plasma alkylresorcinol metabolites as biomarkers for...
TRANSCRIPT

Research Article
Plasma Alkylresorcinol Metabolites as Biomarkers forWhole-Grain Intake and Their Association with ProstateCancer: A Swedish Nested Case–Control Study
Isabel Drake1, Emily Sonestedt1,2, Bo Gullberg1, Anders Bjartell4, Ha�kan Olsson3, Herman Adlercreutz5,
Matti J. Tikkanen6, Elisabet Wirf€alt1, and Peter Wallstr€om1
AbstractBackground: Observational studies have mostly found no association between self-reported whole-grain
intake and prostate cancer. Plasma alkylresorcinol metabolites have been suggested as biomarkers for whole-
grain intake in free-living populations.
Methods: We investigated the major dietary and lifestyle determinants of plasma alkylresorcinol metabo-
lites in a nested case–control study (1,016 cases and 1,817 controls) in the Malm€o Diet and Cancer Study.
Multivariate adjusted ORs and 95% confidence intervals (95% CI) were estimated to assess the association
between plasma alkylresorcinol metabolites and prostate cancer using logistic regression.
Results: Whole-grain intake, waist circumference, educational level, and smoking status were the main
determinants of alkylresorcinol metabolites. We observed significant correlations between alkylresorcinol
metabolites and whole-grain (r ¼ 0.31) and fiber (r ¼ 0.27) intake. Metabolite concentration was positively
associated with prostate cancer risk (Poverall effect ¼ 0.0004) but the association was not linear (P ¼ 0.04). The
lowest risk was seen among men with moderate plasma concentrations. The OR for high compared with
moderate plasma alkylresorcinol metabolites was 1.41 (95% CI, 1.10–1.80) for prostate cancer.
Conclusions:Results suggest thatplasmaalkylresorcinolmetabolites aremainlydeterminedbywhole-grain
intake in this nested case–control study of Swedishmen. The increased risk of prostate cancer seen amongmen
with high plasma alkylresorcinol metabolites requires further study, but residual confounding, detection bias,
or competing risks of nonprostate cancer–related deaths are plausible explanations that could not be ruled out.
Impact: We found no evidence of a protective effect of whole grains on incident prostate cancer. Further
validation of alkylresorcinol metabolites as a biomarker for whole-grain intake is needed. Cancer Epidemiol
Biomarkers Prev; 23(1); 73–83. �2013 AACR.
IntroductionWhole grains have been linked to decreased risk of
many diet-related diseases, including cardiovascular dis-ease (1), type II diabetes (2), and certain cancers (3).Possible mechanisms for the protective effect are that
whole grains slow the digestion, lower insulin secretion,and could potentially improve insulin sensitivity (4).Whole grains are also a major source of fiber, vitamins,minerals, lignans, and other phenolic compounds, all ofwhich may have beneficial health effects (5). Whole-grainproducts are relatively high in antioxidant activity, whichmay protect DNA from oxidative damage and mutationthat can lead to cancer (5). Lignans are hormonally activecompounds that may protect against certain hormonallymediated diseases, including prostate cancer (6). Diet hasbeen suggested as one of many environmental factorsaffecting prostate cancer development and progression(7, 8), but the only established risk factors to date are age,ethnicity, and family history of prostate cancer (9). Smallclinical trials andanimal studies suggest thatwhole grainsmight have a beneficial effect on prostate cancer progres-sion (10–12), mediated by increased apoptosis andlower insulin secretion. Landberg and colleagues alsoshowed that whole grains from rye compared with cel-lulose-supplemented refinedwheat loweredplasmapros-tate-specific antigen (PSA) among patients with prostatecancer (11). The hypothesis that whole grains may lower
Authors' Affiliations: 1Research Group in Nutritional Epidemiology; 2Dia-betes and Cardiovascular Disease, Genetic Epidemiology; 3Department ofCancer Epidemiology and Oncology and Department of Clinical Sciencesin Lund, Lund University, Lund;4Department of Urology and Department ofClinical Sciences, Division of Urological Cancers Ska
�ne University Hospi-
tal, Malm€o, Sweden; 5Folkh€alsan Research Center, Biomedicum andDivision of Clinical Chemistry, University of Helsinki; and 6Folkh€alsanResearch Center, Biomedicum, Helsinki University and Central HospitalHeart and Lung Center, Helsinki, Finland
Note: Supplementary data for this article are available at Cancer Epide-miology, Biomarkers & Prevention Online (http://cebp.aacrjournals.org/).
Corresponding Author: Isabel Drake, Department of Clinical Sciences inMalm€o, Lund University, Jan Waldenstr€omsgata 35, SE-20502 Malm€o,Sweden. Phone: 464-039-1326; Fax: 464-039-1322; E-mail:[email protected]
doi: 10.1158/1055-9965.EPI-13-0878
�2013 American Association for Cancer Research.
CancerEpidemiology,
Biomarkers& Prevention
www.aacrjournals.org 73
on June 15, 2018. © 2014 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst November 12, 2013; DOI: 10.1158/1055-9965.EPI-13-0878

the risk of prostate cancer has been examined in severalepidemiologic studies. Results from cohort studies havemostly found null associations (13–16). Dietary assess-ment methods used in large-scale observational studiesare associated with a varying degree of random andsystematic measurement errors that may attenuate (orbias) diet–disease associations. For this reason, dietarybiomarkers can be used as additional estimates of dietaryintake. Alkylresorcinols are phenolic lipids present in thebran fraction ofwheat, rye, and barley kernels. About half(45%–71%) of alkylresorcinols are absorbed, and intactalkylresorcinols and its metabolites can be measured inplasma (17). The two main metabolites of alkylresorcinol,3,5-dihydroxybenzoic acid (DHBA) and 3,5-dihydroxy-phenylpropanoic acid (DHPPA), have been suggested asbiomarkers of whole-grain intake in Nordic populations(18, 19). There is, however, limiteddataon their usefulnessin large observational studies. The aim of this study wastherefore to identify major dietary and lifestyle determi-nants of plasma alkylresorcinol metabolites in a nestedcase–control study of men in the Malm€o Diet and Cancer(MDC) study and to examine whether alkylresorcinolmetabolite concentration is associatedwith incident pros-tate cancer.
Materials and MethodsStudy population
The MDC study is a population-based prospectivecohort study set in Sweden. The cohort has beendescribedin detail elsewhere (20–22). In short, baseline examina-tions were carried out from March 1991 to October 1996.All men born between 1923 and 1945 and all women bornbetween 1923 and 1950 living in Malm€o were invited toparticipate in the study. Baseline examinations includedan extensive lifestyle and socioeconomic questionnaire,dietary assessment, direct anthropometricmeasurements,and collection of blood samples. With a participation rateof approximately 40%, 28,098 individuals (11,063 men)with complete data represent the cohort. The MDC studywas approved by the Ethics Committee at Lund Univer-sity (Lund, Sweden) and informed written consent wasobtained from all participants.
Ascertainment of cases and selection of controlsIncident prostate cancer cases were identified by link-
age of personal identification numbers with the SwedishCancer Register (SCR). Information on vital status of thestudy population was obtained from the Swedish Causeof Death Registry and the Swedish Tax Agency. All menwith prevalent cancers at baseline were excluded, exceptnonmelanoma skin cancer. A total of 1,016 incident pros-tate cancer cases (as first cancer diagnosis) occurred untilDecember 31, 2009. Data on the clinical and histologiccharacteristics of the tumors were collected from theNational Prostate Cancer Register (NPCR). Data on cases(n ¼ 54) that occurred between 1991 and 1995 weremanually extracted from medical records by using stan-dard routines. The SCR is known to be 98% complete. A
validation of NPCR data from another region showedhigh validity for all variables, including the variables usedin the classification of tumors by case severity in this study(23). High-risk prostate cancer cases were classified aslocal clinical tumor stage T3 or T4, the presence of lymphnode metastasis (N1) or bone metastasis (M1), a Gleasonscore 8, or serum PSA concentrations 50 ng/mL (24).Tumorswere also classified as high-risk cases if theWorldHealth Organization grade was 3 and the Gleason scorewas unavailable (n ¼ 6). Cases diagnosed after subjectspresented with malignancy-related symptoms or lowerurinary tract symptoms were classified as symptomaticcases. The cases were diagnosed 0 to 18 years (mean, 9years) after baseline examinations and the mean age atdiagnosis was 70 years (range 50–85 years). For each case,on average two controls were selected, matched by ageand date of study entry (� 90 days) from the cohortmembers at risk at the time of diagnosis of the case(n ¼ 1,828). Successful blood analysis of alkylresorcinolmetabolites (see below) was available for 2,827 subjects,leaving 1,010 cases and 1,817 controls for the analyses.
