per wretenberg - ki · artificial hip prosthesis in acute and non-union fractures of femoral neck...
TRANSCRIPT

Protesnära fraktur
Per Wretenberg

Problemet

Historik
Första beskrivningen 1954
Artificial hip prosthesis in acute and non-union
Fractures of femoral neck
Horwitz et al. JAMA 155; 564-567 1954

Historik
Traktionsbehandling, 3 månaders balanserat sträck
The healing of human fractures in contact with
acrylic cement
Charnley J. Clin Othop 47; 157-163, 1966

Incidence
1 - 2% after primary THR (increasing)
4 - 20% after revision THR
Kavanagh, JBJS (Br) 2002

Incidence
0.1 – 1% after Cemented THR
Kavanagh, Clin Orthop North Am, 2002
5.4% after uncemenetd THR
Berry, Clin Orthop, 2009

Incidence
Totala incidensen ökar
något.
Lindahl H, The periphrostetic femur fracture 2006 (Thesis)

Periprostetsik fraktur
Intraoperativt
jämfört med cementerad primärplastik
- större risk vid ocementerad protes
- större risk efter revisionevisioner
- större risk vid benpackning?
Postoperative
- trauma
- osteolysis
- tumör

Postop. rtg
Problem?


Reoperation
5 dagar senare

Riskfaktorer
Lös protes
Kvinnor
Metabola bensjukdomar
Osteoporos
RA
Preoperativ deformering av femur
Ocementerad protes

Vancouver classification
Type A: Trochanteric fractures
Type B: Fracture at stem level or just under the stem
Type C: Fracture distal to the stem

Type B fracture
B1: Stable prosthesis
B2: Loose prosthesis, good bone
B3: Loose prosthesis, bad bone

Vancouver classification
A = Type A
B = Type B1
C = Type B2
D = Type B3
E = Type C

Bone defects
Endolink classification

Vancouver classification reliability
Reliable classification,
Brady et al J Arthroplasty vol. 15(1) 2000

Vancouver classification reliability
Intra-observer k-value 0.77
Inter-observer k-value 0.64
K-value 0.10-0.20 = slight agreement
0.21-0.40 = fair
0.41-0.60 = moderate
0.61-0.80 = substantial
> 0.80 = almost perfect

Treatment of periprosthetic fractures
Nonoperativ
• Traction
• Orthosis
• None
» No adequate studies performed

Treatment
Vancover A
• Non operative, mobilization
• Fixation with screws
• Fixation with cables
• Fixation with plate and screws

Treatment
Vancover C
• Fixation with plate and screws
• Fixation with cables
• Fixation with nails
• (Fixation with screws alone)

Female
72-years
Vancover C


Treatment
Vancover B1
• Cables (prox undisplaced fracture)
• Plate and screw, and or cables
• Mennen plate
• Strut graft with or without plate
• Strut graft and bone packing
• Revision THA

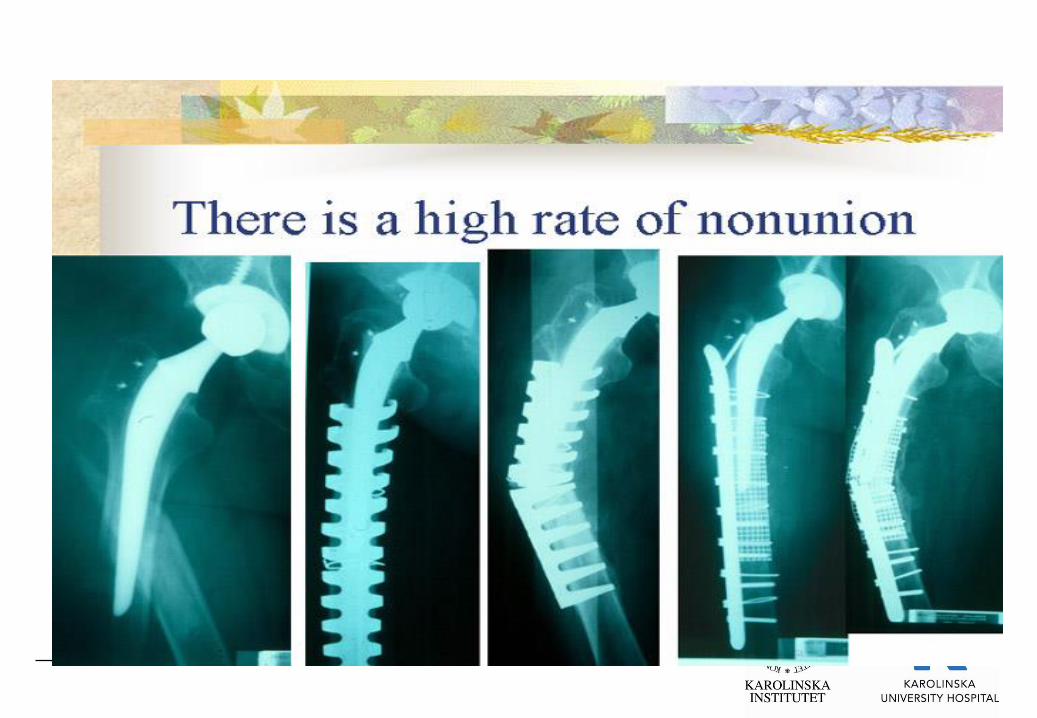
Platefixation
• Good/exact reposition possible
• Early mobilisation
• Partial (or full) weight bearing
• Risk of devsacularisation
• Bone resorption under plate
• Cement influenced by screws?
• Plate fracture
• Non union !
+
-

