pharmaceutical regulations drive
TRANSCRIPT

Pharmaceutical Regulations Drive
Obaid Ali, R. Ph. Ph. D. & Roohi B. ObaidCivil Services Officer, Government of Pakistan
14th April 2016, Thursday, Karachi

DISCLAIMER
Not the view of DRAP
Current judgment
No obligation on DRAP
Regulatory experience
It has nothing to do with any specific commercial
product
It is just a knowledge sharing exercise nothing
more than that

The quality and especially the sterility of products manufactured cannot be assured

The quality and especially the sterility of products manufactured cannot be assured
April 2016

Background
Inspector’s Eyes
From History
Pariculates

Background


A strict definition of sterility is the complete absence of life or inability to reproduce
• Cont’d
However, sterility as defined in the pharmaceutical industry has a more complex technical definition, and is expressed in quantitative terms
The probability definition for sterility derives from the fact that microbial death follows a geometric progression .i.e. the cells do not all die at once when exposed to lethal conditions
• Cont’d
The US FDA defines sterilization as the “reduction of a microbial population to 10° (or one cell) plus an additional 6 log-cycles”

Sterility is defined as the “probability of a non-sterile unit (PNSU) in a lot or batch of product”PNSU is also referred to as the “Sterility Assurance Level” or SAL
A product is considered sterile when the probability of a non-sterile unit is < 1 in 1, 000, 000 units; or a SAL of 10-6
Managing an Aseptic Processing Area (APA)

Drug Product
Sterilization Process
Sterile Drug
Containers Sterilization Process
Sterile Container
Excipient Sterilization Process
Sterile Excipient
Closures Sterilization Process
Sterile Closures
Contact Surface
Sterilization Process
Sterile Contact Surface
Sterile
DP
Managing of all these steps is a real challenge for personnel

Working in an Aseptic Processing Area (APA)

Personnel
Knowledge
Ability
Skill

Atypical Job
Heavy gowning
Physical Exhaustion
Technical understanding

Very important
Educational background
K, A, S
Personal attributes

Grade A
Grade B
Grade C
Grade D

Process, Facilities
& Design
Personnel with
appropriate K,A,S
Training (Knowledge
based & performance)
Monitoring performance
Effective CAPAs
Aseptic Process
Connecting the Dots

Inspector’s Eyes

Build QualityBe proactive …. Rigorous thinking with logical, systematic &
science based approaches to improve effectiveness & efficiency of decision making

Build QualityBe proactive …. Rigorous thinking with logical, systematic &
science based approaches to improve effectiveness & efficiency of decision making
Personnel & material flow
Air flow pattern evaluation
Aseptic operations
Disinfectant/ Sanitization
Cleaning efficiency
EM Plan

Lets understand
GMP Inspection & Inspector’s Interest

Quality
Materials
Production
Laboratory Control
Facilities & Equipment
Packaging & Labeling

Quality
Review/approved
procedure
Documentation of
operation execution
Investigation Deviations
& Complaints
Failures

Production
Control Strategy
for change
Process validation
Investigation of
discrepancy
Missing & incomplete
records
In-process controls

Laboratory Control
Control Strategy
for change
Source of microbial contamina
tion
Investigation of
discrepancy Retention
of raw data
In-adequate sampling

Facilities & Equipment
Contamination
Cleaning procedure
Investigation of
discrepancy
Equipment qualificatio
n
Control strategy
for change

Materials
Identity test
Authenticity of COA
Investigation of
discrepancy
Control strategy for change in
handling of materials
Release of material

Packaging & Labeling
Potential of mislabeling
Mix up potential
Investigation of
discrepancy
Control strategy for
change
Packaging validation

…… Inspector’s eyes looking for ……
Systems that allow inferior product to the market

Quality Management System
Production & Control Strategy
Potential adulteration boulevard
Consistency affairs

Contamination affairs
Identification & Traceability avenues
Reliability & reproducibility of results
Genuineness & accuracy of data

Validation Policy, Plan, Protocol, Report & Raw Data
Reports & Reviews
Developmental reports & Change Controls
Deviation, non-conformance, incidents

OOS, CAPA, OOT
Trainings & Effectiveness
Storage, Transportation
Human practice in aseptic areas

Sterility Failures
Media Fills
Rejects, Reworks, Re-process
Equipment repairing

Utilities & Plumbing Connections
Equipment logs
Maintenance Records
Cleaning Records

Observed Practice vs. Validated Practices
Personnel observed vs. Expected behavior
In-process store
SOP in place

Calibration stickers
Non-validated analytical methods
Growth promotion negative controls

Degree of product & process
understanding
Robustness of Quality System controlling the
process
Manufacturer’ ability to manage
risk associated with product
quality

From History

Equipment and utensils are not cleaned and maintained at appropriate intervals to prevent contamination

Equipment and utensils are not cleaned and maintained at appropriate intervals to prevent contamination
HEPA, their supporting grid work, filter screens and screen tracks possessed varying amount of discolored, chipping paint,
multicolored coalescing droplets and clumps of dark materials

Aging infrastructure
Regular Assessment, Repair, Expertise, Risk Management
Conformance to Standards
compliant, competent in
microbial risk
assessment?
Culture

• Inherent human characteristic
Employee behaviors
• Absent or lagging change or behaviorDocumentation
• Expertise, Knowledge, CommunicationOversight
Key Compliance Root Cause Themes