Laboratory analyses of alkylresorcinol metabolitesThe sum of DHBA and DHPPA was used to approxi-
mate total plasma alkylresorcinols. The nonfasting bloodsamples collected at baseline were processed and sepa-rated for plasma within 1 hour. The samples have beenstored at �80�C until analysis 2012. The quality controlprogram of the biobank in the MDC study has beendescribed previously (25). Alkylresorcinol metaboliteswere analyzed at Folkh€alsan Research Center in Helsinkiby high-performance liquid chromatography (HPLC)with coulometric electrode array detection (ESA Bios-ciences, Inc.) as described by Koskela and colleagues(26). In brief, plasma samples (100 mL) were hydrolyzedovernight at 37�Cwithb-glucuronidase and sulfatase, andthe samplewas extractedwith diethyl ether. Separation ofdiethyl ether and water phase was done by freezing. Thecombined organic phases were evaporated to dryness.The sample was reconstituted in 50 mLmethanol, and 100mL HPLC mobile phase was added. The sample wasfiltered through Gelman GHP 0.2 mm filter and analyzedwith HPLC-coulometric electrode array detection. Themethod is considered accurate, specific, and reproducible(26).
Dietary assessmentThe dietary assessment methodology has been des-
cribed in detail elsewhere (27–30). It combined (i) a 7-daymenu book that collected detailed description of lunchesand dinners, cold beverages, medications, and dietarysupplements, (ii) a 168-itemdietary questionnaire, includ-ing frequencies and portion sizes, and (iii) a 1-hour inter-view. Food intakes were converted to nutrient intake datausing the MDC Food and Nutrient Database, originatingfrom PCKOST2-93 of the SwedishNational FoodAdmin-istration. The nutrient variables examined in this studywere energy (kcal), fiber (grams per day), and percentage
Drake et al.
Cancer Epidemiol Biomarkers Prev; 23(1) January 2014 Cancer Epidemiology, Biomarkers & Prevention74
on June 15, 2018. © 2014 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst November 12, 2013; DOI: 10.1158/1055-9965.EPI-13-0878

of nonalcohol energy contributed by protein, fat, andcarbohydrates. The food groups (grams per day) exam-ined were: cereals (grains, cereals, and flours), low-fiberbread, high-fiber bread, and rice and pasta. The selectionof these food variables was based on their potentialcontribution of whole grains. Whole-grain intake (gramsper day) was estimated using the detailed informationabout consumed foods/brands in the abovementionedfood groups and using the Food andNutrient Database ofthe Swedish National Food Administration (availablefrom: www.slv.se).
Other variablesTrained project staff measured participants’ weight
(kg), height (cm), and waist (cm). Body mass index (BMI)was defined as kg/m2. Lifestyle and socioeconomicvariables were obtained through the standardized ques-tionnaire. Educational status was categorized into ele-mentary, primary and secondary, upper secondary, fur-ther education without a degree, and university degree.Smoking habits were categorized into current smokers(including irregular), former smokers, andnonsmokers.Atotal physical activity score was obtained by combininginformation on leisure-time physical activity, domesticactivity, and work activity (13). Individuals with no con-sumption of alcohol in the menu book and those whoreported no consumption of alcohol during the previousyear in the questionnaire were categorized as zero con-sumers. The other subjects were categorized into threegroups according to their alcohol consumption: <20 galcohol per day (low), 20–40 g (medium), and >40 g (high).Prevalent diabetes at baseline was confirmed through
national and regional registries. Participants were classi-fied as potential underreporters, adequate reporters, oroverreporters of energy intake, as described in detailpreviously (31). Dietary change in the past (yes or no)was derived from the questionnaire item "have you sub-stantially changed your eating habits in the past due toillness or other reasons?" (32).
Statistical analysisAlkylresorcinol metabolite concentrations were highly
skewed (Fig. 1). The differences in total alkylresorcinolmetabolite concentration (DHBAþDHPPA) and partici-pant characteristics between cases and controls weretested using Wilcoxon rank-sum test (alkylresorcinolmetabolite concentrations and whole-grain intake), Stu-dent t test (other continuous variables), and c2 test(categorical variables). Participant characteristics acrossquintiles of plasma alkylresorcinol metabolites were alsoexamined. Median alkylresorcinol metabolite concentra-tion by age, lifestyle factors (smoking status, educationallevel, alcohol consumption, BMI categories, and physicalactivity), diabetes status, past food habit change, andenergy misreporting was calculated among the controls(n¼ 1,817). Because of skewed data and the large numberof zero values (n ¼ 408) for plasma alkylresorcinolmetabolites, normal distribution could not be approxi-mated by natural log transformation, and decile rankingwas used instead. Differences in plasma alkylresorcinolmetabolite concentration (assigning the median value forcontrols in each decile) by these variables were tested,using a general linear model controlling for age and dateof study entry.
Figure 1. Frequency distributionof (A) total plasma alkylresorcinolmetabolite concentration(DHBAþDHPPA), (B) plasmaDHBA concentration, and (C)plasmaDHPPA concentration for1,817 male controls in a nestedcase–control study of the MDCcohort (1991–1996).
Plasma Alkylresorcinol Metabolites and Prostate Cancer Risk
www.aacrjournals.org Cancer Epidemiol Biomarkers Prev; 23(1) January 2014 75
on June 15, 2018. © 2014 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst November 12, 2013; DOI: 10.1158/1055-9965.EPI-13-0878

Food and nutrient variables were energy adjusted byregressing the intake (loge-transformed, dependent vari-able) on the total energy intake (loge-transformed, inde-pendent variable). All food variables (i.e., whole grains,cereals, low-fiber bread, high-fiber bread, and rice andpasta) were divided into approximate deciles based ontheir residual ranking. Partial correlations between alkyl-resorcinol metabolite concentration and energy-adjusteddietary variables and body composition were computedamong the controls (n¼ 1,817), controlling for age, date ofstudy entry, and total energy. We also formulated aminimally adjusted model with all food variables includ-ed simultaneously and adjusting for age, date of studyentry, and total energy. Finally, in an exploratory analysis,all food variables, whole grains, body composition vari-ables, smoking status, educational level, alcohol con-sumption, and physical activity were included in a linearregression model followed by stepwise backward elimi-nation of variables with P > 0.10. The model was adjustedfor age, date of study entry, and total energy.
We examined a potential nonlinear relation betweenplasma alkylresorcinol metabolites and prostate cancerrisk by fitting a restricted cubic spline with five knots(placed at the 10th, 25th, 50th, 75th, and 90th percentiles oftotal plasma alkylresorcinol metabolite concentrations) toa logistic regressionmodel using a continuous variable foralkylresorcinol metabolites and adjusting for all othercovariates. Given the long natural history of prostatecancer and the strong agedependence,we assessedpoten-tial competing risks from nonprostate cancer causes ofdeath by fitting a restricted cubic spline to a logisticregression model for nonprostate cancer mortality. TheWald c2 testwas used to test the overall significance (4 df).Linearity was tested by using the Wald c2 test (2 df), forwhich P < 0.05 is consistent with nonlinearity.
