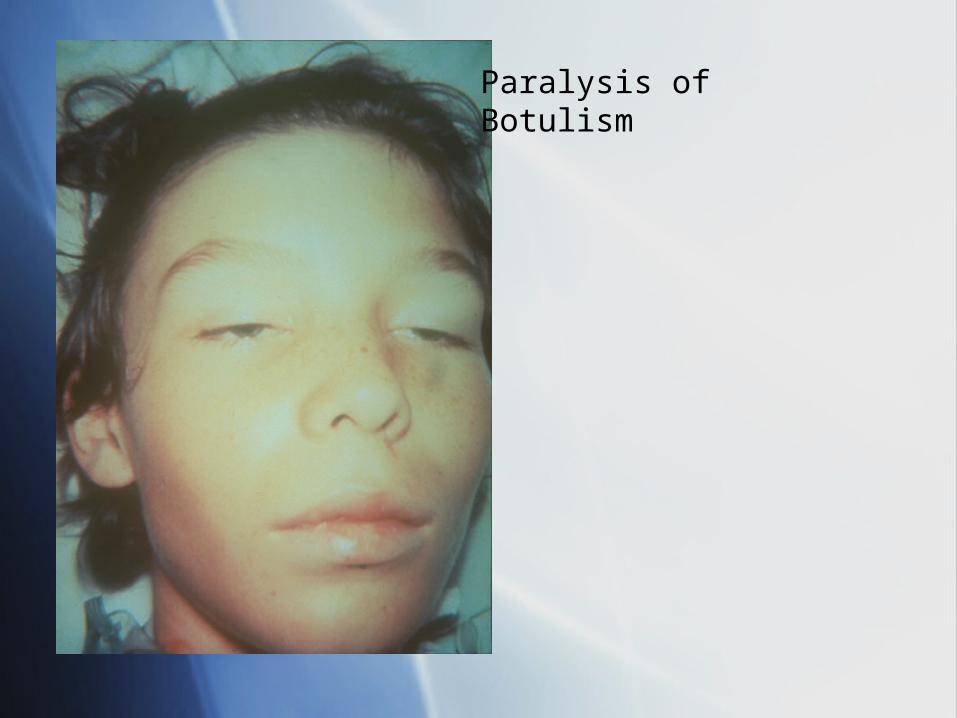
Paralysis ofBotulism
Chemical Terrorism:Which Agents?
Chemical Terrorism:Which Agents?
“Military Grade” Agents Nerve Agents “Blister Agents” (Vesicants) “Blood Agents” (Cyanides) “Choking Agents” (Phosgene, Chlorine)
Weapons of Opportunity Toxic Industrial Chemicals
“Military Grade” Agents Nerve Agents “Blister Agents” (Vesicants) “Blood Agents” (Cyanides) “Choking Agents” (Phosgene, Chlorine)
Weapons of Opportunity Toxic Industrial Chemicals
“Military Grade” Agents Nerve Agents “Blister Agents” (Vesicants) “Blood Agents” (Cyanides) “Choking Agents” (Phosgene, Chlorine)
Weapons of Opportunity Toxic Industrial Chemicals
“Military Grade” Agents Nerve Agents “Blister Agents” (Vesicants) “Blood Agents” (Cyanides) “Choking Agents” (Phosgene, Chlorine)
Weapons of Opportunity Toxic Industrial Chemicals
Chemical Terrorism:Which Agents?
Chemical Terrorism:Which Agents?