Technique
• Good exposure of fracture site needed
• Reduction and preliminary fixation
• Plate adjustment
• Combination of screws, angular stable screws and cables
• With angular stable plates, less invasive technique is
possible.

74 year male, Vancover B1
Bra
funktion
efter
9 år

1 month postop 10 years postop
73-year male, Vancover B1

63-year female, Vancover B1, op 1994
New x-rays from Irak, 2010,
Good
function

79-year female, Vancover B1

4 months postop. 8 years postop
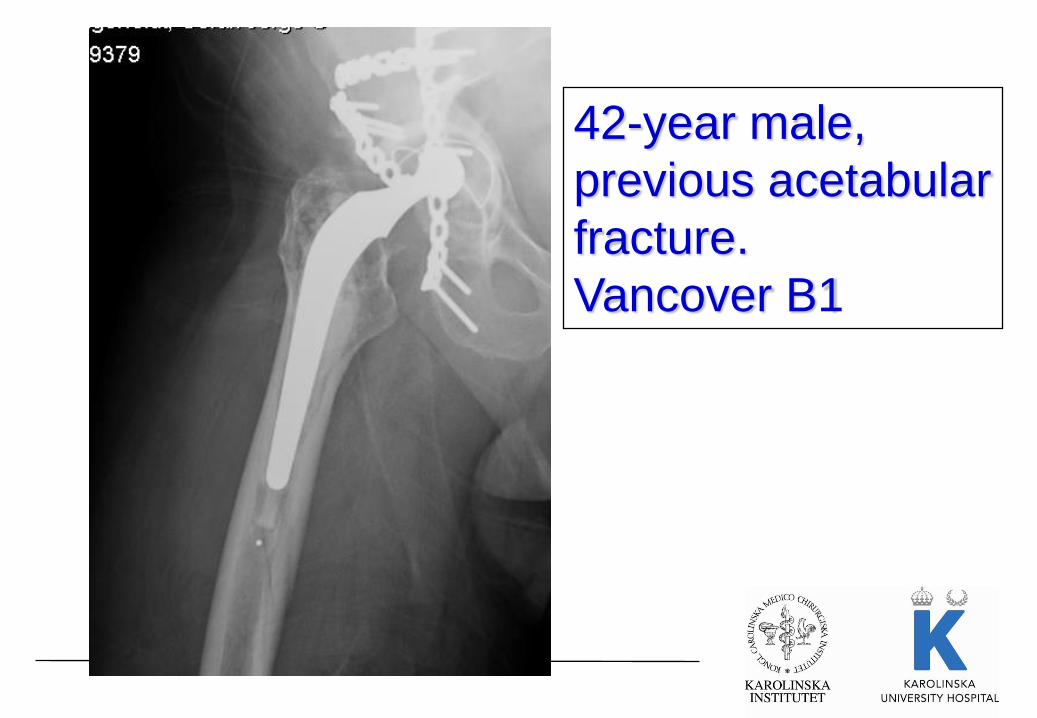
42-year male,
previous acetabular
fracture.
Vancover B1


Vinkelstabil platta
Vancover B1

94-årig kvinna, Vancover B1

Platefixation
Mont et al J Arthroplasty vol 9(5) 1994
Review of litterature 1964-1991
487 patients, 26 articles
Plate fixation not as good as revision arthroplasty

I USA har det varit mycket vanligt med
kombination platta-allograft, nu visar dom
bra resultat med bara platta

Vinkel-
stabila
plattor
fungerer

Mennen plate
Not ment for rigid fixation
Space between plate and bone to not disturbe cirkulation
Results?