For examination of the association between alkylre-sorcinol metabolites and prostate cancer, participantswere ranked into quintiles (Q) of their plasma concen-tration. To make full use of the data without restrictionto the matched cases and controls, we used uncondi-tional logistic regression to estimate ORs and 95% con-fidence intervals (CI) for prostate cancer incidenceadjusting for matching variables (age and date of studyentry). However, estimated ORs were virtually the samewhen using conditional logistic regression (data notshown). Additional analyses included adjustment fortotal energy, height, waist, smoking status, and educa-tional level. These covariates were identified throughthe literature and were graphically evaluated for beingpotential confounders. Because few individuals (n ¼ 12)had missing values on any of the covariates, these wereexcluded from analysis. Inclusion of potential dietaryconfounders (including calcium, vitamin D, selenium,monosaccharides, sucrose, saturated fatty acids, poly-unsaturated fatty acids, total carbohydrates, dairy pro-ducts, soft drinks, vegetables and processed meats) didnot affect risk estimates (data not shown). In addition toa main effect analysis, the models were stratified by
low-risk and high-risk cases to examine whether asso-ciations between alkylresorcinol metabolites and pros-tate cancer incidence differed according to clinical stage.To assess the impact of opportunistic PSA testing, wealso investigated symptomatic cases separately.
We conducted a series of sensitivity analyses. Theanalyseswere repeatedwith exclusion of individualswhoreported dietary change in the past (to include onlyindividuals more likely to have stable food habits andconsequently more stable long-term whole-grain intakeand alkylresorcinol metabolite concentrations). Furtherexclusions included men with prevalent diabetes at base-line and potential energy misreporters. We also investi-gated the association between plasmaDHBAandDHPPAand risk of prostate cancer separately.
Stata/SE 12.0 (StataCorp LP) was used for all statisticalanalyses. All tests were two sided and P < 0.05 wasconsidered statistically significant.
ResultsMedian concentration of alkylresorcinol metabolites
(DHBAþDHPPA) in plasma was 45.8 nmol/L amongcases and 43.1 nmol/L among controls (Table 1). A lowerfrequency of current smokers was observed among thecases compared with controls.
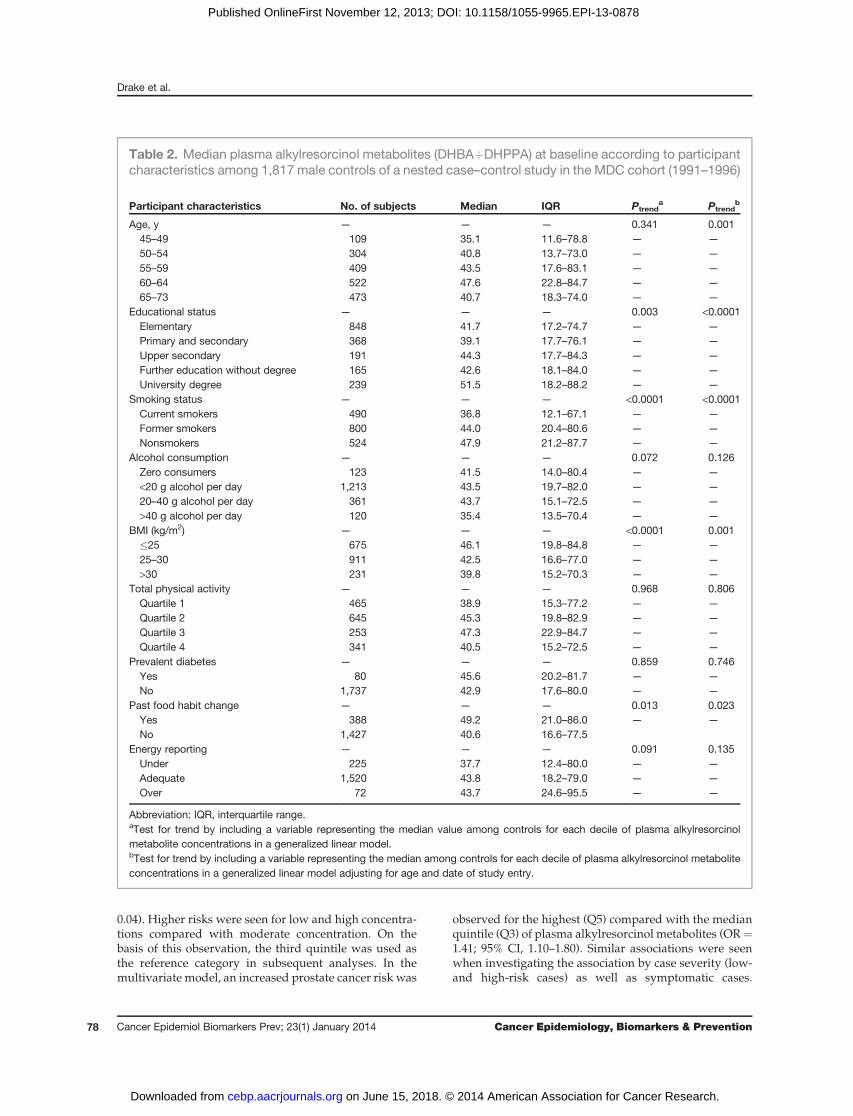
Determinants of plasma alkylresorcinol metaboliteconcentration
Alkylresorcinol metabolite concentration was posi-tively associated with age (P ¼ 0.001) and educationallevel (P < 0.0001). Nonsmokers had 30% higher medianalkylresorcinol metabolite concentration than smokers(P < 0.001), and men with normal weight had 16%higher concentration than obese men (P ¼ 0.001). Therewas no difference in metabolite concentration by alco-hol consumption, physical activity, or diabetes status atbaseline. Past food habit changers had 21% highermedian metabolite concentration (P ¼ 0.023; Table 2).The alkylresorcinol metabolite concentration was pos-itively correlated with fiber intake (r ¼ 0.27; P < 0.001)and whole-grain intake (r ¼ 0.31; P < 0.001). Potentialfood sources of alkylresorcinols were also positivelycorrelated with metabolite concentration, including cer-eals (r ¼ 0.15; P < 0.001) and high-fiber bread (r ¼ 0.34; P< 0.001), whereas low-fiber bread was negatively cor-related with alkylresorcinol metabolite concentration(r¼�0.17; P < 0.001) when examined in separate models.BMI and waist circumference were negatively correlatedwith metabolite concentration (Table 3). When all foodvariables were included simultaneously in the model,high-fiber bread (r ¼ 0.30) and cereals (r ¼ 0.12) werepositively correlated with alkylresorcinol metabolite con-centrations. In the model, including all food variables(model 1) and various potential confounders, cerealsand high-fiber bread as well as height were significantlypositively associated with alkylresorcinol metabolite con-centration, and waist circumference was negatively asso-ciated with metabolite concentration (Table 3). Including
Drake et al.