• Human factorsEquipment design
• Appropriate, regularity, expertise & know-how
Equipment adjustment
• Risk Mitigation Activities absentEnvironment
Key Compliance Root Cause Themes

sterile preservative-free ibuprofin L-lysine at
17 mg/mL in a single-use glass vial
in premature infants no more than 32 weeks
gestational age
Two batches of this product were
voluntarily recalled by the manufacturer,
Lundbeck
interaction between the product and the Type I borosilicate glass vial
It substitutes for the aluminum oxide
forming an ibuprofen aluminum hydroxide
salt as particulate
Case

Particulates ….?
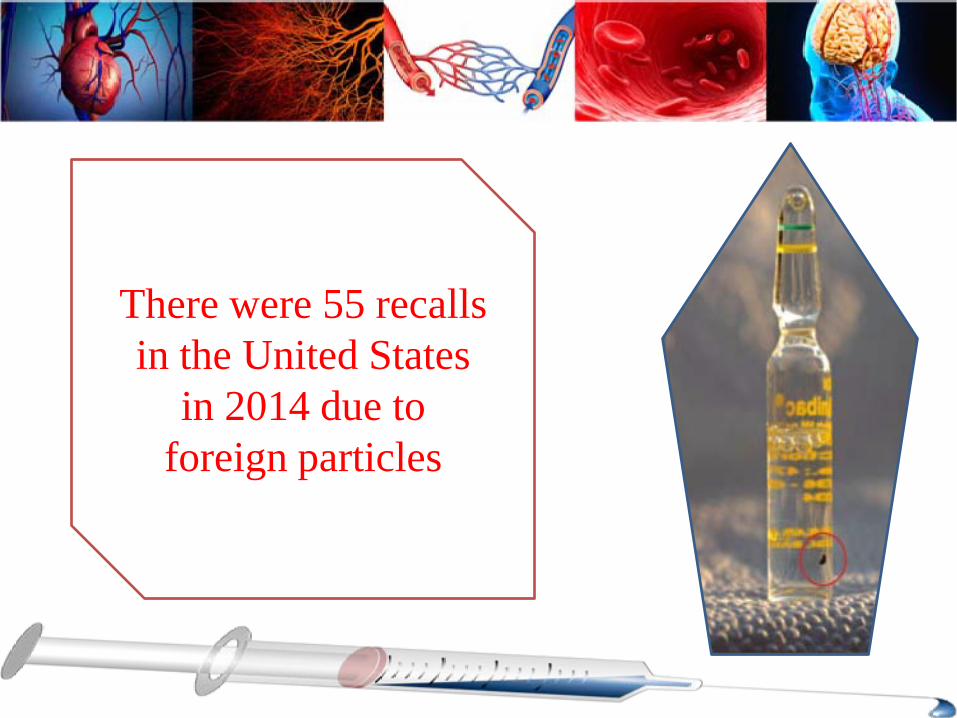
There were 55 recalls in the United States
in 2014 due to foreign particles

Sources of Particulate Matter in Injectable Drug Products
Environment Packaging materials
Solution & formulation components
Product-packaging
interactions
Process generated particles

Clinical Effects of Injected Particulate Matter
Phlebitis Pulmonary emboli
Pulmonary granulomas
Immune system
dysfunction
Pulmonary dysfunction Infarction Death

Clinical Effects of Injected Particulate Matter
Patient risk associated with injected particulate matter depends upon a number factors such as:• Route of administration• Particle size and shape• Number of particles injected• Particle composition• Patient population

Route of Administration
The route influences the
deposition of the injected particles
The total particle load administered
The overall risk to the patient

The risk of systemic reaction is low, if the administration is via IM or SC route as• The delivered volume (overall
particle load) is relatively small • The ability of particles to migrate
far from injection site is negligible
The IV route carries the maximum possibility of • Delivering greater volume of fluids• Broader dissemination &
deposition of particulate matter throughout the body
Route of Administration

Intravenous Route of Administration
Particles injected
IV
Venous system (veins ↑ in size in direction of blood flow)
Heart Pulmonary artery Lungs
Capillary diameter 6-8 um
Particles > 6-8 um remain in
pulmonary capillaries
Smaller particles deposit in organs
e.g. liver & spleen
Cont’d

Intravenous Route of Administration
Processed by the phagocytic cells of the
reticulo-endothelial system
Phagocytic overload of the reticulo-endothelial system by large number of particles
has potential to block the system
Lead to secondary infections in a debilitated host

Intra-arterial Route of Administration
Particles injected IAArteries ↓ in
size in direction of blood flow
Large particles pass through arterioles & capillaries
May cause occlusion
affecting blood flow
Smaller particles are capable of blocking terminal arterial vessels
More detrimental than larger particles
Large particles occlude arterioles due to ↓
collateral blood supply available to the affected
tissue
Cont’d
Intra-arterial Route of Administration
Intravascular Injection of corticosteroid formulation
containing particles is linked with adverse CNS sequelae in humans
versus non-particulate steroid formulations
A study on pigs injected in vertebral artery with particulate or non-particulate based steroids showed brain stem edema
& significant tissue damage in pigs receiving particulate containing steroids

Particle Size and Shape
The shape as well as size of particle is important in determination of potential for harm
The total particle load is also an important factor to consider
Various animal studies with particulate containing injections showed deposition in lungs and liver, as well as in spleen & kidneys
Cont’d

Particle Size and Shape
Adverse event reports & autopsy results are the only source of information about the effect of larger particles on patient populations
Visible particulate matter composed of calcium salt precipitates in drug admixtures have caused a number of serious clinical events

Patient Population
Patients with existing tissue
damage e.g. trauma, surgery or sepsis
Critically ill patients Neonates
At highest risk

Thank you