Increased surface area/volume more absorptive surface more susceptible to volume losses
Increased minute ventilation Thinner epidermis Under-keratinized epidermis Increased absorption Immature blood-brain barrier
Increased surface area/volume more absorptive surface more susceptible to volume losses
Increased minute ventilation Thinner epidermis Under-keratinized epidermis Increased absorption Immature blood-brain barrier
Vulnerabilities of Children to Bio/Chem Agents
Vulnerabilities of Children to Bio/Chem Agents
VEE-- increased morbidity in children Smallpox-- lack of immunity Trichothecenes-- more susceptible ? Melioidosis-- unique parotitis Anthrax-- ?? Less susceptible
VEE-- increased morbidity in children Smallpox-- lack of immunity Trichothecenes-- more susceptible ? Melioidosis-- unique parotitis Anthrax-- ?? Less susceptible
Specific Vulnerabilities to Specific Diseases
Children Do Not Fit the Treatment Mold
Children Do Not Fit the Treatment Mold
The two main antibiotics used to treat biowarfare agents are not typically used in children Ciprofloxacin and Doxycycline
In the opinion of experts, however, their use is warranted if there is a realistic risk of exposure to a biowarfare agent
The two main antibiotics used to treat biowarfare agents are not typically used in children Ciprofloxacin and Doxycycline
In the opinion of experts, however, their use is warranted if there is a realistic risk of exposure to a biowarfare agent
CiprofloxacinCiprofloxacin
First line treatment for: Anthrax Plague
First line treatment for: Anthrax Plague
DoxycyclineDoxycycline
First line treatment for: Anthrax Plague Tularemia Brucellosis Q Fever
First line treatment for: Anthrax Plague Tularemia Brucellosis Q Fever
Vaccination IssuesVaccination Issues
Anthrax vaccine not approved in children under 18
Plague vaccine (not currently in production) not approved in children
Smallpox and Yellow Fever vaccine produces more complications in kids
Anthrax vaccine not approved in children under 18
Plague vaccine (not currently in production) not approved in children
Smallpox and Yellow Fever vaccine produces more complications in kids
Other ConsiderationsOther Considerations
Underavailability of chemical and biological antidotes for children
Poor access to nerve agent autoinjector (Mark 1 kit) or pediatric Atropen™ Recently approved by FDA
National Disaster Medical System does not account for pediatric bedspace
Underavailability of chemical and biological antidotes for children
Poor access to nerve agent autoinjector (Mark 1 kit) or pediatric Atropen™ Recently approved by FDA
National Disaster Medical System does not account for pediatric bedspace

Atropen™ and Mark-1 kitAtropen™ and Mark-1 kit
Kit with Atropine AND
PralidoximePediatric Atropine autoinjectorsPediatric Atropine autoinjectors
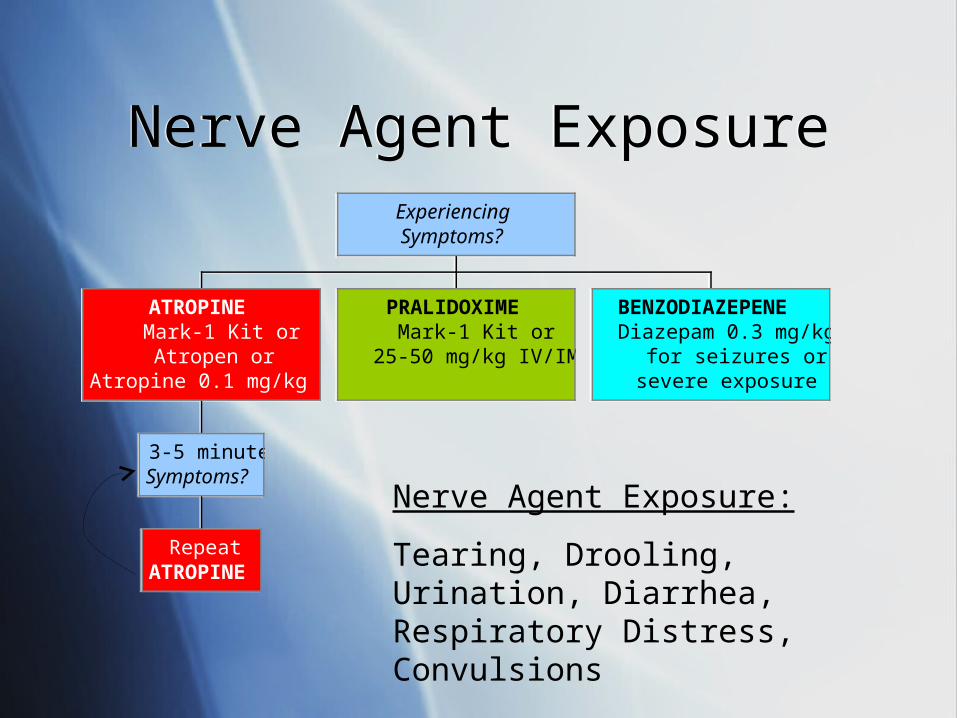
Nerve Agent ExposureNerve Agent Exposure
RepeatATROPINE
3-5 minutesSymptoms?
ATROPINEMark-1 Kit orAtropen or
Atropine 0.1 mg/kg IV/IM
PRALIDOXIMEMark-1 Kit or
25-50 mg/kg IV/IM
BENZODIAZEPENEDiazepam 0.3 mg/kg
for seizures orsevere exposure
ExperiencingSymptoms?
RepeatATROPINE
3-5 minutesSymptoms?
ATROPINEMark-1 Kit orAtropen or
Atropine 0.1 mg/kg IV/IM
PRALIDOXIMEMark-1 Kit or
25-50 mg/kg IV/IM
BENZODIAZEPENEDiazepam 0.3 mg/kg
for seizures orsevere exposure
ExperiencingSymptoms?