Cancer Epidemiol Biomarkers Prev; 23(1) January 2014 Cancer Epidemiology, Biomarkers & Prevention76
on June 15, 2018. © 2014 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst November 12, 2013; DOI: 10.1158/1055-9965.EPI-13-0878
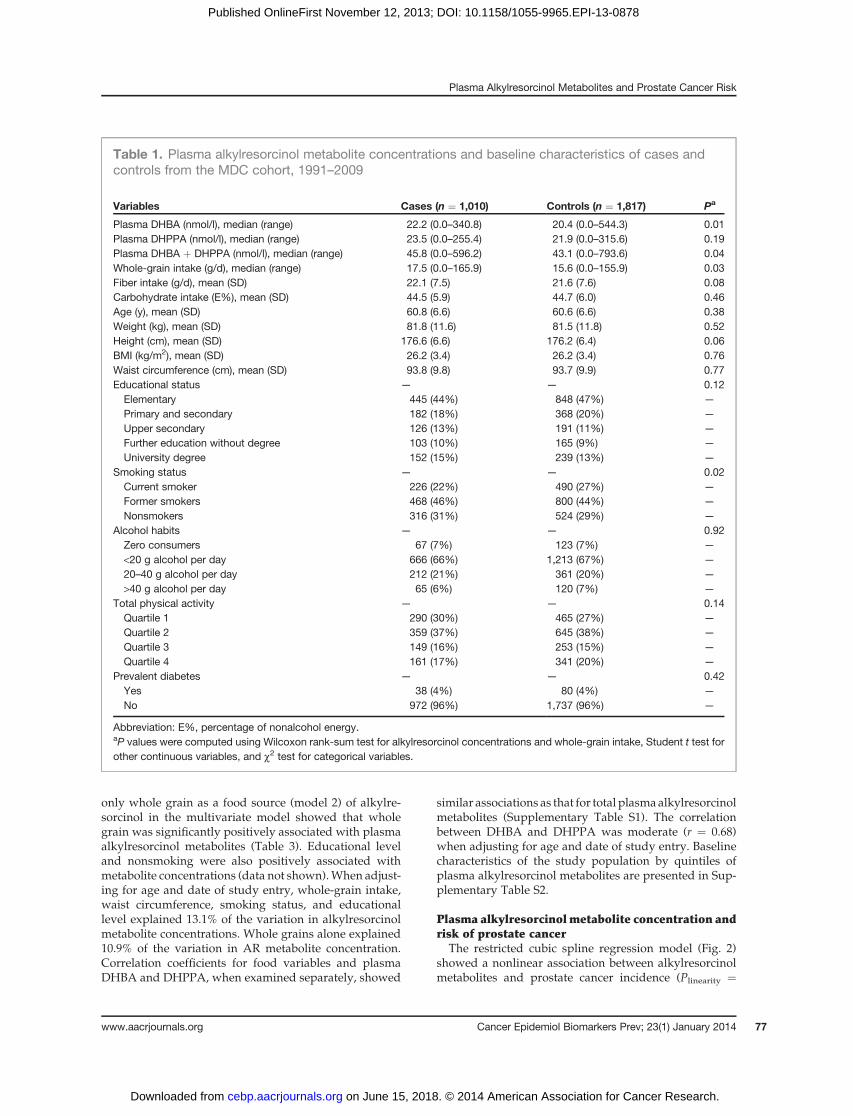
only whole grain as a food source (model 2) of alkylre-sorcinol in the multivariate model showed that wholegrain was significantly positively associated with plasmaalkylresorcinol metabolites (Table 3). Educational leveland nonsmoking were also positively associated withmetabolite concentrations (data not shown).When adjust-ing for age and date of study entry, whole-grain intake,waist circumference, smoking status, and educationallevel explained 13.1% of the variation in alkylresorcinolmetabolite concentrations. Whole grains alone explained10.9% of the variation in AR metabolite concentration.Correlation coefficients for food variables and plasmaDHBA and DHPPA, when examined separately, showed
similar associations as that for total plasmaalkylresorcinolmetabolites (Supplementary Table S1). The correlationbetween DHBA and DHPPA was moderate (r ¼ 0.68)when adjusting for age and date of study entry. Baselinecharacteristics of the study population by quintiles ofplasma alkylresorcinol metabolites are presented in Sup-plementary Table S2.
Plasma alkylresorcinolmetabolite concentration andrisk of prostate cancer
The restricted cubic spline regression model (Fig. 2)showed a nonlinear association between alkylresorcinolmetabolites and prostate cancer incidence (Plinearity ¼
Table 1. Plasma alkylresorcinol metabolite concentrations and baseline characteristics of cases andcontrols from the MDC cohort, 1991–2009
Variables Cases (n ¼ 1,010) Controls (n ¼ 1,817) Pa
Plasma DHBA (nmol/l), median (range) 22.2 (0.0–340.8) 20.4 (0.0–544.3) 0.01Plasma DHPPA (nmol/l), median (range) 23.5 (0.0–255.4) 21.9 (0.0–315.6) 0.19Plasma DHBA þ DHPPA (nmol/l), median (range) 45.8 (0.0–596.2) 43.1 (0.0–793.6) 0.04Whole-grain intake (g/d), median (range) 17.5 (0.0–165.9) 15.6 (0.0–155.9) 0.03Fiber intake (g/d), mean (SD) 22.1 (7.5) 21.6 (7.6) 0.08Carbohydrate intake (E%), mean (SD) 44.5 (5.9) 44.7 (6.0) 0.46Age (y), mean (SD) 60.8 (6.6) 60.6 (6.6) 0.38Weight (kg), mean (SD) 81.8 (11.6) 81.5 (11.8) 0.52Height (cm), mean (SD) 176.6 (6.6) 176.2 (6.4) 0.06BMI (kg/m2), mean (SD) 26.2 (3.4) 26.2 (3.4) 0.76Waist circumference (cm), mean (SD) 93.8 (9.8) 93.7 (9.9) 0.77Educational status — — 0.12Elementary 445 (44%) 848 (47%) —
Primary and secondary 182 (18%) 368 (20%) —
Upper secondary 126 (13%) 191 (11%) —
Further education without degree 103 (10%) 165 (9%) —
University degree 152 (15%) 239 (13%) —
Smoking status — — 0.02Current smoker 226 (22%) 490 (27%) —
Former smokers 468 (46%) 800 (44%) —
Nonsmokers 316 (31%) 524 (29%) —
Alcohol habits — — 0.92Zero consumers 67 (7%) 123 (7%) —
<20 g alcohol per day 666 (66%) 1,213 (67%) —
20–40 g alcohol per day 212 (21%) 361 (20%) —
>40 g alcohol per day 65 (6%) 120 (7%) —
Total physical activity — — 0.14Quartile 1 290 (30%) 465 (27%) —
Quartile 2 359 (37%) 645 (38%) —
Quartile 3 149 (16%) 253 (15%) —
Quartile 4 161 (17%) 341 (20%) —
Prevalent diabetes — — 0.42Yes 38 (4%) 80 (4%) —
No 972 (96%) 1,737 (96%) —
Abbreviation: E%, percentage of nonalcohol energy.aP values were computed using Wilcoxon rank-sum test for alkylresorcinol concentrations and whole-grain intake, Student t test forother continuous variables, and c2 test for categorical variables.
Plasma Alkylresorcinol Metabolites and Prostate Cancer Risk
www.aacrjournals.org Cancer Epidemiol Biomarkers Prev; 23(1) January 2014 77
on June 15, 2018. © 2014 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst November 12, 2013; DOI: 10.1158/1055-9965.EPI-13-0878
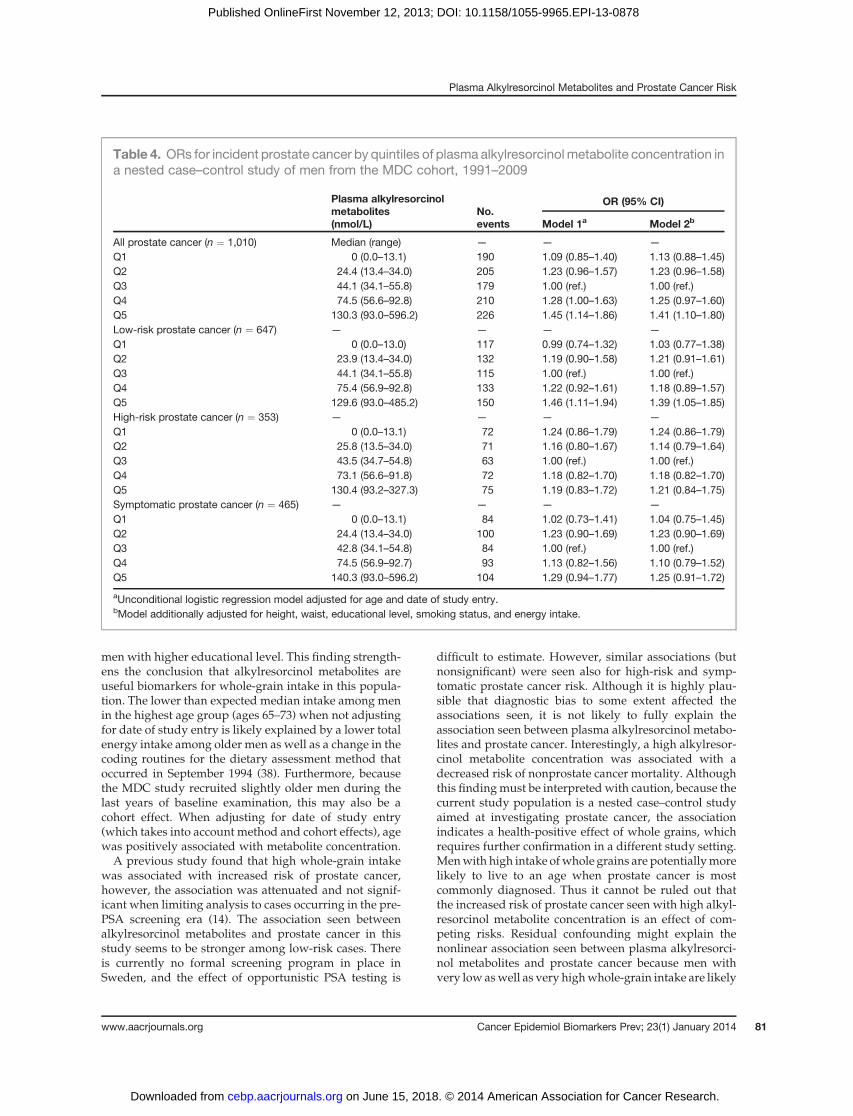
0.04). Higher risks were seen for low and high concentra-tions compared with moderate concentration. On thebasis of this observation, the third quintile was used asthe reference category in subsequent analyses. In themultivariate model, an increased prostate cancer risk was
observed for the highest (Q5) compared with the medianquintile (Q3) of plasma alkylresorcinol metabolites (OR¼1.41; 95% CI, 1.10–1.80). Similar associations were seenwhen investigating the association by case severity (low-and high-risk cases) as well as symptomatic cases.