Mennen plate

Cortical onlay strut allografts
Cortical onlay strut allografts
Good stability
Stimulate fracture healing
Can be incorporated in host bone and increase bone mass
Create less stress-shielding than plates
Expensive, hard to get
Reduced strength of graft after 4-6 months
Initial weigh bearing not recommended
+
-

Technique
Chandler et al JBJS 79A(9) 2012, from instructional course lecture AAOS
Femur allograft best
Divide allograft in two halves
Place allograft not less than 10 cm distal to the fracture site
4 cables on each side of the fracture
Place bone graft from host at the fracture site
Full weight bearing after 3 months

Cortical allografts, results
Haddad et al JBJS 84A(6) 2002
Multicenterstudy (4 centra)
40 patients op 1992-1996
Prosthesis well fixed, no need for revision
19 patients treated with only 1 strut allograft
21 patients treated with 1 or 2 allografts and plate
27 hips revised earlier
Reduced weight bearing 3 moths

Haddad et al,
Follow-up 6-78 months (mean 28 months)
39 of 40 fractures healed
radiograficaly

Treatment
Vancover B2, B3
•Revision THA

When the prosthesis is loose,
revision is necessary

The problem
How do we know
that the prosthesis is
loose?
Exposure!

Revision of prosthesis
Options
1. Cemented revision
2. Uncemented revision

Revision of prosthesis
Cemented revision
1. Option for older patients with less physical demand
2. Option for patients with pathological fracture
3. Good and stable reposition of the fracture must be possible
before cementing the prosthesis in place.
4. Long stem needed to bypass the fracture

Revision of prosthesis
Uncemented revision with distal fixation
1. Younger patients with higher physical demands
2. Complex fractures

55-year male, Vancover B2
Cemented
revision with
long stem

55-year female, Vancover B2

Postop 5 years postop

75-year male, Vancover B2
Wagner

Postop 10 yeras postop

84-year male, Vancover B3
4 – years post op.

Male 67-years, Vancover B2

MP-Link
1 year postop

MP-Link
59-year female, Vancover B2

Female, 55-years, Vancover B1??

3 months later…

MP-Link reconstruction

After 1 year
New bone formation

Male, 47 – years, Vancover B2

MP-Link reconstruction

MP-technique for fracture cases
• Exposure easy proximal, additional osteotomy could be done
• Distal cement must be extracted
• Prophylactic cables distally
• Positioning of stem and trial reduction could be done without
reduction of the proximal fragments
• Proximal fragments fixed with cables around stem

Resultat

Slutsatser
1. Majoriteten av patienter som fick en periprostetisk fraktur
hade redan en lös stam.
2. Implantat relaterade faktorer finns med överrisk för Charnley
och Exeter stammar av de cementerade.
3. Generellt dåliga resultat efter op. oavsett metod. Hög
reoperations frekvens och många komplikationer.

Kvinna född 1956,
HIV, op 4 år sedan

Revision med förtur
för att förhindra
fraktur


Slutsatser
1. B1 frakturer hade sämst resultat troligen beroende på att
stammen inte satt fast.
2. Exploration av stammen rekommenderas vid minsta tvekan
om stammen är lös. Är den ”misstänkt lös” => revidera!!
3. Mycket hög komplikationsrisk för plattfixation, troligen
beroende på att många patienter med lös protes
plattfixerades.
4. Fler infektioner vid plattosteosyntes än revision. Orsak? Fick
revisionerna mer antibiotika?

83-year male, Vancover B1??

Male 42-years, Vancover B1??

Completely stable prosthesis when
exposed => B1!, plate fixation possible

Female, 78 years. Vancover B1?

Completely unstable prosthesis when
exposed => B2!; revision

Tack!!