Nerve Agent Exposure:
Tearing, Drooling, Urination, Diarrhea, Respiratory Distress, Convulsions
Nerve Agent ExposureNerve Agent Exposure
Atropen™ does not contain Pralidoxime Important in the treatment to reverse action of nerve
agent
Any symptomatic child should receive a Mark-1 kit unless alternatives are immediately available The risk of side effects is greatly outweighed by the
benefits Do not delay treatment
Atropen™ does not contain Pralidoxime Important in the treatment to reverse action of nerve
agent
Any symptomatic child should receive a Mark-1 kit unless alternatives are immediately available The risk of side effects is greatly outweighed by the
benefits Do not delay treatment
Summary of Bio/ChemSummary of Bio/Chem Good Biological & Chemical medical
defense requires a high index-of-suspicion on the part of clinicians
Children have unique vulnerabilities Primary Care Providers are likely to be first
responders to a Biological attack Pediatric Treatment Guidelines are now
available to assist the clinician
Good Biological & Chemical medical defense requires a high index-of-suspicion on the part of clinicians
Children have unique vulnerabilities Primary Care Providers are likely to be first
responders to a Biological attack Pediatric Treatment Guidelines are now
available to assist the clinician

ResourcesResources
PDLS is a start Much information exists to guide the
preparation and care for children in disasters
PDLS is a start Much information exists to guide the
preparation and care for children in disasters
ResourcesResources
U.S. Center for Disease Control www.cdc.gov
National Center for Disaster Preparedness http://www.ncdp.mailman.columbia.edu/
American Psychological Association www.apa.org
U.S. Center for Disease Control www.cdc.gov
National Center for Disaster Preparedness http://www.ncdp.mailman.columbia.edu/
American Psychological Association www.apa.org
ResourcesResources
JumpSTART Triage Tool www.jumpstarttriage.org
American Academy of Pediatrics http://www.aap.org/terrorism/topics/disaster_planning.html
Pediatric Disaster Preparedness Consensus Conference Summary http://www.bt.cdc.gov/children/pdf/working/execsumm03.pdf
U.S. Department of Homeland Security www.dhs.gov
JumpSTART Triage Tool www.jumpstarttriage.org
American Academy of Pediatrics http://www.aap.org/terrorism/topics/disaster_planning.html
Pediatric Disaster Preparedness Consensus Conference Summary http://www.bt.cdc.gov/children/pdf/working/execsumm03.pdf
U.S. Department of Homeland Security www.dhs.gov
DisclaimerDisclaimer
The information herein should NOT be used as a substitute of an appropriately certified and licensed physician or health care provider. The information herein is provided for educational and informational purposes only and in no way should be considered as an offering of medical advice. The authors, editors, and publisher of this site have used reasonable efforts to provide up-to-date, accurate information that is within generally accepted medical standards at the time of production. However, as medical science is ever evolving, and human error is always possible, PDLS does not guarantee total accuracy or comprehensiveness of the information on this site, nor are they responsible for omissions, errors, or the results of using this information. The reader should confirm the accuracy of the information in this article from other sources. In particular, all drug doses, indications, and contraindications should be confirmed in package inserts.
The information herein should NOT be used as a substitute of an appropriately certified and licensed physician or health care provider. The information herein is provided for educational and informational purposes only and in no way should be considered as an offering of medical advice. The authors, editors, and publisher of this site have used reasonable efforts to provide up-to-date, accurate information that is within generally accepted medical standards at the time of production. However, as medical science is ever evolving, and human error is always possible, PDLS does not guarantee total accuracy or comprehensiveness of the information on this site, nor are they responsible for omissions, errors, or the results of using this information. The reader should confirm the accuracy of the information in this article from other sources. In particular, all drug doses, indications, and contraindications should be confirmed in package inserts.
Course DirectorsCourse Directors
PDLS 2.0 content revision- March 2006 Andrew L. Garrett MD, FAAP Richard V. Aghababian, MD, FACEP
University of Massachusetts Medical School
PDLS course- 1999 Richard V. Aghababian MD, FACEP
PDLS 2.0 content revision- March 2006 Andrew L. Garrett MD, FAAP Richard V. Aghababian, MD, FACEP
University of Massachusetts Medical School
PDLS course- 1999 Richard V. Aghababian MD, FACEP
Original ContributorsOriginal Contributors
Gregory Ciottone, MD Lucille Gans, MD Patricia Hughes, RN Frank Jehle, MD Taryn Kennedy, MD Gretchen Lipke, MD Mariann Manno, MD Gina Smith, RN Fred Henretig, MD Theodore Cieslak, MD
Gregory Ciottone, MD Lucille Gans, MD Patricia Hughes, RN Frank Jehle, MD Taryn Kennedy, MD Gretchen Lipke, MD Mariann Manno, MD Gina Smith, RN Fred Henretig, MD Theodore Cieslak, MD
Robert McGrath, M.Ed. W. Peter Metz, MD John A. Paraskos, MD Carol Shustak, RN Elizabeth Shilale, RN A. Richard Starzyk Michael Weinstock, MD Sharon Welsh, RN Lou Romig, MD
Robert McGrath, M.Ed. W. Peter Metz, MD John A. Paraskos, MD Carol Shustak, RN Elizabeth Shilale, RN A. Richard Starzyk Michael Weinstock, MD Sharon Welsh, RN Lou Romig, MD