Table 2. Median plasma alkylresorcinol metabolites (DHBAþDHPPA) at baseline according to participantcharacteristics among 1,817 male controls of a nested case–control study in the MDC cohort (1991–1996)
Participant characteristics No. of subjects Median IQR Ptrenda Ptrend
b
Age, y — — — 0.341 0.00145–49 109 35.1 11.6–78.8 — —
50–54 304 40.8 13.7–73.0 — —
55–59 409 43.5 17.6–83.1 — —
60–64 522 47.6 22.8–84.7 — —
65–73 473 40.7 18.3–74.0 — —
Educational status — — — 0.003 <0.0001Elementary 848 41.7 17.2–74.7 — —
Primary and secondary 368 39.1 17.7–76.1 — —
Upper secondary 191 44.3 17.7–84.3 — —
Further education without degree 165 42.6 18.1–84.0 — —
University degree 239 51.5 18.2–88.2 — —
Smoking status — — — <0.0001 <0.0001Current smokers 490 36.8 12.1–67.1 — —
Former smokers 800 44.0 20.4–80.6 — —
Nonsmokers 524 47.9 21.2–87.7 — —
Alcohol consumption — — — 0.072 0.126Zero consumers 123 41.5 14.0–80.4 — —
<20 g alcohol per day 1,213 43.5 19.7–82.0 — —
20–40 g alcohol per day 361 43.7 15.1–72.5 — —
>40 g alcohol per day 120 35.4 13.5–70.4 — —
BMI (kg/m2) — — — <0.0001 0.001�25 675 46.1 19.8–84.8 — —
25–30 911 42.5 16.6–77.0 — —
>30 231 39.8 15.2–70.3 — —
Total physical activity — — — 0.968 0.806Quartile 1 465 38.9 15.3–77.2 — —
Quartile 2 645 45.3 19.8–82.9 — —
Quartile 3 253 47.3 22.9–84.7 — —
Quartile 4 341 40.5 15.2–72.5 — —
Prevalent diabetes — — — 0.859 0.746Yes 80 45.6 20.2–81.7 — —
No 1,737 42.9 17.6–80.0 — —
Past food habit change — — — 0.013 0.023Yes 388 49.2 21.0–86.0 — —
No 1,427 40.6 16.6–77.5Energy reporting — — — 0.091 0.135Under 225 37.7 12.4–80.0 — —
Adequate 1,520 43.8 18.2–79.0 — —
Over 72 43.7 24.6–95.5 — —
Abbreviation: IQR, interquartile range.aTest for trend by including a variable representing the median value among controls for each decile of plasma alkylresorcinolmetabolite concentrations in a generalized linear model.bTest for trend by including a variable representing the median among controls for each decile of plasma alkylresorcinol metaboliteconcentrations in a generalized linear model adjusting for age and date of study entry.
Drake et al.
Cancer Epidemiol Biomarkers Prev; 23(1) January 2014 Cancer Epidemiology, Biomarkers & Prevention78
on June 15, 2018. © 2014 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst November 12, 2013; DOI: 10.1158/1055-9965.EPI-13-0878

However, the increased risk seen inQ5 comparedwithQ3was only significant for, and seemed to be driven by, low-risk prostate cancer (OR ¼ 1.39; 95% CI, 1.05–1.85); Table4). Among the potential confounding factors, smokingstatus and educational level had an attenuating influenceon the risk estimates.We investigated several potential dietary confounders,
but their effect on the observed risk estimates was mar-ginal and the associations remained significant (data notshown). Among plausible dietary confounders, we foundthat plasma alkylresorcinol metabolites were positivelycorrelated with primarily calcium, monosaccharide, andtotal carbohydrate intake (Supplementary Table S3).When we excluded men with prevalent diabetes at base-line, past food habit changers and energy misreporters,the associations between alkylresorcinol metabolite con-centration and prostate cancer were strengthened and theOR in Q5 compared with Q3 was 1.50 (95% CI, 1.10–2.04)for total prostate cancer incidence (datanot tabulated).Weinvestigated potential effectmodification by smoking andwaist circumference on the association between plasmaalkylresorcinol metabolites and prostate cancer, but weobserved no significant interaction (all P > 0.05; data notshown). The association between the twometabolites (i.e.,DHBA and DHPPA) and prostate cancer did not differsignificantly, but the associations seen with prostate can-cer seemed to be driven by DHBA concentration ratherthat DHPPA concentration (data not shown).
Plasma alkylresorcinol metabolite concentration waslinearly associated with decreased risk of nonprostatecancer mortality (Poverall effect ¼ 0.03; Plinearity ¼ 0.58).The OR for nonprostate cancer death in the highestquintile of alkylresorcinol metabolite concentration was0.66 (95% CI, 0.46–0.95) compared with the lowestquintile. The reduced risk for nonprostate cancer deathremained significant in strata-specific analysis by case–control status.
DiscussionIn this large observational study, we investigated the
usefulness of plasma alkylresorcinol metabolites as abiomarker for whole-grain intake in relation to diseaseincidence. We observed that alkylresorcinol metabolitespositively correlated with whole-grain intake. We foundno evidence for a protective association between wholegrains and prostate cancer incidence, but high alkylresor-cinol metabolite concentration was associated with lowerrisk of nonprostate cancer mortality. Unexpectedly, wefound that very high levels of plasma alkylresorcinolmetabolites were associated with an increased risk ofprostate cancer (primarily low-risk prostate cancer) com-pared with moderate concentrations.
Theunderlying concept of using abiomarker fordietaryintake is that it may improve ranking of subjects forexposure compared with dietary assessment methodsrelying on self-report. The coefficients of correlation
Table 3. Partial correlation coefficients between plasma alkylresorcinol metabolites (DHBAþDHPPA),energy-adjusted dietary variablesa, and body composition among 1,817 male controls of a nested case–control study in the MDC cohort (1991–1996)
Separate modelsb Minimal modelb,c Multivariate model 1d Multivariate model 2d
Variables Coefficient P Coefficient P Coefficient P Coefficient P
Energy (kcal) 0.010 0.66 0.003 0.90 0.002 0.963 0.007 0.913Protein 0.028 0.24 — — — — — —
Fat �0.128 <0.001 — — — — — —
Carbohydrates 0.118 <0.001 — — — — — —
Dietary fiber 0.274 <0.001 — — — — — —
Whole grains 0.310 <0.001 — — — — 0.300 <0.001Cereals 0.148 <0.001 0.124 <0.001 0.112 <0.001 — —
Low-fiber bread �0.168 <0.001 �0.000 0.998 — NS — —
High-fiber bread 0.341 <0.001 0.303 <0.001 0.325 <0.001 — —
Rice and pasta 0.039 0.10 0.025 0.295 — NS — —
BMI (kg/m2) �0.062 0.008 — — — NS — NSWaist (cm) �0.089 0.0001 — — �0.072 0.001 �0.087 <0.001Height (cm) 0.030 0.20 — — — NS — NS
aAll nutrient and food variableswere loge-transformed and energy-adjusted using the residualmethod. All food variables (whole grains,cereals, low-fiber bread, high-fiber bread, and rice and pasta) were divided into approximate deciles.bAdjusted for age, date of study entry, and total energy (loge-transformed).cMinimally adjusted model with food variables included simultaneously.dStepwise backward linear regression model with food variables (model 1) or whole grains (model 2), BMI (loge-transformed), waist(loge-transformed), height, smoking status, alcohol habits, educational status, physical activity, adjusted for age, date of study entry,and total energy (loge-transformed); NS is an eliminated variable with P > 0.10.
Plasma Alkylresorcinol Metabolites and Prostate Cancer Risk
www.aacrjournals.org Cancer Epidemiol Biomarkers Prev; 23(1) January 2014 79
on June 15, 2018. © 2014 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst November 12, 2013; DOI: 10.1158/1055-9965.EPI-13-0878

between plasma alkylresorcinol metabolites, wholegrains, and dietary fiber were significant, but moderate.In a free-living population with self-selected diets, thecorrelation between plasma alkylresorcinol metabolitesand self-reported intake of whole grains is however,within the expected range. In an intervention studywheresubjects are assigned a highwhole-grain versus nowhole-grain diet, correlation coefficients are likely to be muchhigher, as previously reported (11). In addition, alkylre-sorcinols are only present in appreciable amounts inwhole grains from rye and wheat, and therefore intakeof other cereals (e.g., oats) may deflate the correlation.Absorbed alkylresorcinols are thought to be metabolizedsimilarly to tocopherols (17). The phase I metabolism ofalkylresorcinols leads to the formation of DHBA and
DHPPA. We measured the plasma concentration ofDHBA and DHPPA due to their longer estimated half-lives (�11–16 hours; ref. 33) compared with intact alkyl-resorcinol (�5 hours; ref. 34). The reliability of plasmaalkylresorcinol (35) and its metabolites (36) over 4-monthtime has been investigated recently. The intraclass corre-lation coefficients for DHBA and DHPPAwere estimatedto 0.23 and 0.33, respectively, among men. Although themean concentrations of the metabolites did not differsignificantly over the 4-month period, these results indi-cate a fairly poor reliability. The results from the study byMontonen and colleagues may however, not be transfer-able to the current study with a different population anda different methodology for the analyses of metaboliteconcentrations (36). However, additional studies areneeded on the validity of alkylresorcinol metabolites asa biomarker for whole grains. Because the estimated half-life seems longer for DHPPA (33) and its reliability ispotentially higher compared with DHBA, it is of concernthat the association between the alkylresorcinol metabo-lites and prostate cancer seems to be driven by DHBA.Among the investigated determinants of alkylresorcinolmetabolites, the concentrations were mainly affected bywhole grains and fiber intake. Additional studies areneeded to assess the impact of various factors that couldpotentially affect the plasma concentrations, includingdietary intakes, anthropometric factors, and drugs. In thisstudy, we found that whole-grain intake alone explainedapproximately 11% of the variation in total plasma alkyl-resorcinol metabolite variation. The large proportion ofunexplained variationmay be due to the use of nonfastingblood samples, and to the measurement error of dietaryintake that combined with a single blood sample is likelyto attenuate the true correlation betweenwhole grains andalkylresorcinol metabolites.
The use of a quantifiable biomarker confirms andstrengthens the previous conclusion that whole grain isnot associated with decreased risk of prostate cancerincidence in this population (13). Given the high colin-earity between dietary factors, we cannot exclude thepossibility that the observed increased risk of prostatecancer seen with high plasma alkylresorcinol metabolitesis an effect of some other dietary factor or environmentalfactor that is correlated with whole-grain intake.Although adjustment for various dietary confounders didnot affect risk estimates, it is virtually impossible to isolatethe effect of a single dietary factor. Furthermore, whole-grain intake may also reflect exposure to dietary cadmi-um, which has been suggested to increase the risk ofprimarily localized prostate cancer (37). Althoughwe hadno information on dietary cadmium exposure, the majorfood sources for dietary cadmium and whole grains arethe same, primarily bread and cereals. It should also benoted that plasma alkylresorcinol metabolites are subjectto confounding by the same risk factors that are associatedwith self-reported whole-grain intakes. Higher plasmaalkylresorcinol metabolite concentrations were observed,as expected, among older and leanmen, nonsmokers, and
Figure 2. Representation of restricted cubic spline logistic regressionmodels for plasma alkylresorcinol metabolites (continuous), and (A)prostate cancer incidence and (B) nonprostate cancermortality using themedian alkylresorcinol metabolite concentration as the reference(41.1 nmol/L). Plasma alkylresorcinol metabolite values above the 95thpercentile were deleted to make the graph more stable; knots wereplaced at the 10th, 25th, 50th, 75th, and 90th percentiles of the remainingobservations. Solid lines, OR as a function of plasma alkylresorcinolmetabolites adjusted for age, date of study entry, height, waistcircumference, energy intake, smoking status, and educational level;dashed lines, 95%CIs.P value for overall effect indicateswhether plasmaalkylresorcinol metabolites are statistically significantly associated withthe outcome,whereas the linearity test indicateswhether the relationshipbetween alkylresorcinol metabolite level and the outcome is nonlinear.For prostate cancer incidence the relationship is nonlinear.
Drake et al.
Cancer Epidemiol Biomarkers Prev; 23(1) January 2014 Cancer Epidemiology, Biomarkers & Prevention80
on June 15, 2018. © 2014 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst November 12, 2013; DOI: 10.1158/1055-9965.EPI-13-0878
men with higher educational level. This finding strength-ens the conclusion that alkylresorcinol metabolites areuseful biomarkers for whole-grain intake in this popula-tion. The lower than expected median intake among menin the highest age group (ages 65–73) when not adjustingfor date of study entry is likely explained by a lower totalenergy intake among older men as well as a change in thecoding routines for the dietary assessment method thatoccurred in September 1994 (38). Furthermore, becausethe MDC study recruited slightly older men during thelast years of baseline examination, this may also be acohort effect. When adjusting for date of study entry(which takes into account method and cohort effects), agewas positively associated with metabolite concentration.A previous study found that high whole-grain intake
was associated with increased risk of prostate cancer,however, the association was attenuated and not signif-icant when limiting analysis to cases occurring in the pre-PSA screening era (14). The association seen betweenalkylresorcinol metabolites and prostate cancer in thisstudy seems to be stronger among low-risk cases. Thereis currently no formal screening program in place inSweden, and the effect of opportunistic PSA testing is
difficult to estimate. However, similar associations (butnonsignificant) were seen also for high-risk and symp-tomatic prostate cancer risk. Although it is highly plau-sible that diagnostic bias to some extent affected theassociations seen, it is not likely to fully explain theassociation seen between plasma alkylresorcinol metabo-lites and prostate cancer. Interestingly, a high alkylresor-cinol metabolite concentration was associated with adecreased risk of nonprostate cancer mortality. Althoughthis findingmust be interpretedwith caution, because thecurrent study population is a nested case–control studyaimed at investigating prostate cancer, the associationindicates a health-positive effect of whole grains, whichrequires further confirmation in a different study setting.Menwith high intake ofwhole grains are potentiallymorelikely to live to an age when prostate cancer is mostcommonly diagnosed. Thus it cannot be ruled out thatthe increased risk of prostate cancer seen with high alkyl-resorcinol metabolite concentration is an effect of com-peting risks. Residual confounding might explain thenonlinear association seen between plasma alkylresorci-nol metabolites and prostate cancer because men withvery low aswell as very highwhole-grain intake are likely
Table 4. ORs for incident prostate cancer by quintiles of plasma alkylresorcinolmetabolite concentration ina nested case–control study of men from the MDC cohort, 1991–2009
OR (95% CI)Plasma alkylresorcinolmetabolites(nmol/L)
No.events Model 1a Model 2b
All prostate cancer (n ¼ 1,010) Median (range) — — —
Q1 0 (0.0–13.1) 190 1.09 (0.85–1.40) 1.13 (0.88–1.45)Q2 24.4 (13.4–34.0) 205 1.23 (0.96–1.57) 1.23 (0.96–1.58)Q3 44.1 (34.1–55.8) 179 1.00 (ref.) 1.00 (ref.)Q4 74.5 (56.6–92.8) 210 1.28 (1.00–1.63) 1.25 (0.97–1.60)Q5 130.3 (93.0–596.2) 226 1.45 (1.14–1.86) 1.41 (1.10–1.80)Low-risk prostate cancer (n ¼ 647) — — — —
Q1 0 (0.0–13.0) 117 0.99 (0.74–1.32) 1.03 (0.77–1.38)Q2 23.9 (13.4–34.0) 132 1.19 (0.90–1.58) 1.21 (0.91–1.61)Q3 44.1 (34.1–55.8) 115 1.00 (ref.) 1.00 (ref.)Q4 75.4 (56.9–92.8) 133 1.22 (0.92–1.61) 1.18 (0.89–1.57)Q5 129.6 (93.0–485.2) 150 1.46 (1.11–1.94) 1.39 (1.05–1.85)High-risk prostate cancer (n ¼ 353) — — — —
Q1 0 (0.0–13.1) 72 1.24 (0.86–1.79) 1.24 (0.86–1.79)Q2 25.8 (13.5–34.0) 71 1.16 (0.80–1.67) 1.14 (0.79–1.64)Q3 43.5 (34.7–54.8) 63 1.00 (ref.) 1.00 (ref.)Q4 73.1 (56.6–91.8) 72 1.18 (0.82–1.70) 1.18 (0.82–1.70)Q5 130.4 (93.2–327.3) 75 1.19 (0.83–1.72) 1.21 (0.84–1.75)Symptomatic prostate cancer (n ¼ 465) — — — —
Q1 0 (0.0–13.1) 84 1.02 (0.73–1.41) 1.04 (0.75–1.45)Q2 24.4 (13.4–34.0) 100 1.23 (0.90–1.69) 1.23 (0.90–1.69)Q3 42.8 (34.1–54.8) 84 1.00 (ref.) 1.00 (ref.)Q4 74.5 (56.9–92.7) 93 1.13 (0.82–1.56) 1.10 (0.79–1.52)Q5 140.3 (93.0–596.2) 104 1.29 (0.94–1.77) 1.25 (0.91–1.72)
aUnconditional logistic regression model adjusted for age and date of study entry.bModel additionally adjusted for height, waist, educational level, smoking status, and energy intake.
Plasma Alkylresorcinol Metabolites and Prostate Cancer Risk
www.aacrjournals.org Cancer Epidemiol Biomarkers Prev; 23(1) January 2014 81
on June 15, 2018. © 2014 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst November 12, 2013; DOI: 10.1158/1055-9965.EPI-13-0878

todiffer in regards to various lifestyle, environmental, andsocioeconomic factors.
ConclusionsIn this nested case–control study of Swedish men, we
found that plasma alkylresorcinol metabolites were pri-marily determined by reported whole-grain intake. Themain conclusion of this study is that high whole-grainintake is unlikely to lower risk of incident prostate cancerbut may be associated with lower mortality from non-prostate cancer causes. The results from this study alsohighlight the problem of excluding alternative explana-tions to findings between diet, lifestyle, and environmen-tal factors in relation to prostate cancer risk. Residualconfounding, detection bias, and undue influences ofcompeting risks may cloud the true associations betweenlifestyle-related risk factors and this disease.
Disclosure of Potential Conflicts of InterestM.J. Tikkanen has a commercial research grant fromFazer Inc. E.Wirf€alt
is a consultant/advisory boardmember of theworking group coordinatingthe revision of the Nordic Nutrition Recommendations (5th edition) underthe Nordic Council of Ministers. No potential conflicts of interest weredisclosed by the other authors.
Authors' ContributionsConception and design: I. Drake, E. Wirf€alt, P. Wallstr€om
Development of methodology: B. Gullberg, H. Adlercreutz, M.J.TikkanenAcquisition of data (provided animals, acquired and managed patients,provided facilities, etc.): A. Bjartell, P. Wallstr€omAnalysis and interpretation of data (e.g., statistical analysis, biostatis-tics, computational analysis): I. Drake, B. Gullberg, P. Wallstr€omWriting, review, and/or revision of themanuscript: I. Drake, E. Sonestedt,B. Gullberg, A. Bjartell, H. Olsson, H. Adlercreutz, M.J. Tikkanen, E.Wirf€alt, P. Wallstr€omAdministrative, technical, or material support (i.e., reporting or orga-nizing data, constructing databases): M.J. Tikkanen, P. Wallstr€omStudy supervision: E. Wirf€alt, P. Wallstr€om
AcknowledgmentsThe authors thank Adile Samaletdin for technical assistance and the
participants of the MDC cohort.
Grant SupportThis studywas supported by the SwedishCouncil forWorking Life and
Social Research, the Swedish Cancer Society, the Albert Pa�hlsson Foun-
dation for Scientific Research, the Gunnar Nilsson Cancer Foundation,Ska
�ne University Hospital – Foundations and Donations, the Malm€o
General Hospital Foundation for the Combating of Cancer, and the Ern-hold Lundstr€om Foundation for Scientific Research.
The costs of publication of this article were defrayed in part by thepayment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely to indicatethis fact.
ReceivedAugust 27, 2013; revisedOctober 10, 2013; acceptedOctober 20,2013; published OnlineFirst November 12, 2013.
References1. Jacobs DR Jr, Gallaher DD. Whole grain intake and cardiovascular
disease: a review. Curr Atheroscler Rep 2004;6:415–23.2. de Munter JS, Hu FB, Spiegelman D, Franz M, van Dam RM. Whole
grain, bran, and germ intake and risk of type 2 diabetes: a prospectivecohort study and systematic review. PLoS Med 2007;4:e261.
3. Aune D, Chan DS, Lau R, Vieira R, Greenwood DC, Kampman E, et al.Dietary fibre, whole grains, and risk of colorectal cancer: systematicreview and dose-responsemeta-analysis of prospective studies. BMJ2011;343:d6617.
4. PereiraMA, JacobsDRJr, Pins JJ, RaatzSK,GrossMD,Slavin JL, et al.Effect of whole grains on insulin sensitivity in overweight hyperinsu-linemic adults. Am J Clin Nutr 2002;75:848–55.
5. Slavin J. Why whole grains are protective: biological mechanisms.Proc Nutr Soc 2003;62:129–34.
6. Adlercreutz H. Lignans and human health. Crit Rev Clin Lab Sci 2007;44:483–525.
7. Hsing AW, Devesa SS. Trends and patterns of prostate cancer: whatdo they suggest? Epidemiol Rev 2001;23:3–13.
8. Gronberg H. Prostate cancer epidemiology. Lancet 2003;361:859–64.9. Hsing AW, Chokkalingam AP. Prostate cancer epidemiology. Front
Biosci 2006;11:1388–413.10. Bylund A, Zhang JX, Bergh A, Damber JE, Widmark A, Johansson A,
et al. Rye bran and soy protein delay growth and increase apoptosis ofhuman LNCaP prostate adenocarcinoma in nudemice. Prostate 2000;42:304–14.
11. Landberg R, Andersson SO, Zhang JX, Johansson JE, Stenman UH,Adlercreutz H, et al. Rye whole grain and bran intake compared withrefined wheat decreases urinary C-peptide, plasma insulin, and pros-tate specific antigen in men with prostate cancer. J Nutr 2010;140:2180–6.
12. Wikstrom P, Bylund A, Zhang JX, Hallmans G, Stattin P, Bergh A. Ryebran diet increases epithelial cell apoptosis and decreases epithelialcell volume in TRAMP (transgenic adenocarcinoma of the mouseprostate) tumors. Nutr Cancer 2005;53:111–6.
13. Drake I, Sonestedt E, Gullberg B, Ahlgren G, Bjartell A, Wallstrom P,et al. Dietary intakes of carbohydrates in relation to prostate cancer
risk: a prospective study in the Malmo Diet and Cancer cohort. Am JClin Nutr 2012;96:1409–18.
14. Nimptsch K, Kenfield S, Jensen MK, Stampfer MJ, Franz M, SampsonL, et al. Dietary glycemic index, glycemic load, insulin index, fiber andwhole-grain intake in relation to risk of prostate cancer. Cancer CausesControl 2011;22:51–61.
15. Egeberg R, Olsen A, Christensen J, Johnsen NF, Loft S, Overvad K,et al. Intake of whole-grain products and risk of prostate cancer amongmen in the Danish Diet, Cancer and Health cohort study. CancerCauses Control 2011;22:1133–9.
16. Suzuki R, Allen NE, Key TJ, Appleby PN, Tjonneland A, Johnsen NF,et al. A prospective analysis of the association between dietary fiberintake and prostate cancer risk in EPIC. Int J Cancer 2009;124:245–9.
17. Ross AB, Kamal-Eldin A, Aman P. Dietary alkylresorcinols: absorption,bioactivities, and possible use as biomarkers of whole-grain wheat-and rye-rich foods. Nutr Rev 2004;62:81–95.
18. Aubertin-LeheudreM,KoskelaA, SamaletdinA, AdlercreutzH. Plasmaalkylresorcinol metabolites as potential biomarkers of whole-grainwheat and rye cereal fibre intakes in women. Br J Nutr 2010;103:339–43.
19. Aubertin-LeheudreM,KoskelaA, SamaletdinA, AdlercreutzH. Plasmaand urinary alkylresorcinol metabolites as potential biomarkers ofbreast cancer risk in Finnish women: a pilot study. Nutr Cancer 2010;62:759–64.
20. Manjer J, Elmstahl S, Janzon L, Berglund G. Invitation to a population-based cohort study: differences between subjects recruited usingvarious strategies. Scand J Public Health 2002;30:103–12.
21. Manjer J, Carlsson S, Elmstahl S, Gullberg B, Janzon L, Lindstrom M,et al. The Malmo Diet and Cancer Study: representativity, cancerincidence and mortality in participants and non-participants. EurJ Cancer Prev 2001;10:489–99.
22. Berglund G, Elmstahl S, Janzon L, Larsson SA. The Malmo Diet andCancer Study. Design and feasibility. J Intern Med 1993;233:45–51.
23. Sandblom G, Dufmats M, Olsson M, Varenhorst E. Validity of apopulation-based cancer register in Sweden–an assessment of data
Drake et al.
Cancer Epidemiol Biomarkers Prev; 23(1) January 2014 Cancer Epidemiology, Biomarkers & Prevention82
on June 15, 2018. © 2014 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst November 12, 2013; DOI: 10.1158/1055-9965.EPI-13-0878

reproducibility in the South-East Region Prostate Cancer Register.Scand J Urol Nephrol 2003;37:112–9.
24. Stocks T, Lukanova A, Rinaldi S, Biessy C, Dossus L, Lindahl B, et al.Insulin resistance is inversely related to prostate cancer: a prospectivestudy in Northern Sweden. Int J Cancer 2007;120:2678–86.
25. Pero RW,Olsson A, Bryngelsson C, Carlsson S, Janzon L, BerglundG,et al. Quality control program for storage of biologically banked bloodspecimens in the Malmo Diet and Cancer Study. Cancer EpidemiolBiomarkers Prev 1998;7:803–8.
26. Koskela A, Samaletdin A, Aubertin-Leheudre M, Adlercreutz H. Quan-tification of alkylresorcinolmetabolites in plasma by high-performanceliquid chromatography with coulometric electrode array detection.J Agric Food Chem 2008;56:7678–81.
27. Wirfalt E, Mattisson I, JohanssonU, Gullberg B,WallstromP, BerglundG. A methodological report from the Malmo Diet and Cancer study:development and evaluation of altered routines in dietary data proces-sing. Nutr J 2002;1:3.
28. Riboli E, Elmstahl S, Saracci R, Gullberg B, Lindgarde F. The MalmoFoodStudy: validity of two dietary assessmentmethods formeasuringnutrient intake. Int J Epidemiol 1997;26:S161–73.
29. Elmstahl S, Gullberg B, Riboli E, Saracci R, Lindgarde F. The MalmoFood Study: the reproducibility of a novel diet history method and anextensive food frequency questionnaire. Eur J Clin Nutr 1996;50:134–42.
30. Elmstahl S, Riboli E, Lindgarde F, Gullberg B, Saracci R. The MalmoFood Study: the relative validity of a modified diet history method andan extensive food frequency questionnaire for measuring food intake.Eur J Clin Nutr 1996;50:143–51.
31. Mattisson I, Wirfalt E, Aronsson CA, Wallstrom P, Sonestedt E, Gull-berg B, et al. Misreporting of energy: prevalence, characteristics ofmisreporters and influence on observed risk estimates in the MalmoDiet and Cancer cohort. Br J Nutr 2005;94:832–42.
32. Sonestedt E,Wirfalt E, Gullberg B, Berglund G. Past food habit changeis related to obesity, lifestyle and socio-economic factors in theMalmoDiet and Cancer Cohort. Public Health Nutr 2005;8:876–85.
33. Soderholm PP, Koskela AH, Lundin JE, Tikkanen MJ, Adlercreutz HC.Plasma pharmacokinetics of alkylresorcinol metabolites: new candi-date biomarkers for whole-grain rye and wheat intake. Am J Clin Nutr2009;90:1167–71.
34. Landberg R, Linko AM, Kamal-Eldin A, Vessby B, Adlercreutz H, AmanP. Human plasma kinetics and relative bioavailability of alkylresorci-nols after intake of rye bran. J Nutr 2006;136:2760–5.
35. Montonen J, Landberg R, Kamal-Eldin A, Aman P, Knueppel S, BoeingH, et al. Reliability of fasting plasma alkylresorcinol concentrationsmeasured 4 months apart. Eur J Clin Nutr 2010;64:698–703.
36. Montonen J, Landberg R, Kamal-Eldin A, AmanP, BoeingH, Steffen A,et al. Reliability of fasting plasma alkylresorcinol metabolites concen-trations measured 4 months apart. Eur J Clin Nutr 2012;66:968–70.
37. Julin B, Wolk A, Johansson J-E, Anderson S-O, Andr�en O, ÅkessonA. Dietary cadmium exposure and prostate cancer incidence: apopulation-based prospective cohort study. Br J Cancer 2012;107:895–900.
38. Wirf€alt E, Mattisson I, JohanssonU, Gullberg B,Wallstr€omP, BerglundG. A methodological report from the Malmo Diet and Cancer study:development and evaluation of altered routines in dietary data proces-sing. Nutr J 2002;1:3.
Plasma Alkylresorcinol Metabolites and Prostate Cancer Risk
www.aacrjournals.org Cancer Epidemiol Biomarkers Prev; 23(1) January 2014 83
on June 15, 2018. © 2014 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst November 12, 2013; DOI: 10.1158/1055-9965.EPI-13-0878

2014;23:73-83. Published OnlineFirst November 12, 2013.Cancer Epidemiol Biomarkers Prev Isabel Drake, Emily Sonestedt, Bo Gullberg, et al.
Control Study−ested CaseIntake and Their Association with Prostate Cancer: A Swedish NPlasma Alkylresorcinol Metabolites as Biomarkers for Whole-Grain
Updated version
10.1158/1055-9965.EPI-13-0878doi:
Access the most recent version of this article at:
Material
Supplementary
http://cebp.aacrjournals.org/content/suppl/2013/11/12/1055-9965.EPI-13-0878.DC1
Access the most recent supplemental material at:
Cited articles
http://cebp.aacrjournals.org/content/23/1/73.full#ref-list-1
This article cites 38 articles, 7 of which you can access for free at:
Citing articles
http://cebp.aacrjournals.org/content/23/1/73.full#related-urls
This article has been cited by 1 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cebp.aacrjournals.org/content/23/1/73To request permission to re-use all or part of this article, use this link
on June 15, 2018. © 2014 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst November 12, 2013; DOI: 10.1158/1055-9965.EPI-13-0878